
Wednesday, September 09, 2015 The Value of eCommerce in the Healthcare Supply Chain.
41
Wednesday, March 16, 2022 The Value of eCommerce in the Healthcare Supply Chain
-
Upload
alan-potter -
Category
Documents
-
view
221 -
download
1
Transcript of Wednesday, September 09, 2015 The Value of eCommerce in the Healthcare Supply Chain.
Wednesday, April 19, 2023
The Value of eCommerce in the Healthcare Supply Chain
2
TRYING TO PREDICT WHERE THE INTERNET AND E-BUSINESS WILL TAKE US … IS LIKE ASKING THE WRIGHT BROTHERS WHAT THEY THOUGHT
ABOUT THE FREQUENT FLIER PROGRAMS!

3
Content of Discussion
•Market Overview
•eBusiness Expectations
•Australian Landscape
•Strategic Issues
•Supply Chain Reform
•GHX Overview

4
Asia-Pacific Market
• The Asia-Pacific market for Medical Equipment and Med/Surg Consumables is estimated at US$24 billion – 21% of the global market
Pharmaceuticals
80% (US $94 bn)
Med Eqpt &Med/Surg Consumables
20% (US$24 bn)
Asia Pacific Human Healthcare Products MarketUS$118 billion*
* Substantial disagreement exists on the market definitionSource : Medistat; Dash Report; PwC Analysis
• Medical Equipment and Med/Surg Consumables account for approximately 20% of the US$118 billion Asia-Pacific Human Healthcare Products Market
Global Medical Device MarketUS$113 billion*
Japan
US $16 bn (14%)
Other Asia-Pacific
US $8 bn (7%)

5
Australian Market
Global Healthcare Exchange Confidential Information
Med/Sur
g
Capital
MDD Market = US$1.1BMDD Market = US$1.1B
Retail
Hospital
Pharma Market = US$3.0BPharma Market = US$3.0B
$0.85B$0.85B
$0.25B$0.25B $0.75B$0.75B
$2.25B$2.25B

6
GHX Equity members alone hold sizable market share
Medical Equipment & Med/Surg Consumables Markets
Total US$24 bn
Source : Medistat; PwC Analysis
11 GHX equity members
c. US$8.4 bn
Other suppliers
(>10,000)
c. US$15.6 bn
65%
35%
GHX equity members have approximately 55% share of the Medical Equipment & Med/Surg Consumables market in Australia/New Zealand
GHX equity members have approximately 55% share of the Medical Equipment & Med/Surg Consumables market in Australia/New Zealand
Market Size US$ mm
Japan 16,100 Australia / New Zealand 1,770 China 1,600 Korea 880 Taiwan 770 Thailand 350 Hong Kong 270 Malaysia 240 Singapore 145 Philippines 130 Indonesia 90 Vietnam 60 India / Pakistan 1,540 Other 55
Total APAC
US$24bn
55%
45%
AUSUS$1.1bn
11 GHX equity members
c. US$0.60 bn
Other suppliers
c. US$0.50 bn

7
Market readiness criteria focus on issues impacting potential speed of launch and rollout
Market size E-readinessEnglish /
single byte
Customerconcentra-
tion
Supply chainoperations
hub
Customer ITconcentra-
tion
Supply chainefficiency
Govt supportfor e-
business
Japan
Australia
China
India
Korea
Taiwan
Thailand
Hong Kong
Malaysia
Singapore
Philippines
Indonesia
% Internet usage
% public sector &
presence of private chains
Exports & production of medical equipment
% using major ERP
systems
Direct distribution & delivery
times
Infrastructure support & investment incentives
Ease of use of US
platform
8
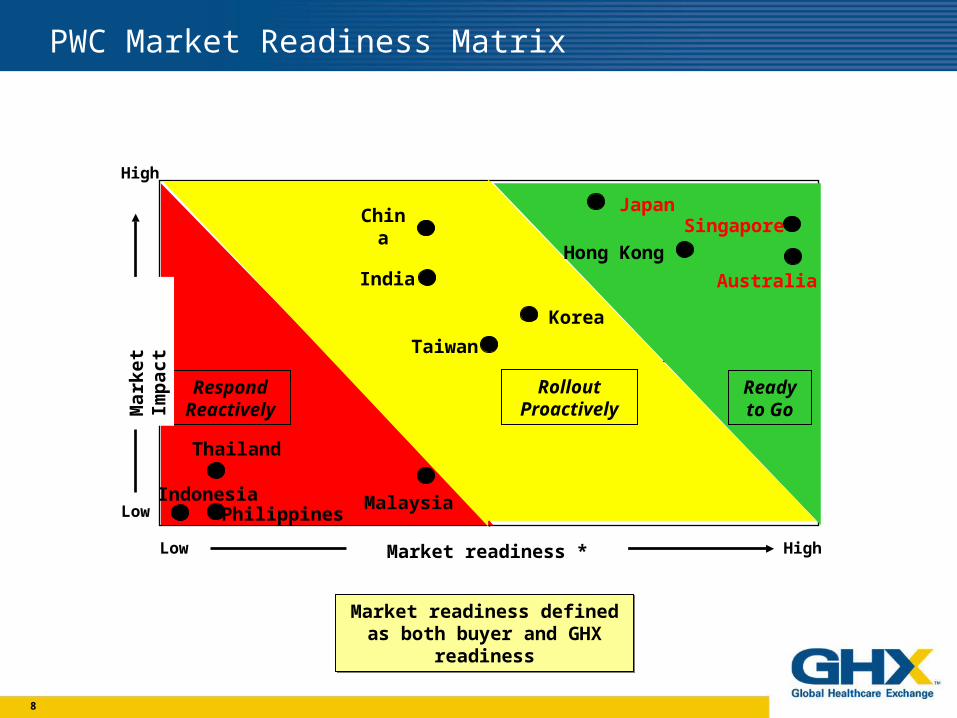
GHX Proposed Strategy & Timing in Asia Pacific is Based on Market Readiness
Low High
High
Low
Ready to Go
Respond Reactively
Market readiness *
Mar
ket
Imp
act
Rollout Proactively
IndonesiaPhilippines
Singapore
Malaysia
Hong Kong
Thailand
Taiwan
Korea
India
China
Australia
Japan
Market readiness defined as both buyer and GHX readinessMarket readiness defined as
both buyer and GHX readiness
PWC Market Readiness Matrix
9
Voice of the Customer -- Australia
• The urgency of demand for eCommerce services is strong in both private and public hospitals with Federal and State governments underwriting major
e-business initiatives
• Hospitals are looking for Reduction in inventory levels and product waste, expiry and obsolescence More efficient means of order entry and processing, with integrated electronic settlement Supply chain transparency, shipment tracking and improved demand forecasting Volume pricing and discounts Accurate and timely management reporting, especially related to patient/procedure costing
• Key issues for hospitals in Australia (particularly major ones) Integration of eCommerce provider to existing computer systems to avoid double-input,
especially with major systems such as Oracle, SAP and IBA Approval of eCommerce provider by State Health Departments, which usually favor a single
preferred platform Correlation of eCommerce provider tracking to government tenders and contracts for both
performance and clinical usage monitoring Ability to pay for eCommerce provider without up front capital investment

