WELCOME! 2009 KPTA Town Meeting
83
1 WELCOME! 2009 KPTA Town Meeting Kansas Physical Therapy Association Topeka, Kansas 66603 785-233-5400 Fax: 785-290-0476 Email: [email protected] www.kpta.com
-
Upload
walker-ortiz -
Category
Documents
-
view
25 -
download
0
description
WELCOME! 2009 KPTA Town Meeting. Kansas Physical Therapy Association Topeka, Kansas 66603 785-233-5400 Fax: 785-290-0476 Email: [email protected] www.kpta.com. AGENDA. APTA Branding Campaign Payment/Reimbursement Update: Local & National Issues APTA Code of Ethics Update - PowerPoint PPT Presentation
Transcript of WELCOME! 2009 KPTA Town Meeting

1
WELCOME! 2009 KPTA
Town Meeting
Kansas Physical Therapy AssociationTopeka, Kansas 66603
785-233-5400 Fax: 785-290-0476Email: [email protected]
www.kpta.com

22
AGENDA
APTA Branding Campaign
Payment/Reimbursement Update: Local & National Issues
APTA Code of Ethics Update 2010 KPTA Legislative Plan Update
KPTA Website Update
2009 TOWN HALL MEETINGS
Pittsburg at Mt. Carmel Medical Center - Oct. 13
K.C. at Shawnee Mission Medical Center - Oct. 19
Manhattan at Mercy Regional Health Center - Oct. 22
Wichita at Via Christi - St. Francis Campus - Oct. 29
Topeka at Washburn University - Nov. 2
K.C. at Olathe Medical Center - Nov. 3
Great Bend at Advance Therapy & Sports Med. - Nov. 3
Salina at Comcare - Nov. 5
Colby at Colby Community College - Nov. 5
SW Kansas via Webconference - Nov. 5
33

4
American Physical Therapy Association
The Physical Therapy Brand
Learn It. Live It. Share it. Wear it.

Brand FundamentalsBrands define expectation
Brands live everywhere
Brands are hard tocreate
Brands are easy to destroy
Brands can be influenced
Brands are not fully controlled
5

6
A good brandevokes emotion.
Good brands connect on a subconscious level.

A good brand is relevant.
It makes a connection.
It stimulates opinions.
A good brand is consistent.
A good brand is strategic.7
8
So, how are we doing?

9
Evaluation of the Physical Therapist Brand
Existing Strength• Esteem: Is it held in high regard?
• Knowledge: What is the level of understanding?
Potential• Differentiation: How distinctive is the brand?
• Relevance: Is it meaningful to those who use us?

Esteem: High
Nearly 90% of all consumers have a positive impression of physical therapists
• 80% of physical therapy users likely to consider using a physical therapist in the future
• 68% of non-users likely to consider a physical therapist in the future
• 84% of physical therapy users would refer a friend or family member to their physical therapist
• 88% of physical therapy users say care was very or somewhat beneficial 10

11
Consumers are confused…
Who do I go to? And for what condition?
Differentiation: Blurred

12
•On the whole, physicians did not believe the DPT would improve clinical abilities and were concerned that it would drive the cost of physical therapy even higher
•Physicians did not support direct access because they do not trust physical therapists to diagnose possible underlying medical conditions
•While consumers do not view physical therapists as doctors, they do see the DPT designation as valuable. In fact, 73% were more likely to consider a physical therapist if they knew that they had completed requirements for a DPT.
Differentiation: Blurred

13
94% of consumers have gone to their PCP for pain relief and improvement in movement or performance of daily activities
While many consumers still want their PCP to “diagnose”, more than half say they are more likely to use physical therapists if they could “treat” patients without a doctor’s referral
Relevance: Growing

14
Consumers are looking for prevention and wellness options
Consumers would be more likely to use a physical therapist if
they knew she/he could:
Significantly improve mobility to perform daily activities
Provide an alternative to surgery, in many cases
Manage or eliminate pain without medication, in many cases
Relevance: Growing

15
ProblemPain
Physical Therapist
PILL/RUB PCP/NP Orthopedists
Chiropractor
Physical Therapist
Brand Opportunity: Earlier Mindshare “What
about the physical therapist option?”

