
What Clinicians Need to Know About Trauma
68
1 What Clinicians Need to Know About Trauma Amelia Roeschlein, DSW, MA, LMFT National Council for Mental Wellbeing June 17, 2021
Transcript of What Clinicians Need to Know About Trauma

1
What Clinicians Need to Know
About Trauma
Amelia Roeschlein, DSW, MA, LMFT
National Council for Mental Wellbeing
June 17, 2021

2
Housekeeping
• You will be muted automatically upon entry. Please
keep your phone line muted for the duration of the
webinar.
• Webinar is being recorded and will be archived for
future viewing at www.pcssNOW.org within 2 weeks.
• Submit questions in the Q&A box at the bottom of
your screen.

3
Amelia Roeschlein, DSW, MA, LMFT
Consultant
National Council for Mental Wellbeing
Today's Presenter

4
Disclosures
• Dr. Roeschlein has no disclosures.

5
Target Audience
• The overarching goal of PCSS is to train healthcare
professionals in evidence-based practices for the
prevention and treatment of opioid use disorders,
particularly in prescribing medications, as well for
the prevention and treatment of substance use
disorders.

6
Educational Objectives
• At the conclusion of this activity participants should be able to:
▪ Describe the impact of trauma
▪ Explain the connection between trauma and substance use
▪ Provide two trauma-informed strategies of engagement with clients with substance use disorders

7
Overview
• Overview of Trauma
▪ Prevalence and impact
▪ Trauma and the human
stress response
▪ Trauma and its
connection to addiction
• Becoming Trauma-Informed
in Your Daily Work

8
Why Address Trauma Now?

9
Trauma and Opioid Use
• Exposure to traumatic events is particularly common among individuals with opioid use disorders. A national survey in Australia found very high rates of trauma among individuals with opioid use disorders compared to individuals without an SUD, 87.8% vs. 56.8% respectively after controlling for age and sex
https://pubmed.ncbi.nlm.nih.gov/16585440/
• Among a consecutive sample of 113 treatment-seeking opioid-dependent outpatients seeking buprenorphine treatment, the majority (80.5%) reported a history of childhood sexual, physical, or emotional abuse, physical neglect, or violent trauma
https://pubmed.ncbi.nlm.nih.gov/19197597/

10
Individual trauma results from an , series of events, or
set of circumstances that is by an individual
as overwhelming or life-changing and that has profound
on the individual’s psychological development or well-being,
often involving a physiological, social, and/or spiritual impact.
Definition (SAMHSA Experts 2012) includes
eventexperienced
effects
three key elements
What is Trauma?
https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf
11

12
Intergenerational (Historical) Trauma
“Cumulative emotional and psychological wounding,
over the lifespan and across generations, emanating
from massive group trauma experiences.”
Heart, M. Y. (2003). The Historical Trauma Response Among Natives and Its
Relationship with Substance Abuse: A Lakota Illustration. Journal of
Psychoactive Drugs, 35(1), 7-13. doi:10.1080/02791072.2003.10399988

13
Intergenerational/ Historical Trauma Events
Genocides Slavery Pandemics Massacres
Prohibition/destruction of cultural practices
Discrimination/Systemic prejudice
Forced relocation

14
Intergenerational (Historical)
Trauma Effects

15
Historical Trauma Perpetuated Today
Microaggressions are everyday experiences of discrimination, racism, and daily hassles that are targeted at individuals from diverse cultural groups (Evans-Campbell, 2008).
• Using endearments
• Same behavior, different description
• Benevolent Sexism
• Underestimating
• Attribution Bias
Evans-Campbell T. Historical trauma in American Indian/Native Alaska
communities: a multilevel framework for exploring impacts on
individuals, families, and communities. J Interpers Violence. 2008
Mar;23(3):316-38. doi: 10.1177/0886260507312290. PMID: 18245571.

16
A Client’s Journey
17
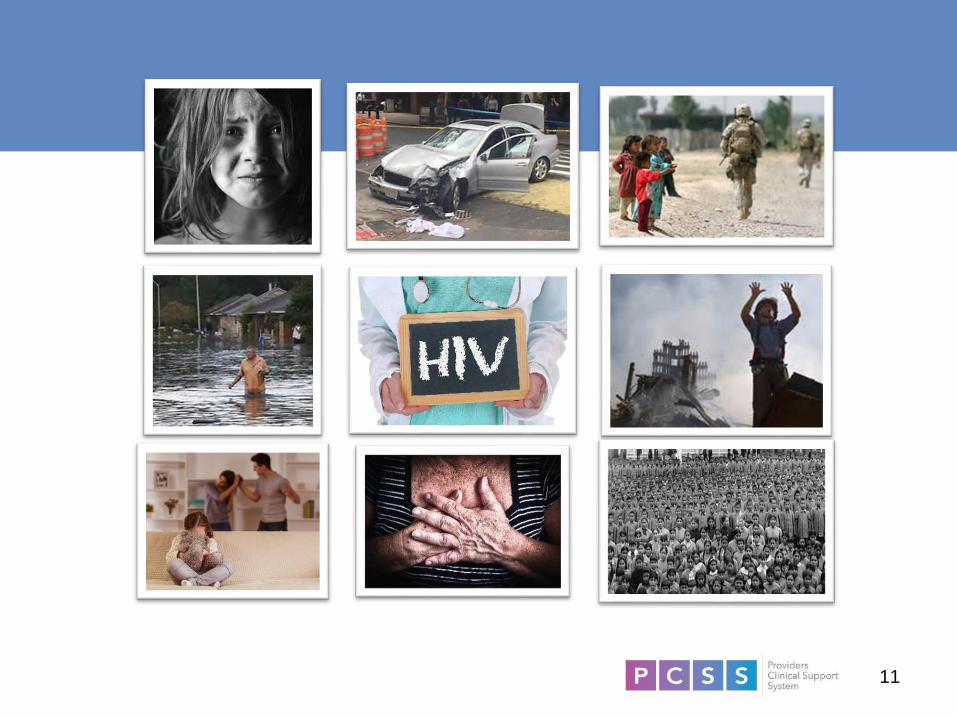
Current Landscape
According to the National Institute of Mental Health, “members of racial and ethnic minority groups in the U.S. are less likely to have access to mental health services, less likely to use community mental health services, more likely to use inpatient hospitalization and emergency rooms, and more likely to receive lower quality care.”1
• Within psychiatry, it has been shown that racial minorities are less likely to achieve symptom remission and are more likely to be chronically impaired given a mental health diagnosis.2
• Bias and racism have been identified as key factors contributing to these inequities. The legacy of slavery and racism, as well as the current realities of racial oppression and violence, has uniquely impacted the mental health of African Americans.3
1https://www.ncsl.org/Portals/1/HTML_LargeReports/DisparitiesBehHealth_Final.htm#:~:text=According%20to%20t
he%20National%20Institute,and%20more%20likely%20to%20receive
2https://academic.oup.com/swr/article-abstract/36/1/41/1646733?redirectedFrom=fulltext
3https://www.mededportal.org/doi/pdf/10.15766/mep_2374-8265.10618

