WHAT ELSE? Education is your main focus. But with children in your care for seven hours a day comes...
17
WHAT ELSE? Education is your main focus. But with children in your care for seven hours a day comes the added responsibility of health and safety.
-
Upload
ethelbert-sharp -
Category
Documents
-
view
225 -
download
0
Transcript of WHAT ELSE? Education is your main focus. But with children in your care for seven hours a day comes...

WHAT ELSE?Education is your main focus. But with children in your care for seven hours a day comes the added responsibility of health and safety.

INCIDENTALSWhat are some of those “extra” responsibilities?

RISK MANAGEMENTNotification Form

Principal• Know what occurs on your campus – you want no surprises
• Knowledge for overall awareness – you want to answer questions
• Responsibility to correct causative issues when possible – you may need to report information

What is Risk Management?
When an unusual event occurs on a campus, it is the district’s responsibility to notify our risk management insurance carrier. Risk management means just that: managing risk by looking ahead and spotting opportunities - and threats. When an organization is successfully managing risk it is taking a proactive approach to reduce the likelihood or severity of some unknown occurrence that could result in poor consequences, like additional costs related to injury claims, repairs, etc.

Who does what?Nurse • If involved, completes a separate student
incident/accident report in Synergy and/or LCPS Accident/Exposure report for visitors
• Sends a notification copy of these reports to Finance, Safety/Security and building principal
Administration• Ensures that the witness to the incident completes the risk
management form• Signs and sends a copy to Cindy Esqueda in Finance

The person filling out the form does not need toconcern themselves with information related tocare that may have been given. Again, the nurse sends a separate report to finance, security and the principal for notification purposes anddetailing care rendered
FYI – Incidents oraccidents involvingemployees/subs arehandled through HRand Workers Comp
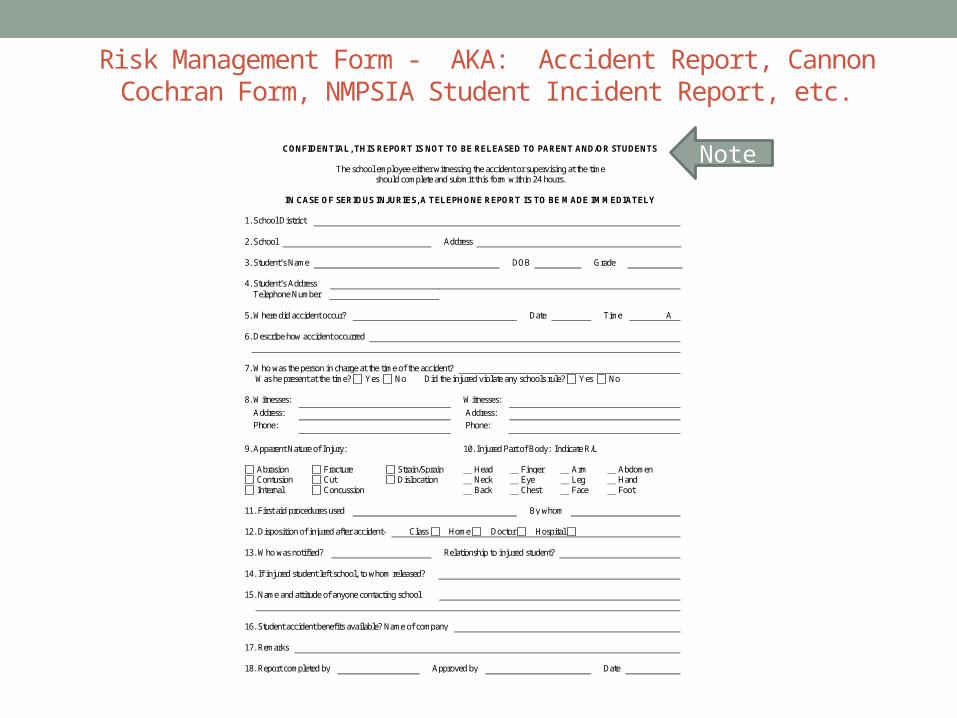
Risk Management Form - AKA: Accident Report, Cannon Cochran Form, NMPSIA Student Incident Report, etc.
NEW MEXICO PUBLIC SCHOOLS INSURANCE AUTHORITY
Cannon Cochran Management Services, Inc. Claims Administrator
P.O. Box 30870 Albuquerque, New Mexico 87190-0870
800-635-0679 505-837-8700 505-888-6901 Fax
CONFIDENTIAL, THIS REPORT IS NOT TO BE RELEASED TO PARENT AND/OR STUDENTS
The school employee either witnessing the accident or supervising at the time
should complete and submit this form within 24 hours.
IN CASE OF SERIOUS INJURIES, A TELEPHONE REPORT IS TO BE MADE IMMEDIATELY
1. School District 2. School Address 3. Student’s Name DOB Grade 4. Student’s Address Telephone Number 5. Where did accident occur? Date Time A 6. Describe how accident occurred 7. Who was the person in charge at the time of the accident? Was he present at the time? Yes No Did the injured violate any schools rule? Yes No 8. Witnesses: Witnesses:
Address: Address:
Phone: Phone:
9. Apparent Nature of Injury: 10. Injured Part of Body: Indicate R/L
Abrasion Fracture Strain/Sprain Head Finger Arm Abdomen Contusion Cut Dislocation Neck Eye Leg Hand Internal Concussion Back Chest Face Foot
11. First aid procedures used By whom 12. Disposition of injured after accident- Class Home Doctor Hospital 13. Who was notified? Relationship to injured student? 14. If injured student left school, to whom released? 15. Name and attitude of anyone contacting school 16. Student accident benefits available? Name of company 17. Remarks 18. Report completed by Approved by Date
Note

