Weight effects associated with antipsychotics: A comprehensive database analysis
8
Weight effects associated with antipsychotics: A comprehensive database analysis Bruce Parsons a, ⁎, David B. Allison b , Antony Loebel a , Kathryn Williams a , Earl Giller a , Steven Romano a , Cynthia Siu c a Pfizer Inc., 235 E. 42nd Street, New York, NY 10017-5755, USA b Clinical Nutrition Research Center and Department of Biostatistics, University of Alabama at Birmingham, Birmingham, AL, 35294-0022, USA c Data Power (DP), Inc., One Palomino Court, Ringoes, NJ 08551-1916, USA article info abstract Article history: Received 9 July 2008 Accepted 29 September 2008 Available online 24 March 2009 Background: Available data on atypical antipsychotic-induced weight gain are limited by a number of methodological factors. The objective of this report is to evaluate short-term (N =1742) and long-term (N =1649) weight effects in patients receiving standard doses of amisulpride, haloperidol, olanzapine, risperidone, ziprasidone, and placebo based on 21 randomized, placebo-controlled, parallel-group studies from an integrated clinical trial database. Method: Analyses of the integrated ziprasidone schizophrenia trials database were performed to estimate the weighted average of weight change and the percentage of subjects experiencing weight gain (or weight loss) across studies for each agent studied, based on fixed- and random- effects models. Durations of treatment exposure in long-term trials were controlled by well- defined time windows (6 month: 150 to 210 days; 1 year: 330 to 390 days). Weight gain or loss was defined using a 7% change from baseline threshold. Results: During long-term therapy with 1-year treatment duration, incidence of weight gain for subjects treated with ziprasidone (17%) was not significantly different from the placebo (13%) or haloperidol (41%) groups based on 95% confidence interval. In contrast, significantly greater weight gain incidence was observed for the olanzapine (57%) and risperidone (39%) groups compared to placebo. Median weight change of + 0.49, -0.18, +1.50 and +0.55 lb/month was observed for haloperidol, ziprasidone, olanzapine and risperidone subjects, respectively, indicating differential weight change patterns compared to placebo (-0.32). Similar results were observed for the short-term (4–12 weeks) and 6-month treatment exposure cohorts. Conclusions: Our results confirm significant differences in long-term weight effects among atypical antipsychotics, consistent with findings from prior meta-analysis of antipsychotic- induced weight gain [Allison, D.B., Mentore, J.L., Heo, M., Chandler, L.P., Capelleri, J.C., Infante, M.C., Weiden, P.J., 1999. Antipsychotic induced weight gain: a comprehensive research synthesis. Am J Psychiatry 156, 1686–1696] and the CATIE schizophrenia study [Lieberman, J.A., Stroup, T.S., McEvoy, J.P., et al., 2005. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 353, 1209–1223]. © 2008 Elsevier B.V. All rights reserved. Keywords: Weight effects Antipsychotics Schizophrenia 1. Introduction Schizophrenia is a chronic, debilitating illness requiring long-term treatment with antipsychotic medications. Patients with schizophrenia are at increased risk for developing obesity (Fontaine et al., 2001; Myer and Nasrallah, 2003; Schizophrenia Research 110 (2009) 103–110 ⁎ Corresponding author. Pfizer, Inc., 235 E. 42nd Street, New York, NY 10017-5755, USA. Tel.: +1212 733 4936; fax: +1 212 808 8777. E-mail address: bruce.parsons.@pfizer.com (B. Parsons). 0920-9964/$ – see front matter © 2008 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2008.09.025 Contents lists available at ScienceDirect Schizophrenia Research journal homepage: www.elsevier.com/locate/schres
-
Upload
bruce-parsons -
Category
Documents
-
view
212 -
download
0
Transcript of Weight effects associated with antipsychotics: A comprehensive database analysis

Schizophrenia Research 110 (2009) 103–110
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres
Weight effects associated with antipsychotics: A comprehensivedatabase analysis
Bruce Parsons a,⁎, David B. Allison b, Antony Loebel a, Kathryn Williams a, Earl Giller a,Steven Romano a, Cynthia Siu c
a Pfizer Inc., 235 E. 42nd Street, New York, NY 10017-5755, USAb Clinical Nutrition Research Center and Department of Biostatistics, University of Alabama at Birmingham, Birmingham, AL, 35294-0022, USAc Data Power (DP), Inc., One Palomino Court, Ringoes, NJ 08551-1916, USA
a r t i c l e i n f o
⁎ Corresponding author. Pfizer, Inc., 235 E. 42nd10017-5755, USA. Tel.: +1 212 733 4936; fax: +1 212
E-mail address: [email protected] (B. Pars
0920-9964/$ – see front matter © 2008 Elsevier B.V.doi:10.1016/j.schres.2008.09.025
a b s t r a c t
Article history:Received 9 July 2008Accepted 29 September 2008Available online 24 March 2009
Background: Available data on atypical antipsychotic-induced weight gain are limited by anumber of methodological factors. The objective of this report is to evaluate short-term(N=1742) and long-term (N=1649) weight effects in patients receiving standard doses ofamisulpride, haloperidol, olanzapine, risperidone, ziprasidone, and placebo based on 21randomized, placebo-controlled, parallel-group studies from an integrated clinical trialdatabase.Method: Analyses of the integrated ziprasidone schizophrenia trials database were performedto estimate theweighted average of weight change and the percentage of subjects experiencingweight gain (or weight loss) across studies for each agent studied, based on fixed- and random-effects models. Durations of treatment exposure in long-term trials were controlled by well-defined time windows (6 month: 150 to 210 days; 1 year: 330 to 390 days). Weight gain or losswas defined using a 7% change from baseline threshold.Results: During long-term therapy with 1-year treatment duration, incidence of weight gain forsubjects treated with ziprasidone (17%) was not significantly different from the placebo (13%)or haloperidol (41%) groups based on 95% confidence interval. In contrast, significantly greaterweight gain incidence was observed for the olanzapine (57%) and risperidone (39%) groupscompared to placebo. Medianweight change of +0.49,−0.18, +1.50 and+0.55 lb/month wasobserved for haloperidol, ziprasidone, olanzapine and risperidone subjects, respectively,indicating differential weight change patterns compared to placebo (−0.32). Similar resultswere observed for the short-term (4–12 weeks) and 6-month treatment exposure cohorts.Conclusions: Our results confirm significant differences in long-term weight effects amongatypical antipsychotics, consistent with findings from prior meta-analysis of antipsychotic-induced weight gain [Allison, D.B., Mentore, J.L., Heo, M., Chandler, L.P., Capelleri, J.C., Infante,M.C., Weiden, P.J., 1999. Antipsychotic induced weight gain: a comprehensive researchsynthesis. Am J Psychiatry 156, 1686–1696] and the CATIE schizophrenia study [Lieberman,J.A., Stroup, T.S., McEvoy, J.P., et al., 2005. Effectiveness of antipsychotic drugs in patientswith chronic schizophrenia. N Engl J Med 353, 1209–1223].
