
Wellbeing Solutions Management Risk Management Policy … _Risk Management Full Policy 2017.pdf**...
20
1 Wellbeing Solutions Management Risk Management Policy (RMP) Produced by Caroline Ribeiro-Nelson June 2016. Amended by Petra Nunzi January 2017
Transcript of Wellbeing Solutions Management Risk Management Policy … _Risk Management Full Policy 2017.pdf**...

1
Wellbeing Solutions Management
Risk Management Policy (RMP)
Produced by Caroline Ribeiro-Nelson June 2016. Amended by Petra Nunzi January 2017

2
Contents
1. WSM Risk Management Policy (RMP)
2. Definition of Risk
3. Assessment of Risk – TACT Telephone Counselling Assessment
4. Risk Criteria Levels & Intervention Table
5. The Risk Assessment Process
6. Risk Assessment Questions
7. Assessment of Risk & Flagging System
8. Risk Management Support Plans (RMSP)
9. Risk Management Session (RMS) at End of EAP Counselling
10. Telephone Counselling Risk Assessment Process
11. The face-to-face Counselling Risk Assessment Process
12. Guidelines for Counsellors: High Risk / Emergency Situations
13. Guidelines for Clients Presenting at Risk of Suicide
14. Suicide: Assessment of Risk Table
15. Suicide Risk Assessment Questions
16. Self Harm
17. Confidentiality
3
1. WSM Risk Management Policy (RMP)
WSM's RMP lays out specific guidelines, standards and procedures, which safeguard the welfare and safety of clients who present at risk. This policy relates to WSM employees and associated parties who have contact with WSM clients. Clinical processes involve the skills, knowledge and practice in the identification, assessment and implementation of a support strategy, which enables a client's clinical needs to be met. Our focus is to maintain a professional, client-centred, respectful and accepting approach. Confidentiality is essential. We strive to only intervene following a client's direct consent. It is in exceptional circumstances of extreme risk where impending and clear harm is assessed, that professional standards and the law permit for a breach of confidentiality. In such cases the counsellor / responsible person must take action to ensure the safety and welfare of the person at risk. All employees and associated persons who hold responsibility for client work and who come into direct contact with clients should be made aware of what constitutes risk. Once risk is identified this should be immediately assessed to determine level of risk: low risk, moderate or high / Emergency and to then determine the appropriate action to be taken.
2. Definition of Risk
Risk can be defined as the presence of internal or external factors, which present existing or possible harm / danger towards oneself or another individual. Risk of harm can be identified in a number of different areas: Physical Risk: Harm relating to the body such as: - the threat or presence of physical injury due to being hit, beaten, strangled, drug or alcohol abuse, self-harm for example: cutting, ingesting harmful chemicals, deliberately engaging in risky behaviour Sexual Risk: Relating to the threat or presence of harmful sexual actions such as: sexual assault / rape/abuse, exposure to sexually explicit actions or media. Emotional / Psychological Risk: Relating to the threat or presence of harm to one's emotional or psychological state due to actions such as: continuous verbal abuse

4
Neglect: particularly for children, elderly people, people with learning / developmental difficulties: Relating to the threat or presence of harm due to situations such as: not being given the basic and necessary care for healthy physical and emotional development, such as food, shelter, clothing emotional care and support. Social Risk Relating to the threat or presence of social factors which could harm one's safety or well-being, such as being homeless, being severely isolated, inadequate housing conditions, lack of financial funds
Environmental Risk “A substance, state or event which has the potential to threaten the surrounding natural environment and / or adversely affect people's health” Relating to the threat or presence of factors in the environment, which cause harm such as: toxic chemicals, unsafe equipment or building conditions, pollution, harmful biological substances such as Ebola, mould and pathogens.
3. Assessment of Risk - Initial Helpline Telephone Call
All clients accessing the clinical services should be assessed for risk in four main areas.
I. Risk of Harm to Self:
Situations which could constitute a risk to the client. Suicidal ideation/ attempts, self- harming behaviour i.e. cutting, hitting, ingestion of harmful substances (e.g. blades/toxic chemicals), deliberately putting oneself in a situation known to be harmful.
II. Risk of harm to or from another person:
This relates to situations such as: domestic violence, all forms of abuse, stalking, threats / existing physical or psychological harm

