Welcome to the Cardiac Rehabilitation Department€¦ · Anatomy Diagrams & Quiz 1. ... to a...
26
1 NHS Greater Glasgow and Clyde Acute Services Division Student Nurse Induction Programme Welcome to the Cardiac Rehabilitation Department Student’s Name………………………..…………………..……….. Mentor’s Name……………….………………Co-Mentor’s Name……………………….……….. Start Date:……………………… Length:………..weeks Finishes on:………………. Planned Assessment Dates – week commencing: • Initial assessment: ……………………… • Interim assessment: …………………….. • Interim assessment: …………………….. • Final assessment: …………………….. (Record & date all progress discussions in Clinical assessment document)
Transcript of Welcome to the Cardiac Rehabilitation Department€¦ · Anatomy Diagrams & Quiz 1. ... to a...

1
NHS Greater Glasgow and Clyde Acute Services Division
Student Nurse Induction Programme
Welcome to the Cardiac Rehabilitation Department
Student’s Name………………………..…………………..……….. Mentor’s Name……………….………………Co-Mentor’s Name……………………….……….. Start Date:……………………… Length:………..weeks Finishes on:……………….
Planned Assessment Dates – week commencing:
• Initial assessment: ………………………
• Interim assessment: ……………………..
• Interim assessment: ……………………..
• Final assessment: ……………………..
(Record & date all progress discussions in Clinical assessment document)

2
Contents Page 3: Cardiac Rehabilitation: Definitions Page 4: Team Members Page 5: Placement Profile Page 6: Preliminary Induction Page 7: Potential Learning Experiences Page 8: Anatomy Diagram and Quiz Page 10: Risk Factors for Heart Disease Page 12: Common Cardiac Terminology & Definitions Page 17: Phases of Rehabilitation Page 18: Secondary Prevention Page 18: Common Cardiac Tests Page 19: Cycle of Change Page 20: Role of Cardiac Rehabilitation Nurse Page 21: Abbreviations Page 24: References & Resources Page 25: Student Placement Diary Page 26: Placement Evaluation

3
Cardiac Rehabilitation: Definitions
“Cardiac rehabilitation is the process by which patients with cardiac
disease, in partnership with a multidisciplinary team of health professionals, are encouraged and supported to achieve and maintain
optimal physical and psychosocial health”.
SIGN 57 (2002)
“The rehabilitation of cardiac patients is the sum of activities required to influence favourably the underlying cause of the disease, as well as the best possible physical, mental and social conditions, so that they
may benefit by their own efforts preserve or resume as normal a place in the community”.
WHO (1993)

4
Team Members
Please complete with staff members from your area) Lead Nurse Manager Coordinator Staff Nurses Physiotherapists Dietician Clinical Psychologist Clerical / Secretarial Staff
5
Placement Profile for Area to be added
(Please cut and paste the Placement Profile for your site)

6
Preliminary Interview & Induction
Environment Area Geography
• Area layout • Area routine • Introduction to staff
Emergency Procedures
Fire Safety
• Phone No 2222 • Fire points & exits • Equipment • Evacuation procedure
Cardiac Arrest
• Phone No 2222 – state cardiac arrest and location
Highlight: • Arrest Trolley • Oxygen equipment • Suction Equipment
Incident Response • Phone No 1111 (GRI)
Policies and Procedures
Location of Manuals & Policies
Highlight: • Cardiac Rehabilitation
procedure manual • Uniform policy • Sickness/Absence policy • Smoking policy
Health & Safety
Highlight: • Risk assessment • Clinical waste • General waste • Laundry • Needle stick injury • Fault reporting
Duty Roster
50% Mentor Contact Time
• Shift Patterns & hours • Off duty negotiated &
documented in Assessment document
• Supernumerary status
Student Documentation Documentation must be available to the mentor during all student contact time
On-Going Record of Achievement (OAR) *must be reviewed within 5 days of placement (NMC) Action Plan Clinical Assessment Document (CAD) Time Sheets
• Review On-going Record of Achievement (previous CADs)
• Discuss learning needs/skills
• Agree action plan & time scale for review
• Establish level of performance to be reached (CAD)
• Discuss time Sheets to be completed weekly & signed by mentor
Signature- Student: ……………………………………. Date…………………
Signature- Mentor: ……………………………………. Date…………………

