
Welcome to the NE QIN-QIO Webinar! Our presentation will...
46
Welcome to the NE QIN-QIO Webinar! Our presentation will begin shortly. Please dial in to the audio line by calling 888-830-8905 Passcode: 519600
Transcript of Welcome to the NE QIN-QIO Webinar! Our presentation will...

Welcome to the
NE QIN-QIO Webinar!
Our presentation will begin shortly.
Please dial in to the audio line by calling
888-830-8905
Passcode: 519600

Lynn McNicoll, MD Hospital and Nursing Home Consultant
Healthcentric Advisors of Rhode Island
Associate Professor of Medicine
Alpert Medical School of Brown University
Division of Geriatrics and Palliative
Medicine 2

The Motivation…
3

Disclosures
None
4

Acknowledgements
AHRQ CUSP Toolkit
http://www.ahrq.gov/professionals/quality-patient-safety/cusp/index.html
Armstrong Institute for Patient Safety and Quality faculty slides
www.onthecuspstophai.org
TeamStepps Department of Defense
http://teamstepps.ahrq.gov/
5

Learning Objectives
Participants will be able to:
1. Explain CUSP impact on safety
2. List CUSP Components
3. Describe how a regional organization (NE QIN-QIO) can support Hospital CUSP efforts
6
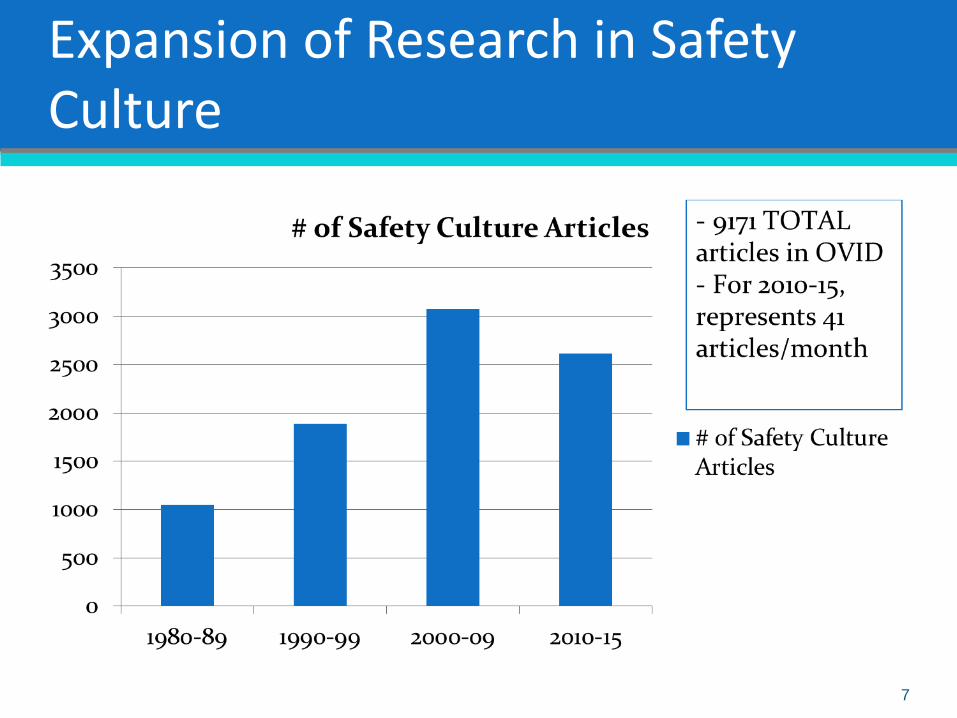
Expansion of Research in Safety Culture
7
Interventions to Promote Safety Culture: Systematic Review
3679 articles 162 full review33 included
8 = multi-faceted interventions
20 included team-training, communication tools
8 included executive walkrounds
29 significantly improved safety culture survey scores or outcomes
Limitations: strength of evidence was low and most studies are pre-post evaluations of low to moderate quality
“Evidence ‘suggests’ that interventions can improve perceptions of safety culture and potentially reduce patient harm”
8 Weaver, et al Annals of Int Med 2013: 158(5);369

