Welcome to Kaiser Permanente Southern California · education institutions, governmental agencies,...
57
Welcome to Kaiser Permanente Southern California Student Unpaid Field Experience and Training Required Readings Inpatient/Hospital and Outpatient/Ambulatory
Transcript of Welcome to Kaiser Permanente Southern California · education institutions, governmental agencies,...
Welcome to Kaiser Permanente Southern California Student Unpaid Field Experience and Training
Required Readings
Inpatient/Hospital and Outpatient/Ambulatory

Table of Contents
1. Policies and Procedures: Student Unpaid Field Experience and Training ...................... 3Appendix A. Onboarding ProcessAppendix B. Dress Code and Hygienic Practices
2. Human Resources: Drug-Free Workplace NATL.HR.030 ............................................... 17
3. Compliance (Principles of Responsibility) ...................................................................... 24
HIPAA 101: Privacy and Security BasicsPrevent Fraud, Waste, and AbuseWhat is Protected Health Information?
4. Ambulatory Health Care and Hospital National Patient Safety Goals ............................ 35
5. SBAR (Situation, Background, Assessment and Recommendation) .............................. 37
6. Emergency Codes………………..………………………………………………………………………………….. 38
Student Nurses Continue with 7-11
7. Regional High-Alert Medication Safety Practices .......................................................... 40
8. KP Nursing Professional Practice Model ........................................................................ 53
9. KP Nursing Vision and Values ........................................................................................ 54
10.Bar Code Scanning Medication Administration- Instructions for Students ................... 55
11.Nurse Knowledge Exchange + ....................................................................................... 56

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
1.0 Policy Statement
This policy was developed to establish guidelines for Southern California Kaiser Permanente upon contractingcolleges/universities/schools for unpaid field experience and training programs of students at Kaiser Permanentefacilities.
2.0 Purpose
The purpose of this policy is to establish the criteria and requirements necessary to ensure the safety of ourpatients, employees, and Program Participants when establishing student unpaid field experience and trainingwithin a Kaiser Permanente facility.
3.0 Scope/Coverage
3.1 This policy applies to all Program Participants who are participating in unpaid field experience and trainingin any of the following entities:3.1.1 Kaiser Foundation Health Plan, Inc. (KFHP) and Kaiser Foundation Hospitals (KFH);3.1.2 Southern California Permanente Medical Group (SCPMG);3.1.3 KFHP, KFH, and affiliated groups.
4.0 Definitions
4.1 Being Under the Influence refers to any individual impaired by alcohol or a drug or the combination ofalcohol and drugs, regardless of the level detected. A determination of under the influence can beestablished by a professional opinion, medically accepted drug or alcohol screening test, and/or based onlay observations by supervisors, colleagues, or others.
4.2 Facility refers to all KPSC Medical Centers and medical office buildings. It also refers to Home Health,including but not limited to, a home health facility, nursing home, hospice, palliative, subacute facility, orpatient’s residence where Program Participants are under the supervision of an employee at KaiserEntities.
4.3 Faculty refers to the School’s unpaid field experience and training instructors.
4.4 Kaiser Permanente Entities (KP Entities, Kaiser, or KP), refers to any Medical Program entity in KaiserPermanente Southern California (KPSC) contracting with Schools for an Unpaid Field Experience andTraining Program, including KFHP, KFH, or SCPMG.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 1 of 8
SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
4.5 KP Academic Liaison and/or Sponsor refers to the KP personnel coordinating Program Participants
4.6 Network Development and Administration (ND&A) refers to the Southern California (SCAL) RegionalDepartment that drafts, negotiates, and executes all SCAL school agreement contracts for unpaid fieldexperience and training.
4.7 Program Participant refers to any Student(s) or Faculty participating and/or covered under KPSC SchoolAgreements for Student Unpaid Field Experience and Training.
4.8 School refers to an educational institution that has a School Agreement Contract with KP.
4.9 Student refers to any person who is enrolled in a School’s healthcare-related program and who will beparticipating in their specified unpaid field experience and training hours at KP.
4.10 Unpaid refers to students who are not paid via W2 by Kaiser Permanente payroll. Some W9 and stipendpayments do fall under these agreements. They are approved and reviewed on a case by case basis by theSchool Agreements Stakeholder Group (SASG) and KP Legal.
5.0 Provisions/Procedures5.1 Affiliation Contracts/Scheduling
5.1.1 A current School Agreement Contract between KP and School (which includes the program ofstudy) must be in place prior to the establishment/implementation of any Program Participant’sunpaid field experience and training rotation/placement with KP.
5.1.2 To add a program to a current School Agreement Contract or to request a new school contract,contact the Medical Center’s Academic Liaison and/or sponsor to obtain process instructions and aSchool Agreement Request Form.
5.1.3 Request for a new program or new school affiliation must meet the following criteria forconsideration:
5.1.3.1 There must be an identified need by the applicable Medical Center(s), DepartmentManager, or Director of Education for the program.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 2 of 8

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
5.1.3.2 Approving Department Manager is responsible for ensuring School meets KPSCaccreditation and curriculum standards and for oversight of unpaid field experience andtraining.
5.1.3.3 Once a School Agreement Contract is in place for the program, Schools will submit writtenrequest for Program Participant’s unpaid field experience and training program placementsto KP’s Academic Liaison and/or Sponsor.
5.1.3.4 Unpaid field experience and training program placement is based on space availability andat the discretion of the Department Administrator and/or Director of Education.
5.1.4 KP’s Academic Liaison and/or Sponsor will coordinate facilities for applicable approved programunpaid field experience and training programs.
5.1.5 The number of Program Participants accepted for a nursing unpaid field experience and trainingprogram will be limited to 10-12 per Faculty or as further limited by the KP Academic Liaisonconsistent with industry best practices and applicable regulations, if any.
5.1.6 Program Participant will not be allowed to participate in the unpaid field experience and trainingprogram unless requirements are met as set forth by this policy.
5.1.7 KP employees who are also Program Participants are required to complete their unpaid fieldexperience and training or rotation outside of their home unit.
5.1.8 KP employees who are adjunct Faculty of an affiliated School must not be Faculty on the sameunit/department where they work.
5.1.9 KP managers in Medical Centers or other locations are not permitted to sign agreements or sideletters, or to agree to terms or conditions of unpaid field experience and training program witheducation institutions, governmental agencies, placement firms, or individuals for any ProgramParticipant’s training program.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 3 of 8

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
5.2 Unpaid Field Experience and Training Program Coordination and Program Participant EligibilityRequirements:
5.2.1 KP SCAL Program Participants at KP facilities must be at least 18 years of age.
5.2.2 A valid School Agreement Contract, including current insurance requirements, must exist betweenthe School and KP during the time of a Program Participant’s placement in the unpaid fieldexperience and training program. The contract will be signed and maintained by the ND&A office.
5.3 Onboarding Process – See Appendix A
5.4 Faculty/School Accountabilities
5.4.1 The School is responsible for evaluating the Faculty’s competence. Faculty must hold a currentCalifornia professional health care license and a current AHA BLS, as appropriate. Documentationwill be available to KP for review upon request.
5.4.2 If Faculty is absent, a qualified substitute who has read, completed, and submitted all the Facultyand KP requirements, must be on duty to supervise the Students. If this is not possible, the unpaidfield experience and training will be cancelled for the day and Students will be directed to leave theKP Medical Center.
5.4.3 Prior to any unpaid field experience and training, the Faculty is responsible to define the Student’sscope of practice, level of capabilities, and limitations to the clinical staff as outlined in the studentsyllabus. A copy is to be provided to KP’s Academic Liaison and/or Sponsor.
5.4.4 Faculty ensures the orientation of the Students to the Medical Center as well as to the individualpatient care areas. The KP Sponsor may orient Students to the Medical Centers and patient careareas if the Student’s unpaid field experience and training does not require the Faculty to be onsite.
5.4.5 Dress code and hygienic practices – See Appendix B
5.4.6 Failure to comply to any provision in this section will result in immediate notification of the Facultyand Academic Liaison/Sponsor.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 4 of 8

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
5.5 Security Issues
5.5.1 Program Participants are required to wear a KP produced photo identification badge while at a KPFacility. Some Facilities may require the Program Participant to wear both the KP and Schoolphoto identification badge.
5.5.1.1 Exceptions to this section are permissible if KP allows the Faculty or Program Participantto wear only a School photo identification badge.
5.5.2 All badges are to be worn on the front upper torso and shall be clearly visible to observers;Including patients. Nothing is to be attached to the badge or cover any portion of the badge.
5.5.3 KP identification badges are the property of KP and are to be returned to KP’s Academic Liaison orSponsor on the last day of the unpaid field experience and training.
5.6 Medication Administration
5.6.1 A Faculty or authorized KP Staff Nurse must co-sign with Students for allowable medicationsadministered to KP patients.
5.7 Unusual Occurrences
5.7.1 KP will provide necessary emergency health care or first aid to an injured Program Participant orFaculty participating in affiliated Program(s) at the Facilities, consistent with KP Entities policiesand procedures pertaining to employees or visitors injured at a KP Facility.
5.7.2 KP Entities shall have no obligation to furnish medical or surgical care beyond emergency care orfirst aid to an injured Program Participant, or provide accident, health, or any insurance coveragefor the Program Participant.
5.7.3 If a Program Participant is injured in a KP Facility during their unpaid field experience and training,or during a visit to a non-Kaiser Facility, such as Home Health, the Program Participant will obtaintreatment at the nearest KP Medical Facility equipped to provide the necessary emergency care orfirst aid.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 5 of 8
SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
5.7.4 If the injured Program Participant is not near a KP Medical Facility equipped to provide thenecessary emergency care or first aid is stable for transport, KP personnel will make arrangementsto transport the Program Participant to the nearest KP Emergency Department.
5.7.5 If the injured Program Participant needs immediate emergency care, KP Personnel will call KP’sRapid or Ambulatory Response Team or 911.
5.7.6 All significant or unusual incidents during the unpaid field experience and training must be reportedimmediately: Faculty/School, KP Charge Nurse (if applicable), Department Manager, andAcademic Liaison and/or Sponsor
5.7.7 KP’s UOR must be completed by the KP Sponsor or appropriate department or unit manager.
5.7.8 The Academic Liaison and/or Sponsor shall notify the SCAL Regional Senior Contracts Manager ofthe UOR.
5.7.9 The Regional Senior Contracts Manager shall notify the Revenue Cycle Personnel of the incidentand inform them not to bill the Program Participant for the emergency care or first aid provided perKP Policy.
5.7.10 The Regional Senior Contracts Manager shall notify KP Legal and KP Risk Management of theincident.
6.0 References/Appendices
6.1 References6.1.1 The Joint Commission, HR.01.02.07 EP5 (www.jointcommission.org)6.1.2 Centers for Disease Control and Prevention (www.cdc.gov)6.1.3 Advisory Committee on Immunization Practices (www.cdc.gov/vaccines/acip/index.html)
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 6 of 8
SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
6.2 Related Policies
6.3 Appendices6.3.1 Appendix A: Onboarding Process6.3.2 Appendix B: Dress Code and Hygienic Practices
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 7 of 8
NATIONAL POLICY AND PROCEDURESPolicy Name/Website Topics ScopeDrug-Free Workplace NATL.HR.030Employment Screening NATL.HR.011Environmental, Health and SafetyNATL.EHS.001Pre-Employment Drug TestingNATL.HR.029Waiver of Fees for Do Not Bill Events NATL.HQCDE.007
REGIONAL POLICIES AND PROCEDURESPolicy Name/Website Topics ScopeIdentification Badges SCR.HPHO.96.1KP HR Policy CA.HR.5.02Obligations Regarding Confidentiality REGL.HR.001b
SERVICE AREA AND LOCAL POLICIES AND PROCEDURESPolicy Name/Website Topics Scope

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
7.0 Signature Lines
Appropriate Signature(s) on file of the senior regional leader(s) that approved the policy and procedure inaccordance with the SCAL regional policy and procedures guidelines.
Policy Title: Student Unpaid Field Experience and Training Policy Number: SC.QRM.PCS.026Regional Business Owner Title: Vice President, Regional Patient Care ServicesRegional Custodian Title:Development and Education
Director, Regional Professional Original Effective Date: 05/11/2018
Medical Center Business Owner Title: MCAT/MSAATMedical Center Custodian Title: Chief Nurse Executives;Education Director
Revision Effective Date:Page: 8 of 8