© 2008 Elsevier B.V. All rights reserved.
Keywords:Weight effectsAntipsychoticsSchizophrenia
Street, New York, NY808 8777.ons).
All rights reserved.
1. Introduction
Schizophrenia is a chronic, debilitating illness requiringlong-term treatment with antipsychotic medications. Patientswith schizophrenia are at increased risk for developingobesity (Fontaine et al., 2001; Myer and Nasrallah, 2003;
104 B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
Wirshing, 2004) and some atypical antipsychotics have beenreported tobeassociatedwithundesirablemetabolic side effectsand weight gain. Clozapine, olanzapine, and to a lesser extent,risperidone and quetiapine, have all been implicated in causingweight gain (Allison et al., 1999; Newcomer, 2005; NewcomerandHennekens, 2007). In contrast, previous reports suggest thataripiprazole and ziprasidone are associated with lower overallrisks for weight gain, diabetes, and worsening lipid profiles(American Diabetes Association et al., 2004; Newcomer, 2005).
Despite heightened interest in the health implications andclinical importance of atypical antipsychotic-induced weightgain, most studies that assess weight change are short-termin duration (b6 months). Long-term data, beyond 6 months,have been typically limited by a number of methodologicaland design factors, and the conclusions are thus lessdefinitive. These limiting factors have included small samplesizes, lack of a control group, biasing effects of individualvariations in treatment exposure and prior antipsychotic use,and the use of study designs that are less rigorous thanrandomized, double-blind trials. Such factors render compar-ison and interpretation of long-term weight change difficult,if not impossible (Wetterling, 2001; Gentile, 2006). Beyondrecognizing clozapine on the one hand and both ziprasidoneand aripiprazole on the other as representing opposite poleson the weight-gain spectrum, review of existing literatureshows contradictory results for the degree of weight gainassociated with long-term use of other atypical agents(American Diabetes Association, et al., 2004; Gentile, 2006).
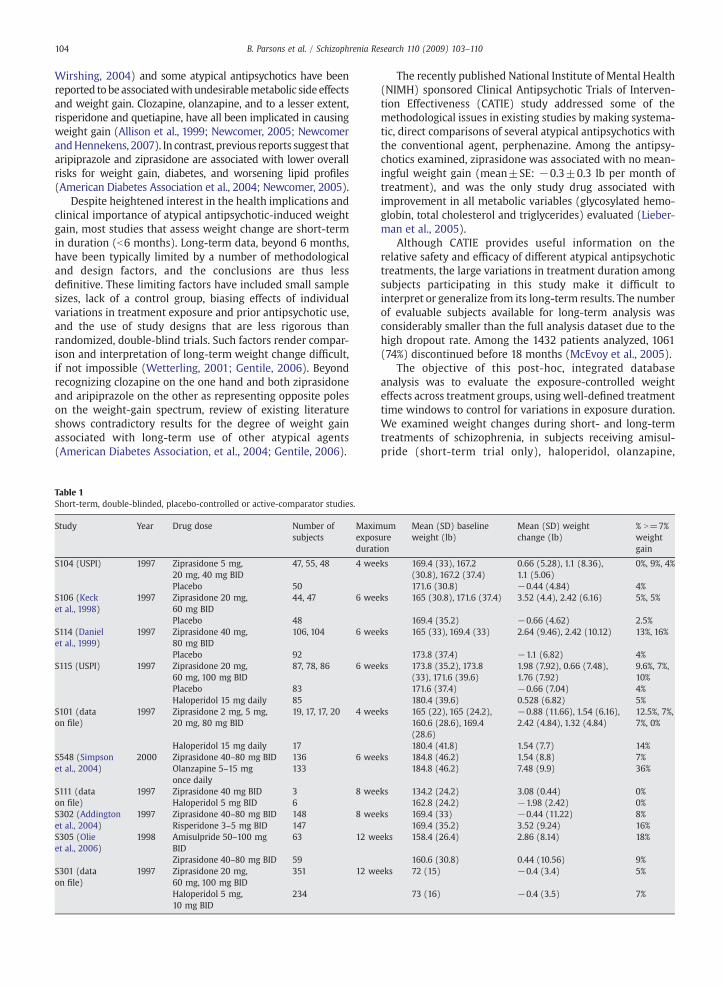
Table 1Short-term, double-blinded, placebo-controlled or active-comparator studies.
Study Year Drug dose Number ofsubjects
Maximexposdurat
S104 (USPI) 1997 Ziprasidone 5 mg,20 mg, 40 mg BID
47, 55, 48 4 wee
Placebo 50S106 (Kecket al., 1998)
1997 Ziprasidone 20 mg,60 mg BID
44, 47 6 wee
Placebo 48S114 (Danielet al., 1999)
1997 Ziprasidone 40 mg,80 mg BID
106, 104 6 wee
Placebo 92S115 (USPI) 1997 Ziprasidone 20 mg,
60 mg, 100 mg BID87, 78, 86 6 wee
Placebo 83Haloperidol 15 mg daily 85
S101 (dataon file)
1997 Ziprasidone 2 mg, 5 mg,20 mg, 80 mg BID
19, 17, 17, 20 4 wee
Haloperidol 15 mg daily 17S548 (Simpsonet al., 2004)
2000 Ziprasidone 40–80 mg BID 136 6 weeOlanzapine 5–15 mgonce daily
133
S111 (dataon file)
1997 Ziprasidone 40 mg BID 3 8 weeHaloperidol 5 mg BID 6
S302 (Addingtonet al., 2004)
1997 Ziprasidone 40–80 mg BID 148 8 weeRisperidone 3–5 mg BID 147
S305 (Olieet al., 2006)
1998 Amisulpride 50–100 mgBID
63 12 we
Ziprasidone 40–80 mg BID 59S301 (dataon file)
1997 Ziprasidone 20 mg,60 mg, 100 mg BID
351 12 we
Haloperidol 5 mg,10 mg BID
234
The recently published National Institute of Mental Health(NIMH) sponsored Clinical Antipsychotic Trials of Interven-tion Effectiveness (CATIE) study addressed some of themethodological issues in existing studies by making systema-tic, direct comparisons of several atypical antipsychotics withthe conventional agent, perphenazine. Among the antipsy-chotics examined, ziprasidone was associated with no mean-ingful weight gain (mean±SE: −0.3±0.3 lb per month oftreatment), and was the only study drug associated withimprovement in all metabolic variables (glycosylated hemo-globin, total cholesterol and triglycerides) evaluated (Lieber-man et al., 2005).