7
Potential Learning Experiences
Learning Experience Discussed/ observed
Observed / practised
Information Giving:
Increasing patients knowledge of their own health and well-being
Misconceptions and emotions
Health Promotion:
Greater understanding of the nature of Coronary Heart Disease
Prevention / modification
Health Education:
Adult learning strategies
Risk Stratification:
Monitoring of patient care to ensure appropriate treatment
Interpretation of cardiac investigations
Secondary Prevention Medication:
Knowledge of drugs and rationale
Needs Assessment:
Menu based cardiac rehabilitation
Outpatient assessments
Communication Skills:
Brief intervention
Motivational interviewing using cycle of change
Effective Multidisciplinary working (MDT)
Multidisciplinary Team Observed / Discussed role Physiotherapist
Dietician
Clinical Psychologist

8
Anatomy Diagrams & Quiz
1. Describe the heart and it’s location
2. Describe the blood flow through the heart
3. Describe the coronary circulation to the myocardium of the heart
4. Define Myocardial Infarction
5. Risk factors for Coronary Artery Disease fall into two groups, modifiable and un-modifiable: list the risk factors for each group
6. If a patient said to you that they did not believe that smoking damaged their health, how might you respond?
7. What factors may inhibit a person’s readiness to receive information in the early stages of recovery from post Myocardial Infarction?
8. Please label all the components of the heart in diagram 1
Diagram 1

9
9. Please label the Coronary circulation on diagram 2

10
Risk Factors for Heart Disease
• Risk factors are not the cause of heart attacks, but the contributors to a heart attack happening!
• They can be split into both non-modifiable and modifiable risks. • Non-modifiable, being the risks we have no control over and modifiable
being the lifestyle changes that we can adapt in order to reduce our risk.
Non-modifiable Risk Factors
Being Male
Family History of Coronary Heart Disease
Ethnicity
Age
Existing Coronary
Heart Disease
Non –
Modifiable Risk
Factors

11
Modifiable risk factors
How do the risk factors add up? Identifying risk factors is undertaken on an individualised basis. The more individual risk factors identified the greater the risk of coronary heart disease.
Psycho-social issues
Smoking
Physical inactivity
Hyper-tension
Diabetes mellitus
Obesity
Poor diet
Excess alcohol intake
High blood cholesterol
levels
Modifiable Risk
Factors

12
Common Cardiac Terminology & Definitions Acute Coronary Syndrome (ACS)
ACS is a term used to describe a pattern of chest pain symptoms, including both unstable angina and myocardial infarction. ACS results from the abrupt, total or subtotal obstruction of a coronary artery. Occlusion may be transient, and typically recurrent, or may be permanent. In most cases it is initiated by the rupture or erosion of a fatty plaque inside a coronary artery.
Angina Symptoms of heaviness or tightness in the chest, which may radiate to the arms, jaw, back or stomach. Angina is caused by ischaemia (inadequate blood flow) to the myocardium (heart muscle). Underlying coronary heart disease is the main cause of angina.
Angioseal A dissolvable device which is sometimes used to close the puncture site in the groin after angioplasty or stenting
Angioplasty with stenting (percutaneous intervention - PCI)
An invasive treatment used to widen a narrowed coronary artery. Performed percutaneously ‘through the skin’, usually using a radial or femoral artery. A catheter with a small, inflatable balloon it passed into a coronary artery at the narrow or blocked area. The balloon is gently inflated to squash the fatty plaque against the artery wall. In the majority of cases a coronary stent (a short tube of stainless-steel mesh) is then left in place to hold open the narrow artery.
Arrythmia A disorder of the heart rhythm
Atherosclerosis The build-up of fatty materials within the walls of the arteries
Atrial fibrillation (AF)
A type of arrhythmia in which the atria beat very rapidly. AF causes quite unpleasant palpitations and sometimes breathlessness. AF may lead to a clot forming in the heart
Body Mass Index (BMI)
A formula used to work out whether a person is overweight or obese. A BMI of over 25 is considered overweight, a BMI over 30 indicates clinical obesity
Bradycardia A slow heart rate, below 60 beats per minute (60bpm)
Cardiovascular Disease
Any disease which affects the heart and blood vessels, e.g. Coronary Heart Disease, Peripheral Arterial Disease or Cerebrovascular Disease.
Coronary Artery Bypass Graft (CABG)
An operation to bypass a narrowed section or sections of coronary arteries and improve the blood supply to the heart. During heart surgery the patient is connected to a Cardiopulmonary Bypass machine (heart-lung machine) which helps to circulate blood while the surgeon is operating. Some CABG operations can be done off bypass.