SOUTHERN CALIFORNIA (SCAL)Appendix A Regional Policy and Procedures
Page 1 of 41.0 Onboarding Process
1.1 All participating Schools agree to adhere to a standardized process for ProgramParticipant prerequisites.
1.1.1 Student/Faculty prerequisites website address:http://kpnursing.org/_SCAL/professionaldevelopment/orientation/index.html
1.1.2 Refer to Nursing Pathways website for Medical Center specific requirements.
1.2 Prior to the start of unpaid field experience and training, the School will verify and attest toKP in writing that the following information is on file for assigned Program Participants:
1.2.1 Criminal Record Search (Background Check): A criminal record check (felonyand misdemeanor) encompassing the seven (7) years preceding the start of theirunpaid field experience and training will be conducted for all Faculty and ProgramParticipants unless a greater or lesser search period is permitted or required bystate law as per KP policy. If a Program Participant is convicted of a crime duringtheir unpaid field experience and training, it is the School’s responsibility to notifyKP within five (5) business days. The Program Participant’s return to the unpaidfield experience and training will be determined by KP. Background screeningperformed by the vendor is valid for 90 days.
1.2.2 Drug Testing: Faculty and Program Participants will be tested for the followingsubstances: amphetamines, benzoylecgonine (cocaine), cannabinoids, opiates,phencyclidine (angel dust), barbiturates, benzodiazepines, propoxyphene,methadone, oxycodone, and meperidine (Demerol). Drug testing is valid for 90days.
1.2.3 If a Program Participant shows signs of being under the influence during theirunpaid field experience and training in a KP Facility, the incident must be reportedimmediately to the Faculty/School and the KP Department Manager or Sponsor.The Faculty will remove the Program Participant from the patient care area andfollow necessary school protocol to dismiss the Program Participant from thepremises.
1.2.4 Factors which may establish a reasonable suspicion include, but are not limited to:
1.2.4.1 Sudden unexplained changes in behavior which adversely impact workperformance.
1.2.4.2 Discovery of presence of alcohol or drugs in a Program Participant’spossession or near the Program Participant’s workplace.
1.2.4.3 Odor of alcohol and/or residual odor suspicious for alcohol or drugs.
See also 1.2.7
See also 1.2.7from the start of the Program.
Page 2 of 4
1.2.4.4 Personality changes or disorientation.
1.2.4.5 Violation of safety policies, involvement in an onsite accident or nearaccident, in combination with any of the above factor(s).
1.2.5 All significant or unusual incidences during the unpaid field experience and trainingmust be reported to the Department Manager, the Academic Liaison/Sponsor, anddocumented on the KP Unusual Occurrence Report (UOR) system.
1.2.6 Regional Contracts Manager for KPSC School Agreements must be notified of theUOR.
1.2.7 The initial background check and drug screening will satisfy the screeningrequirement during continuous matriculation of the Faculty and ProgramParticipant for the duration of their participation in the unpaid field experience andtraining. If the Faculty/Program Participant discontinues participation in theprogram for more than one consecutive semester, a new background check anddrug screening will be required.
1.2.8 A current American Heart Association (AHA) Basic Life Support (BLS) certificationis required.
1.2.9 Immunizations are current to include:
1.2.9.1 Tuberculosis Screening (TB) - Screening may include the following:Tuberculin Skin Test (TST) or Interferon-Gamma Release Assays (IGRA)which encompasses QuantiFERON-TB Gold (QFT) and T-SPOT.Program Participants must present proof of documented negative or non-reactive TST or IGRA history. TST requires two (2) negative or non-reactive results dated within the previous 12 and 24 months of assignmentto a Facility. A single negative IGRA within 12 months is also acceptable.If neither is available, then a 2-step TST or IGRA is required. ProgramParticipants with a history of positive or reactive TST are required topresent documentation of positive screening test or history of INH or otherTB therapy and a written report of a negative chest x-ray within one (1)year of the beginning of their current academic program and proof thatProgram Participants have completed annual TB questionnaires. They arenot required to have follow up chest x-rays unless there is a positiveresponse to the symptom review on the annual TB questionnaire. Morerecent screening may be required if clinically appropriate.
1.2.9.2 Measles, Mumps, and Rubella (MMR) - A documented positiveserological immunity or two (2) documented immunization records signedby a qualified health provider is required per the Centers for DiseaseControl and Prevention (CDC) guidelines and the Advisory Committee onImmunization Practices (ACIP) recommendations. Vaccination ismandatory if non-immune or no vaccine record.
Page 3 of 4
1.2.9.3 Varicella Zoster - A documented positive serological immunity or two (2)documented immunization records signed by a qualified health provider isrequired per CDC guidelines and ACIP recommendations. Vaccination ismandatory if non-immune or no vaccine record.
1.2.9.4 Hepatitis A - Hepatitis A is required for Program Participants whose mainduties involve food preparation or serving food within any KP Facilities.Immunity demonstrated by positive Hepatitis A antibody titer ordocumentation of two (2) vaccinations as required per CDC guidelinesand ACIP recommendations
1.2.9.5 Hepatitis B - Immunity demonstrated by a positive Hepatitis B antibodytiter or documentation of three (3) Hepatitis B vaccinations as required perCDC guidelines and ACIP recommendations.
1.2.9.6 Seasonal Flu Vaccine - Proof of Flu Vaccination during the current FluSeason must be presented to Kaiser Facilities by Program Participantbefore starting the program. If current seasonal flu vaccine is not availableat the start of the rotation (July or August), documentation must beprovided as soon as the current season’s flu vaccine is received.
1.2.9.7 Pertussis (Whooping Cough) - A TDaP immunization record signed by aqualified health provider must be provided to Kaiser Facilities by ProgramParticipant before starting the program as required per CDC guidelinesand ACIP recommendations.
1.2.9.8 Other - Other immunizations and health screenings, as required by law orreasonably requested by Kaiser Entities in accordance with KaiserEntities’ applicable policies and procedures, may be unilaterally amendedby Kaiser Entities by a written notice to the School.
1.2.9.9 Declinations - Immunization declinations will not be accepted at anyKPSC Facility.
1.3 Faculty whose classifications require current California professional licensure orcertification must provide proof to KP in writing.
1.4 KP HealthConnect Access – Program Participants, who are expected to document in thepatient’s electronic medical record, must submit the Common Provider Master (CPM) formto KP at least four (4) weeks prior to the start of the unpaid field experience and training toobtain access to the HealthConnect documentation system.
1.5 KP HealthConnect Training – The School will facilitate access to approved KPHealthConnect training.
Page 4 of 4
1.6 Program Participants will read, complete, and submit all prerequisites prior to the start ofthe unpaid field experience and training.
1.7 Faculty must verify the completion of the prerequisites as stated in this policy. KP mayvalidate compliance by auditing Student files.

SOUTHERN CALIFORNIA (SCAL)Appendix B Regional Policy and Procedures
Page 1 of 21.0 Dress Code and Hygienic Practices
1.1 Students are required to wear their approved School uniform. If the School does not havea uniform requirement they should wear appropriate professional attire:
1.1.1 Undergarments shall be selected with regard to color of outer clothing and noportion of the undergarments may be visible at any time.
1.1.2 No jeans, hoodies, low necklines or visible midriffs may be worn.
1.1.3 Hats, caps, and accessorized head coverings are not permitted.
1.1.4 Closed toe shoes appropriate for the clinical settings must be worn at all times.
1.2 Hair must be kept clean, neat, and well-groomed and should not obstruct eye to eyecontact or create a health /safety hazard. Long hair should be secured back. Hair color andstyles may not be extreme or serve as a distraction to others. Facial hair must be clean,neatly trimmed and sideburns must be no longer than the bottom of the earlobe.
1.3 Tattoos shall be covered.
1.4 Fingernails:1.4.1 The natural nails of healthcare workers are to be kept short, i.e. not extending
beyond the tips of the fingers. Any nail polish must be intact, not chipped.
1.4.2 All artificial nail enhancements including but not limited to: nail tips, jewelry, gels,wraps, etc. are prohibited for all health care workers and providers who providedirect, “hands-on” patient care, across the continuum of care, including but notlimited to: inpatient (including Perinatal services, Labor and Delivery, Post-Partum, Nursery), ambulatory and home care, invasive or diagnostic proceduresor therapies, Laboratory Services, Perioperative Services, Sterile ProcessingDepartment, Intensive care units (adult, pediatric newborn), etc. Other workersinvolved in aseptic procedures or who have contact with the patient environment,etc. must also comply e.g. pharmacy, food handlers, EVS, Social Workers.
1.5 Jewelry:
1.5.1 Only a wedding or simple ring is acceptable and must be limited to one per hand.
1.5.2 Single, short necklace appropriate for the healthcare setting.
1.5.3 No bracelets are permitted. Watches are acceptable.
1.5.4 Exposed pierced facial jewelry must not be worn.
1.5.5 Ear piercings are permitted as follows:

Page 2 of 2
1.5.5.1 No more than two (2) studs per ear
1.5.5.2 Ear stretchers no greater than two (2) millimeters in diameter.
1.5.5.3 Unit protocol may supersede listed permissible items.
1.6 Personal cleanliness is required. Regular baths, showers, use of underarm hygienicproducts, clean teeth and nails are essential.
1.7 Perfumes, colognes, scented lotion, after shave lotion, and body sprays are not to beused.
1.8 Makeup must be appropriate and should not serve as a distraction. Artificial eyelashes are not permitted to ensure patient safety.
1.9 No food, gum/candy or drink allowed in patient care areas.
1.10 Kaiser is a no smoking campus including parking lots and campus sidewalks. Smokersshould refrain from smoking prior to any patient care.

Human Resources
1.0 Policy StatementKaiser Permanente (KP) is committed to protecting the safety, health and well-being ofemployees and other individuals in KP’s workplace and provides an environment that is freefrom the abuse of alcohol and drugs. KP recognizes that alcohol abuse and drug use pose asignificant threat to KP’s goals. KP also acknowledges that alcohol abuse and chemicaldependency may be chronic diseases that require rehabilitative treatment, counseling, and/oraccess to employee assistance programs.
2.0 PurposeThis policy is consistent with requirements of the federal Drug-Free Workplace Act of 1988,applicable state drug-free workplace requirements, and with KP’s obligation to provide a safework environment.
3.0 Scope/Coverage3.1 This policy applies to all employees working in any of the following entities
(collectively referred to as “Kaiser Permanente”):3.1.1 Kaiser Foundation Hospitals and Kaiser Foundation Health Plan, Inc.
(together, KFH/HP);3.1.2 KFH/HP’s subsidiaries;3.1.3 The Permanente Medical Group, Inc. (TPMG) [NOTE: This policy does not
apply to physicians, podiatrists or Vice Presidents of TPMG, who are coveredby separate TPMG policies]; and
3.1.4 Southern California Permanente Medical Group (SCPMG) [NOTE: This policydoes not apply to physicians of SCPMG].
3.2 All organizations who supply temporary or registry personnel, students or trainees toKP will be held accountable for providing personnel who meet the same drug-freestandard imposed by KP on its own employees. Volunteers are also required to meetthis drug-free standard. Violation of applicable provisions or refusal to cooperate inthe implementation of this Policy can result in contract personnel or volunteers beingbarred from company premises or from working in its operations.
3.3 Employees whose jobs require them to drive KP fleet vehicles are subject to the drugand alcohol testing requirements in the applicable Fleet Management policies. Inaddition, employees whose jobs require commercial driver’s licenses are subject to adrug and alcohol testing program that fulfills the requirements of the U.S.Department of Transportation (DOT) Regulations. (See the Addendum toREGL.HR.02a and REGL.HR.02b, Drug and Alcohol Testing.)
4.0 Definitions4.1 Alcohol – means ethanol alcohol in any consumable form (e.g., beer, wine, liquor).
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR PolicyRoundtable
Page: 1 of 7

Human Resources
4.2 Being under the influence – means an individual is impaired by alcohol or a drug,or the combination of alcohol and drugs, regardless of the level detected. Adetermination of “under the influence” can be established by a professional opinion,a medically accepted drug or alcohol screening test, and/or based on layobservations by supervisors, co-workers, or others.
4.3 Company premises -- includes parking lots, vehicles and other facilities andproperty owned, leased or operated by KP, as well as off-site premises used forcompany-sponsored events.
4.4 Drug -- means:4.4.1 any drug which is not legally obtainable: any “illicit” drug or “controlled
substance” the possession or use of which could result in arrest or otherlegal sanction according to state or federal statute. Examples include but arenot limited to, marijuana, cocaine, crystal methamphetamines (ice), andhallucinogens. [NOTE: Although "medical marijuana" or marijuana use lawsmay exist in some states, because marijuana is a Schedule I drug andpossession or use of it is unlawful under federal law, marijuana is an illicitdrug for all purposes under this policy.];
4.4.2 any drug which is legally obtainable but has not been legally obtained;4.4.3 prescribed drugs not being used for prescribed purposes or at prescribed
dosages; and/or4.4.4 any non-prescription substances that are used contrary to manufacturer’s
recommendations.4.5 Work Time -- time during which an employee is representing or conducting
business for KP, or is required or scheduled to be on duty.
5.0 Provisions5.1 Pre-Employment Drug Testing
In accordance with NATL.HR.029, Pre-Employment Drug Testing, KP requires that allindividuals external to KP who have been offered employment complete pre-employment drug testing demonstrating the absence of illegal drugs or prohibiteduse of legal drugs.
5.2 Employees with Drug and Alcohol Problems5.2.1 KP supports the use of treatment and programs to address alcohol or drug
abuse and will provide them when warranted by conditions andcircumstances. However, KP must balance respect and concern forindividuals experiencing these problems with KP’s commitment to maintainan alcohol and drug-free environment. KP encourages employees tovoluntarily seek help with drug and alcohol problems. (See Addendum forCalifornia employees.)
5.2.2 KP encourages any employee covered by this policy who is experiencingalcohol or drug dependency to seek professional assistance, including the
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 2 of 7