10
(A) Some of the supplier cost may be shifted to the hospital if full freight is charged. This is most common in Australia with smaller specialised companies and non-stock products.
(B) Assume: AUD$1.54 billion/year medical-surgical product sales AUD$1.74 billion/year total delivered cost for these same sales
(C) Not including facility costs
Supplier supply chain costs (C)
Hospital supply chain costs(C)
Product manufacturing and sales costs(includes related indirects, taxes and profit margin)
13-14%
12-13%
73-75%
Product sale price (A)
Summary of supply chain (process) costs as a percentage of total delivered cost (B)
© DASH Project Team
11
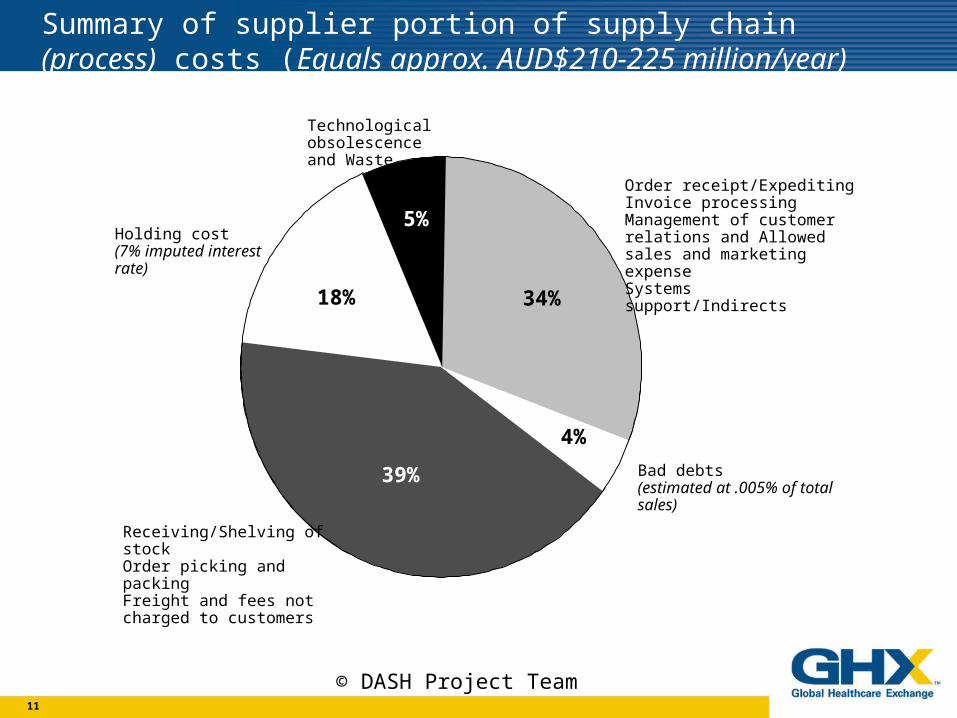
Bad debts (estimated at .005% of total sales)
Order receipt/ExpeditingInvoice processingManagement of customer relations and Allowed sales and marketing expenseSystems support/Indirects
4%
18% 34%
39%
Technological obsolescenceand Waste
Holding cost (7% imputed interest rate)
Receiving/Shelving of stockOrder picking and packingFreight and fees not charged to customers
5%
Summary of supplier portion of supply chain (process) costs (Equals approx. AUD$210-225 million/year)
© DASH Project Team

