Welfare State Restructuring And Policy Feedbackpaperroom.ipsa.org/papers/paper_12212.pdf · Welfare...
30
1 Welfare State Restructuring And Policy Feedback Anna Bendz Department of Political Science University of Gothenburg Box 711 405 30 Gothenburg Sweden [email protected] This paper is in a preliminary stage, please do not cite. All comments welcome! Prepared for presentation at XXII World Congress of Political Science (IPSA). Madrid July 8-12, 2012
Transcript of Welfare State Restructuring And Policy Feedbackpaperroom.ipsa.org/papers/paper_12212.pdf · Welfare...

1
Welfare State Restructuring
And Policy Feedback
Anna Bendz
Department of Political Science
University of Gothenburg
Box 711
405 30 Gothenburg
Sweden
This paper is in a preliminary stage, please do not cite. All comments welcome!
Prepared for presentation at XXII World Congress of Political Science (IPSA).
Madrid July 8-12, 2012

2
Introduction
Welfare policies have consequences. Not just in terms of outcomes like the number of patients treated
by hospitals, the quality of education or how many senior citizens get help from home service.
Welfare policies also have consequences for mass opinion such as perceptions of the welfare state and
government in general, political action, and trust. Peoples’ experience with the welfare state transfer
into opinion and behaviour that is at the heart of democratic functioning. The growing research
tradition of policy feedback captures the relationship between policy (or institutional design) and mass
opinion by seeking to clarify how policies are likely to affect political thought and action in the
citizenry. Research on policy feedback-processes thus clarifies how public policy matter for the
vitality and function of democratic politics (Mettler & Soss 2004).
This paper takes it’s empirical point of departure in the contemporary and ongoing changes of the
Social Democratic Welfare State, with focus on the restructuring of the welfare service sector in
Sweden. The change of the welfare state service arena refers to the New Public Management-inspired
policy aiming to achieve a more efficient and responsive public service sector by creating competition
between different providers of welfare services. As a result, the welfare service sector becomes more
market-like with private and public actors competing to attract the ”consumers”.
For the Social Democratic Welfare states and its citizens, this is a significant change since one of the
most defining features of this type of regime is that it provided public welfare services on a totally
different scale than all other countries outside Scandinavia (Lindbom 2001, Esping-Andersen 1999).
Additionally, Social Democratic welfare states traditionally builds on principles of universality and
entitlements which is in conflict with the market principle of relying on effective demand to bring
forward service supply (Taylor Gooby 2004). Thus, this policy re-orientation challenges one of the
core values of this kind of welfare state, social equality (Bendz 2012).
The general argument in this paper is that the changing character of the Social Democratic welfare
state has implications for the relationship between state and individual since the terms of the social
contract is re-negotiated in several welfare service areas. Instead of being a more or less passive
service recipient, citizens are expected to take responsibility over their welfare in a more active way
by making good and informed (rational) choices according to their preferences. This, in turn, is in this
paper assumed to have consequences for public opinion. By focusing on the connection between
policy and public opinion, the ambition in this paper is to contribute to the growing literature on policy
feedback effects that aims to bridge the gap between policy analysis and research on mass opinion.

3
Why would market-oriented welfare reforms have consequences for public opinion? The key
mechanism put forward here is that the policy-reorientation is tipping the power-balance between state
and individual by empowering the citizens. Empowerment is in this case created by allowing freedom
of choice for the citizens in the welfare service area, by giving the opportunity to choose from an
increased number of available service producers. This means two closely related things: that citizens
may choose an alternative according to their preferences, and that they have the possibility to exit
from this alternative and choose another one if they are not content. The presence of exit options has
been showed to generate positive welfare state experiences, which in turn generates support for the
welfare state (Kumlin 2004). Also, such positive experiences seem to have spill-over effects to
opinions about the government and politics in general (Soss 1999).
This paper focuses on one specific case, and thereby it differs somewhat from most previous research
on policy feedback effects of welfare policy and/or institutions, which have mostly had a comparative
design. The empirical case in the paper concerns the implementation of a consumer’s choice model in
Swedish primary health care in 2009/2010. The reform allows private and public providers of primary
health care to compete on equal terms for clients, financed by tax money (see further below). I argue
that this reform is a most likely case for policy feedback effects because of its high visibility and
proximity (Soss & Schramm 2007, Pierson 1993. See also further below).
The aim of this paper is to elaborate on the correlation between institutionalised empowerment and
public opinion by analysing which consequences for welfare attitudes that follows from the
implementation of consumer’s choice in Swedish primary health care. Do experience from
institutionalised empowerment in one welfare service generates a) contentment with the service and b)
support for the market-orientated restructuring of the welfare service area in general? This, in turn,
would implicate that the institutional design of welfare services can contribute to the reinforcement
and stabilization of a certain welfare policy through creating popular support.
In the next section of the paper, policy feedback and empowerment in the welfare state context is
discussed as a theoretical frame of analysis. After this, the Swedish case is introduced by a description
of the contemporary changes of the welfare state service sector. A brief design and method section is
then followed by results and a final discussion.
How and why public policy matters for public opinion
A key insight from policy feedback research is that public policy matter for the vitality and function of
democracy by affecting how people think and act as members of a community. Thus, policy is not
only output of political decisions, but also inputs that create frames and structures that not only affect

4
costs and benefits associated with future political decisions but also peoples’ incentives and
perceptions which in turn influence political action (Pierson 1993). By connecting research on public
policy and research on mass opinion, it is possible to assess the democratic consequences of policy as
well as contribute to the understanding of mass political behaviour (Mettler & Soss 2004).
Policy feedback is from the start associated with historical institutionalism, where policy feedback
refers to how existing policies affect politics and policy development over time. The research focused
on for example state building, interest group formation and lock-in effects (Pierson 1993, Skocpol
1992, Hall & Taylor 1996). The topic in this paper connects to one of the more recent strands in the
research on policy feedback where the focus is on how policies affect beliefs, preferences and actions
of mass publics where scholars explore the relationship between policies and political participation
and attitudes (see e.g Béland 2010, Mettler & Soss 2004, Soss 1999, Soss & Schram 2007, Campbell
2003, Svallfors 2010, Mau 2003).
The empirical research in this part of policy feedback-inspired research has a certain emphasis on
welfare policies. Soss and Schram (2007) points out welfare reform as a promising case to advance the
policy feedback research field since welfare reform can be seen as a ”most likely”-case for feedback
effects: “In short, welfare reform offers a case in which predictions of mass feedback seem both
plausible and amenable to testing” (p 114). The reason is that welfare policies is important to many
people and also that many have experience from one or several welfare programs during their lifetime,
even though this varies greatly across countries. In Sweden, it is hard for citizens not to have quite a
lot of experiences of the welfare state because of its size and scope. This fact can be argued to make
Sweden one of the most interesting cases among welfare states if one wants to investigate the effects
of welfare policy in general.
What does public policy affect and how?
In an article by Mettler and Soss (2004) on policy feedback as a research area, policy is suggested to
have effects on “political thought and action”, but also “what individuals think, feel and do as
members of the polity” and how public programs shape “citizens’ beliefs, preferences, demands, and
power” (Mettler & Soss 2004). In other words, policy feedback effects on mass opinion can be
expected to be found in a very broad range of human reactions to public policy.
What aspects of mass opinion that is affected by public policy is not a fixed set but rather defined by
the researchers interest and also, of course, tried and shown in empirical studies. Some examples:
Campbell (2003) showed that elderly citizens that participate in US Social Security get more inclined
to electoral participation, and that this participation then affects the politics of Social Security in

