WHAT ARE THE CRITICAL ATTRIBUTES AND … ATTRIBUTES ... effective communication ... for improving...
60
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? SUBMITTED TO THE CANADIAN WORKING GROUP ON PRIMARY HEALTHCARE IMPROVEMENT BY DALE MCMURCHY DALE MCMURCHY CONSULTING JANUARY 2009 www.chsrf.ca
Transcript of WHAT ARE THE CRITICAL ATTRIBUTES AND … ATTRIBUTES ... effective communication ... for improving...

WHAT ARE THE CRITICAL ATTRIBUTES
AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM?
SUBMITTED TO THE CANADIAN WORKING GROUP ON PRIMARY HEALTHCARE IMPROVEMENT
BY DALE MCMURCHY DALE MCMURCHY CONSULTING
JANUARY 2009
www.chsrf.ca

CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
This document is available on the Canadian Health Services Research Foundation web site (www.chsrf.ca).
1565 Carling Avenue, Suite 700 Ottawa, Ontario K1Z 8R1
E-mail: [email protected] Telephone: 613-728-2238 Fax: 613-728-3527
This research report is a publication of the Canadian Health Services Research Foundation. Funded through an agreement with the Government of Canada, CHSRF is an independent, not-for-profit corporation with a mandate to promote the use of evidence to strengthen the delivery of services that improve the health of Canadians. The views expressed herein are those of the authors and do not necessarily represent the views of CHSRF or the Government of Canada.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM?
TABLE OF CONTENTS
Main Messages ........................................................................................................................ 1
Executive Summary ................................................................................................................. 1
Background ............................................................................................................................. 5
Methodology ........................................................................................................................... 6
Findings – Attributes and Outcomes of High-Quality Primary Healthcare ................................ 6
High Performing Healthcare Organizations ....................................................................................... 8
Attributes..................................................................................................................................... 8
Supporting.Change........................................................................................................................ 8
Planning.and.Evaluation............................................................................................................... 9
Leadership.................................................................................................................................... 10
Quality Improvement....................................................................................................................... 10
Quality.Improvement.Initiatives..................................................................................................... 10
Quality.and.Technology................................................................................................................. 12
Provider.Quality.Improvement.Incentives........................................................................................ 14
Payment Incentives................................................................................................................... 14
Performance Frameworks and Agreements ................................................................................. 16
Public Reporting ....................................................................................................................... 16
Provider Training, Monitoring and Recognition ........................................................................... 16
Primary Care Physician Supply ........................................................................................................ 17
Impact.of.Physician.Supply.on.Population.Outcomes........................................................................ 17
Impact.of.Physician.Supply.on.Reducing.Health.Disparities.............................................................. 18
Impact.of.Physician.Supply.on.Costs............................................................................................... 18
Payment / Delivery Models .............................................................................................................. 18
First.Contact.Care./.Accessibility..................................................................................................... 22
Accessibility ............................................................................................................................ 22
Place of First Contact ................................................................................................................ 22
Longitudinality./.Long-term.Person-Focused.Care............................................................................. 23
Access to a Regular Primary Care Provider ................................................................................. 23
Access for At-risk Patients ......................................................................................................... 24
Coordination.of.Care..................................................................................................................... 25
Continuity ............................................................................................................................... 25
Integration ............................................................................................................................... 26
Adequacy of Patient Records and Information Retrieval .............................................................. 27
Information Coordination and Communication........................................................................... 28
Comprehensiveness....................................................................................................................... 29
The Primary Care-Specialist Balance .......................................................................................... 29
Preventative Care ..................................................................................................................... 30
Chronic Disease Management ................................................................................................... 31
Critical supporting factors ......................................................................................................... 31
Impact ..................................................................................................................................... 31
Cost ......................................................................................................................................... 33
CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Patient Education, Involvement and Self-management ................................................................ 34
Inter-professional Team-based Care ........................................................................................... 35
Critical supporting factors ......................................................................................................... 35
Impact ..................................................................................................................................... 36
Costs ....................................................................................................................................... 38
Conclusion .............................................................................................................................. 38
Requisite Attributes ......................................................................................................................... 38
Evidence Required to Support Attributes........................................................................................... 39
References ............................................................................................................................... 39
Background .................................................................................................................................... 39
National Primary Care Orientation ................................................................................................... 40
High-performing Healthcare Organizations ....................................................................................... 41
Quality Improvement....................................................................................................................... 42
Quality Incentives ........................................................................................................................... 43
Physician Supply ............................................................................................................................. 45
Payment/Delivery Models ................................................................................................................ 46
Access ............................................................................................................................................ 47
Longitudinality ............................................................................................................................... 49
Coordination ................................................................................................................................... 49
Coordination of Information ............................................................................................................ 51
Comprehensiveness ......................................................................................................................... 52
Prevention ...................................................................................................................................... 53
Chronic Disease Management .......................................................................................................... 53
Patient Centredness ......................................................................................................................... 55
Team-based Care ............................................................................................................................. 55

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 1
MAIN MESSAGESCanada has not yet achieved a national primary care orientation in the sense of providing high quality patient-centred, comprehensive care – although there is evidence from other jurisdictions that this is achievable with demonstrable benefits.
Primary care practices that provide comprehensive and coordinated care confer the most benefits to patients. What characterizes these practices is that they: have a sound knowledge of their patients and community; use clinical guidelines and provide evidence-based care; provide collaborative team-based care; use and share information through electronic medical records; and have effective patient flow processes.
The factors that facilitate the delivery of comprehensive and coordinated care are: governance and organizational effectiveness including a clear mission and vision, strong leadership and change management strategies; accountability supported by a culture of continuous quality improvement and ongoing performance measurement; and patient empowerment through education, shared decision making, access to their medical records, and improved access for at-risk patients.
Future research efforts to support the delivery of high quality, comprehensive and coordinated primary care should focus on : 1) effective organizational, funding and administrative models; 2) methods for determining the appropriate mix of health professionals; 3) models for improving the coordination of care within primary care and with the rest of the health system; 4) the delivery of comprehensive, person-focused primary care, including chronic disease prevention and management, mental health and addictions services, rehabilitation, etc.; 5) improved care for under-serviced areas and at-risk populations; 6) the use of information technology to improve quality and reduce costs; and 7) methods to ensure quality and performance at the service and patient level.
Better co-ordination is required among the various groups that undertake primary care research and between researchers and decision makers seeking high performing primary care in Canada.
Primary care research conducted to date in Canada has not been fully exploited. More effort is required to promote the uptake and dissemination of existing research, including the preparation of syntheses of the published and grey literature for clinicians, managers and regional, provincial, territorial and federal policy makers.
There should be further investment to support change within the context of research and evaluation, including the development of management tools that support healthcare providers, managers, patients and decision makers in implementing change and improving quality.
EXECUTIVE SUMMARYIn this paper the literature pertaining to the attributes and benefits of a high-quality primary healthcare system in terms of the system’s orientation and design, organizational and process factors, physician supply, and the critical features unique to primary care delivery, such as comprehensiveness and coordination of care, is summarized. The following table presents the main findings:

2 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Attributes Benefits
System Orientation and Design
A national primary care orientation
patient-centred
comprehensive and coordinated care
family and community orientation
equitable distribution of health resources
universal coverage
low or no co-payments
a higher percentage of physicians who are primary care physicians
remuneration of primary care physicians commensurate to other specialists
flexible funding
primary care infrastructure
improved access to appropriate services
reduced inequities in the population’s health
lower costs of care
improved patient outcomes
low birth weight
infant and adult mortality /premature mortality
mental health
High-performing healthcare organizations
a clear mission and vision
effective planning
ongoing performance measurement and monitoring
strategic use of partnerships to achieve integration
patient-focused excellence
sustained leadership
patients treated at the most effective level along the continuum of care
effective management of clinicians
effective information technology
change management
resources for change
stakeholder participation
improved quality of care
effective change processes
improved organizational effectiveness
Quality improvement supporting culture, strategy and structure
ongoing performance measurement
clinical audit
collaborative quality improvement initiatives
quality improvement training
use of registries, clinical decision support, prompts and reminders
patient education
patient input
effective stakeholder involvement
change management
leadership
comparative feedback
recognition of excellence
appropriate technology for patient and population-based planning and care
appropriate incentives
accountability and performance agreements
public reporting
increased patient and provider satisfaction
reduced wait times
improved continuity of care
adherence to clinical guidelines
improved chronic disease management and outcomes
increased preventative care
reduced ED visits and hospitalization
improved prescribing practices
improved quality of life
improved patient data/ information
improved operational efficiency
reduced costs
increased population-based planning and monitoring

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 3
Attributes Benefits
Physician supply higher ratio of general practitioners to population
higher ratio of general practitioners to specialists
improved outcomes:
life expectancy
all-cause mortality
stroke mortality
heart disease mortality
cancer mortality
reduced low birth-weight
postneonatal mortality
reduced acute hospitalizations
increased prevention
increased early cancer detection
reduced health disparities
reduced costs
Payment / delivery models
payment appropriate to the circumstances and that mitigates perverse incentives (e.g., blended payment schemes)
improved access
improved quality of care
increased preventative interventions
better chronic disease management
more rational use of resources (e.g., reduced fragmentation and duplication)
improved team collaboration
improved patient and provider satisfaction
Service Delivery – Unique Attributes
First contact care / accessibility
use of practice as place of first contact
practice accessible in terms of office hours, wait times, etc
coordinated patient flow processes
gatekeeping
reduced wait times
improved coordination
improved referrals
reduction in redundant services
Longitudinality / long-term person-focused care
patient has a regular source of care
practice has knowledge of the patient
long-term patient-provider relationship
more timely care
appropriate preventative care
greater likelihood of health problems recognition
fewer diagnostic tests and prescriptions,
more accurate diagnoses
lower costs
reduced ED and hospital use for ambulatory care sensitive conditions
reduce health disparities associated with socio-economic status

4 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Attributes Benefits
Coordination of care continuity of care
collaborative team-based care
integrated health service delivery
effective communication
standardized referral processes
continuity of patient information from previous visits and other providers
effective electronic medical records with system-to-system interoperability
reduced duplication of services
greater patient satisfaction
better patient compliance
saved consultation time
less hospitalization and ED use for ambulatory care-sensitive conditions
improved screening and immunization rates
improved chronic disease prevention and management
improved patient safety
lower costs
Comprehensiveness adequate personnel, facilities, equipment, supporting services, etc.
wide spectrum of common health problems addressed
services and provider skill mix reflects population needs
referral arrangement
use of clinical pathways and guidelines, and the provision of evidence-based care
comprehensive chronic disease management program
collaboration among providers
inter-professional teams
patient education and self management
shared longitudinal clinical records
improved quality of care
increased prevention and screening activities
improved chronic disease management and markers
reduced morbidity and mortality
improved quality of life
reduced preventable hospitalization
lower hospital readmission rates
reduced length of stay
reduced complications
reduced costs
improved patient knowledge and experience
Primary care practices that provide comprehensive.and.coordinated.quality.primary.healthcare tend to confer the most benefit to their patients. Generally, such practices: 1) have a sound knowledge of their patients and community; 2) use of clinical pathways and guidelines, and provide evidence-based care; 3) provide collaborative team-based care; 4) use and share sophisticated electronic medical records; and 5) have effective patient flow processes.
Achieving the above attributes is facilitated by:1) governance and organizational effectiveness including a clear mission and vision, strong leadership and change management strategies; 2) accountability – whether to funders, managers, professional colleges or the public – supported by a culture of continuous quality improvement and ongoing performance measurement and monitoring; and 3) patients; given the tools (e.g., education, shared decision-making, access to their medical records, convenient access to care for at-risk patients) patients can make a significant contribution toward maintaining and improving their own health and well-being.
While there is universal coverage and efforts to equitably distribute healthcare resources, one cannot say that Canada has achieved a national primary care orientation in the sense of providing patient-centred, comprehensive and co-ordinated care. Nonetheless, the attributes discussed are attainable and can be supported by primary care reform initiatives across the country.
Volumes of research have been conducted by university-based researchers, clinicians, primary care practices, professional organizations, federal, provincial and regional authorities, think-tanks, hospital-based research centres, health quality councils, and the voluntary sector that have not been fully exploited. There are opportunities to realize the potential of work to date through syntheses of the published and grey literature, and through collaboration among these groups.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 5
To support primary care improvement, more actionable evidence and the supporting management and improvement tools need to reach healthcare providers, managers, patients and decision makers. More applied research in the following areas would be beneficial: 1) effective organizational, funding and administrative models; 2) methods for determining the appropriate mix of health professionals; 3) models for improving the co-ordination of care within primary care and with the rest of the health system; 4) effective means by which to deliver ongoing, comprehensive, person-focused primary care; 5) ways in which to effectively improve care in under-serviced areas and to at-risk populations; 6) examples of information technology’s successful use in improving quality and reducing costs; and 7) methods by which to ensure quality and performance at the service and patient level. These efforts could include syntheses and improved dissemination of existing research, and innovative and actionable primary research.
BACKGROUNDThe Communiqué on Health, emanating from the First Ministers’ Meeting in September 2000, identified eight government priorities related to improving the quality of Canada’s healthcare system. One of these priorities was to ensure access to appropriate primary healthcare services. With this focus, the First Ministers committed to ensuring timely access to care and to the receipt of “the most appropriate care, by the most appropriate providers, in the most appropriate settings” and invested $800 million in primary healthcare between 2000 and 2006 through the Primary Healthcare Transition Fund (PHCTF) (Health Canada 2000).
Despite this investment, along with several other provincial and regional initiatives and ample evidence supporting the benefits of a high-functioning, integrated primary healthcare system, Canada’s primary care sector lags behind other countries with similar wealth and health systems, most notably in after-hours care, wait times, chronic disease management, mental health, quality improvement and electronic medical records (Schoen 2006, 2007, Starfield 2005, 2008a). Moreover, Canada’s primary care sectors are characterized by fragmentation, ineffective use of providers, and inefficient use of resources (e.g., redundant testing, overlap of care, a lack of health promotion, poor information sharing and a misalignment of incentives) (Deber 2006).
Barbara Starfield states that “Canada seems to have stalled in its commitment to strengthening primary care. One reason for this lack of movement may be the poor investment in primary care research and evaluation. In this regard, Canada is probably at least 10 years behind” (Starfield 2008a). To address this gap, supported by the Canadian Health Services Research Foundation (CHSRF), researchers, decision makers, providers and other stakeholders have come together to form the Canadian Working Group on Primary Healthcare Improvement, a group dedicated to “concerted action at a pan-Canadian level to promote primary healthcare research and knowledge exchange to inform funding priorities, policy and practice change for the benefit of Canadians.” Based on the report Mapping.the.Future.of.Primary.Healthcare.Research.in.Canada, which included case studies of the system-level structures that support and sustain primary healthcare research and practice change (Russell 2007), and the members of the working group’s respective expertise, the working group is endeavouring to identify an appropriate strategy for supporting the improvement of primary healthcare in Canada.
To support its deliberations, the working group has identified background papers that would help to inform its strategy. This paper is the first in a series of three papers:
1) What are the attributes and benefits of a high-quality primary healthcare system?
2) What are the likely health and economic consequences of closing the gap in access and quality between evidence-based practice and current primary healthcare performance?
3) What organizational models and structures should be considered for a pan-Canadian body that would promote evidence-informed primary healthcare policy and practice?

6 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
METHODOLOGYThis review of the literature focused on material in the Canadian literature relevant to the identification of effective primary healthcare delivery systems and the impact on the health system, patients and providers, as well as international evidence (namely Europe, Australia, New Zealand and the United States) that has the potential of transferability to Canada.
The review focused predominantly on existing syntheses, with augmentation from more recent research and Canadian examples. Document review extended beyond the traditional academic literature to include existing evidence from within Canada from governmental and research agencies, such as Statistics Canada, the Canadian Institute for Health Information, Canadian Health Services Research Foundation, and the Conference Board of Canada. The emphasis of the review was on evaluative studies, and where possible studies that compared interventions in similar populations.
The review reach included bibliographical and data-based searches of published and unpublished literature addressing the benefits of a high-performing primary healthcare system. The principle target was syntheses and systematic reviews from peer-reviewed sources. Canadian working papers and government, professional organizations’ and other reports were also sought. PUBMED and other databases (such as Google Scholar) and those of major health organizations, were used to identify major “components” of search terms. Both Medical Subject Headings (MeSH) and keywords were identified for each component. Searches were limited to publications between 1990 and 2008. The most references and abstracts were catalogued using Endnote, a commercial bibliographic software program.
Citations and abstracts were reviewed for relevance of content, taking the geographic location, system structure, type of programs and health delivery setting into consideration. The outcomes observed and the quality of the evidence supporting the findings was also assessed. Once the studies were selected as potential sources of evidence, they were assessed in terms of the quality of the research design and methodology. Specific issues considered included: sample design and size, the potential generalizability of results, and the appropriateness and/or quality of any statistical analysis. This assessment, along with the significance of the research, its setting and relevance, impacted on the weight allocated to the paper and thus the extent to which it influenced the conclusions drawn. Relevant studies cited in syntheses and systematic reviews were assumed to meet the inclusion criteria.
FINDINGS – ATTRIBUTES AND OUTCOMES OF HIGH-QUALITY PRIMARY HEALTHCAREThis section summarizes the literature as it pertains to the attributes and benefits of a high-quality primary healthcare system in terms of the system’s orientation and design, organizational and process factors, physician supply, and the critical features unique to primary care delivery, such as comprehensiveness and co-ordination of care.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 7
A NATIONAL PRIMARY CARE ORIENTATION
The Commonwealth Fund survey compares adults’ healthcare experiences in Australia, Canada, Germany, the Netherlands, New Zealand, the United Kingdom and the United States. In all countries,
having a “medical home” that is accessible, knows the patient’s medical history, and helps co-ordinate care is significantly associated with more positive primary care experiences. Based on the survey results, 48% of Canadians are deemed to have a medical home, fewer than in Australia, New Zealand and the United States (Schoen 2007).
Countries with a stronger primary healthcare system generally have healthier populations, and particular aspects of their health policies are critical to establishing a high quality primary healthcare system. A greater systemic emphasis on primary healthcare can be expected to improve health outcomes through improved access to appropriate services, reduced inequities in the population’s health and lower costs of care (Starfield 2008).
A study on the association between primary care and health outcomes in 11 industrialized countries found that countries where primary care practices scored the highest in terms patient-centred, comprehensive and co-ordinated care, as well as family and community orientation, were more likely to have the following policy-related characteristics: 1) attempts to distribute health resources equitably based on geographic and demographic health needs; 2) universal or near-universal coverage guaranteed by a government or government-regulated insurance providers; 3) low or no co-payments for primary care services; 4) a higher percentage of physicians who are primary care physicians; and 5) remuneration of primary care physicians commensurate to other specialists (Starfield 1991, 1994, 1998).
Two other studies have found that countries with lower primary care practice and policy scores had poorer healthcare performance and outcomes, most notably in terms of low birth weight, post neonatal mortality and mental health (Starfield 1991, 1994, 1998, 2002). A later longitudinal study of 18 industrialized countries showed the greater the country’s primary care orientation, the lower its rates of all-cause mortality, all-cause premature mortality and premature mortality from asthma and bronchitis, emphysema and pneumonia and cardiovascular disease. These results were maintained after controlling for system and population characteristics. This study also found that a five-point increase (on a 20-point scale) was associated with a reduction in premature deaths from asthma and bronchitis and heart disease by up to 6.5% and 15% respectively (Macinko 2003).
Specifically related to co-payments and user fees, systematic reviews have shown that increasing or introducing user fees significantly reduces the use of primary care services and removing these fees increases use. One of the reviews also showed that co-payment policies can reduce drug use and expenditures; but this applies to the use of life-sustaining drugs and drugs critical to treating chronic conditions, as well as non-essential drugs. Although there were insufficient data on health outcomes, the authors concluded that reduced use of primary care services and essential medications resulting from co-payments could lead to increased health service utilization and costs in the long run (Lewin 2008).
Primary care performance in individual countries has been associated with government policies and the nature of reform. A decline in Germany’s primary care score over time has been associated with reduced access to primary care services due to the introduction of higher co-payments (Macinko 2003). Spain’s primary care performance improved when it moved to tax-based financing, improved its geographic allocation of funds, increased the supply of family physicians, and introduced primary healthcare centres (Larizgoitia 1997). Hypertension and stroke-related mortality rates declined in the areas in Spain where primary healthcare centres were introduced (Villalbi 1999). The United States’