12
(A) Does not include external contract assistance from separate organisation such as HSA, NSW Peak Purchasing Council, Qld Health, Catholic HealthCare Services, etc.
Waste (Expiry, Theft, Loss and Damage)
Freight and fees
Order placement/ExpeditingInvoice payments and creditsManagement of supplier relations (A)Systems support/indirects
4%
9%
20%
40%
21%
6%
Technological obsolescence(Unused non-stock product due to changes in clinical practice, physician preference, or technological development)
Holding cost of stock and non-stock (7% imputed interest rate)
Receiving/Shelving of stockOrder picking and packingDelivery and imprest replenishment
Summary of hospital portion of supply chain (process) costs (Equals approx. AUD$225-245 million/year)
© DASH Project Team
13
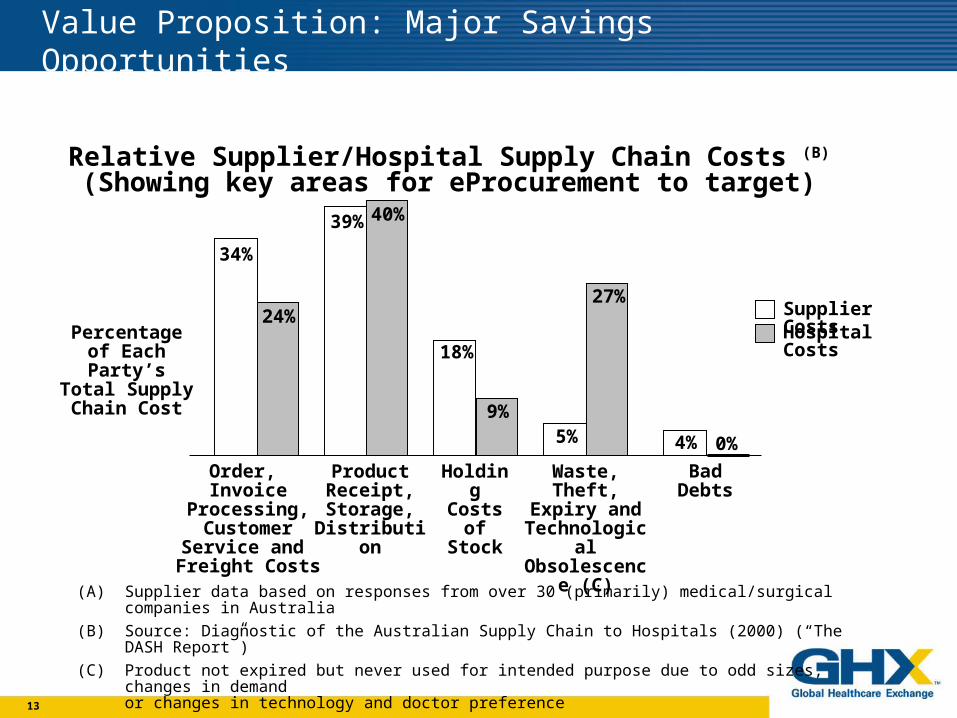
Value Proposition: Major Savings Opportunities
Relative Supplier/Hospital Supply Chain Costs (B)
(Showing key areas for eProcurement to target)
(A) Supplier data based on responses from over 30 (primarily) medical/surgical companies in Australia
(B) Source: Diagnostic of the Australian Supply Chain to Hospitals (2000) (“The DASH Report”)
(C) Product not expired but never used for intended purpose due to odd sizes, changes in demand or changes in technology and doctor preference
34%
24%
39% 40%
18%
9%5%
27%
4% 0%
Percentage of Each Party’s Total
Supply Chain Cost
Order, Invoice Processing, Customer Service
and Freight Costs
Product Receipt,Storage,
Distribution
Holding Costs of
Stock
Waste,Theft,
Expiry andTechnological Obsolescence
(C)
Bad Debts
Supplier CostsHospital Costs

14
Key Findings
• The potential benefits of eCommerce in Healthcare are staggering -$235MM in annual savings
• The savings are derived from: Improved Process efficiency through standardisation & automation Elimination of off-contract buying through better defined, tightly controlled processes Improved standardisation & rationalisation of products Improved productivity associated with efficient, effective product search processes
and improved demand forecasting Reduced product inventories and obsolescence throughout the supply chain
• The initiatives with the highest priority within the trading community include:
Process/Product standardisation Electronic Catalogue eBusiness platform with a National/International Hub
Source: Diagnostic of the Australian Supply Chain to Hospitals (2000) (“The DASH Report”)