5
significant ways. Soss (1999) explore the links between welfare participation and political
involvement. He shows that the design of welfare programs lead to different beliefs about if it is
efficient to make demands in the programs and different perceptions about one’s own ability to
understand and participate in political life. Solevid (2009) investigates how institutions constitute the
relationship between evaluation of public service and political action and shows that the degree of
empowerment is important for the extent to which dissatisfaction with services translates into political
action. Kumlin (2004) shows that institutionalised empowerment leads to general trust in the political
system and in politicians.
As the above examples show, policy feedback effects can be assumed to occur (and be measured on)
different levels or distances from the policy that is assumed to have effects on mass opinion. Just like
the rings spreading outwards when throwing a stone in the water, feedback effects can spread further
away from reactions on the specific policy area or group of policy areas to reactions to the political
system in general. As Soss (1999) points out, for many people welfare experiences serve as their most
direct source of information about how government works. Thus, welfare program users use their
experiences to draw inferences about government in general, for example of the government’s
responsiveness or their own ability to participate in political life. The conclusion is that welfare
programs are sites of political learning: Clients interpret their experiences with welfare bureaucracies
as evidence of how government works in general (Soss 1999).
In some of the previous research in this area, the research question emanates from an ambition to
explain a certain output by using policy feedback approaches, for example social trust (Larsen 2007).
In other, the interest lies in a particular correlation, for example how welfare state retrenchment affects
perceptions of how well democracy works (Kumlin 2010) or how citizens’ aggregate policy
preferences contribute to welfare state persistence (Brooks & Manza 2006). In this paper, the
research interest lies not in explaining a particular dependent variable, nor in elaborating on a
particular correlation. Instead, I ask the question in a more open manner, departing from the
assumption that the policy changes in the Swedish welfare state should have at least some effects on
some of the factors in the possible range of reactions. This assumption emanates from that welfare
policy is pointed out as particularly likely to generate feedback effects, but also from the nature of the
policy that is in focus here. The restructuring of the welfare state in Sweden is assumed to give rise to
what Paul Pierson have named as interpretive effects, that is impact on cognitive processes meaning
that peoples’ opinions, preferences and actions are affected by policy design (Pierson 1993).
Soss and Schram (2007) suggest a general framework for analysis of mass feedback processes. For
this they use two dimensions. Visibility refers to the degree to which a policy is salient to mass publics.
Proximity refers to the direct versus distant form in which a policy is encountered. High proximity

6
means that people have individual experience of a policy or program. These dimensions are put
together in a two by two matrix. The proposition is that the relationship between public policy and
mass opinion will proceed according to different logics depending on a policy’s location on the
dimensions. A policy with low proximity and low visibility will not very likely influence mass opinion,
while a policy that has high proximity and visibility will have the greatest potential for policy
feedback effects on mass opinion.
Following this framework, I argue that the reform studied in this paper is characterized by high
proximity and high visibility for most people, which mean that it is reasonable to expect feedback
effects on public opinion. Most people, or their close relatives, uses a health care centre more or less
often in their lives, thus most people have a direct experience of health care centres. Recent figures
from a national survey show that about 80 % of the Swedes have been in contact with a health care
centre, either themself or a close relative. The health care reform is also highly visible one: not only
are health care in general pointed out as one of the most important areas by the Swedes, the reform
itself was also quite visible in the media especially at the time of the reform’s introduction. This kind
of policies should, according to Soss and Schram, produce feedback effects by the cues they convey to
broader mass audiences either through the policy’s direct impact on peoples’ lives or from it’s
symbolic meanings (Soss and Schram 2007).
Empowering the people
The most tangible consequence of the contemporary restructuring of the welfare service sector in
Sweden is that citizens are given the possibility to choose from a range of private and public service
providers. In other words, the welfare service sector empowers people to a higher extent than before,
foremost by allowing exit options. Empowerment is in this paper seen to be the mechanism that links
public policy to public opinion, that is the mechanism through which feedback effects operate (Solevid
2009).
Empowerment as a concept refers to the power balance between the state and the individual citizens.
The higher the degrees of influence over one’s life circumstances, the higher the degree of
empowerment. Building on Hirschmanns famous distinction there are two main strategies to create
empowerment: Exit and voice. Exit means that people, when dissatisfied with a government or a
public policy, can choose an alternative by for example voting for a new party on election day or
choosing another school for their children if they are not happy with the present one. Exit options are
present whenever there are alternatives. Voice means to try to change things within the existing
alternative instead of choosing another one (Hirschmann 1970).

7
In the welfare state context, exit-options refer mainly to the presence of one or several other
organizations – public or private- that offers comparable service. Since it can be assumed that public
agencies as well as private companies want to keep their clients, bureaucrats should be more likely to
listen to complaints and preferences if there are exit-options. In this way, exit-options make the power-
balance lean over to the citizens (Hoff 1993, Kumlin 2004). The knowledge that exit options exist can
be argued to strengthen individuals’ autonomy and general self-confidence in their encounters with the
welfare state. Thus, possibility of exit strengthens the power balance in favour of the individual
through mechanisms of autonomy and self confidence (Solevid 2009).
Primary health care is in Sweden a universal welfare service with a non-discretionary character in the
sense that access is not granted on economic grounds, that is that citizens is granted access to health
care depending on their ability to pay or that they get access to public health care because of poverty.
Universality can in itself be seen as a dimension of empowerment. Empirically, it has been proved that
citizens in programs with a universal (non-discretionary) character are more positive towards the
welfare state than citizens that have experiences from a program where public officials have
discretionary power (see for example Rothstein 2010).
Welfare institutions can be categorized according to the degree of empowerment. Kumlin (2004) and
Solevid (2009) both show empirically that there is a difference in effects on public opinion and
behaviour depending on if citizens have experience from institutions with high or low institutionalized
empowerment. Institutions with higher levels of institutionalized empowerment generate positive
effects on public opinion, while institutions with lower levels of institutionalized empowerment
generate negative effects. The Swedish primary health care system was by these researchers
categorized as an institution with limited or medium exit options. This was true before the 2010
reform (se below), but an important consequence of this reform is that exit options have increased for
at least the majority of the Swedish citizens. As already mentioned, exit options vary geographically.
In other words, primary health care has moved closer to the consumer or customer type of institution.
This change is a point of departure for the empirical analysis in this paper.
Following previous research on empowerment and it’s effects on public opinion, it is possible to
assume that the change of the primary health care in Sweden from a system with medium exit options
to a system with extensive – or at least better – exit options should lead to positive welfare state
experiences. This in turn is assumed to generate positive feedback effects on attitudes to the specific
policy (primary health care). Additionally, empowerment is hypothesized to generate positive
opinions of the restructuring of the welfare state in other service programs. This is a way of extending
the analysis at least a bit away from the “close” reactions following a specific policy, thus contributing
to the question of generalised feedback effects. The idea underpinning this hypothesis is that positive

