What helps occupational rehabilitation when the doctor cannot explain the symptoms?
24
What helps occupational rehabilitation when the doctor cannot explain the symptoms? Peter White
-
Upload
maxwell-head -
Category
Documents
-
view
215 -
download
1
description
Biopsychosocial management is best___Remove the barriers to recovery__i.e.Relationships at work or home___Iatrogenic bad healthcare advice___Benefit gap financial incentives___Predictions of non-response to GET___Membership of a self-help group___Sickness benefit___(Peter Denton White does voluntary and paid consultancy work for the U.K. Departments of Health and Work and Pensions, as well as for Swiss Re)
Transcript of What helps occupational rehabilitation when the doctor cannot explain the symptoms?
What helps occupational rehabilitation when the doctor cannot explain the symptoms?
Peter White
Agenda
Symptom defined illnesses (SDIs)The example of chronic fatigue
syndromeBiopsychosocial management is bestPrevention is even better
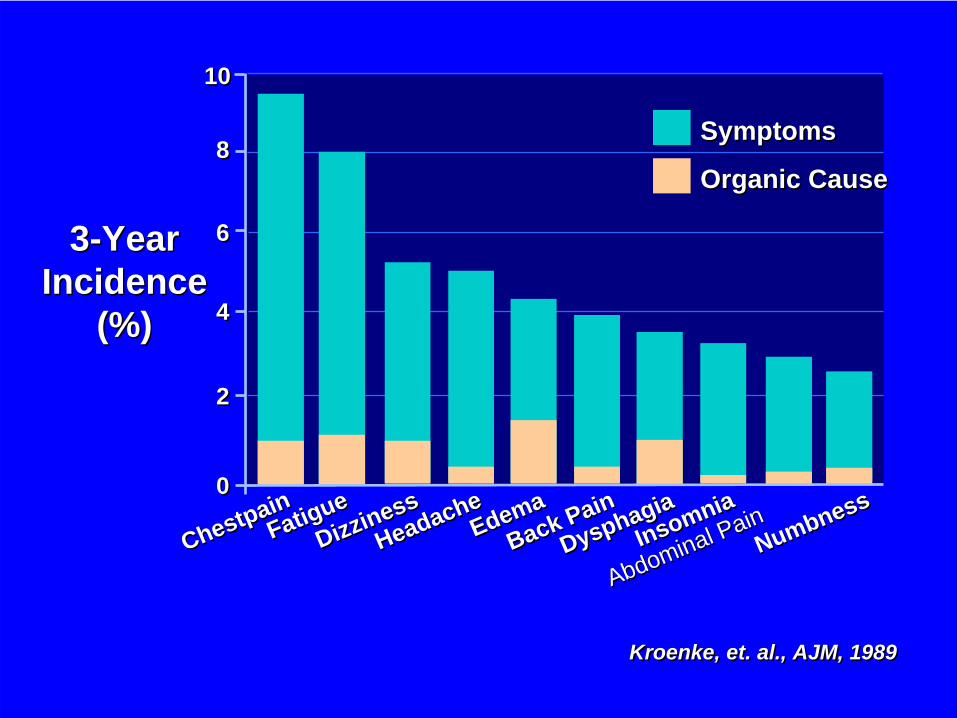
Kroenke, et. al., AJM, 1989Kroenke, et. al., AJM, 1989
Abdominal Pain
Abdominal Pain
3-YearIncidence
(%)
3-YearIncidence
(%)
00
22
1010
44
66
88
ChestpainChestpain
FatigueFatigue
DizzinessDizziness
HeadacheHeadache
EdemaEdema
Back PainBack Pain
DysphagiaDysphagia
InsomniaInsomnia
NumbnessNumbness
SymptomsSymptoms
Organic CauseOrganic Cause
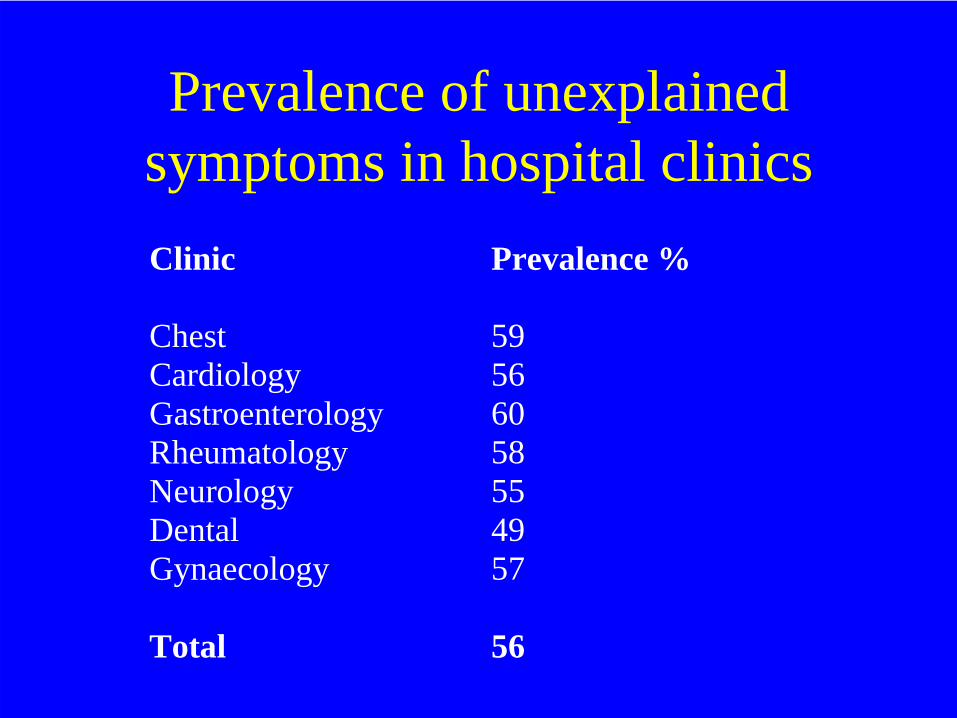
Prevalence of unexplained symptoms in hospital clinicsClinic Prevalence % Chest Cardiology Gastroenterology Rheumatology Neurology Dental Gynaecology
59 56 60 58 55 49 57
Total
56
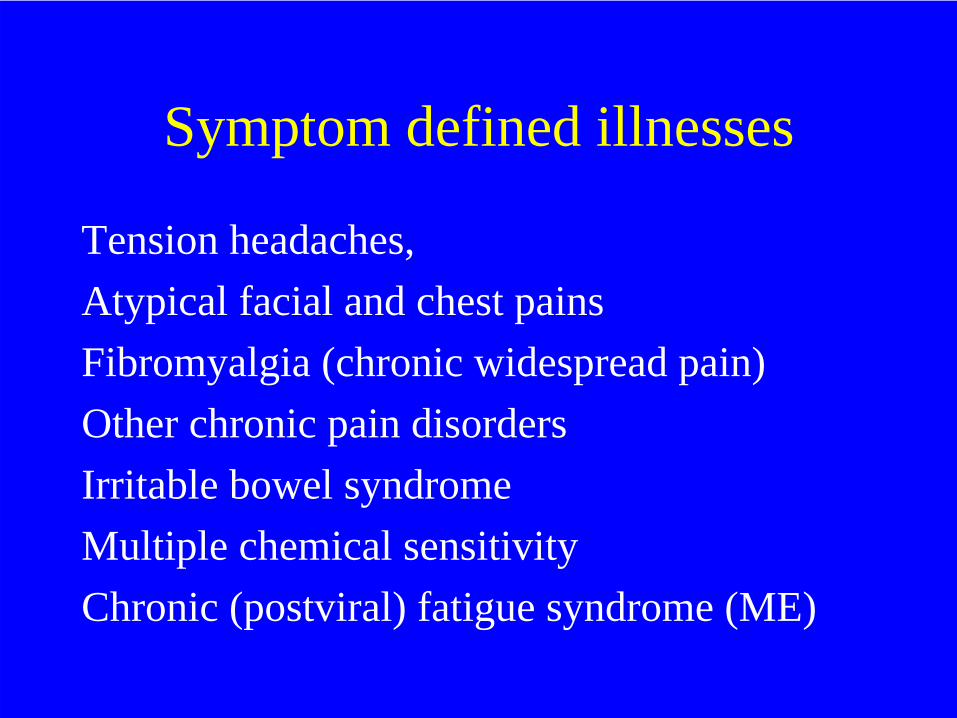
Symptom defined illnesses
Tension headaches,Atypical facial and chest painsFibromyalgia (chronic widespread pain)Other chronic pain disordersIrritable bowel syndromeMultiple chemical sensitivityChronic (postviral) fatigue syndrome (ME)
How common is CFS?