15
Key strategic issues
• Australian Health is struggling to define which entity will lead e-commerce (ie, States, Private, Wholesalers, Industry, etc.)
• Australia will probably have different solutions for payment (Medicare/Private Funds), clinical data and procurement
• Australia will probably have different solutions for B2C (downstream) and B2B (upstream) procurement
16
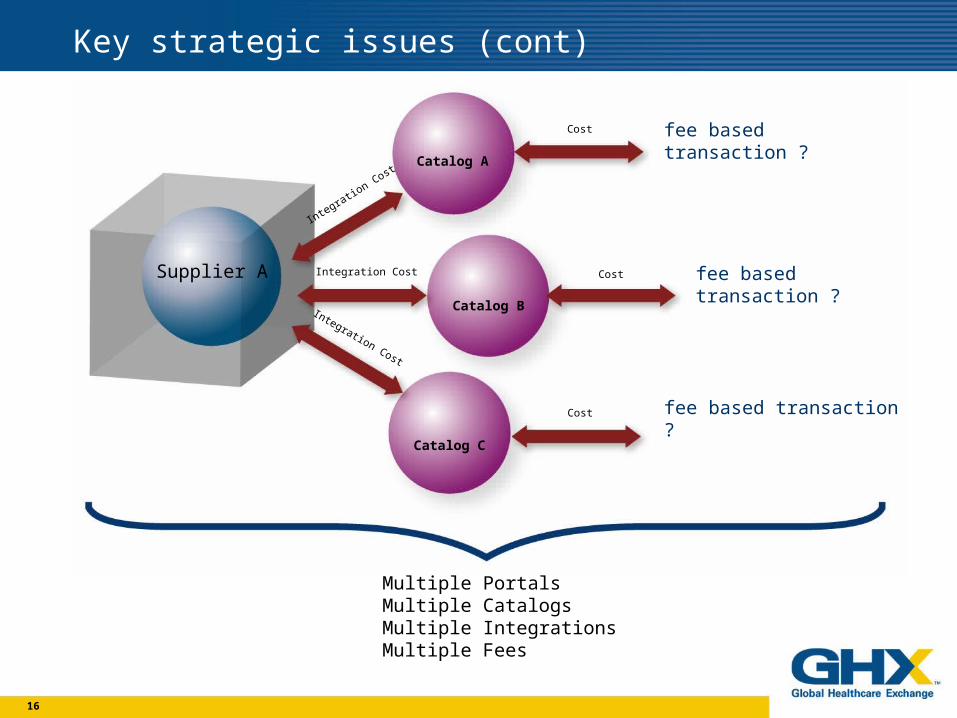
Key strategic issues (cont)
Supplier A
Integration Cost
Integration Cost
Integration Cost
Cost
Cost
Cost
Catalog A
Catalog B
Catalog C
fee based transaction ?
fee based transaction ?
fee based transaction ?
Multiple PortalsMultiple CatalogsMultiple IntegrationsMultiple Fees
17
Key strategic issues (cont)
• B2C has suffered recently because of company negatives – but this is different than concept negatives
• B2C in reality has always been very tough to implement - but very rewarding to those who do.
• Full B2C benefits will require “deep integration” between suppliers/customers in some form

18
Asia Pacific Landscape
• PACIFIC HEALTHCARE EXCHANGE (AUSTRALIA)• Underwent significant capital restructuring
• Change in management
• Layoff about 50% of organization
• Focus on technical consultancy and hardware exchange(core business)
• HEALTHNET ASIA• Operations in Singapore, Thailand and Japan
• Terminate operations in November 2001.
• ASIA RX• Supported by Zuellig Pharma, the largest pharm distributor in
the region
• Targeting small and medium size retail pharmacies with internet based product.
• Possible entry into Australia.
Global Healthcare Exchange Confidential Information

19
The Challenges for Materials Managers
• Purchasing complexities • Wholesaler, no Wholesaler, on contract, off contract, specialty items • Tracking contracts/purchases/rebates • No price validation at the time of order = $$ manual follow-up
• Distribution • Consolidation of hospitals means centralisation of warehousing; distribution to numerous facilities
• Information systems • Disparate standalone or manual systems evolving toward integrated, enterprise-wide IT solutions. • Limited use of data warehouse and historical information • Automated connections to external partners non-existent or under utilised
• Financial responsibility • Responsible for cost/budget management • Total lifecycle costs vs. product costs • Organisationally, link to clinical effectiveness is not well defined
20
What’s Driving Change to the Supply Chain?
• Materials managers are focused on managing costs
• According to the Australian DASH Report, there are significant industry wide savings
•Emerging global drive for common standards in e-healthcare

