Wh d 2010 Background

of 28
-
Upload
mafizur-rahman-kaisar -
Category
Documents
-
view
216 -
download
0
Transcript of Wh d 2010 Background
-
7/27/2019 Wh d 2010 Background
1/28
Why urban health matters
-
7/27/2019 Wh d 2010 Background
2/28
World Healh Organizaion 2010. All righs reserved.
Te designaions employed and he presenaion o he maerial in his publicaion do no imply he expression o any opinion whasoever on he par o he World HealhOrganizaion concerning he legal saus o any counry, erriory, ciy or area or o is auhoriies, or concerning he delimiaions o i s roniers or boundaries.Te boundaries and names shown and he designaion used on maps do no imply he expression o any opinion whasoever on he par o he World Healh Organizaionconcerning he legal saus o any counry, erriory, ciy or area or o is auhoriies, or concerning he delimiaion o is roniers or boundaries. Doted lines on mapsrepresen approximae border lines or which here may no ye be ull agreemen. Te menion o specic companies or o cerain manuacurers producs does no implyha hey are endorsed or recommended by he World Healh Organizaion in preerence o ohers o a similar naure ha are no menioned. Errors and omissions exceped,he names o proprieary producs are disinguished by iniial capial leters.All reasonable precauions have been aken by he World Healh Organizaion o veriy he inormaion conained in his publicaion. However, he published maerial isbeing disribued wihou warrany o any kind, eiher expressed or implied. Te responsibiliy or he inerpreaion and use o he maerial lies wih he reader. In no evenshall he World Healh Organizaion be liable or damages arising rom is use.
Phoo credis: IRIN; ONA SIA (L. Duggleby); Roary Inernaional; UN; WHO (AFRO, SEARO, N. Alexander, M. Decker, V. Dihajohn, O. Hkmies, A. K ari)
WHO/WKC/WHD/2010.1
-
7/27/2019 Wh d 2010 Background
3/28
Why urban health matters
-
7/27/2019 Wh d 2010 Background
4/28
CONTENTS Why urban health matters
2010: A year-long ocus on urbanizaion and healh ......................................................................................................................................................................................................................................1
Direcor-Generals saemen ...................................................................................................................................................................................................................................................................................................................................................2
I. Inroducion ...........................................................................................................................................................................................................................................................................................................................................................................................................6
II. Wha are he issues? ......................................................................................................................................................................................................................................................................................................................................................................8
1. Urbanizaion impacs populaion healh ...................................................................................................................................................................................................................................................................8
2. Urban setings are a healh deerminan ......................................................................................................................................................................................................................................................................9
3. Tere are unair dierences in he healh o ciy dwellers.........................................................................................................................................................................................14
III. Wha can be done: calls o acion ...............................................................................................................................................................................................................................................................................................15
1. Promoe urban planning or healhy behaviours and saey ...........................................................................................................................................................................16
2. Improve urban living condiions .....................................................................................................................................................................................................................................................................................................16
3. Ensure paricipaory urban governance....................................................................................................................................................................................................................................................................17
4. Build inclusive ciies ha are accessible and age-fiendly .........................................................................................................................................................................................18
5. Make urban areas resilien o emergencies and disasers ..........................................................................................................................................................................................18
Annex: A role or all who can do wha? .................................................................................................................................................................................................................................................................................19
Reerences....................................................................................................................................................................................................................................................................................................................................................................................................................................
21
-
7/27/2019 Wh d 2010 Background
5/28
o ensure susained acion on he opic o urbanizaion and healh hroughou 2010, a series o evens areplanned o highligh he healh risks in urban setings and he acions and policy opions ha can be akeno improve healh in ciies.
1. World Health Day 2010
Te aim o World Healh Day 2010 is o draw atenion o urbanizaion and healh, recognizing ha inan increasingly urbanized world, healh issues presen new challenges ha go ar beyond he healh secorand require acion a he global, naional, communiy, and individual levels. World Healh Day 2010 isno seen as an even in and o isel, bu as he launch o he year-long ocus on he issue.
2. A joint WHO/UN-HABITAT Global Report on urban health inequities
Te repor, o be published laer in he year, will expose he exen o which he urban poor suerdisproporionaely om a wide range o diseases and healh problems. I will provide evidence-basedinormaion o help municipal and healh auhoriies reduce healh inequiies in heir ciies.
3. Global Forum, Kobe
Te Forum will bring ogeher mayors, municipal leaders and naional minisers across muliple secorsor a declaraion o acion o reduce healh inequiies in ciies. Te Forum will be held in Kobe, Japan,
1517 November 2010.
2010: A year-long focus on urbanization and health
-
7/27/2019 Wh d 2010 Background
6/28
For a growing proporion o he worlds populaion,prospecs or a beter uure are ied o livingcondiions in ciies.
Ciies concenrae people, opporuniies, and
services, including hose or healh and educaion.In a well-known rend, ciies house he mos andhe bes hospials and hey atrac he mos aleneddocors, nurses and oher healh care sa. Whenciies are planned, managed, and governed well, lieourishes and healh oucomes surpass hose seenin rural areas.