16
Expand Mindshare of Physical Therapy
Rehabilitation
MOTION
The Physical Therapist = MOTION
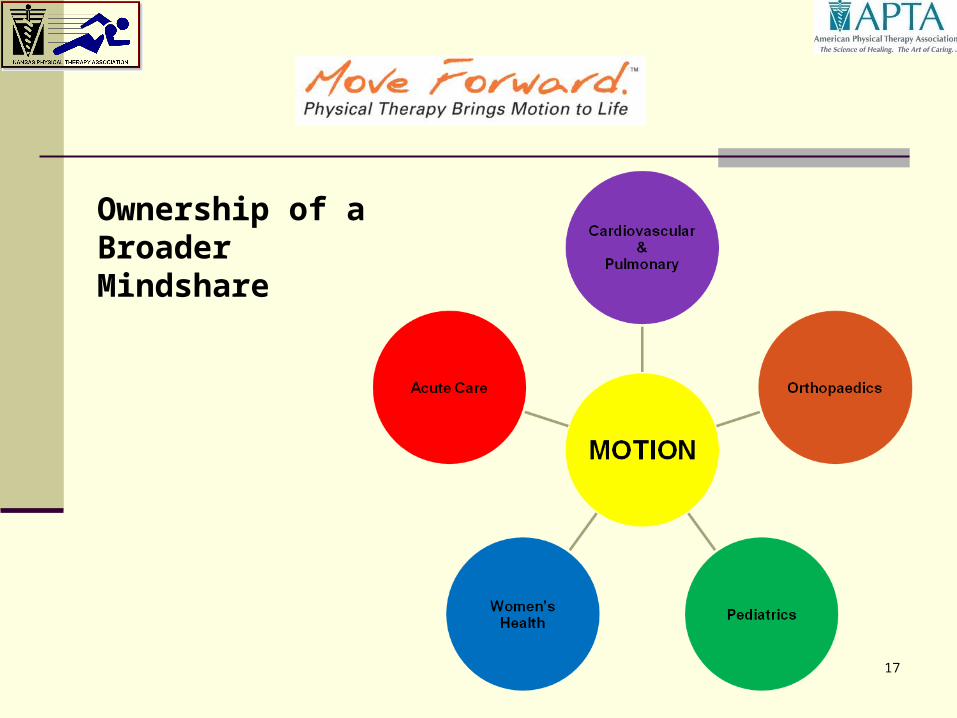
17
Ownership of aBroader Mindshare

18
Our Brand PromiseWhat we do:
Physical therapists help you
restore and improve motion
to achieve long-term quality
of life.

19
Our Key Words and Phrases
What we say:
•Physical therapists can help you improve mobility, in many cases, without surgery or pain medication
•Physical therapists have extensive education and expertise
•Physical therapists can help you prevent or manage a health condition

20
Our Tag Line

21
It matters because our brand can…
Influence
Protect
Differentiate
Command a Premium

22
We need to act now because…
Our future is uncertain.

23
Because we care.
Because we have influence.
Because we are the brand.
Our brand needs us…

How do I start?
Step 1:Learn the
brand
www.APTA.org
Brandbeat Resources
www.MoveForwardPT.com
Step 2:Live the brand Be professional.
Be entrepreneurial.
Be knowledgeable.
Be consistent.24

25
Tools You Can Use to Live
and Breathe the Brand
• BrandBeat at www.apta.org/brandbeat
• Consumer Web site – www.moveforwardpt.com
• Brand Video on www.youtube.com

26
KPTA Plans for the Brand Links on KPTA website
Promote at KPTA and community events
Informational handouts, media advertising
Encouraging you to use APTA resources to promote and “live the brand” in your region

Payment/ Reimbursement Update: Local & National Issues
Maximizing and Protecting It
28

29
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
Documentation
Computerized documentation appears “canned” with little to no originality from provider
Abbreviations are not standard – should avoid
No documented time frames
What was provided for codes billed is not clearly documented

30
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
Documentation
Skill (why service of PT / PTA needed)
BCBSKS released a letter to all Kansas PT providers contracted with BCBSKS on September 21, 2009 that outlines what medical necessity is and standards for documentation

31
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
Modalities (lack of documented rationale or rationale “canned”)
No tapering
Ultrasound and HP to the same body part same day repeatedly
Massage and Man Therapy for the same body part same day repeatedly
Ultrasound and E-stim to the same body part same day repeatedly