Although CATIE provides useful information on therelative safety and efficacy of different atypical antipsychotictreatments, the large variations in treatment duration amongsubjects participating in this study make it difficult tointerpret or generalize from its long-term results. The numberof evaluable subjects available for long-term analysis wasconsiderably smaller than the full analysis dataset due to thehigh dropout rate. Among the 1432 patients analyzed, 1061(74%) discontinued before 18 months (McEvoy et al., 2005).
The objective of this post-hoc, integrated databaseanalysis was to evaluate the exposure-controlled weighteffects across treatment groups, using well-defined treatmenttime windows to control for variations in exposure duration.We examined weight changes during short- and long-termtreatments of schizophrenia, in subjects receiving amisul-pride (short-term trial only), haloperidol, olanzapine,
umureion
Mean (SD) baselineweight (lb)
Mean (SD) weightchange (lb)
% N=7%weightgain
ks 169.4 (33), 167.2(30.8), 167.2 (37.4)
0.66 (5.28), 1.1 (8.36),1.1 (5.06)
0%, 9%, 4%
171.6 (30.8) −0.44 (4.84) 4%ks 165 (30.8), 171.6 (37.4) 3.52 (4.4), 2.42 (6.16) 5%, 5%
169.4 (35.2) −0.66 (4.62) 2.5%ks 165 (33), 169.4 (33) 2.64 (9.46), 2.42 (10.12) 13%, 16%
173.8 (37.4) −1.1 (6.82) 4%ks 173.8 (35.2), 173.8
(33), 171.6 (39.6)1.98 (7.92), 0.66 (7.48),1.76 (7.92)
9.6%, 7%,10%
171.6 (37.4) −0.66 (7.04) 4%180.4 (39.6) 0.528 (6.82) 5%
ks 165 (22), 165 (24.2),160.6 (28.6), 169.4(28.6)
−0.88 (11.66), 1.54 (6.16),2.42 (4.84), 1.32 (4.84)
12.5%, 7%,7%, 0%
180.4 (41.8) 1.54 (7.7) 14%ks 184.8 (46.2) 1.54 (8.8) 7%
184.8 (46.2) 7.48 (9.9) 36%
ks 134.2 (24.2) 3.08 (0.44) 0%162.8 (24.2) −1.98 (2.42) 0%
ks 169.4 (33) −0.44 (11.22) 8%169.4 (35.2) 3.52 (9.24) 16%
eks 158.4 (26.4) 2.86 (8.14) 18%
160.6 (30.8) 0.44 (10.56) 9%eks 72 (15) −0.4 (3.4) 5%
73 (16) −0.4 (3.5) 7%
105B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
risperidone, ziprasidone, and placebo treatment in 21randomized, controlled trials.
2. Materials and methods
2.1. Database description
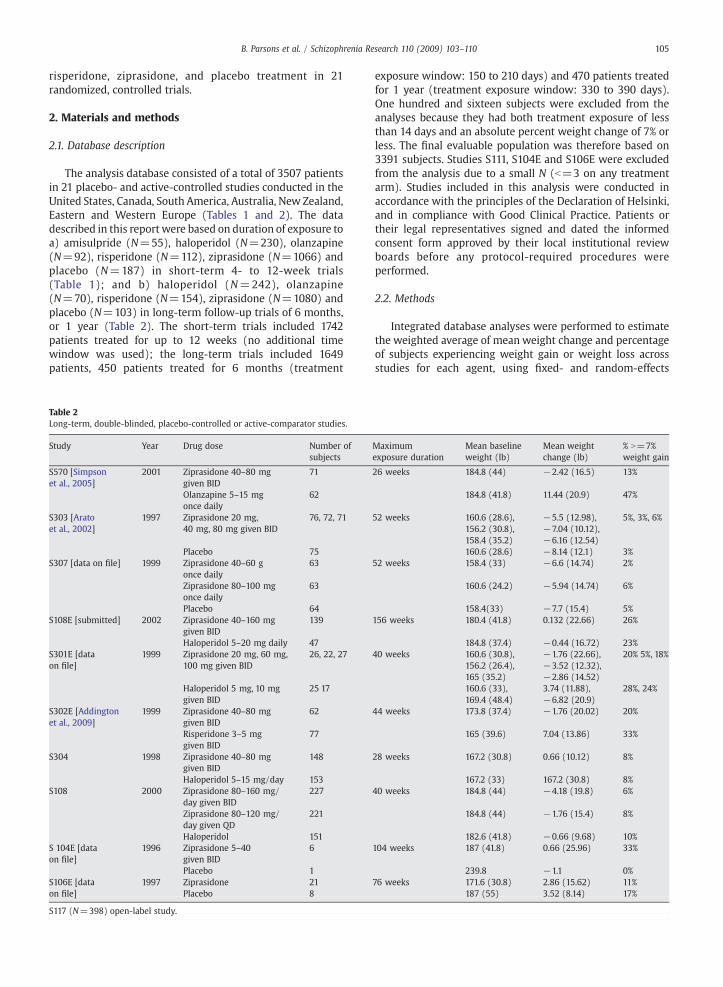
The analysis database consisted of a total of 3507 patientsin 21 placebo- and active-controlled studies conducted in theUnited States, Canada, South America, Australia, New Zealand,Eastern and Western Europe (Tables 1 and 2). The datadescribed in this report were based on duration of exposure toa) amisulpride (N=55), haloperidol (N=230), olanzapine(N=92), risperidone (N=112), ziprasidone (N=1066) andplacebo (N=187) in short-term 4- to 12-week trials(Table 1); and b) haloperidol (N=242), olanzapine(N=70), risperidone (N=154), ziprasidone (N=1080) andplacebo (N=103) in long-term follow-up trials of 6 months,or 1 year (Table 2). The short-term trials included 1742patients treated for up to 12 weeks (no additional timewindow was used); the long-term trials included 1649patients, 450 patients treated for 6 months (treatment
Table 2Long-term, double-blinded, placebo-controlled or active-comparator studies.