8 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
(U.S.) primary care score rose slightly between the 1970s and 1990s with the increase in the number of health maintenance organizations (HMOs), which have a high proportion of primary care providers (Weiner 2004) and a greater community focus (Stevens 2003). After extensive reform, the United Kingdom (U.K.) has shown improvement in several primary care indicators and on average primary care physicians now earn more than specialists (Roland 2008).
In Mexico, Bolivia, Cuba and Costa Rica the introduction of more effective primary care delivery systems was associated with lower child mortality rates – with Cuba and Costa Rica having the lowest infant mortality rates in Latin America; reduced adult mortality was also found in Costa Rica (Reyes 1997, Perry 1998, Waitzkin 1997, Starfield 2005). A study in Brazil showed that a good primary care experience was associated with a higher self-rated health status (Starfield 2005).
The key characteristics of high-performing primary care systems that stood out consistently in the studies discussed above were: comprehensiveness of care (e.g., the extent and range of services provided by primary care providers rather than via referrals to specialists); family orientation (e.g., the extent to which services are provided to all family members by the same providers); government efforts to distribute health resources equitably; government or government-regulated universal coverage; and low or no patient use fees for primary care services. Moreover, countries with weaker primary care systems had significantly higher costs (Starfield 2002).
A comparative study of primary care models in New Zealand, Canada, the U.K., the U.S. and the Netherlands was recently undertaken to inform reform initiatives in Australia. The four key interdependent features identified for achieving reform were: 1) flexible funding; 2) quality frameworks; 3) regional-level primary care organizations; and 4) primary care infrastructure. As well, the report states that for reform to be effective, the tensions and trade-offs in balancing professional and bureaucratic control and in the linking of quality and accountability mechanisms must be addressed. The authors concluded that improved interaction among researchers, policy makers and professional groups would contribute to more effective primary care reform (Naccarella 2008).
HIGH PERFORMING HEALTHCARE ORGANIZATIONSAttributes
In addition to having a national (or provincial) primary healthcare orientation, the effective delivery of primary care services and improved patient outcomes are associated with the performance of primary care practices and their ability to adapt and change.
Based on a review of documents related to the performance of healthcare organizations in general, the key characteristics of high-performing organizations are as follows (Joint Policy and Planning Committee 2004, U.S. General Accounting Office 2004, U.K. Audit Commission 2003, Baldrige National Quality Program 2004, Feacham 2002): 1) a clear mission; 2) ongoing performance management; 3) strategic use of partnerships to achieve integration; 4) client and patient-focused excellence; 5) sustained leadership and strong capacity for managing people; 6) treatment of patients at the most effective level of care, including active management of patients along the care continuum and effective management of clinicians; and 7) sophisticated and efficient information technology.
Supporting Change
Practices that are establishing, changing or endeavouring to improve their performance face several challenges. Change is challenging for all involved, and requires good planning, strong leadership, effective communication and team building. “Clinical governance is about changing the way people work; demonstrating that leadership, teamwork and communication are as important to high-quality care as risk management and clinical effectiveness”(Tait 2004).
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 9
Barriers to implementing change can include low morale resulting from an attempt to implement reform too quickly, inadequate staff experience, insufficient infrastructure, financial constraints (Thomas 2005), and the challenges of human relationships and personalities (Grumbach 2004). Another challenge relates to the experiences of organizations as they grow and become increasingly hierarchical. As a result, they often experience greater communication and decision-making challenges, with increased likelihood of communication failures and decision making being more distant from staff at the point of healthcare delivery (McConnell 2005).
A randomized clinical trial of 79 primary care practices in the U.S. undergoing change identified the critical elements for practice change as: 1) motivation of key stakeholders to achieve the targets; 2) resources for change; 3) support from outside the practice, including the larger healthcare system and community; and 4) opportunities for change and the way in which stakeholders understand the change options (Cohen 2004).
For Primary Care Groups in the U.K., the five features associated with increased organizational capacity for innovation were: 1) clear structures and a vision for governance; 2) opportunities for those involved to reflect and learn; 3) clinicians and managers in leadership roles that encourage participation; 4) the right timing and adaptation to the local context; and 5) external facilitation to help bring perspective to the experience (Thomas 2005).
As with the U.K. study, several studies exploring the experience of change stress the need for organizational capacity to learn and reflect. For providers and practices to evolve through change, they need to make time for continuous learning in order to reform organizational processes and improve performance (Crabtree 2003, Senge 1990). Much of the current healthcare literature on organizational learning focuses on training and professional development (Davidhizar 2000); however, there is less on how the theory can be translated into the day-to-day work of providers within healthcare organizations (Lipshitz 2000).
In one example in Saskatchewan, a systems approach to change management was used in newly forming primary care practices and teams were supported by trained facilitators. Approaching the practices as systems with component parts that need to work together effectively, they implemented a five-step “ABCDE” model to lead organizations systematically through change. The process started with identifying the desired future state, and then guided the practices in developing and implementing a “road map” for change, a plan to manage the change process, and methods to sustain improved performance (Saskatchewan Health 2004).
Planning and Evaluation
Effective planning and evaluation of primary care practices is critical to improved service delivery. “Effective planning must be based on the characteristics and needs of the population served and support interdisciplinary collaborative care and service models” (Conference Board of Canada 2006). Importantly, organizations need to increase the protected time for planning and development (Lord 2003).
Although a handful of primary care organizations in Canada undergo accreditation, performance measurement in primary healthcare has been lacking. The Health Services Restructuring Commission in Ontario urged that systemic change be coupled with performance measurement through performance frameworks and information about performance at the service and patient level (Health Services Restructuring Commission 1996). Performance measures related to patient and system outcomes should be based on clear objectives and targets and allow for comparison across the sector. There are a number of evaluation frameworks and assessment tools to measure the performance of inter-professional collaborative practices and primary healthcare delivery (e.g., CIHI 2006, Association of Ontario Health Centres 2008). Primary care practices should be encouraged to use frameworks and tools that include benchmarks for quality improvement. Increased evidence-based training and education of healthcare providers can also contribute to improved quality and outcomes (Lord 2003).
10 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
As an example, the U.K. Department of Health has introduced a number of nationwide initiatives to improve and evaluate performance in primary care, including annual performance reviews of all physicians by their peers, national standards and service frameworks for the chronic disease management, and clinical audit and reporting programs. These activities have resulted in substantial quality gains, including clinical markers for coronary heart disease, diabetes and asthma (Roland 2008, Campbell 2005).
Leadership
Effective leadership is essential to primary care practices. Importantly, leaders must show commitment to the organization’s vision. “Skills development for managers in communication, change management, teamwork and leadership is critical to the successful operation of interdisciplinary teams. Strong administrative support, coupled with appropriate governance structures, is also necessary” (Conference Board of Canada 2006). Peggy Leatt et al. report that leadership development programs in healthcare should include competency-based development, inter-professional and team learning, and continuous assessment. They conclude that leadership development is not “solely to improve the leadership skills of one individual, but is an essential component of the development of the organization as a whole,” and investments in leadership development for senior team members will have a “significant return on investment in terms of organizational effectiveness” (Leatt 2003).
QUALITY IMPROVEMENTQuality Improvement Initiatives
Twenty-eight percent of Canadians are very confident and 52% are somewhat confident that they would receive high-quality, safe healthcare when they need it; 73% report having received
excellent or very good quality of care from their physician. Notably, reported laboratory, medication and medical errors are highest among patients with a chronic illness and the rate is highest among those with two or more conditions (Schoen 2007).
Canada lags behind other countries in terms of quality improvement and management. The Commonwealth Fund’s comparative study found that 48% of primary care physicians have participated in collaborative quality improvement efforts in conjunction with other practices, hospitals, government or professional associations, 7% have participated in quality improvement in preventative care, and 44% have had training in quality improvement methods and tools, the lowest rates among the seven countries studied (Schoen 2006).
Only 27% of Canadian primary care physicians had set formal targets for clinical performance and they were the least likely to have data available on clinical outcomes (24%). Additionally, only 45% had conducted a clinical audit of patient care in the previous two years compared to 76%, 82% and 96% of those in Australia, New Zealand and the U.K., respectively, and only 20% document and follow-up on all adverse events. Eleven percent said they routinely receive data on patient experience and satisfaction, again the lowest rate in the countries studied (Schoen 2006).
Quality improvement is a term that is used in relation to: continuous improvement; organizational and provider involvement in changing systems; processes and behaviour; evidenced-based review and change; and collaborative inter-professional teams (Baker 2008). There are numerous examples of improvements in quality as a result of primary care practices’ involvement in systematic quality improvement initiatives. Five systematic reviews of strategies to change providers’ behaviour or improve care processes – including guideline dissemination, audit and feedback, educational outreach visits and educational meetings – found small to moderate improvements in professional performance and health outcomes compared with no intervention. For example, improved adherence to clinical practice guidelines
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 11
was found with regard to providing patients with information about the effectiveness and appropriateness of treatment approaches, the use of reminders, dissemination of educational materials, audit and feedback, and educational outreach (Lewin 2008).
Quality improvement programs, often modelled on the Institute for Healthcare Improvements’ breakthrough series model, have increased patient and provider satisfaction and improved health outcomes by enabling participants to share experiences, accelerate learning and spread best practices. These initiatives have resulted in reduced wait times – usually with patients getting appointments on their day of choice – reduced wait times while at the physician’s office, improved continuity of care and increased patient and provider satisfaction (IHI 2008a). Quality improvement collaboratives targeting diabetes and other chronic health conditions have been used in the U.S., the U.K. and Canada. In terms of diabetes management, participation in these initiatives has resulted in improved HbA1c, low-density lipid (LDL) and blood pressure testing rates and results, as well as improved patient education, increased preventative procedures and reduced hospitalization. Quality of life indicators have also shown improvement (Piatt 2006, Asch 2005, Tsai 2005, Sperl-Hillen 2000, Wagner 2001, Camp 2004).
Since the chronic disease management collaborative started in Saskatchewan in 2005, 38% more diabetic patients are at optimal levels for blood sugar, cholesterol and blood pressure. As of March 2008, almost one in five patients with diabetes had achieved this goal, up from one in eight in 2005. As well, since the start of the collaborative, 22% more individuals with coronary artery disease were prescribed cholesterol-lowering medication. In March 2008, almost three-quarters of those with coronary artery disease had been prescribed these drugs (Health Quality Council Sask. 2008). In the Vancouver Island Health Authority collaborative, rates of appropriate testing among patients with diabetes have doubled and patients have fewer visits to the emergency department and hospital stays for diabetes-related conditions. Moreover, the average cost for diabetes care in the province dropped from $4,400 per patient in 2001/02 to $3,966 in 2004/05 (Tregullis 2006).
Other quality improvement examples include Jönköping County in Sweden where system-wide quality improvement initiatives have led to cost savings through reductions in hospital admissions and days, wait times for referrals and the number of asthmatic children visiting acute care facilities, as well as increased influenza vaccinations (IHI 2008b). In the U.K., unnecessary hospital admissions have been reduced, and improved treatment and care for chronic obstructive pulmonary disease – including rapid diagnosis, 24-hour support, patient education, home care and rehabilitation – has improved outcomes (IHI 2008c). The Birmingham East and North Primary Care Trust has changed from having the worst performance in the country with regard to over-prescription of antibiotics to winning an award for reduced prescribing levels, and it has improved coordination of care, decreased wait times, reduced unnecessary hospital admissions and referrals to specialists, and increased patient satisfaction for diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, orthopaedics and elderly care (Baker 2008).
Quality improvement programs in the U.S. have improved care processes for diabetes, hypertension, depression and cancer, reduced obesity through self-management, improved counselling and wellness services in primary care, and increased health literacy programs (IHI 2008d). In Minnesota, the implementation of a comprehensive chronic care model by a healthcare team resulted in more patients receiving appropriate screening and an increase in diabetic patients reaching clinical milestones related to blood sugar, blood pressure and cholesterol (IHI 2008e). A program targeted at high-risk diabetes patients implemented by primary care teams at Kaiser Permanente resulted in an increase in the number of patients on a daily protocol of three cardiovascular risk-reducing drugs and a reduction in the number of cardiovascular events over five years (IHI 2008f). A chronic care quality improvement program in Tallahassee resulted in an increase in primary care physician visits and a concurrent reduction in inpatient days and emergency department visits (IHI 2008g).

12 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
A comprehensive asthma program in Massachusetts reduced the percentage pediatric asthma patients who had hospital admissions by 77% over three years (IHI 2008h).
Based on the findings of systematic reviews, the impact of quality improvement initiatives (e.g., audit and feedback) are likely to be greater when baseline compliance to recommended practice is low, the initiative targets a particular behaviour or barrier to change, and when the intervention is provided more intensively. The impact is also likely to be greater when educational interventions are more interactive and have higher attendance rates (Lewin 2008).
The following have been identified as the key factors for facilitating the implementation of quality improvement: 1) the presence of a supporting culture, strategy and structure; 2) the ready availability of requisite information and supporting systems; 3) education and training of staff; 4) understanding of the time and change management requirements; 5) alignment of goals and incentives; 6) leadership; 7) the presence of the requisite skills; and 8) adequate resources (Baker 2008).
Quality and Technology
The Agency for Healthcare Research and Quality (AHRQ) and the Institute for Healthcare Improvement (IHI) in the U.S. undertook an extensive review of the role of health information technology in quality improvement in various primary care settings. They identified the following issues related to the adoption of health information technology:
More examples of information technology’s successful use in improving quality and reducing costs are needed.
Many clinicians cannot fully articulate what they need to support quality improvement and are often left on their own to assess the varying and often contradictory information from industry leaders, colleagues and vendors.
Many clinicians assume that the existing health information systems include the improvement tools they need, but many important tools are not available, are awkward to use or are expensive (AHRQ 2007).
Most primary care practices start by using information technology to support administrative tasks such as scheduling and billing, and laying this groundwork has shown to be a critical first step. Now, there are numerous examples of the successful implementation of electronic medical records in primary care practices (AHRQ 2007).
The use of information technology – including reminders and clinical decision-support systems –in primary care has been shown to improve both operational efficiency and quality of care. These include increased frequency of screening, improved preventative care and disease management, reduced prescribing errors, improvements associated with computerized physician order entry (CPOE) (e.g., reduced repeat tests and more timely tests and procedures), less missing information, and cost savings (AHRQ 2007, Toth-Pal E 2004, Mitchell 2001, Hunt 1998). Using technology can also lead to improvements to the system of care through proactive planning for populations, queries and follow-up on sub-populations, and having all pertinent patient information in one place allowing for the development of a holistic care plan. Queries can also be used to determine why patients are not responding to their care and may provide guidance for improving an individual’s care or the overall system of care (AHRQ 2007).
The use of electronic medical records has also been shown to improve overall patient satisfaction with their visits, patient satisfaction with physicians’ familiarity with them, patient-provider communication, the use of time during the visit, and comprehension of decisions made during the visit (Hsu et al 2005).
A systematic review looking at the impact of health information technology on the quality, efficiency and costs concluded that “a disproportionate amount of literature on the benefits that have been realized comes from a small set of early-adopter institutions that implemented internally developed

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 13
health information technology systems.” About one-quarter of the 257 studies reviewed came from four academic institutions. Only nine evaluated multifunctional, commercially developed systems. Moreover, there was little cost data or information on their impact in community settings. The authors concluded that context mattered: “how these tools are used, and the context in which they are implemented are critical” (Chaudhryet al 2006).
According to Health Canada, maximizing the benefits of electronic medical records in terms of quality improvement requires “strict adherence to rules regarding the types and amount of data collected and how it is maintained” (Health Canada 2006). The Agency for Healthcare Research and Quality and the Institute for Healthcare Improvement identify the functionality required for improving the quality of care as follows (AHRQ 2007):
Proactive population-based
All involved in quality improvement should be able to query the data
The system should support instant access to query results
The querying system should allow the user to ask any question
Users should be able to construct and run queries without technical assistance
Users should be able to specify the inclusion of any data elements in queries
The system should support “drill down” into data
Users should be able to save queries for re-use and/or refinement
The system should support the sharing of queries
The types of action taken on the lists of patients in a query need to be flexible
The action taken on the list should incorporate and use patient data to further segment the action: e.g., HbA1c follow up
The system should automate the actions whenever possible
Planned care for individual patients
Data for the “whole patient” should be displayed in one place
The “whole patient” display should be dynamic
The “whole patient” display should be used for planning, treatment and follow up
The “whole patient” display should support care across all conditions and health issues, not just the complaint associated with a particular encounter
The “whole patient” display should be the central location for other views of patient data, such as run charts of laboratory results and vitals
The “whole patient” display should incorporate evidence-based prompts and reminders
The system should provide a portal for the patient for both input and viewing data, giving the patient some control over his/her record

14 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Measurement
The measurement module should allow the user to customize any report by adding or changing a filter
The query and filter structures for measurement and reporting should be identical to those used for the population-based care tool and for reminders and prompts
Other
Ability to customize the data presented
Ease of use
Interoperability
Data available across the continuum of care
Appropriate data structures provide information that supports improvement
Automation
Additional areas that need to be addressed are: data structures and the design of systems for information sharing (e.g., one data warehouse versus interoperable systems), data ownership, and ensuring data accuracy.
Provider Quality Improvement Incentives
Examples of existing financial incentives in primary care in Canada include fee-for service codes for chronic disease management and case conferencing, preventative care bonuses and
after-hours payments. There are few incentives based on outcomes and the patient experience.
Ten percent of primary care physicians in Canada report having access to financial incentives to achieve certain clinical care targets, 35% can receive incentives for managing patients with chronic diseases or complex needs, and 41% have financial incentives to enhance preventative care activities. Few receive incentives associated with patient satisfaction (Schoen 2007).
Payment Incentives
There is mixed evidence on the impact of financial incentives on the healthcare system. On an individual basis, the psychological research shows specific and difficult goals motivate individuals to perform at a higher level than they would without them. Performance increases with feedback, and comparative feedback further improves performance. But the evidence is less clear on using pay incentives to improve individual performance; these may or may not improve an individual’s performance and may lead to perverse consequences. The evidence is also mixed on the impact of individual incentives on an organization’s performance; linking pay to organizational results has shown improvements, but in other cases incentives have had no impact. Control by rewards can feel punitive, and rewards can destroy relationships and undermine cooperation. Rewards may also discourage risk taking and undermine task perseverance and motivation (Kohn 1993).
There is limited research on the effects of incentives on teams, and even less on the efficacy of organizational incentives. Team size may affect the impact of an incentive scheme on performance, and teams may make an effort to achieve the rewarded targets, but not to exceed them. Cooperation and knowledge sharing, important to teamwork, are difficult to incent. It is also difficult to develop an incentive structure for