32
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
Length of episode of care
Medically necessary versus maintenance
Co-morbidities and confounding factors not clearly documented
Referral source sends patient back despite PT recommendation to D/C

33
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
“Decompression Therapy” versus “Decompression Traction”
Length of episode of care
Multiple modalities included as well as braces and foot orthotics
All patients get the same type of treatment (package deal)

34
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
PT signs note however handwriting in body of note is different
Qualified provider of services
Utilization of available documentation resources

35
CONCERNS SHARED BY BLUE CROSS BLUE SHIELD KANSAS
Patient signing a waiver for non-covered services This excludes modalities considered “content of service”
When is good enough – “good enough” Trying to achieve function higher than pre morbid function

36
Educate yourself on all codes and proper utilization
Educate yourself on all available resources for documentation
“Say what you see” and “what your skill is”
Documentation “Quality” versus “Quantity”
Ask yourself “if I had to pay for this would I pay based on what is in my documentation?”
READ and become familiar with BCBSKS – Business Procedure Manual ( Appendix F: Occupational and Physical Therapy Guidelines ( pages F 1 – F 33) http://www.bcbsks.com/CustomerService/Providers/Publications/professional/manuals/pdf/BPMappF_OccPT.pdf

37
SEE HANDOUTS

Recovery Audit Contractors (RACs) and Medicare(materials accessed from www. cms.hhs.gov/RAC www. cms.hhs.gov/RAC September 13, 2009) September 13, 2009)
KPTATOWN HALL MEETINGS

39
What is a RAC?
The RACs detect and correct past improper payments so that CMS and Carriers, FIs, and MACs can implement actions that will prevent future improper payments
Providers can avoid submitting claims that do not comply with Medicare rules
CMS can lower its error rate
Taxpayers and future Medicare beneficiaries are protected

40
Will the RACs affect me?
Yes, if you bill fee-for-service programs
Claims will be subject to review by the RACs
If so, when? The expansion schedule can be viewed at
www.cms.hhs.gov/rac
41
CMS RAC Review Phase-in Strategies as of 06/24/09
Earliest possible dates for reviews in yellow/green states
KANSAS (Region D: HealthDataInsights, Inc.-Part A: 866-590-5598, Part B: 866-376-2319, e-mail: [email protected] )
Automated Review-Black & White Issues (June 2009)
DRG Validation-complex review (Aug/Sept 2009)
Complex Review for coding errors (Aug/Sept 2009)
DME Medical Necessity Reviews-complex review (Fiscal year 2010)
Medical Necessity Reviews-complex review (calendar year 2010)

42
RAC Legislation
Medicare Modernization Act, Section 306
Required the three year RAC demonstration
Tax Relief and Healthcare Act of 2006, Section 302
Requires a permanent and nationwide RAC program by no later than 2010
Both Statutes gave CMS the authority to pay the RACs on a contingency fee basis.

43
What does a RAC do? RACs review claims on a post-payment basis
RACs use the same Medicare policies as Carriers, FIsand MACs: NCDs, LCDs and CMS Manuals
Two types of review: Automated (no medical record needed) Complex (medical record required)
RACs will not be able to review claims paid prior to October 1, 2007
RACs will be able to look back three years from the date the claim was paid
RACs are required to employ a staff consisting of nurses, therapists, certified coders, and a physician

44
The Collection Process
Same as for Carrier, FI and MAC identified overpayments (except the demand letter comes from the RAC)
Carriers, FIs and MACs issue Remittance Advice Remark Code N432: Adjustment Based on Recovery Audit
Carrier/FI/MAC recoups by offset unless provider has submitted a check or a valid appeal

45
What is different?Demand letter is issued by the RAC:
RAC will offer an opportunity for the provider to discuss the improper payment determination with the RAC (this is outside the normal appeal process)
Issues reviewed by the RAC will be approved by CMS prior to widespread review
Approved issues will be posted to a RAC website before widespread review
46
What are providers’ options?
If you agree with the RAC’s determination:1. Pay by check2. Allow recoupment from future payments3. Request or apply for extended payment plan4. Appeal
Appeal Timeframes: http://www.cms.hhs.gov/OrgMedFFSAppeals/Downloads/Appealsproce ssflowchartAB.pdf
935 MLN Mattershttp://www.cms.hhs.gov/MLNMatterArticles/downloads/MM6183.pdf