5
III. Difficulties which present risk of harm in the workplace: These are situations which seriously affect one’s ability to work or which present a risk of harm/ danger towards oneself, another person(s) or company. This relates to factors such as: the direct operation of equipment or supervision of people operating equipment, which may put individuals at risk, an individual holding responsibility for the welfare of others, or having responsibility for sensitive or important data.
IIII. Substance Abuse:
The use of drugs, alcohol, toxic chemicals or other harmful chemicals which constitute a risk of harm to the individual(s)
4. Risk Criteria Levels & Intervention Table
This table presents the Risk Criteria Levels providing information on each level of risk. The table describes WSM’s risk policy & procedures explaining the appropriate and necessary intervention and support strategies which are required to be carried out in order to safeguard the person(s) at risk.
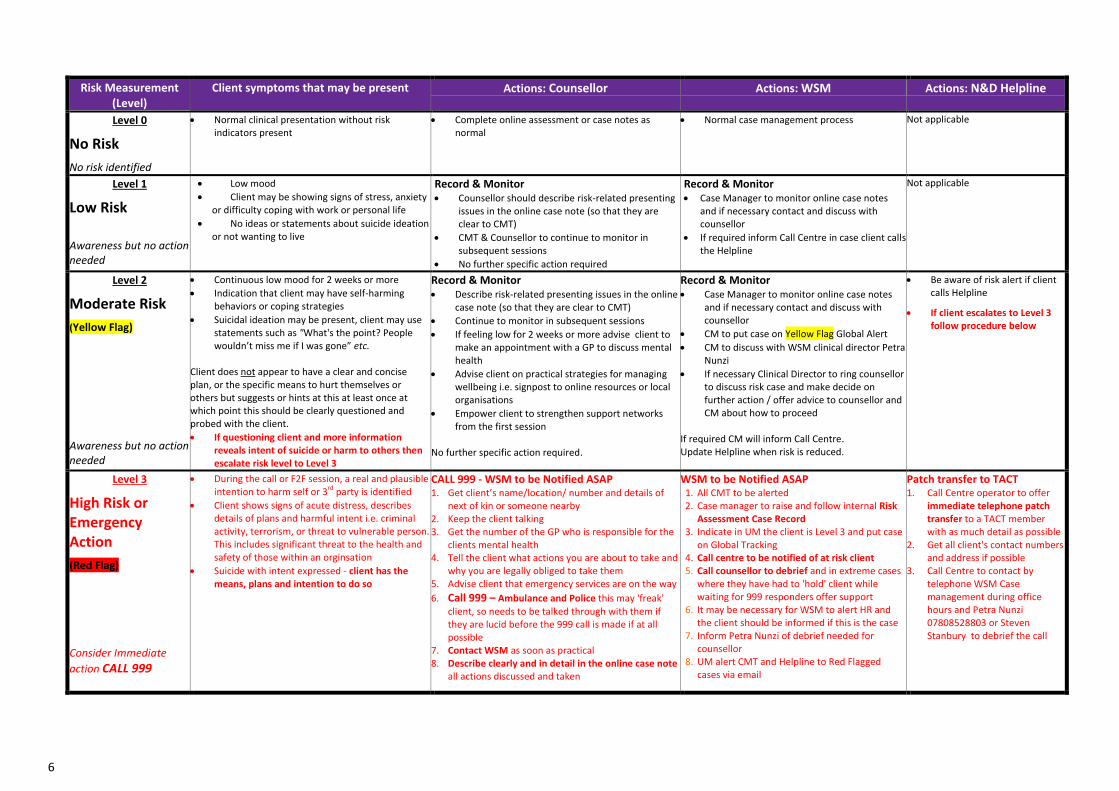
The WSM Risk Criteria Levels & Intervention table relates to risk levels from Low Risk, Moderate Risk, High/Emergency Risk. Risk Assessment Levels & Procedure: After every counselling session, counsellors are required to complete an online note which includes a client risk assessment measuring risk of suicide and/or risk of harming someone else. The following table outlines the Risk Levels and Actions to Take by the Counsellor, WSM Staff and WSM’s 24/7 Call Centre in each level.
6
Risk Measurement (Level)
Client symptoms that may be present Actions: Counsellor Actions: WSM Actions: N&D Helpline
Level 0
No Risk
No risk identified
Normal clinical presentation without risk indicators present
Complete online assessment or case notes as normal
Normal case management process Not applicable
Level 1
Low Risk
Awareness but no action needed
Low mood
Client may be showing signs of stress, anxiety or difficulty coping with work or personal life
No ideas or statements about suicide ideation or not wanting to live
Record & Monitor Counsellor should describe risk-related presenting
issues in the online case note (so that they are clear to CMT)
CMT & Counsellor to continue to monitor in subsequent sessions
No further specific action required
Record & Monitor
Case Manager to monitor online case notes and if necessary contact and discuss with counsellor
If required inform Call Centre in case client calls the Helpline
Not applicable
Level 2
Moderate Risk
(Yellow Flag)
Awareness but no action needed
Continuous low mood for 2 weeks or more
Indication that client may have self-harming behaviors or coping strategies
Suicidal ideation may be present, client may use statements such as "What's the point? People wouldn’t miss me if I was gone” etc.
Client does not appear to have a clear and concise plan, or the specific means to hurt themselves or others but suggests or hints at this at least once at which point this should be clearly questioned and probed with the client.
If questioning client and more information reveals intent of suicide or harm to others then escalate risk level to Level 3
Record & Monitor Describe risk-related presenting issues in the online
case note (so that they are clear to CMT)
Continue to monitor in subsequent sessions
If feeling low for 2 weeks or more advise client to make an appointment with a GP to discuss mental health
Advise client on practical strategies for managing wellbeing i.e. signpost to online resources or local organisations
Empower client to strengthen support networks from the first session
No further specific action required.
Record & Monitor Case Manager to monitor online case notes
and if necessary contact and discuss with counsellor
CM to put case on Yellow Flag Global Alert
CM to discuss with WSM clinical director Petra Nunzi
If necessary Clinical Director to ring counsellor to discuss risk case and make decide on further action / offer advice to counsellor and CM about how to proceed
If required CM will inform Call Centre. Update Helpline when risk is reduced.
Be aware of risk alert if client calls Helpline
If client escalates to Level 3 follow procedure below
Level 3
High Risk or Emergency Action
(Red Flag) Consider Immediate
action CALL 999
During the call or F2F session, a real and plausible intention to harm self or 3
rd party is identified
Client shows signs of acute distress, describes details of plans and harmful intent i.e. criminal activity, terrorism, or threat to vulnerable person. This includes significant threat to the health and safety of those within an orginsation
Suicide with intent expressed - client has the means, plans and intention to do so
CALL 999 - WSM to be Notified ASAP 1. Get client’s name/location/ number and details of
next of kin or someone nearby 2. Keep the client talking 3. Get the number of the GP who is responsible for the
clients mental health 4. Tell the client what actions you are about to take and
why you are legally obliged to take them 5. Advise client that emergency services are on the way
6. Call 999 – Ambulance and Police this may 'freak' client, so needs to be talked through with them if they are lucid before the 999 call is made if at all possible
7. Contact WSM as soon as practical 8. Describe clearly and in detail in the online case note
all actions discussed and taken
WSM to be Notified ASAP 1. All CMT to be alerted 2. Case manager to raise and follow internal Risk
Assessment Case Record 3. Indicate in UM the client is Level 3 and put case
on Global Tracking 4. Call centre to be notified of at risk client 5. Call counsellor to debrief and in extreme cases
where they have had to 'hold' client while waiting for 999 responders offer support
6. It may be necessary for WSM to alert HR and the client should be informed if this is the case
7. Inform Petra Nunzi of debrief needed for counsellor
8. UM alert CMT and Helpline to Red Flagged cases via email
Patch transfer to TACT 1. Call Centre operator to offer
immediate telephone patch transfer to a TACT member with as much detail as possible
2. Get all client's contact numbers and address if possible
3. Call Centre to contact by telephone WSM Case management during office hours and Petra Nunzi 07808528803 or Steven Stanbury to debrief the call

