
Web viewadded the word . mellitus, from the . ... metformin. was first marketed in France in 1979,...
62
Diabetes mellitus From Wikipedia, the free encyclopedia Jump to: navigation , search "Diabetes" redirects here. For the journal, see Diabetes (journal) . See also Diabetes insipidus . Diabetes mellitus Classification and external resources Universal blue circle symbol for diabetes. [1] Diabetes mellitus, often simply referred to as diabetes—is a group of metabolic diseases in which a person has high blood sugar , either because the body does not produce enough insulin , or because cells do not respond to the insulin that is produced. This high blood sugar produces the classical symptoms of polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger). There are three main types of diabetes: Type 1 diabetes : results from the body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.) Type 2 diabetes : results from insulin resistance , a condition in which cells fail to use insulin properly,
Transcript of Web viewadded the word . mellitus, from the . ... metformin. was first marketed in France in 1979,...

Diabetes mellitusFrom Wikipedia, the free encyclopediaJump to: navigation, search "Diabetes" redirects here. For the journal, see Diabetes (journal). See also Diabetes insipidus.
Diabetes mellitusClassification and external resources
Universal blue circle symbol for diabetes.[1]
Diabetes mellitus, often simply referred to as diabetes—is a group of metabolic diseases in which a person has high blood sugar, either because the body does not produce enough insulin, or because cells do not respond to the insulin that is produced. This high blood sugar produces the classical symptoms of polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).
There are three main types of diabetes:
Type 1 diabetes : results from the body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
Type 2 diabetes : results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.)
Gestational diabetes : is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes.

All forms of diabetes have been treatable since insulin became available in 1921, and type 2 diabetes may be controlled with medications. Both type 1 and 2 are chronic conditions that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycemia, diabetic ketoacidosis, or nonketotic hyperosmolar coma. Serious long-term complications include cardiovascular disease, chronic renal failure, retinal damage. Adequate treatment of diabetes is thus important, as well as blood pressure control and lifestyle factors such as smoking cessation and maintaining a healthy body weight.
As of 2000 at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[2] Type 2 diabetes is by far the most common, affecting 90 to 95% of the U.S. diabetes population.[3]
DefinitionThe term diabetes, without qualification, usually refers to diabetes mellitus, which roughly translates to excessive sweet urine (known as "glycosuria"). Several rare conditions are also named diabetes. The most common of these is diabetes insipidus in which large amounts of urine are produced (polyuria), which is not sweet (insipidus meaning "without taste" in Latin).
The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and non-insulin-dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard nomenclature. Various sources have defined "type 3 diabetes" as: gestational diabetes,[4] insulin-resistant type 1 diabetes (or "double diabetes"), type 2 diabetes which has progressed to require injected insulin, and latent autoimmune diabetes of adults (or LADA or "type 1.5 " diabetes)[5]
ClassificationMost cases of diabetes mellitus fall into three broad categories: type 1 , type 2 , and gestational diabetes. A few other types are described.
Type 1 diabetes
Main article: Diabetes mellitus type 1
Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune attack.[6] There is no

known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children.
Type 2 diabetes
Main article: Diabetes mellitus type 2
Type 2 diabetes mellitus is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver.
Gestational diabetes
Main article: Gestational diabetes
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%–5% of all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant production and cause respiratory distress syndrome. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental function. A cesarean section may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia.
A 2008 study completed in the U.S. found that the number of American women entering pregnancy with preexisting diabetes is increasing. In fact the rate of diabetes in expectant mothers has more than doubled in the past 6 years.[7] This is particularly problematic as diabetes raises the risk of complications during pregnancy, as well as increasing the potential that the children of diabetic mothers will also become diabetic in the future.