Bu ciies also concenrae risks and hazards orhealh. Tey magniy some long-sanding hreaso healh and inroduce ohers. When largenumbers o people are linked ogeher in space andconneced by shared services, he consequences oadverse evens like conaminaion o he ood or
waer supply, high levels o air or noise polluion,a chemical spill, a disease oubreak or a nauraldisaser are vasly amplied.
Given he curren scale o urbanizaion, i comes as
no surprise ha ciies hemselves conribue o woglobal rends o direc concern o healh: climaechange and he rise o chronic diseases. According
o he laes esimaes, ciies conribue direclyo more han 60% o greenhouse gas emissions.Tey accoun or 75% o energy consumpionand a similar proporion o all wases. A he same
ime, ciy dwellers are especially vulnerable o heconsequences o climae change, wheher expressedas hea waves, waer scarciy, increasing levels o airpolluion, or rising sea levels in coasal areas.
Ciies also end o promoe unhealhy liesyles, likeconvenien dies ha depend on processed oods,sedenary behaviour, smoking, and he harmuluse o alcohol and oher subsances. Tese liesylechoices are direcly linked o obesiy and he rise o
condiions like hear disease, sroke, some cancers,and diabees. And hese condiions are increasinglyconcenraed in he urban poor.
Perhaps mos alarming, he growh o urban cenresin he 21s cenury is being accompanied by asecond, disincly ominous rend. Povery, whichin previous cenuries was greaes in scatered ruralareas, is now heavily concenraed in ciies. In manycounries, urbanizaion has oupaced he abiliy o
governmens o build essenial inrasrucures andenac and enorce he legislaion ha make lie inciies sae, rewarding, and healhy.
Director-generals statement
Urban healh maters,in criical ways, or moreand more people.
For he frs ime inhisory, more people
are now living in urbansetings han in ruralareas. By he year 2030,an esimaed six ou oevery en people will beliving in owns or ciies,wih he mos explosive
growh expeced in Asiaand Aica.
-
7/27/2019 Wh d 2010 Background
7/28
oday, around one hird o urban dwellers,
amouning o nearly one billion people, live in urbanslums, inormal setings, or sidewalk ens. Whilehe vas majoriy o urban slums more han 90% are locaed in he developing world, nearly everyciy everywhere has pockes o exreme deprivaionogeher wih exreme wealh. Tey have people
who over-consume healh care and people whoorego he mos basic and essenial care or nancialand oher reasons. In every corner o he world,
cerain ciy dwellers suer disproporionaely rompoor healh, and hese inequiies can be raced backo dierences in heir social and living condiions.
On his World Healh Day, he World Healh
Organizaion (WHO) is calling on a wide range ogroups rom municipal auhoriies and he privae
secor, o concerned ciizens, nongovernmenal
organizaions, and advocaes or healhy living o
ake a close look a healh inequiies in ciies and
ake acion.
Why should inequiies in urban healh and living
sandards mater? Mos obviously, he consequences
o povery and ill healh, including menal healh,are conagious in a ciy seting. Tey are derimenal
o all ciy dwellers. Urban povery and squalor are
-
7/27/2019 Wh d 2010 Background
8/28
srongly linked o social unres, menal disorders,crime, violence, and oubreaks o disease associaed
wih crowding and lh. Tese hreas can easilyspread beyond a single neighbourhood or disric o
endanger all ciizens and ain a ciys repuaion.Municipal auhoriies know wha his means inerms o atracing ouriss and new businessesand winning he nex elecion. Ciy dwellers know
wha his means in erms o social cohesion, saey,securiy, and he qualiy o lie.
In addiion, healh inequiies are an excellen socialaccounan. Tey are a reliable way o measure how
well a ciy is meeing he needs o is residens. Poorhealh, including menal healh, is one o he mos
visible and measurable expressions o urban harm.Healh inequiies can also be a rallying poin orpublic demands or change ha compel poliicalleaders o ake acion.
Urban healh maters and urban healh governancematers mos especially. For example, in developingcounries, he bes urban governance can help
produce 75 years or more o lie expecancy. Wihpoor urban governance, lie expecancy can be aslow as 35 years.
Good urban healh governance helps ensure haopporuniies and advanages are more evenlydisribued, and ha access o healh care is air andaordable. Abundan evidence has idenied he
roo causes o urban healh inequiies and shownhow hey can be ackled.
While mos o hese roo causes lie beyond hedirec conrol o he healh secor, local leadershave direc inuence over a wide range o urbanhealh deerminans, rom housing and ransporpolicies, o social services, o smoking regulaionsand he policies ha govern ood markeing andsales. Local leaders are well-posiioned o inuence
land use, building sandards, waer and saniaionsysems, and he enacmen and enorcemen ohealh-promoing legislaion. Moreover, acingin he name o healh can rally sakeholders romdiverse backgrounds and ineress and build poliicalpressure on issues ha are imporan o every ciydweller. Healh is valued universally as an essenialprerequisie or a ullling and producive lie.