Human Resources
use of KP’s confidential Employee Assistance Program. Whenever practical,KP will assist employees in overcoming drug, alcohol, and other problemswhich may affect employee job performance, provided that such assistanceis requested prior to violation of this policy.
5.2.3 Employees' voluntary participation in chemical dependency recoveryprograms or other rehabilitation services will be kept confidential and will notaffect their employment as long as they are meeting the terms andconditions of the program. Both KP policy and existing laws protect theconfidentiality of persons who seek treatment for chemical dependency.
5.2.4 Depending on the circumstances, an employee’s return to work,reinstatement, and/or continued employment may be conditioned on theemployee's successful participation in and/or completion of any and allevaluations, counseling, treatment, rehabilitation programs, or otherappropriate conditions as determined by KP.
5.3 Employees Taking Prescribed MedicationThe use of prescribed medication at prescribed dosages and for prescribed purposesunder the direction of a physician or other appropriate licensed person on either along-term or short-term basis may affect the safety of the employee, co-workers ormembers, the employee's job performance, or the safe or efficient delivery ofservices. Therefore, any employee who experiences an impairment of performancethat could impact his/her work duties due to the use of such medication (e.g., visionimpairment, lack of balance, loss of reflexes, impaired judgment) must report this tohis or her supervisor. If the use of such medication affects the safety of theemployee, co-workers or members, the employee's job performance, or the safe orefficient delivery of services, the employee may be required to be away from worktemporarily using sick leave, PTO, ETO, medical leave, personal leave, or other timeoff benefits.
5.4 Prohibited Conduct and Penalties5.4.1 It is a violation of this policy to use, possess, sell, purchase, trade, and/or
offer for sale or to purchase drugs (as defined in this policy) during worktime or at any time on KP premises. Being under the influence of a drug byany employee on KP premises or during work time is prohibited.
5.4.2 Being under the influence of alcohol by any employee while on KP premisesor during work time is prohibited. The consumption, sale, purchase, or offerfor sale or to purchase of alcohol on KP premises is prohibited. Possessionor transfer of an open container of alcohol on KP premises is a violation ofthis policy, except in circumstances in which consumption of alcohol isspecifically authorized at a KP sponsored or sanctioned function.
5.4.3 Being at work and failing to report to the supervisor that prescribedmedication is impairing the employee’s motor functions is a violation of thispolicy.
5.4.4 Theft, diversion or unauthorized removal of drugs maintained or dispensedon KP premises is a violation of this policy.
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 3 of 7

Human Resources
5.4.5 It is a violation of this policy for employees to unlawfully manufacture,distribute, dispense, possess, sell, purchase, or use an illegal drug while offduty or off premises, where the conduct adversely affects the employmentrelationship or KP’s business interests.
5.4.6 Violation of this policy will subject employees to corrective/disciplinary action,up to and including termination of employment, and may result in a referralto law enforcement agencies for possible criminal prosecution.
5.5 Notification of Convictions5.5.1 Any employee who is convicted of a criminal offense for a drug violation
must, as a condition of employment, notify Human Resources within fivedays of that conviction. Failure to provide timely notification will result incorrective/disciplinary action, up to and including termination of employment.
5.5.2 Federal contracting agencies will be notified of employee convictions whenappropriate.
5.6 Reasonable Suspicion of Prohibited Alcohol or Drug Use5.6.1 A supervisor may have a “reasonable suspicion” that an employee is under
the influence based upon observation of conduct and/or events. Factorswhich may establish reasonable suspicion include, but are not limited to:5.6.1.1 Sudden unexplained changes in behavior which adversely impact
work performance.5.6.1.2 Discovery or presence of alcohol or illegal drugs in an
employee’s possession or near the employee’s work space.5.6.1.3 Odor of alcohol and/or residual odor peculiar to alcohol or
controlled substances.5.6.1.4 Personality changes or disorientation.5.6.1.5 Violation of safety policies, or involvement in an on the job
accident or near accident.5.6.2 When reasonable suspicion has been established to indicate an employee is
under the influence of alcohol or drugs, the employee will be asked, at thesole discretion of management, to provide breath, blood and/or urinespecimens for laboratory testing. Employees are required to follow regionalpolicies/procedures regarding drug and alcohol testing. (See REGL.HR.02aand REGL.HR.02b, Drug and Alcohol Testing.)
5.6.3 Where there is reasonable suspicion that employees possess or theirpersonal effects (including vehicles, purses, briefcases, clothing, personalcontainers) contain an illegal drug or an open container of alcohol, KP may,with consent, search such individuals or their personal effects. Refusal toconsent to such searches may be considered insubordination (seeNATL.HR.014, Corrective/Disciplinary Action). Illegal drugs which areconfiscated will be turned over to local law enforcement agencies.
5.7 Confidentiality
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 4 of 7

Human Resources
KP recognizes the importance of maintaining confidentiality in any situation wherecurrent and former employees covered by this policy are suspected of alcohol or drugrelated infractions. Every effort will be made to assure the privacy of suspectedemployees throughout investigatory and corrective/disciplinary action proceedings.
5.8 Policy AttestationAt a minimum, this policy is communicated and reviewed at New EmployeeOrientation. New employees are required to sign an attestation that theyacknowledge, understand, accept, and agree to comply with this policy, and thatthey understand that failure to comply with this policy may result incorrective/disciplinary action up to and including termination.
5.9 State RequirementsIn addition to the federal requirements regarding a drug-free workplace some stateshave related laws or statutes that KP must comply with in applicable regions (e.g.,see Addendum).
5.10 Additional Employee Obligations and ResponsibilitiesEmployees who abuse drugs and/or alcohol often affect the performance of otheremployees. KP cannot provide quality health care without the cooperation andassistance of all employees. As discussed in the "Principles of Responsibility”,employees who observe activities prohibited by this policy are responsible for alertingtheir supervisors or whatever management is necessary to resolve the issues.Failure to report violations may result in corrective/disciplinary action.
6.0 References/Appendices6.1 Addendum – Alcohol & Drug Rehabilitation for California employees6.2 Drug-Free Workplace--Employee Acknowledgement6.3 REGL.HR.02a and REGL.HR.02b, Drug and Alcohol Testing6.4 NATL.HR.011, Employment Screening6.5 NATL.HR.014, Corrective/Disciplinary Action6.6 NATL.HR.029, Pre-Employment Drug Testing
6.7 Employee Assistance Program: http://xnet.kp.org/hr/ca/eap/index.htm6.8 Federal Drug-Free Workplace Act of 19886.9 California Drug-Free Workplace Act of 19906.10 Cal Govt Code § 8355 et seq.6.11 Virginia Drug-free Workplace Act6.12 Virginia Code § 2.2-4312
7.0 Approval
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 5 of 7

Human Resources
Update approval 7/21/17In accordance with the charter of the National HR Policy Roundtable, this policy update wasapproved by the National HR Policy Roundtable members, as chaired by Derek Reimer.
Policy Revision History
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 6 of 7
Original Approvals Update Approvals Revision Approvals
Approval Date: 1/28/10Approval Date: 10/30/12;11/29/12; 4/30/15; 7/21/17
Approval Date: 9/9/10
Effective Date: 4/5/10Effective Date: 10/30/12;11/29/12/ 4/30/15; 8/1/17
Effective Date: 11/3/10
Communicated Date: n/a Communicated Date: n/a

Human Resources
Addendum
Alcohol & Drug RehabilitationFor employees working in California
Time OffEmployees may take time off work to voluntarily enter and participate in an alcohol or drugrehabilitation program. The amount of time off must be reasonable and not create an unduehardship on KP operations.Nothing in this policy prohibits KP from refusing to hire or discharging an employee due tocurrent use of drugs or alcohol, inability to perform his or her duties due to drug or alcoholuse, or inability to perform his or her duties without endangering the health or safety of theemployee or others.
EligibilityAny employee who voluntarily enters and participates in an alcohol or drug rehabilitationprogram.
Notice & Documentation RequirementsTime off for this purpose will be granted if an employee provides reasonable notice of therequest and a doctor’s note to his/her manager. In the alternative, the employee mayprovide notice to his/her local Human Resources Representative.
Paid or Unpaid Time OffEmployees are required to use available paid time off for this purpose (sick leave, vacation,Paid Time Off or Earned Time Off) before taking leave without pay.
ConfidentialityAny records and information regarding an employee’s absence for participation in an alcoholor drug rehabilitation program will be maintained as confidential. Managers and supervisorswill take all reasonable steps to safeguard the privacy of an employee regarding participationin an alcohol or drug rehabilitation program.
Law/statuteCalifornia Labor Code, Sections 1025-1028
Proprietary Information. Kaiser Permanente. All rights reserved.
Policy Title: Drug-Free Workplace Policy Number: NATL.HR.030Owner Department: Human Resources Effective Date: 8/1/17Custodian: Chair, National HR Policy Roundtable
Page: 7 of 7

HIPAA 101: Privacy and Security Basics
HIPAA 101: Privacy and SecurityBasicsPurpose
2. The information is related to past, presentThis document provides important informationor future health care or payment for thatabout Kaiser Permanente (KP) policies andhealth care.state and federal laws for protecting the privacy
and security of individually identifiable member 3. The information identifies a member orand patient information. You are responsible for patient, or there is enough information to beunderstanding this information and any able to identify the individual.additional information you need to comply withall laws and policies that affect your job. Only health information about an individual that
is linked to that individual by an identifier isIn most cases, you have received this protected health information.information because you are a “limited timeworkforce member”—you work or volunteer at Health information that is not linked to anKP less than 160 hours/year. However, if your individual by one or more of 18 HIPAAjob description or contract requires you to identifiers and for which there is no reasonableroutinely receive, access, create, use or
basis to believe that the information can bedisclose member and patient information, youused to identify the individual is not protectedmust take additional privacy and securityhealth information.training. Contact your contract manager or
supervisor immediately to enroll in KP GeneralCompliance Training for New Employees web- Removal of all 18 HIPAA identifiers means thebased or instructor-led training for new information is de-identified and no longeremployees. protected health.
Individually identifiable health informationWhat is HIPAA?ceases to be PHI 50 years after death.HIPAA – is the Health Insurance Portability and
Accountability Act and requires all KPworkforce members, regardless of job title or Individually identifiable information, even if nothours worked, to understand the risks and PHI, may still be subject to other state andsafeguard the privacy and security of federal privacy protections.individually identifiable information of ourmembers and patients. What Does This Mean to Me?
You are expected to be able to:What is PHI? 1. Recognize PHI that requires protection.For information to be considered PHI, it must 2. Determine when it is permissible to access,meet all of the following three conditions: use or disclose PHI.1. The information is created, received, or 3. Reduce the risk of impermissible access to,
maintained by a health provider or health use or disclosure of PHI.plan.
1 kp.org/compliance

HIPAA 101: Privacy and Security Basics
There are other uses and disclosures whereWhen it is permissible to access or usepatient authorization is not required, including:PHI?§ Appointment reminders – PHI may beOnly access, use or disclose PHI if your job used to contact members and patients
allows you access and that access is required about appointments for health care andfor your job. treatment.
§ Business Associates – PHI may be usedby KP’s contracted business associates ofWhat Uses or Disclosures of PHI Area Kaiser Permanente regional Health Plan,Permitted by Law? hospital or of one of the regional
HIPAA allows a KP workforce member to Permanente Medical Groups to performcreate, receive, access, use, or disclose PHI certain functions on KP’s behalf. Business
associates must sign a business associatewithout patient authorization when theagreement with the regional Health Plan orworkforce member’s job duties involve certainthe regional Permanente Medical Groupactivities. These activities include, but are notand agree to safeguard KP member andlimited to: patient PHI.
§ Health care treatment—the treatment team § Communications with family and otherscan use PHI to provide, coordinate, or when the member or patient is present -manage health care and related services, PHI may be discussed in the presence of aincluding consultation between health care family member or other person involved inproviders of an individual, and referral of a the member’s or patient’s care, but make
sure the member or patient does notpatient for health care from one provider toobject.another provider for treatment. However,
§ Communications with family and othersUNLESS the provider is directly involved inwhen the member or patient is notthe care of the patient, and needs thepresent - PHI may be disclosed to a familyinformation for treatment, a health caremember or other person involved in theprovider can not access, use, or disclose member or patient’s care when there is anPHI for other purposes—such as to check emergency, the member or patient is noton the health care status of a colleague or present, or the member or patient lacks
friend or family member, without the the decision making capacity to agree orpatient’s specific authorization. object to the disclosure. Use professional
judgment to determine if it is in the§ Health care or health plan payment —PHImember or patient’s best interest tocan be used for premium payment, billing,disclose their PHI to a family member, andclaims management, utilization review, limit the disclosure to the PHI that iscoordination of benefits, eligibility and/or directly relevant to the person'scoverage determinations, and collection involvement with the member or patient’s
activities. health care.§ Health care or health plan operations— § Marketing - PHI can be used to contact
PHI can be used for quality assessment, members about KP benefits, and certainhealth-related products or services thatcase management, population-basedadd value to, but are not a part of, the planactivities such as disease management,of benefits offered to a KP member.accreditation, underwriting, legal and audit
functions, fraud and abuse protection andcompliance, and business management.
2 kp.org/compliance