18
Current Landscape(2)
• Additionally, African Americans have higher rates of severe depression, yet lower rates of treatment compared to white populations. 1
• African Americans are less likely to receive office-based counseling for psychological stressors and are more likely to be seen in emergency rooms.2
• The disproportionate diagnosis of schizophrenia among African Americans persists today, and they are more likely to be treated with antipsychotic medications that can have lasting, negative side effects.3
1https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1199525/2https://archive.ahrq.gov/research/findings/nhqrdr/nhdr10/nhdr10.pdf3https://www.ncsl.org/Portals/1/HTML_LargeReports/DisparitiesBehHealth_Final.htm#:~:text
=According%20to%20the%20National%20Institute,and%20more%20likely%20to%20receive

19
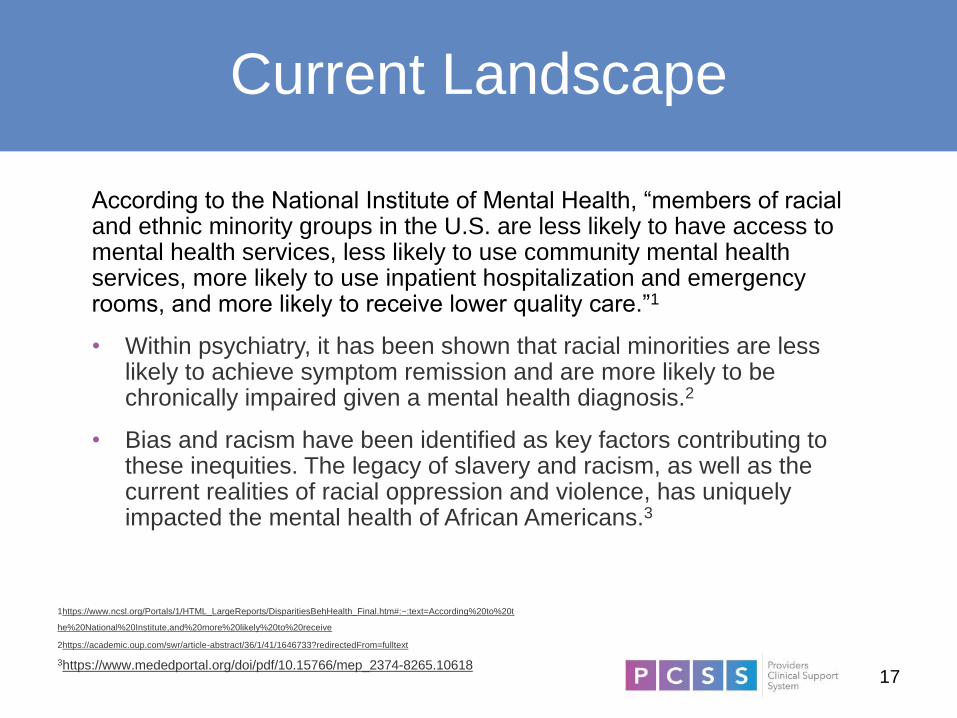
➢Worldview
➢Spirituality
➢Identity
Trauma Shapes Our Beliefs
20https://www.echotraining.org/we-love-science/
Hedges, F. (2012). Fight or Flight. Retrieved from
https://www.acesconnection.com/blog/fight-or-flight-infographic.

21
Impact of Trauma on Behavior
Triggers
External reminders
of traumatic event
• Smell
• Sound
• Sight
• Touch
• Taste
Internal reminders
of traumatic event
• Emotions
• Thoughts

22
Loneliness
Ali, S. (2018, July 12). What You Need to Know About the Loneliness
Epidemic. Retrieved from https://www.psychologytoday.com/us/blog/modern-
mentality/201807/what-you-need-know-about-the-loneliness-epidemic