8
experiences from one welfare service program may transfer into positive attitudes to similar policies.
The general policy underlying the reform in primary health care is to increase efficiency and freedom
of choice by allowing private companies (or non-profit organisations) to provide welfare services. For
consumer’s choice to become realistic for the citizens, it is necessary that several – and preferably
different – actors provide welfare services. The reason why experiences from choosing welfare
provider in one area should have effects on attitudes towards market-orientated reforms, is that letting
private actors in on the welfare service market is actually what creates the possibility to choose.
As Mettler and Soss points out, to develop the research area on policy feedback it is important to try to
specify how, where and when policy feedback effects occur (Mettler & Soss 2004, see also Pierson
1993). My argument is that not only could there be differences between programs with different
degrees of empowerment, but also differences in to what extent institutionalised empowerment have
effects within a specific program. The point of departure is that welfare program participants can
experience empowerment in a direct or an indirect way and this may in turn be of importance for the
effects that empowerment has on public opinion and behaviour. In this paper, this idea is tried out in a
first empirical study.
What does it mean to have direct experience from empowerment? The idea is that welfare service
users may have very different experiences even though they use the same kind of (empowering)
welfare service. If the welfare service involves customer’s choice, people can choose to participate
actively or not by making active choice or merely being placed with a designated provider. Also, there
might be geographical variations when it comes to what service alternatives that are actually available
within a reasonable distance, which in turn makes it more unlikely that people use the possibility to
exit even if they are discontent with the service. This line of thought is further discussed below.
Exit can in theory occur either to another service provider or to no alternative at all (Hirschman 1970).
An important institutional factor that determines the degree of empowerment is the presence or
absence of realistic exit options (Möller 1996). This means for example that for exit options to be
empowering, citizens should have a reasonable short geographical distance to another service
alternative. If not, it is unlikely that citizens express their dissatisfaction with the service by leaving.
Their experience of the welfare state is certainly different from residents of city areas, where there are
plenty of service alternatives to choose from. Also, the service provider is more unlikely to adjust the
service according to citizens’ preferences because of the “threat” of exit. In this paper, present or
absence of realistic exit options in terms of geographical distance is used as a way to vary exit options
within the Swedish population in order to be able to draw conclusions about the effects of exit options.
Even if there are realistic exit options, not all people choose to use them. The experience of using the

9
possibility to re-make the initial choice of health care centre may enhance the effect of
institutionalised empowerment since it is a direct experience of using exit as a way to influence one’s
situation. In the empirical analysis, this is investigated by grouping people according to if they have
used the option to exit or not.
Realistic exit options presuppose not only the existence of alternatives, but also that welfare programs
are designed in a way that makes it possible for citizens to make an informed and active choice of
service provider. This means that the concept of exit options is closely related to freedom of choice
but not exactly the same (see for example Sen 1988). Exit and choice can be obstructed by for
example emotional attachment or feelings of loyalty (Sörensen 1997). This is related to the fact that
not all people wants to, or have the opportunity to, use the given freedom of choice. It is likely that the
experience of empowerment are stronger among those who actively participate in the system, in this
case by actively choosing health care centre, than among those who for different reasons do not make
an active choice. To use the possibility to choose health care centre actively indicates that the service
is important to the person. Also, it is more likely that active choosers have reasonably good
information about the system. This should generate a stronger sense of empowerment with this group,
compared to the group of persons that are passive users of the service, and thus lead to more positive
opinions. In the empirical analysis of this paper, active or passive participation in the program is tried
out as a possible factor that can mediate the effects of institutional empowerment.
Specific research questions:
Does empowerment in terms of (increased) exit options generate a) positive attitudes to the primary
health care system and b) support for the restructuring of the welfare service sector in Sweden?
Under what circumstances (if any) do exit options matter for attitudes?
- Does realistic exit options make a difference for opinions?
- Do active participants have more positive attitudes than passive?
The Restructuring of the Swedish Welfare State
The value of equality is (or maybe has been) a core value of the Social Democratic welfare model
(Esping-Andersen 1990). As a consequence of the embracement of equality as a primary value, the
public welfare sector is traditionally extensive and the private sector has been given limited space, in
order to give citizens equal access to welfare services. Access to services should, according to this
model, be based on need, not wealth. Additionally, the social services should be the same for everyone,
and because of that they have been constructed in a unitary way and provided by the public sector
(Rothstein 2010).

10
The restructuring of the Swedish welfare state has been going on since the beginning of the 1990’s.
The right wing government started to open up for competition and models of consumers’ choice in
their period in government 1991-1994. This development was slowed down somewhat when the
social democrats regained power 1994-2006, but still went on. When the right wing government
coalition came to power in 2006, the reforms aiming towards competition and increase of private
actors in welfare services was again implemented at a faster pace (Hartmann 2011). This development
implies that values like consumerism, individual rights, economic efficiency and private initiative are
stronger today than a couple of decades ago. A policy re-orientation – or perhaps even an institutional
change - has taken place in the Swedish welfare state since the public sector is today to a larger extent
seen as mainly a service producer instead of an instrument of social transformation (and promoter of
social equality). This changes the role of the citizen from a passive service recipient to an actively
choosing service consumer. The citizens are thus expected to take responsibility over their welfare in
an active way by making good and informed (rational) choices according to their preferences.
The welfare program that is analysed in this paper, the primary health care system, builds on The Act
on System of Choice in the Public Sector (”Lagen om Valfrihet”, LOV) which was implemented by
the centre-right government in 2009 (government’s proposition 2008/09:29). The Act opens the
opportunity for the local municipalities to let private companies compete on equal terms with the
public sector organisations for the providing of welfare services within health care and social services.
The local authorities set the economic compensation given to the suppliers. The service is financed
publicly, through tax money.
The Act on System of Choice in the Public Sector can be characterised as a form of consumer’s choice,
which is defined by that there are at least two providers for citizens to choose between in a certain
service area (Edebalk and Svensson 2005). The general idea with consumers’ choice is that the
politicians uses the active choice making of citizens to organise the public services, instead of
deciding how these services should be organised from the top. The citizen’s own preferences and
interests affect which service providers will remain on the market. For consumer’s choice to create the
freedom of choice that is intended, it is necessary that there are several actors that compete for the
customers. The main motive for introducing consumers’ choice is to grant the citizens influence over
the welfare services, the alternative being that the state (on some level) decides on what service the
citizens get to use. To give citizens direct influence over the welfare state services is also put forward
as a democratic argument. Another argument for consumers’ choice is based on the assumption that
people are perfectly capable to decide for themselves and thus have a right to make choices when it
comes to welfare services (Kastberg 2010).
Since 2010 The Act on System of Choice in the Public Sector is applied in primary health care,

11
meaning that private and public providers of primary health care are allowed to establish in the
counties, which is the local level that is responsible for health care in Sweden. The county politicians
decide the terms and conditions that the health care providers are to fulfil, and every provider that
fulfils these conditions is allowed to compete with other providers for the patients. Every county
council is allowed to determine the economic terms, including how much money the providers get for
each patient and also if the economic replacement should be higher in some areas of the county in
order to encourage providers to establish there. The citizens then get the possibility to choose between
the public and private providers available in the county (proposition 2008/09:74). The share of health
care centres that are run by private companies have almost doubled since the reform started, partly
because some of the public health care centres have been privatized, but also because of new
establishments. Since the start of this reform, 208 new private health care centres have established,
mainly in the larger city areas.
Design and method
The design of this case study builds on two kinds of comparisons in order to draw conclusions about
the effects of empowerment. First, a comparison over time where public opinion is measured before
and after the introduction of the reform. Second, a comparison between groups based different
indicators of experienced empowerment which are assumed to mediate the effects of institutionalised
empowerment. The first indicator is variation in realistic exit options, where the fact that exit options
vary across Sweden is used to compare opinions between citizens that live in local communities with
good exit options to those who live in local communities with limited or no exit options. The second
indicator is if users of health care centres have made an active choice of health care centre or not. The
third indicator differs between those who have actually chosen to use exit options and those who have
not (see further below).
The effects are measured on two levels of opinions of welfare service. First, a policy-specific variable
that measures the opinion of primary health care service in the local community. Second, the effects
on the more general support of the restructuring of the welfare state service sector is measured.
In the analysis, both users and non-users of primary health care are included. Quite few do not use
health care centres at all (about 10 %), but it might be the case that users differ in their opinion from
non-users in this case since they have a direct experience from the welfare service in question. In the
tables measuring opinions over time, the results for only users are also presented to be able to assess
differences. In the rest of the analysis, differences are commented when the results for users deviate in
a way that is interesting for the results. Also, a division into user groups are included in the regression
analysis concerning contentment with health care.