HIPAA 101: Privacy and Security Basics
§ Facility Directories – PHI can be used to How Can I Help Prevent Breaches ofcreate directories that include patient PHI?names, room locations, general medical A breach is the unauthorized acquisition,conditions, and religious affiliation. Room access, use, or disclosure of PHI thatlocation, and general medical condition compromises the privacy or security of the PHI.may be disclosed to any person who asks We are all responsible for protecting ourfor the patient by name. All of this members’ and patients’ confidentialinformation, including religious affiliation, information. If a breach occurs, immediatelymay be disclosed to members of the notify your manager/supervisor, complianceclergy, if the patient has not restricted this officer, or privacy and security officer.disclosure. Patients have the right toobject to the use and disclosure of some
Do Not Peekor all of this information; if so, KP will notdisclose the information to visitors or other § No matter how curious you might bemembers of the public. regarding the health of a coworker, a friend,
a celebrity, or a family member, do notaccess a medical record unless you areOther uses and disclosures require prior written authorized to do so.authorization. If you are not sure about whether
§ Never access or discuss a fellowor not you can use or disclose PHI, check withemployee’s PHI unless it is for purposesyour manager/supervisor, compliance officer,allowed by law and required for your jobor privacy and security officer.
Think Twice When You Talk About PHIWhat Uses or Disclosures of PHI are§ Do not discuss patient information at homeProhibited by Law and KP Policy?
or outside of work, including who you saw as§ When you stop doing work for KP — eithera patient.as a KP employee, vendor or contractor—
§ Avoid discussing PHI in public areas,you may not remove, make copies of orincluding talking on a cell phone wherecontinue to use, access, receive, or discloseothers may overhear.KP PHI. Doing so is a violation of the law
and KP policy. § Lower your voice when you must share PHIin areas where others might overhear.§ If you are a contractor, you may not copy,
use, or disclose KP PHI for any purpose § If possible, close the door when consultingother than specifically allowed in your with patients and/or family members orBusiness Associate contract. If you when dictating.inadvertently access or disclose PHI in ways § Be sure to ask the patient in advance if it isnot allowed in your contract, the law requires acceptable to speak with his or her familyyou to immediately report the disclosure to members.your supervisor or contract manager, andyour company to report the breach to KP.
3 kp.org/compliance

HIPAA 101: Privacy and Security Basics
Prevent Unauthorized Access to Facilities Protect the Privacy of PHI in Printed orand Secure Areas Written Documents§ When you are at work, wear your KP ID § Check to make sure that you are giving the
badge and be sure it is prominently correct paperwork to the right member ordisplayed. patient. Examples include after-visit
summaries, discharge instructions,§ Notify Security if you notice someonemedication bottles or packages, andwithout an ID/card badge in a restrictedpharmacy inserts. Many incidents are paperaccess area. Ask the individual, “May I helprelated and preventable.you?” or “You seem to be lost”, and then
direct them to Security to obtain a temporary § Keep paper medical records out-of-sight,badge. and in locked storage areas. Access to
these areas should be limited to those§ Keep doors locked and restrict access toindividuals with designated rights of access.areas where sensitive information or
equipment is kept. § Always double check the fax number beforesending a fax. Use a cover sheet with a§ Do not post keypad access codes.confidentiality statement when transmitting§ Shield the key strokes when entering anfaxes containing PHI.access code to prevent others from seeing
§ Place machines that process PHI in securethe code.areas.§ Follow the same guidelines for facility
§ Check fax machines, printers, copiers, andaccess as you would for password, includingmailboxes frequently to retrieve PHI.changing codes periodically; using complex
codes that are not obvious; not sharing your § Cover, put away, or turn over paperworkaccess code or access badge; and, not with PHI.allowing others to use your access rights to § Use cabinets with locks to store cameras,enter a facility or secure area. and printed or written documents containing
§ Do not allow others to “tailgate”, or follow PHI.you into a restricted area. Each employee § Use a shredder or confidential destructionmust have a badge to enter restricted areas, bin when disposing of PHI.or otherwise be directed to Security to obtain § When creating training and presentationa badge. materials, including screen shots, remove
§ Turn in your badge and keys to your patient identifiers so the materials do notsupervisor or HR when you leave KP, or are display PHI.transferred to another KP job where yourcurrent ID badge will not be re-used.
4 kp.org/compliance

HIPAA 101: Privacy and Security Basics
Provide Physical Security for PortablePrevent Unauthorized Access to andComputing and Storage DevicesDisclosure of Electronic PHI§ Store confidential information such as PHI§ Create complex passwords with a minimum
on KP’s secured network severs. Neverof eight characters--at least one number, store PHI on a laptop or other portable,symbol and/or one letter. Use a mixture of endpoint device unless you have specificcapital and lower case letters. Do not use approval from your supervisor andconsecutive identical characters or all Regional Leadership. If granted, the mobilealphabetical groups or consecutive device must have encryption softwarecharacters on the keyboard (e.g., aaaaaa, installed. If you have been approved to use
and store PHI on a portable, end-point111111, qwerty).computing device— e.g., a laptop, PDA, cell§ Do not use actual words (e.g., Kaiser, phone, hand-held device, mp3 player, flashpassword). or jump drive, CD or DVD, etc.—you should
§ Do not use your individual identifiers obtain the Privacy and Security training that(names, driver’s license number, Social is required for all workforce members. See
your supervisor or contract managerSecurity number).immediately about the training.§ If you suspect your password has been
§ Know where your portable devices (laptop,compromised or misused, you shouldPDA, cell phone, hand-held device, mp3immediately change the password, and player, flash or jump drive, CD or DVD, etc.)report the incident to your supervisor. are at all times. Never check them as
§ Do not share or post passwords or user IDs baggage or leave them unattended oron your computer. If someone asks to use unsecured at home, work, or in transit.your password, report it to your supervisor. § Whenever you leave your work area, make
sure your laptop is secured by a locking§ Use a password, and secure or lock yourcable, or securely locked in the dockingworkstation, before stepping away andstation.leaving it unattended for any period of time
§ If you are leaving for the day, take the laptop§ If you share a workstation, only use your or other device with you or lock it in a desk
own password and logon ID to access data. or cabinet.Log-off when you are finished. Never share § If your device is stolen or lost, immediatelyyour passwords with other users; you could report the loss to your manager/supervisor.be held responsible if an unauthorized § If the lost or stolen device contained PHI—person uses your logon or password to encrypted or unencrypted—you must reportaccess or disclose PHI. the loss of the data immediately to your
regional privacy and security officer or§ Turn your computer screen away fromcompliance officer.viewing by visitors if you work in an open
area. If PHI is frequently displayed on yourscreen, install a “privacy screen” to protectthe display.
5 kp.org/compliance
HIPAA 101: Privacy and Security Basics
Secure PHI in email and email Attachments Violating KP policies, federal regulations, andstate laws and regulations can lead to§ Encrypt all emails containing PHI that aredisciplinary action – up to and includingsent from an internal KP.org address to atermination, personal fines, civil and criminalnon-kp.org external address (e.g.,penalties and suspension of professionalyahoo.net). Lotus Notes users can use thelicenses“Send Secure“ function, which automatically
encrypts the email message.§ If your Lotus Notes does not have the “Send You are responsible for understanding this
Secure” button, you can encrypt an email by information and any additional informationincluding any of the two “keywords” in the necessary to comply with all laws and policiessubject line, with either parentheses or that affect your job.brackets around the word. A keyword can becapitalized or lower case: If you have questions about what you must do,§ PHI (phi), {PHI}, [phi] consult with your supervisor, contract manager,§ Encrypt (encrypt), {encrypt}, [ENCRYPT] local KP compliance officer or KP regional
privacy and security officer. You can also§ Use Secure File Transfer to send large filesaccess KP privacy and security information atsecurely to both internal and externalkp.org/compliance.addresses.
§ Never open attachments in email messagesfrom people you don’t know or can’t identify. Appendix – HIPAA Identifiers
§ Always double-check the address line(s) “HIPAA identifiers” means any of the followingbefore sending an email message to ensure identifiers, either of the individual or of his/herit’s going to the right party. If you send an relatives, employers or household members:email containing PHI to the wrong § Names.addressee, report the mis-mailing
§ All geographical subdivisions smaller than aimmediately to your manager/supervisor and State, including street address, city, county,privacy and security officer. precinct, zip code, and their equivalent§ Do NOT rely on the Lotus Notes functionality geocodes, except for the initial three digits of
to accurately auto fill or auto-populate the a zip code, if according to the currentaddress lines. Instead, use the Lotus Notes publicly available data from the Bureau ofaddress book and select the name of each the Census: (a) The geographic unit formedintended recipient. by combining all zip codes with the same
§ If you must use a distribution list to send three initial digits contains more than 20,000PHI, verify the names on the list as each people; and (b) The initial three digits of ahaving a need to receive the email. Take a zip code for all such geographic unitscritical view of any email address that is not containing 20,000 or fewer people iswithin Kaiser Permanente’s email system. changed to 000.
6 kp.org/compliance

HIPAA 101: Privacy and Security Basics
§ All date elements (except year) for datesdirectly related to an individual, including ofbirth date, an admission or discharge date,date of death; and all ages over 89 and anydate (including year) indicative of such age,however such ages and elements may beaggregated into a single category of age 90or older.
§ Telephone numbers.§ Fax numbers.§ Email addresses.§ Social Security numbers.§ Medical record numbers.§ Health plan beneficiary numbers.§ Account numbers.§ Certificate/license numbers.§ Vehicle identifiers and serial numbers,
including license plate numbers.§ Device identifiers and serial numbers.§ URLs.§ Internet protocol address numbers.§ Biometric identifiers including finger and
voice prints.§ Full face photographic images and any
comparable images.§ Any other unique identifying number,
characteristic, or code (provided that (a) thecode or other record identifier is not derivedfrom or related to other information (forexample scramble MRNs and SSNs are notpermitted) and not otherwise translatable toidentify the individual; (b) the covered entitydoes not use or disclose the code or otherrecord identifier for any other purpose; (c)and the covered entity does not disclose themechanism for re-identification.
7 kp.org/compliance

Prevent Fraud, Waste, and Abuse
Prevent Fraud, Waste, and AbuseAre There Fraud Laws and RegulationsFraud, waste, and abuse (FWA) puts ourYou Should Know About?patients at risk and increases the cost of health
care for us all. It is everyone’s responsibility to Yes. The federal government has regulationsto control fraud and abuse in healthcare. Thesafeguard our organizational assets. OurFederal False Claims Act and similar state lawsnational Fraud, Waste, and Abuse policymake it a crime to present a false claim to thearticulates Kaiser Permanente’s (KP)government for payment. If your role includescommitment to “do the right thing.” Find outcoding and documentation, accuracy is criticalmore at the National Compliance, Ethics &to avoid a false claim. These laws also protectIntegrity Office website at kp.org/compliance.whistleblowers — people who report fraud orwho assist in investigations. KP prohibitsretaliation of any kind against individuals whoWhat Is Fraud?in good faith report or participate in theFraud occurs when someone misrepresents investigation of non-compliance or fraud, waste
the truth to get a benefit or advantage. or abuse.
Example: Using another person’s medical What Are Red Flags?identity to receive treatment or submitting A red flag is a pattern, practice, or activity thatreceipts for personal expenses for business indicates possible fraud. A common example isreimbursement when a person checks in without photo
identification. This may be a red flag for identitytheft. The staff checking in the patient must
What Is Waste? then take appropriate steps to validate thepatient’s identity.Waste is the extravagant, careless, or needless
expenditure of KP or government funds.
Example: Going to a local store to purchaseoffice supplies instead of using KP approvedvendors and discounts.
What Is Abuse?Abuse is the wrongful or improper use of KP orgovernment resources. This includes, but is notlimited to, the misuse of position or authoritythat causes the loss or misuse of organizationassets such as funds, medical equipment,
If You Suspect Fraud, Waste, or Abusevehicles, computers, or copy machines.Talk to your manager/supervisor, complianceofficer, or Human Resources representative.Example: Using a company car for personal Or call the Compliance Hotlineuse or using the copy machine to make fliers
1-888-774-9100for your child’s school.
1 | Compliance Hotline: 1.888.774.9100 | kp.org/compliance

