Welcome to NHS Tayside. The Unique Role of Organisation Leaders Set the tone and values system in...
47
Welcome to NHS Tayside
-
Upload
clarence-woods -
Category
Documents
-
view
216 -
download
1
Transcript of Welcome to NHS Tayside. The Unique Role of Organisation Leaders Set the tone and values system in...

Welcome to NHS Tayside
The Unique Role of Organisation Leaders• Set the tone and values system in their organisations, • Establish strategic goals for activities to be undertaken, • Align efforts within the organisation to achieve those
goals, • Provide resources for the creation of effective systems
remove obstacles for staff, and• Require adherence to revised practices• Create leverage for continuous improvement

Leadership
• Patient Safety as a Strategic Imperative• Clear Goals and Measurement • Reduce variability, waste and harm• Skill building • Encouragement with expectations• Ask important questions- What is preventing
movement? How can we help?• Expectations without capability breeds fear
and hopelessness

Jutland

ShetlandShetland
GrampianGrampian
HighlandHighland
WesternWesternIslesIsles
BordersBorders
FifeFife
LothianLothian
GreaterGreaterGlasgow ClydeGlasgow Clyde
Ayrshire Ayrshire & Arran& Arran
OrkneyOrkney
Forth ValleyForth Valley
LanarkshireLanarkshire
Dumfries &Dumfries &GallowayGalloway
Scotland’s Pop. 5.2 millionScotland’s Pop. 5.2 million
14 health Boards 150,000 staff14 health Boards 150,000 staff
TaysideTayside
And 7 Special Boards NHS 24NHS Education ScotlandNHS Health ScotlandHealth Improvment Scotland Scottish Ambulance State Hospitals Board The National Waiting Times

Projected Scottish Government spending
20,000
22,000
24,000
26,000
28,000
30,000
32,000
£ M
illio
ns (
2010
-11
Pric
es)
2009-10 2025-2616 years
£42 billion

• Population - 400,000
• Services; Acute/Teaching Hospital , Mental Health, Community Services, Primary Care & Regional Services
• 22 Hospitals – 1192 Beds
• 68 GP Practices - 322 GPs
• 3 Local Authorities
• Budget c£800m
• Efficiency Savings Target 2011/12 – £27m
NHS Tayside Profile

Proposed New Quality Aims
1. To make NHS Scotland a world leader in healthcare quality improvement.
2. To do so in a way that is meaningful to all.
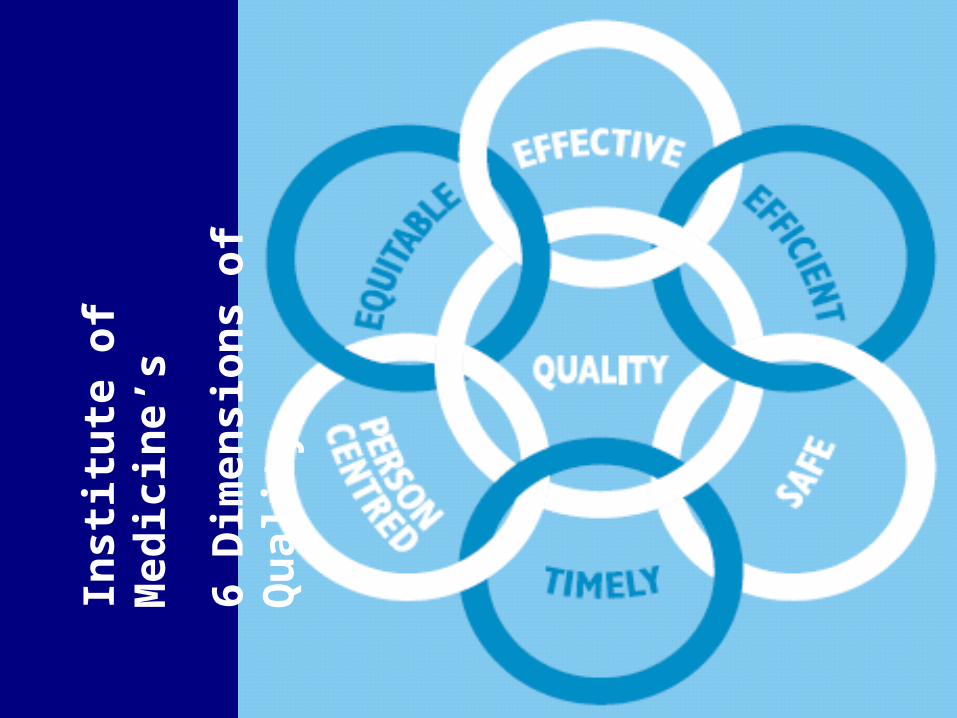
Inst
itu
te o
f M
edic
ine’
s
6 D
imen
sion
s of
Qu
alit
y