HAI’s and CUSP
CUSP has been traditionally implemented in ICU
Literature is most supportive of ICU and specifically CLA-BSI
On the CUSP: Stop BSI
On the CUSP: Stop CAUTI
HAI’s are not limited to ICU (especially SSI, CAUTI, CLA-BSI), i.e. HAI occur on surgical and medical units throughout the hospital
CUSP is one strategy to help create a culture of safety to help prevent HAI’s
9
Has your hospital participated in ANY of the following CUSP initiatives?
a) ICU Collaborative
b) On the CUSP: Stop BSI
c) On the CUSP: Stop CAUTI
d) 2 or more of the above
e) None of the above
10
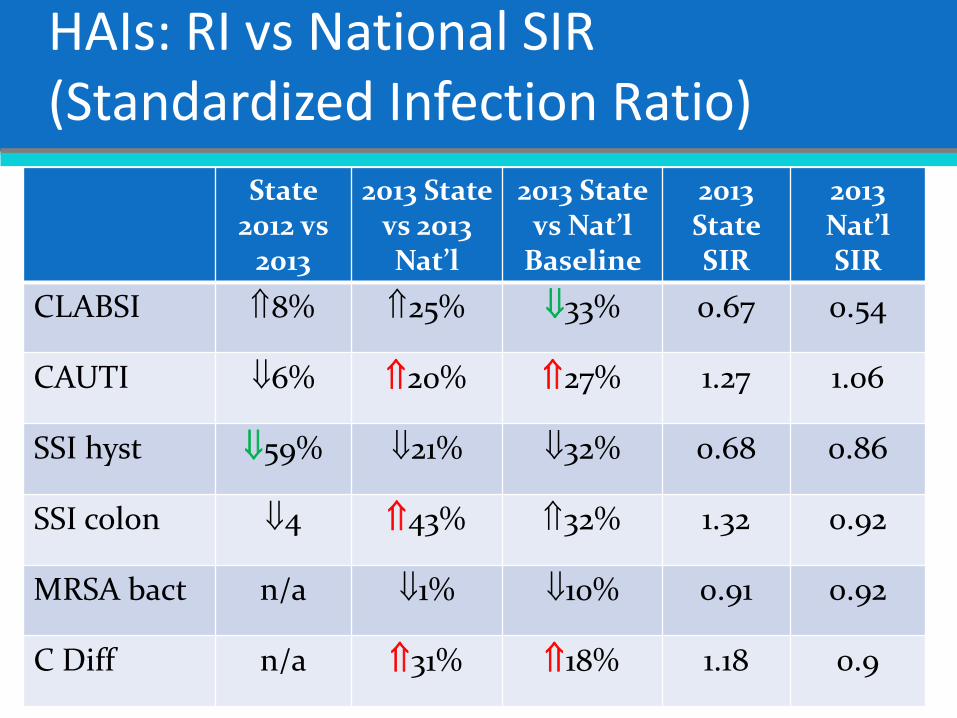
HAIs: RI vs National SIR (Standardized Infection Ratio)
11
State 2012 vs
2013
2013 State vs 2013 Nat’l
2013 State vs Nat’l
Baseline
2013 State SIR
2013 Nat’l SIR
CLABSI 8% 25% 33% 0.67 0.54
CAUTI 6% 20% 27% 1.27 1.06
SSI hyst 59% 21% 32% 0.68 0.86
SSI colon 4 43% 32% 1.32 0.92
MRSA bact n/a 1% 10% 0.91 0.92
C Diff n/a 31% 18% 1.18 0.9

What are the foundational elements of CUSP?
Focus on systems, not individuals
Value communication and teamwork
Emphasize infrastructure and support
Accept responsibility for the systems in which we work
Recognize that culture is local
Respect transparency
12

The 4E’s Principle
1. Engage with stories, show baseline and benchmarking data
2. Educate staff on evidence
3. Execute
Standardize: foley removal protocol/order set
Create independent checks: Create BSI checklist
Empower any providers to ‘stop the line’
Learn from mistakes
4. Evaluate
Provide updated and accurate results
Do analysis of deficits
13