7
** Support Strategy at End of Counselling **
If client remains at risk at end of EAP counselling: Case Managers with WSM Clinical responsible person & allocated counsellor are to implement a clear support strategy to ensure, as far as possible, that the client:
Has access to a professional support network i.e. GP, Psychiatrist, Crisis Team, specialist physician, CPN, inpatient / outpatient psychiatric care, counselling services, social services, community support services: MIND, RELATE, CRUSE etc....
Is not left isolated and has social contact via: family, friends, colleagues, clubs & hobbies, social engagements & activities
If appropriate / required / beneficial, contact can be made with a professional support service to present client assessment, needs and recommendations for possible further support
Before closure of risk cases any contact that has been made by WSM with a professional support service should be followed up by CMT or counsellor and documented
** Risk Management Session (RMS) **
A Risk Management Session is an intermediary / follow up call in cases where there is serious concern for a client safety. These are sessions that counsellors offer to clients (employees) who are at suspected High Risk / Red Flagged Level 3 status as identified via the WSM risk assessment process.
The purpose of a Risk Management Session is in the moment support for a client who is in a vulnerable state. The purpose is to check on the client’s safety and to identify and signpost to appropriate crisis support
All RMS are telephone sessions
Counsellors RMS fee is £25.00 per session. (It is assumed that sessions will usually last between 15 – 30 minutes)
Counsellors will always be paid if they feel it is necessary to offer an RMS session to a client
Ideally 1 RMS will be allocated to 1 client with the aim of signposting to crisis services. If client is Red Flagged/Level 3 High/Emergency risk then more sessions can be offered without authorisation from WSM clinical responsible