Making ciies good or healh akes ime, bu asabundan examples rom all around he world show,i can be done.
Director-generals statement
-
7/27/2019 Wh d 2010 Background
9/28
Urban healh maters, in criical ways, or more andmore people. And WHO will be doing more, odayand well ino he uure, o suppor hese eors.
1. Promoe urban planning or healhybehaviours and saey
2. Improve urban living condiions
3. Ensure paricipaory urban governance
4. Build inclusive ciies ha are accessibleand age-iendly
5. Make urban areas resilien o emergenciesand disasers
Laer in he year, WHO and UN-HABIA willbe launching a repor on urban healh inequiiesand how o address hem. iled Hidden ciies, herepor is aimed a unmasking and overcoming healh
inequiies in urban setings, and includes abundanpracical examples and policy advice on specic,evidence-based inervenions.
In November 2010, a global orum on urbanizaionand healh, o be held in Kobe, Japan, will bringogeher municipal auhoriies and decision-makersacross muliple secors wih he aim o promoing
inersecoral acion o reduce urban healhinequiies.
In a dedicaed programme, WHO and is sixregional o ces will work wih specic ciies andnaional auhoriies o assess urban healh inequiiesand ideniy appropriae acions o reduce hem.
o mainain momenum, urban healh advocaes arebeing idenied and successul ciy experiences will
be shared as menus o policy opions and models ogood pracice.
WHO will help municipal auhoriies in assessinghe healh impac o planning opions in ohersecors, such as urban ransporaion and he saeyo roads or boh vehicles and pedesrians.
Dr Margare ChanDirecor-General o he World Healh Organizaion
-
7/27/2019 Wh d 2010 Background
10/28
Te year 2007 saw, or he rs ime, hemajoriy o human beings living in urban areas.Tis rend will coninue wih 6 in 10 peopleliving in owns and ciies by 2030. In recenimes, he growh o urban areas in low-incomecounries has been our imes aser han hegrowh in high-income counries. Tis rend,oo, is expeced o coninue in coming years.
Urban areas provide grea opporuniies orindividuals and amilies o prosper and canprovide a healhy living environmen hroughenhanced access o services, culure andrecreaion. However, ciy dwellers coninue oace healh hazards and new healh challengeshave emerged.
While he characerisics o each ciy vary
by local conex, common urban healh andsocial challenges include: overcrowding; airpolluion; rising levels o risk acors like
I. Introduction
Where people live aecs heir healh and opporuniies or leadinglives o heir ull poenial.
obacco use, unhealhy die, physical inaciviyand he harmul use o alcohol; road racinjuries; inadequae inrasrucure, ransporaciliies and solid wase managemen sysems,and insucien access o healh aciliies inslum areas.
World Healh Day in 2010 oers anopporuniy o ake a closer look a hecondiions ha deermine healh oucomesor he majoriy o he worlds populaion,he issues ha need o be addressed, and heacions ha can be aken. By undersandinghese issues, limied resources can be allocaedo more argeed inervenions, and achievebeter healh oucomes.
Te ocus on urbanizaion and healh as aheme or World Healh Day 2010 is imely andhighly relevan or he ollowing reasons.
-
7/27/2019 Wh d 2010 Background
11/28
F,wih he majoriy o he worldspopulaion now living in urban areas andhis proporion expeced o grow, urbanhealh should become a major ocus o global
public healh policy. Whils urbanizaionand he growh o ciies may be associaedwih increasing prosperiy and good healha an aggregae level, urban populaionsdemonsrae he worlds mos obvious healhdispariies in boh low- and high-incomecounries. Rapid migraion rom rural areas aswell as naural populaion growh are putingurher pressure on limied resources in ciies,
especially in low-income counries.
S, much o he naural and migraiongrowh in urban populaion is among hepoor. More han one billion people onehird o he urban populaion live inovercrowded and lie-hreaening condiionsin urban slums and inormal setlemens. I
ciies ail o deliver on he perceived promiseo economic opporuniies or he poor, largeconcenraions o unemployed young people
may hreaen social sabiliy, securiy andhe healh o communiies as a consequence.In low-income counries, in paricular,dispariies will increase, as he combinaion
o in-migraion, naural growh and scarciyo resources resuls in ciies being unable oprovide he services needed by hose whocome o live in hem.
T, here is evidence ha rapid,unplanned urbanizaion can have negaiveconsequences or he healh and saey opeople.
-
7/27/2019 Wh d 2010 Background
12/28
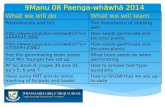
Virtually all population growth over thenext 30 years will be in urban areas (1).
By 2030, 6 out of every 10 people will becity dwellers, rising to seven out of 10 peopleby 2050 (2).
Key poins o consider on urban growhand is impac on healh
Mos o he worlds populaion growhis expeced in urban areas in low- andmiddle-income counries (Figure 1).