How does CUSP Contribute to a Culture of Safety?
Designed to improve safety culture and help staff learn from mistakes
Integrates safety practices into the daily work of a unit or clinical area
Provides a scalable intervention
Can be implemented throughout the hospital or organization
Draws wisdom from frontline staff to fix hazards
Creates the forum necessary to speak up
Empowers staff to improve safety culture
14

What is CUSP?
Comprehensive Unit-Based Safety Program
Steps:
1. Evaluate your culture
2. Understanding the Science of Safety
3. Assembling a team
4. Implement teamwork and communication
5. Identify and learn from defects
6. Engage senior executive members
15

CUSP Step 1: Evaluate your culture
Tools to help evaluate the domains of a culture of safety – assesses safety CLIMATE – shared perception or attitude about the norms, policies, and procedures related to patient safety in a snapshot in time
SAQ – Safety Attitude’s Questionnaire
Most are using AHRQ Hospital Survey on Patient Safety Culture
Can measure, create action plan for addressing weak areas, then re-measure (usually annually or biannually)
RI ICU Collaborative Example …
16

RI State Aggregate SAQ Domain Improvement Trends
Ave
rage
Pe
rce
nt P
erc
ep
tio
n
17

Is your hospital currently administering any type of Safety Climate Survey?
a) SAQ: Safety Attitudes Questionnaire
b) AHRQ Hospital Survey on Patient Safety Culture
c) Home grown
d) None
e) Do not know
18

CUSP Step 2: Understanding the Science of Safety
Science of safety video on website is accessible and quite inspiring
www.onthecuspstophai.org
www.safercare.net
Josie King story/video/book as told by
Sorrel King
Standardize, create checklists
Eliminate steps
Learn when things go wrong
19

CUSP Step 2: Train Staff in the Science of Safety
Science of Safety Training principles:
Understand that safety is a property of systems
Identify principles of safe design (standardize, create independent checks, learn from mistakes)
Understand that teams make wise decisions with diverse and independent input – avoid blame culture
Recognize that principles of safe design apply to both technical and team work – speaking up when concerns arise and listening when others speak up!
20

CUSP Step 3: Establish a Team
Unit Level
Mostly engaged and passionate members
Consider including biggest critics (with the goal of converting them to your cause eventually)
21

Who is essential to the CUSP Team?
CUSP
Frontline Staff
Senior Hospital Executive
CUSP Coach
Physician Champion
CUSP Unit Champion
Nurse Manager
Patient Safety Coordinator/ Patient Safety
Officer
22

CUSP Step 4: Implement Teamwork Tools and Communication
Tools to improve:
1. Daily Goals Checklist
2. Morning Briefing
3. Observing Rounds
4. Shadowing another Profession
5. Culture debriefing Tool
23