12
The datasets used is the West Sweden SOM Survey from 2007, 2008 and 2010. This is a survey sent
to a random selection of citizens of West Sweden by the SOM institute, an independent survey
organisation at the University of Gothenburg. The region of West Sweden contains about 1,5 million
of the 9 million citizens of Sweden. The reason why I use West Sweden and not the nation-wide
survey is simply that in the West Sweden survey, the questions correspond better to what I need in
order to perform the analyses. For example, in this survey there are some questions directly related to
consumer’s choice in primary health care while in the national survey these questions are not asked.
That the survey do not cover the whole country is not too problematic, since many previous analyses
show that the results from West SOM-data is very similar to those generated by the nation-wide SOM-
surveys.
Before and after
Consumer’s choice was introduced (at the latest, in some regions during autumn 2009) in January
2010. This was marked for the citizens through information from the county council where citizens
were asked to choose among a list of health care centres. Information was also available through the
internet and since the reform was also discussed in media, there are good chances that citizens had
knowledge of the change.
In the analysis, data from the years 2007 and 2008 is used to measure attitudes before the reform and
from 2010 to measure attitudes after the reform. The year 2009 is excluded since the reform was
implemented in West Sweden in October that year, a short while before the survey was sent out to the
respondents. This makes it hard to interpret the answers since it is not possible to know if the
respondents’ answers refer to the old system of primary health care or the newly implemented one.
Since the access to health care already before the reform differed across the country, the division into
groups (see below) according to exit options is also used as a control variable to rule out the
possibility that the results depend on geographical differences and not the introduction of the reform.
Realistic exit options
Even though consumer’s choice in primary health care was introduced at the same time all over
Sweden, the exit options vary geographically. New health care centres have mainly been established in
the larger cities and the surrounding areas, while some regions have practically no new establishments.
This means that in some areas, exit options are realistic due to the presence of many alternatives, and
in some not since there simply are no more health care centres nearby.
This fact is in this case study used to vary exit options among the population. For this purpose, I have
noted the amount of health care centres in each local community at the start of 2012 (which roughly is

13
the same as in 2010 when the survey was sent out since the majority of the new health care centres
started in 2009 or 2010) and incorporated this information in the data set, which means that every
respondent is ascribed a value depending on their access to more than one health care centre. The
variable is categorized in three groups: 1) local communities with one health care centre or two health
care centres that is far from each other. 2) Local communities with two or sometimes three health care
centres. 3) Local communities with four or more health care centres. In category 1, the exit options
are none or very limited. In category 2, the exit options are present but if a person for example has
special preferences about opening hours or what kind of specialist doctors or nurses they need, the
choices are probably limited. In category 3, there should be enough exit options to be able not only to
exit and find a similar service, but also to choose from a range of different health care centres with
different specialities and services.
While coding this information, I have also looked at maps, to try and assess the distance from other
local communities with more or less health care centres. For example, local communities in the
vicinity of the larger cities are coded as second or third group since it is reasonable to assume that the
residents have the opportunity to choose from health care centres in the larger city even if there is only
one or two health care centres in the local community where they live. Still, a word of caution about
this categorization is that it might not always reflect the circumstances in terms of exit options for the
individuals since it is hard to assess how realistic it is to for example drive to the next town for a
health care centre.
Active choice
Citizens that use welfare service where the possibility to choose is given, can also choose to be active
or not. Being active might lead to a stronger empowerment effect than being passive by not
participating in the system. Also, it is reasonable to assume that the welfare service is more proximate
to those who actively participate which should increase the likelihood of effects on opinions. In the
analysis, I use a question that measures if the respondent have made an active choice of primary health
care or not, when the opportunity was first given in 2009/2010.
Using exit options
Another factor that could possibly be of importance for the effect that empowerment has is if the
health care centre clients actually have used the possibility to exit or not. Those who have used the
option to choose another health care centre if they are not happy with the original one have direct
experience of exit and it is therefore likely to have a more positive opinion of welfare service than
those who don’t have this experience. In the West Sweden Survey this is measured by asking the
respondents if they have re-made their choice of health care centre one or several times.

14
The dependent variables
At this stage I am limited to the existing data sets and the questions put there. This means that I have
looked for the questions regarding opinions on health care centres and also on welfare state
restructuring in general that is present in the West Sweden SOM datasets from 2007, 2008 and 2010.
The question that is closest to what I want to measure and also put in all data sets I want to use is the
one asking how content the respondents are with the primary health care service in their local
community. This question is a bit tricky to interpret, since contentment with the primary health care
centre could mean anything from liking the doctor you are going to that it is easy to get appointments.
But it could also mean that the respondents are happy with the organisation of primary health care
centres as a whole.
As indicators on the attitudes to the restructuring of the welfare state in general, I use three items in a
question that asks the respondents’ opinions on a number of suggestions that are present in the
political debate. The items are:
- letting private companies run elder care
- letting more of health care be provided by private actors
- invest more resources in independent (private) schools
The point of using these items is to capture opinions of the restructuring of the welfare state service
area in general, referring to the changes in who provides welfare (from public actors to a mix of public
and private actors). This is a way of measuring the more generalised effects of public policy on
opinion, although I’m not going beyond the welfare state. The reason is that this is a limited
investigation and also that since I only focus on one specific policy area and a reform that took place
very recently, it is maybe a bit far fetched to expect effects on even more general attitudes.
The results are continuously discussed and valued by including other variables and comparisons when
it is possible, as a way of strengthening or weakening the results. The analysis technique used is,
firstly, straightforward univariate and bivariate statistical analyses presented in tables and secondly,
multivariate OLS regression analyses in order to check the robustness of the results by including
relevant control variables (only for 2010).
As to the regression analyses for contentment with primary health care as a dependent variable, the
original ordinal scale variable is used. This is, of course, not unproblematic. But as the variable
includes five steps (from very content to very discontent) it can be assumed that the distance between
the values are roughly equal. One problem is the middle alternative, which is “neither content nor
discontent”. It may be the case that those choosing this alternative expresses indifference rather than
an actual opinion but as the question includes also the alternative “no opinion” (not included in the

15
analysis), this risk is after all quite small.
The attitudes towards privatization of health care, elderly care and schools are in the regression
analyses put together in an additive index as they are tightly correlated (Cronbach’s alpha = .859). The
control variables that are used in regressions are discussed below.
Results
In this section, the results from the statistical analysis are presented. First, the results from the analysis
of policy-specific attitudes are discussed, then the results from the analysis of the more general
attitudes towards privatization of welfare services.
Empowerment and policy-specific attitudes
The first section of the results deals with the policy-specific welfare attitude, contentment with
primary health care.
Before and after
Does the possibility to choose health care centre and to be able to re-make the choice if not happy
make citizens more content with primary health care? This question is investigated by analysing
contentment with primary health care in the respondent’s local community before and after the
implementation of consumer’s choice in October 2009.
Table 1: Contentment with primary health care centre service in local community, 2007-2008 and
2010. All respondents (users) Percent.
Year Content Neither content nor discontent
Discontent Sum percent/N
2007 60 (66) 22 (18) 18 (15) 100/2937 2008 63 (68) 21 (18) 16 (14) 100/2792 2010 72 (76) 18 (15) 10 (9) 100/2815
Comment: The question in the survey is: What do you think about the service in your local community on the following areas: primary health care.
Evidently, the proportion of West Swedes that is content with the primary health care is higher in 2010
than in the years before, at the same time as the discontent figure decreases. The same pattern goes for
both respondents in general and users, although users are generally more content with the service than
non-users. It is possible that this is a temporary or random variation between the years, but it is also
reasonable to assume that the consumer’s choice reform has had some effect on contentment since no
other significant reforms or other incidents have been taken place in the policy area during the time