23
The Elephant in the Room
AngerDifficult concentrating
Physical Illness
Hyper arousal
Low self-esteem
Avoidant behavior
Traumatic grief
Mistrust
Trauma re-enactment
Depression
Sensory sensitivity
Dissociation
Aggression
ShameNeed to control
Inattention
Persistent irritability
Defiance
Difficulty forming relationships
Disrupted MoodRegressive behavior
Perfectionism
Fear
Guilt
Sleep problems
24
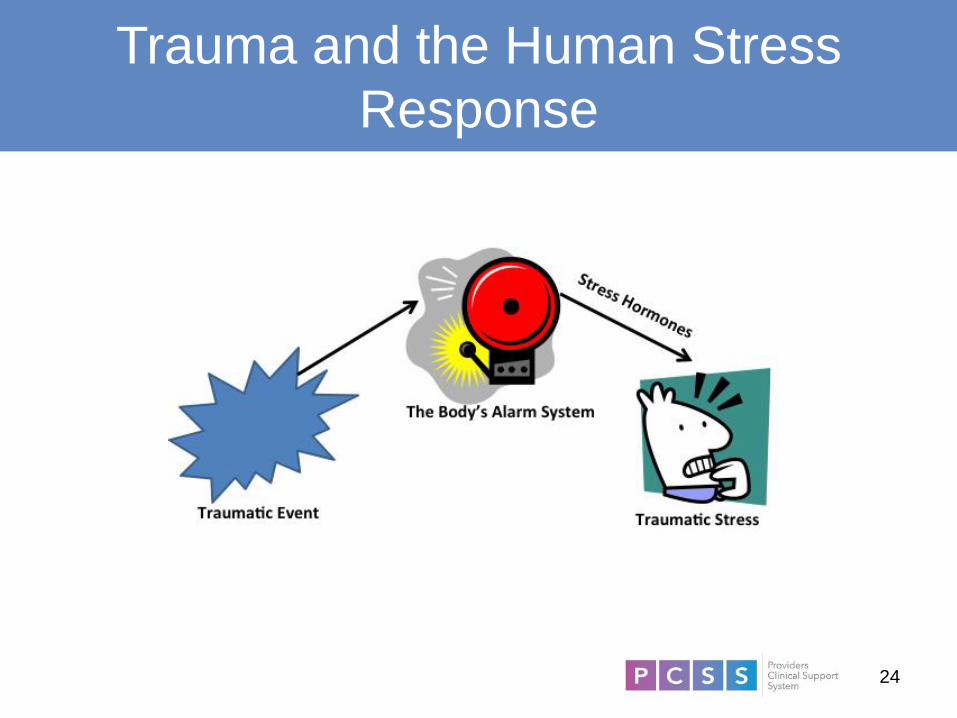
Trauma and the Human Stress
Response
25
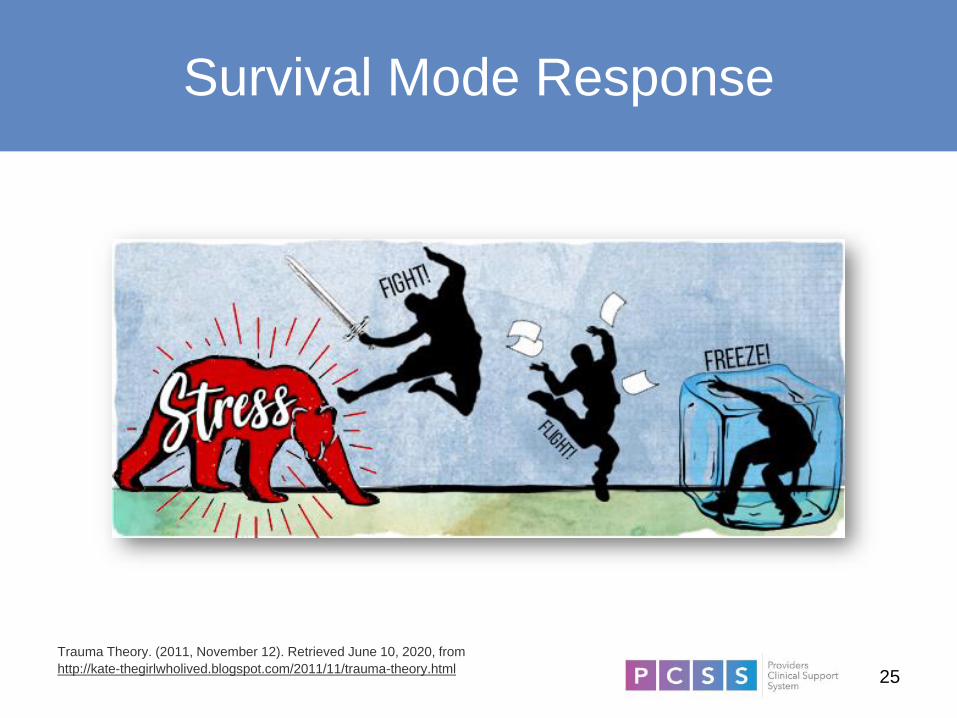
Survival Mode Response
Trauma Theory. (2011, November 12). Retrieved June 10, 2020, from
http://kate-thegirlwholived.blogspot.com/2011/11/trauma-theory.html
26
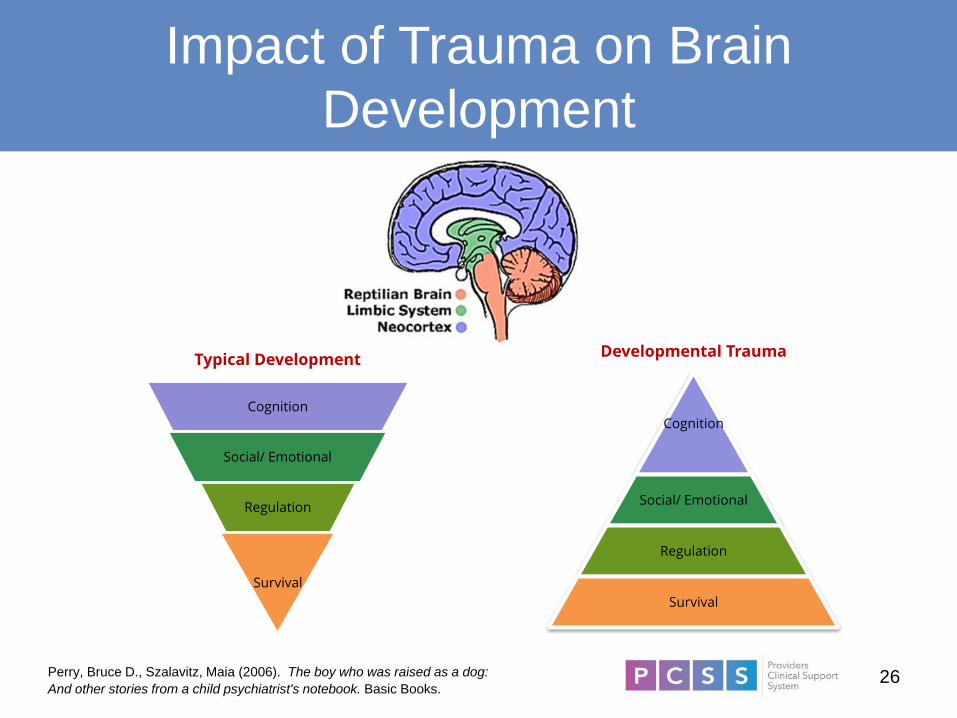
Cognition
Social/ Emotional
Regulation
Survival
Cognition
Social/ Emotional
Regulation
Survival
Typical DevelopmentDevelopmental Trauma
Impact of Trauma on Brain
Development
Perry, Bruce D., Szalavitz, Maia (2006). The boy who was raised as a dog:
And other stories from a child psychiatrist's notebook. Basic Books.

