What Do We Mean by Co- - Cone Health Foundation · Challenges in Treating Co-Occurring Disorders...
28
Transcript of What Do We Mean by Co- - Cone Health Foundation · Challenges in Treating Co-Occurring Disorders...

What Do We Mean by CoWhat Do We Mean by Co--Occurring Disorders?Occurring Disorders?
Different terms are used such as co-occurring or co-morbidCan be used to refer to:– mental health and physical health– mental health and/or substance abuse and/or
developmental disabilities– co-occurring mental health diagnoses

Why Should We Focus on CoWhy Should We Focus on Co--Occurring Disorders?Occurring Disorders?
The rule rather than the exception (Armstrong & Costello, 2007)Differences in incidence due to: how you measure; nature of population served (e.g., juvenile justice/criminal justice, homeless); sophistication of psychiatric diagnostic methods used (e.g., interview versus checklist) and severity of diagnoses included (e.g., major depression vs.dysthymia)

Rates of CoRates of Co--OccurrenceOccurrenceEstimates of psychiatric co-morbidity among clinical populations in substance abuse treatment settings range from 20-80% (Merikangas et al., 1998; SAMHSA, TIP 42)Estimates of substance use co-morbidity among those in mental health treatment settings range from 10-35%20% of the general population with a substance use disorder also had one or more mood disorders, and 18% had an anxiety disorder (Flynn & Brown, 2008)Young adults (18-25) were found to be most vulnerable to co-occurring problems (Chan, Dennis, & Funk, 2008)
Rates of CoRates of Co--OccurrenceOccurrenceNational Co-Morbidity Survey– 42.7% of individuals with a 12-month addictive disorder
had at least one 12-month mental disorder– 14.7% of individuals with a 12-month mental disorder
had at least one 12-month addictive disorderEpidemiological Catchment Area Survey– 47% of individuals with schizophrenia also had a
substance use disorder; more than 4 times as likely as general population
– 61% of individuals with bi-polar disorder also had a substance use disorder, more than 5 times as likely as general population
Challenges in Treating Challenges in Treating CoCo--Occurring DisordersOccurring Disorders
Varies by severity, chronicity,symptomotology, degree of impairment, and motivation to address the problemPhysical safety and overall health risks are greater; the impairment of life skills is greater; and the chances for successful treatment are much lessMore likely to receive treatment for their mental health alone (34.3%) than for their substance abuse alone (4 1%) or for both
Challenges in Treating CoChallenges in Treating Co--Occurring DisordersOccurring Disorders
Substance abuse treatment helps to reduce the frequency of use and the number of abuse/dependence symptoms but typically only has indirect impact on emotional and behavioral problems (Dennis, 2004)Psychiatric treatment alone for those with mood disorders and co-occurring substance use disorders does not significantly reduce substance use, especially among youth (Geller et al., 1998)

“There is no single locus of responsibility for people with COD. The mental health and substance abuse treatment systems operate independently of one another, as separate cultures, each with its own treatment philosophies, administrative structures, and funding mechanisms. This lack of coordination means that neither consumers nor providers move easily among service settings.”NASMHPD/NASADAD, 1999; SAMHSA/CSAT TIP 42, 2005

Treatment System Paradigms of Treatment System Paradigms of CoCo--OccurringOccurring
–Independent, disconnected–Sequential, disconnected –Parallel, connected–Integrated

Treatment ModelsTreatment ModelsIndependent-Disconnected
Sequential-Disconnected
Result of very different and somewhat antagonistic systemsContributed to by different funding streamsFragmented, inappropriate and ineffective care
Treat SA Disorder, then MH disorderTreat MH Disorder, then SA disorderUrgency of needs often makes this approach inadequateDifficult to keep engaged