1. Daily Goals
• What needs to be done for the patient to be discharged?
• What is the patients greatest safety risk?
• What can we do to reduce the risk?
• Can any tubes, lines, or drains be removed?
24
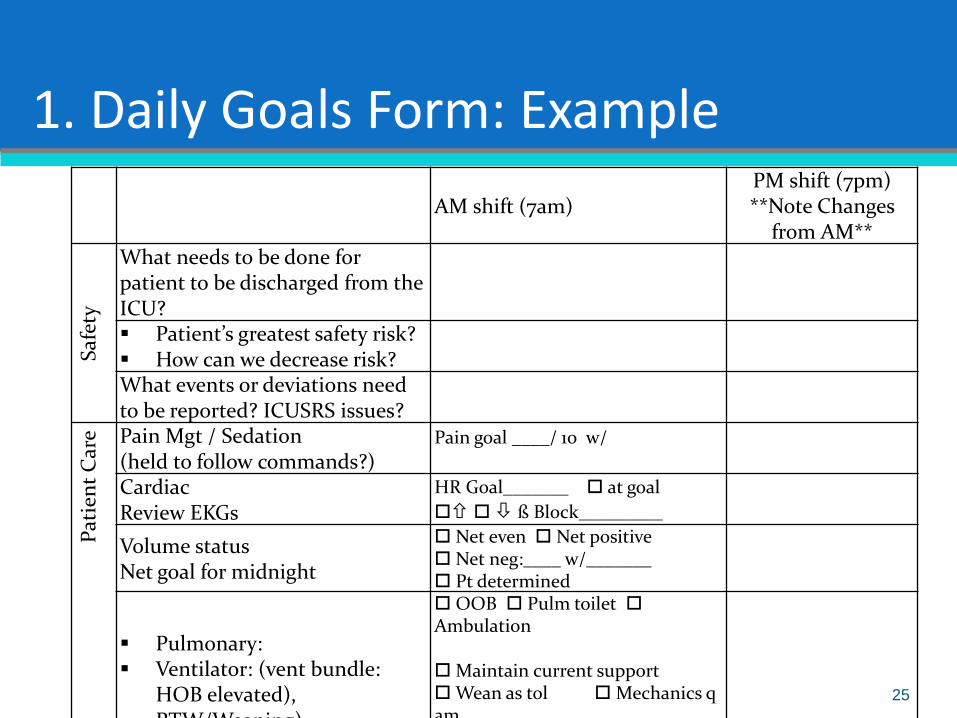
1. Daily Goals Form: Example
AM shift (7am) PM shift (7pm) **Note Changes
from AM**
Saf
ety
What needs to be done for patient to be discharged from the ICU?
Patient’s greatest safety risk? How can we decrease risk?
What events or deviations need to be reported? ICUSRS issues?
Pat
ien
t C
are Pain Mgt / Sedation
(held to follow commands?) Pain goal ____/ 10 w/
Cardiac Review EKGs
HR Goal_______ at goal
ß Block_________
Volume status Net goal for midnight
Net even Net positive Net neg:____ w/_______ Pt determined
Pulmonary: Ventilator: (vent bundle:
HOB elevated), RTW/Weaning)
OOB Pulm toilet Ambulation Maintain current support Wean as tol Mechanics q am FIO2 <_____ PEEP____ PS / Trach trial___h
SIRS/Infection/Sepsis Evaluation SIRS Criteria Temp > 38° C or < 36 ° C HR > 90 BPM RR > 20 b/min or PaCO2 < 32 torr WBC > 12K < 4K or > 10% bands
no current SIRS / Sepsis issues Known infection: PAN Cx Bld x2 Urine Sputum Other ABx changes; D/C AG Levels: Sepsis Bundle
Can catheters/tubes be removed?
Y N
GI / Nutrition / Bowel regimen (TPN line, NDT, PEG needed?)
TPN TF NPO
Is this patient receiving DVT/PUD prophylaxis?
DVT: Hep q8 / q12 / gtt PUD: PPI TEDS/SCDs H2B LMWH
Anticipated LOS > 2 days: TGC 3 days: fluconazole PO, KCl SS
TGC Fluc KCl N/A
Can any meds be discontinued, converted to PO, adjusted?
N/A D/C: PO: Renal: Liver:
To
Do
:
Tests / Procedures today N/A Scheduled labs N/A
AM lab needed CXR?
CMP BMP H8 Coags ABG Lactate Core 4 CXR Wed: Transferrin Iron Prealb 24h urine
Consultations Y N
Dis
po
siti
on
Is the primary service up-to-date?
Y N
Has the family been updated? Social issues addressed (LT care, palliative care)
Y N Y N N/A
25

2. AM Briefing
• Have a morning meeting with charge nurse and physician champion/attending
• Discuss work for the day
– What happened during the evening?
– Who is being admitted and discharged today?
– What are potential risks during the day, how can we reduce these risks?
– Patient scheduling? Equipment problems? Staffing? Provider Skill mix?
–Assign person to follow-up 26

3. Shadowing
• Follow another type of clinician doing their job for 2-4 hours
• Discuss with the team what they will do differently now that they walked in another person’s shoes
27