Study Year Drug dose Number ofsubjects
S570 [Simpsonet al., 2005]
2001 Ziprasidone 40–80 mggiven BID
71
Olanzapine 5–15 mgonce daily
62
S303 [Aratoet al., 2002]
1997 Ziprasidone 20 mg,40 mg, 80 mg given BID
76, 72, 71
Placebo 75S307 [data on file] 1999 Ziprasidone 40–60 g
once daily63
Ziprasidone 80–100 mgonce daily
63
Placebo 64S108E [submitted] 2002 Ziprasidone 40–160 mg
given BID139
Haloperidol 5–20 mg daily 47S301E [dataon file]
1999 Ziprasidone 20 mg, 60 mg,100 mg given BID
26, 22, 27
Haloperidol 5 mg, 10 mggiven BID
25 17
S302E [Addingtonet al., 2009]
1999 Ziprasidone 40–80 mggiven BID
62
Risperidone 3–5 mggiven BID
77
S304 1998 Ziprasidone 40–80 mggiven BID
148
Haloperidol 5–15 mg/day 153S108 2000 Ziprasidone 80–160 mg/
day given BID227
Ziprasidone 80–120 mg/day given QD
221
Haloperidol 151S 104E [dataon file]
1996 Ziprasidone 5–40given BID
6
Placebo 1S106E [dataon file]
1997 Ziprasidone 21Placebo 8
S117 (N=398) open-label study.
exposure window: 150 to 210 days) and 470 patients treatedfor 1 year (treatment exposure window: 330 to 390 days).One hundred and sixteen subjects were excluded from theanalyses because they had both treatment exposure of lessthan 14 days and an absolute percent weight change of 7% orless. The final evaluable population was therefore based on3391 subjects. Studies S111, S104E and S106E were excludedfrom the analysis due to a small N (b=3 on any treatmentarm). Studies included in this analysis were conducted inaccordance with the principles of the Declaration of Helsinki,and in compliance with Good Clinical Practice. Patients ortheir legal representatives signed and dated the informedconsent form approved by their local institutional reviewboards before any protocol-required procedures wereperformed.
2.2. Methods
Integrated database analyses were performed to estimatethe weighted average of mean weight change and percentageof subjects experiencing weight gain or weight loss acrossstudies for each agent, using fixed- and random-effects
Maximumexposure duration
Mean baselineweight (lb)
Mean weightchange (lb)
% N=7%weight gain
26 weeks 184.8 (44) −2.42 (16.5) 13%
184.8 (41.8) 11.44 (20.9) 47%
52 weeks 160.6 (28.6),156.2 (30.8),158.4 (35.2)
−5.5 (12.98),−7.04 (10.12),−6.16 (12.54)
5%, 3%, 6%
160.6 (28.6) −8.14 (12.1) 3%52 weeks 158.4 (33) −6.6 (14.74) 2%
160.6 (24.2) −5.94 (14.74) 6%
158.4(33) −7.7 (15.4) 5%156 weeks 180.4 (41.8) 0.132 (22.66) 26%
184.8 (37.4) −0.44 (16.72) 23%40 weeks 160.6 (30.8),
156.2 (26.4),165 (35.2)
−1.76 (22.66),−3.52 (12.32),−2.86 (14.52)
20% 5%, 18%
160.6 (33),169.4 (48.4)
3.74 (11.88),−6.82 (20.9)
28%, 24%
44 weeks 173.8 (37.4) −1.76 (20.02) 20%
165 (39.6) 7.04 (13.86) 33%
28 weeks 167.2 (30.8) 0.66 (10.12) 8%
167.2 (33) 167.2 (30.8) 8%40 weeks 184.8 (44) −4.18 (19.8) 6%
184.8 (44) −1.76 (15.4) 8%
182.6 (41.8) −0.66 (9.68) 10%104 weeks 187 (41.8) 0.66 (25.96) 33%
239.8 −1.1 0%76 weeks 171.6 (30.8) 2.86 (15.62) 11%
187 (55) 3.52 (8.14) 17%

106 B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
models. The effects of the antipsychotic drugs were analyzedseparately for each agent, using 95% confidence intervals forpre-treatment-to-post-treatment mean weight change in allstudies (Allison et al., 1999). Tests for heterogeneity in fixed-and mixed-effects models were performed using the Chi-square test. Sensitivity analyses were conducted usingdifferent treatment exposure cohorts. Durations of treatmentin long-term trials were controlled by well-defined timewindows (6 months: 150 to 210 days; 1 year: 330 to390 days). Body weight changes were analyzed in terms ofmean changes from baseline (Day 0 or subject's lastpretreatment weight measurement), as well as body weightchanges N7% of baseline weight. A 7% weight gain isequivalent to a gain of 10.5 lb in a 150 lb individual. It is awidely accepted standard for clinically relevant weight gain,and is an analysis of weight change that is requested byregulatory agencies such as the FDA (Geodon USPI, 2008). Theziprasidone dose effect on weight change was also evaluatedby analysis of covariance, using the fixed-dose, short-term,placebo-controlled studies of ziprasidone. Baseline wasdefined as the weight measurement obtained at first dose ofstudy medication prior to randomization. Subjects evaluatedfor weight effects included all subjects who had baseline (Day0 or subject's last pretreatment weight measurement) andfollow-up weight data. If a patient had two weight measure-ments within the defined interval, the higher value wasutilized. It should be noted that for many studies included inthe analyses summarized here, weight was only measured atbaseline and at the final visit. All statistical tests were 2-sidedat alpha=5%.
2.3. Results
Studies were classified as a) short-term (4–12 week),double-blind, comparative studies (N=1742), and b) long-term, double-blind, or open-label comparative studies(N=1649). The specific attributes associated with these
Fig. 1. Distribution of weight change in double-blind,
short- and long-term cohorts are summarized in Tables 1 and2, respectively. The overall treatment exposure in thedatabase was 1179 person-years.