Urbanizaion rends vary across dierenpars o he world. Some ciies and regionsare experiencing rapid growh, whereas oherciies and regions are in populaion decline.However, he worlds urban populaion in he
less developed regions is projeced o increaserom 1.9 billion people living in ciies in 2000o 3.9 billion in 2030 (3).
Growh will be primarily in small andmid-sized ciies
Urbanizaion and is healh impacs are nojus an issue or megaciies ciies wih over10 million residens. In ac, much o heurban populaion growh will occur in small andmid-sized ciies. While large ciies o developingcounries will accoun or 20% o he increase inhe worlds populaion beween 2000 and 2015,small and mid-size ciies (less han 5 million)will accoun or 45% o his increase (4).
Urbanizaion involves migraion,reclassicaion and naural growh
In addiion o migraion, ciies add populaionhrough reclassicaion, when hey expandhorizonally and absorb hamles and owns.Migraion and reclassicaion accoun or
40% o urban growh, wih he remaining60% coming rom naural growh o exisingpopulaions (5).
II. What are the issues?
1. Urbanizaion impacs populaion healh
FIGURE 1
Distribution of world
population Growth, 1950-2030
Source: Cohen B. Urban Growth
in Developing Countries. WorldDevelopment. Vol. 32, No. 1, pp. 2351, 2004.
Data source: UNDESA. World urbanization
prospects: the 2001 revision.
Mean years of education
Urban high-income countries
19501975
2500
2000
1500
1000
500
0Populationi
ncrease,in
thousands
19752000
time frames
20002030
Urban Middle-and-low income countries
Rural High and Middle-and-low income
-
7/27/2019 Wh d 2010 Background
13/28
Ciies are growing horizonally
Te rend or he pas 50 years is or ciies o
grow horizonally in he orm o urban sprawl,wheher as suburbs in he developed world orperi-urban expansion in he developing world.
Tis has implicaions or he e ciency ourban services, including delivery o waer andsaniaion, provision o public ranspor, as wellas or access o jobs, educaion, ood and healhservices.
Speed o growh can oupaceinfasrucure requiremens
In many cases, especially in he developingworld, he speed o urbanizaion has oupacedhe abiliy o governmens o build essenialinrasrucure. Failure o plan or coninued
growh resuls in inadequae healh services,waer, saniaion, educaion, and essenialinrasrucure.
Many cities are currently burdened and willbe confronted by a triple threat:
o Inecious diseases exacerbaed by poorliving condiions;
o Noncommunicable diseases such ashear disease, cancers and diabees and condiions uelled by obacco use,unhealhy dies, physical inaciviy, andharmul use o alcohol; and
o Accidens, injuries, road accidens, violence
and crime.Tese are he resul a complex ineraciono various deerminans o healh, includinginsu cien inrasrucure and services haparicularly impac he healh o he poor andslum dwellers. Living and working condiionsvary widely wihin and beween ciies acrosshe world and are he causes o he causeso ill-healh.
2. Urban setings are a healh deerminan
-
7/27/2019 Wh d 2010 Background
14/28
Housing, land tenureand security
Most, but not all, urban poor live in slums andsquaer selements. ese seings tend to be
unregulated, precarious, overcrowded, and areoen exposed to hazards, such as steep hillsidessubject to landslides, riverbanks and waterbasin locations subject to ooding, or sites nearindustrial hazards. Inadequate, overcrowded ordeteriorating housing in informal selements,especially where tenure is insecure, increasesthe health risks from environmental hazards,violence and crime, and is associated with
injuries, respiratory problems, infectiousdiseases, and mental health problems (6).
Water
Approximately 5.9 billion people 87% of theworlds population are now using safe drinking-water sources, according to the new WHO/
UNICEF Joint Monitoring Programme report onsanitation and drinking-water (7). Although 94%of urban residents in developing countries use
improved drinking-water sources (that is, theavailability of at least 20 litres per person per dayfrom a source within 1 km of the users dwelling),grave risks of water contamination still exist dueto the unreliability of supplies and related waterstorage practices (8).
Sanitation
Although the vast majority without access towater and sanitation live in rural areas (7),some 807 million city dwellers (24% globallyand 32% in developing cities) lack access to
what WHO denes as improved sanitation household latrines or ush toilets that areconnected to sewer, septic, compost or coveredpit hygienically separating excreta from humancontact. Of these, more than 170 million urbanresidents do not have access to even the simplestlatrine and are forced to defecate in the open.About 500 million urban dwellers worldwideshare sanitation facilities with other households
(8). Globally, an estimated 3% of all deaths arethe result of diarrhoeal diseases caused by unsafedrinking-water, sanitation and hygiene (9).