3. Shadowing Process Questionnaire
Were any healthcare providers difficult to approach?
Did one provider get approached more often for patients issues? Why?
Did you observe an error in transcription of orders?
Did you observe an error in the interpretation or delivery of an order?
Were patient problems identified quickly?
28
4. Culture Debriefing Tool
In RI, we referred to this as SAQ Action Plan
Pick an area that is poor from your safety climate survey
Convene a group to discuss the item and develop a plan on how to address
Use debriefing tool to develop improvement actions
Use active listening skills to guide the feedback but do not run the meeting
29

4. Culture Debriefing Tool: Discussion Form
Choose a statement to be discussed from the item
1. What does this statement mean to you?
2. How accurately does the unit score reflect your experience on this unit?
3. How would it look (i.e. what behaviors or processes would we see) on this unit if 100% of caregivers responded agree strongly with this item?
4. Identify at least one actionable idea to improve unit results in this area
30

RI Results- % change in SAQ Scores 2007 to 2008
-10
-5
0
5
10
15
20
25
30
Teamw
ork
Safety
Clim
ate
Job Satis
Stress R
ec
Work
ing C
ond
Perc o
f Mgm
t
Units withPlans
UnitswithoutPlans
31

RI Results- % change in BSI and VAP 2007 to 2008
-16
-14
-12
-10
-8
-6
-4
-2
0
2
4
6
CLA-BSI VAP
Units with
SAQAP
Units
without
SAQAP
Vigorito MC et al. Improving safety culture results in Rhode Island ICUs: lessons learned from the
development of action-oriented plans. Joint Comm J on Qual & Pat Safety. 2011;37(11):509-14 32

CUSP Step 5: Identify Defects
Defect = anything the you don’t want to happen again!
Staff Safety Assessment- all staff are asked to identify:
How will the next patient will be harmed?
What can we do to prevent that harm?
Use defects identified in the event reporting system
Use sentinel events
Near misses or ‘good catches’
Use results from your culture assessment scores and debreifings
33

CUSP Step 5: Learn from Defects Tool
1. What happened?
2. Why did it happen? Which factors contributed? 1. Patient factors (elderly, language, refusal)
2. Task (protocol, inaccurate results)
3. Provider (fatigue, personal issues)
4. Team (orders clearly communicated)
5. Training (follow protocol, lack of supervision)
6. IT (computer error/malfunction)
7. Local (insufficient staffing, skill mix, overloaded)
8. Institutional (financial resources)
3. How will you reduce the likelihood of this defect happening again?
34

Rank Order of Error Reduction Strategies
35
Forcing functions and constraints
Automation and computerization
Standardization and protocols
Checklists and double check systems
Rules and policies
Education / Information
Be more careful, be vigilant
Eliminate
Replace
Facilitate
Replace
Facilitate
Facilitate
Facilitate
Eliminate
Replace
Facilitate

Strength of Interventions Adapted from John Gosbee, MD, MS Human Factors Engineering
Weaker Actions Intermediate Actions Stronger Actions
Double Check Checklists/ Cognitive Aid Architectural/physical plant
changes
Warnings and labels Increased Staffing/Reduce
workload
Tangible involvement and
action by leadership in
support of patient safety
New procedure,
memorandum or policy
Redundancy Simplify the
process/remove
unnecessary steps
Training and/or education Enhance Communication
(read-back, SBAR etc.)
Standardize equipment
and/ or process of care
map
Additional Study/analysis Software
enhancement/modifications
New device usability
testing before purchasing
Eliminate lookalike and
sound-alikes
Engineering Control of
interlock (forcing
functions)
Eliminate/reduce
distractions
36

CUSP Step 6: Executive Partnership
Goal = bridge the gap between senior management and frontline staff
The role of the senior executive is one of advocacy and action in support of the unit’s safety efforts and to work to obtain needed resources for improvement efforts
The executive is encouraged to discuss safety issues, help to remove barriers, and implement improvement efforts
Brief frontline providers prior to visit
Affords opportunity to solicit staff input on errors, near misses and other safety issues
Identify, manage and track improvement projects
37
Executive WalkRounds Questions
Can you think of any incidents or adverse events that happened in the past few days that have resulted in prolonged hospitalization for a patient?
Can you think of patients we have harmed as a result of problems with how we deliver care?
What could leadership do to support you in providing safe patient care?
What changes could be made in this unit to promote patient safety more consistently?
38