16
period. The result from the West Sweden survey is strengthened by that the pattern looks the same
when the same analyses are performed on national data (based on a survey that was sent out to a
random selection of citizens in the whole country).
Realistic exit options
In table 2 the respondents are grouped according to realistic exit options in their local community.
Are those living in areas with good exit options more content with primary health care than those
living in local communities with none or limited exit options?
Table 2: Contentment with primary health care centre service in local community by realistic exit
option groupings, 2010.
None or limited exit options
Medium exit options Extensive exit options
Content 68 71 73 Neither content nor discontent
20 19 17
Not content 12 10 10 Sum percent/N 100/638 100/222 100/2812 Comment: The question in the survey is: What do you think about the service in your local community on the following areas: primary health care. The groups of exit options are categorized based on the number and vicinity of primary health care centres in the local communities.
Those with no or limited exit options are less content with the service than those living in areas where
there are medium or extensive exit options even though a majority also in this group is content.
Among users of primary health care, the differences are more distinct (70 percent in group with no
exit options as compared to 78 in group with extensive exit options). It is possible that the differences
between the groups that we see in 2010 is not a consequence of the differences in exit options that
comes from the implemented reform, but stems from the fact that there already before have been
differences in how content people are with primary health care in different parts of the country and
that these geographical variations correlates with the categorization into exit option-groups. For
example, the local communities of the larger cities and their surrounding areas are included in the
group with high exit options. These are areas where primary health care service was already before the
reform more developed than for example in most places in the northern part of Sweden. Varying exit
options in primary health care is thus not an entirely new phenomenon in Sweden.
An analysis shows that both in 2007 and 2008, there are differences in contentment with primary
health care between the groups, although smaller than in 2010. That the differences between the
groups are more distinct in 2010 compared 2007 and 2008 might after all mean that the exit options
does make a difference.

17
Table 3: The impact of exit options on contentment with primary health care, with control variables
(Unstandardised OLS estimates).
Variable B
None or limited exit options -.049
Extensive exit options -.138
Users/non-users .-.43***
Opinion of choice reform -.63***
Age .01***
Gender .08
Constant −16,947
Adjusted R Square .12
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: exit options is a dummy variable, where medium group is used as a base category. Users-non-users is a binary variable, where those who either use primary health care themselves or have a close relative that do are added in one group. Opinion of choice reform is a binary variable (like/dislike). Age is year of birth.
So, how do these results hold when relevant control variables are included? Since women are
generally more content with welfare service than men, and elder citizens more content than the
younger, gender and age are included. Additionally, earlier results show that users of a service
generally are more content with services than non-users, also this is included. Citizens who are
positive towards consumer’s choice in health care are probably more happy with the service than those
who are negative to the reform, a variable measuring respondents attitudes to consumer’s choice in
health care is therefore included.
As we can see in the table, differences in exit options are not significantly correlated to how content
citizens are with primary health care services: those who have many health care centres within close
distance are not more content than those that have one or two. Instead, age (the older the more content),
opinion about the choice reform in health care and if you use primary health care or not seem explain
some of the variation in content.
Active choice
The next question to be answered is if there is a difference in opinion of service between those that
made an active choice of health care centre and those who did not, when the consumer’s choice was
first implemented. As mentioned above, in the fall of 2009 all citizens in the region got a letter from
the council authorities with information about consumer’s choice and a list of health care centres to
choose from. A majority, 87 percent of the users of primary health care, chose to use this opportunity.
Table 4: Active choice and contentment with service in primary health care service in the local

18
community, 2010.
Active choice No active choice Content 74 60 Neither content nor discontent
17 26
Discontent 9 14 Sum percent/N 100/2196 100/376 Comment: The question in the survey is: What do you think about the service in your local community on the following areas: primary health care. The question used for groups of active choice is: Which health care centre did you choose the first time you had the opportunity to choose? The alternative “made no active choice” is compared to the merged alternatives “chose the health care centre that was suggested” and “chose another health care centre than suggested”.
The table shows that those who have made an active choice of health care centre are more content with
the primary health care service in their local community (the result is statistically significant). A
majority of those who have not made an active choice are also content. This might mean that the
existence of choice is enough to be content – or simply that this is a group of respondents that had
been content also if the reform had not been implemented. Unfortunately, it is not possible to check
this by an analysis of previous years, since the question of active choice was for natural reasons not
included before the reform.
Table 5: The impact of active choice on contentment with primary health care, with control variables.
(Unstandardised OLS estimates).
Variable B
Active choice -.19**
Users/non-users .-.42***
Opinion of choice reform -.61***
Age .01***
Gender .087
Constant −15,377
Adjusted R Square .12
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: Active choice is a binary variable (active/not active). Users-non-users is a binary variable, where those who either use primary health care themselves or have a close relative that do are added in one group. Opinion of choice reform is a binary variable (like/dislike). Age is year of birth.
The regression analysis show that the differences we see in the bivariate analysis are still significant
when control variables are added: Those who have made an active choice of health care centre are
significantly more content with primary health care service centre than others. A note of caution is that
the causal direction is not self-evident here. Those content with the service might be more inclined to
participate actively than those who are not content. An analysis shows that this is the case: 88 % of
those who are content with the service have made an active choice, compared to 79 % of those who
are not content.

19
Using Exit Options
Are the primary health care clients who actually have used the opportunity to exit more content with
the service in primary health care than those who have not? In this case, using the opportunity to exit
refers to those who did make an active choice at first, but later decided to leave the health care centre
they chose for another one. Citizens are allowed to change their minds any number of times, although
the number of people who had switched health care centre more than once was quite small (34) when
the survey was answered compared to those who changed once (426).
Table 6: contentment with primary health care service in local community, by exit or no exit, 2010
No Exit Exit Content 73 67 Neither content nor discontent
18 17
Discontent 9 16 Sum percent/n 100/2328 100/413 Comment: The question in the survey is: What do you think about the service in your local community on the following areas: primary health care. The question used to categorize exit groups is: Did you during the last year choose a new health care centre? No/Yes, once/Yes, more than once. The two “yes”-alternatives are merged in the table.
The difference between the groups is small but significant. In this case there is obviously a risk of
reversed causality: those not happy with the service over all, almost certainly use the possibility to
change health care centre more frequently than those that were content from the start. It may be the
case that their answer relates to their experience from the first chosen health care centre. An analysis
shows that those who are not content with the primary health care more often chooses to exit (22 vs
16 %). The result is confirmed in the regression, where those who have used the option to exit are not
more content than those who have not (table 7).
Table 7: The impact of exit on contentment with primary health care, with control variables.
(Unstandardised OLS estimates).
Variable B
Used exit-option -.11
Users/non-users .-.44***
Opinion of choice reform -.65***
Age .01***
Gender .085
Constant −14,915
Adjusted R Square .12
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: exit options is a dummy variable, where medium group is used as a base category. Users-non-users is a binary variable, where those who either use primary health care themselves or have a close relative that do are added in one group.