8
5. Risk Assessment Process 6. Risk Assessment Questions
Risk Assessment Process / Risk Assessment Questions
The following questions present risk criteria which are provided as a guide in assessing the type and level of risk that exists for the client or third party. These questions can be used by the counsellor in the process of gaining relevant information, in order to plan appropriate action and support strategies for the client at risk.
1. How long has the client been dealing with the situation?
2. Has the client had thoughts of suicide (past or present)? Is there a family history of suicide?
3. Has the client attempted suicide in the past?
4. Has the client previously suffered from or is suffering from any conditions, which could lead to suicidal ideation, such as depression, psychological diagnosis of schizophrenia, sexual/physical/emotional abuse or neglect?
5. Is there present or historical domestic violence?
6. Is there any past or present risk of harm from another person? What type of contact does the client have with this person?
8. What personal and work stress factors exist?
9. What is the client’s support network: Family, Friends, work, social activities / clubs?
10. What medical input does the client have? - who, when & how is this given?
11. Is the client on medication? If so what is the medication & dosage?
12. What are the client’s internal and external resources in being able to cope with the situation?
13. How isolated is the client?
14. How well can the client assess his / her own needs?
15. Is substance abuse present and at what level?

9
WSM Risk Management Policy/Caroline Ribeiro-Nelson/June 2016. Confidential material not to be copied or redistributed
7. Assessment of Risk & Flagging System
Assessment of Risk Levels & WSM Flagging System
The WSM Risk Management Policy assesses and assigns risk on four levels: No Risk - Low Risk - Moderate Risk (YELLOW FLAG) - High Risk (RED FLAG). The table below presents details for the risk levels and flagging criteria. Low Risk
Low mood. Client may be showing signs of stress, anxiety or difficulty coping with work or personal life. No ideas or statements about suicide ideation.
Moderate Risk (Yellow Flag)
Continuous low mood for 2 weeks or more. Indication that client may have self-harming behaviours or coping strategies. Suicidal ideation may be present, client may use statements such as ‘What’s the point? People wouldn’t miss me if I was gone’ etc. Client does not appear to have a clear and concise plan or the specific means to hurt themselves or others but suggests or hints at this at least once at which point this should be clearly questioned and probed with the client.
High Risk / Emergency (Red Flag)
During a call or F2F session, a real and plausible intention to harm self or 3rd party is identified. Client shows signs of acute distress, describes details of plans and harmful intent i.e. criminal activity, terrorism or threat to vulnerable person. This includes significant threat to the health and safety of those within an organisation. Suicide with intent expressed – client has the means, plans and intention to do so.
10
WSM Risk Management Policy/Caroline Ribeiro-Nelson/June 2016. Confidential material not to be copied or redistributed
8. Risk Management Support Plans (RMSP)
Risk Management Support Plan (RMSP)
The following process relates to all clients who have been assessed at being at Moderate risk Yellow Flag and High/Emergency Risk Red Flag:
A clear support plan to be produced by the allocated counsellor or WSM Clinical Responsible
Support Plan to follow the below format, including details of the following:
Risk issues presented
How the counsellor will be working to stabilise the client
The internal and external support and coping strategies the counsellor will be encouraging the client to use
The external support network that is in place for the client
Recommendations for further support / next steps
The RMSP is to be created directly following the session from which the client has been Yellow or Red flagged The Risk Management Support Plan is to be written and updated following each session by the counsellor in the relevant section of the counsellor case notes.