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 15
those who perform multiple types of tasks, do not specialize, and/or have multiple accountabilities. Output may be difficult to measure in these circumstances (Joint Policy and Planning Committee 2004).
The evidence related to pay-for-performance schemes is mixed. While some schemes have shown improvements on the targeted interventions, a number of unintended consequences have been identified. Pay-for-performance schemes can exacerbate existing disparities. High performers tend to do better, while poor performers improve more slowly or even do worse. Resource-poor service providers may not be able to invest sufficiently to reap rewards, and net revenue may decline for those who need to invest the most in quality improvement. Improvement in some areas may be to the detriment of others and the incentive structure may promote the cherry picking of patients. Moreover pay-for-performance schemes tend to reward processes rather than outcomes, and the processes rewarded are only a subset of delivery processes (often those for which data are available) and an emphasis on these may divert attention from other areas (Hutchison 2008, Miller 2007, Rosenthal 2004).
In a review of the literature on the effects of financial incentives on quality in primary care, five out of six studies on individual physician incentives found partial or positive effects on quality measures. Seven of the nine studies on incentives directed at provider groups also reported partial or positive effects, although the size of the effects was small. Two studies on system level incentives showed mixed results. Unintended consequences included adverse selection of patients and other manipulations of the system to maximize payments (Petersen 2006).
A Cochrane review found targeted payments in primary care were associated with improved immunization rates, but the improvement was only statistically significant in one of the two trials (Giuffrida 1999). In the U.S., a pay-for performance initiative aimed at getting physicians in a large health plan to increase cervical cancer screening, mammography and HbA1c testing rates resulted only in an improvement in cervical cancer screening rates compared to a comparator group. Physicians who were at or above the performance threshold improved the least, but they received the greatest share of bonus payments (Rosenthal 2005).
In Ontario, a provider and patient reminder system that supported bonus payments for preventative interventions provided approximately 250 physicians with reminder lists for preventative services. Practices were sent patient lists of those due or overdue for Pap smears, mammograms or flu shots, and patients were sent reminder letters. As a result, the rate of Pap smears increased from 71% to 78% and mammograms increased from 69% to 76% among eligible women over the 12-month study period (Sebaldt 2006).
Starting in 2004, family physicians in the U.K. had a component of their income based on their performance on 146 quality indicators (for ten chronic diseases, organization of care and the patient experience). The indicators were assigned points and each point was worth £76. Data from 7,547 practices found high achievement levels and the gap in achievement between affluent and practices serving the poor declined over three years (Doran 2006, 2008a, 2008b). But the program failed to reward the extra work required to achieve targets in deprived areas (McLean 2006) and some argue that overall the targets were set too low. Unintended effects included the sacrificing of patient-centred care during office visits to the quality improvement agenda, a decline in relational continuity and staff resentment. The potential for gaming, diagnostic creep and cream skimming has also been identified (Hutchison 2008).
A diabetes pay-for performance program in an HMO in the U.S. withheld 10% of payments and made them available based on shared savings. Performance improved for targeted indicators – HbA1c, LDL cholesterol, UA or U Microalbumin, diabetic retinal tests and an annual flu shot – but benefits were accrued in the first years of the program and then plateaued (Beckman 2008).
Similar challenges have been found in hospital-based pay-for-performance schemes. Related to the Value-based Purchasing (VBP) program in Medicare Hospitals, a study of 3,665 hospitals found resource-poor hospitals (serving minority and low-income patients) improved the least, and in some
16 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
instances fell further behind (Werner 2008). In Rand hospitals, the incentive payments often did not match level of investment required to improve performance; smaller hospitals were the most challenged (Sobero 2008). For the Hospital Quality Incentive Demonstration (HQID) project, two studies concluded that it improved quality (Grossbart 2006, Lindauer 2007), one found no effect on quality (Glickman 2007), and another found no effect on mortality or cost (Ryan 2008).
Performance Frameworks and Agreements
Provincial-regional and regional-service performance frameworks and agreements with evidence-based benchmarks can support continuous quality improvement by providing both a system and service-based perspective for achieving integrated, quality care. However, attributes of quality and patient experience indicators have traditionally been missing from these. Moreover, ideally performance agreements should be more closely aligned with quality improvement initiatives like the Quality Improvement collaboratives and Safer.Healthcare.Now! (OHQC 2008).
As an example, England’s National Health Service has national service frameworks which outline common indicators, explicit targets and standards for performance. The Department of Health sets system-wide priorities, policies, directives and timelines for the strategic health authorities. Each strategic health authority has multiple primary care trusts that contract with local general practitioner practices and hospital and mental health trusts. Primary care trusts and strategic health authorities develop clinical governance frameworks through which local health service provider groups are held accountable for continuous quality improvement and standards of care. Quality improvement activities are aligned with targets and performance agreements (Baker 1999).
Public Reporting
Public reporting is an integral part of a quality-focused healthcare system, and the public has a right to know how its tax dollars are spent and whether the healthcare system is meeting its expectations. Studies show a link between public reporting and quality improvement (Fung 2008, Sorbero 2008, Doran 2008, Werner 2008, Lindenauer 2007).
Ideally, performance agreements should align with public reporting. The Health Care Commission in the U.K. – an independent body that monitors and reports to the public on the performance of the healthcare system – reports on the performance measures included in the national performance framework. The public can view ratings for individual primary care trusts and hospitals. (See http://www.qof.ic.nhs.uk/ ). In Canada, Health Quality Councils are potential avenues for public reporting on primary care.
There can be unintended consequences resulting from public reporting. A culture of fear in healthcare organizations regarding the reporting of errors could impact on reporting. As an example, public reporting of adverse events may inadvertently discourage open disclosure of such events. Thus, public reporting needs to take place in conjunction with efforts to promote a “just culture” of quality improvement, where the focus is on improving systems rather than assigning individual blame.
Provider Training, Monitoring and Recognition
A quality improvement culture can be instilled in healthcare professionals through: its inclusion in medical school curricula; continuous medical education (CME) modules; team-based training (e.g., “Closing the Gap”); quality improvement skills building and training, (e.g., collaboratives); professional recognition awards; provider report cards based on comparative outcomes and patient-experience surveys; and licensing, accrediting bodies and board certification processes that include quality and patient-centred criteria (e.g., American Board of Medical Specialties).

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 17
As an example, three primary care practices in Ontario participating in an accreditation pilot project achieved improvements through: team behaviour and morale changes; regular practice meetings; human resource policies; implementation information protection and other legal requirements; physical facility improvements; waiting room changes; patient surveys; patient information and handouts; practice audits; infection control; medication management; and record keeping. The researchers concluded that the practice members gained increased confidence that they are providing quality care and planned to continue with continuous quality improvement processes (Levitt 2006).
A Patient Bill of Rights or Covenant, and an Ombudsman or Commissioner might also support quality improvement initiatives.
PRIMARY CARE PHYSICIAN SUPPLY
In 2006, there are 32,000 family physicians in Canada, up 5.7% from 2002. During that time the rate of growth of Canadian-trained specialists was 6.4% compared to 4.1% for family physicians.
In 2006, the ratio of family physicians to 100,000 population in Canada was 98; ranging from 84 in Ontario to 120 in Nova Scotia. The ratio of family physicians to specialists was 1.06. The average age of a family physician was 48.4 years, an increase of 1.8 years since 2002; one-third were female (CIHI 2007).
Impact of Physician Supply on Population Outcomes
There is significant evidence – mainly out of the U.S., but also from the U.K. – that the supply of primary care physicians has an impact on health outcomes. Evidence from the U.S. indicates that a higher ratio of general practitioners to population can result in improved outcomes in terms of life expectancy, all-cause mortality, stroke mortality, heart disease mortality, cancer mortality, reduced low birth-weight rates, and post neonatal mortality even after controlling for demographics and lifestyle factors such as smoking status (Shi 1994, 1999, 2004, Vogel 1998). The effect was found to be greater in non-urban areas (Shi 2005, Mansfield 1999) and with an increased primary care physician supply per 10,000 population (Starfield 2005). Conversely, a greater supply of specialists than family physicians was associated with higher mortality (Shi 2003, Campbell 2003).
In England, all-cause mortality rates were found to be lower in areas with a greater supply of primary care physicians per 10,000 population; one additional physician was found to be associated with a 6% decrease in mortality (Gulliford 2002). Lower rates of acute myocardial infarction mortality, avoidable mortality, acute hospital admissions and teenage pregnancies were also found, but statistical significance did not hold after controlling for socioeconomic status and practice structure and size (Gulliford 2004). Conversely, a study assessing the impact of access to primary care on health outcomes in Norway using the number of primary care physicians as a proxy for access to primary care found no significant relationship between mortality rates and the number of primary care physicians per capita (Aakvik 2006).
The supply of primary care physicians to the population has also been found to impact on prevention. In the U.S., states with higher ratios of primary care physicians to population have lower smoking rates, less obesity and higher seatbelt use than states with lower primary care physician ratios (Shi 1994, Shi 2000). A greater supply of family physicians has also been associated with earlier detection of breast cancer, colon cancer, cervical cancer and melanoma (Campbell 2003, Ferrante 2000, Roetzheim 1999, 2000, Schappert 1994).

18 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Canadian data on outcomes related to physician supply are few. However, in Ontario, fewer women receive prenatal care exclusively from family physicians then in the past and the majority of deliveries are performed by obstetricians. This is less so in northern regions. For children, there is an inverse relationship between the frequencies of primary and preventative care visits, and emergency department visits (ICES 2006).
Similar studies related to the supply of other primary care providers within a region or population were not found. However, some suggest that the structural characteristics of primary care practices may have as much, if not a greater, an impact on patient health outcomes than simply the availability of a primary care physician (Gulliford 2004). The impact of primary care teams is discussed further in the section entitled.Inter-professional.Team-based.Care.below.
Impact of Physician Supply on Reducing Health Disparities
In the U.S., studies have shown that the supply of primary care physicians is associated with reduced disparities in health status across racial and socioeconomic groups, after controlling for individual, community and state-level characteristics. Having a greater number of primary care physicians per population has a greater impact on all-cause, heart disease, stroke, cancer, low birth weight and infant mortality – as well as self-rated health status – the more disadvantaged the area served (Shi 1999, 2000, 2004, 2005).
In Ontario, disadvantaged populations have a lower health status, but they have a similar rate of annual primary care and specialist visits and receive less preventative care compared to those with a higher socioeconomic status, as do rural residents. These groups do receive a similar continuity of care to other socioeconomic groups (ICES 2006). While these disparities may be somewhat attributable to physician supply, structural and socioeconomic barriers are also important factors. (See the section entitled Access.for.At-risk.Patients.below).
A systematic review on the impact of interventions aimed at increasing the number of healthcare providers practising in underserved communities found evidence, although weak, that professionals from rural backgrounds were more likely to practice in rural areas. Clinical rotations in underserved areas might also impact on medical students’ decisions to work there, and incentive and support programs could potentially increase physician retention rates (Lewin 2008).
Impact of Physician Supply on Costs
Related to the cost associated with a greater supply of primary care physicians, based on Medicare spending in the U.S., states with a higher proportion of family physicians have lower costs and higher quality of care than those with a higher proportion of specialists (Baicker 2004). This result was also found within the U.S. adult (Franks 1998) and urban elderly populations (Mark 1996, Welch 1993). This is potentially due to better preventative care and lower hospitalization rates.
In contrast, the supply of specialists can be associated with higher costs and lower quality care. For example, the cost of care for common illnesses, such as community-acquired pneumonia, is higher when provided by specialists rather than general practitioners, with no difference in outcomes (Rosser 1996, Whittle 1998).
PAYMENT / DELIVERY MODELSThere is no definitive evidence on a “best” physician payment model, although a blended model appears to best mitigate the perverse incentives associated with each a fee-for-service, salary and capitation model (Coyte 1995, Hollander 1997, Robinson 2001, Deber 2004, Demers 2004, Gillet 2001).
A Cochrane review of primary care physician payment models found considerable variation in study setting and outcomes measured. Fee-for-service was found to result in more primary care visits, more specialist visits and more diagnostic and curative services, but fewer hospital referrals and repeat
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 19
prescriptions compared with capitation. Fee-for-service also resulted in greater continuity of care and higher compliance with a recommended number of visits, but patients were less satisfied with their access to their physician compared with salaried payment. There was no evidence on patient outcomes or the relative impact of salary versus capitation payment. The authors concluded that there was evidence to suggest that the method of payment can affect physicians’ behaviour, but the generalizability of the findings was unknown (Gosden 2000).
Fee-for-service does not adequately compensate for preventative care; may not adequately compensate for the time needed to make an accurate diagnosis and develop a care plan especially in complex cases; rewards providers for volume versus quality and adherence to guidelines; pays providers to treat adverse events; reinforces fragmentation of care; and increases the possibility of duplication of care (Miller 2007). Fee-for-service is also associated with weaker physician-patient relationships and reduced attractiveness of general practice (Gervas 1994).
There is evidence that community health centres – that generally have a salaried staff and target vulnerable populations – have had a significant impact on the quality of care. Generally, their patients, despite having poorer health status than the general population, are healthier than those similarly at risk who receive care at other types of primary care practices (O’Malley 2005). Patients who receive care in community health centres also receive more of the indicated preventative services (e.g., Pap smears and vaccinations) than the general population (AHRQ 2004, Regan 2003). In the U.S., across races and regions these patients are less likely to have low birth weights and there is less difference in birth weight between white and African American infants of mothers receiving care at community health centres, compared with the entire population (Politzer 2001, Regan 2003).
The Primary Healthcare Transition Fund projects in Ontario add to the evidence base related to impact of the various models of primary care practice on quality of care, health service utilization and physician satisfaction (McMurchy 2007):
In a comparison of primary care models among 138 practices, Community Health Centre (CHCs) scores for comprehensiveness of care, chronic disease management and health promotion were statistically significantly higher than those for capitated and fee-for-service (FFS) practices. CHCs were significantly more likely than other models to address healthy foods, home safety, exercise, and family conflicts. They were also more likely to cover smoking and alcohol consumption with their patients than FFS and Health Service Organizations. Health Service Organizations scored the highest in terms of accessibility — the ability to get same-day appointments, advice over the phone or after-hours care.
Among 44 primary care practices (CHCs, group and solo practices), an audit of 3,894 randomly selected charts, direct observation and key informant surveys found CHCs were significantly more likely than solo or group practices to have superior performance in prevention and promotion activities, well-baby visits, disease prevention for women, antenatal care, the management of type 2 diabetes, and up-to-date patient record systems.
In a study of 73 physicians in 45 salaried (CHC), capitation and fee-for-service practices, physician and practice characteristics explained a small proportion of the variance in scores from a chart audit. But payment by salary was statistically significantly associated with higher scores for preventative care and the treatment of diabetes, hypertension and urinary tract infections in this population. Scores for accommodations to disabled patients and accessibility were also higher in CHCs. Capitated and fee-for-service practices did not differ significantly in terms of their scores for accessibility, quality of care or practice or provider characteristics.

20 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
A study comparing chart data with respect to the screening, detection and control of hypertension among 135 physicians from fee-for-service (FFS), salaried (CHC) and capitation practices showed that screening rates for hypertension were high in all three models. Treatment with anti-hypertensives was highest for capitated patients, as was the percentage of patients within a range below the target set for their blood pressure.
Among 332 physicians, those in non-FFS models (salaried and capitation) had higher levels of work satisfaction, were more likely to be satisfied with their model of care and income, and were more likely to recommend it to others than physicians in the traditional fee-for-service models.
As well, in some projects, the nature of the primary care funding model impacted on collaboration and integrated service provision. For example, FFS payment appeared to present barriers to interprofessional collaboration (McMurchy 2007).
With regard to managed care programs, some have been found to result in decreased hospitalization rates, but to a lesser extent when targeted at disadvantaged populations (Medicaid) in the U.S. (Gill 1998, Paramore 1999). Managed care (e.g., the Kaiser Permanente diabetes management, Group Health Cooperative chronic care model and Veteran Affairs) has also been associated with improvements in preventative care and chronic disease management (Bodenheimer 2002, CHSRF 2005). The Kaiser Permanente triangle of care and the NHS improvement plan which stratify patients based on their needs and target services accordingly have has also shown some success. 1
Starting in the early 1990s, the National Health Service in the U.K. provided groups of family physicians (GP fundholders) budgets to purchase services for their patients. Hospitals were to compete for fundholder patients by offering shorter waiting times and could gain by attracting new fundholder business. Using this internal market approach had mixed results. It was found to somewhat improve communication and co-ordination of care, but was not found to be cost-effective and was associated with inequities in access (Deber 2006, Coulter 1995). Studies found the scheme reduced waiting times for procedures with long average waits, but no overall effect on fundholder waiting lists and no gains for non-fundholder patients were found. Moreover, fundholder incentives did not lead to more general changes in the hospitals; the narrow incentives in one part of the system did not lead to broader system reform (Deber 2006, Propper 2000).
1 In the Kaiser model level 1 is supportive self care, level 2 is chronic disease management, and level 3 is case management.
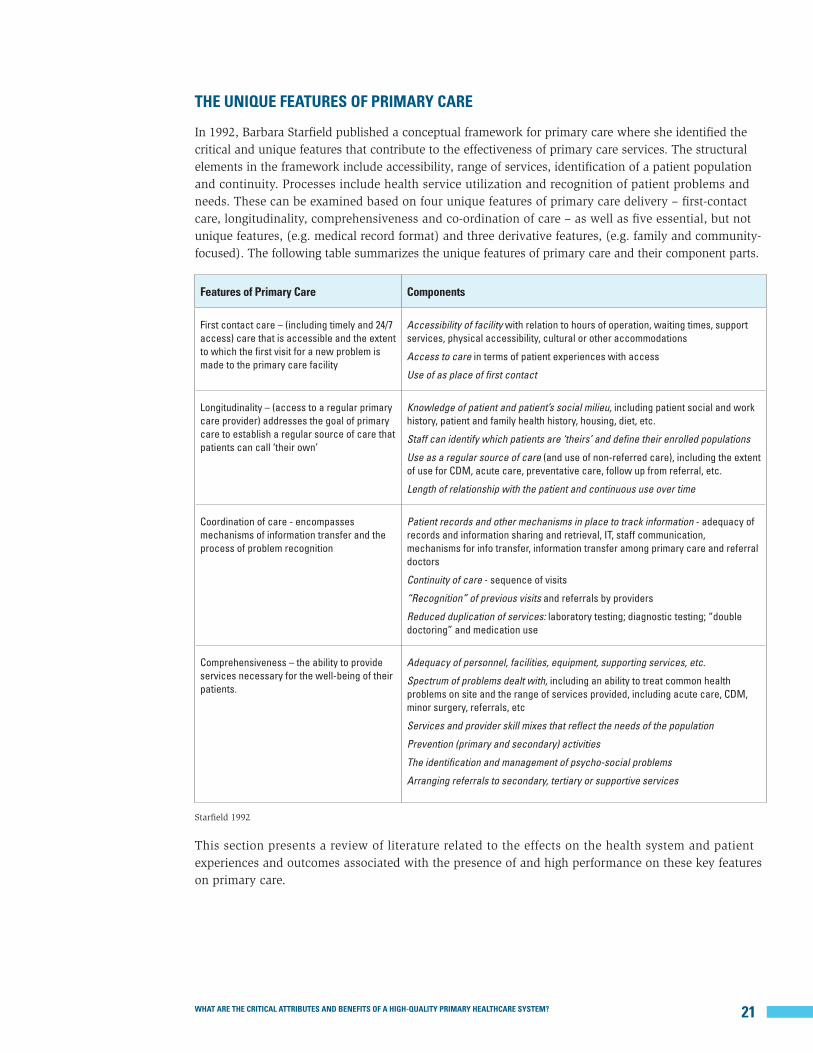
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 21
THE UNIQUE FEATURES OF PRIMARY CARE
In 1992, Barbara Starfield published a conceptual framework for primary care where she identified the critical and unique features that contribute to the effectiveness of primary care services. The structural elements in the framework include accessibility, range of services, identification of a patient population and continuity. Processes include health service utilization and recognition of patient problems and needs. These can be examined based on four unique features of primary care delivery – first-contact care, longitudinality, comprehensiveness and co-ordination of care – as well as five essential, but not unique features, (e.g. medical record format) and three derivative features, (e.g. family and community-focused). The following table summarizes the unique features of primary care and their component parts.
Features of Primary Care Components
First contact care – (including timely and 24/7 access) care that is accessible and the extent to which the first visit for a new problem is made to the primary care facility
Accessibility of facility with relation to hours of operation, waiting times, support services, physical accessibility, cultural or other accommodations
Access to care in terms of patient experiences with access
Use of as place of first contact
Longitudinality – (access to a regular primary care provider) addresses the goal of primary care to establish a regular source of care that patients can call ‘their own’
Knowledge of patient and patient’s social milieu, including patient social and work history, patient and family health history, housing, diet, etc.
Staff can identify which patients are ‘theirs’ and define their enrolled populations
Use as a regular source of care (and use of non-referred care), including the extent of use for CDM, acute care, preventative care, follow up from referral, etc.
Length of relationship with the patient and continuous use over time
Coordination of care - encompasses mechanisms of information transfer and the process of problem recognition
Patient records and other mechanisms in place to track information - adequacy of records and information sharing and retrieval, IT, staff communication, mechanisms for info transfer, information transfer among primary care and referral doctors
Continuity of care - sequence of visits
“Recognition” of previous visits and referrals by providers
Reduced duplication of services: laboratory testing; diagnostic testing; “double doctoring” and medication use
Comprehensiveness – the ability to provide services necessary for the well-being of their patients.
Adequacy of personnel, facilities, equipment, supporting services, etc.
Spectrum of problems dealt with, including an ability to treat common health problems on site and the range of services provided, including acute care, CDM, minor surgery, referrals, etc
Services and provider skill mixes that reflect the needs of the population
Prevention (primary and secondary) activities
The identification and management of psycho-social problems
Arranging referrals to secondary, tertiary or supportive services
Starfield 1992
This section presents a review of literature related to the effects on the health system and patient experiences and outcomes associated with the presence of and high performance on these key features on primary care.