47
Three Keys to Success
Minimize Provider Burden
Ensure Accuracy
Maximize Transparency

48
Minimize Provider Burden
Limit the RAC “look back period” to three years
Limit the number of medical record requests
Maximum look back date is October 1, 2007
RACs will accept imaged medical records on CD/DVD (CMS requirements coming soon)

49
Summary of Medical Record Limits (FY 2009)
Inpatient Hospital, IRF, SNF, Hospice 10% of the average monthly Medicare claims (max 200) per 45 days per NPI
Other Part A Billers (HH) 1% of the average monthly Medicare episodes of care (max 200) per 45 days per
NPI
Physicians (including podiatrists, chiropractors) Sole Practitioner: 10 medical records per 45 days per NPI Partnership (2-5 individuals): 20 medical records per 45 days per NPI Group (6-15 individuals): 30 medical records per 45 days per NPI Large Group (16+ individuals): 50 medical records per 45 days per NPI
Other Part B Billers (DME, Lab, Outpatient Hospital) 1% of the average monthly Medicare claim lines (max 200) per NPI per
45 days

50
Ensure Accuracy
Each RAC employs: Certified coders Nurses Therapists A physician CMD
CMS’ New Issue Review Board provides greater oversight
RAC Validation Contractor provides annual accuracy scores for each RAC
If a RAC loses at any level of appeal, the RAC must return its contingency fee

51
Maximize Transparency
New issues are posted to the web
Vulnerabilities are posted to the web
RAC claim status website (2010)
Detailed Review Results Letter following all Complex Reviews

52
What can providers do to get ready?
Know where previous improper payments have been found
Look to see what improper payments were found by the RACs: Demonstration findings: www.cms.hhs.gov/rac Permanent RAC findings: will be listed on the RACs’
websites
Look to see what improper payments have been found in OIG and CERT reports: OIG reports: www.oig.hhs.gov/reports.html CERT reports: www.cms.hhs.gov/cert
53
Know if you are submitting claims with improper payments
Conduct an internal assessment to identify if you are in compliance with Medicare rules
Identify corrective actions to promote compliance
Appeal when necessary
Learn from past experiences

54
Prepare to respond to RAC medical record requests
Tell your RAC the precise address and contact person they should use when sending Medical Record Request Letters Call RAC No later 1/1/2010: Use RAC websites
When necessary, check on the status of your medical record (Did the RAC receive it?) Call RAC No later 1/1/2010: use RAC websites

55
Appeal when necessary
The appeal process for RAC denials is the same as the appeal process for Carrier/FI/MAC denials
Do not confuse the “RAC Discussion Period” with the Appeals process
If you disagree with the RAC determination… Do not stop with sending a discussion letter
File an appeal before the 120th day after the Demand letter

56
Learn from past experiences
Keep track of denied claims
Look for patterns
Determine what corrective actions you need to take to avoid improper payments

57
APTA RECOMMENDATIONSAPTA RECOMMENDATIONS
APTA website: apta.org.
Log in and search for
the RAC link.
NEW Code of Ethics and Standards of Conduct
Effective July 1, 2010

60
Adopted by the 2009 House of Delegates
Disseminated to all members Shared with the state licensing boards Shared with all Education Program Directors Available on the APTA website which will also
include a Frequently Asked Questions about the Code/Standards
Ethics and Judicial Committee will develop online courses
PT Magazine …”Ethics in Action”

61
Encompasses the five roles we play in contemporary medicine
Clinical Management of the patient/client
ConsultantEducatorResearcherAdministrator

62
Code/Standards is built upon the seven core values of the profession
Accountability Altruism Compassion/caring Excellence Integrity Professional Duty Social Responsibility
63
PurposeDefines the ethical principles that form the foundation of physical therapy practice.

64
PurposeProvides standards of
behavior and performance that form the basis of professional accountability to the public.

65
PurposeProvides guidance for
facing ethical challenges, regardless of their professional roles and responsibilities.

66
PurposeEducate physical therapists,
physical therapist assistants, students, other health care professionals, regulators and the public regarding the core values, ethical principles and standards that guide our professional conduct.