27
Inability to
• Respond
• Learn
• Process
Survival Mode Response

28
How Childhood Trauma Can Make You
a Sick Adult
Davis, B. (Director). (2015). How Childhood Trauma Can Make You A Sick
Adult [Video file]. Retrieved from http://mentalhealthchannel.tv/episode/how-
childhood-trauma-can-make-you-a-sick-adult
29
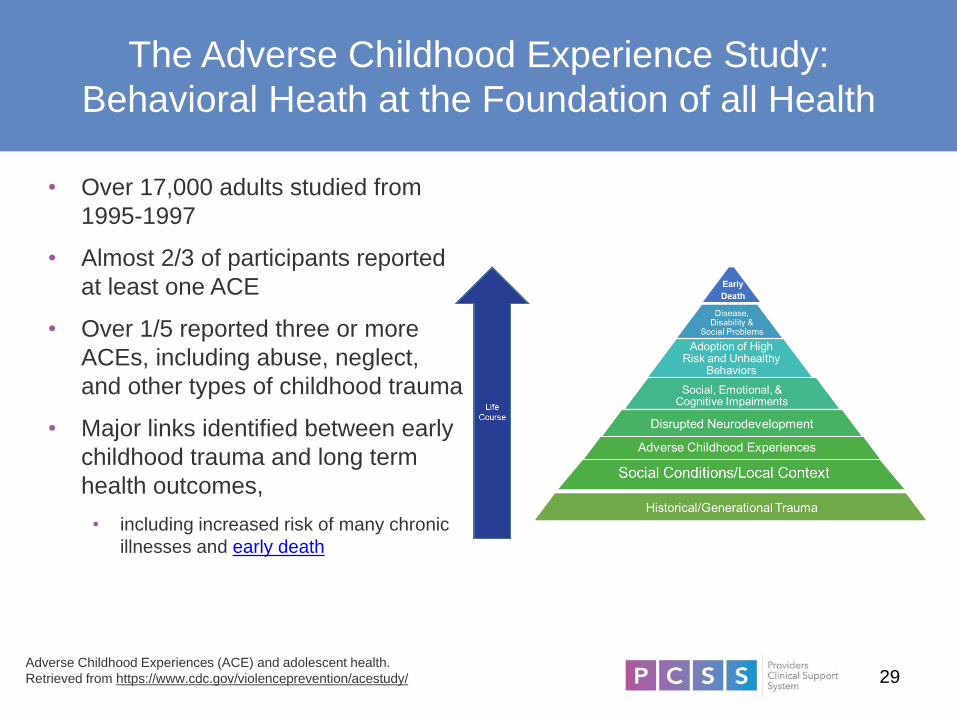
The Adverse Childhood Experience Study:
Behavioral Heath at the Foundation of all Health
• Over 17,000 adults studied from
1995-1997
• Almost 2/3 of participants reported
at least one ACE
• Over 1/5 reported three or more
ACEs, including abuse, neglect,
and other types of childhood trauma
• Major links identified between early
childhood trauma and long term
health outcomes,
• including increased risk of many chronic
illnesses and early death
Adverse Childhood Experiences (ACE) and adolescent health.
Retrieved from https://www.cdc.gov/violenceprevention/acestudy/

30https://www.sciencemag.org/news/2019/07/parents-emotional-trauma-may-change-
their-children-s-biology-studies-mice-show-how
Epigenetics

31
Dose gets bigger
Re
spo
nse
ge
ts b
igg
er
Severe obesity 1.6 xDiabetes 1.6 xCigarette Smokers 2.0 xFair/poor health 2.2 xHepatitis/jaundice 2.4 xHad an STD 2.5 x50+ intercourse partners 3.2 x COPD 3.9 xDepressed 2 weeks 4.6 xIllegal drug use 4.7 xAlcoholic 7.4 xInjected drugs
10.3 xSuicide attempt 12.2 x
Dose-Response Relationship:
More ACEs = More Disease
National Center for Injury Prevention and Control, Division of Violence
Prevention. (n.d.). Adverse Childhood Experiences (ACEs). Retrieved from
https://www.cdc.gov/violenceprevention/acestudy/

32
Life-Long Physical, Mental & Behavioral Health
Outcomes Linked to ACEs
• Alcohol, tobacco & other drug addiction
• Auto-immune disease
• Chronic obstructive pulmonary disease &
ischemic heart disease
• Depression, anxiety & other mental
illness
• Diabetes
• Multiple divorces
• Fetal death
• High risk sexual activity, STDs &
unintended pregnancy
• Intimate partner violence—perpetration
& victimization
• Liver disease
• Lung cancer
• Obesity
• Self-regulation & anger management
problems
• Skeletal fractures
• Suicide attempts
• Work problems—including absenteeism,
productivity & on-the-job injury
Mate, G. (2003). When the Body Says No: The Cost of Hidden Stress

33
Trauma is a risk factor for Substance Abuse
Substance Abuse is a risk factor for Trauma
34
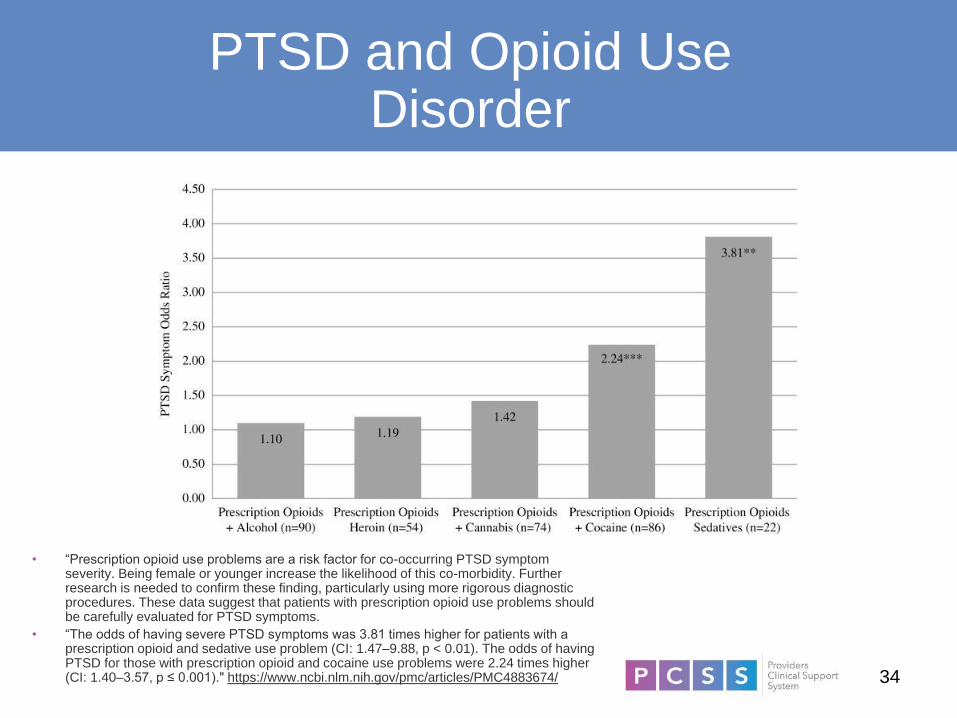
PTSD and Opioid Use Disorder
• “Prescription opioid use problems are a risk factor for co-occurring PTSD symptom severity. Being female or younger increase the likelihood of this co-morbidity. Further research is needed to confirm these finding, particularly using more rigorous diagnostic procedures. These data suggest that patients with prescription opioid use problems should be carefully evaluated for PTSD symptoms.
• “The odds of having severe PTSD symptoms was 3.81 times higher for patients with a prescription opioid and sedative use problem (CI: 1.47–9.88, p < 0.01). The odds of having PTSD for those with prescription opioid and cocaine use problems were 2.24 times higher (CI: 1.40–3.57, p ≤ 0.001)." https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4883674/