21
Win - Win B2C Exchange Goals
Customer Goals• Reduce inventory / waste / obsolescence• Improve supply chain efficiency• Standardise on (govt./mgt.) tenders• Conform to (govt./mgt.) reporting needs • Overall – decrease total cost Supplier Goals• Single Industry Catalog• Protect market position• Improve customer support/service• Improve supply chain efficiency• Obtain key market/usage data• Overall – increase market share
22
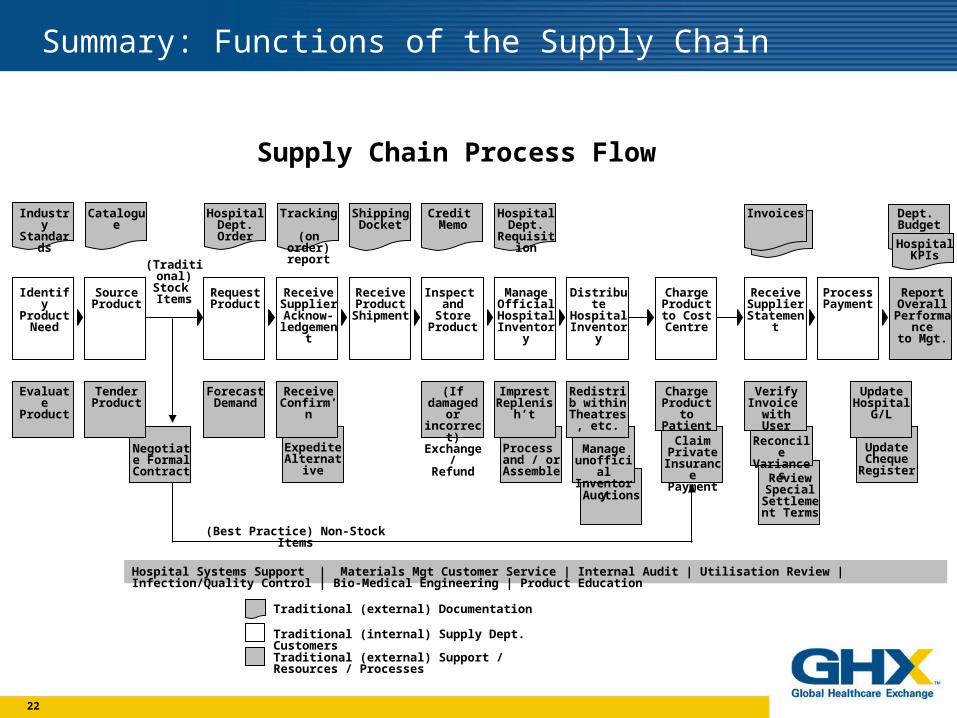
Summary: Functions of the Supply Chain
Industry Standards
Catalogue Hospital Dept. Order
Tracking (on order)
report
Shipping Docket
Credit Memo
Hospital Dept.
Requisition
Invoices Dept. Budget
Identify Product
Need
Source Product
Request Product
Receive Supplier Acknow-
ledgement
Receive Product
Shipment
Inspect and Store Product
Manage Official
Hospital Inventory
Distribute Hospital
Inventory
Charge Product to
Cost Centre
Receive Supplier
Statement
Process Payment
Report Overall
Performanceto Mgt.
Evaluate Product
Tender Product
Forecast Demand
Receive Confirm’n
(If damaged or incorrect)Exchange/
Refund
Imprest Replenish’t
Redistrib within
Theatres, etc.
Charge Product to
Patient
Verify Invoice
with User
Update Hospital
G/L
Hospital KPIs
Negotiate Formal
Contract
Expedite Alternative
Process and / or
Assemble
Manage unofficial Inventory
Auctions
Claim Private
InsurancePayment
Reconcile Variances
Review Special
Settlement Terms
Update Cheque Register
Supply Chain Process Flow
(Traditional)Stock Items
Hospital Systems Support | Materials Mgt Customer Service | Internal Audit | Utilisation Review | Infection/Quality Control | Bio-Medical Engineering | Product Education
Traditional (internal) Supply Dept. Customers
Traditional (external) Documentation
Traditional (external) Support / Resources / Processes
(Best Practice) Non-Stock Items
23
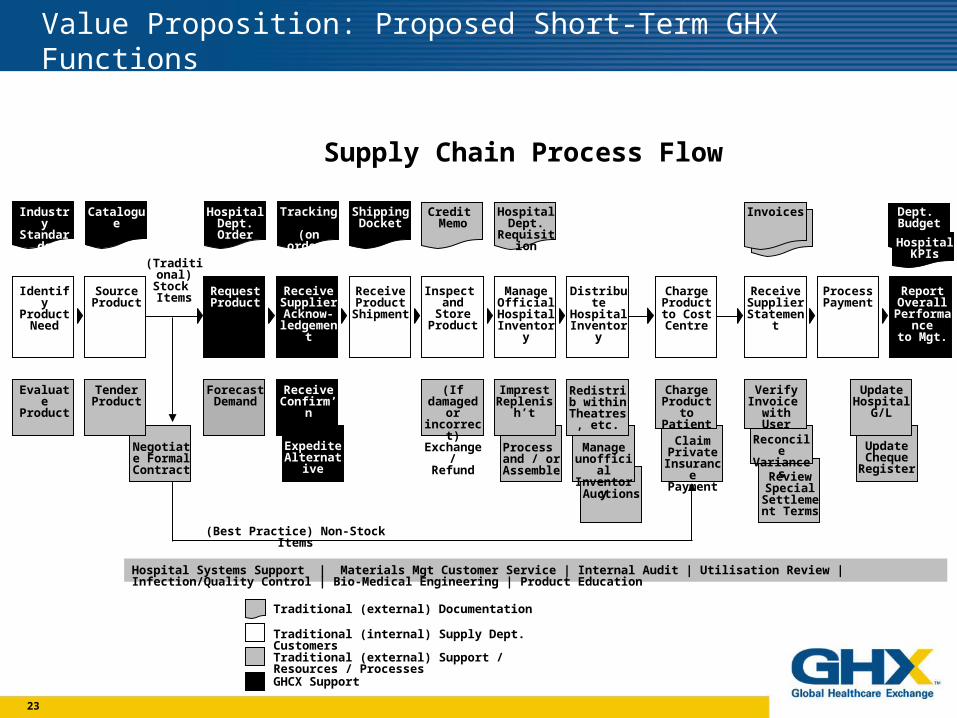
Value Proposition: Proposed Short-Term GHX Functions
Industry Standards
Catalogue Hospital Dept. Order
Credit Memo
Invoices
Identify Product
Need
Source Product
Request Product
Receive Product
Shipment
Manage Official
Hospital Inventory
Distribute Hospital
Inventory
Charge Product to
Cost Centre
Receive Supplier
Statement
Process Payment
Evaluate Product
Tender Product
Forecast Demand
Receive Confirm’n
(If damaged or incorrect)Exchange/
Refund
Imprest Replenish’t
Charge Product to
Patient
Verify Invoice
with User
Update Hospital
G/L
Hospital KPIs
Negotiate Formal
Contract
Expedite Alternative
Manage unofficial Inventory
Auctions
Reconcile Variances
Review Special
Settlement Terms
Update Cheque Register
Supply Chain Process Flow
(Traditional)Stock Items
Hospital Systems Support | Materials Mgt Customer Service | Internal Audit | Utilisation Review | Infection/Quality Control | Bio-Medical Engineering | Product Education
(Best Practice) Non-Stock Items
Tracking (on order)
report
Shipping Docket
Hospital Dept.
Requisition
Dept. Budget
Receive Supplier Acknow-
ledgement
Inspect and Store Product
Report Overall
Performanceto Mgt.
Redistrib within
Theatres, etc.
Process and / or
Assemble
Traditional (internal) Supply Dept. Customers
Traditional (external) Documentation
Traditional (external) Support / Resources / Processes
GHCX Support
Claim Private
InsurancePayment