Other types
Pre-diabetes indicates a condition that occurs when a person's blood glucose levels are higher than normal but not high enough for a diagnosis of type 2 diabetes. Many people destined to develop type 2 diabetes spend many years in a state of pre-diabetes which has been termed "America's largest healthcare epidemic."[8]:10–11
Latent autoimmune diabetes of adults is a condition in which Type 1 diabetes develops in adults. Adults with LADA are frequently initially misdiagnosed as having Type 2 diabetes, based on age rather than etiology.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon. Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell function. Abnormal insulin action may also have been genetically determined in some cases. Any disease that causes extensive damage to the pancreas may lead to diabetes (for example, chronic pancreatitis and cystic fibrosis). Diseases associated with excessive secretion of insulin-antagonistic hormones can cause diabetes (which is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some toxins damage pancreatic beta cells. The ICD-10 (1992) diagnostic entity, malnutrition-related diabetes mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization when the current taxonomy was introduced in 1999.[9]
Following is a comprehensive list of other causes of diabetes:[10]
Genetic defects of β-cell Function o Maturity onset diabetes of the
young (MODY)o Mitochondrial DNA mutations
Genetic defects in insulin processing or insulin action
o Defects in proinsulin conversiono Insulin gene mutationso Insulin receptor mutations
Exocrine Pancreatic Defects o Chronic pancreatitis o Pancreatectomy o Pancreatic neoplasia o Cystic fibrosis o Hemochromatosis o Fibrocalculous pancreatopathy
Endocrinopathies o Growth hormone excess
(acromegaly)o Cushing syndrome o Hyperthyroidism o Pheochromocytoma o Glucagonoma
Infections o Cytomegalovirus infection o Coxsackievirus B
Drugs o Glucocorticoids o Thyroid hormone o β-adrenergic agonists
Signs and symptoms

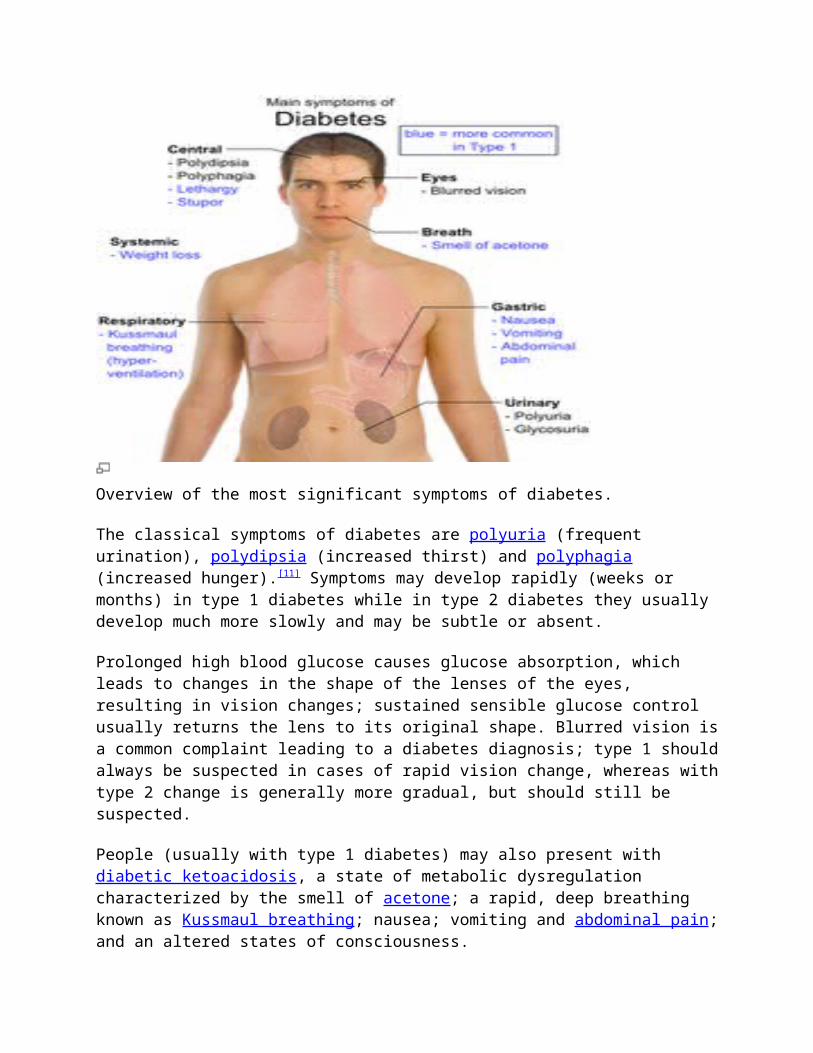
Overview of the most significant symptoms of diabetes.
The classical symptoms of diabetes are polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).[11] Symptoms may develop rapidly (weeks or months) in type 1 diabetes while in type 2 diabetes they usually develop much more slowly and may be subtle or absent.
Prolonged high blood glucose causes glucose absorption, which leads to changes in the shape of the lenses of the eyes, resulting in vision changes; sustained sensible glucose control usually returns the lens to its original shape. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected.
People (usually with type 1 diabetes) may also present with diabetic ketoacidosis, a state of metabolic dysregulation characterized by the smell of acetone; a rapid, deep breathing known as Kussmaul breathing; nausea; vomiting and abdominal pain; and an altered states of consciousness.
A rarer but equally severe possibility is hyperosmolar nonketotic state, which is more common in type 2 diabetes and is mainly the result of dehydration. Often, the patient has been drinking extreme amounts of sugar-containing drinks, leading to a vicious circle in regard to the water loss.
A number of skin rashes can occur in diabetes that are collectively known as diabetic dermadromes.