Ninewells HospitalPerth Royal Infirmary
Stracathro Hospital


S + P = O
Source: Donabedian, A. Explorations in+ Quality Assessment and Monitoring. Volume I: The Definition of Quality and Approaches to its Assessment.
Ann Arbor, MI, Health Administration Press, 1980.
The Theory for Change
Structure + Process = OutcomesStructure + Process = Outcomes
+Culture

13
Appreciation of a system
Understanding Variation
Theory of Knowledge
Psychology
A
im or V
alues
The Lens of Profound Knowledge
QI
The system of profound knowledge provides a lens. It provides a new map of theory by which to understand and optimize our organizations. It provides an opportunity for dialogue and learning!

14
Appreciation for a System• Interdependence, dynamism• World is not deterministic• Optimization, interactions• System must have an aim• Whole is greater than sum of the parts
Understanding Variation• Variation is to be expected• Common or special causes• Ranking, tampering• Potential mistakes
Theory of Knowledge• Prediction• Learning from theory, experience• Operational definitions • PDSA for learning and improvement
Psychology• Interaction between people• Intrinsic motivation, movement• Beliefs, assumptions • Will to change
What insights might be obtained by looking through the Lens of Profound
Knowledge?

Exercise
• Work with the person next to you • For 5 minutes discuss your project and
theories and assumptions that relate to your local projects
• Consider appreciation of the system• Theory of knowledge

The “Quality Curve”
Shift and narrow the curve:What is the norm?
Shift and narrow the curve:What is the norm?
Cut the tail:What is unacceptable?
Cut the tail:What is unacceptable?
Extend the ambition: What is great? (What is possible?)
Extend the ambition: What is great? (What is possible?)
11
22
33

Mesosystem
Macrosystem
Microsystem
Nursing Services
Nursing Divisions
FrontlineNursingUnits
Source: G. Hendriks & M. Bojestig, Jonkoping County Council, Sweden
System Level Thinking: Jonkoping Sweden