13
Cardiomyopathy -a disease of the heart muscle)
Dilated cardiomyopathy (DCM) is a disease of the heart muscle that causes the heart to become enlarged and to pump less strongly Hypertrophic Obstructive Cardiomyopathy (HOCM) is an excessive thickening of the heart muscle (hypertrophy literally means to thicken) in the absence of an apparent cause. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) is an inherited heart muscle disorder where damaged heart muscle is gradually replaced by scar tissue and fat. Restrictive cardiomyopathy (RCM) is the least common of the cardiomyopathies, it can be idiopathic (cause is unknown) or secondary to a number of rare cardiac and systemic disorders.
Cerebrovascular Disease
Atherosclerotic disease process affecting the cerebral arterial system. Causes Cerebrovascular Accidents (CVA/strokes) or Transient Ischaemic Attacks (TIA).
Cholesterol A fatty material made mainly in the body by the liver, it is important for cell function and for the production of vital chemicals. Too much cholesterol in the blood (hypercholesterolaemia or hyperlipidaemia) can increase the risk of developing Cardiovascular Disease.
Coronary Heart Disease (CHD)
When the coronary arteries become narrowed by a gradual build-up of fatty material called atheroma. CHD causes angina, myocardial infarction or sudden death.
Ischaemic Heart Disease (IHD)
Also known as Coronary Artery Disease (CHD) - See entry above.
Congenital Heart Disease
Heart Disease caused by abnormalities of the heart or major blood vessels which are due to abnormal development of the foetus and which are present at birth.
Defibrillator A device which delivers a controlled electric shock through the chest wall to the heart, in order to restore a normal heartbeat. Implantable Cardioverter Defibrillator (ICD) -A device which is implanted within the chest wall to monitor the heart rhythm, and if necessary, deliver an electrical shock.
Diastole Describes the phase in the cardiac cycle when the ventricles are at rest.
Ectopic Beat An extra heartbeat.
Endocarditis An infection of the inner lining of the heart, usually affecting the valves.
Ejection Fraction (EF)
The fraction of blood pumped out by the left ventricle with each contraction. A normal ejection fraction is 60-70%
14
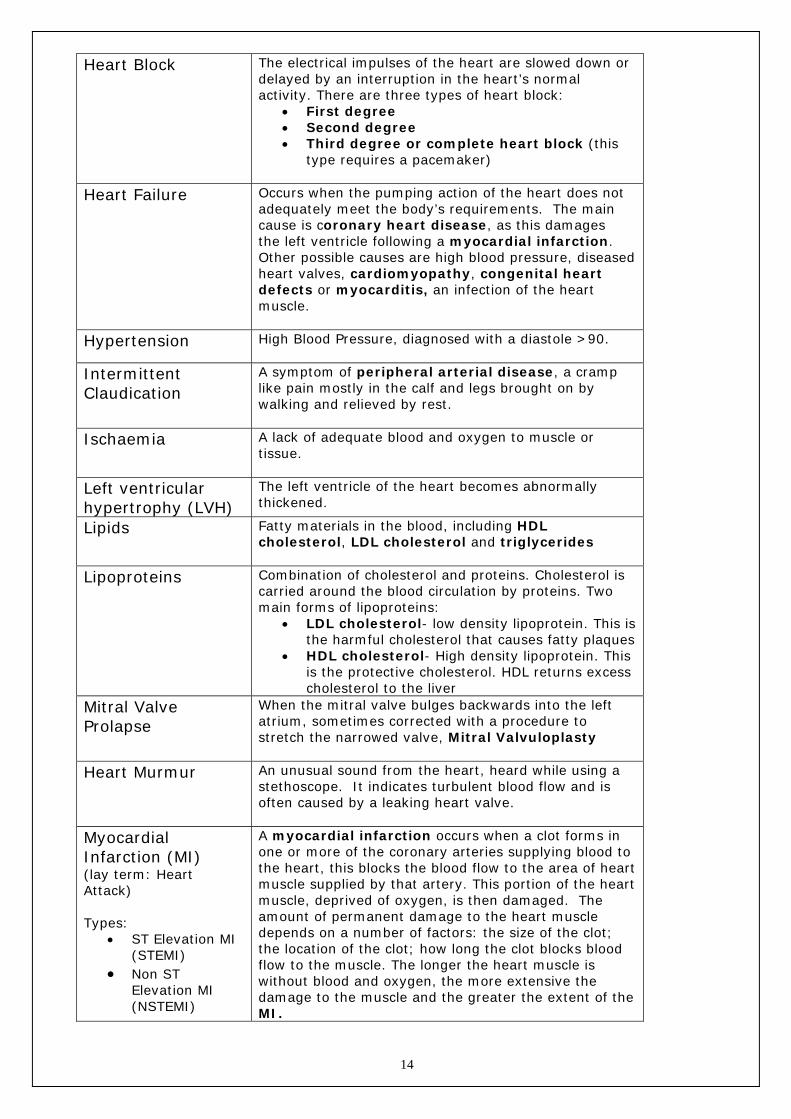
Heart Block The electrical impulses of the heart are slowed down or
delayed by an interruption in the heart’s normal activity. There are three types of heart block:
• First degree • Second degree • Third degree or complete heart block (this
type requires a pacemaker)
Heart Failure Occurs when the pumping action of the heart does not adequately meet the body’s requirements. The main cause is coronary heart disease, as this damages the left ventricle following a myocardial infarction. Other possible causes are high blood pressure, diseased heart valves, cardiomyopathy, congenital heart defects or myocarditis, an infection of the heart muscle.
Hypertension High Blood Pressure, diagnosed with a diastole >90.
Intermittent Claudication
A symptom of peripheral arterial disease, a cramp like pain mostly in the calf and legs brought on by walking and relieved by rest.
Ischaemia A lack of adequate blood and oxygen to muscle or tissue.
Left ventricular hypertrophy (LVH)
The left ventricle of the heart becomes abnormally thickened.
Lipids Fatty materials in the blood, including HDL cholesterol, LDL cholesterol and triglycerides
Lipoproteins Combination of cholesterol and proteins. Cholesterol is carried around the blood circulation by proteins. Two main forms of lipoproteins:
• LDL cholesterol- low density lipoprotein. This is the harmful cholesterol that causes fatty plaques
• HDL cholesterol- High density lipoprotein. This is the protective cholesterol. HDL returns excess cholesterol to the liver
Mitral Valve Prolapse
When the mitral valve bulges backwards into the left atrium, sometimes corrected with a procedure to stretch the narrowed valve, Mitral Valvuloplasty
Heart Murmur An unusual sound from the heart, heard while using a stethoscope. It indicates turbulent blood flow and is often caused by a leaking heart valve.
Myocardial Infarction (MI) (lay term: Heart Attack) Types:
• ST Elevation MI (STEMI)
• Non ST Elevation MI (NSTEMI)
A myocardial infarction occurs when a clot forms in one or more of the coronary arteries supplying blood to the heart, this blocks the blood flow to the area of heart muscle supplied by that artery. This portion of the heart muscle, deprived of oxygen, is then damaged. The amount of permanent damage to the heart muscle depends on a number of factors: the size of the clot; the location of the clot; how long the clot blocks blood flow to the muscle. The longer the heart muscle is without blood and oxygen, the more extensive the damage to the muscle and the greater the extent of the MI.