CausesThe cause of diabetes depends on the type. Type 2 diabetes is due primarily to lifestyle factors and genetics.[12]
Type 1 diabetes is also partly inherited and then triggered by certain infections, with some evidence pointing at Coxsackie B4 virus. There is a genetic element in individual susceptibility to some of these triggers which has been traced to particular HLA genotypes (i.e., the genetic "self" identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 diabetes mellitus seems to require an environmental trigger.
Pathophysiology
The fluctuation of blood sugar (red) and the sugar-lowering hormone insulin (blue) in humans during the course of a day with three meals. One of the effects of a sugar-rich vs a starch-rich meal is highlighted.
Mechanism of insulin release in normal pancreatic beta cells. Insulin production is more or less constant within the beta cells, irrespective of blood glucose levels. It is stored within vacuoles pending release, via exocytosis, which is primarily triggered by food, chiefly food containing absorbable glucose. The chief trigger is a rise in blood glucose levels after eating
Insulin is the principal hormone that regulates uptake of glucose from the blood into most cells (primarily muscle and fat cells, but not central nervous system cells). Therefore deficiency of insulin or the insensitivity of its receptors plays a central role in all forms of diabetes mellitus.
Humans are capable of digesting some carbohydrates, in particular those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms most notably the monosaccharide glucose, the principal carbohydrate energy source used by the body. The rest are passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-cells), found in the Islets of Langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the beta cells and in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon which acts in the opposite manner to insulin. Glucose thus forcibly produced from internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export mechanism. Normally liver cells do this when the level of insulin is low (which normally correlates with low levels of blood glucose).
Higher insulin levels increase some anabolic ("building up") processes such as cell growth and duplication, protein synthesis, and fat storage. Insulin (or its lack) is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic to an anabolic direction, and vice versa. In particular, a low insulin level is the trigger for entering or leaving ketosis (the fat burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or resistance), or if the insulin itself is defective, then glucose will not have its usual effect so that glucose will not be absorbed properly by those body cells that require it nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis.
When the glucose concentration in the blood is raised beyond its renal threshold (about 10 mmol/L, although this may be altered in certain conditions, such as pregnancy), reabsorption of glucose in the proximal renal tubuli is incomplete, and part of the glucose remains in the urine (glycosuria). This increases the osmotic pressure of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria) and increased fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body compartments, causing dehydration and increased thirst.
DiagnosisSee also: Glycosylated hemoglobin and Glucose tolerance test
2006 WHO Diabetes criteria[13] editCondition 2 hour glucose Fasting glucose
mmol/l(mg/dl) mmol/l(mg/dl)Normal <7.8 (<140) <6.1 (<110)
Impaired fasting glycaemia <7.8 (<140) ≥ 6.1(≥110) & <7.0(<126)