The beginning…………

A History of Quality as a Business A History of Quality as a Business Strategy in TaysideStrategy in Tayside
Source: System thinking and spreading knowledge, Bojestic M., Henriks, G., Provost L. IHI European Forum, Prague 2006
Awareness•Safer Patient Initiative•Change & Innovation Plan
Education•Learning from Qulturum and IHI•Patient Safety Officer training•Improvement experts and practitioners training •Board Effectiveness Development Programme
Process Thinking•Lean and Rapid Improvement work•Real time data and measurement for improvement
Redesign•Improvement as a Systems Property•Steps to Better Healthcare•Triple Aim
Movement•Triple Aim •System Infrastructure - TCOE•Creating breakthrough
Full Scale•Public Sector Infrastructure to support improvement •Working with Communities
2006 2007 2008 2009 2010 2011 Beyond
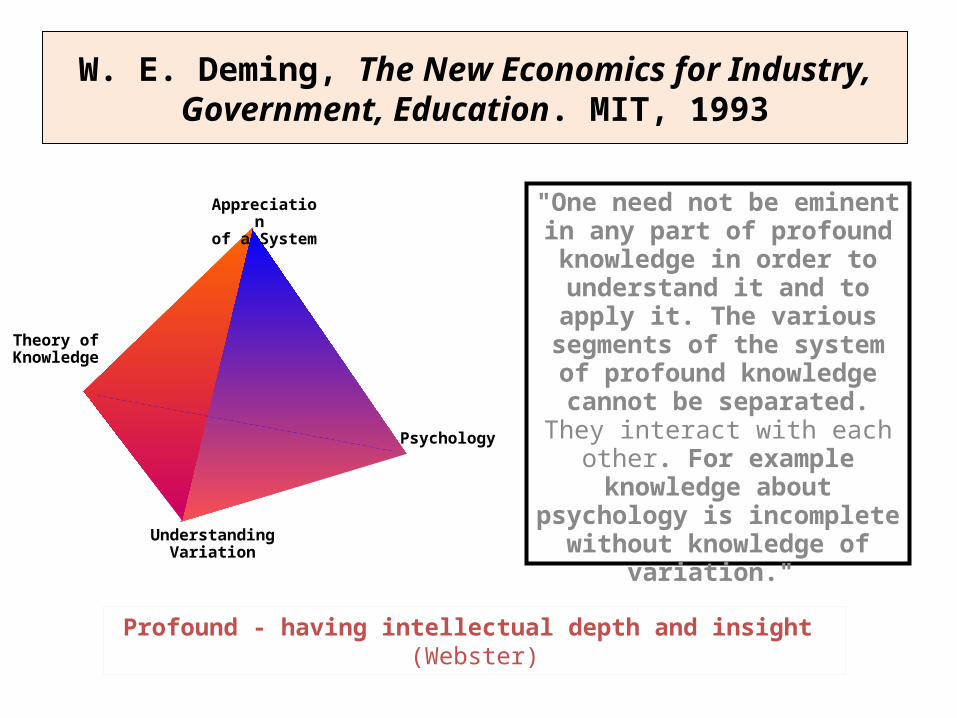
W. E. Deming, The New Economics for Industry, Government, Education. MIT, 1993
"One need not be eminent in any part of profound knowledge in order to understand it and to
apply it. The various segments of the system of profound
knowledge cannot be separated. They interact with each other. For
example knowledge about psychology is incomplete without
knowledge of variation."
Profound - having intellectual depth and insight (Webster)
Appreciation of a System
Theory of Knowledge
Psychology
UnderstandingVariation
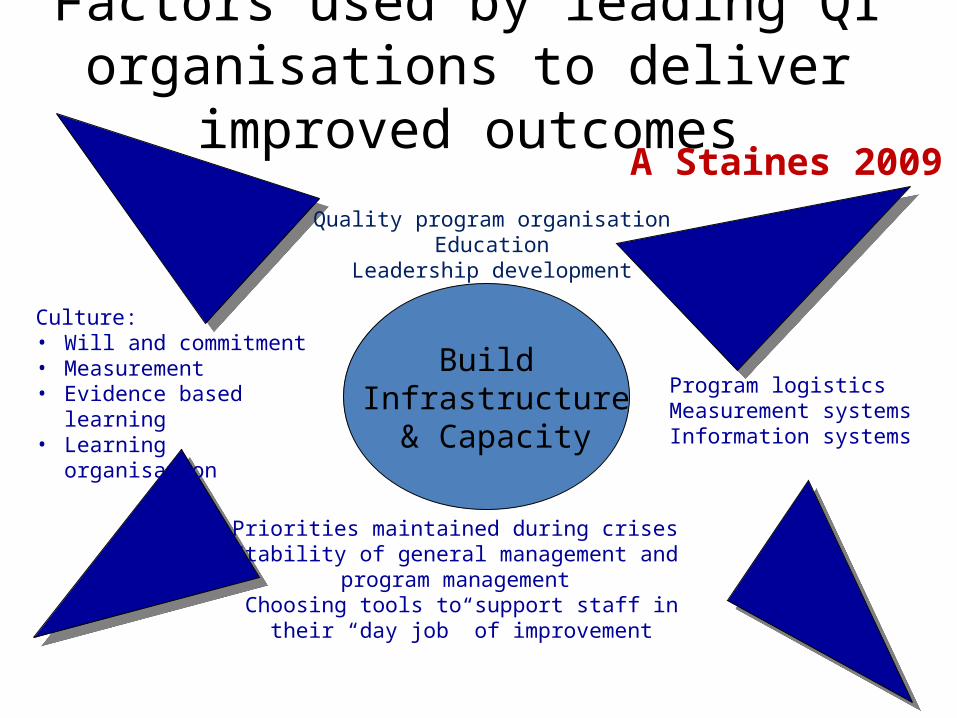
Factors used by leading QI organisations to deliver improved outcomes
Build Infrastructure
& Capacity
Quality program organisation Education
Leadership development
Priorities maintained during crises Stability of general management and
program management Choosing tools to support staff in their “day job”
of improvement
Program logisticsMeasurement systemsInformation systems
Culture:• Will and commitment• Measurement• Evidence based learning• Learning organisation
A Staines 2009