22 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
First Contact Care / Accessibility
Accessibility
Two-thirds of Canadians say that it is very or somewhat difficult to get after-hours care without going to the emergency department. Based on the Commonwealth Fund’s study of seven
countries’ healthcare systems, 40% of Canadians do not have access to after- hours care (care other than 9 a.m. to 5 p.m. weekdays) from their regular healthcare provider, and 34% of primary care physicians report that they do not provide these services (Schoen 2006, 2007). This rate is similar to that in the U.K., but higher than the other countries studied.
Additionally, 22% of Canadians reported that it is somewhat or very difficult to contact their physician by phone during regular practice hours, and only 9% can communicate with their doctor or the practice by email (Schoen 2007). Twenty-two percent reported that they got an appointment to see their regular doctor on the same day they called, the lowest rate among the seven countries studied. Three in 10 waited six days or more – 10% more that the next closest countries, the U.S. and Germany (Schoen 2007).
Wait times that exceed expert-defined “clinically reasonable” waits for services can impact negatively on patient quality of life and outcomes, and increase costs (Western Canada Waiting List Project 2001, Canadian Institute for Health Information 2006, Saint-Jacques 2007, Lynch 2008). As well, where there is no after-hours care, long office waits, and long travel times, there is a reduced chance of a first-contact visit with a primary care physician for acute health problems (Forrest 1998).
Long waits for care are often viewed as a symptom of inadequate funding in the healthcare system, but they are also a reflection of inefficiencies. “For those who view waiting lists as mechanisms to allocate services, policy options focus on ensuring that waiting lists are properly managed and patients are appropriately prioritized to ensure equitable access to services and reduced adverse effects” (Western Canada Waiting List Project 2001). Studies indicate that long wait times often result from inadequate and uncoordinated processes related to patients flow and that process engineering approaches, including queuing theory and other industrial engineering techniques, can improve wait times through better management of queues (McIntosh 2005, Hurst 2003, Health Council of Canada 2005). Reforms in Canada and internationally have included: setting wait time standards based on the clinical judgment of experts; ensuring referrals are based on set criteria; standardized patient assessment and prioritization (e.g., the most urgent cases are seen more quickly); ensuring the systems work effectively together, including centralized wait lists rather than multiple queues; and wait time guarantees (Western Canada Waiting List Project 2001, Deber 2006).
Place of First Contact
Canada, the U.K., the Netherlands, Australia and New Zealand have primary care systems that require patients to see a primary care physician before getting care from a specialist.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 23
There is evidence to support the effectiveness of this model of care referred to as “gatekeeping” (Franks 1992). Having a primary care provider as an initial point of contact is associated with reduced consultation times, lower visit rates, fewer laboratory tests, less use of specialists and emergency departments, improved coordination of care and lower costs (Delnoij 2000, Hurley 1989, Martin 1989, Forrest 1996, 1998, Hjortdahl 1991, Raddish 1999, Roos 1998, Gervas 1994).
A study in Canada found that post-surgery outcomes for children with recurrent tonsillitis or otitis media were better when care was first sought from a primary care physician who then referred the children to a specialist compared to self-referral to a specialist (Roos 1979).
Gatekeeping does not necessarily compromise patient satisfaction (Gervas 1994), but it may impact on patient satisfaction if it is perceived to limit the responsiveness of the system or support rationing (Delnoij 2000, CHSRF 2002).
Longitudinality / Long-term Person-Focused Care
Access to a Regular Primary Care Provider
In the 2005 Canadian Community Health Survey, 85.6% of Canadians 12 years of age and over reported having a regular medical doctor (CCHS 2005, 3.1). According to the Commonwealth
Fund, 95% of Canadians feel that it is important to have one practice or clinic where the doctors and nurses know them and provide and coordinate their care. However, 9% report having no usual place or doctor from whom they regularly get care (Schoen 2007).
Those with a regular source of primary care tend to receive more appropriate preventative care, be more likely to have their health problems recognized, have fewer diagnostic tests and prescriptions, receive more accurate diagnoses, and have lower costs of care than individuals without a regular source of care (Starfield 1998). People without a regular source of primary care are more likely to delay visiting a physician in the presence of symptoms, are less likely to seek timely, requisite preventative services, and have higher mortality and healthcare costs (Starfield 2005).
Individuals who do not have a regular source of primary care are also more likely to receive care in emergency departments and to be hospitalized than those with a regular provider (Starfield 2005). There is evidence of an inverse relationship between adequate access to primary care and hospital admission rates for ambulatory care-sensitive conditions (ACSCs), particularly for complications related to diabetes, asthma, hypertension, diabetes and pelvic inflammatory disease (Brown 2001).
In Canada, 16% of the adult population reported going to the emergency department for a condition that could have been treated by their regular physician if he/she were available, and 45% of those with a chronic illness reported visiting the emergency department in the past two years, the highest rates among Commonwealth Fund study countries (Schoen 2007). Research from Manitoba suggests hospital admission rates for asthma, angina, pelvic inflammatory disease, gastroenteritis, congestive heart failure, severe ENT infections, epilepsy, bacterial pneumonia, tuberculosis, iron deficiency anaemia in children under six, dental conditions and cellulitus are impacted by access to primary care (Roos 2005).
Among those with chronic conditions in Ontario, individuals without a regular medical doctor were 1.22 times more likely to have visited an emergency department and 1.32 times more likely to have had a non-elective medical hospital admission in the past two years than those who reported having a regular doctor. Moreover, people with chronic illnesses who had fewer than three annual physician visits were 1.17 times more likely to have visited an emergency department and 1.19 times more likely to have had a non-elective medical hospital admission compared to those who had three or more physician

24 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
visits (Glazier 2008). Ontarians are also more likely to receive primary and secondary preventative care if they have a regular physician. For example, those who rely on walk-in or after-hours clinics for the majority of their primary care were less likely to have had a periodic health exam or a flu shot in 2003/04 (ICES 2006).
The length of the relationship with their primary care provider is associated with patient care experiences and outcomes. Very short-term relationships with physicians are associated with poorer outcomes (Starfield 2005); at least two years (and as many as five) are usually required for patients and providers to develop a relationship that will result in optimal patient-focused care (Starfield 1998). For example, previous knowledge of a patient increases the chances of a healthcare provider recognizing psychosocial problems that could impact on the patient’s health (Gulbrandsen 1997), and the longer the duration of the patient relationship with the primary care physician and those scheduling appointments with specialists is associated with a greater likelihood that patients referred to a specialist will actually follow through on the referral (Forrest 2007).
Some studies point to benefits related to an ongoing relationship with specific providers rather than simply with a particular practice (Starfield 2005). But others have found that physician continuity is not so much associated with better outcomes as the nature of the practice; the structure of the primary care practice – including practice and team coordination and adherence to guidelines – were found to have a greater impact on outcomes (Gill 2003, Parkerton 2004, Gill 1998).
Access for At-risk Patients
Having a regular source of primary care can reduce the adverse effects of low socioeconomic status on health, and can result in less difference in self-rated health between those in the higher and lower income categories (Shi 2002). The disadvantaged report better healthcare experiences when they have good access to regular primary care (Starfield 2005).
In the U.S., rates of access to a regular source of primary care range from 80% for those in the lower income categories to about 90% for those in the middle income range and 95% for those with high incomes (AHRQ 2004). In one U.S. study of disadvantaged populations, fewer of those receiving adequate regular primary care reported poor health and depression than those receiving less adequate primary care (Shi 2002), and adolescents with a regular source of care were more likely to receive the requisite preventative care and less likely to receive care in emergency departments (Ryan 2001).
A study in England found immigrants, refugees, the elderly and those with mental health conditions had difficulty accessing health services. They faced problems navigating an entry point to services, especially complex services under different administrative or organizational jurisdictions. Initiatives aimed at increasing the supply of services and helping people access services, through improved coordination, collaboration and integration were most likely to improve system navigation for disadvantaged groups. Improvement was greater when local initiatives were supported by national frameworks and policies that addressed social exclusion and provided financial incentives (Goddard 2008).
Several targeted primary care initiatives – funded by the Primary Healthcare Transition Fund – aimed at addressing the needs of at-risk, vulnerable patients in Ontario and providing them with a regular source of care increased their regular access to, and continuity of, care (McMurchy 2007):
Nurses providing care in Canadian Mental Health Association offices where patients were most comfortable and spending more time with patients increased the quality and continuity of care for those who otherwise would not likely have accessed primary care services.
An interdisciplinary team at a Salvation Army site effectively delivered primary and mental healthcare and social services to homeless men, women and street youth.
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 25
Street youth, who would not have otherwise accessed care, received primary care at a drop-in centre; most declined to join the associated primary care practice.
For pregnant substance users, “one-stop shopping” with coordinated and comprehensive medical and addictions care helped overcome treatment barriers and improve maternal and neonatal outcomes. Receiving multiple services at one location meant they were more likely to continue attending and develop positive relationships with providers.
Eight clinics based at Early Years Centres, public housing complexes and public elementary schools provided well-baby checks, breastfeeding support, reproductive health counselling, diabetes education, parenting support, treatment of common illnesses, immunization, chronic disease screening, annual health exams and health promotion services to those at high-risk.
Minority women received the following services at a homeless women’s drop-in centre: i) primary care services focusing on homelessness, mental health, anti-oppression and cultural competency; ii) a navigator program to coordinate referrals to referral agencies and specialty clinics; and iii) health education workshops.
Having health insurance has a significant impact on access to primary care. In the U. S., having health insurance facilitates access to primary care and the disadvantaged who do not have health insurance are less likely to have a regular source of primary care, and are thus hindered in their access to the entire healthcare system (Lillie-Blanton 2005, Starfield 2004). Better health outcomes have been found among minorities in the U.K. (where there is universal coverage) compared to minorities in the U.S. For example, a black population in London had similar rates of diabetes-related lower-extremity amputation to whites, whereas in the U.S., they had rates two to three times higher than the white population after controlling for socioeconomic differences (Leggetter 2002, van Doorslaer 2004), suggesting that a universal healthcare system oriented toward primary care services can reduce disparities in health outcomes (AHRQ 2004).
Coordination of Care
Continuity
The literature discusses three main types of continuity of care. Relational continuity –referred to above as longitudinality – is “the ongoing therapeutic relationship between patient and provider(s).” Managerial continuity is “the consistent and coherent approach of several professions to the management of health conditions (especially if chronic or complex) that is responsive to a patient’s changing needs.” Informational continuity is the “use of information, either documented or in the memory of providers, on past events and personal circumstances, to make current care appropriate for the individual” over time (Boerma 2006, Haggerty 2003).
Effective managerial continuity of care is associated with greater patient satisfaction, better patient compliance, saved consultation time, fewer laboratory tests, less hospitalization and emergency department use and lower costs (Freeman 1997, Mainous 1998, Rosenblatt 2000, Forrest 1996, 1998, Hjortdahl 1991, Raddish 1999, Roos 1998).
Studies have found associations between hospitalization and continuity of care for chronic ambulatory care-sensitive conditions (ACSC), but not necessarily for acute ambulatory care-sensitive conditions (Gill 1998). People with chronic illnesses in Ontario who visited a physician three or more times in a two-year period – but had poor continuity of care – had 1.55 times more visits to the emergency department than those with high continuity of care. They also had 1.35 times more non-elective medical hospital admissions (Glazier 2008). As well, a population-based study in Manitoba found a small but statistically significant relationship between continuity of care and the frequency of emergency department visits. Greater continuity of care was also associated with the frequency of cervical cancer screening, influenza vaccinations and pneumococcal vaccinations. However, the association between
26 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
continuity and improved preventative care and reduced emergency department did not hold after controlling for socioeconomic status (Menec 2005).
Collaborative models have been shown to promote continuity of care, as has case management, although there is no evidence that any one model is superior (Saltman 2006, Poulton 1993, Temmink 2000, Shum 2000, Calnan 1996, Renders 2001, Faulkner 2003, Murchie 2003, Oakeshott 2003, Vlek 2003). In Ontario, care navigators working in a family practice helped to improve continuity and quality of care (McMurchy 2006).
Long wait times for appointments, the lack of insurance and no after-hours care have been associated with lower levels of continuity (Forrest 1998). A U.K. report on improving continuity recommends targeting, flexibility and evaluation (Deber 2006).
Integration
Among Canadians surveyed for the Commonwealth Fund study, 47% always get help from their main place of care coordinating their care with other health services. The last time they saw a
new specialist, 63% were helped by their regular provider decide who to see (Schoen 2007).
Forty-six percent of their primary care physicians reported that they often (5%) or sometimes (41%) experience problems because care is not well coordinated across multiple sites or
providers (Schoen 2006). Moreover, 16% of patients with chronic conditions reported they often or sometimes received conflicting information from different doctors, nurses or other health professionals (Schoen 2007)
Systematic reviews suggest that the integrated delivery of health services is associated with improved patient outcomes (Wensing 2006). Systems specifically designed to enhance coordination between primary care physicians and specialists may result in lower hospitalization rates and resource use (Talbot-Smith 2004, Feachem 2002). Studies indicate that communication is critical to improved integration and that effective coordination depends on existing organizational structures (Deber 2006).
In Taber, Alberta, an integrated primary care project showed that more integrated delivery of primary care services can result in: improved service delivery; more efficient use of physicians, hospital and laboratory services; healthier lifestyles; reduced health service utilization; and higher patient satisfaction (Hasselback 2002).
A systematic review, looking at the impact of formalized relationships between primary care physicians and specialists on patient health outcomes, found most health outcomes unchanged. However, some physical and functional health outcomes improved, especially among patients with mental health conditions. Improvements were found in patient retention rates in treatment programs, patient satisfaction, and primary care and specialist physician behaviour – including “more rational use of resources and diagnostic tests, improved clinical skills, more frequent use of appropriate treatment strategies, and more frequent clinical behaviours designed to detect disease complications” (Mitchell 2002).
A Cochrane review of shared chronic disease care between generalists and specialists found improvements in prescribing, but no consistent improvements in physical or mental health outcomes, psychosocial

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 27
outcomes, measures of disability and functioning, hospital admissions, default or participation rates, recording of risk factors, or satisfaction with treatment. The authors concluded that these results were likely due to methodological shortcomings, the multifaceted nature of the interventions, and short follow up (Smith 2007).
Some maintain that as long as the services are available to patients, there are no apparent gains from co-location of specialists within the primary care setting (Wensing 2006). But the results are mixed depending on the type of provider. For example, when pharmacotherapy specialists were based at primary care sites, they identified a greater number of patient problems and made more medication-related recommendations, although no differences in health-related quality of life were found (Dolovich 2001).
A Cochrane review of interventions aimed at improving referrals to specialists from primary care concluded that the referral process would likely improve if referral guidelines were distributed with the standard referral forms and providers were involved in the teaching about appropriate referring. Simply distributing guidelines and giving feedback to physicians about their referring practices were deemed unlikely to improve practise. As well, seeking a second in-house opinion before referring and/or enhancing the comprehensiveness of the in-house services provided (e.g., access to other primary care providers) may improve the referral process. The impact of various physician payment schemes on referrals is inconclusive (Akbari 2005). Another study concluded that patient referral completion rates could be increased by primary care practices further assisting patients with scheduling their specialist appointments (Forrest 2007).
Adequacy of Patient Records and Information Retrieval
Electronic medical records form an information “backbone” for many health administrators and providers in Canada and are “fundamental to the ability of a team of health professionals to
collaborate” (Standing Committee on Social Affairs, Science and Technology 2002). But many primary care physicians lag behind in the use of technology and clinical information systems. The Commonwealth Fund survey revealed that only 23% of primary care physicians in Canada use electronic medical records compared to 79% or more of the primary care physicians in Australia, the Netherlands, New Zealand and the U.K. Use within Canada is highest in Alberta, where approximately 60% of family physicians use computers for their medical records (Protti 2007). Additionally, only 27% and 15% of Canadian primary care physicians respectively have electronic access to patients’ test results and hospital records. And only one in ten have systems that generate drug alerts, prompts to provide patients with test results or reminders for preventative or follow-up care (Schoen 2006, Hutchison 2007).
Even among those with electronic medical records, their functionality is inferior to that in New Zealand, Australia and the U.K. Canadian physicians mainly lag behind because implementation has been at their discretion and investing in them is perceived as forgone personal income (Hutchison 2007); they often lack the training and requisite skills to adopt the technology; there is no standardization of use across most jurisdictions (College of Family Physicians of Canada 2007); and there are challenges related privacy concerns (Protti 2007) and behavioural change (Lorenzi 2000).
There is recognition in Canada of the importance of moving to electronic medical records in order to improve quality and timeliness in healthcare delivery (Standing Committee on Social Affairs, Science and Technology 2002); moving from paper to electronic records is said to be “essential to modernizing and transforming the healthcare system”(Canada Health Infoway 2002) In its October 2002 report, the Standing Senate Committee on Social Affairs, Science and Technology, chaired by Senator Michael Kirby, summarized the benefits of EHRs:

28 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
[They].can.make.patient.data.available.to.healthcare.providers.and.institutions.anywhere.on.a.need-to-know.basis.by.connecting.interoperable.databases.that.have.adopted.the.required.data..and.technical.standards..Not.only.can.a.[EMR].system.greatly.improve.quality.and.timeliness..in.healthcare.delivery;.it.can.also.enhance.healthcare.system.management,.efficiency.and.accountability.(Standing.Committee.on.Social.Affairs,.Science.and.Technology.2002).
Electronic medical record functionality can support the delivery of high-quality primary care, and the use of these information systems can highlight and clarify where improvements are needed. Systematic reviews have found that using electronic medical records with reminder systems and clinical decision-support systems can lead to enhanced preventative care and the management of conditions like hypertension, diabetes and HIV, increased the prescribing of generic drugs and improved drug dosing, longer consultations, fewer unnecessary tests and cost savings. The evidence is not as definitive in terms of improving diagnoses, but there is evidence of improvements in disease markers (Mitchell 2001, Hunt 1998).
Disease registries can also be used to monitor and improve clinical care, develop best practices and guidelines and monitor system performance. These population-based registries have the potential to be used as reminder systems, feedback to physicians and/or planning and monitoring individual patient care. Electronic medical records can augment the use of disease registries and administrative data to monitor and manage treatment (Robinson 1997, Lix 2006).
Information Coordination and Communication
Ten percent of primary care physicians in Canada reported that a patient’s medical record or clinical information is often unavailable at the time of a scheduled visit (Schoen 2006). For example,
three in ten Canadians reported that their physician was not informed and up-to-date about follow-up plans post-hospitalization (Schoen 2007). Fifty-eight percent of their physicians usually wait 15 days or more for a full report post discharge, and 25% wait more than 30 days or rarely receive a report (Schoen 2006). After a visit to the emergency department, 57% of patients reported that their regular doctor was informed and up-to-date about their care. Three-quarters said their regular doctor provided the specialist with information about their condition the last time they saw one (Schoen 2007), rates generally as high as or higher than the six other countries in the Commonwealth study. But, 15% of primary care physicians said they get information back for only half or fewer of their patients after a referral (Schoen 2006).
Two-thirds of Canadians reported that their physician or the place where they usually get healthcare always knows important information about their medical history (Schoen 2007); 23% report their physician has an electronic medical report (Schoen 2006). Eleven percent said their test results or medical records were not available at time of a scheduled appointment, 9% reported delays in receiving the results of abnormal tests at some point over the past two years, and 5% reported having had a duplicate test (Schoen 2007). Twenty percent of primary care physicians confirm that they often (3%) or sometimes (17%) need to repeat tests or procedures because results are unavailable (Schoen 2006).
Communication and the longitudinal information sharing among providers within the circle of care are critical to effective primary care delivery. “Continuity of information between and among healthcare providers correlates with improved quality of care, administrative processes and patient safety” (Conference Board of Canada 2006).
Using technology, such as e-mail, electronic medical records and videoconferencing, can make it easier for healthcare providers to collaborate, get the patient information they need and reduce duplication.
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 29
Information technology can improve the team’s ability to access and share data, including relaying “just-in-time” information about a patient, accessing information when they are off site, and communicating about scheduling, work hours and events such as training sessions (College of Family Physicians of Canada 2007). Information sharing is also facilitated by system-to-system interoperability, which requires standardized data format and content and an overall information exchange infrastructure (Gamble 2006). But, as the College of Family Physicians of Canada points out: “it is important to acknowledge that information technology itself is merely a tool that facilitates information management” (College of Family Physicians of Canada 2007). The rest is up to the individuals using it.
Comprehensiveness
The Primary Care-Specialist Balance
As mentioned above, the degree of comprehensiveness in primary care (i.e., the extent to which a broader range of services are provided within primary care rather than through referrals to specialists) is one of the defining features among countries with high performing primary care systems (Starfield 2002).
Achieving the right balance between primary and specialist care is important to optimizing health outcomes. Patients cared for by family physicians with specialist consultation have been found to have lower hospital readmission rates than those cared for by family physicians alone (ICES 2006). Studies on quality indicate that specialists tend to be better at adhering to the treatment guidelines for their area of speciality, including preventative procedures, laboratory tests and appropriate prescriptions (Starfield 2005, Harrold 1999). In Ontario, rates of dispensing medications for congestive heart failure were lower and mortality rates higher for patients under the care of family physicians rather than specialists (ICES 2006). A systematic review suggests specialist outreach clinics could positively impact access to care, quality of care, health outcomes, patient satisfaction and the use of hospital services, although the quality of the evidence was poor (Lewin 2008).
Nevertheless, other studies conclude that the quality of care for common conditions is the same or better in primary care (Starfield 2008, Donohoe 1998, Grumbach 1999). For example, in a U.S. study, those who reported having a primary care physician rather than a specialist as their regular source of care had lower five-year mortality rates after controlling for differences in health and demographic characteristics (Franks 1998). As well, primary care physicians were as effective, if not more effective, in monitoring and reducing rates of diabetic complications, achieving glycemic control and reducing hospital readmissions (Parnell 1993, Kaag 1996).
Studies in the U.S. have found no effects related to an increase in the supply of specialists in terms of all-cause total mortality, heart and cerebrovascular disease mortality, cancer mortality, infant mortality and low birth weight, as well as the early detection of cervical cancer, colorectal cancers, breast cancer, and melanoma (Starfield 2005b). There is evidence that community-based specialists may overestimate the likelihood of illness in patients and consequently use inappropriate diagnostics and treatments (Franks 1992, Hashem 2003, Sox 1996).
Referral decisions are influenced by patient, physician and health system characteristics, but patient characteristics have been found to have the greatest effect on referrals. Low provider tolerance for uncertainty, large practice size, gatekeeping arrangements and practices with high levels of managed care were also associated with referral rates. Discretionary referrals have been found to be higher with capitated payment models and a high concentration of specialists in the community (Forrest 2006).
Barbara Starfield concludes that:
Primary.care.physicians.do.at.least.as.well.as.specialists.in.caring.for.specific.common.diseases,.and.they.do.better.overall.when.the.measures.of.quality.are.generic..For.less.common.conditions,.the.care.provided.by.primary.care.physicians.with.appropriate.backup.from.specialists.may.be.the.best;.for.rare.

