Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Tropical Diseases Judd Walson, MD, MPH...
45
Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Tropical Diseases Judd Walson, MD, MPH April 22, 2010
-
Upload
chastity-ball -
Category
Documents
-
view
218 -
download
0
Transcript of Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Tropical Diseases Judd Walson, MD, MPH...

Welcome to I-TECH HIV/AIDS Clinical Seminar Series
HIV and Tropical Diseases
Judd Walson, MD, MPH
April 22, 2010


Case #1
• 23 year old female presents to HIV Care Clinic where she receives care complaining of fever for 1 day.
• Family lives in an area that is holoendemic for malaria.
• She is anemic (Hb of 6.5), tachypneic, mildly confused and has fever to 40.1 C.

Malaria and HIV

Classification of endemicityType Spleen Rates Parasite Rates Description
Hypoendemicity <= 10% of children aged 2-9 years
<= 10% of children aged 2-9 years but may be higher for part of the
Areas where there is a little transmission and the effects, during the average year, upon the general population are unimportant
Mesoendemicity 11-50% of children aged 2-9 years
11-50% of children aged 2-9 years
wide geographical variations in transmission risk exist
Hyperendemicity Constantly > 50% in children aged 2-9 years; also high in adults (>25%)
Constantly > 50% among children aged 2-9
Areas where transmission is intense but seasonal; immunity is insufficient in all age groups
Holoendemicity Constantly > 75% in children aged 2-9 years, but low in adults
Constantly > 75% among infants aged 0-11 months
Intense transmission resulting in a considerable degree of immunity outside early childhoodhttp://www.malaria.am/eng/epidemiology.php
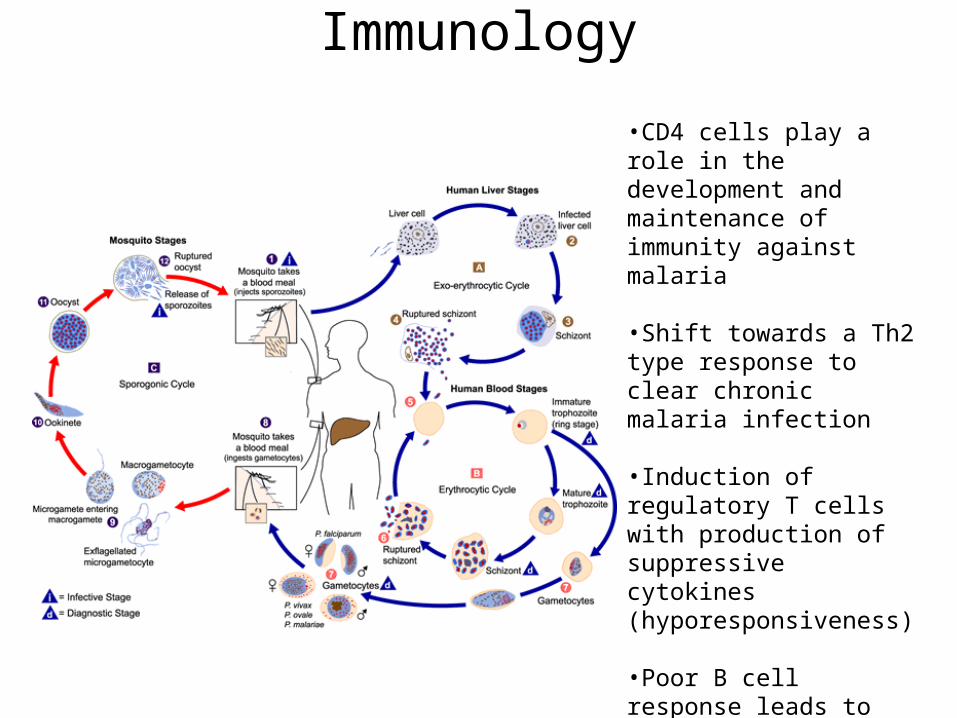
Immunology
•CD4 cells play a role in the development and maintenance of immunity against malaria
•Shift towards a Th2 type response to clear chronic malaria infection
•Induction of regulatory T cells with production of suppressive cytokines (hyporesponsiveness)
•Poor B cell response leads to reduced clearance of parasites
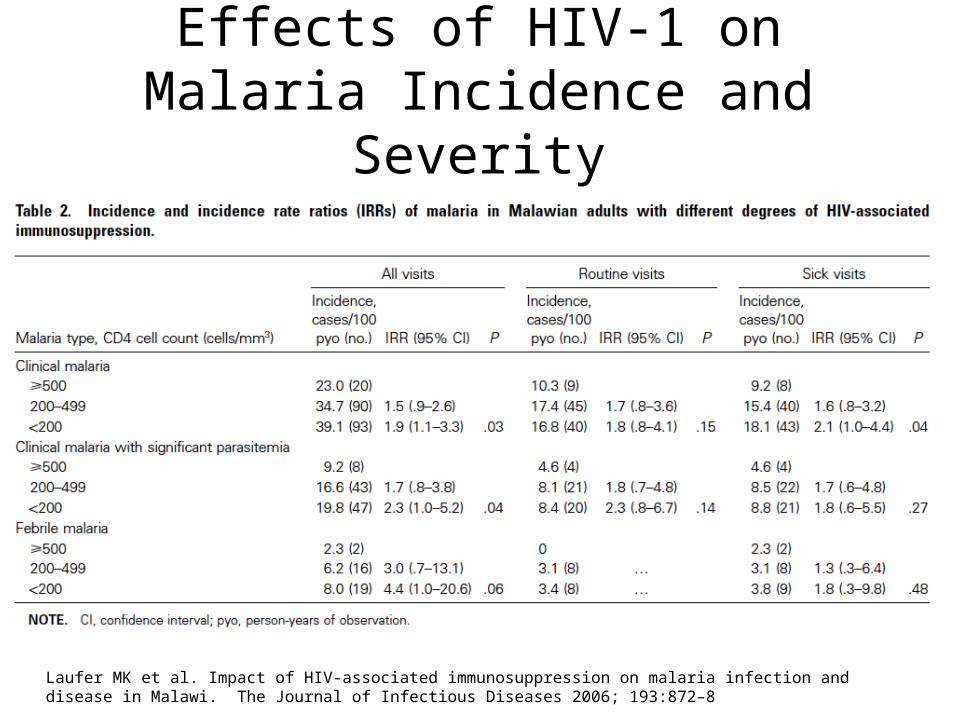
Effects of HIV-1 on Malaria Incidence and Severity
Laufer MK et al. Impact of HIV-associated immunosuppression on malaria infection and disease in Malawi. The Journal of Infectious Diseases 2006; 193:872–8