Treatment Models Treatment Models –– Parallel Parallel ModelModel
– Treat SA disorder in SA system, while concurrently treating MH disorder in MH system, connecting treatments with ongoing communication
– Easier said than done– Differences in terms, cultures, and training between
systems– Logistics of getting to appointments challenging– Increased chance of conflicting recommendations
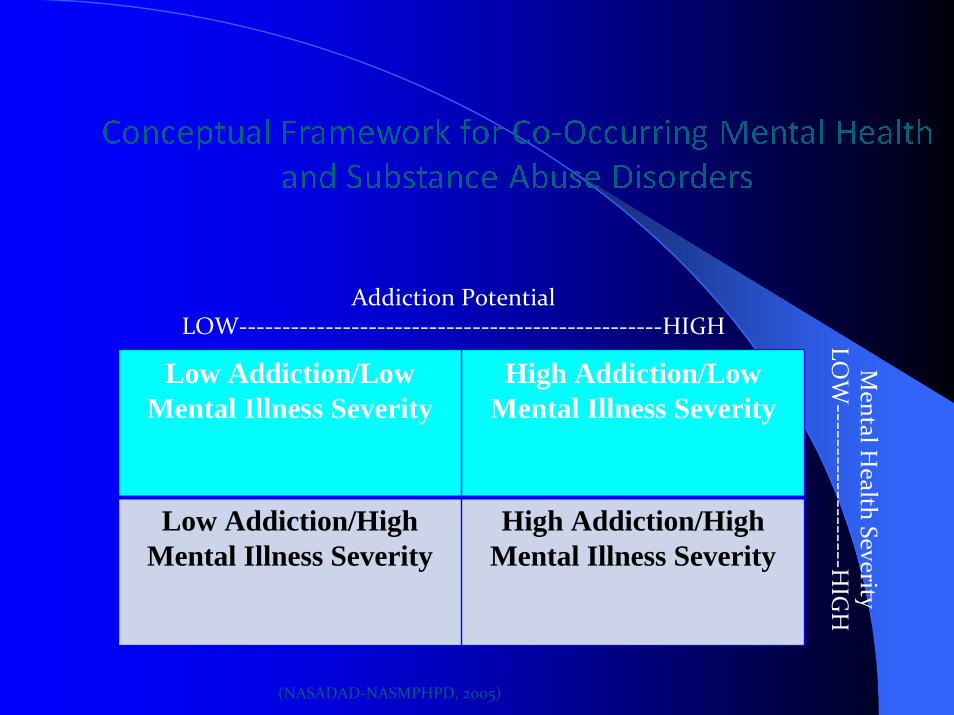
Addiction PotentialLOW‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐HIGH
Low Addiction/Low Mental Illness Severity
High Addiction/Low Mental Illness Severity
Low Addiction/High Mental Illness Severity
High Addiction/High Mental Illness Severity
Mental H
ealth SeverityLO
W‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐H
IGH
(NASADAD‐NASMPHPD, 2005)


Assumptions of an Integrated Model Assumptions of an Integrated Model Conceptual FrameworkConceptual Framework
All individuals fall along this spectrum of substance use and mental health-related symptoms.Supports service coordination by severity rather than by diagnostic category.More likely to be successful in recovery if receive integrated treatment (both mental health and substance abuse at the same time and in the same setting)SAMHSA’s Co-Occurring Center for Excellence/Co-Occurring Disorders Initiative (http://coce.samhsa.gov/)

Comprehensive, Continuous, Integrated Comprehensive, Continuous, Integrated Systems of Care Model (CCISCSystems of Care Model (CCISC))
State LevelAlaskaArizonaDistrict of Columbia MaineMarylandNew MexicoVermontCO-SIG (LA, HI, AK, PA)
Network LevelMid-Valley Behavioral Care Network, OregonMental Health Systems, CaliforniaSouthwest Counseling, Michigan
City/County LevelSan Diego County, CaliforniaBirmingham, AlabamaLynchburg, VirginiaKent County, MichiganDetroit, MichiganBay City, MichiganTampa, FloridaBroward County, FloridaVictoria, British ColumbiaWinnipeg, ManitobaWorcester County, MarylandBlair County, Pennsylvania

Addressing CoAddressing Co--Occurring Disorders within a Occurring Disorders within a System of Care Framework: System of Care Framework:
Six Guiding PrinciplesSix Guiding Principles
Principle 1: Co-occurring disorders (COD) are to be expected in all behavioral health settings, and system planning must address the need to serve people with COD in all policies, regulations, funding mechanisms, and programming.
Principle 2: An integrated system of mental health and addiction services that emphasizes continuity and quality is in the best interest of consumers, providers, programs, funders, and systems.
(Center for Substance Abuse Treatment, 2007)