30 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
conditions,.appropriate.specialist.care.is.undoubtedly.important,.as.primary.care.physicians.would.not.see.such.conditions.frequently.enough.to.maintain.competence.in.managing.them.(Starfield.2005).
Importantly, the role of primary care providers in providing effective, quality healthcare is to ensure appropriate referral of patients and reduce unnecessary or inappropriate specialist care.
Preventative Care
In 2005, 34% of Canadians aged 12 or older received a flu vaccine within the past year, and 53% of those with one or more chronic condition received one. Rates varied from 22% in
Newfoundland to 41% in Nunavut and 42% in Ontario (Statistics Canada 2005). Two-thirds of Canadians 65 and over received a flu shot, a rate lower than that of the U.K. and France (Health Canada 2006).
In 2005, 73% of women 18 to 69 had a cervical screening within the past three years, and 51% of women 50 to 69 had a mammogram within the two previous years (Statistics Canada CCHS 3.1).
Prevention strategies occur at the population and individual level. Immunization provides benefit by reducing the incidence of certain infectious diseases. Systematic reviews of strategies to improve immunization rates have found moderate evidence of increased immunizations supported by reminder and recall systems, such as letters, telephone calls and the use of text messaging reminders (Lewin 2008). Health promotion, prevention activities and screening (e.g., for cancer, diabetes, hypertension) can help prevent chronic illness or mitigate its severity, although the benefits will mainly accrue over time.
For the elderly, falls prevention can save money and improve health outcomes (Wagner 1994). Preventative primary care outreach for the elderly can reduce the risk of mortality among those living in community and increase their probability of living in the community (Ploeg 2003).
The impact of preventative interventions depends on the nature of the intervention and the individual. Some of the literature suggests that primary prevention is potentially valuable in the long run, but is unlikely to have a major short-term impact on the use of hospital and specialist services for most non-infectious diseases (Hirdes 1994, van Haastregt 2000, Elkan 2001, Congressional Budget Office 2007).
Reasons for inadequate prevention include a lack of awareness about the benefits among the public and a focus on treatment rather than prevention among clinicians.
There is an association between performance related to the unique features of primary care and the provision of preventative services. Strong performance on the primary care attributes discussed in the section has been significantly associated with patients being up-to-date on screening, immunization and lifestyle counselling services, as well as having smoking cessation interventions (Flocke 1998, Saver 2002).

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 31
Chronic Disease Management
According to the Conference Board of Canada, compared to 16 other developed countries, Canada ranks tenth in performance on ten indicators. We get a “B” on mortality rates due to
cancer, circulatory and respiratory disease, and mental health conditions, and a “C’ for mortality related to diabetes and musculoskeletal diseases (Conference Board of Canada 2008).
Fifty-five percent of Canadian primary care physicians reported that their practice is well prepared and 40% say it is somewhat prepared to provide optimal care for patients with chronic diseases; 50% reported being well prepared and 48% somewhat prepared to address patient mental health problems, including depression. These rates are the lowest among the seven countries included in the Commonwealth Fund primary care study (Schoen 2006).
Canadian primary care physicians are also the least likely to routinely provide their patients with written instructions about how to manage their chronic disease at home. One-quarter never do so (Schoen 2006). One-third of patients with a chronic condition reported having been given a written plan or instructions to manage their care at home, and 40% have received reminders when they were due for preventative or follow-up care for their condition, again the lowest among the seven countries (Schoen 2007).
Critical supporting factors
The effective prevention and management of chronic diseases can improve outcomes and help to avoid the high cost of acute care in future. Critical elements identified for ensuring high quality chronic disease prevention and management are: the development and use of clinical pathways, protocols and guidelines and the provision of evidence-based care; collaboration among providers; improved screening and disease control; integration, coordination and continuity of care; and longitudinal clinical records shared among providers (Health Council of Canada 2005, Deber 2006, Temmink 2000).
Another study identified the ten essential components of chronic disease management as: using inter-professional teams; using information systems to get patient and population data; identifying patients with chronic disease; stratifying patients by risk; involving patients in their care; coordinating care; integrating specialist and generalist expertise; integrating care across organizational boundaries; minimizing unnecessary visits; and providing care in the least intensive setting (Dolovich 2001).
Impact
Interventions aimed at managing and preventing chronic disease in primary and community care settings have been shown to be effective and have a positive impact on the use of secondary and emergency care, waiting lists and other services (Health Council of Canada 2005).
Inadequate prevention and treatment of chronic diseases can result in increased health service utilization and costs. For example, among Medicare patients in the U.S., those with chronic conditions were more likely to have a preventable hospitalization and they account for up to 17% of Medicare reimbursements for inpatient, outpatient and physician services (Culler 1998).
There is significant variation in the content of disease management programs and the outcomes measured. Nonetheless, the evidence strongly suggests that chronic disease management programs have the potential to lead to improved clinical outcomes, including reduced morbidity and mortality and improved quality of life, although this depends on the severity of the disease. The Congressional Budget Office in the U.S. found that congestive heart failure, coronary artery disease, and diabetes programs could reduce hospital readmissions and lengths of stay (Congressional Budget Office 2002).
32 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
The literature suggests that a multi-faceted and tailored approach to patient care, part of many chronic disease management programs, construes the greatest benefit (Deber 2006).
There are numerous examples of the benefits of effective chronic disease management:
A Cochrane review of 41 studies of multifaceted interventions to improve the management of diabetes by targeting health professionals and/or the management of care (e.g., regular patient reminders, recall and review) found improved process outcomes (most studies did not assess clinical outcomes). Positive effects on patient health outcomes were found in the interventions that included patient education or an enhanced nurse role (Renders 2000).
A systematic review found that in 32 out of 39 studies interventions using chronic disease management models improved at least one process or outcome measure for diabetic patients (Bodenheimer 2002).
The Veterans Affairs Administration chronic disease management program has halved hospital days and reduced urgent care visits, while increasing primary care-based visits, consultations and tests (U.K. Department of Health 2004).
In a U.S. HMO, a disease management program was associated with improvement in the federal government Health Plan Employer Data and Information Set (HEDIS) quality measures, (e.g., cancer screening, immunization, diabetes care and cholesterol management) (Sidorov 2002).
Patients in a diabetes management program at a large primary care network in the U.S. had improved blood glucose control and were 16% less likely to be hospitalized (Greisinger 2004).
In Australia, compared to control sites, a recall system with outreach services achieved significant improvements in diabetes monitoring and test results and reduced hospitalizations for diabetes-related conditions by 32% in an indigenous population (McDermott 2001).
An asthma intervention in a large group practice that included a patient registry, a systematic approach to asthma assessment, case management and physician education improved asthma diagnosis and patient education, and reduced emergency department visits and hospitalizations related to asthma, but did not improve the documentation of peak flow meter ownership or use, smoking cessation advice or influenza vaccination rates (Patel 2004).
A randomized controlled trial of an asthma intervention for children in the U.K. found changes in consultation and prescriptions patterns and reduced hospital admissions in the intervention year, but not in subsequent years (McCowan 1997).
Research suggests that comprehensive management programs for chronic obstructive pulmonary disease can reduce patient limitations, health service utilization and medical costs, and improve health-related quality of life (Ferguson 1998, Lacasse 1996, Lacasse 1997).
Programs for managing congestive heart failure have shown improvements in the quality and outcomes of care, including fewer hospitalizations (Lorig 1999).
A Disease Management Outcomes Consolidation survey found reduced self-reported hospital admissions, increased preventative care and improved clinical outcomes (Fitzner 2005).
A study of hospital admission rates for asthma, diabetes, heart failure, hypertension and chronic obstructive pulmonary disease for patients at 31 primary care trusts in London found no relationship between improved asthma services in primary care and asthma-related admission rates. But admission rates for diabetes were significantly associated with the presence of diabetes programs in primary care. There was no association between prescribing levels in the primary care trusts

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 33
and admission rates for the conditions examined. A significant association was found between admission rates and overall measures of health status and material deprivation (Saxena 2006).
The active management of chronic conditions at the Castlefield Health Centre in the U.K. resulted in a reduction in hospital admissions, length of stay and bed days for the elderly, as well as more appropriate referrals and response times for social service assessments (U.K. Department of Health 2004).
The Evercare case management model for the elderly in the U.S. halved unplanned hospital admissions, reduced medication use with concurrent health benefits and increased patient and provider satisfaction (Department of Health, U.K. 2004).
Despite of the proven benefits of chronic disease management programs, Starfield maintains that the impact of primary care on mortality and morbidity can be somewhat attributed to a person-centred focus in primary care settings rather than simply the management of a particular disease (Starfield 2005). She argues against single-disease management models, advocating for management in the context of ongoing, comprehensive primary care accompanied by close coordination between generalists and specialists (Starfield 2003). The evidence would indicate that targeting the most groups most likely to benefit, including the most vulnerable, is likely to construe the most benefit. This will likely vary by condition (Deber 2008).
Cost
Chronic disease management programs have been found to reduce hospital admissions, readmissions and length of stay, but the impact on costs is indeterminate. There is inconclusive evidence that these programs translate into cost savings, but there is also insufficient evidence to conclude that they do not save money (Starfield 2005, Congressional Budget Office 2002).
Eighteen out of 27 studies on congestive heart failure, asthma and diabetes programs found reduced healthcare costs or reduced healthcare service utilization. Authors concluded that the chronic disease management model had the potential to improve care and reduce costs (Bodenheimer 2002). A study in a U.S. HMO found a chronic disease management program to be associated with reduced costs and healthcare utilization suggesting that chronic disease management may result in cost savings and that quality improvement efforts are not necessarily associated with overall increased costs (Sidorov 2002).
An analysis of chronic disease management programs implemented by the Kaiser Permanente Medical Group in Northern California found evidence of substantial quality improvement, but not cost savings. “The causal pathway—from improved care to reduced morbidity to cost savings—has not produced sufficient savings to offset the rising costs of improved care. We conclude that the rationale for chronic disease programs, like the rationale for any medical treatments, should rest on their effectiveness and value” (Fireman 2004).
Critics of chronic disease management models that include specialized teams working with primary care physicians argue the programs are not sustainable in the long term because of their cost and the need for sophisticated information systems. Supporters contend that despite their cost, the programs can pay for themselves through reduced hospitalization rates (Bodenheimer 2003).
In this regard, policy makers are often faced with the challenge of making resource allocation decisions to invest in improving outcomes where there are proven cost savings versus instances where physical and mental well-being has improved and patient satisfaction is higher, but there is no evidence of decreased visits to emergency departments or hospital admissions.
34 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Patient Education, Involvement and Self-management
Patient-centred approaches can improve the quality of care and outcomes, and improved education and information can increase patient knowledge and engagement in care. The patient experience, service use, behaviour and health outcomes can improve with increased specificity and personalization of information, team-based care, and sufficient time for long-term behaviour change (O’Connor 2008). A Cochrane review of interventions to promote patient-centred approaches among providers found that (in spite of the heterogeneity of the studies) some interventions can lead to a significant increase in patient centredness during patient encounters. There was also evidence that provider training in patient-centred approaches could have a positive impact on patient satisfaction (Lewin 2001).
Improved management of diabetic patients, with an emphasis on coordination of care and self-management, was found to decrease hospital admissions and unscheduled primary care visits (Graham 1998). A Cochrane review of programs with patient action plans for those with chronic obstructive pulmonary disease (COPD) found increased recognition and appropriate reaction to symptom exacerbation among patients through self-initiation of antibiotics or steroids, although there was no evidence of changes in health service utilization (Turnock 2005). A self-help course that taught those with arthritis about their disease and its treatment, combined with tailored treatment and support, reduced patients’ perceived pain and costs (Kruger 1998).
A Cochrane review of interventions to improve the involvement of elderly patients found pre-visit preparation led to more questions and active self-reporting by the intervention group. One study (with a booklet and pre-visit session) showed no difference in consultation length between the intervention and control groups. Another showed greater satisfaction with the interpersonal aspects of care, but not in overall satisfaction. There was no long-term follow up to determine whether the effects were sustained (Wetzels 2007).
In Ontario, COMPETE III included patients in the monitoring and care of their vascular health. Patients valued, used and were motivated by online access to personal health information. They liked the easy access to their information and making appointments online. Patients showed improvement in follow-up consultations, made behavioural changes and rated their continuity of care and ability to improve their vascular health significantly better than control patients. Physicians reported it helped patients become more involved in their care and improved patient and family knowledge of vascular risk and disease (Holbrook 2006).
Also in Ontario, diabetic patients using a mobile phone monitoring system to monitor blood pressure had improved blood pressure control. The system improved patient self-monitoring, autonomy and clinical decision making. Patients were enthusiastic about the self-care aspect of the system, confident in their ability to use it, perceived only a few barriers to use and were comfortable using mobile phones as the primary means of communication (Logan 2006).
A systematic review of strategies with greater patient involvement in their care found that shared clinical decision-making interventions improved patient experience and knowledge, and that self-care and chronic disease self-management interventions resulted in improved behaviour, health status, care experience, knowledge and health service utilization (Coulter 2007). As well, patient decision aids have been shown to reduce the rates of discretionary surgery (O’Connor 2001).
There are a number of examples of effective models of patient shared decision making, including the Group Health Cooperative in Seattle, the Dartmouth-Hitchcock Medical Center, Veteran Affairs, and the Foundation for Informed Medical Decision Making. In Canada, the Primary Healthcare Transition Fund projects with a shared decision-making component included: Alberta’s Misericordia Health-Lifestyle Improvement Education Centre project; Integrated Population Approach Care Model for Patients Suffering from a Chronic Illness project in Quebec; and a Program Evaluation of Diabetes Centres in the Capital Health Region.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 35
Inter-professional Team-based Care
In a recent Statistics Canada report, almost 40% of Canadians reported having access to a primary care team (a nurse or other health professional) at their regular place of care. Those
with two or more chronic conditions and those reporting a “fair or poor” health status were more likely than those reporting a better health status to have access to a primary care team (Khan 2008).
One-third of Canadian primary care physicians report that they routinely use inter-professional teams in their practice, one-quarter routinely use other professionals to help manage patients with multiple chronic diseases, and 22% use them to routinely provide primary care services to their patient population. However, only three in ten definitely support expanding the roles of non-physicians in delivering care to their patients (Schoen 2006). In Ontario, most primary care is delivered in the solo practices, with approximately 30% of primary care physicians practising in this manner in 2003/04. Having a group affiliation is associated with physician age and geographic location, but not gender (ICES 2006).
Critical supporting factors
The Enhancing Interdisciplinary Collaboration in Primary Healthcare (EICP) framework describes the characteristics of a systemic approach to primary healthcare and identifies the following elements required to sustain collaborative teamwork: 1) health human resources; 2) funding; 3) liability; 4) regulation; 5) information and communications technology; 6) management and leadership; and 7) planning and evaluation (Conference Board of Canada 2006).
Grumbach and Bodenheimer identify five key characteristics of cohesive healthcare teams: 1) clear goals with measurable outcomes; 2) clinical and administrative systems; 3) division of labour; 4) training of all team members; and 5) effective communication. Moreover, the research suggests that teams with greater cohesiveness are associated with better clinical outcome measures and higher patient satisfaction (Grumbach 2004). The Ministry of Health and Long-Term Care in Ontario provides the following suggestions to Family Health Teams regarding maintaining their collaborative team (Ministry of Health and Long-Term Care 2005):
maintain a shared focus
regularly re-appraise team/project goals
have regular ongoing communication
resolve difficulties or conflicts as they arise
have regular meetings in which all feel involved
recognize the contributions of all team members
recognize the impact of the arrival and departure of team members
hold appropriate orientation of new team members
provide opportunities for team members to meet for social events
Team building is a critical factor in the ongoing success of a primary care practice. While it is most intensive at the beginning, it is an ongoing incremental process. Every group or team will go through
36 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
a number of stages as members get to know each other, learn about their respective skills and potential contributions, build trust and common purpose, establish roles and working relationships and gradually become able to take greater responsibility for decisions and activities.
Impact
A CHSRF-funded synthesis presents evidence to support the positive effects on providers, patients and the system as a result of enhanced inter-professional collaboration, particularly for chronic disease, mental health and special needs populations. There is well-documented evidence of increased access to primary care services, improved care experiences, more preventative services and increased patient satisfaction across Canada as a result of access to primary care teams (Barrett 2007).
There is growing evidence that inter-professional models improve care processes. They can provide a broader range of services, use resources more efficiently, create better access to services, shorten wait times, better coordinate care and improve comprehensiveness (Barrett 2007). Zwarenstein suggests that effective inter-professional collaboration allows one provider to report effectively to another about a patient’s condition, may increase the likelihood of detecting an error, and lead to more effective implementation of evidence-based decisions related to patient care (Zwarenstein 2006). Those with access to a team are more likely to receive health promotion and disease prevention, particularly those who have chronic conditions (Khan 2008). These patients have greater health knowledge and skills and undertake more self-care than those who do not receive inter-professional care (Barrett 2007).
There is good to moderate evidence that patients receiving inter-professional care have a more positive perception of their health services (Barrett 2007). By better addressing patient needs and improving coordination of care, collaborative teams can contribute to patient confidence in the healthcare system. However, if access to team-based care does not result in improved processes of care, there may be a negative effect on confidence (Khan 2008).
Collaborative models have been shown to contribute to better health outcomes, particularly in terms of blood pressure control, diabetes control, health status and quality of life (Barrett 2007). People with chronic conditions who receive team-based care are more likely to receive whole-person care, better coordination of care and a higher quality of care. Access to primary care teams has also been shown to reduce emergency room use and hospitalization through a reduction in unmet needs and uncoordinated care (Khan 2008). However, there is little evidence on how variation in the collaborative models can impact on outcomes (Barrett 2007).
Evidence from several of the Primary Healthcare Transition Fund studies in Ontario suggests that collaboration among providers can increase patient access to an expanded set of healthcare services, and effective internal and external referral systems can improve accessibility, continuity and quality. Although it is difficult to directly link collaboration with improved patient outcomes in isolation from other components of an intervention, several projects involving collaboration showed improved health outcomes. The studies also found improvement in process outcomes, such as patient and provider satisfaction (McMurchy 2007b). Examples include:
The East End Health Network in Timmins — which provided general primary healthcare, chronic disease management, geriatric care, chronic pain management, and mental health — improved patient access and resulted in statistically significant improvements in HbA1c, blood pressure, BMI and the Hamilton Rating Scale for Depression.
An occupational and physical therapist integrated into a family practice significantly reduced the number of planned hospital days among patients with chronic diseases and increased their satisfaction with care, compared to a patient control group.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 37
A physiotherapist and nurse integrated into a practice were able to reduce the number of seniors who fell, the number of falls, and either maintain or improve several physical functioning parameters (e.g., balance, gait speed).
Projects with pharmacists on site in primary care settings showed greater identification of medication-related problems and improved completeness of medication lists, documentation of allergies and adverse events, increased appropriateness of medication use, and, in some instances, better control of conditions like diabetes, hypertension and hyperlipidemia.
Three palliative care projects showed that when primary care providers collaborated with palliative experts, 24/7 access to care was expanded and client satisfaction increased.
A rehabilitation network of various providers and community organizations, improved access to and coordination of rehabilitation services.
Related to mental health, improved collaboration and communication between primary care and mental health providers led to improvements in access, service delivery, mental health outcomes and patient and provider satisfaction. In eastern Ontario and in Ottawa, on-site collaborative care increased access to mental health services and significantly improved mental health outcomes. In a Hamilton CHC, the number of clients identified with a mental illness, active mental health clients and primary care visits by clients with mental health issues increased. Integrating mental health services into an Aboriginal health centre and collaborating with Aboriginal providers and elders in northwestern Ontario expanded patients’ access to services and improved the quality, continuity and cultural appropriateness of services being provided.
A Cochrane review of on-site mental health workers in primary care found the “replacement model” and “consultation model” achieved short-term reductions in psychotropic prescribing, mental health referrals, and consultation rates. But there were few studies on the lasting effects on physician behaviour and no indirect effects in prescribing behaviour on the wider population were found (Bower 1999). Another Cochrane review of the effectiveness of counselling from a trained counsellor for psychological problems in primary care found significantly greater clinical effectiveness in the counselling group compared with usual physician care in the short term, but not long term. Patients were satisfied with counselling, and although there were reductions in the use of some health services, the counselling did not appear to reduce overall healthcare costs (Bower 2006).
There is some high and moderate quality evidence and a great deal of lower grade evidence showing individuals working in inter-professional primary care teams: 1) are more satisfied and have a more positive work experience compared to providers who work alone; 2) develop a positive perception of working collaboratively; 3) have improved knowledge and skills; and 4) change practice behaviours (e.g., referral patterns, follow up, preventative care) (Barrett 2007).
A Cochrane systematic review found no significant differences between physicians and nurses in terms of patient health outcomes, processes of care, resource use or cost when a nurse assumed responsibility for first contact and ongoing patient care. Patient health outcomes were similar to those of physicians, but patient satisfaction was higher with the care from nurses. “Nurses tended to provide longer consultations, give more information to patients and recall patients more frequently than did doctors” (Laurant 2004). Another systematic review assessing whether nurse practitioners provide care at first point of contact equivalent to family physicians found patients were more satisfied with nurse practitioners and no difference in health status, prescriptions, return consultations or referrals were found (Horrocks 2002). These findings were supported by another review (Chopra 2008).
A systematic review of 48 randomized controlled trials on the effects of community or lay health workers (those trained in the context of an intervention but having no formal professional, certificated or degreed tertiary education) in primary healthcare found promising benefits, compared with usual
38 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
care, in increasing the uptake of childhood immunizations, promoting breastfeeding, reducing childhood mortality and reducing morbidity from common childhood illnesses (Shaw 2005). Other reviews of task shifting have found positive impacts of community-based providers on prenatal, neonatal and maternal outcomes (Lewin 2008).
Costs
There is limited evidence related to the impact of inter-professional collaboration on costs. Existing evidence points to lower costs for team-managed primary care, lower readmission rates, and lower average costs for blood pressure control (Barrett 2007). Cost savings resulting from nurse substitution “depend on the magnitude of the salary differential between doctors and nurses, and may be offset by the lower productivity of nurses compared to doctors,” as well as more ordering of tests by nurses. The impact on physician workload and direct cost of care was variable (Laurant 2004).
CONCLUSIONREQUISITE ATTRIBUTESWhile all the attributes discussed in this paper are desirable, some emerge in the literature more consistently than others in terms of having a positive impact on improving the delivery and quality of primary healthcare services, overall health service utilization, and patient experience and outcomes. By and large, primary care practices that provide comprehensive.and.coordinated.quality.primary.healthcare confer the most benefit to their patients. Generally, such practices:
have a sound knowledge of their patients and community
use of clinical pathways and guidelines, and provide evidence-based care
provide collaborative team-based care (including.all members of the care team whether co-located or not)
use and share sophisticated electronic medical records (that include clinical decision support, prompts, reminders, registries, etc.)
have effective patient flow processes
Achieving the above attributes is generally facilitated by three main factors. The first is the requisite governance and organizational effectiveness. This includes having a clear mission and vision, sustained leadership and change management strategies. The second attribute that facilitates the provision of comprehensive and coordinated quality primary healthcare is accountability, whether to funders, managers, professional colleges, other healthcare providers, the patient or the public. Accountability can be supported by a culture of continuous quality improvement and ongoing performance measurement and monitoring. Finally, the role of the patient should not be underestimated. Given the tools (e.g., education, shared decision making, access to personal medical records, convenient access to care for at-risk, vulnerable patients) patients can make a significant contribution towards maintaining and improving their own health and well being.
While there is universal coverage and an attempt to achieve relatively equitable distribution of healthcare resources in this country, one cannot say that Canada has achieved a national primary care orientation in the sense of providing patient-centred, comprehensive and coordinated care. Nonetheless, the attributes discussed above are attainable in Canada. Primary care reform initiatives across Canada that promote team or network-based primary care delivery provide an opportunity to improve organizational effectiveness and coordination of care in primary care practices, and quality improvement initiatives – such as performance frameworks and scorecards, collaboratives and LEAN processes – are gaining traction in primary care.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 39
EVIDENCE REQUIRED TO SUPPORT ATTRIBUTESTo support existing primary care reform measures and to spur new ones, more actionable evidence (existing and new) and the supporting management and improvement tools need to reach healthcare providers, managers, patients and decision makers.
Volumes of research have been conducted by university-based researchers – health administration, faculties of medicine, pharmacy, nursing, rehabilitation, etc. – clinicians, primary care practices, (e.g., Community Health Centres), professional organizations, federal, provincial and regional authorities, think tanks (e.g., CHSRF, Change Foundation), hospital-based research centres, health quality councils, and the voluntary sector that have not been fully exploited. There are opportunities to realize the potential of work to date through syntheses of the published and grey literature, and collaboration among the groups listed above.
To support the advancement of a comprehensive and coordinated quality primary care system, more applied research in the following areas would be beneficial: 1) effective organizational, funding and administrative models; 2) methods for determining the appropriate mix of health professionals; 3) models for improving the coordination of care within primary care and with the rest of the health system; 4) effective means by which to deliver ongoing, comprehensive, person-focused primary care, including chronic disease prevention and management, mental health and addictions services, rehabilitation, etc.; 5) ways in which to effectively improve care in under-serviced areas and to at-risk populations; 6) examples of information technology’s successful use in improving quality and reducing costs; and 7) methods by which to ensure quality and performance at the service and patient level. These efforts could include syntheses and improved dissemination of existing research, and innovative and actionable primary research.
REFERENCESBACKGROUNDHealth Canada 2000. Online at: http://www.hc-sc.gc.ca/hcs-sss/prim/phctf-fassp/index_e.html
Russell G, Geneau R, Johnston S, Liddy C, Hogg W, Hogan K. Mapping.the.Future.of.Primary.Health.Care.Research.in.Canada. 2007. Canadian Health Services Research Foundation.
Schoen C, Osborn R, Doty MM, Bishop M, Peugh J, Murukutla N. Toward higher-performance health systems: adults’ health care experiences in seven countries, 2007. Health.Aff.(Millwood) 2007;26:w717-34.
Schoen C, Osborn R, Huynh PT, Doty M, Peugh J, Zapert K. On the front lines of care: primary care doctors’ office systems, experiences, and views in seven countries..Health.Aff.(Millwood) 2006;25:w555-71.
Starfield B. Primary Care in Canada: Coming or going? Healthcare.Papers 2008;8(2):58-62
Starfield B. Shi L. Commentary: primary care and health outcomes: a health services research challenge. Health.Services.Research, 2007;42:2252-2256.