Prevent Fraud, Waste, and Abuse
What Can You Do?§ Do not participate in fraud, waste, or abuse
and report when you suspect potential FWA.§ Follow the Principles of Responsibility and
all policies, laws, and regulations.
Allegations are taken seriously andinvestigated. When you report suspected FWA,provide as much detail as possible so it can beinvestigated thoroughly. We also activelymonitor and audit systems to detect indicatorsor “red flags” of fraud, waste, or abuse.Corrective action can include operational orpolicy changes, disciplinary action, and legalaction. Consequences for individuals who areout of compliance include disciplinary action,up to and including termination; loss of licensesand accreditation; legal prosecution, fines, andpenalties; and, possibly, jail time.
2 | Compliance Hotline: 1.888.774.9100 | kp.org/compliance

What is Protected Health Information?
What is Protected Health Information?For information to be considered protected Writtenhealth information (PHI), it must meet all of the § Paper medical records.following three conditions: § Printed After Visit Summaries (AVS) or1. The information is created, received, or Discharge Instructions.
maintained by a health provider or health § Paper bills.plan.
§ Labels on medication bottles or packages2. The information is related to past, present and medication warning inserts.
or future health care or payment for thathealth care.
Electronic (referred to as ePHI)3. The information identifies a member orInformation maintained in or on:patient, or there is enough information to be§ Laptops or desktop computers.able to identify the individual.§ Hand-held devices.§ Flash drives.Health information that is not linked to an
individual by one or more of the 18 HIPAA § Electronic medical records.identifiers* and for which there is no reasonable § Digital images or recordings.basis to believe that the information can be § Email.used to identify the individual is not protectedhealth information.
“HIPAA identifiers” means any of the followingidentifiers, either of the individual or of his/her
Individually identifiable health information relatives, employers or household members:ceases to be PHI 50 years after death.
§ Names.§ All geographical subdivisions smaller than a
PHI can be in oral, written, or electronic State, including street address, city, county,form: precinct, zip code, and their equivalent
geocodes, except for the initial three digits ofOral or Spokena zip code, if according to the current§ Hallway or elevator conversations Nurses’publicly available data from the Bureau ofstation conversations Telephonethe Census: (a) The geographic unit formedappointment reminders – only leave theby combining all zip codes with the sameminimum necessary.three initial digits contains more than 20,000
§ Names called in the waiting room – first and people; and (b) The initial three digits of alast name is allowable; do not add any zip code for all such geographic unitsinformation related to the reason for the visit. containing 20,000 or fewer people ischanged to 000.
1 kp.org/compliance

What is Protected Health Information?
§ All date elements (except year) for dates Removal of all 18 HIPAA identifiers means thedirectly related to an individual, including of information is de-identified and no longerbirth date, an admission or discharge date, protected health information unless thedate of death; and all ages over 89 and any covered entity has actual knowledge that thedate (including year) indicative of such age, remaining information could be used alone orhowever such ages and elements may be in combination with other information to identifyaggregated into a single category of age 90 an individual.or older.
§ Telephone numbers. Individually identifiable information, even if not§ Fax numbers. PHI, may still be subject to other state and
federal privacy protections.§ Email addresses.§ Social Security numbers.§ Medical record numbers.§ Health plan beneficiary numbers.§ Account numbers.§ Certificate/license numbers.§ Vehicle identifiers and serial numbers,
including license plate numbers.§ Device identifiers and serial numbers.§ URLs.§ Internet protocol address numbers.§ Biometric identifiers including finger and
voice prints.§ Full face photographic images and any
comparable images.§ Any other unique identifying number,
characteristic, or code (provided that (a) thecode or other record identifier is not derivedfrom or related to other information (forexample scramble MRNs and SSNs are notpermitted) and not otherwise translatable toidentify the individual; (b) the covered entitydoes not use or disclose the code or otherrecord identifier for any other purpose; (c)and the covered entity does not disclose themechanism for re-identification.
2 kp.org/compliance

2019 Hospital National Patient Safety Goals
The purpose of the National Patient Safety Goals is to improve patient safety. The goals focus on problems in health care safety and how to solve them.
This is an easy-to-read document. It has been created for the public. The exact language of the goals can be found at www.jointcommission.org.
Get important test results to the right staff person on time.
Find out which patients are at risk for suicide.
Use the hand cleaning guidelines from the Centers for Disease Control and Prevention or the World Health Organization. Set goals for improving hand cleaning. Use the goals to improve hand cleaning.
Use proven guidelines to prevent infections that are difficult to treat.
Use proven guidelines to prevent infection of the blood from central lines.
Use proven guidelines to prevent infection after surgery.
Use proven guidelines to prevent infections of the urinary tract that are caused by catheters.
Make sure that the correct surgery is done on the correct patient and at the correct place on the patient’s body.
Mark the correct place on the patient’s body where the surgery is to be done.
Pause before the surgery to make sure that a mistake is not being made.
Use at least two ways to identify patients. For example, use the patient’s name and date of birth. This is done to make sure that each patient gets the correct medicine and treatment. Make sure that the correct patient gets the correct blood when they get a blood transfusion.
Identify patients correctlyNPSG.01.01.01
NPSG.01.03.01
Prevent infectionNPSG.07.01.01
NPSG.07.03.01
NPSG.07.04.01
NPSG.07.05.01
NPSG.07.06.01
Improve staff communicationNPSG.02.03.01
Identify patient safety risksNPSG.15.01.01
Prevent mistakes in surgeryUP.01.01.01
UP.01.02.01
UP.01.03.01
Before a procedure, label medicines that are not labeled. For example, medicines in syringes, cups and basins. Do this in the area where medicines and supplies are set up.
Take extra care with patients who take medicines to thin their blood.
Record and pass along correct information about a patient’s medicines. Find out what medicines the patient is taking. Compare those medicines to new medicines given to the patient. Make sure the patient knows which medicines to take when they are at home. Tell the patient it is important to bring their up-to-date list of medicines every time they visit a doctor.
Use medicines safely
NPSG.03.04.01
NPSG.03.05.01NPSG.03.06.01
Make improvements to ensure that alarms on medical equipment are heard and responded to on time.
Use alarms safely
NPSG.06.01.01

2019 Ambulatory Health Care National Patient Safety Goals
The purpose of the National Patient Safety Goals is to improve patient safety. The goals focus on problems in health care safety and how to solve them.
This is an easy-to-read document. It has been created for the public. The exact language of the goals can be found at www.jointcommission.org.
Use at least two ways to identify patients. For example, use the patient’s name and date of birth. This is done to make sure that each patient gets the correct medicine and treatment.
Make sure that the correct patient gets the correct blood when they get a blood transfusion.
Before a procedure, label medicines that are not labeled. For example, medicines in syringes, cups and basins. Do this in the area where medicines and supplies are set up.
Take extra care with patients who take medicines to thin their blood.
Record and pass along correct information about a patient’s medicines. Find out what medicines the patient is taking. Compare those medicines to new medicines given to the patient. Make sure the patient knows which medicines to take when they are at home. Tell the patient it is important to bring their up-to-date list of medicines every time they visit a doctor.
Identify patients correctly
NPSG.01.01.01
NPSG.01.03.01
Use medicines safely
NPSG.03.04.01
NPSG.03.05.01
NPSG.03.06.01
Prevent infection
NPSG.07.01.01
NPSG.07.05.01
Prevent mistakes in surgery
UP.01.01.01
UP.01.02.01
UP.01.03.01
Use the hand cleaning guidelines from the Centers for Disease Control and Prevention or the World Health Organization. Set goals for improving hand cleaning. Use the goals to improve hand cleaning.
Use proven guidelines to prevent infection after surgery.
Make sure that the correct surgery is done on the correct patient and at the correct place on the patient’s body.
Mark the correct place on the patient’s body where the surgery is to be done.
Pause before the surgery to make sure that a mistake is not being made.

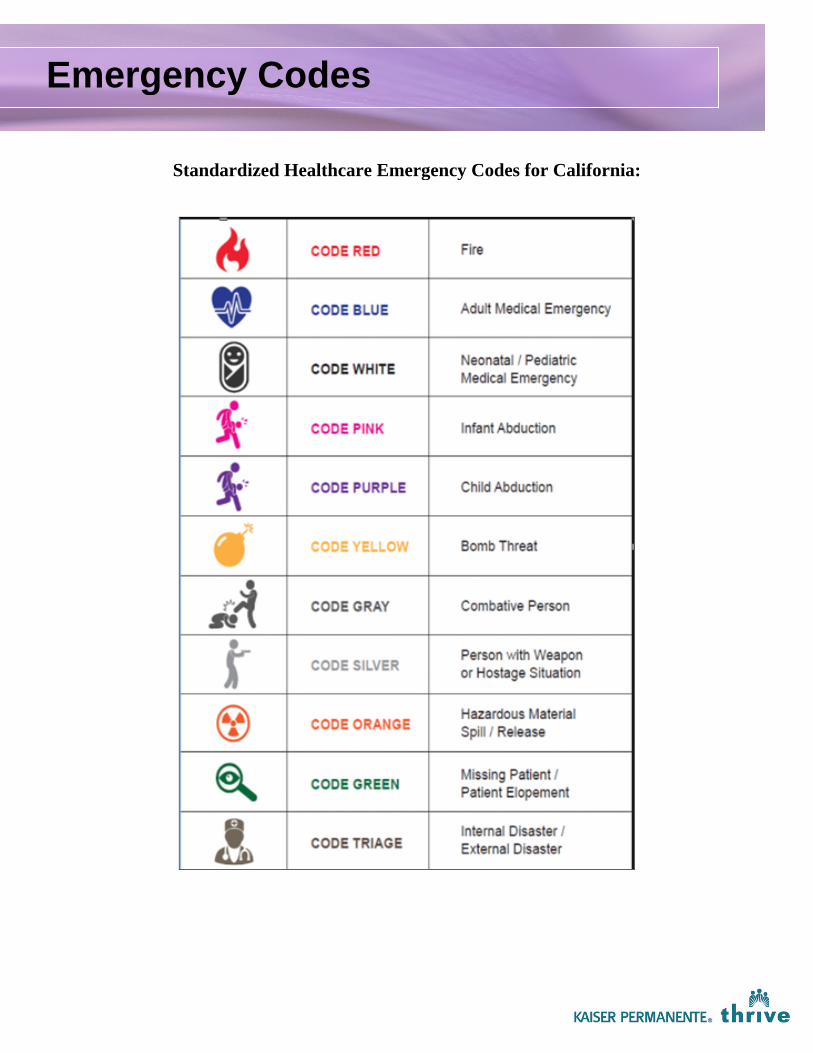
Emergency Codes
Standardized Healthcare Emergency Codes for California:

Stop HereUnless You Are a
Student Nurse
Student NursesPlease Continue Reading
Southern California Regional High-Alert Medication PolicyMEDICAL CENTER ADMINISTRATIVE
POLICIES & PROCEDURES
1.0 Policy Statement
Regional high-alert medications are defined as those drugs which are involved in a higher percentage of medicationincidents and/or sentinel events, or that carry an increased risk for error or other adverse outcomes. These medications areidentified from KP facility data, literature, and regulatory agency standards.
2.0 Purpose
The purpose of this policy is to standardize medication safety practices and to serve as the minimum standard for SouthernCalifornia Regional High-Alert Medications. To maximize the safety of all the medication processes associated with thesemedications, each high-alert medication has specific medication safety practices required when they are administered. Notall medication safety practices are required for each high-alert medication. Refer to the Procedure section of this documentfor specific high-alert medications and the required medication safety practices.
3.0 Scope/Coverage
3.1 The Southern California Regional Pharmacy/Nursing Committee is responsible for the creation andmaintenance of the Regional High-Alert Medication List. The Regional High-Alert Medication List establishedby this policy is the sole list and is standardized throughout the Southern California Region of KaiserPermanente. Requests for changes to the Regional High-Alert Medication List shall be forwarded forconsideration to the Regional Pharmacy/Nursing Committee. The work of the Regional Pharmacy/NursingCommittee will be referred to the Regional Pharmacy and Therapeutics Committee for final approval.
3.2 The medication safety practices, special processes and interventions required for the Southern CaliforniaRegional High-Alert Medication List must be adopted and implemented in all the patient care areas/units of KPfacilities.
3.3 All registry/travelers are required to complete the High Alert Medication Training prior to start of assignment.3.3.1 Registry/travelers will not administer or assist in the administration of any Intrathecal
Medications.3.4 Medications used during medical emergencies (e.g. immediate life-threatening event) are exempt from the
High-Alert Medication Safety Practices in this policy.3.5 The High-Alert Medication safety practices are special safeguards that may be applicable to any step in the
medication administration process. These steps include but are not limited to:3.5.1 Prescribing3.5.2 Prescription order communications3.5.3 Product labeling3.5.4 Packaging and nomenclature3.5.5 Compounding3.5.6 Dispensing3.5.7 Distribution3.5.8 Administration
MCW P&P 2723
SCOPE KFH/SCPMG Section No.
CATEGORYQuality Assurance, Medication Safety Issue No.
Page
1
1 of 13
TITLERegional High-Alert Medication SafetyPractices
Effective Date
Revision Date
2006
11/2017Accountable Department/Committee: Regional Pharmacy Nursing CommitteeApproved by: Regional Pharmacy and Therapeutics Committee