NHS Tayside Governance DashboardsNHS Tayside Governance Dashboards
Board
ET
EMT
Directorate / CHP
Ward / Team Level
Patient / Practitioner Level
ASSURANCE
Validated Data for 6 domains: Access, Efficiency, Infection & Prevention, Quality & Patient
Experience, Patient Safety and Data Quality
PERFORMANCE
Validated and un-validated data across 6 domains:Clinical Excellence, Finance & Activity, Valuing Staff, Capacity &
Activity Planning, Patient Experience and Patient Safety
Impr
ovem
ent
Patient to Board
“focusing on information and data to provide assurance on improvement and quality to deliver better, safer care”.
Perf
orm
ance
Assu
ranc
e
Dat
a an
d M
easu
rem
ent f
or
IMPROVEMENT
Un-validated data provided in real time through Unified Patient Tracking, Clinical Portal and operational dashboard with metrics covering Patient Flow, Inpatient Activity, Out Patients, Waiting
Times, Patient Safety, Infection Control, Clinical Outcomes

Steps to Better Healthcare Programme
Mental Health
OutPatients
Elective Care
Workforce Integrated Care
Older People
Optimisation of Health Facilities
across Tayside
Medicines Leadership
Finance Support
Workforce Support
Scenario Planning, Financial Baselines, Benefits Tracking, Business Cases
Workforce Modelling, Engagement, Partnership & Communications with staff
Comms SupportCommunications with public and staff
OE SupportOrganisational Effectiveness support

Productivity and EfficiencyCompliance with Tayside Area Formulary - PCDevelopment of Specialist formularies – SC
Service OptimisationElimination of waste Procurement and supplies
CRESCost minimisationMinimising variation in prescribing across TaysideWorkforce efficiency savings
Service TransformationReduce harmful prescribing in the elderlyImprove repeat prescribing systemsCoeliac patient pathwayPain patient pathway
TACTICAL STRATEGIC
DEALING WITH THE 5% SPENDING THE 95% BETTER
Medicines Leadership WorkstreamObjectives 2011/12

Efficiency and Productivity Strands
Whole Systems Approach
Whole system Improvement

Experts OperationalLeaders (Executives)
ChangeAgents
(Middle Managers, Stewards, project leads)
Everyone
(Staff, Supervisors,UBT lead triad)
Unit Based Teams
Continuum of PI Knowledge and Skills
Deep Knowledge
Many People Few People
Our approach will be to make sure that each group receives the knowledge and skill sets they need when they need them and in the appropriate amounts.
A key operating assumption of building capacity is that different groups of people will have different levels of need for PI knowledge and skill.
Content: What Skills Do We Need?
Source: Kaiser Permanente, 2008
SharedKnowledge