35
Addiction and the Brain
As Gabor Mate notes in his book, In the Realm of Hungry Ghosts, those with
substance use disorder
“self-medicate to sooth their emotional pain – but more than
that, their brain development was sabotaged by their
traumatic experiences.”
Mate, Gabor, MD. (2010). In the Realm of the Hungry Ghosts. Berkeley, CA:
North Atlantic Books. Print. page 203.

36
Why do People Use Alcohol and
Drugs?
To feel good
To have
novel:
Feelings
Sensations
Experiences
AND
to share them
To feel better
To lessen:
Anxiety
Worries
Fears
Depression
Hopelessness
Withdrawal
Slide credit: Thomas E. Freese, Ph.D., Co-Director of the UCLA Integrated Substance
Abuse Programs, Director of the Pacific Southwest ATTC
37
Shame is the intensely painful feeling or experience of believing
that we are flawed and therefore unworthy of love and
belonging – something we’ve experienced, done, or failed to do
makes us unworthy of connection. Brene Brown
Brene’ Brown, (2012). Daring Greatly: How the Courage to be Vulnerable
Transforms the Way We Live, Love, Parent, and Lead.
38
Adverse Childhood Experiences
The #1 Chronic Health Epidemic
in the United States
“The impact of ACEs can now only be ignored as a
matter of conscious choice. With this information
comes the responsibility to use it.”
-Anda and Brown, CDC
• ACE Study DVD from Academy on Violence and Abuse

39
ACEs are not Destiny – So What Can We Do?
40
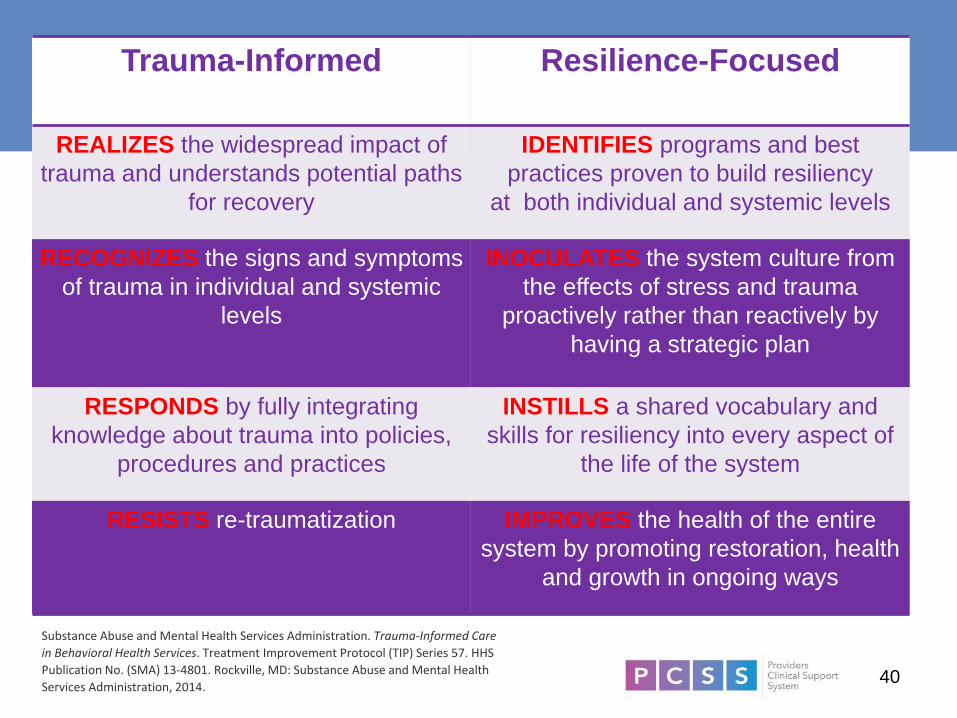
Trauma-Informed Resilience-Focused
REALIZES the widespread impact of
trauma and understands potential paths
for recovery
IDENTIFIES programs and best
practices proven to build resiliency
at both individual and systemic levels
RECOGNIZES the signs and symptoms
of trauma in individual and systemic
levels
INOCULATES the system culture from
the effects of stress and trauma
proactively rather than reactively by
having a strategic plan
RESPONDS by fully integrating
knowledge about trauma into policies,
procedures and practices
INSTILLS a shared vocabulary and
skills for resiliency into every aspect of
the life of the system
RESISTS re-traumatization IMPROVES the health of the entire
system by promoting restoration, health
and growth in ongoing ways
Substance Abuse and Mental Health Services Administration. Trauma-Informed Care
in Behavioral Health Services. Treatment Improvement Protocol (TIP) Series 57. HHS
Publication No. (SMA) 13-4801. Rockville, MD: Substance Abuse and Mental Health
Services Administration, 2014.

41
Safety and Respect: Creating a Safe and
Secure Environment for EVERYBODY
We need to create a mutually respectful
interpersonal climate that fosters safety, trust,
choice, collaboration, and empowerment
“Mistakes made here often.”