40 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
NATIONAL PRIMARY CARE ORIENTATIONHsu J, Huang J, Kinsman J, Fireman B, Miller R, Selby J, Ortiz E. Use of e-health services between 1999 and 2002: A growing digital divide. J Am Med Inform Assoc. 2005;12:164–171
Larizgoitia I, Starfield B. Reform of primary health care: the case of Spain. Health.Policy 1997;41:121-37.
Macinko J, Starfield B, Shi L. The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970-1998. Health.Serv.Res 2003;38:831-65.
Naccarella L, Southern D, Furler J et al. Primary care funding and organisational policy options and implications: a narrative review of evidence from five comparator countries. Med.J.Aust 2008;188:S73-6.
Perry H, Robison N, Chavez D, Taja O, Hilari C, Shanklin D, Wyon J. 1998. The census-based, impact-oriented approach: its effectiveness in promoting child health in Bolivia. Health.Policy.and.Planning 13:140–51.
Reyes H, Perez-Cuevas R, Salmeron J, Tome P, Guiscafre H, Gutierrez G. 1997. Infant mortality due to acute respiratory infections: the influence of primary care processes. Health.Policy.and.Planning 12:214–23.
Roland M. The future of Primary Care: lessons from the U.K. N.Engl.J.Med. Nov, 2008;359(20)2087& 2092
Starfield, B. Primary Care and Health. A Cross-National Comparison. Journal.of.the.American.Medical.Association.1991;266:2268–71.
Starfield B. Is primary care essential? The.Lancet 1994;344:1129-33
Starfield B. Primary Care: Balancing Health Needs, Services, and Technology. 1998. New York: Oxford University Press.
Starfield B, Shi L. Policy Relevant Determinants of Health: An International Perspective. Health.Policy 2002;60:201–18.
Starfield B. Shi L. 2002. Policy Relevant Determinants of Health: An International Perspective. Health.Policy 60:201–18.
Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank.Q.2005;83:457-502.
Starfield B. The future of Primary Care: refocusing the System. N.Engl.J.Med. Nov, 2008;359(20)2087&2091
Stevens, G.D., and L. Shi. 2003. Racial and Ethnic Disparities in the Primary Care Experiences of Children: A Review of the Literature. Medical.Care.Research.and.Review 60:3–30.
Villalbi JR, Guarga A, Pasarin MI, Gil M, Borrell C, Ferran M, Cirera E. 1999. An evaluation of the impact of primary care reform on health..Atenci´on.Primaria.24:468–74.
Waitzkin H, Wald K, Kee R, Danielson R, Robinson L. 1997. Primary Care in Cuba: Low- and High-Technology Developments Pertinent to Family Medicine. Journal.of.Family.Practice.45:250–58.
Weiner J.P. 2004. Prepaid Group Practice Staffing and U.S. Physician Supply: Lessons for Workforce Policy. Health.Affairs (suppl.) Web Exclusives:W4–59.
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 41
HIGH-PERFORMING HEALTHCARE ORGANIZATIONSAssociation of Ontario Health Centres. A.Performance.Framework.and.Associated.Indicators.for.Community.Health.Centres.in.Ontario:.Final.Report.to.the.Ministry.of.Health.and.Long-Term.Care prepared by Jan Barnsley. June 5, 2008
Baldrige National Quality Program, Health.Care.Criteria.for.Performance.Excellence, 2004 education materials.
Campbell SM, Roland MO, Middleton E, Reeves D. Improvements in the quality of clinical care in English general practice 1998-2003: longitudinal observational study. BMJ 2005;331: 1121-3.
Canadian Institute for Health Information..Enhancing.the.primary.health.care.data.collection.infrastructure.in.Canada:.Report.2,.Pan-Canadian.Primary.Health.Care.Indicator.Development.Project..(2006).
Cohen D, McDaniel Jr, et al. A practice change model for quality improvement in primary care practice. Journal.of.Health.Care.Management.2004;49(3):155–170.
Conference Board of Canada. Enhancing.Interdisciplinary.Collaboration.in.Primary.Health.Care:.The.Principles.and.Framework.for.Interdisciplinary.Collaboration.in.Primary.Health.Care. 2006. Ottawa.
Crabtree BF. Primary Care Practices Are Full of Surprises! Health.Care.Management.Review 2003;28(3):279–283/289–290.
Davidhizar R, Bechtel GA. Neglected aspects of the learning process. Hosp.Mater.Manage.Q. 2000;21(3):26–31.
Feacham R, Sekhri N, White K. “Getting More for their Dollar: A Comparison of the NHS with California’s Kaiser Permanente,”.BMJ, January, 2002, 324
Grumbach K, Bodenheimer T. Can Health Care Teams Improve Primary Care Practice?
Health Services Restructuring Commission. 1996. Online at: www.health.gov.on.ca/hsrc/vision.htm.
JAMA 2004;291:1246–1251.
Leatt P, Porter J. Where Are the Health Care Leaders? The Need for Investment in Leadership Development..HealthcarePapers.2003;4(1) :14–31.
Lipshitz R, Popper M. Organizational Learning in a Hospital. The.Journal.of.Applied.Behavioral.Science 2000;36(3):345–361
Lord J. Future of primary health care education: current problems and potential solutions. Postgrad.Med.J.2003;79:553–560.
McConnell CR. Larger, Smaller, and Flatter: The Evolution of the Modern Health Care Organization. Health.Care.Manager 2005;24(2):177–188.
Ontario Joint Policy and Planning Committee. Working Group. Incentives & Performance Improvement – A working paper of the Incentives, Remediation and Consequences April 2004
Saskatchewan Health. Team.Development.and.Implementation.in.Saskatchewan’s.Primary.Health.Care.Sector:.Final.Report.to.Primary.Health.Services Branch. April, 2004. Regina.
Senge P. The Fifth.Discipline:.The.Art.&.Practice.of.the.Learning.Organization. 1990. New York: Doubleday Currency.
Tait AR. Clinical governance in primary care: a literature review. J.Clin.Nurs.2004;13(6):723–730.
42 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Thomas P, McDonnell J, McCulloch J, While A, Bosanquet N, Ferlie E. Increasing Capacity for Innovation in Bureaucratic Primary Care Organizations: A Whole System Participatory Action Research Project. Ann.Fam.Med 2005;3:312–317.
U.K. Audit Commission, Achieving.the.NHS.Plan, London, 2003.
U.S. General Accounting Office, High-Performing.Organizations, highlights of a GAO forum (GAO-04-343SP), February 13, 2004.
QUALITY IMPROVEMENTAsch SM, Baker DW, Keesey JW et al. Does the collaborative model improve care for chronic heart failure? Medical.Care.2005;43(7): 667-675.
Baker GR. MacIntosh-Murray A. Porcellato C, Dionne L, Stelmacovich K. Born K. High.Performing.Health.Care.Systems:.Delivering.Quality.by.Design. 2008. Toronto: Longwoods Publishing.
Camp A, Chaufournier R, Hupke C, Langley G, Little K. Transforming diabetes health care part 2: Changing lives. Diabetes Spectrum. 2004;17(2):107-111.
Care.Settings. Prepared by the Institute for Health Care Improvement for the National Opinion
Health Canada. The.EMR.Toolkit:.Implementing.electronic.medical.records.in.primary.care.settings. 2006. Ottawa
Health Quality Council, Quality Insight. 2008. Saskatchewan. Online at: www.hqc.sk.ca/portal.jsp?2mNBKJRScGdPwhhXV6lZvTBIzBf0QfLQkUwK4QBZaJsWHawXTufIaFVvI5thiwzu
Institute for Healthcare Improvement 2008a. Online at: http://www.ihi.org/IHI/Topics/OfficePractices/Access/ImprovementStories/ImprovingAccessandEfficiencyinPrimaryCareatHealthServe.htm
Institute for Healthcare Improvement. Charting the Way to Greater Success Pursuing Perfection in Sweden 2008b. Online at: http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/ImprovementStories/ChartingtheWaytoGreaterSuccessPursuingPerfectioninSweden.htm
Institute for Healthcare Improvement. Pursuing Perfection A View from Across the Pond 2008c. Online at: http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/ImprovementStories/PursuingPerfectionAViewfromAcrossthePond.htm
Institute for Healthcare Improvement. Reinventing Diabetes Care Through A.L.L. 2008d. Online at: http://www.ihi.org/IHI/Topics/ChronicConditions/Diabetes/ImprovementStories/ReinventingDiabetesCareThroughALL.htm
Institute for Healthcare Improvement. Pursuing Perfection: Report from Health Partners on Prepared Practice Teams 2008e. Online at: http://www.ihi.org/IHI/Topics/ChronicConditions/AllConditions/ImprovementStories/PursuingPerfectionReportfromHealthPartnersonPreparedPracticeTeams.htm
Institute for Healthcare Improvement. Reinventing Diabetes Care Through A.L.L. 2008f. Online at: http://www.ihi.org/IHI/Topics/ChronicConditions/Diabetes/ImprovementStories/ReinventingDiabetesCareThroughALL.htm
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 43
Institute for Healthcare Improvement. Report from Tallahassee Memorial Hospital on Enhancing Continuity of Care 2008g. Online at: http://www.ihi.org/IHI/Topics/ChronicConditions/AllConditions/ImprovementStories/ReportfromTallahasseeMemorialHospitalonEnhancingContinuityofCare.htm
Institute for Healthcare Improvement. Cambridge Health Alliance on Improving Asthma Care 2008h. Online at: http://www.ihi.org/IHI/Topics/ChronicConditions/Asthma/ImprovementStories/CambridgeHealthAllianceonImprovingAsthmaCare.htm
Langley J, Beasley C. Health.Information.Technology.for.Improving.Quality.of.Care.in.Primary
Piatt GA, Orchard TJ, Emerson S et al. Translating the chronic care model into the community: results from a randomized controlled trial of a multifaceted diabetes care intervention..Diabetes.Care 2006;29(4): 811-817.
Research Center under contract No. 290-04-0016. AHRQ Publication No. 07-0079-EF.
Rockville, MD: Agency for Health Care Research and Quality. July 2007.
Rosenthal MB, Fernandopulle R, Song HR, Landon B. Paying for quality: providers’ incentives for quality improvement. Health.Aff.(Millwood) 2004;23:127-41.
Rosenthal MB, Frank RG, Li Z, Epstein AM. Early experience with pay-for-performance: from concept to practice. Jama 2005;294:1788-93.
Sperl-Hillen J, O’Connor PJ, Carlson RR, Lawson TB, Halstenson C, Crowson T, Wuorenma J. Improving diabetes care in a large system: An enhanced primary care approach. Joint Commission Journal on Quality Improvement. 2000;26(11):615-622.
Tregullis V, Primary Health Care, Medical Services Division, BC Ministry of Health. Citation in: Why.health.care.renewal.matters:.lessons.from.diabetes..Health Council of Canada. March 2007. Online at: http://healthcouncilcanada
Tsai AC, Morton SC, Mangione CM, and Keeler EB. A metaanalysis of interventions to improve care for chronic illnesses. American Journal of Managed Care 2005;11(8): 478-488.
Wagner EH, Grothaus LC, Sandhu N, Galvin MS, McGregor M, Artz K, Coleman EA. Chronic care clinics for diabetes in primary care: A system-wide randomized trial. Diabetes Care. 2001;24(4):695-700.
QUALITY INCENTIVESBaker R. Lakhani M. Fraser R. Cheater F. A.model.for.clinical.governance.in.primary.care.groups..BMJ 1999;318:779-783.
Beckman H. The.ROI.(Return.on.Investments).for.a.P4P.Diabetes.Program”.Do.the.benefits.persist? AcademyHealth Annual Research Meeting. June 8-10, 2008. Washington D.C.
Doran T, Fullwood C, Gravelle H et al. Pay-for-performance programs in family practices in the United Kingdom. N.Engl.J.Med 2006;355:375-84.
Doran T, Fullwood C, Kontopantelis E, Reeves D. Effect of financial incentives on inequalities in the delivery of primary clinical care in England: analysis of clinical activity indicators for the quality and outcomes framework. Lancet 2008a;372:728-36.
Doran T, Fullwood C, Reeves D, Gravelle H, Roland M. Exclusion of patients from pay-for-performance targets by English physicians. N.Engl.J.Med.2008b;359:274-84.