11
WSM Risk Management Policy/Caroline Ribeiro-Nelson/June 2016. Confidential material not to be copied or redistributed
9. Risk Management Session (RMS) at End of EAP counselling If a client remains assessed at risk at end of EAP contact the CM is to contact the client’s counsellor to clarify that the client is in stable condition and if required has access to a support network. If the assessment shows the client to still be at risk the counsellor is to carry out a Risk Management Session (RMS): This is to assess whether the client is presently safe & has appropriate support options before the case is closed.
Possible support resources relate to: GP, psychiatrist, CPN, neurologist, Social Services, OH, Mental Health Crisis Team, outpatient support services, specialist practitioner, private face-to-face counselling, friends, family, colleagues, Church, local community support services, such as: RELATE / MIND.
10. Telephone Counselling Risk Assessment Process
Telephone Counselling Risk Assessment Process (please also refer to the WSM risk criteria & intervention table)
An appropriately trained and professional service representative answers calls. A counsellor carries out the risk assessment. A decision for appropriate action can then be made. The counsellor is to inform the case manager of the risk level assessed. The counsellor will explore the area of risk, in order to determine: The immediacy of the risk:
Has the client or third party person carried out or are they about to carry out an action, which constitutes a clear, present and imminent action, which could result in death or serious harm to self or another person?

12
The likelihood of any threatened action being carried out:
What factors are present which indicate that serious harm or possible death could result?
Does a clear plan exist?
Does the person possess or have access to the means of carrying out harmful action?
Has the person carried out similar actions in the past?
Are there highly stressful or distressing factors present?
Are mental health / psychological issues present, which could cause the person to carry out harmful acts? An assessment of the risk to the client should then be made in terms of Low Risk, Moderate Risk Yellow Flag or High/Emergency Risk Red Flag Once the level of risk has been established, the counsellor will take whatever action is necessary to safeguard the client. This may include any combination of the following actions (which can be adapted to both the resources available and the legal requirements in its relevant context):
Contact with the emergency services: Police / Ambulance Contact with the client’s G.P. by telephone, fax or letter. In situations of high risk, it is essential to speak directly to the practitioner
concerned and to follow up the conversation with a letter (usually faxed, with a copy also sent through the post). Telephone contact with family members, partner, friend, colleague, neighbour or anyone present in the client’s immediate area. Regular client telephone support to the client until it is possible for the client to access local professional support. An urgent referral to the EAP’s face-to-face counselling service. (Where possible and appropriate). Telephone support (a Risk Management Session: RMS) between counselling sessions to stabilise client and signpost to further support.

13
WSM Risk Management Policy/Caroline Ribeiro-Nelson/June 2016. Confidential material not to be copied or redistributed
11. The face-to-face Counselling Risk Assessment Process
The Face-to-Face Counselling Risk Assessment Process
The risk assessment carried out by face-to-face counsellors follows a similar format to telephone counsellors, however in a broader and deeper form. In some instances, risk issues only become evident in the face-to-face situation, even though the client has been assessed for risk in the in their initial call to the Helpline. The clinical assessment in this context focuses on all the risk areas already described.
Where any form of risk is identified, the counsellor should sensitively explore the detail of the risk situation, thereby establishing what, if any, actions need to be undertaken to ensure the client’s safety. Actions carried out will depend on the nature and severity of the risk, but these will normally involve referral of the client to an appropriate resource. Depending on the clinical presentation, EAP support may continue or may be closed. Whichever is the appropriate decision, support should not usually be stopped abruptly the remaining sessions should be used to facilitate and promote the referral process. The WSM Clinical Director is available to the affiliate counsellor for discussion of any risk issues. Counselling affiliates are expected to inform the Case Management Team immediately of any issues of concern; so that WSM can ensure that any necessary steps are taken promptly.