42
Cultural Humility
https://thelinkbetweenworlds.com/tag/cultural-humility/

43
We need to have…
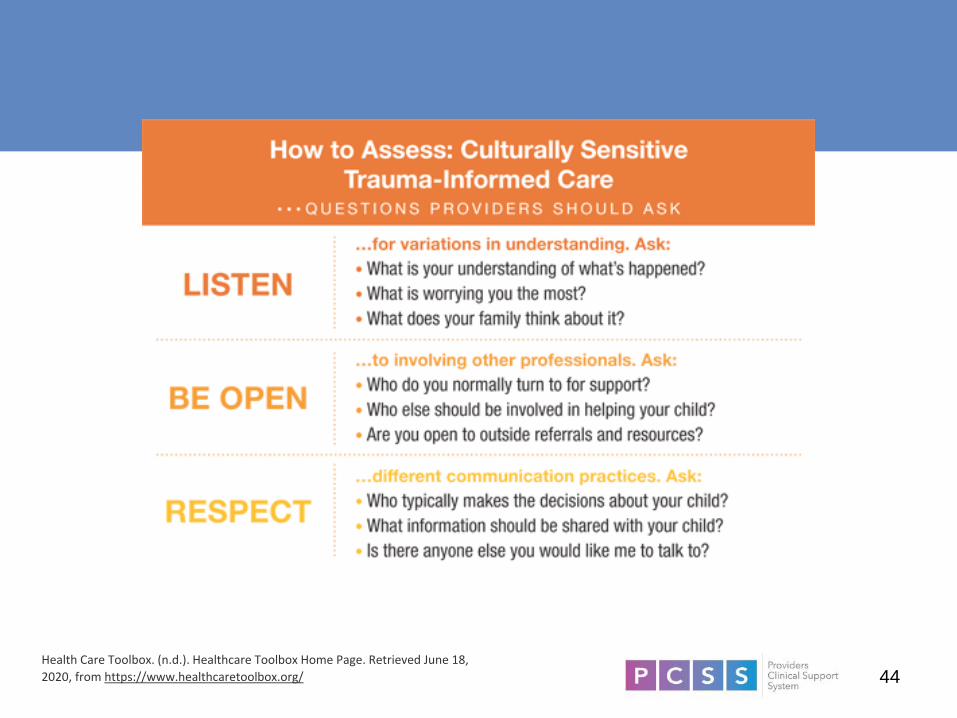
44Health Care Toolbox. (n.d.). Healthcare Toolbox Home Page. Retrieved June 18,
2020, from https://www.healthcaretoolbox.org/

45
Build Relationships
Honor voice and choice
Partner with people
Request feedback
Ensure comfort
“Keep the Human in Human Services”
-Dr. Pat Deegan
Masten, A. (2001). Ordinary Magic: Resilience Processes in Development. American
Psychologist 56, 227-238.
Beardslee et al. (2010). Building Resilience: The Power to Cope with Adversity. Zero to
Three.

46
The RSA. (2013, December 10). Brené Brown on Empathy [Video file]. Retrieved from
https://www.youtube.com/watch?v=1Evwgu369Jw

47
Organizational Strategies for combatting
bias/stigma in patient-provider relationships
Simplify and translate client-facing forms and documentation
Adopt community-defined , promising practices
Hire providers that represent the local community
Client engagement- provide language support and build mental health literacy
Develop a plan for addressing engagement during the current pandemic, and beyond
Develop an organizational approach to case management
Checks for patient understanding of treatment decisions and next steps

48
Be Attentive to All Language
“Lazy”
“Naughty”
“Non-compliant”
“Manipulative”
49
Why It Matters How We Conceptualize It, What
We Call It, People with It

50
Studies have shown that…
• Compared to other psychiatric symptoms, Substance Use is more stigmatized, tend to view those using substances as more to blame for their use and consequences of use
• Describing Substance Use as Treatable Helps
• Individuals shown to hold stigmatizing biases against those using substances; view them as unmotivated, manipulative, dishonest
• Survivors who hold more stigmatizing beliefs about Substance Use are less likely to seek treatment; discontinue sooner
https://www.shatterproof.org/about-addiction/stigma/stigma-reducing-language
52
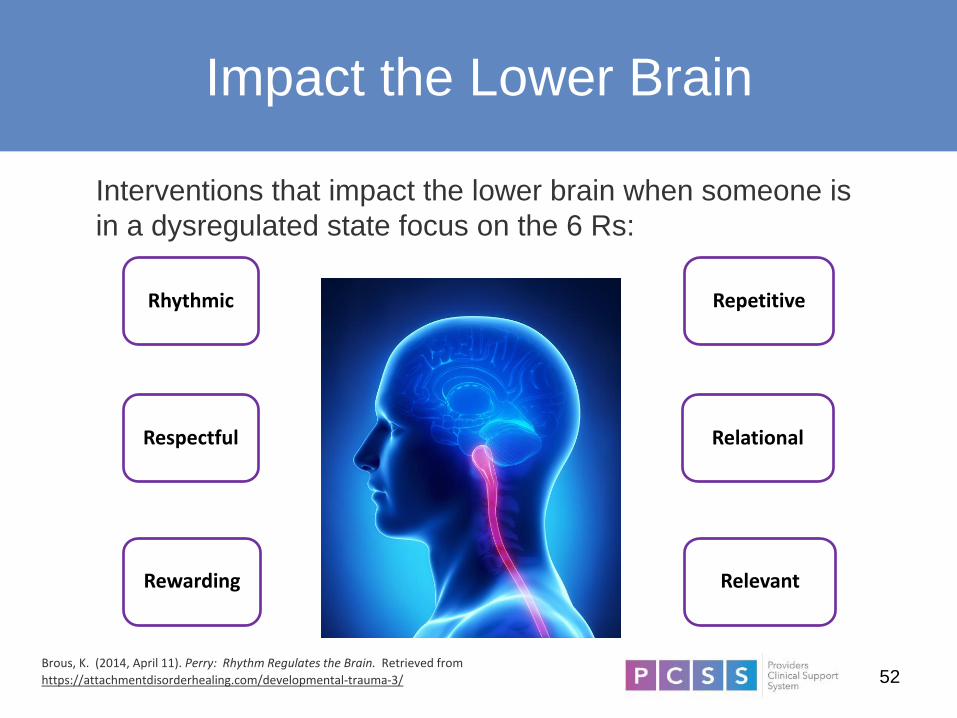
Impact the Lower Brain
Interventions that impact the lower brain when someone is
in a dysregulated state focus on the 6 Rs:
Rhythmic Repetitive
Relational
RelevantRewarding
Respectful
Brous, K. (2014, April 11). Perry: Rhythm Regulates the Brain. Retrieved from
https://attachmentdisorderhealing.com/developmental-trauma-3/