44 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Fung CH, Lim YW, Mattke S, Damberg C, Shekelle PG. Ann Intern Med. Systematic.Review:.The.Evidence.That.Publishing.Patient.Care.Performance.Data.Improves.Quality.of.Care. 2008 Jan 15;148(2):111-23.
Giuffrida A, Gosden T, Forland F, Kristiansen IS, Sergison M, Leese B, Pedersen L, Sutton M. Target payments in primary care: effects on professional practice and health care outcomes. Cochrane.Database.of.Systematic.Reviews.1999, Issue 4. Art. No.: CD000531. DOI: 10.1002/14651858.CD000531.
Glickman SW, Ou FS, DeLong ER, Roe MT, Lytle BL, Mulgund J, Rumsfeld JS, Gibler WB, Ohman EM, Schulman KA, Peterson ED. Pay.for.Performance,.Quality.of.Care,.and.Outcomes.in.Acute.Myocardial.Infarction. JAMA. 2007 Jun 6;297(21):2373-80.
Grossbart SR. What’s the return? Assessing the effect of “pay-for-performance” initiatives on the quality of care delivery. Med.Care.Res.Rev 2006;63:29S-48S.
Hutchison B. Pay for Performance in Primary Care: Proceed with Caution, Pitfalls Ahead. Healthcare.Policy. 2008;4(1):10-15
Kohn A, Punished.by.Rewards.(Boston, 1993)
Levitt C. Price D. Hilts L. Kasperski J..Quality.in.Family.Practice.–.Phase.2:.A.Demonstration.Pilot.Project.prepared for the Primary Health care Transition Fund. 2006.
Lindenauer PK, Remus D, Roman S, Rothberg MB, Benjamin EM, Ma A, Bratzler DW. Public.Reporting.and.Pay.for.Performance.in.Hospital.Quality.Improvement. N Engl J Med. 2007 Feb 1;356(5):486-96. Epub 2007 Jan 26.
McLean G, Sutton M, Guthrie B. Deprivation and quality of primary care services: evidence for persistence of the inverse care law from the UK Quality and Outcomes Framework. J.Epidemiol.Community.Health 2006;60:917-22.
Miller HD. Creating Payment Systems to Accelerate Value-driven Healthcare: Issues and Options of Policy Reform, The Commonwealth Fund, September 2007
Ontario Health Quality Council/Joint Policy and Planning Committee. Accountability.Agreements.in.Ontario’s.Health.System:.How.Can.They.Accelerate.Quality.Improvement.and.Enhance.Public.Reporting? July31, 2008. Ontario Health Quality Council.
Petersen LA, Woodard LD, Urech T, Daw C, Sookanan S. Does pay-for-performance improve the quality of health care? Ann.Intern.Med 2006;145:265–72.
Ryan A. The.Effects.of.the.Hospital.Quality.Incentive.Demonstration.on.Medicare.Patient.Mortality.and.Cost..AcademyHealth Annual Research Meeting. June 8-10, 2008. Washington D.C.
Sebaldt R, Kaczorowski J..Provider.and.Patient.Reminders.in.Ontario:.Multi-Strategy.Prevention.Tools.(P-PROMPT) prepared for the Primary Health Care Transition Fund. 2006.
Sorbero ME, Damberg C, Lovejoy S, Mehrotra A, Teleki S. Hospitals’.Experiences.with.Pay-for-Performance.and.Pay-for-Reporting. AcademyHealth Annual Research Meeting. June 8-10, 2008. Washington D.C.
Werner RM, Goldman LE, Dudley RA. Comparison of Change in Quality of Care Between Safety-Net and Non-Safety-Net Hospitals. JAMA. 2008 May 14;299(18):2180-7.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 45
PHYSICIAN SUPPLYAakvik A, Holmas TH. Access to primary health care and health outcomes: the relationships between GP characteristics and mortality rates. J.Health.Econ.2006;25:1139-53.
Baicker K, Chandra A. Medicare spending, the physician workforce, and beneficiaries’ quality of care. Health.Affairs 2004;Web Exclusive:184–197.
Campbell RJ, Ramirez AM, Perez K, Roetzheim RG. Cervical Cancer Rates and the Supply of Primary Care Physicians in Florida..Family.Medicine.2003;35:60–64.
Canadian Institute for Health Information, Supply, Distribution and Migration of Canadian Physicians, 2006, Revised November 2007, (Ottawa: CIHI, 2007).
Ferrante JM, Gonzalez EC, Pal N, Roetzheim RG. Effects of Physician Supply on Early Detection of Breast Cancer. Journal.of.the.American.Board.of.Family.Practice 2000;13:408–14.
Franks P, Fiscella K. Primary Care Physicians and Specialists as Personal Physicians. Health care Expenditures and Mortality Experience. Journal.of.Family.Practice.1998;47:105–9.
Gulliford MC, Jack RH, Adams G, Ukoumunne OC. Availability and Structure of Primary Medical Care Services and Population Health and Health care Indicators in England. BMC.Health.Services.Research.2004;4:12.
Gulliford MC. Availability of Primary Care Doctors and Population Health in England: Is There an Association?.Journal.of.Public.Health.Medicine 2002;24:252–4.
Jaakkimainen L, Upshur R, Klein-Geltink J, Leong A, Maaten S, Schultz S, Wang L. Primary.Care.in.Ontario. Institute for Clinical Evaluative Sciences. November 2006
Mansfield CJ, Wilson JL, Kobrinski EJ, Mitchell J. Premature Mortality in the United States: The Roles of Geographic Area, Socioeconomic Status, Household Type, and Availability of Medical Care. American.Journal.of.Public.Health 1999;89:893–8.
Mark DH, Gottlieb MS, Zellner BB, Chetty VK, Midtling JE. Medicare Costs in Urban Areas and the Supply of Primary Care Physicians..Journal.of.Family.Practice.1996;43:33–9.
Roetzheim RG, Pal N, Gonzalez EC, Ferrante JM, Van Durme DJ, Ayanian JZ, Krischer JP. The Effects of Physician Supply on the Early Detection of Colorectal Cancer. Journal.of.Family.Practice.1999;48:850–58.
Roetzheim RG, Pal N, Van Durme DJ, Wathington D, Ferrante JM, Gonzalez EC, Krischer JP. Increasing Supplies of Dermatologists and Family Physicians Are Associated with Earlier Stage of Melanoma Detection..Journal.of.the.American.Academy.of.Dermatology.2000;43:211–8.
Rosser WW. Approach to Diagnosis by Primary Care Clinicians and Specialists: Is There a Difference? Journal.of.Family.Practice.1996;42:139–44.
Schappert SM. National Ambulatory Medical Care Survey 1991. Vital.and.Health.Statistics 1994;13:1–110.
Shi L. Primary Care, Specialty Care, and Life Chances. International.Journal.of.Health.Services 1994;24:431–58.
Shi L. Experience of Primary Care by Racial and Ethnic Groups in the United States. Medical.Care 1999;37:1068–77.
46 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Shi L, Starfield B, Kennedy B, Kawachi I. Income inequality, primary care, and health indicators. J.Fam.Pract.1999;48:275-84.
Shi L, Starfield B. Primary Care, Income Inequality, and Self-Rated Health in the United States: A Mixed-Level Analysis..International.Journal.of.Health.Services.2000;30:541–55.
Shi L, Starfield B, Politzer R, Regan J. Primary care, self-rated health, and reductions in social disparities in health..Health.Serv.Res.2002;37:529-50.
Shi L, Macinko J, Starfield B, Wulu J, Regan J, Politzer R. The relationship between primary care, income inequality, and mortality in US States, 1980-1995. J.Am.Board.Fam.Pract 2003;16:412-22.
Shi L, Macinko J, Starfield B et al. Primary care, infant mortality, and low birth weight in the states of the USA. J.Epidemiol.Community.Health 2004;58:374-80.
Shi L, Macinko J, Starfield B, Politzer R, Wulu J, Xu J. Primary care, social inequalities and all-cause, heart disease and cancer mortality in US counties: a comparison between urban and non-urban areas. Public.Health 2005;119:699-710.
Shi L, Macinko J, Starfield B, Politzer R, Wulu J, Xu J. Primary Care, Social Inequalities, and All-Cause, Heart Disease, and Cancer Mortality in U.S. Counties, 1990. American.Journal.of.Public.Health 2005;95:674–80.
Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank.Q.2005;83:457-502.
Vogel RL, Ackermann RJ. Is Primary Care Physician Supply Correlated with Health Outcomes? International.Journal.of.Health.Services 1998;28:183–96.
Welch WP, Miller ME, Welch HG, Fisher ES, Wennberg JE. Geographic Variation in Expenditures for Physicians’ Services in the United States. New.England.Journal.of.Medicine 1993;328:621–7.
Whittle J, Lin CJ, Lave JR, Fine MJ, Delaney KM, Joyce DZ, Young WW, Kapoor WN. Relationship of Provider Characteristics to Outcomes, Process, and Costs of Care for Community-Acquired Pneumonia. Medical.Care 1998;36:977–87.
PAYMENT/DELIVERY MODELSCoyte PC. Review of physician payment and service delivery mechanisms. Ontario.Med.Rev 1995:1–14.
Hollander MJ, Deber RB, Jacobs P, Glouberman S. A.critical.review.of.models.of.resource.allocation.and.reimbursement. Health Network, Canadian Policy Research Networks Inc, 1997.
Robinson JC. Theory and practice in the design of physician payment incentives. Milbank.Q 2001;79(2):149–177.
Deber R. Rationales for primary health care reform: Why are we doing this? An economic perspective. In: Wilson R, Shortt SED, Dorland J, eds..Implementing.Primary.Care.Reform:.Barriers.and.Facilitators..Montreal and Kingston: McGill-Queen’s University Press, 2004:25–38.
Demers M. The predictability of individual primary care costs and its impact on managed care plans. Health.Policy.2004;68(3):345–352.
Gillet J, Hutchison B, Birch S. Capitation and primary care in Canada: Financial incentives and the evolution of health service organizations. Int.J.Health.Serv.2001;31(3):583–603.
Gosden T, Forland F, Kristiansen IS, Sutton M, Leese B, Giuffrida A, Sergison M, Pedersen L.

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 47
Capitation, salary, fee-for-service and mixed systems of payment: effects on the behaviour of primary care physicians. Cochrane.Database.of.Systematic.Reviews 2000, Issue 3. Art. No.: CD002215. DOI: 10.1002/14651858.CD002215.
Miller HD, Creating Payment Systems to Accelerate Value-driven Health care: Issues and Options of Policy Reform, The Commonwealth Fund, September 2007
Coulter A. Evaluating general practice fundholding in the United Kingdom. European.Journal.of.Public.Health.1995;5(4):233–239.
Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations. Arch.Fam.Med.1998;7(4):352-357.
Paramore LC, Elixhauser A. Assessment of quality of care for managed care and fee-for-service patients based on analysis of avoidable hospitalizations. Value.in.Health 1999;2(4):258–268.
Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: The chronic care model, Part 2. JAMA.2002;288(15):1909–1914.
Canadian Health Services Research Foundation. Myth:.Managed.care=.mangled.care. Mythbusters, December, 2005.
O’Malley AS, Forrest CB, Politzer RM, Wulu JT, Shi L. Health Center Trends, 1994–2001: What Do They Portend for the Federal Growth Initiative? Health.Affairs.2005; 24:465–72.
Regan J, Schempf AH, Yoon J, Politzer RM. The Role of Federally Funded Health Centers in Serving the Rural Population. Journal.of.Rural.Health.2003;19:117–24.
Politzer RM, Yoon J, Shi L, Hughes RG, Regan J, Gaston MH. Inequality in America: The Contribution of Health Centers in Reducing and Eliminating Disparities in Access to Care. Medical.Care.Research.and.Review.2001;58:234–48.
McMurchy D. Building.and.Maintaining.a.Primary.Healthcare.Practice:.A.Synthesis.of.the.PHCTF.Ontario.Grants prepared for the Ministry of Health and Long-term Care. August 2007.
ACCESSAgency for Healthcare Research and Quality. 2004.National.Healthcare.Disparities.Report. 2004. AHRQ Publication no. 05-0014. Rockville, Md.
Canadian Health Services Research Foundation. Health.Human.Resources.in.Canada’s.Healthcare.System. Ottawa: Commission on the Future of Healthcare in Canada, Issue/Survey Paper prepared for the Commission on the Future of Healthcare in Canada, July, 2002.
CIHI Waiting for Health Care in Canada: What We Know and What we Don’t Know March 7, 2006
Delnoij D, Van Merode G, Paulus A, Groenewegen P. Does general practitioner gatekeeping curb Health care expenditure? J.Health.Serv.Res.Policy 2000;5:22–26.
Franks P, Clancy CM, Nutting PA. Gatekeeping Revisited—Protecting Patients from Overtreatment. New.England.Journal.of.Medicine.1992;327:424–9.
Forrest CB, Starfield B. Entry into primary care and continuity: the effects of access. Am.J.Public.Health.1998;88:1330-6.
Forrest CB, Starfield B. The effect of first-contact care with primary care clinicians on ambulatory Health care expenditures. J.Fam.Pract 1996;43:40-8.