II. What are the issues?
2. Urban setings are a healh deerminan(coninued)
-
7/27/2019 Wh d 2010 Background
15/28
Food
Another health determinant in cities is access tosafe and quality food, and in su cient quantity(10). Inadequate diet reduces resistance to
disease, especially for slum dwellers, becausethey live in the constant presence of pathogenicmicro-organisms (11). Urban poor populationsin the developed and developing world oen relyon street food, fast food, processed and cheapfood, leading to nutritional problems such asvitamin/mineral deciencies, dental problemsand obesity, which in turn is associated withdiabetes and cardiovascular problems.
Urban transport
Public transport, walking and cycling assuredthrough good land use and transit planning are the major travel modes in some large citiesof Europe, Asia and the Americas. But in manydeveloped and fast-developing cities, trends are
moving in the opposite direction. As peoplebecome more a uent, the lack of publictransport infrastructure and services or good
networks for cycling and walking along witharaction to a more a uent lifestyle has spurreda rapid transition to cars or motorcycles leading
to enormous increases in tra c, along withtra c-related pollution, injur y risks topedestrians and cyclists, and a reduction inphysical activity.
Physical inactivity is a major risk factor forcardiovascular disease, diabetes and certaincancers. While everyone in a city may beaected by a lack of transport options, poorneighbourhoods oen lose out the most, asthey lack good public transport access to healthcentres, grocery stores, schools, and jobs(9, 12, 13).
Road tra c injuries also stand out as animportant and growing transport-related publichealth problem, with most deaths occurring inlow- and middle-income countries. Globally,road tra c injuries constitute the ninth leading
cause of death and ill-health, and will rise to thethird position by 2030 unless immediate andsustained action is taken (14).
Noise exposure
Noise, a common urbanproblem, is a consequenceof transportation and
construction. Intense andcontinuous exposure maybe associated with hearingimpairment, high bloodpressure and cardiovasculardisease (15).
-
7/27/2019 Wh d 2010 Background
16/28
Outdoor and indoorair pollution
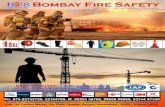
In 2004, outdoor urban air pollution killed some1.2 million people worldwide(9). WHO estimates
that 1.5 billion urban dwellers face levels ofoutdoor air pollution that are above the maximumrecommended limits (16).
Of urban air pollutants, ne particulate maer,mostly from vehicle and industrial fuel combustion,has the greatest eect on human health. Worldwide,ne particulate maer is estimated to cause about8% of lung cancer deaths, 5% of cardiopulmonarydeaths and about 3% of respiratory infection deaths
(9).
About 25% of city dwellers in developingcountries and 70% of city dwellers in leastdeveloped countries use solid fuels for householdheating and cooking. In 2004, exposure to indoorpollution was estimated to cause about 2 milliondeaths worldwide, mostly from pneumonia,chronic lung disease and cancer. As poor
households tend to be more dependent on solidfuel for heating and cooking, they are thus mostexposed to indoor pollution (17).
UAP deaths/1 million population
050
50150
150250
250400
> 400
Data not available Source: WHO Global health risks, 2009
II. What are the issues?
FIGURE 2
Deaths attributable to urban air pollution, 2004
2. Urban setings are a healh deerminan(coninued)
-
7/27/2019 Wh d 2010 Background
17/28
Climate change
Climate change has major environmental healthimpacts in the cities of the developing world,which can be generally more vulnerable to the
impacts of climate change. Key vulnerabilityfactors include coastal location and exposureto the urban heat-island eect, whereby urbantemperatures may be as much as 511 C higherthan in surrounding rural areas due to the greaterheat absorption of dense urban built spacesand lowered capacity for evaporative cooling(18). Urban areas concentrate both emiers ofgreenhouse gases and people at risk from climate
change. e potential health impacts of climatechange range from direct (e.g. ill-health fromheat exposure) to highly indirect (e.g. spreadof infectious diseases to new locations throughecological changes) (19).
Social environment
A citys social environment can support ordamage health (20). Positive urban featuresinclude higher levels of social support.
Problematic characteristics of the urban socialenvironment may include social pressure for health-damaging behaviour like drug abuse and violenceand high levels of social stressors such as socialisolation and extreme poverty(21). Interpersonal
violence is fast becoming a major security and publichealth issue (22). Violence tends to be greater infaster-growing and larger cities. In urban areas,young people aged 15 to 24 commit the largestnumber of violent acts and are also the principalvictims of violence. e lives and health of citydwellers are at risk during wars and conicts.
Health and social services
Cities are frequently characterized as having a richarray of health and social services in comparisonto rural areas. Yet for low- and middle-incomecountries in particular, the story is more complex.Access to services for the urban poor may belimited by ability to pay, even in the context freehealth services where medications and suppliesare not free, location or hours of operation is
inconvenient, and care is of poor quality. eresult is low utilization of even the most basicpreventative and curative health services.
-
7/27/2019 Wh d 2010 Background
18/28
Figure 3 shows a map o communiy disricsin New York Ciy by measures o concenraeddisadvanage including or educaion.