24
Value Proposition: Proposed Long-Term GHX Functions
Industry Standards
Catalogue Hospital Dept. Order
Credit Memo
Invoices
Identify Product
Need
Source Product
Request Product
Receive Product
Shipment
Manage Official
Hospital Inventory
Distribute Hospital
Inventory
Charge Product to
Cost Centre
Receive Supplier
Statement
Process Payment
Evaluate Product
Forecast Demand
Receive Confirm’n
(If damaged or incorrect)Exchange/
Refund
Imprest Replenish’t
Redistrib within
Theatres, etc.
Verify Invoice
with User
Update Hospital
G/L
Hospital KPIs
Negotiate Formal
Contract
Expedite Alternative
Process and / or
Assemble
Manage unofficial Inventory
Auctions
Reconcile Variances
Review Special
Settlement Terms
Update Cheque Register
Supply Chain Process Flow
(Traditional)Stock Items
Hospital Systems Support | Materials Mgt Customer Service | Internal Audit | Utilisation Review | Infection/Quality Control | Bio-Medical Engineering | Product Education
(Best Practice) Non-Stock Items
Tracking (on order)
report
Shipping Docket
Hospital Dept.
Requisition
Dept. Budget
Receive Supplier Acknow-
ledgement
Inspect and Store Product
Report Overall
Performanceto Mgt.
Tender Product
Charge Product to
Patient
Claim Private
InsurancePayment
Traditional (internal) Supply Dept. Customers
Traditional (external) Documentation
Traditional (external) Support / Resources / Processes
GHCX Support

25
Need to better understand the value proposition in Australia
• To succeed in building an efficient and functional B2C in healthcare:
Suppliers and Buyers must collaborate to drive overall supply chain costs down on both sides.
Understand the 3 key category: MedSurg, Pharm and Non-Medical product groups have unique challenges.
Not just focus on the technology, but on adopting open standards and making the process more transparent and efficient.
The CATALOG is a significant task to normalise but is the cornerstone of any B2C.
Look beyond transactional efficiency -- drive operational efficiencies, eg. Reduce safety stock thus reducing risk of obsolescence and free up working capital
Need to speak the same “language”– need for an independent market value analysis so that we can work from the same page.

26
GHX Founding Members
• Founded by leading healthcare manufacturers in early 2000
• Focused on customer value, not market value
• Independent, open and integrated
• Providers and suppliers collaborating to drive inefficiency out of the healthcare supply chain
27
GHX Operating Principles
• No IPO in business plan
• Break even by end of 2002
• Subscription fees paid by suppliers
• Global presence and leverage
• Open to all
• Not a distributor nor GPO

28
Introducing GHX

29
How Can GHX Help Lead Change?
• Shared motivation • All participants share the pain of inefficient processes in healthcare
• Business model • No transaction fees to suppliers or providers
• Stability • Focused on customer value, not market value
• True value proposition for all participants • Adding measurable value across the supply chain
• Breadth of suppliers & products • Independent and open to all manufacturers and distributors
• Deliver technology excellence • 18 months of focused development in healthcare vertical • End-to-end connectivity • Centralised content management
30
GHX in Asia-Pacific will. . .
• Offer expertise and experience that the individual market needs
• Lead by providing an industry wide catalog standard, which is the key benefit and foundation of the healthcare B2C.
• Take a global approach so that standards and connectivity are not country specific, but regional and global—as our companies are.
• Take a long term approach in Asia – not under the significant pressure of the dotcoms
• Not try to change the way business is done but leverage the long standing relationships of companies that have been key players in the Asian market for many years.