Laufer MK et al. Impact of HIV-associated immunosuppression on malaria infection and disease in Malawi. The Journal of Infectious Diseases 2006; 193:872–8
French N et al. Increasing rates of malarial fever with deteriorating immune status in HIV-1-infected Ugandan adults. AIDS 2001 vol. 15 (7) pp. 899-906.
Case #1
• 23 year old female presents to HIV Care Clinic where she receives care complaining of fever for 1 day.
• Family lives in an area that is holoendemic for malaria.
• She is anemic (Hb of 6.5), tachypneic, mildly confused and has fever to 40.1 C.

Case #1
• Any other info needed?• What testing needed?• What treatment needed?

The diagnosis of Malaria
• Malaria is often over diagnosed! • Most clinics and hospitals in Africa do NOT do
any testing but make a clinical diagnosis of malaria

The diagnosis of Malaria
• The sensitivity and specificity of malaria thin and thick smears are 50% and 96% respectively.
• The proportion of patients with positive smears DECREASES with age.
• In endemic areas, a positive smear may confirm malaria…but is that why the patient is sick??
Malaria Journal 2006, 5:4, BMJ 2004; 329; 1212

BMJ 2004;329:121

Tanzanian Study
• 4474 people admitted to hospital met criteria (clinical) for severe malaria.
• 2062 (46.1%) had positive slides• 2375 were slide negative
– 66.1% did NOT receive antibiotics– Case fatality rates were significantly different
• 12.1% in the slide negative patients (16.5% in age>15)• 6.9% in the slide positive patients (10.7% in age>15)
BMJ 2004;329;1212-

Malaria and Bacteremia
JID 2007;195; 985-904.

Case #1
• Attending clinic since diagnosis 11 months ago.
• CD4 count 437 cells/mm3 about 9 weeks ago.• ART naïve.• On co-trimoxazole for past 7 months.• Thin Smear POSITIVE for P. falciparum with a
parasite density of 600 parasites per microL (7.5%).
Treatment
• 23 year old female with documented parasitemia, CD4 count of 437 cells/mm3, on co-trimoxazole.– What are the treatment options?– Doe the fact that she is on co-trimoxazole and
NOT on ART matter?