The Primary Drivers of Improvement
Will
Ideas Execution
Having the Will (desire) to change the current state to one that is better
Developing Ideas that will contribute to making processes and outcome better
Having the capacity to apply CQI theories, tools and techniques that enable the Execution of the ideas
QI

The Improvement Guide, API, 1996
A Model for Learning and Change
When you combine the 3 questions with the…
…the Model for Improvement.PDSA cycle,
you get…
PDSA(Please Do Something, Anything!)
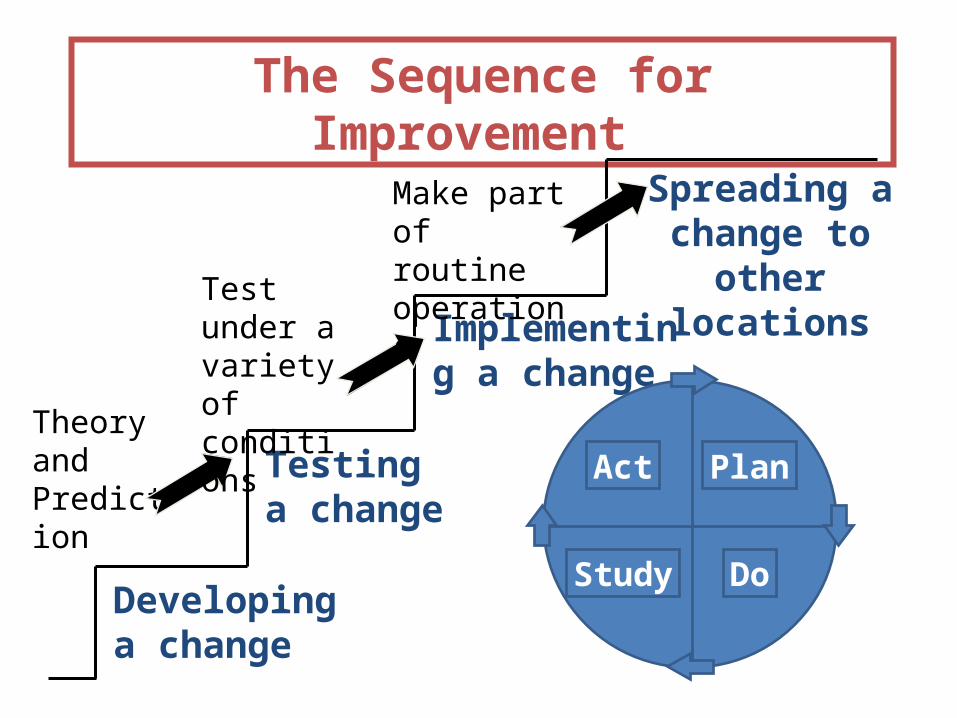
The Sequence for Improvement
Spreading a change to other
locations
Developing a change
Implementing a change
Testing a change
Act Plan
Study Do
Theory and Prediction
Test under a variety of conditions
Make part of routine operations