Impaired glucose tolerance ≥7.8 (≥140) <7.0 (<126)Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126)
Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by demonstrating any one of the following:[9]
Fasting plasma glucose level ≥ 7.0 mmol/L (126 mg/dL). Plasma glucose ≥ 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose load as in
a glucose tolerance test. Symptoms of hyperglycemia and casual plasma glucose ≥ 11.1 mmol/L (200 mg/dL). Glycated hemoglobin (Hb A1C) ≥ 6.5%.[14]
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. It is preferable to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test.[15] According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
People with fasting glucose levels from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) are considered to have impaired fasting glucose. Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired glucose tolerance. Of these two pre-diabetic states, the latter in particular is a major risk factor for progression to full-blown diabetes mellitus as well as cardiovascular disease.[16]
ManagementMain article: Diabetes management
Diabetes mellitus is a chronic disease which is difficult to cure. Management concentrates on keeping blood sugar levels as close to normal ("euglycemia") as possible without presenting undue patient danger. This can usually be with close dietary management, exercise, and use of appropriate medications (insulin only in the case of type 1 diabetes mellitus. Oral medications may be used in the case of type 2 diabetes, as well as insulin).
Patient education, understanding, and participation is vital since the complications of diabetes are far less common and less severe in people who have well-managed blood sugar levels.[17][18] Wider health problems may accelerate the deleterious effects of diabetes. These include smoking, elevated cholesterol levels, obesity, high blood pressure, and lack of regular exercise.
Lifestyle modifications
Main article: Diabetic diet

There are roles for patient education, dietetic support, sensible exercise, with the goal of keeping both short-term and long-term blood glucose levels within acceptable bounds. In addition, given the associated higher risks of cardiovascular disease, lifestyle modifications are recommended to control blood pressure.[19]
Medications
Oral medicationsMain article: Anti-diabetic drug
Routine use of aspirin has not been found to improve outcomes in uncomplicated diabetes.[20]
InsulinMain article: Insulin therapy
Type 1 treatments usually include combinations of regular or NPH insulin, and/or synthetic insulin analogs.
Support
In countries using a general practitioner system, such as the United Kingdom, care may take place mainly outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood sugar control, or research projects. In other circumstances, general practitioners and specialists share care of a patient in a team approach. Optometrists, podiatrists/chiropodists, dietitians, physiotherapists, nursing specialists (e.g., DSNs (Diabetic Specialist Nurse)), nurse practitioners, or Certified Diabetes Educators, may jointly provide multidisciplinary expertise. In countries where patients must provide for their own health care (e.g. in the US, and in much of the undeveloped world).
Peer support links people living with diabetes. Within peer support, people with a common illness share knowledge and experience that others, including many health workers, do not have. Peer support is frequent, ongoing, accessible and flexible and can take many forms—phone calls, text messaging, group meetings, home visits, and even grocery shopping. It complements and enhances other health care services by creating the emotional, social and practical assistance necessary for managing disease and staying healthy.
PrognosisMain article: Prognosis of diabetes mellitus
Diabetes doubles the risk of vascular problems, including cardiovascular disease.[21]
According to one study, women with high blood pressure (hypertension) were three times more likely to develop type 2 diabetes as compared with women with optimal BP after adjusting for various factors such as age, ethnicity, smoking, alcohol intake, body mass index (BMI), exercise, family history of diabetes, etc.[22] The study was conducted by researchers from the Brigham and