15
Palpitations
An uncomfortable awareness of the heart beating.
Pacemaker Types:
• Temporary pacing line(TPL)
• Permanent pacemaker (PPM)
A device to stimulate contractions of the heart when the heart fails to produce its own signal. It includes a pulse generator (the actual pacemaker) and one, two or three electrodes. The pacemaker is usually implanted in the upper left chest and the lead is secured in the heart
Peripheral Vascular Disease (PVD)
Any abnormal condition that affects the blood vessels outside the heart and lymphatic vessels (including Peripheral Arterial Disease)
Primary Prevention To reduce the risk of asymptomatic individuals developing Coronary Heart Disease or other atherosclerotic vascular disease
Revascularisation A term used to describe a range of procedures to unblock narrowed arteries and restore normal coronary blood flow; includes angioplasty and stenting and Coronary Artery Bypass Grafting (CABG)
Sinus rhythm (SR) Normal rhythm of the heart in which electrical activity is originated in the sinoatrial node (60-90 heart beats per min).
ST segment (ST) Seen on the ECG this represents the period between the ventricle contracting (depolarisation) and returning to their resting state (repolarisation) The ST segment is affected by ischaemia (ST depression or T wave changes) or infarction (ST elevation)
Sinus tachycardia A normal but fast heart rhythm (more than 100 heart beats per minute).
Supraventricular tachycardia (SVT) (or paroxysmal SVT -PSVT)
A disturbance of the heart rhythm caused by rapid electrical activity in the upper chambers of the heart (Atria)
Systole
Describes the period in the cardiac cycle when the ventricles are contracting
Unstable Angina (UA)
Angina which has just developed for the first time or angina which was previously stable but has recently got worse or changed in pattern of presentation. For example, symptoms may be triggered after doing much less exercise or less stress than usual, or angina symptoms may be experienced when at rest.
Ventricular tachycardia (VT)
An abnormal fast heart rate in the ventricles
Ventricular fibrillation (VF)
A life threatening disturbance in the heart rhythm which causes the heart to quiver or fibrillate in a disordered way