14
12. Guidelines for Counsellors: High Risk or Emergency Situations Red Flag
Guidelines for Counsellors: High Risk or Emergency Situations
The following guidelines provide information for counsellors on procedures for handling clients presenting in High Risk or Emergency situations.
High Risk or Emergency situations consist of factors which clearly indicate that the client or third party is at clear, severe and immediate risk of harm or death. These relate to situations such as; but are not limited to:
Suicide attempts Clear expression of suicide intent – plan and means present and imminent Clear expression of harm / danger to a third party: e.g. death threats, present or imminent physical / sexual attack, bomb / terror
threats Severe abuse to child / vulnerable person Severe physical injury / medical conditions: e.g. life threatening wounds, stroke / heart attack etc.
The counsellor should let the client know that you are highly concerned for their welfare. Explain that there is a serious risk present and that you are obligated to take action, in order to help the individual(s) in danger. Focus on engaging the client and maintaining contact. Has the client already taken action? When does the client intend to act? If action has been taken how long ago? What is the extent / level of risk or injury? i.e. in case of an overdose, what was taken, how much, when, what with Identify if there is any other person at risk of imminent harm If you need to put the client on hold, make an agreement that he / she will not carry out any harmful intent or take any further
harmful action while help is being organised. Record these details clearly in the case notes

15
Making direct contact with the emergency services:
Without ending the contact with the client call 999 and present details to the appropriate emergency service: Ambulance / Police State your name and explain that you are a psychological professional reporting a person in immediate danger / at life threatening risk Confirm with the operator that you are speaking with the appropriate emergency service Once you have confirmed that you are speaking to the correct service provide the operator with full and precise details of the client in danger Provide the client’s personal details: name, gender and age Provide the client’s contact details: home address and present location, if different, and phone number Details of other persons present at the location, particularly any possible vulnerable persons such as: young children or dependents Present the details of the situation stating the type of risk present: i.e. suicide attempt, wounds or injuries, chest pains, loss of ability to feel or
move, threat to a third party Present details of the client’s physical / medical state: known and diagnosed physical or mental health condition Continue to speak with the client until the arrival of the emergency services or professional Before ending the call speak directly to the emergency personnel who attend at the scene Confirm who you are and provide relevant factual information if asked to do so Identify what medical location / facility the client will be taken to Provide your contact details, in the event that the emergency or medical services need to contact you Contact WSM as soon as is practically possible Record clear and detailed information in the online case notes ASAP In discussion with WSM CMT / WSM clinical responsible person the counsellor, should carry out a follow up risk management session at an
appropriate time with the client / relevant support service
** Risk Management Session (RMS) refers to the WSM risk assessment criteria and intervention table **

16
13. Guidelines for Clients Presenting at Risk of Suicide (See 5.2 for information on Self-harm which is distinctly different than suicidal ideation or suicide)
Guidelines for Clients Presenting at Risk of Suicide
The following guidelines provide information on the assessment and management of clients presenting at risk of suicide. There is no clear or reliable method to predict if an individual may attempt suicide. The National Institute for Health and Care Excellence (NICE) point out that scoring system’s for suicide are not good predictors of suicidal risk. It is recommended that a full assessment by a clinical professional is carried out.
It is important to understand the specific factors which may increase or decrease the possibility of suicide. The specific identification of circumstances which contribute to increased risk of suicide can be useful in assessing the level of risk for the individual. In the management of clients, the recognition and utilisation of factors which decrease the risk of suicide constitute protective factors which can be used to formulate a clear support plan and strategy.
Suicide can be described as ‘the act of killing oneself intentionally’ (Oxford Dictionary). Although suicide is often seen as impulsive, it may be associated with years of suicidal behaviour including suicidal ideation or untreated mental illness.

17
Office of National Statistics [ONS] UK Classification of suicide: 2015
The table below provides information for factors that increase or decrease suicidal risk (protective factors)
14. Suicide: Assessment of Risk Table
Assessment of Risk Table Factors which increase suicide risk Factors which decrease suicide risk
Strongest risk factor: Past suicide attempt.
Males are 3x more likely than females.
Age range: Males, 40-44 years of age and Female, 50-55 years of age.
Mental health conditions. Diagnosis of mental health condition(s): Depression (highest), schizophrenia / psychosis, personality disorder. Irrational and erratic thought patterns and behaviour. Feelings of hopelessness, despair, shame and / or guilt.
Stable mental status. Strong inner resources / resilience and the ability to use coping strategies. Sense of humour. Positivity.
Lack of access to mental health treatment. Good and consistent access to mental health support services and treatment.
Presence of a clear plan. Absence of a clear plan.
Access to means for self-harm or suicide. Lack of access to means of self-hard or suicide.
Past family history of suicide.
Isolation / lack of a support network. Presence of a supportive, positive and consistent support network (personal and professional).
Alcohol / drug abuse.
Impulsive and / or aggressive tendencies. Good ability to recognise destructive tendencies and a strong ability to utilise constructive coping strategies.
History of child abuse
Cultural beliefs (e.g., belief that suicide is a noble resolution of a personal dilemma).
Cultural beliefs which discourage suicide.
Physical or medical illness. Good and consistent access to health support services and treatment.
Unwillingness to seek or accept help. Willingness to seek or accept help.
Recent significant bereavement / loss. Presence of a supportive, positive and consistent support network