48 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Gervas J, Perez Fernandez M, Starfield BH. Primary care, financing and gatekeeping in western Europe. Fam.Pract.1994;11:307-17.
Goddard MK. Quality in and Equality of Access to Health Care Services in England. CHE Research Paper 40. August 2008. Centre for Health Economics, University of York, UK.
Health Council of Canada..10.Steps.to.a.common.framework.for.reporting.on.wait.times. November, 2005.
Hjortdahl P. Borchgrevink CF. Continuity of Care: Influence of General Practitioners’ Knowledge about Their Patients on Use of Resources in Consultations..British.Medical.Journal.1991;303:1181–4.
Hurley RE, Freund DA, Taylor DE. Emergency Room Use and Primary Care Case Management: Evidence from Four Medicaid Demonstration Programs. American.Journal.of.Public.Health 1989;79:843–6.
Hurst J, Siciliani L. Tackling.excessive.waiting.times.for.elective.surgery:.A.comparison.of.policies.in.twelve.OECD.countries. OECD Health Working Papers, Annexes 1, 2, 3, 2003.
Leggetter S. Chaturvedi N. Fuller JH. Edmonds ME. Ethnicity and Risk of Diabetes-Related Lower Extremity Amputation: A Population-Based, Case-Control Study of African Caribbeans and Europeans in the United Kingdom. Archives.of.Internal.Medicine.2002;162:73–8.
Lillie-Blanton M. Hoffman C. The Role of Health Insurance Coverage in Reducing Racial/Ethnic Disparities in Health Care..Health.Affairs.2005;24:398–408.
Lynch ME, Campbell F, Clark AJ et al. A systematic review of the effect of waiting for treatment for chronic pain. Pain 2008;136:97-116.
Martin DP, Diehr P, Price KF, Richardson WC. Effect of a Gatekeeper Plan on Health Services Use and Charges: A Randomized Trial. American.Journal.of.Public.Health 1989; 79:1628–32.
McIntosh T. The.taming.of.the.Queue.II:.Wait.time.measurement,.monitoring.and.management. Colloquium Report, March 31-April 1, 2005 Ottawa, Ontario, 2004.
Raddish M. Horn SD, Sharkey PD. Continuity of Care: Is It Cost Effective? American.Journal.of.Managed.Care.1999;5:727–34.
Roos NP, Carriere KC, Friesen D. Factors Influencing the Frequency of Visits by Hypertensive Patients to Primary Care Physicians in Winnipeg..Canadian.Medical.Association.Journal.1998;159:777–83.
Saint-Jacques N, Younis T, Dewar R, Rayson D. Wait times for breast cancer care. Br.J.Cancer.2007;96:162-8.
Starfield B. Primary Care: Concept, Evaluation and Policy. 1992. Oxford University Press, New York.
Starfield B. Shi L. The Medical Home, Access to Care, and Insurance: A Review of Evidence. Pediatrics 2004;113:1493–8.
van Doorslaer E. Koolman X. Jones AM. Explaining Income-Related Inequalities in Doctor Utilisation in Europe. Health Economics 2004;13:629–47.
Western Canada Waiting List Project, From Chaos to Order: Making Sense of Waiting Lists in Canada Final Report March 31, 2001
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 49
LONGITUDINALITYBrown AD, Goldacre MJ, Hicks N, et al. Hospitalization for ambulatory care-sensitive conditions: A method for comparative access and quality studies routinely collected statistics. Can.J.Public.Health.2001;92(2):155–159.
Forrest CB, Shadmi E, Nutting PA, Starfield B. Specialty referral completion among primary care patients: results from the ASPN Referral Study. Ann.Fam.Med 2007;5:361-7.
Gill JM, Mainous AG, Diamond JJ, Lenhard MJ. Impact of provider continuity on quality of care for persons with diabetes mellitus. Annals.of.Family.Medicine 2003;1(3):162–170.
Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations. Arch.Fam.Med.1998;7(4):352–357.
Glazier RH MR, Agha MM, Zagorski B, Hall R, Manuel DG, Sibley LM, Kopp A. The Impact of Not Having a Primary Care Physician among People with Chronic Conditions. ICES 2008
Gulbrandsen P, Hjortdahl P, Fugelli P. General Practitioners’ Knowledge of Their Patients’ Psychosocial Problems: Multipractice Questionnaire Survey. British.Medical.Journal 1997;314: 1014–8.
Parkerton PH, Smith DG, Straley HL. Primary care practice coordination versus physician continuity. Family.Medicine.2004;36(1):15–21.
Roos LL, Walld R, Uhanova J, Bond R. Physician visits, hospitalzations, and socioeconomic status: Ambulatory care sensitive conditions in a Canadian setting. Health.Serv.Res 2005;40(4):1167–1185.
Ryan S, Riley A, Kang M, Starfield B. The Effects of Regular Source of Care and Health Need on Medical Care Use among Rural Adolescents. Archives.of.Pediatric.and.Adolescent.Medicine.2001;155:184–90.
Starfield, B. Primary.Care:.Balancing.Health.Needs,.Services,.and.Technology. 1998. New York: Oxford University Press.
Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank.Q.2005;83:457-502.
COORDINATIONBoerma WGW. Coordination and integration in European primary care. In: Saltman RB, Rico A, Boerma W, eds. Primary.care.in.the.driver’s.seat?.1st ed. Berkshire, England: Open University Press, 2006:3–21.
Calnan M, Cant S, Williams S, Killoran A. Involvement of the primary Health care team in coronary heart disease prevention..British.Journal.of.General.Practice.1996;46:465–468.
Conference Board of Canada..Enhancing.Interdisciplinary.Collaboration.in.Primary.Health.Care:.The.Principles.and.Framework.for.Interdisciplinary.Collaboration.in.Primary.Health.Care. 2006. Ottawa.
Dolovich L, Levine MAH, Marshman J, Sellors J, Burns S. A.Randomized.Controlled.Trial.of.Pharmacotherapy.Specialist.Team.Consultation.Integrated.into.Primary.Care.Practice.Settings.versus.Specialty.Service.Provided.in.a.Hospital.Outpatient.Clinic..Ottawa: CHSRF, December, 2001.
Faulkner A, Mills N, Bainton D, et al. A systematic review of the effect of primary care based service innovations on quality and patterns of referral to specialist secondary care. British.Journal.of.General.Practice.2003;53(496):878–884.
50 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Feachem RG, Sekhri NK, White KL. Getting More for Their Dollar: A Comparison of the NHS with California’s Kaiser Permanente. British.Medical.Journal 2002;324:135–41.
Franks P, Clancy CM, Nutting PA. Gatekeeping Revisited—Protecting Patients from Overtreatment. New.England.Journal.of.Medicine.1992;327:424–9.
Freeman G, Hjortdahl P. What Future for Continuity of Care in General Practice? British.Medical.Journal 1997;314:1870–73.
Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations. ArchFam.Med 1998;7(4):352–357.
Haggerty JL, Reid RJ, Freeman GK, Starfield, Adair CE, McKendry R. Continuity of Care: A Multidisciplinary Review..BMJ 2003;327(7425):1219–1221.
Hasselback P, Saunders D, Dastmalchian A, et al. The.Taber.integrated.primary.care.project:.Turning.vision.into.reality. Canadian Health Services Research Foundation, August, 2002.
Hjortdahl P, Borchgrevink CF. Continuity of Care: Influence of General Practitioners’ Knowledge about Their Patients on Use of Resources in Consultations..British.Medical.Journal 1991;303:1181–4.
Mainous AG III, Gill JM. The Importance of Continuity of Care in the Likelihood of Future Hospitalization: Is Site of Care Equivalent to a Primary Clinician? American.Journal.of.Public.Health.1998 ;88:1539–41.
Menec VH, Sirski M, Attawar D. Does continuity of care matter in a universally insured population? Health.Serv.Res 2005;40(2):389–400.
Mitchell G, del Mar C, Francis D. Does primary medical practitioner involvement with a specialist team improve patient outcomes? British.Journal.of.General.Practice.2002;52(484):934–939.
Murchie P, Campbell NC, Ritchie LD, Simpson JA, Thain J. Secondary prevention clinics for coronary heart disease: Four year follow up of a randomised controlled trial in primary care..BMJ.2003;326:84–90.
Oakeshott P, Kerry S, Austina A, Cappuccio F. Is there a role for nurse-led blood pressure management in primary care? Fam.Pract 2003;20(4):469–473.
Poulton BC, West MA. Effective multidisciplinary teamwork in primary Health care..J.Adv.Nurs 1993;18:918–925.
Raddish M, Horn SD, Sharkey PD. Continuity of Care: Is It Cost Effective? American.Journal.of.Managed.Care 1999;5:727–34.
Renders CM, Valk GD, Griffin S, Wagner EH, Eijk JTHM, van Assendelft WJJ. Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. The.Cochrane.Database.of.Systematic.Reviews 2001;1(2).69
Roos NP, Carriere KC, Friesen D. Factors Influencing the Frequency of Visits by Hypertensive Patients to Primary Care Physicians in Winnipeg. Canadian.Medical.Association.Journal.1998;159:777–83.
Rosenblatt RA, Wright GE, Baldwin LM, Chan L, Clitherow P, Chen FM, Hart LG. The Effect of the Doctor-Patient Relationship on Emergency Department Use among the Elderly. American.Journal.of.Public.Health 2000;90:97–102.
Saltman RB, Rico A, Boerma W, eds. Primary.care.in.the.driver’s.seat? First ed. Berkshire, England: World Health Organization, 2006.
WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 51
Shum C, Humphreys A, Wheeler D, Cochrane M-A, Skoda S, Clement S. Nurse management of patients with minor illnesses in general practice: multicentre, randomized controlled trial. BMJ 2000;320:1038–1043.
Starfield B, Shi L. Policy Relevant Determinants of Health: An International Perspective. Health.Policy.2002;60:201–18.
Talbot-Smith A, Gnani S, Pollock AM, Gray DP. Questioning the Claims from Kaiser. British.Journal.of.General.Practice.2004;54:415–21.
Temmink D, Francke AL, Hutten JBF, van der Zee J, Huijer Abu-Saad H. Innovations in the nursing care of the chronically ill: A literature review from an international perspective..J.Adv.Nurs.2000;31(6):1449–1458.
Vlek JFM, Vierhout WPM, Knottnerus JA, et al. A randomised controlled trial of joint consultations with general practitioners and cardiologists in primary care. British.Journal.of.General.Practice.2003;53(487):108–112.
Wensing M, Wollersheim H, Grol R. Organizational interventions to implement improvements in patient care: A structured review of reviews. Implementation.Science.2006;1(2):1–9.
COORDINATION OF INFORMATIONCanada Health Infoway 2002. Romanow Report provides major boost to the development of Electronic Health Records. Online at: http://www.infoway-inforoute.ca/lang-en/about-infoway/news/news-releases/80-romanow-report-provides-major-boost-to-the-development-of-electronic-health-records accessed on November 26, 2009
Chaudhry B, Wang J, Wu S, et al. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care..Ann.Intern.Med 2006;144(10):12–22.
College of Family Physicians of Canada. Primary.Care.Toolkit.for.Family.Physicians. 2007. Online at: www://toolkit.cfpc.ca/en/information-technology/.
Gamble B. Future Practice, Using IT to Make Primary Care Reform Work for You. April 2006. Online at: www.cma.ca/multimedia/CMA/Content_Images/Inside_cma/Future_Practice/English/2006/April/using_IT.pdf.www.cma.ca/multimedia/CMA/Content_Images/Inside_cma/Future_Practice/English/ 2006/April/using_IT.pdf
Hunt D, Haynes B, Hanna S, Smith K. Effects of Computer-based Clinical Decision Support Systems on Physician Performance and Patient Outcomes. JAMA.1998;280:1339–1346.
Hutchison B. Cracks in the Foundation: The Precarious State of Canada’s Primary Care Infrastructure. Electronic.Health.Care 2007;5(4).
Lix LM, Yogendran M, Burchill C, et al. Defining.and.validating.chronic.diseases:.An.administrative.data.approach. Manitoba Centre for Health Policy, May, 2006.
Lorenzi NM, Riley RT. Managing Change: an Overview. J.Am.Med.Inform.Assoc 2000;7(2):116–124.
Mitchell E, Sullivan F. A descriptive feast but an evaluative famine: systematic review of published articles on primary care computing during 1980-97. BMJ 2001;322:279–282. Online at: www://bmj.bmjjournals.com/cgi/content/full/322/7281/279.
Protti D, Edworthy S, Johansen I. Adoption of Information Technology in Primary Care Physician Offices in Alberta and Denmark, Part 1: Historical, Technical and Cultural Forces. Electronic.Health.Care.2007;6(1):95–102.
52 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Robinson JR, Young TK, Roos LL, Gelskey DE. Estimating the burden of disease: Comparing administrative data and self-reports. Med.Care.1997;35(9):932–947.
The Standing Committee on Social Affairs, Science and Technology. The.Health.of.Canadians—The.Federal.Role—Interim.Report,.Volume.Six:.Recommendations.for.Reform, October 2002, Chapter 10, paragraph 10.2. Online at: www.parl.gc.ca/37/2/parlbus/commbus/senate/com-e/soci-e/rep-e/repoct02vol6part4-e.htm#CHAPTER%20TEN.
COMPREHENSIVENESSDonohoe MT. Comparing Generalist and Specialty Care: Discrepancies, Deficiencies, and Excesses. Archives.of.Internal.Medicine 1998;158:1596–1608.
Forrest CB, Starfield B. Entry into Primary Care and Continuity: The Effects of Access. American.Journal.of.Public.Health 1998;88:1330–36.
Forrest CB, Nutting PA, von Schrader S, Rohde C, Starfield B. Primary care physician specialty referral decision making: patient, physician, and Health care system determinants. Med.Decis.Making 2006;26:76-85.
Franks P, Fiscella K. Primary Care Physicians and Specialists as Personal Physicians. Health Care Expenditures and Mortality Experience..Journal.of.Family.Practice 1998;47:105–9.
Harrold LR, Field TS, Gurwitz JH. Knowledge, Patterns of Care, and Outcomes of Care for Generalists and Specialists. Journal.of.General.Internal.Medicine.1999;14:499–511.
Hashem A, Chi MT, Friedman CP. Medical Errors as a Result of Specialization..Journal.of.Biomedical.Informatics.2003;36:61–9.
Grumbach K, Selby JV, Schmittdiel JA, Quesenberry Jr. CP. Quality of Primary Care Practice in a Large HMO according to Physician Specialty. Health.Services.Research.1999;34:485–502.
Kaag ME, Wijkel D, de Jong D. Primary Health Care Replacing Hospital Care—The Effect on Quality of Care..International.Journal.for.Quality.in.Health.Care 1996 ;8:367–73.
Lewin S, Lavis JN, Oxman AD, et al. Supporting the delivery of cost-effective interventions in primary Health care systems in low-income and middle-income countries: an overview of systematic reviews. Lancet.2008;372:928-39.
Parnell SJ, Zalin AM, Clarke CW. Care of Diabetic Patients in Hospital Clinics and General Practice Clinics: A Study in Dudley. British.Journal.of.General.Practice 1993;43:65–9; erratum 1993;43 (369):163.
Sox HC. Decision-Making: A Comparison of Referral Practice and Primary Care. Journal.of.Family.Practice.1996;42:155–60.
The Senate Standing Committee on Social Affairs, Science and Technology. (2002). The Health of Canadians – The Federal Role. Final Report
Starfield B, Shi L, Grover A, Macinko J. The Role of Evidence in Physician Workforce Policy. Health.Affairs.2005b;W5:97–107
Starfield B, Shi L. Policy Relevant Determinants of Health: An International Perspective. Health.Policy.2002;60:201–18.
Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank.Q 2005;83:457-502.
Starfield B. Refocusing the System. N.Engl.J.Med. Nov, 2008;359(20)2087&2091

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 53
PREVENTIONCongressional Budget Office. Health.Care.and.the.Budget:.Issues.and.Challenges.for.Reform. Testimony before the Committee on the Budget United States Senate. June 21, 2007
Elkan R, Kendrick D, Dewey M, Hewitt M, Robinson J, Blair M. Effectiveness of home based support for older people: systematic review and meta-analysis. BMJ 2001;323:1–9.
Flocke SA, Stange KC, Zyzanski SJ. The Association of Attributes of Primary Care with the Delivery of Clinical Preventive Services. Medical.Care 1998;36:AS21–30.
Health Canada. Healthy Canadians – A Federal Report on Comparable Health Indicators 2006 Online at: www.statcan.ca/english/freepub/82-003-IE/2006010/articles/vaccination/tables/table1-en.htm
Hirdes JP, Naus PJ, Young JE. The use of preventive home visits among frail elderly persons: Evidence from three European countries. CJOA 1994;13:499–509.
Hirdes JP, Naus PJ, Young JE. The use of preventive home visits among frail elderly persons: Evidence from three European countries. CJOA.1994;13:499–509.
Jasper J, Williams AP, Deber R. Falls.prevention.for.seniors. CRNCC In Focus, November. Online at: www.cmcc.ca (Canadian Research Network for Care in the Community, 2005.
Ploeg J, Feightner J, Hutchison B, Siqouin C, Gauld M. Effectiveness.of.Preventive.Primary.Care.Outreach.Interventions.with.Older.Persons:.Meta-analysis.of.Randomized.Controlled.Trials. Hamilton: McMaster Centre for Health Economics and Policy Analysis Working Paper 03-05, 2003.
Saver B. Financing and Organization Findings Brief. Academy.for.Research.and.Health.Care.Policy 2002.;5:1–2.
van Haastregt JCM, Diederiks JPM, van Rossum E, de Witte LP, Crebolder HFJM. Effects of preventive home visits to elderly people living in the community: Systematic review. BMJ 2000;320:754–758.
Wagner EH, LaCroix AZ, Grothaus L, et al. Preventing disability and falls in older adults: A population-based randomized trial. Am.J.Pub.Health.1994;84:1800–1806.
CHRONIC DISEASE MANAGEMENTBodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: The chronic care model, Part 2. JAMA 2002;288(15):1909–1914.
Bodenheimer T. Interventions to improve chronic illness care: Evaluating their effectiveness. Disease.Management 2003;6(2):63–71.
Conference Board of Canada. A Report Card on Canada. October 28 2008 Online at: http://sso.conferenceboard.ca/HCP/Details/Health.aspx.
Congressional Budget Office Disease.Management.in.Medicare:.Data.Analysis.and.Benefit.Design.Issues. Testimony before the Special Committee on Aging, United States Senate. September 19, 2002.
Culler SD, Parchman ML, Przybylski M. Factors related to potentially preventable hospitalizations among the elderly. Med.Care 1998;36(6):804–817.
Dolovich L, Levine MAH, Marshman J, Sellors J, Burns S. A.Randomized.Controlled.Trial.of
Ferguson GT. Management of COPD: Early identification and active intervention are crucial. Postgraduate.Medicine.1998;103(4):129–134, 136–141.

54 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Fireman B, Bartlett J, Selby J. Can disease management reduce Health care costs by improving quality? Health.Affairs.2004;23(6):63–75.
Fitzner K, Fox K, Schmidt J, Roberts M, Rindress D, Hay J. Implementation and outcomes of commercial disease management programs in the United States: The disease management outcomes consolidation survey. Disease.Management 2005;8(4):253–264.
Greisinger AJ, Balkrishnan R, Shenolikar RA, Wehmanen OA, Muhammad S, Champion PK. Diabetes care management participation in a primary care setting and subsequent hospitalization risk. Disease.Management.2004;7(4):325–332.
Health Council of Canada. Primary.Care. A background paper to accompany health care renewal in Canada: Accelerating Change, January 2005.
Lacasse Y, Guyatt GH, Goldstein RS. The components of a respiratory rehabilitation program: A systematic overview. Chest 1997;111(4):1077–1088.
Lacasse Y, Wong E, Guyatt GH, King D, Cook DJ, Goldstein R. Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. Lancet.1996;348:1115–1119.
Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self management program can improve health status while reducing hospitalization: A randomized trial. Med.Care.1999;37(1):5–14.
McCowan C, Neville RG, Crombie IK, Clark RA, Warner FC. The facilitator effect: Results from a four-year follow-up of children with asthma. British.Journal.of.General.Practice.1997;47(416):286–288.
McDermott RA, Schmidt BA, Sinha A, Mills P. Improving diabetes care in the primary health care setting: A randomised cluster trial in remote Indigenous communities. Med.J Aust 2001;174(10):497–502.
Patel PH, Welsh C, Foggs MB. Improved asthma outcomes using a coordinated care approach in a large medical group. Disease.Management 2004;7(2):102–111.
Pharmacotherapy.Specialist.Team.Consultation.Integrated.into.Primary.Care.Practice.Settings.versus.Specialty.Service.Provided.in.a.Hospital.Outpatient.Clinic. Ottawa: CHSRF, December, 2001.
Renders CM, Valk GD, Griffin S, Wagner EH, van Eijk JThM, Assendelft WJJ. Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings. Cochrane.Database.of.Systematic.Reviews.2000, Issue 4. Art. No.: CD001481. DOI: 10.1002/14651858.CD001481.
Saxena S, George J, Barber J, Fitzpatrick J, Majeed A. Association of population and practice factors with potentially avoidable admission rates for chronic diseases in London: Cross sectional analysis. J.R.Soc.Med 2006;99:81–89.
Sidorov J, Shull R, Tomcavage J, Girolami S, Lawton N, Harris R. Does diabetes disease management save money and improve outcomes? A report of simultaneous short-term savings and quality improvement associated with a health maintenance organization sponsored disease management program among patients fulfilling health employer data and information set criteria. Diabetes.Care.2002;25(4):684–689.
Starfield B, Lemke KW, Bernhardt T, Foldes SS, Forrest CB, Weiner JP. Comorbidity: Implications for the importance of primary care in ‘case’ management. Annals.of.Family.Medicine.2003;1(1):8–14.
Temmink D, Francke AL, Hutten JBF, van der Zee J, Huijer Abu-Saad H. Innovations in he nursing care of the chronically ill: A literature review from an international perspective. J.Adv.Nurs.2000;31(6):1449–1458.
UK Department of Health,.Improving.Chronic.Disease.Management, March 2004. Online at: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4075214

WHAT ARE THE CRITICAL ATTRIBUTES AND BENEFITS OF A HIGH-QUALITY PRIMARY HEALTHCARE SYSTEM? 55
PATIENT CENTREDNESSCoulter A, Ellins J. Effectiveness of strategies for informing, educating, and involving patients. BMJ 2007;335:24-7.
Graham JD, Corso PS, Morris JM, Segui-Gomez M, Weinstein MC. Evaluating the cost effectiveness of clinical and public health measures. Annu.Rev.Public.Health 1998;19:125–152.
Kruger J, Helmick CG, Callahan LF, Haddix AC. Cost-effectiveness of the arthritis self-help course. Arch.Intern.Med.1998;158(11):1245–1249.
Lewin SA, Skea ZC, Entwistle V, Zwarenstein M, Dick J. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane.Database.of.Systematic.Reviews 2001, Issue 4. Art. No.: CD003267. DOI: 10.1002/14651858.CD003267.
O’Connor A. Patient.Perspective:.Patient-Centred.Care. October 2008, Saskatchewan.
Turnock AC,Walters EH,Walters JAE,Wood-Baker R. Action plans for chronic obstructive pulmonary disease. Cochrane.Database.of.Systematic.Reviews.2005, Issue 4. Art. No.: CD005074. DOI: 10.1002/14651858.CD005074.pub2.
Wetzels R, Harmsen M, Van Weel C, Grol R, Wensing M. Interventions for improving older patients’ involvement in primary care episodes. Cochrane.Database.of.Systematic.Reviews.2007, Issue 1. Art. No.: CD004273. DOI: 10.1002/14651858.CD004273.pub2.
TEAM-BASED CAREBarrett J, Curran V, Glynn L, Godwin M..CHSRF.Synthesis:.Interprofessional.Collaboration.and.Quality.Primary.Healthcare..December 2007. Canadian Health Services Research Foundation
Bower P, Rowland N. Effectiveness and cost effectiveness of counselling in primary care. Cochrane.Database.of.Systematic.Reviews.2006, Issue 3. Art. No.: CD001025. DOI: 10.1002/14651858.CD001025.pub2.
Bower P, Sibbald B. On-site mental health workers in primary care: effects on professional practice. Cochrane.Database.of.Systematic.Reviews 1999, Issue 4. Art. No.: CD000532. DOI: 10.1002/14651858.CD000532.
Chopra M, Munro S, Lavis JN, Vist G, Bennett S. Effects of policy options for human resources for health: an analysis of systematic reviews. Lancet 2008; 371:668–74.
Conference Board of Canada. Enhancing.Interdisciplinary.Collaboration.in.Primary.Health.Care:.The.Principles.and.Framework.for.Interdisciplinary.Collaboration.in.Primary.Health.Care. 2006, Ottawa.
Grumbach K., Bodenheimer T. Can Health Care Teams Improve Primary Care Practice?.JAMA.2004;291:1246-1251.
Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ.2002;324:819-23.
Laurant M, Reeves D, Hermens R, Braspenning J, Grol R, Sibbald B. Substitution of doctors by nurses in primary care. Cochrane.Database.of.Systematic.Reviews.2004, Issue 4. Art. No.: CD001271. DOI: 10.1002/14651858.CD001271.pub2.
McMurchy D. Hodgson C. Chronic.Disease.Prevention.and.Management.in.Primary.Health.Care:.A.Synthesis.of.the.PHCTF.Ontario.Grants prepared for the Ministry of Health and Long-term Care. August 2007.
Ministry of Health and Long-Term Care. Family.Health.Teams:.Advancing.Primary.Health.Care:.Guide.to.Collaborative.Team.Practice. July, 2005.

56 CANADIAN HEALTH SERVICES RESEARCH FOUNDATION
Shaw B, Cheater F, Baker R, et al. Tailored interventions to overcome identifi ed barriers to change: effects on professional practice and Health care outcomes. Cochrane.Databaseof.Systematic.Reviews 2005;3: CD005470.
Smith SM, Allwright S,O’Dowd T. Effectiveness of shared care across the interface between primary and specialty care in chronic disease management..Cochrane.Database.of.Systematic.Reviews 2007, Issue 3. Art.No.:CD004910.DOI: 10.1002/14651858.CD004910.pub2.
Zwarenstein M, Reeves S. Knowledge Translation and Interprofessional Collaboration: Where the Rubber of Evidence-Based Care Hits the Road of Teamwork. The.Journal.of.Continuing.Education.in.the.Health.Professions, 2006;26:46–54.