FIELD TRIPSNotification

Request, Rationale, and Notification all on one form
Per LCPS Board Policy IJOA:
“Staff should complete LCPS Form IJOA E-6: Field Trip Request, Rationale and Notification Form, to ensure that prior to any proposed field trip; 1) administrative approval has been received; 2) all appropriate school staff have been notified, 3) funding has been secured; 4) transportation has been secured; 5) scheduling has been completed; and 6) appropriate rationale has been provided.”

What does this have to do with health and safety?
Involved parties will have the opportunity to address aspects of student needs. For example:
• Notification of cafeteria – students with food allergies will be provided the proper lunch
• Notification of transportation – students with mobility needs will be accommodated
• Notification of nurse – students with health conditions will have their medications or other health related items available and staff will receive proper training on use should care be needed. In most cases, the first aid kits are also received from the nurse.

Las Cruces Public Schools
Form IJOA-E6
Field Trip Request, Rationale and Notification
Requesting teacher(s): _________________________________Cell phone #: ________________Grade: ________Date: __________
Date of field trip: _________________________________________Departure time: ______________Return time: ______________
Field trip destination/address: ___________________________________________________________________________________
EPSS justification for trip: _____________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
# of students participating: __________Classes participating (list teachers): _____________________________________________
Mode of transportation: Walking _______ Bus _______
# of buses requested: _________Transportation to be paid by: _________________________________________________________
Fee/entry cost for trip destination: Y___ N ___ How will it be paid? __________________________________________________
Complete the above portion and turn into your school administration for initial approval. Proceed with bottom portion after initial approval.
_________________________________ Approved Disapproved Date: ______________________ Principal’s signature (circle one)
________________________________ Comments: ____________________________________________________________ Asst. Principal’s signature ____________________________________________________________
Please notify the following staff members well before of your scheduled field trip and get their initials or signatures:
Cafeteria _________ Sack lunches needed? _______ (two weeks advance notice required)
Nurse ___________ Special medical needs addressed/First aid kit (two weeks advance notice required)
Secretary ________ Fees collected Y___ N ___
Additional staff:
P.E. teacher ________ Librarian ________ Music ________ Counselor ________ Art ________
Computer lab ________ Special education teachers (OT, PT, SLP, Psychologist) ________ ESL ________
Final Approval:
_________________________________ Approved Disapproved Date: ______________________ Principal’s signature (circle one)
________________________________ Asst. Principal’s signature Funding source: __________________________________________________ Transportation cost: _________________________

PERMISSION FOR MUTUAL EXCHANGE OF INFORMATIONGathering Health Information

Medical Provider to Medical Provider• Several laws exist related to the protection of an
individual’s health information.• We must follow those laws.• Some providers charge a fee to provide written medical
information that may be necessary to provide care for a child at school, i.e., seizure action plan, asthma action plan, etc.
• Other school staff members may need medical information in order to address the educational needs of students they serve.

Continued…• Medical information should only be shared between
medical persons. • The Permission for Mutual Exchange of Information form
is a Health Services Department, not a district, form.• When other district employees have a need for health
information related to their educational work with a student, they must “without exception” contact the school nurse to obtain that information. (JLC-R: Student Health Services)

Continued…• If the information needed is from a provider that charges a
fee, it must be determined ahead of time who will pay that fee (depending on “why” the information is needed the payer may be the principal, Sped Department or Health Services)
• Approval signatures and PO# must be obtained before the form is submitted to the provider.
For more information, please refer to the regulation for Student Health Services Policy JLC-R: Student Health Services, II. Guidelines, section H. Student Health Records, #3. Permission for Mutual Exchange of Information Form

Report of Examination
Diagnosis: Current Medications: Recommendations to School:
________________________________________________________________________________________
LCPS Form JLC-E1: Health Services
Permission for Mutual Exchange of Information
Anyone using this form shall, without exception, contact the school nurse. This form is available only from the school nurse, and is not to be duplicated.
Student:_______________________________________ Parents:__________________________________________
DOB:_________________________________________ Requested by:______________________________________
School:________________________________________ Provider:__________________________________________
Information Requested and Purpose:
_____________________________________________________
School Nurse Signature Date
_____________________________________________________
Administrator Signature Health Services Department Director Signature P.O.#
I hereby authorize the mutual exchange of information regarding my child between LCPS and __________________________________________________________for the reason stated above. ________________________________________________________________________________ Parent’s Signature Date White – Health Services LCPS Form E-1: Health Services Permission for Mutual Exchange of Information Yellow – School Nurse Revised 6/14
Please Return To: Health Services Dept. May be faxed to a dedicated line Las Cruces Public Schools Fax: 575-527-5886 505 S. Main St., Suite 249 Las Cruces NM 88001