2.3.1. Short-term patient cohort (4–12 week studies)The distribution of weight change in this patient cohort
through short-term(4–12week) follow-up is shown inFig.1 andTable 3. Based on comparison of the 95% confidence intervals(CI) for weighted mean of weight change and the proportion ofsubjectswith N7%weight gain, haloperidol (+0.5 lb,12%weightgainN7%)andziprasidone (+1.8 lb, 9%) showeda similarweightgain distribution compared to placebo (−0.5 lb, 5%) in short-term trials. In contrast, amisulpride (+2.9 lb, 17%), olanzapine(11.1 lb, 48%), and risperidone (+4.3 lb, 17%) had significantlydifferent meanweight change patterns and significantly greaterincidences of weight gain, when compared with placebo. In asensitivity analysis using 5% as a threshold, the incidences of 5%(or greater) weight gain observed were, respectively, 8.6% forplacebo, 14% for haloperidol, 15% for ziprasidone, 18% foramisulpride, 30% for risperidone, and 55% for olanzapine.
These short-term weight change findings were confirmedbased on the full analysis dataset of two double-blind, head-to-head, randomized controlled studies (S548 and S302 inTable 1). At study endpoints, the increases inweight and bodymass index in subjects who received risperidone (t=2.98,p=0.003) or olanzapine (t=4.32, pb0.001) were clinicallyand statistically significantly greater than in those whoreceived ziprasidone at study endpoints.
There were also no consistent gender (p=0.44) or dose-related (p=0.89) effects on weight change in the 4 short-term, 4–6 weeks, fixed-dose studies (S104, S106, S114, S115)across the four ziprasidone dose groups (40 mg/day, 80 mg/day, 120 mg/day and 160 mg/day).
2.3.2. Long-term studiesThe long-term weight changes among antipsychotics
continued the trends observed in the short-term studies
comparative, short-term (4–12 weeks) studies.

Table 3Short-term, placebo-controlled or active-comparator 4–12 weeks studies.
Drugs Weight change(lb)
Test forheterogeneity
Weight change(lb)
Wt lossN7%
Wt gainN7%
Test for heterogeneitywt gain
Fixed effects model Fixed effectsmodel
Random effectsmodel
Randomeffectsmodel
Randomeffects model
Fixed effects model
Mean 95%CI Chi-sq (p) Mean 95%CI % 95%CI % 95%CI Chi-sq (p)
Amisulpride N=55 2.9 (0.8, 5.0) ⁎ N/A 2.9 (0.8, 5.0) ⁎ 6 (0, 13) 17 (7, 27) N/AS305
Haloperidol N=229 a 0.06 (−1.0, 1.1) 4.6 (p=0.10) 0.5 (−1.4, 2.5) 5 (2, 7) 12 (5, 19) 3.5 (p=0.32)S101 N=8 5.6 (0.1, 11.1) 5.6 (0.1, 11.1) 6 (−11, 23) 31 (14, 48)S115 N=67 0.4 (−1.5, 2.2) 0.4 (−1.5, 2.2) 2 (−1, 6) 7 (3, 10)S301 N=154 −0.4 (−1.8, 0.9) −0.4 (−1.8, 0.9) 7 (3, 12) 11 (7, 15)
Olanzapine N=92 11.1 (9.0, 13.1) ⁎ N/A 11.1 (9.0, 13.1) ⁎⁎⁎ 2 (−1, 4) 48 (38, 59) ⁎ N/AS548
Placebo N=187 −0.5 (−1.4, 0.4) 2.0 (p=0.57) −0.5 (−1.4, 0.4) 3 (1, 6) 5 (2, 8) 2.2 (p=0.53)S104 N=31 0.6 (−1.3, 2.4) 0.6 (−1.3, 2.4) 5 (−3, 12) 8 (−2, 18)S106 N=34 −0.7 (−2.4, 1.0) −0.7 (−2.4, 1.0) 1 (−3, 6) 4 (−2, 11)S114 N=68 −1.3 (−3.1, 0.6) −1.3 (−3.1, 0.6) 7 (1, 13) 4 (−1, 8)S115 N=54 −0.5 (−2.7, 1.7) −0.5 (−2.7, 1.7) 3 (−2, 7) 6 (0, 13)
Risperidone N=112 4.3 (2.6, 6.1) ⁎ N/A 4.3 (2.6, 6.1) ⁎⁎ 2 (−1, 5) 17 (10, 24)⁎ N/AS302
Ziprasidone N=1063 a 1.4 (0.9, 1.9) ⁎ 55.5 (pb0.001) 1.8 (0.4, 3.2) 3 (1, 5) 9 (6, 11) 12.9 (p=0.12)S101 N=32 4.5 (2.2, 6.8) 4.5 (2.2, 6.8) 2 (−3, 6) 12 (1, 24)S104 N=112 1.1 (−0.2, 2.5) 1.1 (−0.2, 2.5) 0 (−1, 2) 5 (1, 10)S106 N=70 3.4 (2.0, 4.8) 3.4 (2.0, 4.8) 1 (−1, 3) 7 (1, 13)S114 N=174 2.6 (1.1, 4.1) 2.6 (1.1, 4.1) 4 (1, 7) 15 (10, 20)S115 N=193 1.9 (0.8, 3.1) 1.9 (0.8, 3.1) 3 (1, 6) 10 (6, 15)S301 N=250 −1.2 (−2.2, −0.2) −1.2 (−2.2, −0.2) 9 (5, 13) 6 (3, 9)S302 N=103 −0.05 (−2.4, 2.3) −0.05 (−2.4, 2.3) 7 (2, 12) 10 (4, 15)S305 N=51 −0.2 (−2.4, 2.1) −0.2 (−2.4, 2.1) 7 (0, 14) 6 (−1, 12)S548 N=78 4.5 (2.4, 6.6) 4.5 (2.4, 6.6) 1 (−1, 2) 10 (4, 17)
Weighted average of proportion for weight gain or weight loss was based on (count+0.5)/N within in each study to avoid excluding studies with zero count.a Study 111 with Nb3 was excluded.
⁎ pb0.05.⁎⁎ pb0.01.⁎⁎⁎ pb0.001.