Figure 4 shows he same map or HIV/AIDS.In boh gures, he darkes areas are he mosdisadvanaged and have he highes rae o poorhealh oucomes. Tese dierences in healhoucomes wihin urban areas disaggregaed byabsolue or relaive povery are seen aroundhe world. Tis highlighs he need or deailedinra-urban daa in ciies o show where
inervenions can have he mos eec.
Healh inequiies are he resul o acombinaion o poor social policiesand programmes, and unaireconomic and social arrangemens.
Puting righ hese inequiies, aboveall, is a mater o social jusice.
3. Tere are unair differences in he healh o ciy dwellers
Healh inequiies are a concern in all ciies.For example, in Glasgow, Scoland, malelie expecancy in Calon ward is 54 yearsin conras o 82 years in Lenzie, EasDunbaronshire, a nearby ward in he same ciy(23). A child who lives in a slum in Kenya isar more likely o die beore he age o 5 hanhis or her compario living in anoher moreaffl uen par o he ciy, or even in rural Kenya.In he Embakasi slum in Nairobi, he under-5moraliy rae per 1000 children is 254 whilehe average or Nairobi is 62 (24).
Inra-urban dierences are seen or more hanlie expecancy and under-ve moraliy.
FIGURE 3
average educational attainment
FIGURE 4
Age-adjusted HIV/AIDS rate
Source: Vlahov, D et al. Knowledge Network
on Urban Settings Thematic Paper 1.
WHO Centre for Health Development 2008.
(Available at http://www.who.or.jp/CHP/
thematic_papers/KNUS_ThematicPaper01.pdf)
10 20 30 4050 Miles
HIV/AIDS rate
011
1223
2437
3864
65126
Miles
Mean years of education
10.0610.90
10.9011.93
11.9312.85
12.8514.43
14.4316.10
0 10 20 30 405
Intra-urban dierences in New York City, 2000
II. What are the issues?
-
7/27/2019 Wh d 2010 Background
19/28
On World Health Day 2010, WHO
recommends the following ve calls to
action to build a healthy and safe urban
environment:
Promote urban planning forhealthy behaviours and safety
Improve urban living conditions
Ensure participatory urban
governance
Build inclusive cities that areaccessible and age-friendly
Make urban areas resilient toemergencies and disasters
III. What can be done:calls to action
We are a a clear urningpoin a which we aremoving owards an
increasingly urbanizedworld. We need oappreciae he posiive andnegaive impac on healhdue o urbanizaion andake appropriae acionso address hem. Tere is
a pressing need or acionnow o ensure ha growingciies are healhy ciies. ese ve calls to action do
not necessarily requireadditional funding, butpolitical commitment is vitalto redirect resources topriority interventions, therebyachieving greater e ciency.
1!
2!
3!
4!
5!
-
7/27/2019 Wh d 2010 Background
20/28
III. What can be done: calls to action
Promote urban planning forhealthy behaviours and safety
Urban planning can promoe healhybehaviours and saey in many dieren ways,
applicable boh o exising and new areas.Tese would include design or physicalaciviy in ciies, where healhy ood isavailable, sae, accessible and aordable,where healh services or all are providedand where roads are sae.
Concrete and feasible actions that can be
taken include: Design ciies o promoe physical aciviy
Make healhy ood available, sae, andaordable
Provide adequae healh services or all
Improve road saey
Improve urban livingconditions
Improvemens in housing and housingcondiions, conrol o polluion and
improvemen in waer and saniaion go a longway o miigaing healh risks. Land securiyand enure is a oundaion on which healh canbe buil. Squater setlemens are ofen illegalbu generally represen he only opion openo poor people, migran or local, in searcho sheler. Inormal setlemens are rarelyprovided wih basic social services.
Concrete and feasible actions that can betaken include:
Locae houses in sae places
Improve housing condiions
Conrol indoor and oudoor polluion
Ensure sae waer and improved saniaion
1! 2!
-
7/27/2019 Wh d 2010 Background
21/28
Ensure participatory urbangovernance
Local paricipaory governance mechanismsshould be esablished ha enable communiies
and local governmens o parner inbuilding healhier and saer ciies. Goodurban governance means paying ateniono concerns and planning horizons haexend beyond curren needs (25). In manydeveloping naions, presen urban problemsare only he beginning. Ciies need a longererm sraegy in order o urn urbanizaionspoenial ino realiy.
Acion and success ul implemenaion requireour precondiions or change: poliicalcommimen a he highes level where healh,equiy and susainable developmen are corevalues in a ciys policies and vision; sharedvision, undersanding and commimen oa comprehensive and sysemaic approach
or urban healh; organizaional srucuresand processes o coordinae, manage and
suppor change and o aciliae inersecoralacion and acive ciizen involvemen; andopporuniies or parnership-building andneworking wih sauory and non-sauorybodies and communiy groups (26).
Concrete and feasible actions that can betaken include:
Share inormaion abou ciy planningor healh
Encourage public dialogue
Involve communiies in decision-making
Creae opporuniies or paricipaion
3!