Addressing Co‐Occurring Disorders within a System of Care Framework:
Six Guiding Principles
Principle 3: The integrated system of care must be accessible from multiple points of entry (i.e., no wrong door) and be perceived as caring and accepting by the consumer.
Principle 4: The system of care for COD should not be limited to a single “correct” model or approach.
(Center for Substance Abuse Treatment, 2007)

Addressing CoAddressing Co--Occurring Disorders within a Occurring Disorders within a System of Care Framework: System of Care Framework:
Six Guiding PrinciplesSix Guiding Principles
(Center for Substance Abuse Treatment, 2007)
Principle 5: The system of care must reflect the importance of the partnership between science and service, and support both the application of evidence- and consensus-based practices for persons with COD and evaluation of the efforts of existing programs and services.
Principle 6: Behavioral health systems must collaborate with professionals in primary care, human services, housing, criminal justice, education, and related fields in order to meet the complex needs of persons with COD.
-

Prevention of CoPrevention of Co--Occurring Occurring DisordersDisorders
Limited research but appears that risk factors for mental and substance abuse disorders may be identical, (e.g. low socioeconomic status, family conflict, exposure to violence)Programs designed to prevent one disorder may prevent or forestall development of the other

Prevention of CoPrevention of Co--Occurring Occurring DisordersDisorders
May be especially true for adolescents where emotional and behavioral problems, social problems, and risky health behaviors often co-occur as an organized pattern of adolescent risk factors (Greenberg et al., 2000)Children and adolescents already experiencing serious mental disorders are at heightened risk for substance abuse disorders, suggesting a "window of opportunity“ to prevent the development of co-occurring substance abuse disorders in these youth by intervening early (SAMHSA, 2000; Ziedonis, 1995)
Prevention of CoPrevention of Co--Occurring Occurring DisordersDisorders
For adults, key life changes may precipitate mental and/or substance abuse disorders in vulnerable individuals (e.g., older adults and prescription drug misuse and alcohol-related problems, as well as for depression and suicide). Prevention programs that include outreach and support as well as early identification and intervention can help increase the protective factors and may prevent or deter development of more serious problems or exacerbation of symptoms
Essential Elements to Treating Essential Elements to Treating CoCo--Occurring Occurring -- SAMHSASAMHSA
Screening and Assessment of Both Mental Health and Substance Abuse SymptomsKnowledge of Diagnostic Categories Across Mental Health and Substance AbuseEnhanced StaffingTraining On and Use of Appropriate Psychotropic Medications

Essential Elements to Treating Essential Elements to Treating CoCo--Occurring Occurring -- SAMHSASAMHSA
Treatments that Utilize Evidence-Based Approaches Proven to Be Successful with Both MH and SA– Motivational Interviewing– Contingency Management– Cognitive-Behavioral Therapy– Assertive Community Treatment– Intensive Case Management
Community-Based Dual Recovery Self-Help Groups
http://mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/cooccurring/

Develop Community Action Develop Community Action Strategic PlanStrategic Plan
Support community dialogueIncrease awareness of rates of co-occurringBuild capacity to deliver integrated mental health/substance abuse treatment by focusing on integrated services, integrated system or both

Suggested Action StepsSuggested Action Steps
– Expand SA treatment to include MH; expand MH to include SADeliver integrated treatment, particularly in situations where one knows high likelihood of co-occurringUtilize shared case management models, existing local service coalitions, and interagency task forces
Action StepsAction StepsSupport Workforce Development Efforts
– Training (In-Service and AHEC) related to co-occurring disorders (e.g., educational, assessment, and treatment) and knowledge of the availability of services available to and needs of those with substance abuse and/or mental disorders
– Expanding the focus to include discussions among self-help and community provider groups regarding co-occurring disorders (modeled after local Say-It chapter)
– Monthly provider meetings on evidence-best practices around co-occurring models and specific interventions

Contact InformationContact InformationDr. Kelly Graves: [email protected] Buford: [email protected]. Sonja Frison: [email protected] Ireland: [email protected]. Terri Shelton: [email protected]
330 S. Greene StreetSuite 200Greensboro, NC 27401336-217-9713