Degree of belief that the changes
will result in improvement
High
Prototype Pilot Adapt & Spread
Successful changes
Changes still need further testing. There is a risk of moving to spread.
Unsuccessful proposed changes
Low
Moder- ate
Where is Your Project?
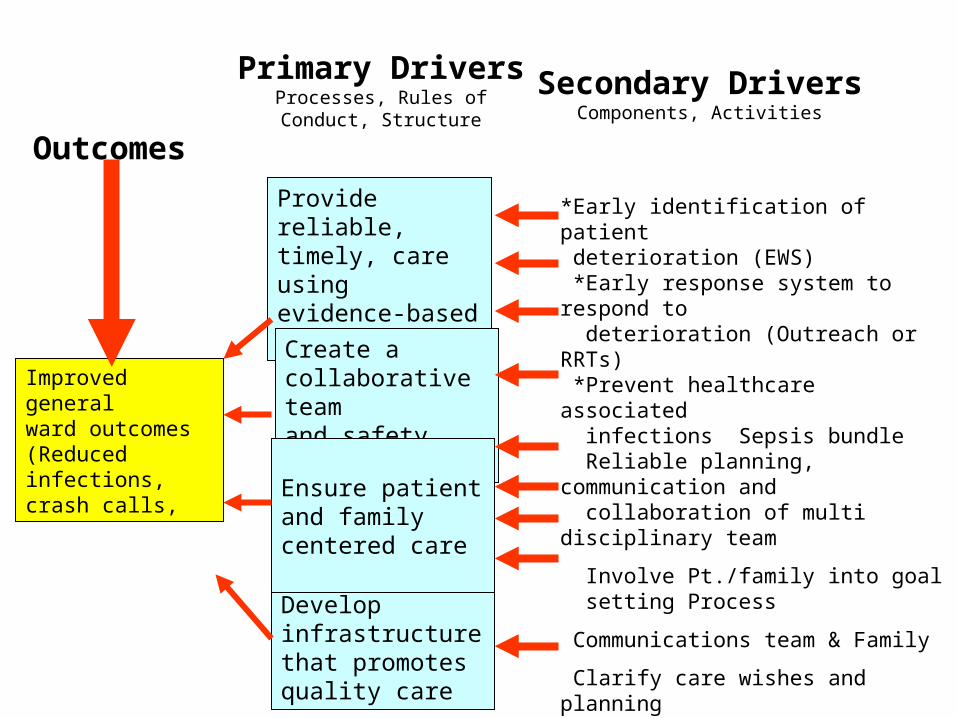
Scottish Patient Safety ProgrammeGeneral Ward Driver Diagram
Outcomes
Primary DriversProcesses, Rules ofConduct, Structure
Secondary DriversComponents, Activities
Improved generalward outcomes(Reduced infections,crash calls,
Provide reliable, timely, care using evidence-based therapies
Create a collaborative team and safety culture
Develop infrastructure that promotesquality care
Ensure patient and family centered care
*Early identification of patient deterioration (EWS) *Early response system to respond to deterioration (Outreach or RRTs) *Prevent healthcare associated infections Sepsis bundle Reliable planning, communication and collaboration of multi disciplinary team
Involve Pt./family into goal setting Process
Communications team & Family
Clarify care wishes and planning
Ensure patients physical comfort
Appropriate infrastructure to provide reliable, evidence based care
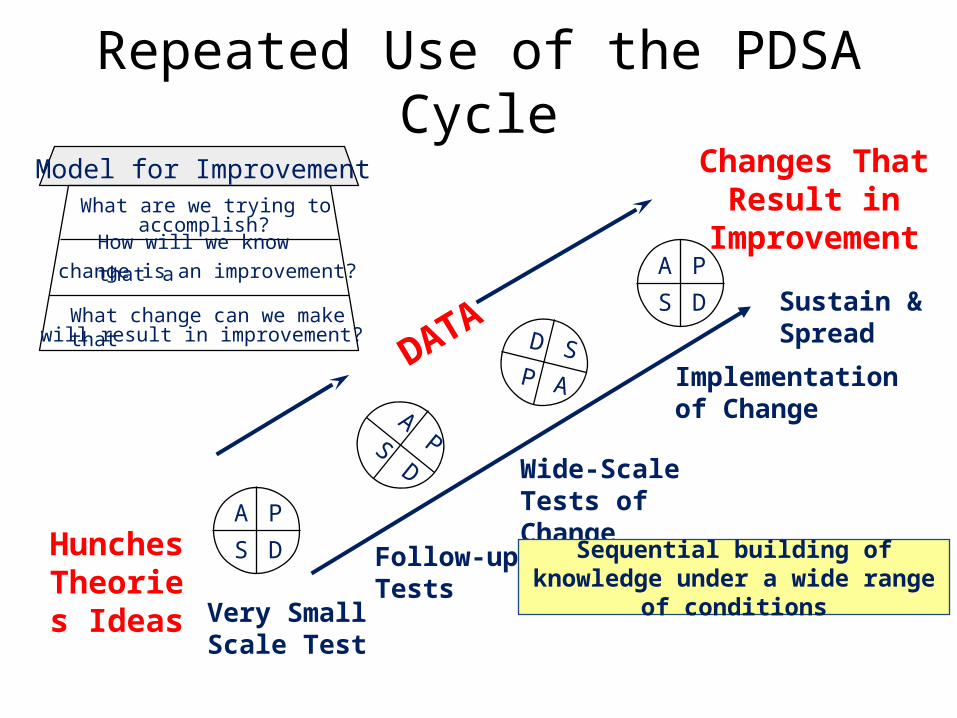
Repeated Use of the PDSA Cycle
Hunches Theories
Ideas
Changes That Result in
Improvement
A P
S D
APS
D
A P
S D
D SP A
DATA
Very Small Scale Test
Follow-up Tests
Wide-Scale Tests of Change
Implementation of Change
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Sustain & Spread
Sequential building of knowledge under a wide range of conditions