-
7/27/2019 Wh d 2010 Background
22/28
III. What can be done: calls to action
Build inclusive cities that areaccessible and age-friendly
Globally, populaions are rapidly ageing,leading o more older persons, many o
whom will experience mobiliy and sensoryimpairmens. WHO has developed a guideha is aimed primarily a urban planners omonior progress owards more age-riendlyciies in general (27).
Concrete and feasible actions that can betaken include:
Make public ranspor accessible o disabledpeople
Develop sae walkways or hose wihspecial needs
Build public places and buildings or easyaccess
Promoe acive ciy lie and spors or all
Make urban areas resilient toemergencies and disasters
Urban setings ace complex emergencies,including naural and human-made disasers.
Local governmens can play a crucial rolein urban disaser risk reducion, emergencypreparedness, and assessmen and responsein coordinaion wih oher emergencymanagemen mechanisms a he global,regional and naional levels.
Concrete and feasible actions that can be
taken: Locae healh aciliies in sae areas
Build more resilien healh aciliies owihsand known dangers
Srenghen communiy preparedness andresponse capaciy
Improve disease surveillance
In summary, or he frsime in hisory, we are livingin a predominanly urbanworld. Urbanizaion isconinuing, and local and
naional governmens aswell as communiies areacing many challengesas more people are livingin ciies. I is our colleciveresponsibiliy o ake acionnow o make sure ha ciies
are healhy or all people aall imes.
4! 5!
-
7/27/2019 Wh d 2010 Background
23/28
Ministries of health
o Become more informed abou hesocial deerminans o healh, and howurban policy choices impac healh anddevelopmen.
o Engage oher secors proacively in
dialogue, including housing, ranspor,indusry, waer and saniaion, educaion,environmen and nance agencies.
o Lead by examplebysupporinghealhier and more livable ciies.
o Suppor healh and environmenalimpac assessmen or urban plans andpolicies.
Local governments
o Show leadership by providing rolemodels and by seting an example.Champion walking, cycling, aciveliesyles and communiy designs hasuppor hese aciviies.
o Foser collaboraion wihin localgovernmen hrough orums or ciy
deparmens (such as ranspor, healh,public saey, parks and recreaion andeducaion) o discuss he developmeno an inegraed urban healh sraegy.Encourage public healh and urbanplanners o work closely ogeher.
o Parner wih volunary organizaions,professionals and communiyorganizaions and esablish a mechanismha will give healh proessionalshe opporuniy o provide inpu onplanning and ranspor plans.
o Share informaion and se upmechanisms or sharing daa on aciveliving, or example on he healh coss
o inaciviy and pedesrian ravel andsaey paterns, across governmendeparmens and wih civil sociey andhe communiy.
o Encourage and enable communiyparicipaionby engaging henongovernmenal, privae and publicsecors as well as ciizens o all ages inplanning and implemening iniiaiveso encourage acive living and physicalaciviy.
Civil society
o Ensure ha people are fully engaged inshaping he policies and programmesha aec heir lives.
o Include residens of informalsetlemens in ormal processes
by seting up groups, associaionsand ederaions. Large or small,organizaions o he urban poor shouldcome ogeher o ideniy he socialand economic condiions ha heyace; o nd pracical soluions ohese problems; o sruggle againsmarginalizaion; and o ensure accesso he goods and services o which
hey are eniled.
o Work wih governmens onparicipaory planning and
budgeingo allocae a greaerporion o he municipal invesmenbudge o prioriies deermined byneighbourhoods and communiygroups.
Annex:A role for all who can do what?
-
7/27/2019 Wh d 2010 Background
24/28
Researchers
o Generae and sysemaize knowledgeo address he many exisinginformaion gaps, including:
potentialadvantagesofurbanizaion and urban growh;
theinequitiesofhealthdisaggregaed by inra-urban area;
theeectivenessofproactiveapproaches o deal wih healhinequiy in ciies; and
theimportanceofinvolvingallciizens in he decisions ha aecheir habia and heir healh.
Urban planners
o Use zoning and land use regulaionsas a way o preven exposure o ciydwellers o polluion emissions andhazards rom indusrial aciviies,wase and chemicals, and well as
ranspor.o Develop/adop building pracices
ha proec healh among buildingusers regarding indoor airenvironmen, saey, noise, waer,saniaion and wase managemen,among several oher healhdeerminans in urban setings.
o Build compac ciies,where dwellershave easy access o green areas, publicranspor, cycle pahs and healh,educaion and oher undamenalsocial services.
o Incorporae Healh Impac
Assessmen (HIA) ino heconsideraion o alernaive planning
choices and policies.
International agencies
o Promoe and suppor policies opromoe healhy environmens.
o Disseminae lessons learnedrom onepar o he world o oher.
o Suppor womens righs, poveryreducion and equiy-promoingsraegies and programmes.
o Encourage policy-makers ogenerae and use sociodemographicinormaion o make beter decisionsregarding he urban uure.
Annex: A role for all who can do what?