16
Valvular Heart Disease
When one or more of the four valves in the heart are diseased or damaged, affecting the flow of blood in the heart. If the valve is narrow or does not open fully (stenosis) it will restrict the flow of blood. If the valve does not close properly, it will allow blood to leak backwards (regurgitation)
Please record any definitions you come across which are not listed

17
Phases of Rehabilitation
Phase I: Inpatient stay Involves patient and significant others. The approach should be client led and information (verbal and written) is given to the patient to help him understand the disease process, recovery, and preventative measures for the future. Phase II: Immediately post discharge Contact is made via telephone or home visit to assess:
• Symptoms • Medication concordance • Risk factor stratification • Liaison made with Primary Care team as required
Phase III: Out patient rehabilitation One to one assessment for all patients by nurse and physiotherapist at nurse-led post MI clinic at 4 and 16 weeks post MI. A report is forwarded to the GP. Choice of:
• supervised outpatient exercise classes, educational talks on group basis for 12 weeks
• Home video exercise programme • Education only component of rehabilitation if concomitant disease
excludes exercise Phase IV: Maintenance
• Maintenance of exercise by referral to local sports centre or exercise of choice e.g. swimming, dancing, etc.
• Continued monitoring of risk factors and secondary prevention measures by Primary Care Team as necessary.