0.2 - 2.6 % population or primary care
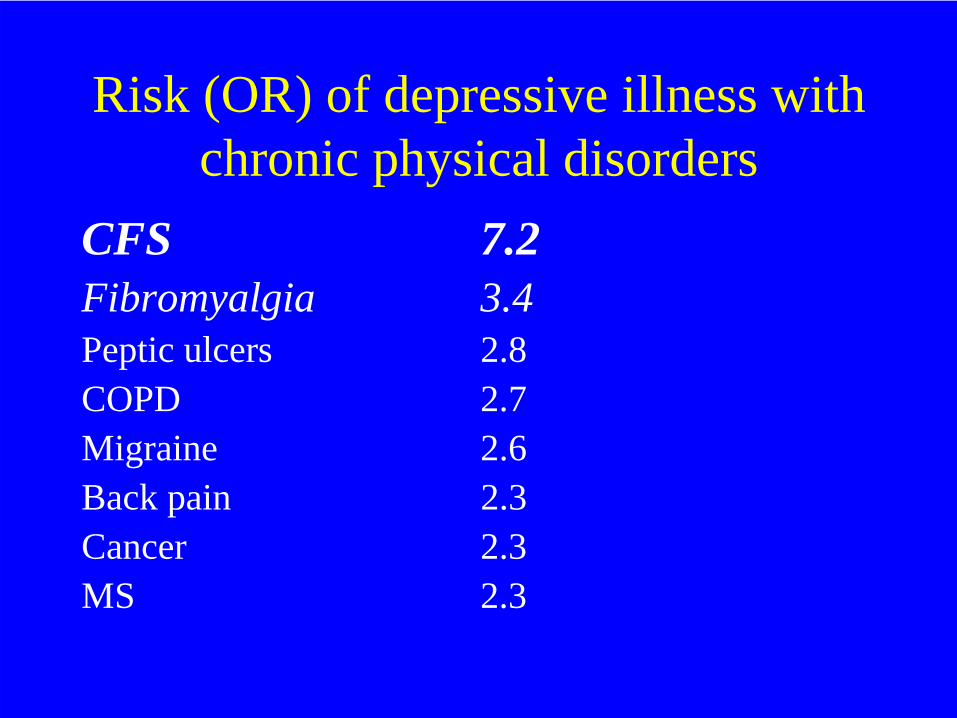
Risk (OR) of depressive illness with chronic physical disorders
CFS 7.2Fibromyalgia 3.4Peptic ulcers 2.8COPD 2.7Migraine 2.6Back pain 2.3Cancer 2.3MS 2.3
UK costs of CFS
118,000 on incapacity benefit19,000 on disability living allowance+ Cost of medical and social care+ Loss of employment
Outcome is poor without treatment
Systematic review of longitudinal studies
5 % (range 0 - 31) recovered by follow up39 % (range 8 - 63) some improvement
Cairns R, Hotopf M, Occup Med 2005
Use the biopsychosocial model
The biopsychosocial model “takes into account the patient, the social content in which he lives and ... the physician role and the health care system.”
George Engel, 1977
Management is biopsychosocial
• Biological e.g. medication, physical rehabilitation
• Psychologicale.g. CBT
Social
Remove the barriers to recovery -
Relationships .. at work or homeIatrogenic .. bad healthcare advice Benefit gap .. financial incentives
The lost art of rehabilitation
We have forgotten not only how to rehabilitate patients, but that we need to do so for the patient to make a full recovery.