Women’s Hospital, Harvard Medical School and the Harvard School of Public Health, USA, who followed over 38,000 female health professionals for ten years.
Except in the case of type 1 diabetes, which always requires insulin replacement, the way type 2 diabetes is managed may change with age. Insulin production decreases because of age-related impairment of pancreatic beta cells. Additionally, insulin resistance increases because of the loss of lean tissue and the accumulation of fat, particularly intra-abdominal fat, and the decreased tissue sensitivity to insulin. Glucose tolerance progressively declines with age, leading to a high prevalence of type 2 diabetes and postchallenge hyperglycemia in the older population.[23] Age-related glucose intolerance in humans is often accompanied by insulin resistance, but circulating insulin levels are similar to those of younger people.[24] Treatment goals for older patients with diabetes vary with the individual, and take into account health status, as well as life expectancy, level of dependence, and willingness to adhere to a treatment regimen.[25] Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and death from any cause.[26]
Epidemiology
Prevalence of diabetes worldwide in 2000 (per 1000 inhabitants). World average was 2.8%. no data ≤ 7.5 7.5–15 15–22.5 22.5–30 30–37.5 37.5–45 45–52.5 52.5–60 60–67.5 67.5–75 75–82.5 ≥ 82.5

Disability-adjusted life year for diabetes mellitus per 100,000 inhabitants in 2002.[27] no data ≤ 100 100-200 200-300 300-400 400-500 500-600 600-700 700-800 800-900 900-1000 1000-1500 ≥ 1500
In 2000, according to the World Health Organization, at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[2] Its incidence is increasing rapidly, and it is estimated that by 2030, this number will almost double.[2] Diabetes mellitus occurs throughout the world, but is more common (especially type 2) in the more developed countries. The greatest increase in prevalence is, however, expected to occur in Asia and Africa, where most patients will probably be found by 2030.[2] The increase in incidence of diabetes in developing countries follows the trend of urbanization and lifestyle changes, perhaps most importantly a "Western-style" diet. This has suggested an environmental (i.e., dietary) effect, but there is little understanding of the mechanism(s) at present, though there is much speculation, some of it most compellingly presented.[2]
For at least 20 years, diabetes rates in North America have been increasing substantially. In 2008 there were about 24 million people with diabetes in the United States alone, from those 5.7 million people remain undiagnosed. Other 57 million people are estimated to have pre-diabetes.[28]
The Centers for Disease Control has termed the change an epidemic.[29] The National Diabetes Information Clearinghouse estimates that diabetes costs $132 billion in the United States alone every year. About 5%–10% of diabetes cases in North America are type 1, with the rest being type 2. The fraction of type 1 in other parts of the world differs. Most of this difference is not currently understood. The American Diabetes Association cite the 2003 assessment of the National Center for Chronic Disease Prevention and Health Promotion (Centers for Disease Control and Prevention) that 1 in 3 Americans born after 2000 will develop diabetes in their lifetime.[30][31]
According to the American Diabetes Association, approximately 18.3% (8.6 million) of Americans age 60 and older have diabetes.[32] Diabetes mellitus prevalence increases with age, and the numbers of older persons with diabetes are expected to grow as the elderly population increases in number. The National Health and Nutrition Examination Survey (NHANES III)