18
Secondary Prevention
The target group for secondary prevention are people who already have atherosclerotic disease
The aim of secondary prevention is to halt the progress of symptomatic Coronary Heart Disease. The objective is to slow the progression of atherosclerosis and to preserve left ventricular function following myocardial Infarction. The modification of risk factors and medication are the cornerstone of secondary prevention. Secondary prevention medication reduces death, vascular events and hospital readmissions:
Medication Groups Name Examples Anti-platelets
Beta-blockers
ACE Inhibitors
Statins
Exercise: Complete the tables
Common Cardiac Tests Test Indication Management ECG (Electrocardiogram)
ETT (Exercise Tolerance Test)
Echocardiogram
TOE (Transoesphageal echocardiogram)
Cardiac Enzyme Tests
Coronary Angiograms
Thallium Scan

19
Cycle of Change
(Prochaska and Diclemente 1983)
Pre-contemplation (Content with status quo)
Relapse Contemplation
(Thinking about change)
Maintenance Planning (Maintaining change) (Preparing to change) Action (Making changes)
Pre-contemplation: • No evidence of intention to change behaviour in the forseeable future • Lack of awareness of any problem relating to self • Ability to see solution to problem only in relation to others • Hallmark; resistance to recognising or modifying lifestyle.
Contemplation:
• Awareness of problem relating to self. • Thinking of change. • Not yet committed to action. • Patient can remain stuck in contemplation for long periods. • They weigh up costs and benefits of change and seek information to
assist their decision. • Stage can last for minutes, months, years.
Preparation -Deciding to change:
• Perceived benefits of the change seem to outweigh costs. • Patient believes that change is possible and worthwhile. • May need extra knowledge, skills and support to move into action. • Stage usually associated with some small behaviour change, e.g. smoking
less.

20
Action - Trying to change, changing:
• Modification of behaviour, experiences or environment in order to overcome problem.
• Requires positive decisions to do things differently. • Sometimes a need to make temporary changes in other aspects of
lifestyle to support change: e.g. avoiding pub for new non-smokers. • Features of success at this stage:
clear goal realistic plan appropriate support rewards
Maintenance:
• Continuation of change • Working to prevent relapse and consolidate changes made. • Time needed to 'break habit' and establish 'safer' lifestyle. • Maintaining the new behaviour can be difficult and remains a struggle for
some time; requires constant vigilance and support to avoid relapse.
Relapse: • A normal part of the change process. • Often happens in high risk situations. • Can sometimes be prevented by planning ways to cope with a high risk
situation.
NB: in one study 85% of smokers who relapsed went back to contemplation and only 15% went back to pre-contemplation.
Role of Cardiac Rehabilitation Nurse
Facilitator
Communicator
Innovator
Advisor
Leader
Carer
Manager
Conduit
Advocate

21
Abbreviations
24o tape 24 hour ECG monitor ACS Acute Coronary Syndrome AED Automatic External Defibrillator AF Atrial Fibrillation Afl Atrial Flutter AMI Acute Myocardial Infarction Ant Anterior Wall of myocardium AP Angina Pectoris AI Aortic incompetence AR Aortic Regurgitation AS Aortic Stenosis AVR Aortic Valve replacement BACR British Association Cardiac Rehabilitation BM Blood Monitoring BMI Body Mass Index BMS Bare Metal Stent BP Blood Pressure CA Coronary Angiogram CABG Coronary Artery Bypass Graft CCF Congestive Cardiac Failure CCU Coronary Care Unit CHD Coronary Artery Disease CK Creatinine Kinase CLASP Cardiovascular Limitations and Symptoms Profile COPD Cardiology OutPatient Department CP Chest Pain CR Cardiac Rehabilitation CRT Cardiac resynchronisation therapy CRT-D Cardiac resynchronisation therapy with
defibrillator CST Chester Step Test CV CardioVascular CVD CerebroVascular Disease Cx Circumflex (coronary artery) DES Drug Eluting Stent DC shock
Direct current shock (administered from cardiac defibrillator)
DM Diabetes Mellitus