Co-trimoxazole?
• Why do we use co-trimoxazole in Africa?• What are the implications for treatment of
malaria in a patient on co-trimoxazole?• What other interventions can we add to
prevent malaria? Are any of these beneficial if the patient is compliant with co-trimoxazole?

co-trimoxazole• co-trimoxazole reduces MORTALITY in HIV
infected individuals in Africa!!! (46% reduction in mortality in Uganda).
• co-trimoxazole decreases rates of malaria, diarrhea and hospitalizations in those on prophylaxis.
• co-trimoxazole taken for prophylaxis reduces mortality in family members (63% percent less mortality in children less than 10!) and reduces malaria, diarrhea and hospitalizations in family members as well!
Lancet 2004; 364 (9443) pp. 1428-34, AIDS; 2005; 19 (10) pp. 1035-42

Resistance
• There is demonstrated in-vitro cross-resistance between SP (fansidar) and co-trimoxazole.
• Most countries do NOT use SP as first line malaria treatment (except IPT for pregnant women!)
• In a randomized trial of co-trimoxazole to prevent malaria, there was no demonstrated increase in resistant parasites over 12 weeks and co-trimoxazole was 99.5% effective in preventing clinical malaria.
JID 2005;192;1823.
Additional Interventions
• Bednets – In Uganda, insecticide Treated Nets (ITN’s) resulted in a 40% reduction in the incidence of symptomatic malaria, OVER AND ABOVE the benefit seen with prophylactic co-trimoxizole.
• ITN’s are simple, effective, and, in contrast to TMP/SMZ, do not pose risk to the individuals of drug toxicity or development of resistant microbial flora.
Lancet. 2006;367:1256-61.
Treatment and ART
• Efavirenz is metabolized by CYP 3A4 and alters artesunate and amodiaquine levels (may result in increased liver toxicity) NOT DEMONSTRATED.
• Ritonovir inhibits P450 and may increase mefloquine and artemisinin levels. (One study showed increased neutropenia in children on ART receiving artesunate plus amodiaquine.
• Most protease inhibitors have direct anti-malarial activities (? Effective prophylaxis?)
Clin. Infect. Dis. 46, 985–991, Trends in Parasitology. 24 (6) pp. 264-71

Hoffman IF et al. The effect of Plasmodium falciparum malaria on HIV-1 RNA blood plasma concentration. AIDS 1999 vol. 13 pp. 487-494
Effects of Malaria on HIV-1

J . Kublin , P . Patnaik , C . Jere , W . Miller , I . Hoffman , N . Chimbiya , R . Pendame , T . Taylor , M . Molyneux. Effect of Plasmodium falciparum malaria on concentration of HIV-1-RNA in the blood of adults in rural Malawi: a prospective cohort study. The Lancet , Volume 365 , Issue 9455 , Pages 233 – 240.

Gupta et al. JID 2007; 195 (Feb 15).
Effect of modest VL reductionEffect of modest VL reduction

Abu-Raddad LJ et al. Dual infection with HIV and malaria fuels the spread of both diseases in sub-Saharan Africa. Science 2006 vol. 314 (5805) pp. 1603-6.

Summary Malaria and HIV
• HIV infected individuals are at risk for more frequent and more severe malaria. Both are CD4 count dependent.
• Malaria increases plasma viral load. This may have important implications for both HIV disease progression and transmission.
• Co-trimoxazole works for patients and their families and benefits ALL HIV infected individuals in resource poor settings REGARDLESS OF CD4 COUNT.

CASE # 2
• 38 year old man presents to clinic with complaints of weight loss. Slowly losing weight over past year (from about 60kg to 54kg).
• No other complaints (no fever, cough, chills, etc.)
• Says he has noticed large 6-7cm worms in his stool.