3.5.9 Education3.5.10 Monitoring3.5.11 Use
3.6 Orders for High-Alert Medications will include at a minimum:3.6.1 Patient name and medical record number3.6.2 Date and time the order is written or placed in KP HealthConnect3.6.3 Drug name (generic), dose, route, and date of administration for each drug3.6.4 Rate and/or duration of administration (if applicable)
3.7 The following will be available on the patient’s medical record:3.7.1 All elements used to calculate the dose (e.g. height, weight used for medication dosing during that
encounter, and/or BSA, if applicable)3.7.2 Allergies3.7.3 Informed consent (if applicable)
3.8 All High-Alert Medications will be documented on Medication Administration Record/Anesthesiarecord/Ambulatory medical record, or other part of the medical record where drug administration isdocumented.
4.0 Definitions: New High-Alert Medication Safety Practices
4.1 Qualified Health Care Practitioner: individuals who are qualified to perform double checks or independent doublechecks within the context of their normal responsibilities and scope of practice. Qualified health care practitionersinclude physicians, physician assistants, nurse practitioners, certified nurse midwives, registered nurses, andpharmacists. Licensed vocational nurses may participate in double checks in specific circumstances as describedin the Procedures Section below.
4.2 Independent Double Check is defined as a check of the factors listed below. It is performed independently by twoqualified health care practitioners (MD/RN/Pharmacist), against the current medication order, before each high-alert medication is administered.
4.2.1 These checks must be documented on the Medication Administration Record/Anesthesiarecord/Ambulatory medical record or other part of the medical record where drug administration isdocumented.4.2.2 Refer to Procedure section 5.0 for Independent Double Check Detailed Workflow Checklist.4.2.3 Refer to the Procedure section of this document to determine when an Independent Double Checkis required prior to the administration of a specific high-alert medication.4.2.4 The factors to be verified during the independent double check must include:
4.2.4.1 Right patient4.2.4.2 Right drug4.2.4.3 Right dose4.2.4.4 Right route4.2.4.5 Right day/time4.2.4.6 Right weight
4.2.3.6.1 For patients receiving drugs programmed on the IV pump using the drug library,verify the correct drug, concentration, correct entry of patient weight (for weight-based drugs) or body surface area (for BSA dosed drugs), correct dose/rate orduration, and line attachment. The pump settings must be double checkedagainst the current medication order.
4.2.3.6.2 For patients receiving drugs on the IV pump that cannot be administered usingthe drug library (i.e. the drug or concentration is not in the library, or hard limitsprevent the infusion) – mathematical calculations of the rate must be performedindependently by two qualified health care practitioners. These independentdouble checks must be documented on the Medication Administration
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 2 of 13

Record/Anesthesia Record/Ambulatory Medical Record, or other part of themedical record where drug administration is documented.
4.2.3.6.3 If the drug library cannot be used because: 1) the drug and/or concentration isnot in the library, or 2) concentration, dose, duration or rate hard limits do notallow the infusion; the clinician programming the infusion will consult with apharmacist before proceeding. The pharmacist will assist in determining if theinfusion must be administered as a "Basic Infusion" (in mL/hour). If the "BasicInfusion" is used, the mathematical calculations performed to determine theinfusion rate will be independently double checked by two qualified health carepractitioners.4.2.3.6.3.4 If the “Basic Infusion” mode is being used, and If the medication order
is changed, the clinician will assess whether the drug library can beused.
4.2.3.6.3.4 At handoff, the clinician would discuss the continued use of "BasicInfusion" with the oncoming clinician.
4.2.4 Refer to the Procedure section of this document to determine when Double Checks are required forspecific high-alert medications
4.3 Time Out: Time Out is defined as the period of time immediately before initiating a high-alert medicationadministration /procedure, when two qualified health care practitioners verify the factors listed below, at thepatient’s side in the location where the medication administration /procedure will be performed. The Time Outmust be documented on the medical record at the time of occurrence. Refer to the Procedure section of thisdocument to determine when a Time Out is required prior to the administration of a specific high-alertmedication. The factors to be verified during the Time Out must include:
4.3.1 Availability of any specific equipment for administration of the medication (e.g. infusion devices, ambu bagfor neuromuscular blockers), if applicable. For patients with I.V. Pumps – verify the setting and rate ofinfusion
4.3.2 Right patient identity – patient name and medical record number.4.3.3 Correct side and site - verify appropriateness and adequacy of IV access.4.3.4 Agreement on the medication administration/procedure to be done with the patient - discuss with the
patient/family the medication and administration procedure.4.3.5 Correct patient position for epidural and intrathecal medication administration.
4.4Pharmacy Pause: A Pharmacy Pause is defined as checks performed independently by two pharmacists or apharmacist and a pharmacy technician, before a specified high-alert medication is dispensed from the pharmacy. Thefactors to be verified during the Pharmacy Pause must include:
4.4.1 Right patient identification using two identifiers – patient name, medical record number.4.4.2 Right Drug (verified against original physician order)
4.5Hand-off: Hand-off is defined as an interactive process of passing patient specific information from one caregiver toanother for the purpose of ensuring the continuity and safety of the patient’s care. Hand-off occurs when a nursetransfers responsibility for the patient for the remainder of the workday – e.g. change of shift. Hand-off does notinclude coverage for breaks or meal periods.
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 3 of 13

5.0 Procedures5.1 Independent Double Check Detailed Workflow Checklist (see MCW P&P 2723 Attach E & MCW P&P 2723
Attach F)
This workflow starts with the primary nurse.• Enter the medication safety mindset.
• View the medication order.
• Independently verify the 5+ rights and calculations. Note: your region or facility may have additionalrights associated with medication administration.
1.Right patient: Scan patient armband and ask patient for two patient identifiers (name, medical record number,date of birth)
2.Right drug: Scan the medication in hand and verify it against the order
3.Right dose: Double check the dose against the order and the medication in hand, and if applicable, perform thenecessary calculations
4.Right route: Double check the route against the order and the medication in hand
5.Right day/time: Double check the date and time of the next scheduled administration.
+ Right Indication: Confirm that this is the right medication for this patient’s medical history, vitals, anddiagnosis.
+ + Right Weight: Confirm current patient weight (for weight-based drugs) or body surface area (BSA) for BSA-dosed drugs
• Release and/or acknowledge the medication order. Note: different care settings may vary in howmedication orders are transmitted from physician to nurse - please adhere to local regulations, and askyour manager if you have any questions.
• Obtain/prepare the medication.
• Educate the patient and family and let them know that a second verifier will be brought in for safety.Note: this recommended practice may vary by circumstance, department, or facility. Sample script: “Toensure your safety, we have a verifier double check certain medications before I administer them to you,which means another nurse will be coming into your room to double check the medication.”
• If the pump is being used to administer the medication, program the pump using the library, attach andclamp tubing, ensure the right line is connected to the patient, and set the pump to pause/delay. Note:when and how the line is validated may vary by region and facility.
• Then the primary nurse requests a second verifier to double check the medications. Note: the verifier mustbe a registered nurse, pharmacist, or physician.
• The verifier comes to the patient's bedside and independently double checks the 5 rights, includingcalculations.
• If the pump is being used, the verifier independently double checks the pump settings, ensures that thetubing is correctly attached, and traces the tubing to the point of origin. Then the two compare theirresults. Note: when and how the line is validated may vary by region and facility.
• If a pump is not being used, the primary nurse and the verifier compare their results.
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 4 of 13
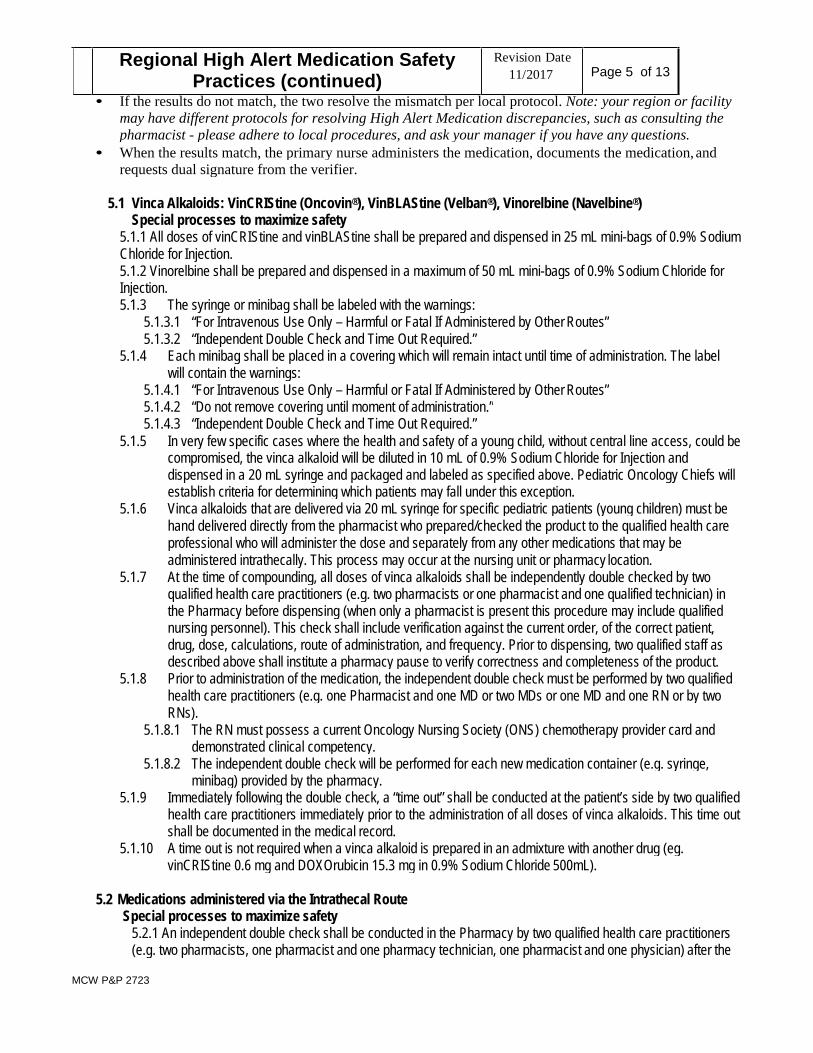
• If the results do not match, the two resolve the mismatch per local protocol. Note: your region or facilitymay have different protocols for resolving High Alert Medication discrepancies, such as consulting thepharmacist - please adhere to local procedures, and ask your manager if you have any questions.
• When the results match, the primary nurse administers the medication, documents the medication, andrequests dual signature from the verifier.
5.1 Vinca Alkaloids: VinCRIStine (Oncovin®), VinBLAStine (Velban®), Vinorelbine (Navelbine®)Special processes to maximize safety
5.1.1 All doses of vinCRIStine and vinBLAStine shall be prepared and dispensed in 25 mL mini-bags of 0.9% SodiumChloride for Injection.5.1.2 Vinorelbine shall be prepared and dispensed in a maximum of 50 mL mini-bags of 0.9% Sodium Chloride forInjection.5.1.3 The syringe or minibag shall be labeled with the warnings:
5.1.3.1 “For Intravenous Use Only – Harmful or Fatal If Administered by Other Routes”5.1.3.2 “Independent Double Check and Time Out Required.”
5.1.4 Each minibag shall be placed in a covering which will remain intact until time of administration. The labelwill contain the warnings:
5.1.4.1 “For Intravenous Use Only – Harmful or Fatal If Administered by Other Routes”5.1.4.2 “Do not remove covering until moment of administration.”5.1.4.3 “Independent Double Check and Time Out Required.”
5.1.5 In very few specific cases where the health and safety of a young child, without central line access, could becompromised, the vinca alkaloid will be diluted in 10 mL of 0.9% Sodium Chloride for Injection anddispensed in a 20 mL syringe and packaged and labeled as specified above. Pediatric Oncology Chiefs willestablish criteria for determining which patients may fall under this exception.
5.1.6 Vinca alkaloids that are delivered via 20 mL syringe for specific pediatric patients (young children) must behand delivered directly from the pharmacist who prepared/checked the product to the qualified health careprofessional who will administer the dose and separately from any other medications that may beadministered intrathecally. This process may occur at the nursing unit or pharmacy location.
5.1.7 At the time of compounding, all doses of vinca alkaloids shall be independently double checked by twoqualified health care practitioners (e.g. two pharmacists or one pharmacist and one qualified technician) inthe Pharmacy before dispensing (when only a pharmacist is present this procedure may include qualifiednursing personnel). This check shall include verification against the current order, of the correct patient,drug, dose, calculations, route of administration, and frequency. Prior to dispensing, two qualified staff asdescribed above shall institute a pharmacy pause to verify correctness and completeness of the product.
5.1.8 Prior to administration of the medication, the independent double check must be performed by two qualifiedhealth care practitioners (e.g. one Pharmacist and one MD or two MDs or one MD and one RN or by twoRNs).
5.1.8.1 The RN must possess a current Oncology Nursing Society (ONS) chemotherapy provider card anddemonstrated clinical competency.
5.1.8.2 The independent double check will be performed for each new medication container (e.g. syringe,minibag) provided by the pharmacy.
5.1.9 Immediately following the double check, a “time out” shall be conducted at the patient’s side by two qualifiedhealth care practitioners immediately prior to the administration of all doses of vinca alkaloids. This time outshall be documented in the medical record.
5.1.10 A time out is not required when a vinca alkaloid is prepared in an admixture with another drug (eg.vinCRIStine 0.6 mg and DOXOrubicin 15.3 mg in 0.9% Sodium Chloride 500mL).
5.2 Medications administered via the Intrathecal RouteSpecial processes to maximize safety
5.2.1 An independent double check shall be conducted in the Pharmacy by two qualified health care practitioners(e.g. two pharmacists, one pharmacist and one pharmacy technician, one pharmacist and one physician) after the
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 5 of 13