22
Dx Diagonal Artery ECG ElectroCardioGram Echo Echocardiogram EF Ejection Fraction ETT Exercise Tolerance Test GTN Glycerine Trinitrate HADS Hospital Anxiety and Depression Scale HBP High Blood Pressure HR Heart Rate ICD Implantable Cardioverter Defibrillator (N) IDDM
(Non) Insulin dependent Diabetes Mellitus
IHD Ischaemic Heart Disease Inf Inferior aspect of myocardium INR International Normalised Ratio LAD Left Anterior Descending (coronary artery) LIMA Left Internal Mammary Artery LMS Left Main Stem LV Left Ventricle LVEF Left ventricular ejection fraction LVF Left Ventricular Failure LVSD Left Ventricular Systolic Dysfunction METs Metabolic Equivalents MI Myocardial Infarction MOPD Medical OutPatient Department MVR Mitral Valve Replacement NSTEMI Non ST Elevation Myocardial Infarction NYHA New York Heart Association OHTx Orthotopic Heart Transplant OM Obtuse Marginal (coronary artery) OOH VFA Out Of Hospital Ventricular fibrillation Arrest PAF Paroxysmal Atrial Fibrillation PAP Pulmonary Artery Pressures PCI Percutaneous Coronary Intervention PDA Posterior Descending Artery PEA Pulseless Electrical Activity PMIC Post Myocardial Infarction Clinic PPM Permanent Pacemaker PTCA Percutaneous Transluminal Coronary Angioplasty PVD Peripheral Vascular Disease RCA Right Coronary Artery
23
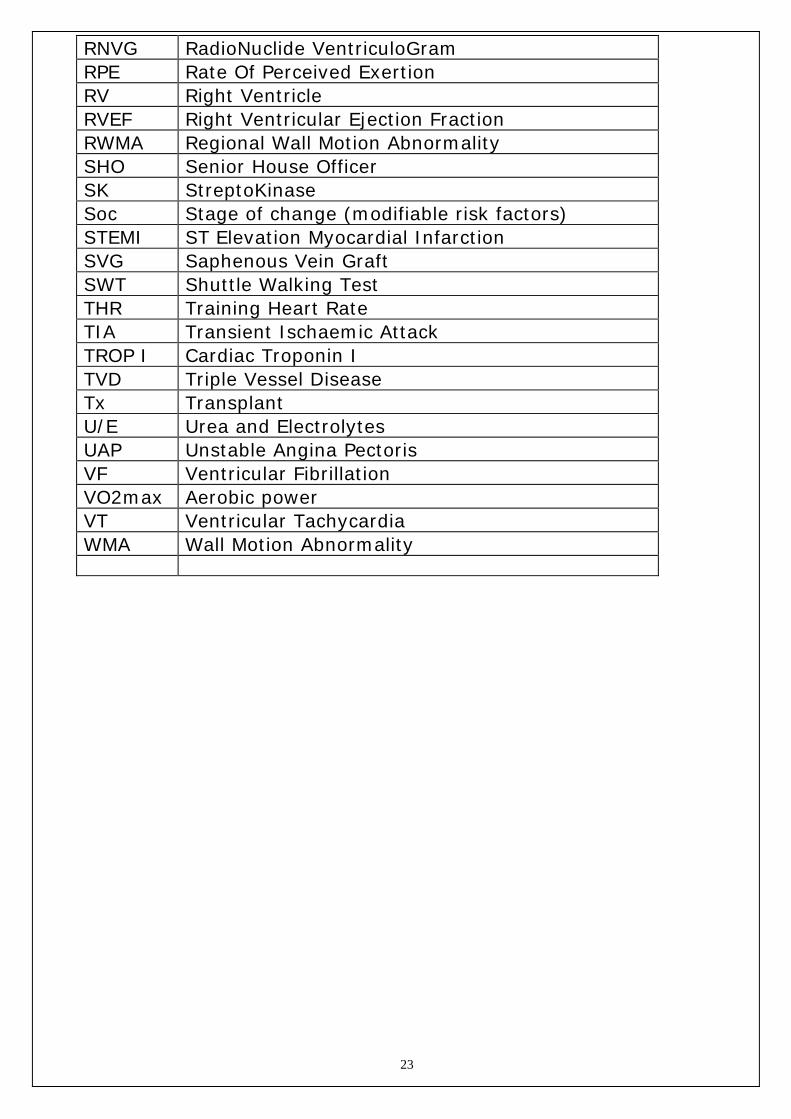
RNVG RadioNuclide VentriculoGram RPE Rate Of Perceived Exertion RV Right Ventricle RVEF Right Ventricular Ejection Fraction RWMA Regional Wall Motion Abnormality SHO Senior House Officer SK StreptoKinase Soc Stage of change (modifiable risk factors) STEMI ST Elevation Myocardial Infarction SVG Saphenous Vein Graft SWT Shuttle Walking Test THR Training Heart Rate TIA Transient Ischaemic Attack TROP I Cardiac Troponin I TVD Triple Vessel Disease Tx Transplant U/E Urea and Electrolytes UAP Unstable Angina Pectoris VF Ventricular Fibrillation VO2max Aerobic power VT Ventricular Tachycardia WMA Wall Motion Abnormality