18
(personal / professional).
Personal conflicts / relationship breakdowns / child custody issues.
On-going legal prosecution / battles.
Bullying. Strong inner resources / (resilience) and ability to utilise coping strategies stable mental status. Presence of a supportive, positive and consistent support network (personal / professional).
Unemployment or financial difficulties Access and participation in social activities. Ability to plan and utilise practical strategies in dealing with difficulties.
**Suicide statistics reports 2014-2015/UK/ Samaritans**
19
15. Suicide Risk Assessment Questions
Guidelines for Clients Presenting at Risk of Suicide
Risk Assessment Questions
The following questions present criteria which are provided as a guide in assessing the type and level of risk that exists for the client or third party. These questions can be used by the counsellor in the process of gaining relevant information, in order to assess the level of risk and to plan appropriate action and support strategies for the client at risk.
1. Is the client thinking about ending his / her life? 2. How likely does the client feel he / she will take action? 3. How long has the client been dealing with suicidal thoughts / intent? 4. Is there a family history of suicide? 5. Does the client have concrete plans? 6. Has the client previously suffered from or is suffering from any conditions, which could lead to suicidal ideation or self-harm, such as
depression, psychological diagnosis of schizophrenia, sexual/physical/emotional abuse or neglect? 7. What personal and work stress factors exist? 8. How isolated is the client? 9. What is the client’s support network: Family, Friends, work, social activities / clubs? 10. What medical input does the client have? - Who, when & how is this given? 11. Is the client on medication? If so what is the medication & dosage? 12. What are the client’s internal and external resources in being able to cope with the situation? 13. How well can the client assess his / her own needs? 14. Is there alcohol/ substance abuse present and at what level?

20
16. Self Harm
Guidelines for Clients Presenting at Risk of Suicide
Suicide intent and ideation are not to be confused with Self-harm which is defined as any act of self-poisoning or self-injury irrespective of motivation. The phrase ‘self-harm’ is used to describe a wide range of behaviours. Self-harm is often understood to be a physical response to an emotional pain of some kind, and can be very addictive. Some of the things people do are quite well known, such as cutting, burning or pinching, but there are many, many ways to hurt your self, including abusing drugs and alcohol or having an eating disorder. Sometimes, it’s more important to focus on how someone is feeling rather than what they do to themselves. Quite often, people find that more helpful. People who self-harm normally do not wish to kill themselves. Suicide is a way of ending one’s life, but for many people, self-harm is a way of coping with life and being able to continue with living despite the emotional difficulties they may be experiencing. For some, the physical pain of self-harm reassures them they are still alive – this might be because they are experiencing emotional numbness or feeling disconnected from the world around them, or at the other end of the spectrum, feeling more connected and alive than they did previously. Self-harm can also cause changes in the brain chemistry, which, although ‘satisfying’, can easily become addictive and therefore dangerous.. Sometimes people do die as a result of self-harm. This may be because they have taken an act of harming too far, and they lose their lives before help is found, or it may be they engage in something such as self-poisoning, which carries an incredibly high risk of death if untreated. There is believed to be an increase in suicidal intent if someone is prevented from self-harming. As difficult and challenging as it can be to understand, sometimes self-harm may be the safest option, if the alternative involves a desire to end life. It’s dangerous to prevent someone from harming without providing them with a realistic, alternative coping mechanism that they are willing to engage with. Self Harm UK www.selfharm.co.uk.
17. Confidentiality
Confidentiality
Clients should be told of the limits of confidentiality at the earliest and most appropriate time within the first call. In rare situations, this may not be possible. There will always be circumstances where a client is so distressed that it feels inappropriate to explain the confidentiality policy, or the call may be cut short. If it was not possible to inform the client about confidentiality during his / her first call the client should be immediately informed about confidentiality on the next contact. Before beginning telephone counselling, awareness and understanding of confidentiality should again be clarified. We should bear in mind, at all times, that it is unethical not to inform clients of the limits to confidentiality before they disclose material to us, which could necessitate a breach of this right.


