20
Opinion of choice reform is a binary variable (like/dislike). Age is year of birth.
Empowerment and attitudes to the restructuring of the welfare state
The second part of the result section deals with the assumption that people with experience from
empowerment are more positive to the restructuring of the welfare state in terms of private actors in
the welfare service arena than others. But first, a comparison of the attitudes over time to assess if the
implementation of the consumer’s choice seems to have made any differences in attitudes to similar
policy in elder care, health care and schools. Privatization is here used as an indicator of the ongoing
restructuring of the welfare service sector.
As above, OLS regressions are used for the purpose of checking whether the bivariate results still exist
when control variables are added. A vital variable to add is left-right orientation since privatization of
welfare is a highly ideological issue in Sweden (Bendz 2011). Also, educational level (where those
with higher education is generally more positive) and age (younger more positive than older) are
included as well as opinion about the choice reform (positive opinions on the choice reform in primary
health care and privatization in general is likely related). The attitudes to privatization are, as
explained in the above section, put together in an additive index.
Before and after
In the question, respondents are asked to give their opinions about a number of suggestions or
statements that are present in the political debate in Sweden in terms of positive or negative. In the
table, only the proportion of those that are positive towards the suggestions is showed.
Table 8: Attitudes to suggestions about privatization of welfare services, 2007, 2008 and 2010.All
respondents (users of primary health care) Proportion of positive answers.
Year 2007 2008 2010 Health care 29 (29) 29 (27) 30 (30) Elderly care 25 (25) 26 (24) 26 (25) Independent schools
22 (21) 23 (22) 23 (22)
Comment: The statements in the survey question have the following formulations. Health care: Letting more of health care be provided by private actors. Elderly care: Letting private companies run elderly care. Independent schools: invest more in independent schools.The sum of respondents for health care for respective year is 3242, 3065, 3080. Elderly care 3248,3066,3091. Independent schools 3228, 3079,3043.
The attitudes to the suggestions of privatisation of welfare service have hardly changed at all during
the years included in this analysis, for any of the three areas. Thus, the conclusion is that introducing
consumer’s choice in primary health care does not seem to have any consequences for the general
attitudes to related welfare policy, at least not over time. In an analysis of attitudes to privatisation in

21
Sweden over a longer time period, Nilsson (2007) concludes that the support for privatization in the
health care sector have increased since the middle of the 1990’s to 2006. Although this trend seem to
have stagnated during the last years according to the table above, the small increase in the proportion
that are positive towards privatization of health care in 2010 might be a part of this long term trend
rather than the implementation of consumer’s choice.
Realistic exit options
To save some space, the results for all three items are also here gathered in one table, only showing the
share of positive respondents.
Table 9: Attitudes to suggestions about privatization of welfare services by exit options in primary
health care, 2010. Proportion of positive answers.
None or limited exit options
Medium exit options Extensive exit options
Health care 28 25 32 Elderly care 23 17 28 Independent schools 20 23 23 Comment: The statements in the survey question have the following formulations. Health care: Letting more of health care be provided by private actors. Elderly care: Letting private companies run elderly care. Independent schools: invest more in independent schools. The groups of exit options are categorized based on the number and vicinity of primary health care centres in the local communities.The sum of answers is about 718 in group 1, about 255 in group 2 and about 2300 in group 3.
The results show that residents in local communities with good exit options, are more positive towards
letting health care be provided by private actors than those living in local communities with no or
limited exit options. Also the differences between exit-groups for the attitudes towards letting private
companies run elderly care shows the same pattern. The results concerning independent schools do not
show any significant differences between groups.
To check these results, we again take a look at the corresponding results from 2007 and 2008. For
health care, results from 2007 and 2008 show a similar pattern (although not significant for 2008).
Compared to 2007, the differences between the groups are a bit more distinct in 2010, where the share
that is positive in high exit option communities have increased. For elderly care, the pattern we see in
the table above is about the same in 2007 and 2008.
The tentative conclusion is that differences between the groups seem to have more to do with other
factors than with positive experiences from exit options in primary health care. A look at the
regression analysis confirms this conclusion: ideological orientation as well as age and opinion about
health care choice reform contributes to explain variation in privatization opinions, but not exit options.

22
Table 10: The impact of exit options on attitudes towards privatization of welfare services, with
control variables. (Unstandardised OLS estimates).
Variable B
None or limited exit options .11
extensive exit options -.45
Left-wing 1,8***
Right-wing --2,1***
Opinion of choice reform -.95***
Educational level .05
Age -.03***
Constant −65,139
Adjusted R Square .33
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: exit options is a dummy variable, where medium group is used as a base category. Left-right orientation is a dummy variable with neither left nor right as a base category. Opinion of choice reform is a binary variable (like/dislike). Age is measured as year of birth. Educational level is a binary variable with high/low education. Privatization is an index consisting of attitudes to privatization of health care, elder care and independent schools.
Active choice
Also in the table below, the share of positive respondents are presented for each item.
Table 11: Attitudes to suggestions about privatization of welfare services by activity, 2010. Share of
positive to the suggestions.
Active Not active Health care 31 25 Elderly care 26 24 Independent schools 23 21 Comment: The statements in the survey question have the following formulations. Health care: Letting more of health care be provided by private actors. Elderly care: Letting private companies run elderly care. Independent schools: invest more in independent schools. The question used for groups of active choice is: Which health care centre did you choose the first time you had the opportunity to choose? The alternative “made no active choice” is compared to the merged alternatives “chose the health care centre that was suggested” and “chose another health care centre than suggested”. N for the active group is about 2426, for the not active group about 450.
As regards attitudes towards privatizing more of the health care sector, the results in the table show
that the active choosers are more positive than those not active. For the other items, there is no
difference between groups.