107B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
(Table 4, Fig. 2). The 95% CI of weight change for olanzapine(mean +0.8 lb/month, median +1.5 lb/month) andrisperidone (mean or median +0.6 lb/month) did notoverlap with the 95% CI derived for both placebo-treatedsubjects (weighted mean +0.1 lb/month, median −0.3 lb/month) and ziprasidone-treated subjects (mean −0.3 lb/month, median −0.2 lb/month) at the 1-year follow-up,indicating significantly greater weight change per monthassociated with risperidone and olanzapine treatments(pb0.05). Based on the 95% CI, there was also a significantlylarger proportion of subjects in the olanzapine or risper-idone groups than in placebo- and ziprasidone-treatedgroups who had N7% weight gain from baseline (pre-treatment assessment) in the 1-year cohort (pb0.05). Incontrast, haloperidol- and ziprasidone-treated subjects hadweight profiles not significantly different from placebo-treated subjects (pN0.05, 95% CI overlapping with placebo).In a sensitivity analysis using 5% as a threshold, theincidences of 5% (or greater) weight gain in the 6 monthand 1-year cohorts were, respectively, 16% and 13% forplacebo, 15% and 39% for haloperidol, 16% and 20% forziprasidone, 27% and 45% for risperidone, and 58% and 60%for olanzapine.
Interestingly, the proportion of subjects with weight lossN7% was higher than those with weight gain in theziprasidone- and placebo-treated groups, a trend notobserved in the other treatment groups. These findings
suggest overall weight neutrality for ziprasidone. The patternof weight change at 1 year for the antipsychotic drugsevaluated (Fig. 2) was consistent with those observed in allsubjects, and in the 6-month follow-up cohort (Table 4).
3. Discussion
Our comprehensive analysis of a large schizophreniaclinical trial database examining body weight changes duringshort- and long-term treatments of patients randomized toplacebo or antipsychotic agents confirms that there aresubstantial differences among antipsychotics in their effectson body weight. In short-term, 4- to 12-week studies,ziprasidone-treated subjects experienced the lowest clinicallysignificant weight gain (i.e., N7% increase compared tobaseline) in comparison to risperidone and olanzapine.These results were confirmed for weight gain based on thefull analysis dataset of two double-blind, randomized, head-to-head, controlled studies: S302 (Addington et. al., 2004)and S548 (Simpson et. al., 2004) (Table 1). Mean increases inweight and body mass index in subjects who receivedrisperidone or olanzapine were also significantly greaterthan in those who received ziprasidone at primary endpointin these studies.
Published data regarding the weight effect profile ofaripiprazole suggest comparability to ziprasidone in 4-weekand 6-week trials in adults with schizophrenia (Abilify

Table 4Long-term, placebo-controlled or active-comparator studies.
Drug name(number of studies)
Weight change fromfirst dose of studymedication permonth (lb)
Test forheterogeneity
Weight changeper month (lb)
Wt lossN7% Wt gainN7% Test forheterogeneitywt gain
Fixed Effects Model Fixed EffectsModel
Random effects model Random effectsmodel
Random effectsmodel
Fixed effectsmodel
Man a 95%CI Chi-sq (p) Mean/med 95%CI mean % 95%CI % 95%CI p-value
1-year cohort (treatment days 330 to 390, N=470)Haloperidol (1) N=16b +0.41 (−0.52, 1.33) N/A +0.41/+0.4 (−0.52, 1.33) 16% (−2%, 33%) 41% (17%, 65%) N/AOlanzapine (1) N=15 +0.80 (0.53, 1.06) c N/A +0.80/+1.50 (0.53, 1.06) c 10% (−5%, 25%) 57% (32%, 82%) c N/APlacebo (2) N=30 +0.09 (−0.01, 0.2) 0.63 +0.09/−0.32 (−0.01, 0.20) 41% (−10%, 92%) 13% (0%, 25%) 0.70Risperidone (2) N=85 +0.62 (0.34, 0.91) c 0.74 +0.60/+0.55 (0.34, 0.91) c 8% (2%, 14%) 39% (28%, 49%) c 0.94Ziprasidone (7) N=321 b −0.36 (−0.52,−0.2) d 0.004 −0.27/−0.18 (−0.61, 0.06) d 27% (21%, 34%) 17% (10%, 24%) 0.01
6-month cohort (treatment days 120 to 150 days, N=450)Haloperidol (3) N=71 +0.16 (−0.18, 0.5) c 0.57 +0.16/0.0 (−0.18, 0.5) 13% (−4%, 30%) 11% (4%, 18%) 0.60Olanzapine (1) N=45 +2.31 (1.34, 3.27) c N/A +2.31/1.65 (1.34, 3.27) c 8% (0%, 16%) 50% (35%, 65%) c N/APlacebo (2) N=31 −1.31 (−2.1, −0.52) 0.74 −1.31/−1.82 (−2.1, −0.52) 45% (28%, 63%) 15% (3%, 28%) 0.56Risperidone (2) N=22 +0.47 (−0.17, 1.11) c 0.02 +0.5/+0.62 (−0.94, 1.93) 8% (−3%, 19%) 16% (11%, 21%) 0.01Ziprasidone (9) N=279 b −0.38 (−0.6, −0.15) 0.003 −0.25/−0.18 (−0.74, 0.25) 19% (10%, 27%) 11% (8%, 15%) 0.46
All subjects in long-term trials (N=1649)Haloperidol (4) N=242 0.05 (−0.34, 0.44) 0.23 +0.05/0.00 (−0.47, 0.57) 8% (3%, 13%) 8% (3%, 13%) 0.06Olanzapine (1) N=70 3.60 (2.37, 4.83) N/A +3.60/+2.00 (2.37, 4.83) 6% (1%, 12%) 48% (36%, 60%) c N/APlacebo (2) N=103 −2.06 (−2.86, −1.26) 0.60 −2.06/−0.15 (−2.86, −1.26) 32% (23%, 41%) 6% (1%, 10%) 0.66Risperidone (2) N=154 0.97 (0.49, 1.45) 0.05 +0.9/+0.74 (−0.08, 1.88) 5% (1%, 10%) 28% (21%, 35%) c 0.95Ziprasidone (11) N=1080 −0.14 (−0.26, −0.02) 0.03 −0.37/−0.17 (−0.83,−0.09) 16% (11%, 21%) 12% (8%, 16%) b0.001
Weighted average of proportion for weight gain or weight loss was based on (count+0.5)/N within in each study to avoid excluding studies with zero count.a Medianweight changes of−0.32, +0.49,−0.18, +1.50 and+0.55 lb/month were observed for placebo, haloperidol, ziprasidone, olanzapine and risperidone
in a 1-year treatment duration cohort (time window: 330 to 390 days), respectively.b S104E (N=2, ziprasidone) was excluded. S106E (N=1, ziprasidone) was excluded. S108E (N=2, haloperidol) was excluded.c pb0.05 for significantly higher than placebo based on 95% CI (vs. placebo) in the 6-month and 1-year cohorts.d pb0.05 for significantly lower than placebo based on 95% CI (vs. placebo) in the 6-month and 1-year cohorts.