67
PurposeEstablishes the standards by
which the APTA can determine if a physical therapist/physical therapist assistant has engaged in unethical conduct.

68
Now 8 vs 11 principles Ex. Principle # 7 in the Code of Ethics: Physical therapists shall promote
organizational behaviors and business practices that benefit patients/clients and society.
7A. PTs shall promote practice environments that support autonomous and accountable professional judgments.
7B. PTs shall seek remuneration as is deserved and reasonable for PT services.

69
Principle 7 Continued…7C. PTs shall not accept gifts or other considerations that
influence or give an appearance of influencing their professional judgment.
7D. PTs shall disclose any financial interest they have in products or services that they recommend to patients/clients.
7E. PTs shall be aware of charges and shall ensure documentation and coding for PT services accurately reflect the nature and extent of services provided.
7F. PTs shall refrain from employment arrangements, or other arrangements, that prevent PTs from fulfilling professional obligations to patients/clients.

70
Standard #7 in Ethical Conduct for the PTA
PTAs shall support organizational behaviors and business practices that benefit patients/clients and society.
7A. PTAs shall promote work environments that support ethical and accountable decision-making.
7B. PTAs shall not accept gifts or other considerations that influence or give an appearance of influencing their decisions.

71
Standard #7 continued…7C. PTAs shall fully disclose any financial interest
they have in products or services they recommend to patients/clients.
7D. PTAs shall ensure that documentation for their interventions accurately reflects the nature and extent of the services provided.
7E. PTAs shall refrain from employment arrangements, or other arrangements, that prevent PTAs from fulfilling ethical obligations to patients/clients.

72
Fundamental to Code/Standard…A special obligation to empower, educate
and enable those with impairments, activity limitations, participation restrictions, and disabilities to facilitate greater independence, health, wellness, and enhanced quality of life.

2010 KPTA LEGISLATIVE PLAN
MOVE FORWARD!
73

74
2010 LEGISLATIVE PLAN Propose legislation to remove the direct
access provisions:
Remove the previous referral to a PT provision Remove the referral within one year provision Remove the provision for same diagnosis
74

75
2010 LEGISLATIVE PLAN Keep:
Treatment for thirty (30) days before referring to a M.D., D.O., etc.
Transmit evaluation report to one of the above practitioners of patient’s choice within five days
75

76
QUESTIONS / CONCERNS? Does everyone support this legislative plan?
Concerns about it or about expanding direct access in Kansas?
Questions?
Interest in getting involved in making this happen? Key contact, etc.
76

KPTA Website UPDATE
www.kpta.com
77

78
WEBSITE UPDATE
78

SPRING, 2010CALL FOR AWARDS
Please submit nominations
by January 4, 2010.
79

80
KPTA AWARDSSusan Tork Distinguished Service Award: to honor a member who has
given honorable, dedicated, and meritorious service to the chapter and community at large.
Distinguished Clinical Service Award: to honor a peer who has given long, loyal, and professional clinical service to the profession through serving the needs of their patients, coworkers, and community at large.
Carolyn Bloom Lifetime Achievement Award: to honor long-standing members of the KPTA.
Outstanding Physical Therapist Student Award and the Candy Bahner Outstanding Physical Therapist Assistant Student Award: to honor outstanding students
Award for Academic Excellence: to recognize a faculty member within Kansas who has made significant contributions to physical therapy education.
Friend of Physical Therapy: to honor those who have contributed to the profession of physical therapy and the chapter as a whole.
80

81
Contact Information
Please contact the members of the nominating committee if you have any questions:
Julie Newman, PTA
Candy Bahner, PT, DPT
KPTA Office: Phone: (785) 233-5400 Fax: (785) 290-0476
KPTA website: www.kpta.com81

82
KPTA PAC FundraiserBeautiful San Diego for APTA’S CSM in February!
3 nights in hotel, dinner for 2 at hotel and CSM registration = $1200 value!!!
Tickets: 1 for $20 or 3 for $50
Contact KPTA PAC for tickets.
82

8383
Thank you
for attending the KPTA Town Meeting.
If you have any questions regarding membership or any of the issues discussed
tonight please contact the KPTA office at 785.233.5400 or [email protected].