24
References & Resources *Scottish Intercollegiate Guidelines Network (SIGN) www.sign.ac.uk
SIGN 57: Cardiac Rehabilitation
SIGN 93: Acute Coronary Syndromes
SIGN 94: Cardiac Arrythmias In Coronary Heart Disease
SIGN 95: Management Of Chronic Heart Failure
SIGN 96: Management Of Stable Angina
SIGN 97: Risk Estimation And The Prevention Of Cardiovascular Disease *Useful Organisations and websites
British Heart Foundation (BHF): Publications www.bhf.org Chest, Heart & Stroke: Publications www.nhsggc.org.uk/hsd NHS Smoking Concerns: Publications www.smokingconcerns.com British Association Of Cardiac Rehabilitation (BACR) www.bacr.org/ Scotland Health On The WEB (SHOW) www.show.scot.nhs.uk/ Health Education Board For Scotland (HEBS) www.opsi.gov.uk/si/991/uksi Nursing & Midwifery Council (NMC) Publications www.nmc.org/ *Cardiac Rehabilitation Booklets Cardiac Rehabilitation Protocols For Greater Glasgow & Clyde Lindsay, G. and Gaw A. (????) Coronary Heart Disease Prevention, A handbook for the health care team, Churchill Livingstone Wilson, Kathleen J. W. (????) Anatomy & Physiology in Health in Illness, Churchill Livingstone Chapter 6 pp 70 – 108 British National Formulary (BNF) British Medical Association, London 2008-11-20
25
Student Placement Diary
Week MON TUES WED THURS FRI SAT SUN
1
2
3
4
5
6
26
Placement Evaluation
(Please circle the most appropriate answer)
1. This placement was an enjoyable experience.
Strongly agree Agree Disagree Strongly agree
2. The staff were friendly and welcoming.
Srongly agree Agree Disagree Strongly disagree
3. This placement was a valuable learning opportunity.
Strongly agree Agree Disagree Strongly disagree
4. The level of support received was appropriate to my level of training.
Strongly agree Agree Disagree Strongly disagree Thank you for taking the time to complete our evaluation, your comments will help us to provide a quality learning experience for students in the future. Please comment on any aspect of your learning experience
Please return this completed questionnaire to Cardiac Rehabilitation Team