Secondary DriversComplications from Ventilators
Complications from CVCs
Optimal Glucose Control
Hospital Acquired Infections
Sepsis Recognition and Treatment
Aim: Provide appropriate, reliable and timely care to critically ill patients using evidence-based therapies in Hospital X, Pilot Site
Y, by December 2010
Change Concep
t 1
Change Concep
t 2
Change Concep
t 3
Change Concep
t 4
Change Concep
t 1
Change Concep
t 2
Change Concep
t 3
Change Concep
t 4
Change Concep
t 1
Change Concep
t 2
Change Concep
t 3
Change Concep
t 4
Change Concep
t 1
Change Concep
t 2
Change Concep
t 3
Change Concep
t 4
Change Concep
t 1
Change Concep
t 2
Change Concep
t 3
Change Concep
t 4

A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
Central Line Insertion Bundle
CVC Maintenance Bundle
Partner with Accident and Emergency and Operating Theatres for Standardisation
Standardise Process:Line Carts and Dressing Kits
Lead 1 Lead 2Lead 1 Lead 3
Aim: Reduce Complications from CVCs in Hospital X, Pilot Site by October 2010

A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
A P
S D
A PS D
A P
S D
D S
P A
Daily Checking and Need for CVC
Dressing in Tact and Changed w/i 7 Days
Hand Hygiene Prior to Access
CVC Hub Decontamination
A P
S D
A PS D
A P
S D
D S
P A
Chlorhexidine Gluconate
Lead A Lead A Lead B Lead B Lead C
Aim: Design a Reliable Process for CVC Maintenance Bundle by September 2010

39
Key Components* Self-Assessment • Will (to change)• Ideas• Execution
• Low Medium High• Low Medium High• Low Medium High
*All three components MUST be viewed together. Focusing on one or even two of the components will guarantee suboptimized performance. Systems thinking lies at the heart of CQI!
How prepared is your organization?

40
Creativity Tools• Brainstorming
• Mind mapping
• Six thinking hats
• Innovation/IDEO
Measurement Tools• Cost of quality analysis
• Benchmarking
• Dashboards/indicators
• Survey analysis
Design Tools• QFD
• FMEA
Statistical Tools• SPC
• Descriptive statistics
• Multivariate statistics
CQI Tools by Function

41
Tools to Understand Variation in Data
Waiting Time for Clinic Visit
20
25
30
35
40
45
50
55
60
Ave
rage
Day
s
Waiting Time for Clinic Visit
20
25
30
35
40
45
50
55
60
Ave
rage
Day
s
Distribution of Wait Times
0
10
20
30
40
50
60
5 15 25 35 45 55 65 75 85 95 105Wait time (days) for Visit
num
ber of
vis
its
Clinic Wait Times > 30 days
0
2
4
6
8
10
12
14
16
C F G D A J H K B I L EClinic ID
# of
wai
ts >
30 d
ays
Relationship Between Long Waits and Capacity
0
5
10
15
20
75 95Capacity Used
# w
ait tim
es >
30
day
s
Run Chart Shewhart Chart
Frequency Plot Pareto Chart Scatterplot
IH p. 8-34