108 B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
USPI, 2008; Zimbroff et al., 2007). A 4-week, double-blindstudy comparing ziprasidone and aripiprazole (Zimbroffet al., 2007) in patients with schizophrenia has beenconducted; however, due to its recent completion, thisstudy was not included in the current integrated analysis.Median weight change in this 4-week study was +0.99 lbfor both groups, which is slightly lower than the overallshort-term effect of ziprasidone reported here (+1.8 lb inup to 12-week trials) and aripiprazole reported elsewhere(+1.54 lb in the 4-week to 6-week phase 2/3 trials)(Abilify USPI, 2008).
Similarly, in our analyses of long-term, randomized,controlled trials, olanzapine and risperidone were alsoassociated with a significantly greater likelihood thanplacebo to cause weight gain, a trend not observed withziprasidone and haloperidol. The magnitudes of weightchange (per month) controlled for treatment duration for6-month (150 to 210 days) and 1-year (330 to 390 days)cohorts were consistent with results observed in the CATIEschizophrenia study (Lieberman et al., 2005), whichreported mean weight gains or losses of +2.0 lb/month forolanzapine, +0.4 lb/month for risperidone, and −0.3 lb/month for ziprasidone.
Reliable information on differential weight effects amongantipsychotics is of critical importance to clinical and healthpolicy decision-making. Second-generation, atypical antipsy-chotics have emerged as first-line treatment for manypsychotic conditions due to their reduced risk of extrapyr-
amidal side effects (EPS) and related movement disorders(Harrington et al., 2000). However, some atypical antipsy-chotics have been associated with excessive weight gain,which to a large extent has replaced EPS as the main adverseevent of concern for atypical agents. In this paper, we haveattempted to address some existing methodological limita-tions in the analysis and interpretation of antipsychotic-induced weight change by using: 1) long-term, randomized,controlled trial data involving both atypical and conventionalagents, 2) a placebo control, 3) well-defined treatmentexposure timewindows in stratified analyses, 4) meanweightchange per month and a 7% threshold for weight gain or lossto characterize weight change.
In the analyses, we pooled 10 short-term (N=1742) and11 long-term follow-up (N6 months), randomized controlledtrials (N=1649) to create a large integrated analysis dataset.For many long-term and short-term studies included in theanalyses summarized here, weight was only measured atbaseline and at final visit. Although missing data due to earlydropouts in these studies were not imputed by the usualmixed effects model (as cohorts differed based on definedtime windows), the large integrated analysis databaseprovides adequate double-blind data (N86%) to make validcomparisons across antipsychotic drugs within well definedtreatment exposure cohorts. Specifically, we use well-definedtime-windows to define treatment duration cohorts: subjectsreceiving 6-month (within 150 to 210 treatment days) or 1-year (within 330 to 350 treatment days) exposure to study

Fig. 2. Distribution of weight change at 1 year: long-term, double-blind, comparative studies.
109B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
medications. The use of this post-stratification approach tocontrol for confounding bias due to large variations inexposure durations has an advantage of not requiringstringent model assumptions on the trajectory of the meanweight gain over time. In addition, it is also possible that mostof the dropouts occurring in the studies used in our analyseswere not related to weight change. Although the studiesexamined here were based on all rigorously conducted trialsand provided a randomized, controlled database, expandedanalyses that included non-Pfizer sponsored studies were notconducted. Therefore, generalizations from these studies maybe limited. Results from both fixed and random effects modelsare presented with tests for heterogeneity of results acrossstudies. These results provide some assurance that it wasreasonable to combine effect sizes from multiple studies.The robustness of our results are confirmed by showingconsistency across short-term (4 to 12 weeks), 6-monthand 1-year treatment duration cohorts and with publishedliterature. Interestingly, the 6-month and 1-year treatmentduration cohorts produced similar magnitudes of weightchange (lb/month of treatment) in the olanzapine, risper-idone, and ziprasidone treated subjects, when compared tothe exposure-adjusted weight changes reported in theCATIE study (Lieberman, 2005). We note that ziprasidonewas per protocol taken with food in all studies reportedhere; meal size of at least 500 cal has been shown toprovide optimal bioavailability of this agent (Lombardo etal., 2007).
Our findings presented here confirm that in both short-and long-term studies, ziprasidone is associated with anoverall weight neutral profile, whereas olanzapine andrisperidone produced significant weight gain. There wereno observable dose- or duration-related trends. Thesefindings confirm significant differences in weight effectsamong antipsychotic agents, consistent with findings fromCATIE and several earlier studies. Further research iswarranted to elucidate the effect of these differences onhealth outcomes.
Role of funding sourceThis study was sponsored by Pfizer Inc. The sponsor was involved in all
stages from conception, analysis to review of the manuscript. Data analysiswas supported by Pfizer Inc., and interpreted collectively by all of the authors.
ContributorsAll authors contributed to the analysis of data and writing of this
manuscript. Analysis and interpretation of data: authors Parsons, Allison,Loebel, Giller, Williams, Romano and Siu. Drafting of the manuscript: authorsParsons, Allison, Loebel, Giller, and Siu. Statistical analysis: Allison and Siu.Critical revision of the manuscript for important intellectual content andapproval of the final version for publication: authors Parsons, Allison, Loebel,Giller, Williams, Romano and Siu.