demonstrated that, in the population over 65 years old, 18% to 20% have diabetes, with 40% having either diabetes or its precursor form of impaired glucose tolerance.[23]
Indigenous populations in first world countries have a higher prevalence and increasing incidence of diabetes than their corresponding non-indigenous populations. In Australia the age-standardised prevalence of self-reported diabetes in Indigenous Australians is almost 4 times that of non-indigenous Australians.[33] Preventative community health programs such as Sugar Man (diabetes education) are showing some success in tackling this problem.
HistoryThe term diabetes (Greek: διαβήτης, diabētēs) (pronounced /ˌda ɪ .əˈbiːtiːz/ or /ˌdaɪ.əˈbiːtɨs/; /mɨˈlaɪtəs/ or /ˈmɛlɨtəs/) was coined by Aretaeus of Cappadocia. It was derived from the Greek verb διαβαίνειν, diabaínein, itself formed from the prefix dia-, "across, apart," and the verb bainein, "to walk, stand." The verb diabeinein meant "to stride, walk, or stand with legs asunder"; hence, its derivative diabētēs meant "one that straddles," or specifically "a compass, siphon." The sense "siphon" gave rise to the use of diabētēs as the name for a disease involving the discharge of excessive amounts of urine. Diabetes is first recorded in English, in the form diabete, in a medical text written around 1425. In 1675, Thomas Willis added the word mellitus, from the Latin meaning "honey", a reference to the sweet taste of the urine. This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians, Indians, and Persians. In 1776, Matthew Dobson confirmed that the sweet taste was because of an excess of a kind of sugar in the urine and blood of people with diabetes.[34]
Diabetes mellitus appears to have been a death sentence in the ancient era. Hippocrates makes no mention of it, which may indicate that he felt the disease was incurable. Aretaeus did attempt to treat it but could not give a good prognosis; he commented that "life (with diabetes) is short, disgusting and painful."[35]
Sushruta (6th century BCE) identified diabetes and classified it as Medhumeha.[36] He further identified it with obesity and sedentary lifestyle, advising exercises to help "cure" it.[36] The ancient Indians tested for diabetes by observing whether ants were attracted to a person's urine, and called the ailment "sweet urine disease" (Madhumeha). The Chinese, Japanese and Korean words for diabetes are based on the same ideographs (糖尿病) which mean "sugar urine disease".
In medieval Persia, Avicenna (980–1037) provided a detailed account on diabetes mellitus in The Canon of Medicine, "describing the abnormal appetite and the collapse of sexual functions," and he documented the sweet taste of diabetic urine. Like Aretaeus before him, Avicenna recognized a primary and secondary diabetes. He also described diabetic gangrene, and treated diabetes using a mixture of lupine, trigonella (fenugreek), and zedoary seed, which produces a considerable reduction in the excretion of sugar, a treatment which is still prescribed in modern times. Avicenna also "described diabetes insipidus very precisely for the first time", though it was later Johann Peter Frank (1745–1821) who first differentiated between diabetes mellitus and diabetes insipidus.[37][verification needed]

Although diabetes has been recognized since antiquity, and treatments of various efficacy have been known in various regions since the Middle Ages, and in legend for much longer, pathogenesis of diabetes has only been understood experimentally since about 1900.[38] The discovery of a role for the pancreas in diabetes is generally ascribed to Joseph von Mering and Oskar Minkowski, who in 1889 found that dogs whose pancreas was removed developed all the signs and symptoms of diabetes and died shortly afterwards.[39] In 1910, Sir Edward Albert Sharpey-Schafer suggested that people with diabetes were deficient in a single chemical that was normally produced by the pancreas—he proposed calling this substance insulin, from the Latin insula, meaning island, in reference to the insulin-producing islets of Langerhans in the pancreas.
The endocrine role of the pancreas in metabolism, and indeed the existence of insulin, was not further clarified until 1921, when Sir Frederick Grant Banting and Charles Herbert Best repeated the work of Von Mering and Minkowski, and went further to demonstrate they could reverse induced diabetes in dogs by giving them an extract from the pancreatic islets of Langerhans of healthy dogs.[40] Banting, Best, and colleagues (especially the chemist Collip) went on to purify the hormone insulin from bovine pancreases at the University of Toronto. This led to the availability of an effective treatment—insulin injections—and the first patient was treated in 1922. For this, Banting and laboratory director MacLeod received the Nobel Prize in Physiology or Medicine in 1923; both shared their Prize money with others in the team who were not recognized, in particular Best and Collip. Banting and Best made the patent available without charge and did not attempt to control commercial production. Insulin production and therapy rapidly spread around the world, largely as a result of this decision. Banting is honored by World Diabetes Day which is held on his birthday, November 14.
The distinction between what is now known as type 1 diabetes and type 2 diabetes was first clearly made by Sir Harold Percival (Harry) Himsworth, and published in January 1936.[41]
Despite the availability of treatment, diabetes has remained a major cause of death. For instance, statistics reveal that the cause-specific mortality rate during 1927 amounted to about 47.7 per 100,000 population in Malta.[42]
Other landmark discoveries include:[38]
Identification of the first of the sulfonylureas in 1942 Reintroduction of the use of biguanides for Type 2 diabetes in the late 1950s. The initial
phenformin was withdrawn worldwide (in the U.S. in 1977) due to its potential for sometimes fatal lactic acidosis and metformin was first marketed in France in 1979, but not until 1994 in the US.
The determination of the amino acid sequence of insulin (by Sir Frederick Sanger, for which he received a Nobel Prize)
The radioimmunoassay for insulin, as discovered by Rosalyn Yalow and Solomon Berson (gaining Yalow the 1977 Nobel Prize in Physiology or Medicine)[43]
The three-dimensional structure of insulin (PDB 2INS) Dr Gerald Reaven's identification of the constellation of symptoms now called metabolic
syndrome in 1988