Cultural Elements• Robust Governance and Risk management
arrangements• A preoccupancy with failure • A culture of openness• Abandoning blame as a major mode of action • Trust in the workforce• Involvement of patients and families
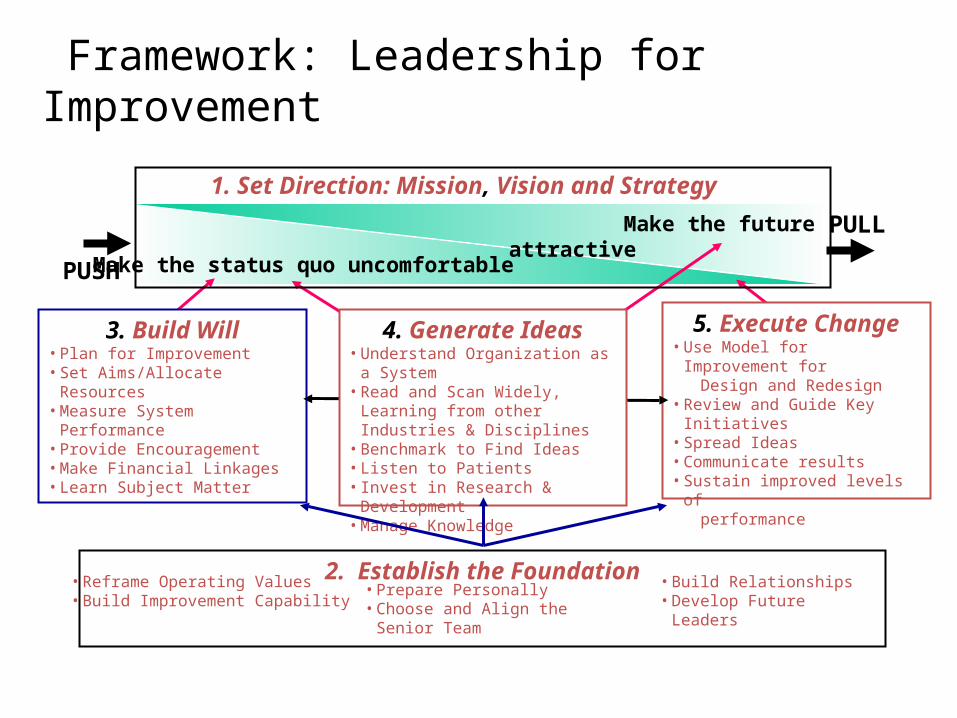
PULL
PUSH
1. Set Direction: Mission, Vision and Strategy
Make the status quo uncomfortable
Make the future attractive
3. Build Will• Plan for Improvement• Set Aims/Allocate Resources• Measure System Performance• Provide Encouragement• Make Financial Linkages• Learn Subject Matter
5. Execute Change• Use Model for Improvement for Design and Redesign• Review and Guide Key Initiatives• Spread Ideas• Communicate results• Sustain improved levels of performance
4. Generate Ideas• Understand Organization as a System• Read and Scan Widely, Learning from
other Industries & Disciplines• Benchmark to Find Ideas• Listen to Patients• Invest in Research & Development• Manage Knowledge
Framework: Leadership for Improvement
2. Establish the Foundation• Prepare Personally• Choose and Align the Senior Team
• Build Relationships• Develop Future Leaders
• Reframe Operating Values• Build Improvement Capability

44
Where we want to be!
Where we are!
How do you
bridge the gap
between these
two conditions?
Considerations
• The context within which the program will apply
• Pre-existing capacities to support change• Sphere of influence to effect change
– Individual – Team – Organisation
47
“We are what we repeatedly do. Excellence then, is not an act but a
habit!
Aristotle (384 – 322 BC)