53
Implications for Practice

54
Screen for Trauma
1. Unhealthy substance use is common.
2. Relying on personal impressions is unreliable and may
underestimate prevalence.
3. Opens up a dialogue about other impacts on a person’s
life.
4. Early interventions can prevent development of more
severe substance use disorders.
5. SBIRT has a role in fighting the opioid epidemic
alongside MAT, naloxone and safe prescribing

55
Screening to quickly identify the severity of substance use
and appropriate level of treatment.
Brief Intervention to raise awareness of risks and
consequences, internal motivation for change, and help set
healthy lifestyles goals.
Referral to Treatment to facilitate access to specialized
services and coordinate care for patients with higher risk.
SBIRT is a comprehensive, integrated public health model
56
Evidence-Based Screening Tools
• AUDIT
• DAST
• ASSIST
• CRAFFT (adolescents)
• S2BI (adolescents)
• PHQ-9 (depression)
• GAD-7 (anxiety)
• ACES
57
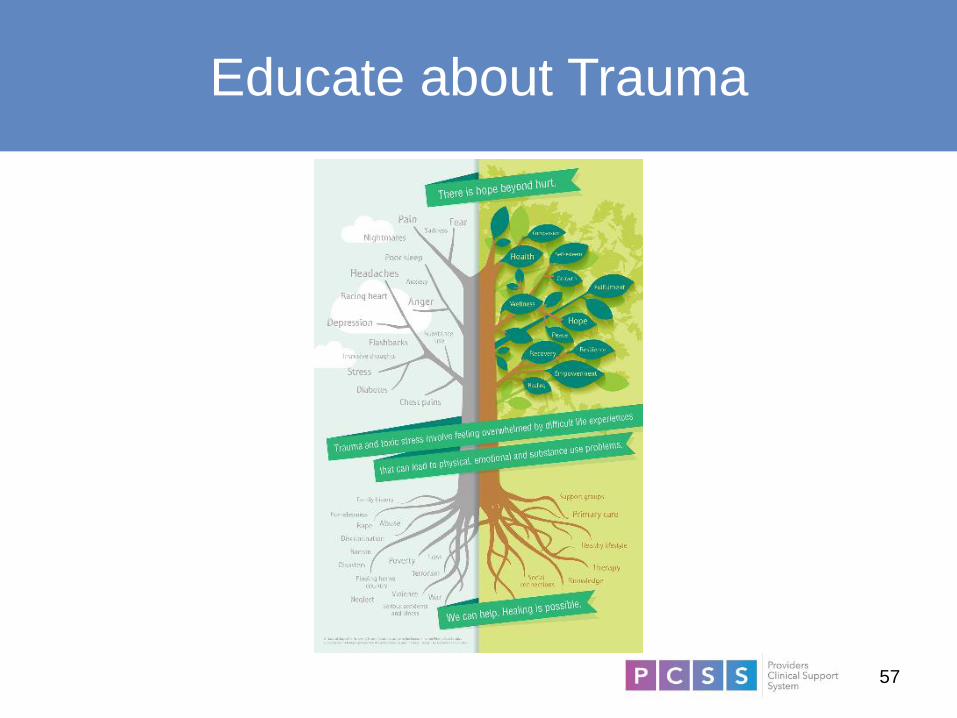
Educate about Trauma

58
Taking Care of Ourselves

59
Understand Daily Translation of
TIROC Principles
Principles of trauma-informed, recovery-oriented care (TIROC):
• Be patient and persistent
• Convey respect
• Be validating and affirming
• Read clients’ needs and respond accurately
• Set realistic expectations and goals
• Provide ongoing choices and supports
• Know your role
• Follow through with what you say you will do
• Provide consistency; minimize surprises

60
Recognize our Humanity
We’re all just trying to survive
We frequently observe misplaced Coping Strategies
We are all part of the problem therefore we can all be part of the Solution