Demonstration that intensive glycemic control in type 1 diabetes reduces chronic side effects more as glucose levels approach 'normal' in a large longitudinal study,[44] and also in type 2 diabetics in other large studies
Identification of the first thiazolidinedione as an effective insulin sensitizer during the 1990s
In 1980, U.S. biotech company Genentech developed human insulin. The insulin is isolated from genetically altered bacteria (the bacteria contain the human gene for synthesizing human insulin), which produce large quantities of insulin. The purified insulin is distributed to pharmacies for use by diabetes patients.
Society and cultureThe 1990 "St. Vincent Declaration"[45][46] was the result of international efforts to improve the care accorded to those with diabetes. Doing so is important both in terms of quality of life and life expectancy but also economically—expenses due to diabetes have been shown to be a major drain on health-and productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve treatment of the disease.[47]
A study shows that diabetic patients with neuropathic symptoms such as numbness or tingling in feet or hands are twice as likely to be unemployed as those without the symptoms.[48]
Diabetes Mellitus


Diabetes mellitus is a disorder in which blood sugar (glucose) levels are abnormally high because the body does not produce enough insulin to meet its needs.
Urination and thirst are increased, and people lose weight when they are not trying to.
Diabetes damages the nerves and causes problems with sensation. Diabetes damages blood vessels and increases the risk of heart attack,
stroke, and kidney failure. Doctors diagnose diabetes by measuring blood sugar levels. People with diabetes need to follow a low-sugar, low-fat diet, exercise,
and usually take drugs.
Insulin, a hormone released from the pancreas, controls the amount of sugar in the blood. When people eat or drink, food is broken down into materials, including the simple sugar glucose, that the body needs to function. Sugar is absorbed into the bloodstream and stimulates the pancreas to produce insulin. Insulin allows sugar to move from the blood into the cells. Once inside the cells, it is converted to energy, which is either used immediately or stored as fat or glycogen until it is needed.
The levels of sugar in the blood vary normally throughout the day. They rise after a meal and return to normal within about 2 hours after eating. Once the levels of sugar in the blood return to normal, insulin production decreases. The variation in blood sugar levels is usually within a narrow range, about 70 to 110 milligrams per deciliter (mg/dL) of blood. If people eat a large amount of carbohydrates, the levels may increase more. People older than 65 years tend to have slightly higher levels, especially after eating.
If the body does not produce enough insulin to move the sugar into the cells, the resulting high levels of sugar in the blood and the inadequate amount of sugar in the cells together produce the symptoms and complications of diabetes.
Doctors often use the full name diabetes mellitus, rather than diabetes alone, to distinguish this disorder from diabetes insipidus, a relatively rare disorder that