-
7/27/2019 Wh d 2010 Background
25/28
1. Human Setlemens Programme. Te saeo he worlds ciies, 20102011. Nairobi [inproducion 2010].
2. Populaion Division o he Deparmen oEconomic and Social Aairs o he UniedNaions Secrearia (UNDESA). WorldPopulaion Prospecs: Te 2006 Revision and
World Urbanizaion Prospecs: Te 2007Revision. Unied Naions, New York, 26February 2008. [htp://esa.un.org/unup].
3. Brockerho M. An urbanizing world.Populaion Bullein. 2000; 55(3):34.Source: UNDESA. World UrbanizaionProspecs: Te 1999 Revision. UniedNaions, New York, 2001.
4. Saterhwaie D. Will mos people live inciies?BMJ, 2000; 321(7269):1143-1145.
5. Mongomery MR. Te Urbanransormaion o he Developing World.Science, 2008; 319(5864):761764.
6. Krieger J, Higgins DL. Housing andhealh: ime again or public healh acion.American Journal o Public Healh, 2002;92(5):758-68.
7. WHO/UNICEF Join Monioring
Programme or Waer Supply andSaniaion, 2010. [htp://www.who.in/waer_saniaion_healh/
publicaions/9789241563956/en/index.hml accessed 17 March 2010].
8. Progress on saniaion and drinking waer.World Healh Organizaion/UniedNaions Childrens Fund, Geneva, 2010.
9. Global healh risks: moraliy and burden odisease atribuable o seleced major risks.
World Healh Organizaion, Geneva, 2009.10. Capon AG. Healh impacs o urban
developmen: key consideraions.NSWPublic Healh Bullein, Sep.Oc. 2007;18(9-10):155-156.
11. Ghosh S, Shah D. Nuriional problems inurban slum children. Indian Pediarics,July2004; 41(7):682-696.
12. Dora C, Phillips M, eds. ranspor,
environmen and healh.WHO RegionalPublicaions, European Series, No. 89. WorldHealh Organizaion, Copenhagen, 2000.
13 WHO/UNEP. Healhy ranspor indeveloping ciies. Healh and EnvironmenLinkages Policy Series. World HealhOrganizaion, Geneva, 2008.
14. Peden M, Scureld R, Slee D, Mohan,Hyder AA, Jarawan E, Mahers A. World
Healh Repor on road raffi c injuryprevenion.World Healh Organizaion,Geneva, 2004.
15. Passchier-Vermeer W, Passchier WF. Noiseexposure and public healh.EnvironmenalHealh Perspecives, 2000; 108 Suppl 1:123-131.
16. Ciy Mayors Healh Repor. WHO callsor sronger ciies o help preven Asianhealh crisis. [htp://www.ciymayors.com/repor/asian_healh.hml accessed
26 February 2010].17. Te energy access siuaion in developing
counries. A review ocusing on he leasdeveloped counries and sub-Saharan Afica.UNDP and World Healh Organizaion,New York, 2009.
18. Campbell-Lendrum D and Corvaln C.Climae change and developing-counryciies: implicaions or environmenal
healh hazards and healh equiy.Journalo Urban Healh: Bullein o he New YorkAcademy o Medicine, 2007; Vol. 84, No. 1,pp. i86-i97.
19. McMichael AJ, Woodru RE, Hales S.Climae change and human healh.Lance,11 March 2006; 367(9513):859869.
20. Geronimus A. o miigae, resis, orundo: addressing srucural inuences on
he healh o urban populaions.AmericanJournal o Public Healh,June 2000;90(6):867872.
References
-
7/27/2019 Wh d 2010 Background
26/28
21. Marsella AJ. Urbanizaion, menal healh,and social deviancy. A review o issuesand research. American Psychology, 1998;53(6):624634.
22. Moser CON. 2004. Urban violence andinsecuriy: an inroducory roadmap.Environmen and Urbanizaion; 16(2):316.
23. WHO Commission on Social Deerminans
o Healh. Closing he gap in a generaion:healh equiy hrough acion on he socialdeerminans o healh. Final repor ohe Commission on Social Deerminanso Healh.World Healh Organizaion,Geneva, 2008.
24. WHO Cenre or Healh Developmen.Our ciies, our healh, our uure. Reporo he WHO Commission on SocialDeerminans o Healh fom he Knowledge
Nework on Urban Setings. Kobe, Japan.2008.
25. Unied Naions Populaion Fund. 2007Sae o he World Repor: Unleashing hepoenial o urban growh. New York, 2007.
26. Edwards P and souros A. Promoingphysical aciviy and acive living in urbanenvironmens: Te role o local governmens.
WHO Regional Oce or Europe,Copenhagen, 2006.
27. Global age-fiendly ciies: a guide.WorldHealh Organizaion, Geneva, 2007.
References
-
7/27/2019 Wh d 2010 Background
27/28
-
7/27/2019 Wh d 2010 Background
28/28
www.who.int/world-health-day/2010