CASE # 2
• Given weight loss, HIV testing advised and performed and patient is HIV positive.
• Stool test done and is positive for eggs of Ascaris lumbricoides and hookworm species.
WHAT SHOULD BE DONE (IF ANYTHING?).
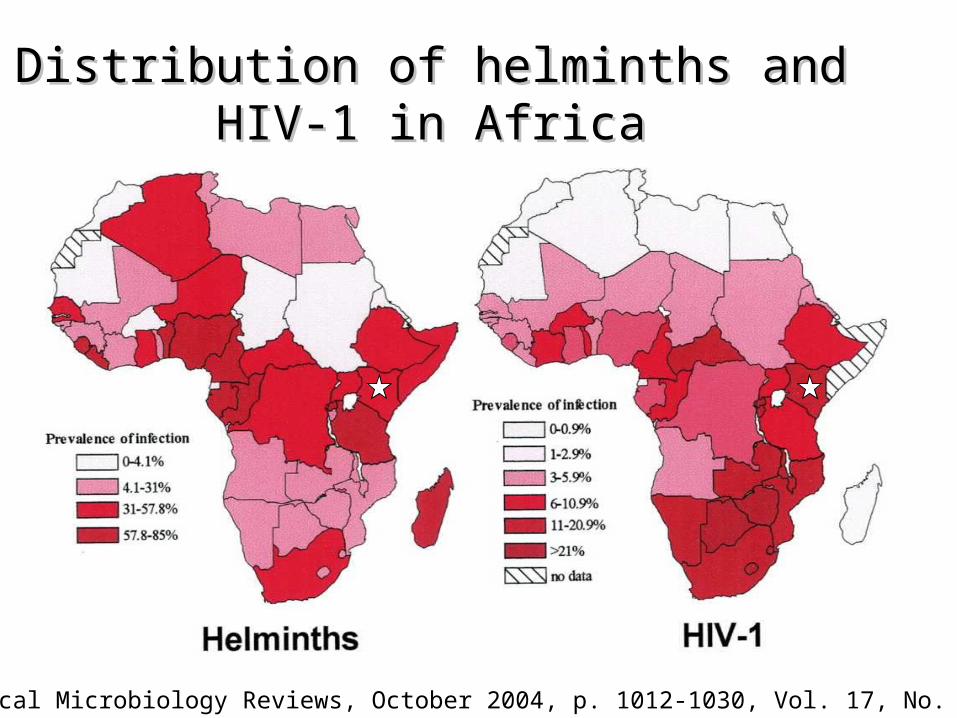
Distribution of helminths and HIV-1 in Distribution of helminths and HIV-1 in AfricaAfrica
Clinical Microbiology Reviews, October 2004, p. 1012-1030, Vol. 17, No. 4

Epidemiology Over Over 2 billion 2 billion people are estimated to be infected with people are estimated to be infected with
at least one species of helminths.at least one species of helminths.
In fact, about 25% of the worlds population is infested In fact, about 25% of the worlds population is infested with one or more soil transmitted helminth.with one or more soil transmitted helminth.
Of the approximately 25 million people infected with Of the approximately 25 million people infected with HIV-1 in Africa, as many as HIV-1 in Africa, as many as 50-90% 50-90% may also be may also be infected with a soil transmitted helminth.infected with a soil transmitted helminth.


1.1. Helminth egg burden correlated with Helminth egg burden correlated with HIV-1 viral loadHIV-1 viral load
J Acquir Immune Defic Syndr, Volume 31(1).September 1, 2002.56-62

Walson JL, John-Stewart G. Treatment of helminth co-infection in HIV-1 infected individuals in resource-limited settings. Cochrane Database of Systematic Reviews 2008, Issue 1. Art. No.: CD006419. DOI: 10.1002/14651858.CD006419.pub2.

AIDS 2008; 22:1–9.

Effects on CD4 and Viral Load
AIDS 2008; 22:1–9.

Case #3
• An HIV infected mother brings her 1 year old son in to clinic because his sibling (age 3) has had “measles” (diagnosed at local facility).
• The child is HIV positive by antibody testing.• Currently the child is well, playing and does
not appear ill.– What can/should be done to protect the child?– What other interventions/testing could be done
for the child?

Measles and HIV
• Measles is exacerbated by HIV infection.• HIV infected individuals shed the virus longer.• Vaccination is less effective in individuals with
HIV.• Measles vaccine is a “live” virus vaccine so
there may be risks with it’s use.

HIV and Measles - Mortality
CID 2008; 46:523-7.
Measles occurs at younger ages (more likely to occur at age <9 months)
AND is associated with increased mortality even after controlling for age, sex, and measles vaccination status.

PREVENTION
• In areas where there is a risk of measles transmission – ALL children (including those with HIV – regardless of degree of immunosuppression) should be vaccinated??
• Consider early vaccination in HIV infected children at 6-9 months
• Where available, monthly IgG can be given to exposed children who have poor vaccine response.
CID 2007. 45 (9) pp. 1214-20

Treatment
• Supportive care• Vitamin A – shown to reduce mortality and
lead to more rapid resolution of pneumonia and diarrhea. Most data in children under 2.
• ?Ribavirin where available for severe cases. No RCT data.
N Engl J Med 1990 Jul 19;323(3):160, JAMA 1989 May 5;261(17):2512-6.
Thank you!Next session: May 6, 2010
HIV Dermatology – Most Interesting Case Contest
Dr Roy Colven