23
Table 12: The impact of active choice on attitudes towards privatization of welfare services, with
control variables. (Unstandardised OLS estimates).
Variable B
active choice -.06
Left-oriented 1,7***
Right-oriented --2,3***
Opinion of choice reform -1,0***
Educational level -.16
Age -.03***
Constant 64,670
Adjusted R Square .33
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: Active choice is a binary variable (active/not active). Left-right orientation is a dummy variable with neither left nor right as a base category. Opinion of choice reform is a binary variable (like/dislike). Age is measured as year of birth. Educational level is a binary variable with high/low education. Privatization is an index consisting of attitudes to privatization of health care, elder care and independent schools.
The regression analysis show the same pattern as for exit groups above, empowerment in terms of
choosing actively do not have a significant effect for opinions about privatization when controlling for
other variables. Left-right orientation show a significant effect, as do age and opinion about choice
reform.
Using Exit Options
How do the attitudes to the welfare service policy look for those who have chosen to use the exit
opportunities in the primary health care system?
Table13: Attitudes to suggestions about privatization of welfare services by exit, 2010. Proportion of
positive answers.
Not exit Exit Health care 29 37 Elderly care 25 32 Independent schools 22 28 Comment: The statements in the survey question have the following formulations. Health care: Letting more of health care be provided by private actors. Elderly care: Letting private companies run elderly care. Independent schools: invest more in independent schools. The question used to categorize exit groups is: Did you during the last year choose a new health care centre? No/Yes, once/Yes, more than once. The two “yes”-alternatives are merged in the table. N for not -exit-group is about 2659, for exit-group about 460.
As is seen in the table, there is a distinct difference between the groups on all three items, but
especially regarding the privatization of health care. Those who have experience from using exit
opportunities are clearly more positive towards privatization in other areas. Thus, it seems like the
24
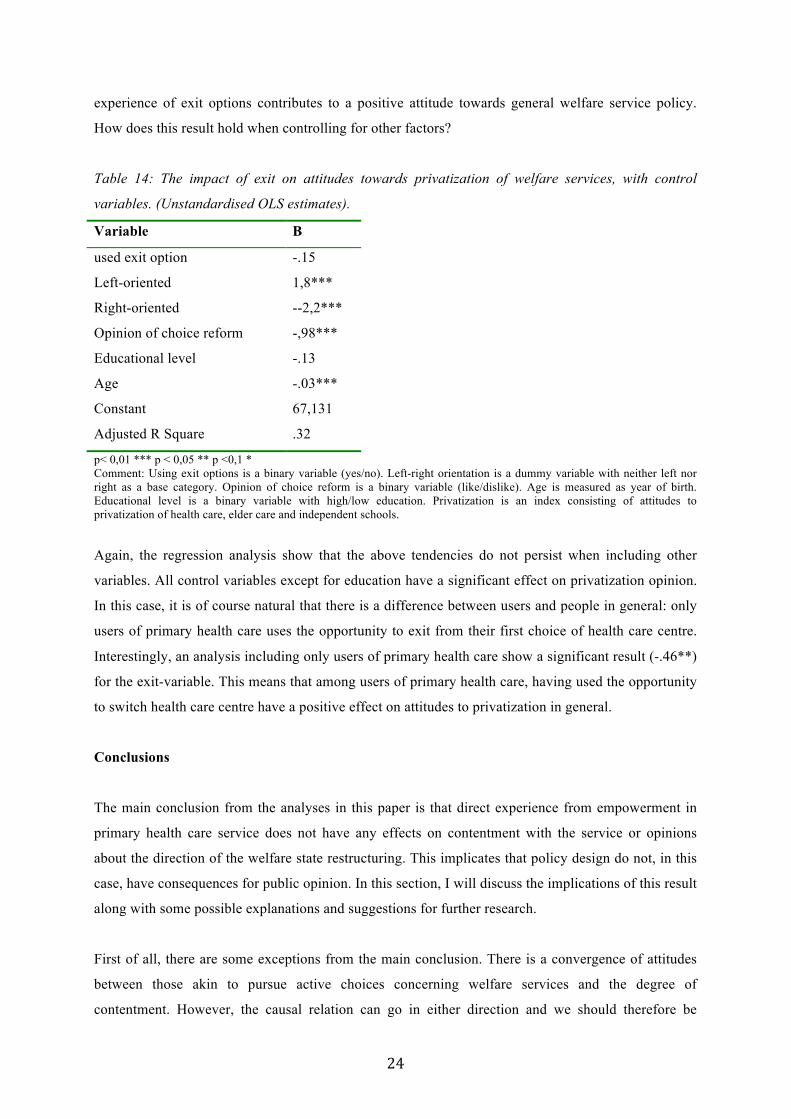
experience of exit options contributes to a positive attitude towards general welfare service policy.
How does this result hold when controlling for other factors?
Table 14: The impact of exit on attitudes towards privatization of welfare services, with control
variables. (Unstandardised OLS estimates).
Variable B
used exit option -.15
Left-oriented 1,8***
Right-oriented --2,2***
Opinion of choice reform -,98***
Educational level -.13
Age -.03***
Constant 67,131
Adjusted R Square .32
p< 0,01 *** p < 0,05 ** p <0,1 * Comment: Using exit options is a binary variable (yes/no). Left-right orientation is a dummy variable with neither left nor right as a base category. Opinion of choice reform is a binary variable (like/dislike). Age is measured as year of birth. Educational level is a binary variable with high/low education. Privatization is an index consisting of attitudes to privatization of health care, elder care and independent schools.
Again, the regression analysis show that the above tendencies do not persist when including other
variables. All control variables except for education have a significant effect on privatization opinion.
In this case, it is of course natural that there is a difference between users and people in general: only
users of primary health care uses the opportunity to exit from their first choice of health care centre.
Interestingly, an analysis including only users of primary health care show a significant result (-.46**)
for the exit-variable. This means that among users of primary health care, having used the opportunity
to switch health care centre have a positive effect on attitudes to privatization in general.
Conclusions
The main conclusion from the analyses in this paper is that direct experience from empowerment in
primary health care service does not have any effects on contentment with the service or opinions
about the direction of the welfare state restructuring. This implicates that policy design do not, in this
case, have consequences for public opinion. In this section, I will discuss the implications of this result
along with some possible explanations and suggestions for further research.
First of all, there are some exceptions from the main conclusion. There is a convergence of attitudes
between those akin to pursue active choices concerning welfare services and the degree of
contentment. However, the causal relation can go in either direction and we should therefore be

25
careful not to draw too strong inferences on this possible exception to the general rule. But still, if the
direct experience of empowerment in terms of active participation in the program generates more
happiness with public service, then active participation might be a factor contributing to legitimacy for
the public sector. Also, active participation is a prerequisite for exit-mechanisms to work: if citizens
do not make active choices of service provider, then they will hardly be able to show the decision-
makers their opinion by either staying with an alternative or leave it.
The other significant result found was that among users of primary health care, there is an effect of
experience of exit on opinions of privatisation. Exit is a rather powerful way for citizens to make their
voice heard between elections and because of that a democratic tool in order to gain influence on
politics. If the mechanism works properly, citizens who are discontent with the welfare service
provided will exit and choose another alternative, thereby signalling their preferences to the politicians.
The amount of people who have used exit is this far rather small, since consumer’s choice in primary
health care is still new. It is quite safe to assume that this number will increase over time, not
necessarily only because people are discontent with their primary care but since people move or
change other life circumstances which might affect their choice of health care centre. It would thus be
interesting to re-make the analyses when there are a greater number of people to analyse.
An argument for implementing consumer’s choice is to give welfare users influence over the service,
foremost by freedom of choice and exit. For exit to be possible citizens must be willing to participate
in the system (being active) and there must be enough realistic exit options to choose from. As the
results in this paper show, neither of these factors have in itself effects on welfare opinion as measured
here. But since they are necessary conditions for the actual action of exiting, they are still important
for the functioning of democracy. An interesting question to elaborate on would be if those who have
experience from active participation in one program were more inclined to participate in other
programs. Since those who are positive towards privatization of welfare services tend to be more
active, positive experiences from a consumer’s choice model might spill over into more active citizens.
If tipping the power balance towards the citizens in one welfare service would have generated positive
responses also in other areas, this might have created a policy feedback mechanism that contribute to
reinforce the general policy change of the Swedish welfare service sector as described in the paper,
making the restructuring hard to reverse since the policy itself generates public support (c f Campbell
2003). The results from this study show that this kind of effect is unlikely in this case, at least as a
consequence of one reform in one policy area. An interesting question that could not be answered with
the presently available empirical material is what would happen if citizens got experience from
empowerment in several welfare service areas: would this have a stronger effect on opinions of the

26
general restructuring policy?
An argument in the paper, following research from for example Soss (1999) and Soss & Schramm
(2007), is that welfare state policy is a most likely-case for trying policy feedback-effects and also,
that the case that is analysed in this paper is particularly likely to generate effects since it is both
visible and proximate to the citizens. Also, it might be argued that Sweden as a country is an
especially interesting case because of it’s traditionally very extensive public sector that almost every
citizen meets frequently during their lifetime, which also means that the ongoing restructuring of the
welfare service sector have tangible consequences for the citizens. So, how come that the results in
this paper show very few effects? To conclude this section, I will briefly discuss some possible
explanations for this and also suggest some ways forward.
First, it might be the case that the implementation of consumer’s choice in primary health care is not
significant enough to create effects on public opinion: high visibility and proximity is not enough. But
it might also be the case that I’m barking up the wrong tree when it comes to where the effects should
be found, that there in fact are effects on public opinion and/or behaviour in other ways than
contentment with service and attitudes to privatization.1
Another explanation for the results is that people do not transfer direct experiences of empowerment
into opinions, either in general or just in this particular case. Is empowerment a mechanism that is
strong enough to create a link between welfare state experiences and public opinion? Since this have
been tested and proven in previous research, it is likely that the zero result is due to this particular case,
not to the theory in general. A related issue to be mentioned here is the possibility that the assumption
that direct experiences of empowerment have a stronger effect on public opinion than institutionalised
empowerment in general, is not that fruitful. But it could also be argued that this assumption should be
tried in more cases and with other designs before it is discarded. After all, the significant result
discussed above concerning the effects of experiencing exit is interesting enough to be further
elaborated on. A suggestion for further research is to try the effects of experience of empowerment in
cases where the group of “exiters” are larger and also in other welfare service programs than health
care, as well as in other institutional contexts and countries. Of course, the results could also be
attributed to methodological weaknesses such as a too “blunt” instrument for measuring opinions of
how primary health care works (contentment is, as mentioned above, not ideal), the use of statistical
technique or the fact that there are quite few respondents in some groups.
Consumer’s choice in primary health care is only one reform of many that puts new demands on the 1 During the process, I have analysed effects on for example trust (following previous research, e g Kumlin