preparation of the intrathecal dose to assure it is prepared and labeled correctly. For intrathecal drugs prepared ina sterile environment outside the Pharmacy (e.g., operating room, labor and delivery), the independent doublecheck shall be conducted by any two qualified health care practitioners (e.g., two registered nurses, one physicianassistant and one nurse anesthetist, one certified nurse midwife and one physician, etc.) after the preparation ofthe intrathecal dose to assure it is prepared and labeled correctly.5.2.1.1 Label to include the warning:
5.2.1.1.1 “Caution: For intrathecal use only.”5.2.1.1.2 “Independent Double Check and Time Out Required.”
5.2.1.2 The independent double check will be performed for each new medication container provided by thepharmacy and at hand-offs.
5.2.1.3 When an intrathecal drug is prepared or dispensed by the Pharmacy, intrathecal medications must bedelivered directly from the pharmacist who prepared or verified the product to the physician who willadminister the drug to encompass the sterile process. This process may occur in the patient care area orthe Pharmacy.
5.2.2 Intrathecal chemo medication will be compounded and dispensed in a syringe that is 10 mL orsmaller. No other cytotoxic drugs will be present at the patient bedside during the intrathecalchemo administration process.
5.2.3 A “time out,” including an independent double check, shall be conducted at the bedside immediately priorto the administration of all doses of intrathecal medications. (See definition above, III B.) These checksshall be documented in the medical record.
5.3 Continuous intravenous infusions of Heparin and ArgatrobanSpecial processes to maximize safety
5.3.1 The abbreviation “u” will not be accepted in heparin medication orders. Units must be spelled out.5.3.2 A standard concentration will be utilized for all continuous heparin and argatroban infusions.
5.3.3 When not ordered by Pharmacy protocol, order sets shall be utilized for prescribing continuous infusions ofheparin.
5.3.4 Infusion pumps will be used with the safety software activated when heparin and argatroban areadministered.
5.3.5 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)is required initially, at each bag change, rate change, and at hand-offs.
.5.4 Continuous intravenous infusions of Insulin
Special processes to maximize safety5.4.1 The abbreviation “u” shall not be accepted in the medication order. Units must be spelled out.5.4.2 A standard insulin concentration of 1 unit/ml shall be utilized for all adult continuous insulin infusions.5.4.3 Prime insulin tubing with 20 mL.5.4.4 Maximum will be insulin 250 units in 250 mL.5.4.5 Order sets shall be utilized for prescribing continuous infusions of insulin.5.4.6 Infusion pumps will be used with the safety software activated when insulin drips are administered.5.4.7 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)
is required initially, at each bag change, and at hand-offs.
5.5 Distribution and storage of multi-dose Insulin VialsSpecial processes to maximize safety
5.5.1 Inpatient Practice AreaMCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 6 of 13
Heparin 100 units/mL
Argatroban 1mg per mL

5.5.1.1 Multi-dose vials of insulin shall be stored separately in appropriately labeled bins.5.5.1.2 All multi dose vials of insulin must be discarded within 28 days of initially entering or opening (e.g.
needle punctured). A revised expiration date that is 28 days from the initial entering or openingmust be written or affixed on the vial.
5.5.1.3 All insulins other than approved floor stock insulin will be supplied as other medications on apatient specific basis.
5.5.2 Ambulatory Practice Areas5.5.1.4 Multi-dose vials of insulin should be limited to those commonly used in the practice area.5.5.1.5 Different types of insulin vials shall be stored separately in appropriate labeled bins.5.5.1.6 All multi-dose vials of insulin must be discarded within 28 days of initially entering or opening (e.g.,
needle-punctured). A revised expiration date that is 28 days from the initial entering or openingmust be written or affixed on the vial.
5.6 U-500 Insulin Injection for Inpatient and Emergency Department Use
5.6.1 U-500 insulin vials shall be stocked in Pharmacy department only. U-500 insulin vials shall not be stockedin patient care areas. Warnings, signs, labels or other methods shall be used to differentiate the U-500concentration from other insulin products.
5.6.2 Prescribing of U-500 insulin will be limited. U-500 insulin will appear in the Endocrinology and Pharmacistpreference lists in KP HealthConnect, but will not appear in the preference lists for other providers.
5.6.3 The abbreviation “u” (indicating units) will not be accepted in the medication order.5.6.4 U-500 insulin orders must be verified by two pharmacists (dual pharmacist verification in KP
HealthConnect)5.6.5 The term “Conc” (Concentrated) will appear immediately following the drug name and preceding U-500 in
the product name description on the KP HealthConnect drug label and Medication Administration Record(eMAR)
5.6.6 Pharmacy personnel shall prepare and dispense all doses of U-500 insulin syringes with a patient-specificlabel
5.6.7 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)is required prior to administering each dose of U-500 insulin.
5.7 Concentrated Electrolytes >0.9% Sodium chloride injection, and > 0.4 mEq/mL Potassium injection(chloride, acetate, and phosphate) Special processes to maximize safety
5.7.1 Concentrated electrolyte injections will be stored only in the pharmacy.5.7.2 There are two identified exceptions: Cardiac ORs at the KP Los Angeles and Fontana Medical Centers5.7.3 Commercially available, ready-to-administer products will be used whenever possible (e.g., Sodium
Chloride 3% in 500mL bags). Patient-specific labeling will be affixed to each container prior to dispensing.5.7.4 All concentrated sodium chloride infusions shall be affixed with a special label e.g., “Hypertonic Sodium
23.4%)” (letters in Red).5.7.5 Infusion pumps will be used with the safety software activated concentrated electrolytes are administered.5.7.6 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)
is required initially, at each bag change, rate change, and at hand-offs.
5.8 Storage of Sterile Water for Injection5.8.1 In order to reduce the risk of sterile water for injection being administered intravenously, Materials
Management may only store sterile water for injection in vials or ampules less than 100mL.5.8.2 Containers greater than or equal to 100mL will be stored in the Inpatient Pharmacy.
5.9 Magnesium Sulfate Infusions5.9.1 Magnesium sulfate is considered to be a High Alert Medication if the:
5.9.1.1 Concentration is greater than 40 mg/mL in a volume of less than or equal to 150mL, or if theMCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 7 of 13
5.9.1.2 Concentration is greater than 6 mg/mL in a volume larger than 150mL.5.9.2 If these limits are exceeded, the following will be required:
5.9.2.1 Independent double checks by two qualified health care practitioners (e.g. nurse, pharmacist,physician) is required initially, at each bag change, rate change, and at hand-offs.
5.9.2.2 Infusion pumps will be used with the safety software activated when magnesium sulfate infusions areadministered
5.10 Alteplase (t-PA, Activase®) Intravenous InfusionsSpecial processes to maximize safety
5.10.1 Alteplase (t-PA) may only be prescribed using a KP HealthConnect order set. Exception: prescribing lowdose alteplase (CathfloTM) for catheter clearance
5.10.2 All infusions of Alteplase (t-PA) for use in all departments including, but not limited to, the hospital andemergency departments shall be prepared by pharmacy personnel in an inpatient pharmacy setting.Administration of Alteplase via IV, intra-arterial push or instillation for resolving clots in tubing is excludedfrom the High Alert Policy.
5.10.3 Prepared mixtures of Alteplase will include only the patient specific dose ordered. No excess medicationis allowed in the final container to be used for drug administration to the patient (i.e. only the exact dose ofthe drug is to be in the final administration container).
5.10.4 The label for each dose shall include at a minimum; the Patient Name and Medical Record Number, thepatient location, the generic and brand name of the drug, the concentration of the drug supplied in mg/mL,the total drug quantity/total volume of solution that is contained in the package, the expiration date and therate of infusion/administration. Each label, e.g. the bolus syringe and the infusion container) shall bepatient specific for that dose to be administered.
5.10.5 The compounding of the medications should be accomplished without interruption and in an area that issequestered from other activities of disruption.
5.10.6 Infusion pumps will be used with the safety software activated when alteplase is in the pump library5.10.7 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)
is required initially, at each bag change, rate change, and at hand-offs.5.10.8 To ensure the entire dose of alteplase is administered, flush the I.V. line to clear residual drug from I.V.
tubing.
5.11 Tenecteplase (TNKase®) Intravenous InjectionsSpecial Processes to maximize safety
5.11.1 Tenecteplase (TNKase®) may only be prescribed using a KP HealthConnect Order Set/preprinted order.5.11.2 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)
is required whenever an injection of tenecteplase (TNKase®) is initiated.5.11.3 Whenever tenecteplase (TNKase®) is stored in an automated dispensing cabinet (e.g. PYXIS®
SureMed®, Omnicell®, etc) a “Clinical Data Category:” warning shall be used to differentiate the productfrom alteplase (t-Pa) and minimize the possibility of a substitution error.
5.11.4 Whenever tenecteplase (TNKase®) is stored in an automated dispensing cabinet (e.g. PYXIS®SureMed®, Omnicell®, etc), it will not be placed on the device override list. This will minimize thepossibility of clinical staff removing the drug without a medication order being placed in KPHealthConnect.
5.12 Neuromuscular Blocking AgentsSpecial processes to maximize safety
5.12.1 Neuromuscular blockers shall only be stored in specific areas within the hospital, e.g. OR, PACU, CriticalCare (PICU/NICU/ICU), ED, Cath Lab.
5.12.2 Distinctive labeling and/or storage shall be utilized to distinguish neuromuscular blockers from othermedications outside the O.R., e.g. segregation, colored bins, etc. Pharmacy will affix a label to all vialsprior to dispensing to areas outside the OR – e.g. Critical Care, ED, PACU
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 8 of 13

5.12.3 All infusions of neuromuscular blockers shall be affixed with the following label prior to being dispensedfrom Pharmacy:
5.12.3.1 **Caution: Paralyzing Agent** Patient must be on a ventilator or other ventilation support"5.12.4 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)
is required for each intravenous push dose. For infusions, independent double checks are requiredinitially, at each bag change, rate change, and at hand-offs.
5.12.5 Infusion pumps will be used with the safety software activated when neuromuscular blocker infusions areadministered.
5.12.6 Policies and procedures regarding the responsibilities of anesthesia providers in the High Alert MedicationProgram are specified in Regional High Alert Medication Safety Practices for Anesthesia.
5.12.7 A “time out,” shall be conducted at the bedside immediately prior to the administration of all bolus dosesand infusions of neuromuscular blocking agents. (See definition above.) These checks shall bedocumented in the medical record.
5.12.8 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for prescribingneuromuscular blocking agents. Orders must also state:
5.12.8.1 “Patient must be on a ventilator”
5.13 Opiate/Narcotic infusions including PCA therapySpecial processes to maximize safety
5.13.1 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for prescribingopiate/narcotic infusions and PCA therapy.
5.13.2 The following standard concentrations shall be utilized for PCA therapy:5.13.2.1 morphine 1 mg/mL5.13.2.2 fentanyl 10 mcg/mL5.13.2.3 hydromorphone 0.2 mg/mL
5.13.3 In clinical situations where more concentrated infusions are required, the syringes/bags shall be affixedwith a “Note Concentration” label.
5.13.4 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist, physician)is required initially, at each bag or syringe change, rate change, and at hand-offs.
5.13.5 Continuous Opiate/Narcotic Infusions:5.13.5.1 Infusion pump will be programmed using the drug library.
5.13.6 PCA Therapy:5.13.6.1 PCA Pumps with “Smart Technology” and a “Drug Library”
5.13.6.1.1 PCA pumps with a drug library will be programmed using the drug library.5.13.7 Policies and procedures regarding the responsibilities of anesthesia providers in the High Alert Medication
Program are specified in Regional High Alert Medication Safety Practices for Anesthesia..
5.14All medication infusions administered via the epidural route including Opiate/Narcotic MedicationsSpecial processes to maximize safety
5.14.1 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for prescribingepidural infusion.
5.14.2 All epidural infusions shall be administered utilizing a programmable/advanced mode pump and label onpump display with appropriate medication.
5.14.3 Whenever feasible, commercially prepared bags of medications shall be utilized for epidural infusion.5.14.4 Specific identified (e.g. yellow stripe) tubing without injection ports shall be utilized for administering
epidural infusions.5.14.5 Infusion pumps will be used with the safety software activated when specific drugs, concentrations and
volumes are in the pump library.5.14.6 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist,
physician) is required initially, at each bag change, rate change, and at hand-offs.MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 9 of 13