31
GHX Business Model
• Common connection point • Open and independent exchange • Focus on supply chain cost reduction • Improve accuracy of information (pricing / status / content / rebating) • Deliver value to all members of the healthcare supply chain
IDN
Distributors
Office ProductsSuppliers
Other Suppliers
HospitalsGPO’s
Healthcare ProductsSuppliers
Capital EquipmentSuppliers
Pharmacy Suppliers
32
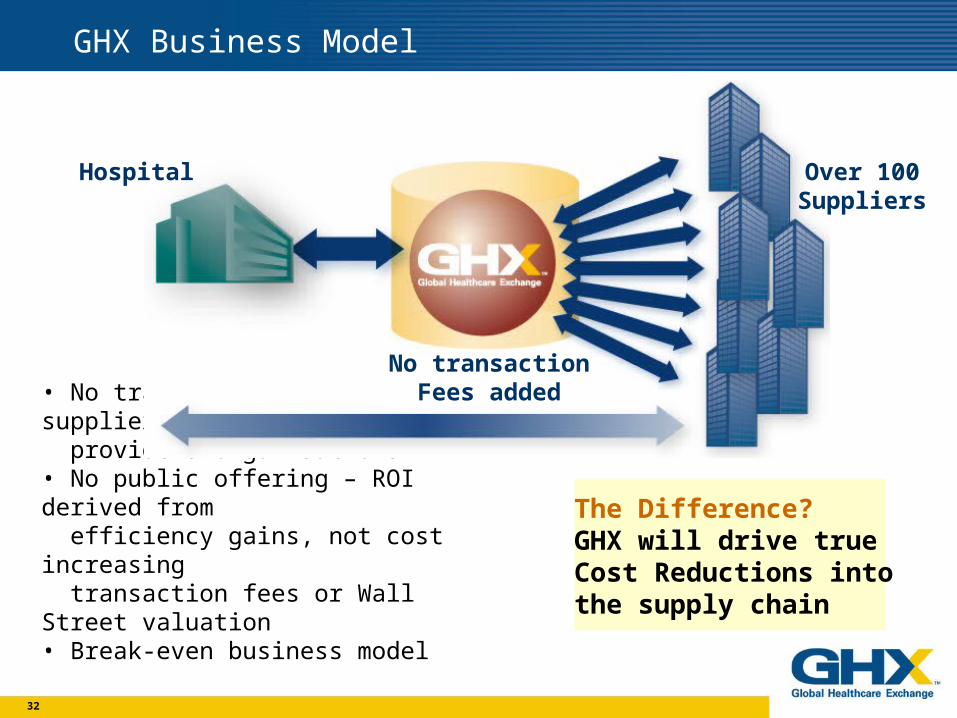
GHX Business Model
• No transaction fees to suppliers or providers organisations• No public offering – ROI derived from efficiency gains, not cost increasing transaction fees or Wall Street valuation• Break-even business model
Hospital
No transactionFees added
Over 100Suppliers
The Difference?GHX will drive true Cost Reductions intothe supply chain

33
GHX Strengthens Existing Relationships
The Difference?GHX supports the existing supply chain, allowing relationships between hospitals and their trusted business partners to prosper.
GHX brings• Support to relationships between hospitals, suppliers, GPOs and distributors• Opportunities for savings to all members of the supply chain
Hospital
Supplier
Supplier
Supplier
GPO
Distributors
34
Industry Common Pain Points & Shared Motivation
The Difference?GHX is uniquely positioned to connect providers, suppliers and distributors in a real time environment for efficiencies and savings throughout the supply chain.
• All participants share the pain of inefficient processes in healthcare
• Suppliers spend millions on marketing and communication to providers, physicians and patients
• Reaching out to community is a priority for GHX member suppliers

35
GHX Core Focus in Building the Exchange
ALLSOURCE* Catalog Services • Catalog data is reviewed, maintained and updated by the manufacturers - "normalized, verified and connected" • Ability for ERP vendors to integrate into GHX catalog solution
Core Exchange Functionality • Transfer of information is reliable and efficient • Supports workability with existing systems
Connectivity Solutions • High quality, deep integration with suppliers and providers • Reproducible process, without GHX resource dependency

36
2002 Standards Approach
• Provide Industry Standard Catalog (UPN, Normalized format, support both EAN & HIBCC)
• Implement ECRI clinical taxonomy into GHX catalog
• Provide catalog synchronization services
• Industry Registry (HIN)
• Publication of GHXml 2.0 Schema for industry review
Standard Bodies + Critical Mass = Adoption
37
GHX Core Competencies
Foundation for Success
• Connectivity•suppliers and providers
• Catalog•normalized content
• Core•transaction•service