Conflict of interestDavid Allison has received grants, honoraria, consulting fees, and
contributions from multiple food, pharmaceutical, and for profit and not-for-profit entities concerned with obesity and/or antipsychotic drugs. BruceParsons, Antony Loebel, Kathryn Williams, Earl Giller, and Steven Romanowere employees of Pfizer, Inc. during development and writing of themanuscript. Cynthia Siu was a paid consultant to Pfizer, Inc., in connectionwith the development and analysis of this manuscript. She reported alsobeing a consultant to Dainippon Sumitomo Pharma America, MemoryPharmaceuticals, Prescient Medical, and Wyeth.
AcknowledgementsThis study was supported by Pfizer Inc.This studywas previously presented as a poster at the American Psychiatric
Association 159th Annual Meeting, Toronto, Canada, 20–25 May, 2006.
References
Abilify UPSI [US Package Insert], 2008. Princeton, NJ: Bristol-Myers SquibbCompany.
Addington, D.E., Pantelis, C., Dineen, M., Benattia, I., Romano, S.J., 2004.Efficacy and tolerability of ziprasidone versus risperidone in patientswith acute exacerbation of schizophrenia or schizoaffective disorder: an8-week, double-blind, multicenter trial. J Clin Psychiatry 65, 1624–1633.
Addington, D.E., Labelle, A., Kulkami, J., Johnson, G, Loebel, A., Mandel, F.S.,2009. A comparison of ziprasidone and risperidone in the long-termtreatment of schizophrenia: a 44-week, double-blind, continuationstudy. Can J Psychiatry 54, 46–54.
Allison, D.B., Mentore, J.L., Heo, M., Chandler, L.P., Capelleri, J.C., Infante, M.C.,Weiden, P.J., 1999. Antipsychotic induced weight gain: a comprehensiveresearch synthesis. Am J Psychiatry 156, 1686–1696.

110 B. Parsons et al. / Schizophrenia Research 110 (2009) 103–110
American Diabetes Association, American Psychiatric Association, AmericanAssociation of Endocrinologists, North American Association for theStudy of Obesity, 2004. Consensus development conference on anti-psychotic drugs and obesity and diabetes. Diabetes Care 27, 596–601.
Arato, M., O'Connor, R., Meltzer, H., 2002. The Ziprasidone Extended Use inSchizophrenia (ZEUS) study: a double-blind, placebo-controlled, 1-yearclinical trial. Int Clin Psychopharmacol 17, 207–215.
Daniel, D.G., Zimbroff, D.L., Potkin, S.G., et al., 1999. Ziprasidone 80 mg/day and160mg/day in the acute exacerbation of schizophrenia and schizoaffectivedisorder: a 6-weekplacebo-controlled trial. Neuropsychopharmacology20,491–505.
Fontaine, K.R., Heo, M., Harrigan, E.P., Shear, C.L., Lakshminarayanan, M., Casey,D.E., Allison, D.B., 2001. Estimating the consequences of anti-psychoticinduced weight gain on health and mortality rate. Psychiatry Res 101,277–288.
Gentile, S., 2006. Long-term treatment with atypical antipsychotics and therisk of weight gain. Drug Safety 29 (4), 303–319.
Geodon USPI [US Package Insert], 2008. New York, NY; Pfizer Inc.Harrington, C., Gregorian, R., Gemmen, E., et al., 2000. Access and weight gain
may be due to a complex overlapping of utilization of new antidepres-sants and antipsychotic medication. The Office of the Assistant Secretaryfor Planning and Evaluation, the National Institute of Mental Health, USDept. of Health and Human Services. Available at http://aspe.hhs.gov/health/reports/Psychmedaccess/: Accessed 30 Aug 2005.
Keck Jr., P., Buffenstein, A., Ferguson, J., et al., 1998. Ziprasidone 40 and 120mg/day in theacute exacerbationof schizophrenia and schizoaffectivedisorder:a 4-week placebo-controlled trial. Psychopharmacology (Berl) 140,173–184.
Lieberman, J.A., Stroup, T.S., McEvoy, J.P., 2005. Effectiveness of antipsychoticdrugs in patients with chronic schizophrenia. N Engl J Med 353,1209–1223.
Lombardo, I., Alderman, J., Preskorn, S., 2007. Effect of food on absorption ofziprasidone. Presented at the11th International Congress on SchizophreniaResearch, March 28–April 1, 2007, Colorado Spring, CO.
McEvoy, J.P., Lieberman, J.A., Stroup, T.S., et al., 2005. Effectiveness of clozapineversus olanzapine, quetiapine, and risperidone in patients with chronicschizophrenia who did not respond to prior atypical antipsychotictreatment. Am J Psychiatry 163, 600–610.
Myer, J.M., Nasrallah, H.A. (Eds.), 2003. Medical Illness and Schizophrenia.American Psychiatric Press, Washington DC.
Newcomer, J.W., 2005. Second-generation (atypical) antipsychotics and meta-bolic effects: a comprehensive literature review. CNS Drugs 19 (Suppl 1),1–93.
Newcomer, J.W., Hennekens, C.H., 2007. Severe mental illness and risk ofcardiovascular disease. JAMA 298 (15), 1795–1796.
Olie, Z.P., Spina, E., Murray, S., et al., 2006. Ziprasidone and amisulprideeffectively treat negative symptoms of schizophrenia: results of a 12-week,double-blind study. Int Clin Psychopharmacol 21, 143–151.
Simpson, G.M., Glick, I.D., Weiden, P.J., 2004. Comparison of the efficacy andtolerability of ziprasidone and olanzapine in acutely ill patients withschizophrenia or schizoaffective disorder. Am J Psychiatry 161, 1837–1847.
Simpson, G.M., Weiden, P.J., Pigott, T., 2005. Six-month, blinded, multicentercontinuation study of ziprasidone versus olanzapine in schizophrenia.Am J Psychiatry 162, 1535–1538.
Wetterling, T., 2001. Bodyweight gain with atypical antipsychotics. Acomparative review. Drug Safety 24 (1), 59–73.
Wirshing, D.A., 2004. Schizophrenia and obesity: impact pf antipsychoticmedications. J Clin Psychiatry 65 (Suppl. 18), 13–26.
Zimbroff, D., Warrington, L., Loebel, A., et al., 2007. Comparison of ziprasidoneand aripiprazole in acutely ill patients with schizophrenia or schizoaf-fective disorder: a randomized, double-blind, 4-week study. Int ClinPsychopharmacol 22, 363–370.