27
Swedish citizens and contributes to change the character of the welfare state. The general research
question about the policy feedback effects of empowerment on public opinion could be more fully
answered if more aspects of the changes in the Swedish welfare sector were included. Also, it would
be interesting to extend the analysis to include more dependent variables on different levels. In
previous research, policy feedback effects are found on a very broad range of possible human
reactions to policy. To further develop the research area, it would be interesting to classify different
effects according to their distance from the policy, from policy-specific to generalised opinions on
how well government functions. This also raises questions such as how “far” in time and space from a
policy it is interesting and relevant to measure effects. In this paper, effects are measured quite close in
time from the policy change. This might for example mean that the public opinion reactions to the
policy in focus in this paper will change over time. The analysis will hopefully be more elaborated and
developed in this direction further on.
As mentioned in the introduction, the general idea that motivates this paper is that the changing
character of the welfare state may have implications for the relationship between state and individual.
With empowering comes responsibility. With the restructuring of welfare services, the individual
citizen gets more responsible for the quality and content of his or her own welfare than in the
traditional Social Democratic welfare model. What does this mean for how the citizen views his or her
relationship to the government? In further research, this question could be elaborated by extending the
analysis in the paper to include not only opinions and attitudes on specific welfare policy, but also on
how the relationship between individual and government is perceived by people in general and by
those who have direct experiences from empowerment. A related question is if and how a change in
the relationship between state and individual would affect the character of the Social Democratic
Welfare State and the consequences for how this kind of regime would be viewed in a comparative
perspective.

28
References
Bendz, Anna (2011): ”Västsvenskarna och vårdvalet”. I: Nilsson, L (red) Västsvensk demokrati i tid och rum. SOM-institutet, Göteborgs universitet. Bendz, Anna (2011): Providing Welfare. The Importance of Public or Private actors in Welfare State Regimes. Conference paper presented at MPSA Yearly Conference, Chicago, March 31 – April 04 2011 and ECPR Reyjkavik, august 25-27 2011. Bendz, Anna (2012): ”Vårdvalet i Västsverige”. In: Bergström, A (ed) Västsvensk vardag. Göteborg: SOM-institutet. Brooks, C; Manza, J (2006): “Why Do Welfare States Persist?” The Journal of Politics, Vol 68, No.4. Campbell, A (2003): How Policies Make Citizens: Senior Political Activism and the American Welfare State. Princeton, NJ: Princeton University Press. Edebalk, PG; Svensson M (2005): Kundval för äldre och funktionshindrade i Norden. Tema Nord 2005: 507 Esping-Andersen, G (1990): The Three Worlds of Welfare Capitalism. Cambridge: Polity Press Hall, P; Taylor, R (1996): ”Political Science and the three New Institutionalisms”. Political Studies 44:4. Hartman, Laura (2011) (red): Konkurrensens konsekvenser. Vad händer med svensk välfärd? Stockholm: SNS Hirschman, A (1970): Exit, Voice and Loyalty: Responses to Decline in Firms, Organizations, and States. Cambridge,MA: Harvard University Press. Hoff, J (1993): “Medborgerskap, brukerrolle og magt.” In: Andersen, J; Christensen, A-D; Langberg, K; Siim, B, Torpe Lars (eds): Medborgerskab – Demokrati og politisk deltagelse. Viborg: Systeme Hood, C (1991): ”A Public Management for All Seasons”? Public Administration, Vol 69, pp 3-19. Johansson, F; Nilsson, L; Strömberg, L (2001): Kommunal demokrati under fyra decennier. Liber. Jordan (2010): “Institutional Feedback and Support for the Welfare State: The Case of National Health care. “Comparative Political Studies, Vol 43, No 7. Kastberg, G (2010): Vad vet vi om kundval - en forskningsöversikt. Stockholm: Sveriges kommuner och landsting Kumlin, S (2004): The Personal and the Political: How Personal Welfare State Experiences Affect Political Trust and Ideology. New York: Palgrave MacMillan Kumlin, S (2010): “Dissatisfied Democrats, Policy Feedback and European Welfare states, 1976 – 2001.” Quality of Government Institute, University of Gothenburg. Working paper Series 2010:4. Larsen, C A (2007): “How Welfare Regimes Generate and Erode Social Capital: The Impact of Underclass Phenomena.” Comparative Politics vol 40, No 1. Lindbom, A (2001): ”Dismantling the social democratic welfare model? Has the Swedish Welfare

29
State lost its defining character?” Scandinavian Political Studies, Vol 24, No 3, 171-193. Mau, S (2003): The Moral Economy of Welfare States. Britain and Germany compared. Routledge Mettler, S; Soss, J (2004): “The Consequences of Public Policy or Democratic Citizenship: Bridging Policy Studies and Mass Politics.” Perspectives on politics 2:1 Möller, T (1996): Brukare och klienter I välfärdsstaten. Om missnöje och påverkansmöjligheter inom barn-och äldreomsorg. Stockholm: Publica Nilsson, L (2007): ”Trovärdig välfärdspolitik?” In: Holmberg, S; Weibull, L (eds): Det nya Sverige. Göteborgs universitet, SOM-institutet. Nilsson, L (2008): ”Välfärd, service och demokrati”. In: Nilsson, L; Johansson, S (eds): Regionen och flernivådemokratin. Göteborgs universitet, SOM-institutet. Pierson, Paul (1993): “When Effect Becomes Cause. Policy Feedback and Political Change”. World Politics, vol 45, nr 4, pp 595-628 Rothstein, B (2010): Vad bör staten göra. Stockholm:SNS Skocpol, T (1992): Protecting Soldiers and Mothers: The Political Origins of Social Policy in the United States. Cambridge: Harvard University Press. Sen, A (1988): “Freedom of Choice. Concept and Content.” European Economic Review 32. Solevid, M (2009): Voices from the Welfare State. Dissatisfaction and Political Action in Sweden. University of Gothenburg, Dep of Political Science. Soss, Joe (1999): “Lessons of Welfare: Policy Design, Political Learning, and Political Action.” American Political Science Review, vol 93, no 2. Soss, Joe; Schram, S F (2007): “A Public Transformed? Welfare Reform as Policy Feedback”. American Political Science review, vol 101, no 1. Svallfors, S (2010): “Policy feedback, generational replacement and attitudes to state intervention: Eastern and Western Germany, 1990-2006.” European Political Science Review 2:1 Sörensen, Eva (1997): “Democracy and Empowerment.” Public Administration, vol 75, autumn 1997. Taylor-Gooby, P (2004): ”Open markets and welfare values. Welfare values, Inequality and Social Change in the Silver Age of the Welfare State”. European Societies, Vol 6, No 1, 29-48.

30