38
GHX Core Competencies
Services • Data services • Decision support • Contracting/rebates • ASP • Advanced/rich content
Strong foundation provides a good base to build on
• Connectivity•suppliers and providers
• Catalog•normalized content
• Core•transaction•service
39
GHX Financial Model
• SUPPLIERS PAY: Equity Partner fund capital to build the exchange All members will pay an annual subscription fees based on the
potential sales in the market subject to a worldwide cap. No transaction fees to suppliers and distributors who transact
member products on their behalf. Integration expenses
• HEALTHCARE PROVIDERS PAY: No joining or entry fees No annual subscription fees No transaction fees Integration costs.
40
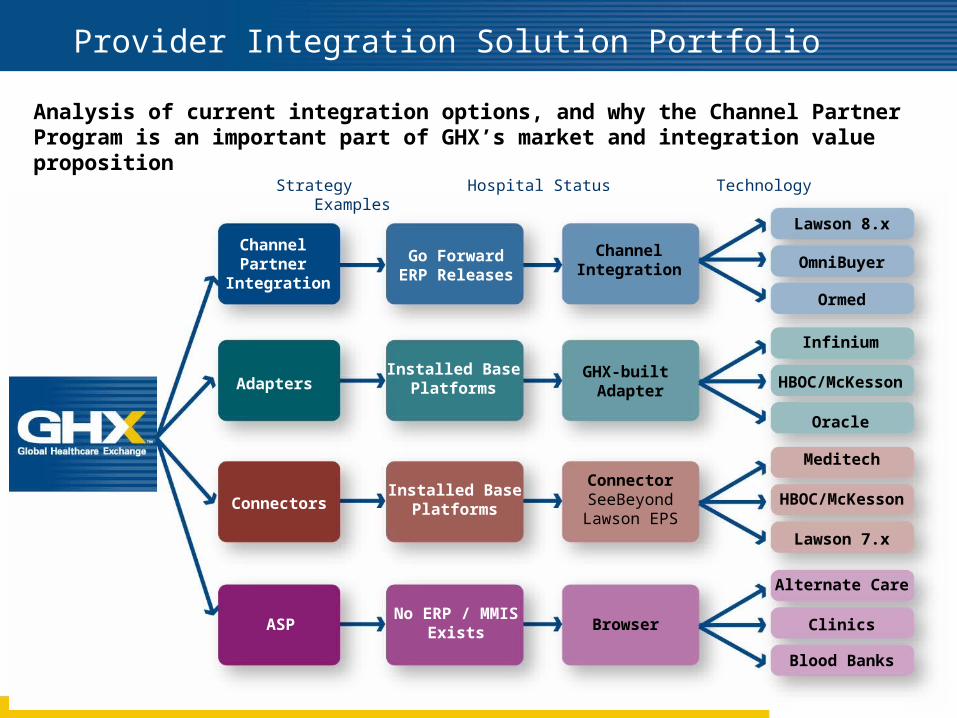
Provider Integration Solution Portfolio
Adapters
ASP
Go ForwardERP Releases
Installed BasePlatforms
No ERP / MMISExists
Channel Partner
Integration
Clinics
HBOC/McKesson
Oracle
Ormed
OmniBuyer
Lawson 8.x
Alternate Care
Blood Banks
Infinium
Strategy Hospital Status Technology Examples
Browser
ConnectorSeeBeyondLawson EPS
ChannelIntegration
Analysis of current integration options, and why the Channel Partner Program is an important part of GHX’s market and integration value proposition
ConnectorsInstalled Base
Platforms
GHX-built Adapter
HBOC/McKesson
Lawson 7.x
Meditech
41
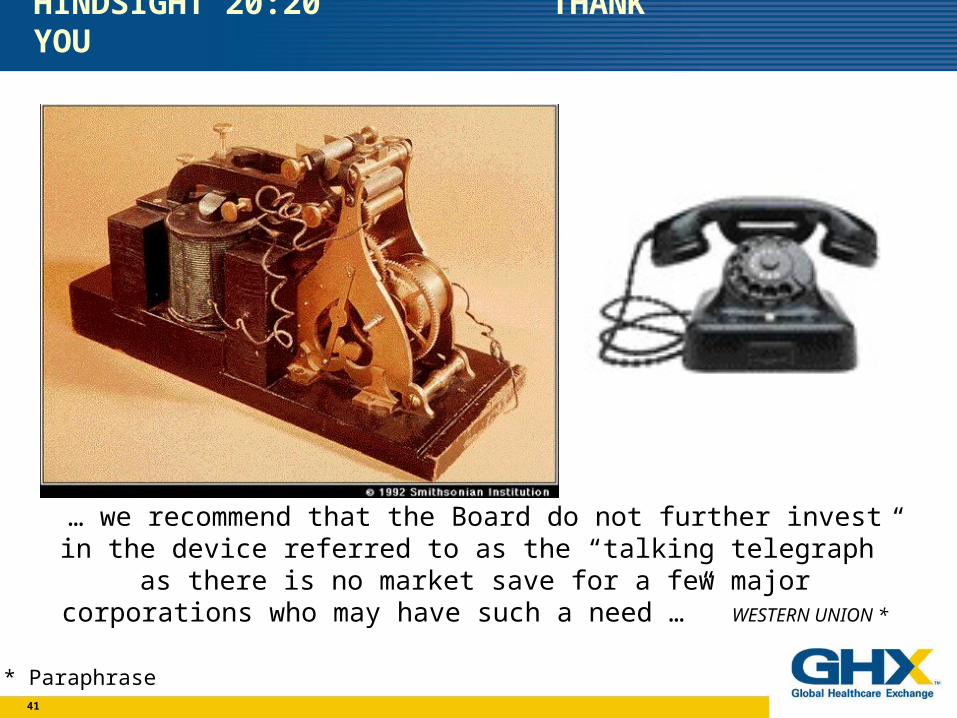
… we recommend that the Board do not further invest in the device referred to as the “talking telegraph” as there is no market save for a
few major corporations who may have such a need …” WESTERN UNION *
* Paraphrase
HINDSIGHT 20:20 THANK YOU



![[Srijan Wednesday Webinars] Truly Scalable eCommerce with Drupal Commerce](https://static.fdocuments.in/doc/165x107/587f71dc1a28ab3f4e8b45df/srijan-wednesday-webinars-truly-scalable-ecommerce-with-drupal-commerce.jpg)