61
References
• Mills, K. L., Teesson, M., Ross, J., & Peters, L. (2006). Trauma, PTSD, and substance use disorders: findings from the Australian National Survey of Mental Health and Well-Being. American Journal of
Psychiatry, 163(4), 652-658.
• Sansone, R. A., Whitecar, P., & Wiederman, M. W. (2009). The prevalence of childhood trauma among those seeking buprenorphine treatment. Journal of Addiction & Addictive Disorders, 28(1), 64-67.
• https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf
• Heart, M. Y. (2003). The Historical Trauma Response Among Natives and Its Relationship with Substance Abuse: A Lakota Illustration. Journal of Psychoactive Drugs, 35(1), 7-13.
doi:10.1080/02791072.2003.10399988
• Evans-Campbell T. Historical trauma in American Indian/Native Alaska communities: a multilevel framework for exploring impacts on individuals, families, and communities. J Interpers Violence. 2008
Mar;23(3):316-38. doi: 10.1177/0886260507312290. PMID: 18245571.
• National Conference of State Legislatures. (2018, Feb). The Costs and Consequences of Disparities in Behavioral Health
Care. https://www.ncsl.org/Portals/1/HTML_LargeReports/DisparitiesBehHealth_Final.htm#:~:text=According%20to%20the%20National%20Institute,and%20more%20likely%20to%20receive
• Eack, S. M. & Newhill, C. E. (2012). Racial Disparities in Mental Health Outcomes after Psychiatric Hospital Discharge among Individuals with Severe Mental Illness. Social Work Research, 36(1), 41-52.
• Medlock, M., Weissman, A., Wong, S. S., Carlo, A., Zeng, M., Borba, C., Curry, M., & Shtasel, D. (2017). Racism as a Unique Social Determinant of Mental Health: Development of a Didactic Curriculum for
Psychiatry Residents. MedEdPORTAL, 13, 10618.
• Dunlop, D. D., Song, J., Lyons, J. S., Manheim, L. M., & Chang, R. W. (2003). Racial/Ethnic Differences in Rates of Depression Among Preretirement Adults. American Journal of Public Health, 93(11), 1945-
1952.
• Agency for Healthcare Research and Quality. (2011, Mar). 2010 National Healthcare Disparities Report. AHRQ Publication No. 11-0005. https://archive.ahrq.gov/research/findings/nhqrdr/nhdr10/nhdr10.pdf
• Echo. (2019). Physical Impact of Trauma. https://www.echotraining.org/we-love-science/
• Hedges, F. (2012). Fight or Flight. Retrieved from https://www.acesconnection.com/blog/fight-or-flight-infographic.
• Ali, S. (2018, July 12). What You Need to Know About the Loneliness Epidemic. Retrieved from https://www.psychologytoday.com/us/blog/modern-mentality/201807/what-you-need-know-about-the-loneliness-
epidemic
• Trauma Theory. (2011, November 12). Retrieved June 10, 2020, from http://kate-thegirlwholived.blogspot.com/2011/11/trauma-theory.html
• Perry, Bruce D., Szalavitz, Maia (2006). The boy who was raised as a dog: And other stories from a child psychiatrist's notebook. Basic Books.
• Davis, B. (Director). (2015). How Childhood Trauma Can Make You A Sick Adult [Video file]. Retrieved from http://mentalhealthchannel.tv/episode/how-childhood-trauma-can-make-you-a-sick-adult
• Adverse Childhood Experiences (ACE) and adolescent health. Retrieved from https://www.cdc.gov/violenceprevention/acestudy/
• Curry, A. (2019, July 18). Parents' emotional trauma may change their children's biology. Studies in mice show how. Science. https://www.sciencemag.org/news/2019/07/parents-emotional-trauma-may-
change-their-children-s-biology-studies-mice-show-how
• National Center for Injury Prevention and Control, Division of Violence Prevention. (n.d.). Adverse Childhood Experiences (ACEs). Retrieved from https://www.cdc.gov/violenceprevention/acestudy/
• Mate, G. (2003). When the Body Says No: The Cost of Hidden Stress.
• Meier, A., Lambert-Harris, C., McGovern, M. P., Xie, H., An, M., & McLeman, B. (2014). Co-occurring prescription opioid use problems and posttraumatic stress disorder symptom severity. American Journal of
Drug and Alcohol Abuse, 40(4), 304-311.
• Mate, Gabor, MD. (2010). In the Realm of the Hungry Ghosts. Berkley, CA: North Atlantic Books. Print. page 203.
• Brene’ Brown, (2012). Daring Greatly: How the Courage to be Vulnerable Transforms the Way We Live, Love, Parent, and Lead.
• Substance Abuse and Mental Health Services Administration. Trauma-Informed Care in Behavioral Health Services. Treatment Improvement Protocol (TIP) Series 57. HHS Publication No. (SMA) 13-4801.
Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
• https://thelinkbetweenworlds.com/tag/cultural-humility/
• Health Care Toolbox. (n.d.). Healthcare Toolbox Home Page. Retrieved June 18, 2020, from https://www.healthcaretoolbox.org/
• Masten, A. (2001). Ordinary Magic: Resilience Processes in Development. American Psychologist 56, 227-238.
• Beardslee et al. (2010). Building Resilience: The Power to Cope with Adversity. Zero to Three.
• Shatterproof. (2021). Stigma-reducing language. https://www.shatterproof.org/about-addiction/stigma/stigma-reducing-language
• The RSA. (2013, December 10). Brené Brown on Empathy [Video file]. Retrieved from https://www.youtube.com/watch?v=1Evwgu369Jw
• Brous, K. (2014, April 11). Perry: Rhythm Regulates the Brain. Retrieved from https://attachmentdisorderhealing.com/developmental-trauma-3/
62
Resources
• Robert Wood Johnson Foundation (2013) Health Policy Brief: Patient Engagement.
People actively involved in their health and health care tend to have better
outcomes—and, some evidence suggests, lower costs.
https://www.rwjf.org/content/dam/farm/reports/issue_briefs/2013/rwjf404446
• Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness Matters: A Theoretical and
Empirical Review of Consequences and Mechanisms. Annals of Behavioral
Medicine : A Publication of the Society of Behavioral Medicine, 40(2),
10.1007/s12160–010–9210–8. http://doi.org/10.1007/s12160-010-9210-8
• Trauma 101- https://youtu.be/1pNwHMjPrxY
• Trauma-informed Care Guiding Principles-
https://www.samhsa.gov/samhsaNewsLetter/Volume_22_Number_2/trauma_tip/gui
ding_principles.html
• Trauma-informed Care in BH Services-
https://store.samhsa.gov/shin/content/SMA14-4816/SMA14-4816.pdf

63
TIP 57: Trauma-Informed Care in Behavioral Health Services
Assists behavioral health professionals in understanding the impact and consequences for those who experience trauma. Discusses patient assessment, treatment planning strategies that support recovery, and building a trauma-informed care workforce. Inventory#: SMA14-4816
View All New Products
Link to Us
Get and use our easy-to-use widgets, APIs, and banners on your website to offer your visitors access to free behavioral health resources.
View Tools and Widgets
SAMHSA TIC TIP

64
Thank You!
Amelia Roeschlein, DSW, MA, LMFT
Consultant
National Council for Mental Wellbeing

65
PCSS Mentoring Program
▪ PCSS Mentor Program is designed to offer general information to
clinicians about evidence-based clinical practices in prescribing
medications for opioid use disorder.
▪ PCSS Mentors are a national network of providers with expertise in
addictions, pain, evidence-based treatment including medications for
addiction treatment.
• 3-tiered approach allows every mentor/mentee relationship to be unique
and catered to the specific needs of the mentee.
• No cost.
For more information visit:
https://pcssNOW.org/mentoring/

66
PCSS Discussion Forum
Have a clinical question?
http://pcss.invisionzone.com/register

67
PCSS is a collaborative effort led by the American Academy of Addiction
Psychiatry (AAAP) in partnership with:
Addiction Technology Transfer Center American Society of Addiction Medicine
American Academy of Family Physicians American Society for Pain Management Nursing
American Academy of Pain MedicineAssociation for Multidisciplinary Education and
Research in Substance use and Addiction
American Academy of Pediatrics Council on Social Work Education
American Pharmacists Association International Nurses Society on Addictions
American College of Emergency Physicians National Association for Community Health Centers
American Dental Association National Association of Social Workers
American Medical Association National Council for Behavioral Health
American Osteopathic Academy of Addiction
MedicineThe National Judicial College
American Psychiatric Association Physician Assistant Education Association
American Psychiatric Nurses Association Society for Academic Emergency Medicine

68
Educate. Train. Mentor
www.pcssNOW.org
@PCSSProjects
www.facebook.com/pcssprojects/
Funding for this initiative was made possible (in part) by grant no. 1H79TI081968 from SAMHSA. The views expressed in written conference materials or
publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does
mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government.


