CUSP Lessons Learned
Culture is local Implement in a few units, adapt and spread Include frontline staff on improvement team
Not linear process Iterative cycles Takes time to improve culture
Couple with clinical focus No success improving culture alone CUSP alone viewed as ‘soft’ Lubricant for clinical change
39
Seven Spreadly Sins
1. Start with large projects
2. Find one person willing to do it all
3. Expect vigilance and hard work to solve a problem
4. If a pilot project works then spread it unchanged
5. Require the person and team who drove the pilot project to be responsible for system-wide spread
6. Look at process and outcome measures quarterly
7. Expect marked improvement in outcomes early on without attention to process reliability
40

How can the NE QIN-QIO support Hospital CUSP efforts?
Use us (and each other) as a resource
Many members have done versions of CUSP or TeamStepps and we can learn from each other
NE QIN-QIO will provide reports on HAI data quarterly
We will continue to provide regional webinars on HAI, let us know which topic area you would like to hear about
41

Summary
CUSP components are straightforward but difficult to implement in non-ICU settings where the team is not well defined (especially physician members)
Introducing the Science of Safety and some tools (one at a time) is doable
Engage executive champion early and often
Improving the Culture of Safety is an ongoing challenge
42
a) Connecticut (CT)
b) Maine (ME)
c) Massachusetts (MA)
d) New Hampshire (NH)
e) Rhode Island (RI)
f) Vermont (VT)
g) Other
43
What state are you from?

a) One (1)
b) Two (2)
c) Three (3)
d) Four (4)
e) Five (5)
f) Six (6)
g) Seven (7)
h) Eight (8)
i) Nine (9)
j) Ten or More (10+)
44
How many people are watching on your computer or login information?
Questions?
45

References Andrews LB, Stocking C. An alternative strategy for studying adverse events in medical care. The Lancet. 1997;349(9048):309-
313.
Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Critical Care Medicine. 1995;23(2):294-300.
Leape LL, Cullen DJ, et al. Pharmacist participation on physician rounds and adverse drug events in the intensive care unit. JAMA. 1999;282(3):267-270.
Pronovost PJ, Dang D, Dorman T, et al. Intensive care unit nurse staffing and the risk for complications after abdominal aortic surgery. Eff Clin Pract. 2001;4:199-206.
Tucker AL, Edmondson AC. Why Hospitals Don’t Learn from Failures: Organizational and Psychological Dynamics that Inhibit System Change. California Management Review, 2003 ;45(2):55-72.
Reason J. Human Error. Cambridge, UK: Cambridge Univ Pr; 1990.
Bagian JP, Lee C, et al. Developing and deploying a patient safety program in a large health care delivery system: you can't fix what you don't know about. Jt Comm J Qual Improv. 2001;27:522-32.
Pronovost PJ, Holzmueller CG, et al. A practical tool to learn from defects in patient care. Jt Comm J Qual Patient Saf. 2006;32(2):102-108.
Pronovost PJ, Wu Aw, et al. Acute decompensation after removing a central line: practical approaches to increasing safety in the intensive care unit. Ann Int Med. 2004;140(12):1025-1033.
Vincent C. Understanding and responding to adverse events. New Eng J Med. 2003;348:1051-6.
Wu AW, Lipshutz AKM, et al. The effectiveness and efficiency of root cause analysis. JAMA 2008;299:685-87.
Berenholtz SM, Hartsell TL, Pronovost PJ. Learning From Defects to Enhance Morbidity and Mortality Conferences. Am J Med Qual. 2009;24(3):192-5.
46











![Belt QIN-QIO Webinar Significant change and discharges 2019 jm jb …€¦ · s ] ] µ E X } P n } Ç ] P Z î ì í õ Title Microsoft PowerPoint - Belt_QIN-QIO Webinar_Significant](https://static.fdocuments.in/doc/165x107/5fc18910c76f0c5f1044869d/belt-qin-qio-webinar-significant-change-and-discharges-2019-jm-jb-s-e-x-.jpg)