5.14.7 Policies and procedures regarding the responsibilities of anesthesia providers in the High AlertMedication Program are specified in Regional High Alert Medication Safety Practices for Anesthesia.
5.15Intravenous, Intraperitoneal, Intraarterial, Intrahepatic and Intrapleural Cytotoxic ChemotherapySpecial processes to maximize safety
5.15.1 Verbal orders shall not be accepted when prescribing intravenous, intraperitoneal, intraarterial,intrahepatic and intrapleural cytotoxic chemotherapy except for date or time changes and clarifications.
5.15.2 Whenever feasible, KP HealthConnect order sets, panel orders, treatment plans, or preprinted ordersshall be used for prescribing intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleuralcytotoxic chemotherapy.
5.15.3 When prescribing intravenous cytotoxic chemotherapy, orders shall be written for individual doses, notthe total amount of drug for the entire course of therapy.
5.15.4 Complete orders for intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleural cytotoxicchemotherapy should include:5.15.4.1 Patient name and medical record number, date and time the order is written5.15.4.2 All elements used to calculate the initial dose or change of treatment of a chemotherapy agent
should be included on the order or prescription (height, weight, and/or BSA if applicable)5.15.4.3 Indication that written informed consent was obtained for research protocols5.15.4.4 Allergies5.15.4.5 Chemotherapy agent name, dose, route, and date of administration for each drug5.15.4.6 Cycle number and/or week number as appropriate to the regimen, if applicable
5.15.5 All doses of intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleural cytotoxicchemotherapy shall be independently double checked by two qualified health care practitioners (e.g.two pharmacists or one pharmacist and one qualified technician) in the Pharmacy before dispensing(when only a pharmacist is present this procedure may include qualified nursing personnel). Thischeck shall include, against the current order, a verification of the correct patient, drug, dose, route ofadministration, and frequency. This check shall be documented in appropriate pharmacy record.
5.15.6 If a Beacon treatment plan is used, pharmacists will perform and document independent doublechecks as specified in the Beacon Pharmacy Job Aid (see MCW P&P 2723 Attach D).
5.15.7 Distinctive labeling/packaging shall be utilized to distinguish intravenous, intravenous, intraperitoneal,intraarterial, intrahepatic and intrapleural cytotoxic chemotherapy from other medications.
5.15.8 All doses of intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleural cytotoxicchemotherapy shall be affixed with a “Caution: Chemotherapeutic Agent” label.
5.15.9 Missing dose requests for intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleuralcytotoxic chemotherapy shall be investigated immediately by a pharmacist and a replacement doseshall not be dispensed until the disposition of the first dose is verified.
5.15.10 RNs must possess a current Oncology Nursing Society (ONS) chemotherapy provider card anddemonstrated clinical competency to administer intravenous, intraperitoneal, and intraarterial cytotoxicchemotherapy. Pediatric RNs must possess either a current ONS chemotherapy provider card or acurrent Association of Pediatric Hematology and Oncology Nurses (APHON) Chemotherapy &Biotherapy provider card and demonstrated clinical competency. RNs with the above qualificationsmust have additional training on the use of arterial pumps if they will be administering intraarterialcytotoxic chemotherapy. Physicians will administer intrapleural and intrahepatic cytotoxicchemotherapy.
5.15.11 Two qualified health care practitioners (per Independent Double Check Definition) shall independentlydouble check all doses of intravenous, intraperitoneal, intraarterial, intrahepatic and intrapleuralcytotoxic chemotherapy at the bedside before administration, at each bag change, rate change, and athand-offs.
5.15.12 The Infusion pumps will be used with the safety software activated when specific drugs, concentrationsand volumes are in the pump library.
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 10 of 13
5.16 Bortezomib (Velcade®)Special processes to maximize safety
5.16.1 This drug is can be administered intravenously or subcutaneously. (Intrathecal administration can befatal.) Route-specific administration instructions will appear (e.g. For intravenous use only. Harmful orFatal if Administered by Incorrect Route):
5.16.1.1 In the “summary sentence” of the KP HealthConnect medication order at the prescribing step;5.16.1.2 On the patient-specific medication label;5.16.1.3 In the medication administration instructions on the electronic medication administration record
eMAR.5.16.2 Immediately following the independent double check, a “time out” shall be conducted at the patient’s
side by two qualified health care practitioners immediately prior to the administration of all doses ofbortezomib (Velcade®). This time out shall be documented in the medical record. A reminder to performthe time out will appear on the KP HealthConnect locations in 1a, 1b, and 1c above.
5.16.3 All other labeling and packaging requirements described in Section IV.O above (CytotoxicChemotherapy) will apply
5.17 Intravenous Infusions of ketamine, pentobarbital5.17.1 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for prescribing
infusions of ketamine, and pentobarbital.5.17.2 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist,
physician) is required initially, at each bag change, rate change, and at hand-offs.5.17.3 Infusion pumps will be used with the safety software activated when specific drugs, concentrations and
volumes are in the pump library.
5.18 Intravenous infusions of propofol, midazolam, lorazapam, dexmedetomidine (Precedex)5.18.1 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for prescribing
infusions of propofol, midazolam, lorazepam, and dexmedetomidine (Precedex).5.18.2 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist,
physician) is required initially, at each bag change, and at hand-offs.5.18.3 Infusion pumps will be used with the safety software activated when specific drugs, concentrations and
volumes are in the pump library.
5.19 Parenteral (intravenous and subcutaneous) Infusions of Prostacyclins – epoprostenol (Flolan®,Veletri®) and treprostinil (Remodulin®)Special processes to maximize safety5.19.1 Whenever feasible, KP HealthConnect Order Sets/preprinted orders should be utilized for
prescribing parenteral prostacyclins.5.19.1.1 Prostacyclin concentrations are ordered in “mcg/mL”.5.19.1.2 Prostacyclin doses are ordered in “nanograms/kg/minute”.5.19.1.3 During order verification in KP HealthConnect, the pharmacist will select a concentration to
deliver a final rate between 2 mL/hour and 20 mL/hour for intravenous infusions.5.19.2 An independent double check by two qualified health care practitioners (e.g. nurse, pharmacist,
or physician) is required initially, at each bag change, rate change, and at hand-offs.5.19.2 Prostacyclins will be administered using an infusion pump with the safety software (drug library)
activated.
5.20 Medication Administration to Pediatric and Neonatal PatientsSpecial processes to maximize safety5.20.1 The High Alert Medications for use in all Pediatric and Neonates will include those drugs and
medication management requirements in the adult High Alert Medication Policy.MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 11 of 13

5.20.2 In addition, an independent double check by two qualified health care practitioners (e.g. nurse,pharmacist, physician) is required initially, at each bag or syringe change, and at hand-offs for thesemedications:
5.20.2.1 Remicade, all routes5.20.2.2 Chloral hydrate, all routes5.20.2.3 Insulin, all routes5.20.2.4 Digoxin, P.O. and I.V.
5.20.3 Licensed vocational nurses may participate in independent double checks for subcutaneous insulininjections in medical office settings.
5.20.4 DOPamine, DOBUTamine, Epinephrine, Norepinephrine and Phenylephrine Infusions: An independentdouble check by two qualified health care practitioners (e.g. nurse, pharmacist, physician) is requiredinitially, at each bag change, rate change, and at hand-offs. Infusion pumps will be used with the safetysoftware activated when specific drugs, concentrations and volumes are in the pump library
5.20.5 The table below lists standard concentrations for continuous I.V. infusions for all patients admitted topediatric, pediatric intensive care (PICU) and neonatal intensive care units (NICUs).
5.20.5.1 Affix a “Note concentration” sticker to all bags/syringes that contain customized concentrations.5.20.5.2 See Table A for Standard Concentrations for Pediatrics, PICU and NICU
TABLE A - Standard Concentrations for Pediatrics, PICU and NICU
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 12 of 13
Concentration #1 #2 #3Potassium Chloride
0.1 mEq/mL(10 mEq/100 mL)
0.2 mEq/mL(20 mEq/100 mL)infuse via central line only
Pediatrics/PICU specificDOPamine 1600 mcg/mL
(400 mg/250 mL)3200 mcg/mL(800 mg/250 mL)
DOBUTamine 2000 mcg/mL(500 mg/250 mL)
4000 mcg/mL(1 Gm/250 mL)
Epinephrine 16 mcg/mL(4 mg/250 mL)
64 mcg/ mL(16 mg/250 mL)
Norepinephrine 16 mcg/mL(4 mg/250 mL)
32 mcg/mL(8 mg/250 mL)
Phenylephrine 40 mcg/mL(10 mg/250 mL)
80 mcg/mL(20 mg/250 mL)
Insulin, Regular 0.5 Unit/mL 1 Unit/mLNICU specificDOPamine 400 mcg/mL 800 mcg/mL 1600 mcg/mLDOBUTamine 500 mcg/mL 1000 mcg/mL 2000 mcg/mLEpinephrine 20 mcg/mL 40 mcg/mLInsulin, Regular 0.1 Unit/mL 0.5 Unit/mL
6.0 Appendices6.1 Appendix A - Independent Double Check Detailed Workflow Checklist
6.2 Appendix B - Oncology Medication Verification and Independent Double CheckDetailed Workflow Checklist
6.3 Appendix C – Beacon Pharmacy Job Aid
MCW P&P 2723
Regional High Alert Medication SafetyPractices (continued)
Revision Date11/2017 Page 13 of 13

4 Key pillars thatKP Nursing Professional Practice Modelsupportwork/practices
KP Nursing Values(underpin our work)
Core of work

Nursing Vision &Values

SOUTHERN CALIFORNIA (SCAL)Regional Policy and Procedures
BARCODE SCANNING MEDICATION ADMINISTRATIONInstructions for Students
Tips:
Ø Hand held barcode scanners are programmed to specific individual computers.Therefore, you must use the computer and scanner in the patient’s room or, if needed,you must bring the entire mobile cart with computer/scanner into a patient’s room.
Ø Meds are NOT to be opened until they are scanned at the patient’s bedside.
Ø Three (3) beeps will sound when an item is successfully scanned.
Ø Do not place anything close to the scanner when it is not in use because the scanner lightwill remain on, thereby using up the battery. DO NOT face scanner close to or against thebedside table or wall.
Procedure at Patient Bedside:
1. Scan UCI (unique contact identifier) number on the patient’s armband. Thiswill automatically open up the computer & eMAR (electronic medicationadministration record) screen.
v Please Note: Patients do not have armbands in Outpatient/ Ambulatorysetting. You will verify patient using 2 patient identifiers. (Name andDOB (date of birth) or MRN (medical record number))
2. Scan drug that is to be administered, drug order will show in eMAR. Click“accept” and eMAR will automatically label the med as given.
3. KP pharmacy barcode labels will be placed on any medication that comes withtheir own manufacturer barcode. Make sure to scan the KP barcode label.
4. If patient has a medication ordered with 2 different administrative routesidentified, make sure you select the correct route on the eMAR.
5. If you scan an item that is not showing on the eMAR, the order may not have beencompleted by Pharmacy yet. You will receive a notice “No orders for--were foundfor this patient.” Please follow up with Pharmacy to verify order.
6. If a scanner does not read the medication’s barcode, BUT the med is listed on theeMAR and is there is an order for it to be given, call the Pharmacy for assistance.
7. For intravenous (IV) piggy back, scan the vial of medication that is to be mixed, not the IVsolution bag.
8. For IV bags, please be aware that there needs to be dark color contrast behind theIV bag, in order for the barcode to be picked up by the scanner.
The armband maker is available at the Nurses’ Station for any patient in need of a newarmband. HOWEVER, NO ONE CAN MAKE DUPLICATE COPIES OF ARMBANDS.

Nurse Knowledge Exchange Plus (NKE+)Inpatient/Hospital Shift Change Communication
NKE+ is an evidence-based Shift Change Communication framework designed to enhance safety,communication and efficiency. It incorporates proactive measures to structure and support nurses duringshift changes.
Proactive preparation to prepare of the oncoming shiftEstablishes a standardized last hourly round and pre-shift assignments to help the unit prepare for oncoming shifts.
Coordinated roles to minimize disruptions during shift changeThe unit works together to minimize interruptions to nurses, allowing them to get off to a strong hand-off and a strongstart-of-shift.
In-room patient engagementIncorporates the use of a careboard, in-room SBAR, and an in-room safety check to engage patients and drivesafety.

Thank You
for completing the KPSC Student Unpaid Field Experience and Training Required Readings. Please proceed to the Kaiser Required Forms and complete
the remaining on-boarding requirements.