Graded exercise therapy for CFS
Exercise = “an activity requiring physical effort”
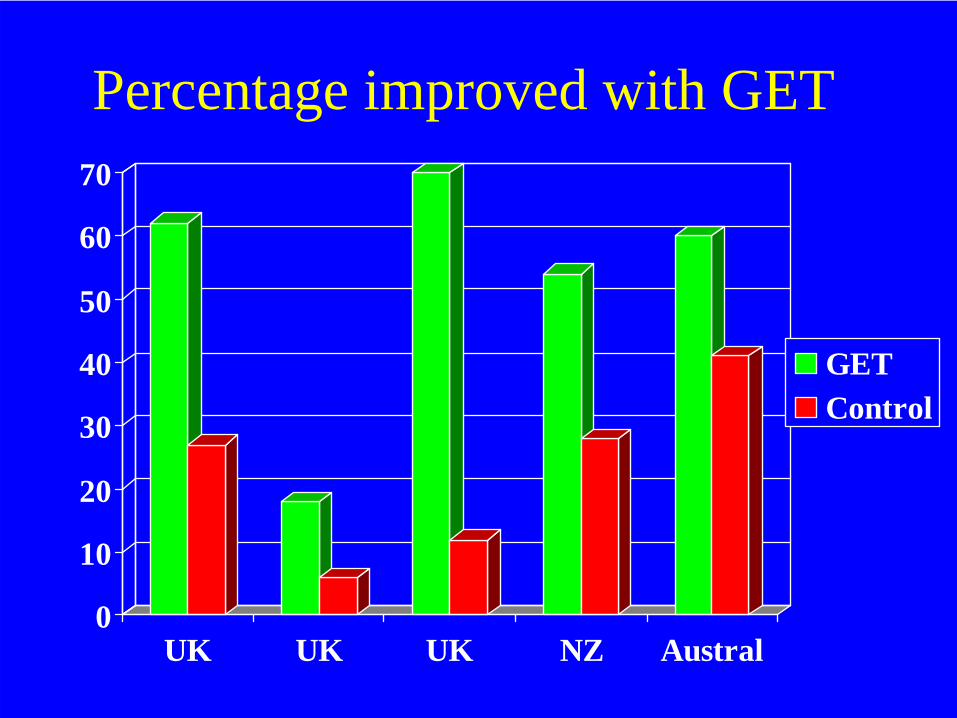
Percentage improved with GET
0
10
20
30
40
50
60
70
UK UK UK NZ Austral
GETControl
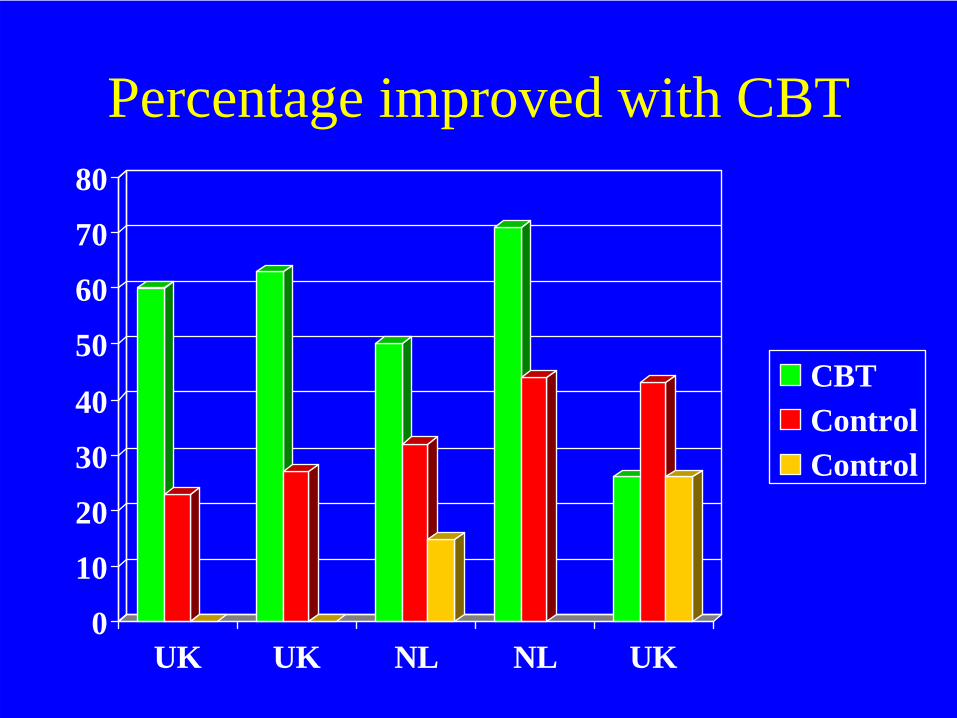
Percentage improved with CBT
0
10
20
30
40
50
60
70
80
UK UK NL NL UK
CBTControlControl
But do these treatments help patients return to work?
“Only cognitive behavior therapy, rehabilitation, and exercise therapy interventions were associated with restoring the ability to work.”
- Even without occupation as the aim.
Systematic review: SD Ross et al, Arch Intern Med 2004
Predictions of non-response to GET
• High psychological distress• Membership of a self-help group• Sickness benefit
R Bentall et al, 2002
Social risks
“If you have to prove you are ill, you can’t get well.” (N Hadler, 1996)
“ME is an incurable disease.”(UK doctor, 2008)
Does the BPS approach work?
• CFS• Low back pain• IBS• Depressive illness• (Cardiac disease)• (DM)

Preventing SDIs
Patients with infectious mononucleosis– Brief rehabilitation, with graded return to
activities– Compared to leaflet
By 6 months, 26% had abnormal fatigue after rehab, compared to 50% of controls.
B Candy et al, 2004