does not affect blood sugar levels (see Pituitary Gland Disorders: Central Diabetes Insipidus).
Types
Prediabetes: Prediabetes is a condition in which blood sugar levels are too high to be considered normal but not high enough to be labeled diabetes. People have prediabetes if their fasting blood sugar level is between 101 mg/dL and 126 mg/dL or if their blood sugar level 2 hours after a glucose tolerance test is between 140 mg/dL and 200 mg/dL. Identifying people with prediabetes is important because the condition carries a higher risk for future diabetes as well as heart disease. Decreasing body weight by 5 to 10 % through diet and exercise can significantly reduce the risk of developing future diabetes.
Type 1: In type 1 diabetes (formerly called insulin-dependent diabetes or juvenile-onset diabetes), more than 90% of the insulin-producing cells of the pancreas are permanently destroyed. The pancreas, therefore, produces little or no insulin. Only about 10% of all people with diabetes have type 1 disease. Most people who have type 1 diabetes develop the disease before age 30.
Scientists believe that an environmental factor—possibly a viral infection or a nutritional factor in childhood or early adulthood—causes the immune system to destroy the insulin-producing cells of the pancreas. A genetic predisposition may make some people more susceptible to the environmental factor.
Type 2: In type 2 diabetes (formerly called non-insulin-dependent diabetes or adult-onset diabetes), the pancreas continues to produce insulin, sometimes even at higher-than-normal levels. However, the body develops resistance to the effects of insulin, so there is not enough insulin to meet the body's needs.
Type 2 diabetes was once rare in children and adolescents but has recently become more common. However, it usually begins in people older than 30 and becomes progressively more common with age. About 15% of people older than 70 have type 2 diabetes. People of certain racial and ethnic backgrounds are at increased risk of developing type 2 diabetes: blacks, Native Americans, and Hispanics who live in the United States have a twofold to threefold increased risk. Type 2 diabetes also tends to run in families.
Obesity is the chief risk factor for developing type 2 diabetes, and 80 to 90% of people with this disorder are overweight or obese. Because obesity causes insulin resistance, obese people need very large amounts of insulin to maintain normal blood sugar levels.
Certain disorders and drugs can affect the way the body uses insulin and can lead to type 2 diabetes. High levels of corticosteroids (from Cushing's disease or from

taking corticosteroid drugs) and pregnancy (gestational diabetes—see Pregnancy Complicated by Disease: Gestational Diabetes) are the most common causes of altered insulin use. Diabetes also may occur in people with excess production of growth hormone (acromegaly) and in people with certain hormone-secreting tumors. Severe or recurring pancreatitis and other disorders that directly damage the pancreas can lead to diabetes.
Symptoms
The two types of diabetes have very similar symptoms. The first symptoms are related to the direct effects of high blood sugar levels. When the blood sugar level rises above 160 to 180 mg/dL, sugar spills into the urine. When the level of sugar in the urine rises even higher, the kidneys excrete additional water to dilute the large amount of sugar. Because the kidneys produce excessive urine, people with diabetes urinate large volumes frequently (polyuria). The excessive urination creates abnormal thirst (polydipsia). Because excessive calories are lost in the urine, people lose weight. To compensate, people often feel excessively hungry. Other symptoms include blurred vision, drowsiness, nausea, and decreased endurance during exercise.
Type 1: In people with type 1 diabetes, the symptoms often begin abruptly and dramatically. A condition called diabetic ketoacidosis may quickly develop. Without insulin, most cells cannot use the sugar that is in the blood. Cells still need energy to survive, and they switch to a back-up mechanism to obtain energy. Fat cells begin to break down, producing compounds called ketones. Ketones provide some energy to cells but also make the blood too acidic (ketoacidosis). The initial symptoms of diabetic ketoacidosis include excessive thirst and urination, weight loss, nausea, vomiting, fatigue, and—particularly in children—abdominal pain. Breathing tends to become deep and rapid as the body attempts to correct the blood's acidity (see Acid-Base Balance: Acidosis). The breath smells like nail polish remover, the smell of the ketones escaping into the breath. Without treatment, diabetic ketoacidosis can progress to coma and death, sometimes within a few hours.
Type 2: People with type 2 diabetes may not have any symptoms for years or decades before they are diagnosed. Symptoms may be subtle. Increased urination and thirst are mild at first and gradually worsen over weeks or months. Eventually, people feel extremely fatigued, are likely to develop blurred vision, and may become dehydrated.
Sometimes during the early stages of diabetes, the blood sugar level is abnormally low, a condition called hypoglycemia (see Hypoglycemia).
Because people with type 2 diabetes produce some insulin, ketoacidosis does not usually develop. However, the blood sugar levels can become extremely high

(often exceeding 1,000 mg/dL). Such high levels often happen as the result of some superimposed stress, such as an infection or drug use. When the blood sugar levels get very high, people may develop severe dehydration, which may lead to mental confusion, drowsiness, and seizures, a condition called nonketotic hyperglycemic-hyperosmolar coma.
Complications
People with diabetes may experience many serious, long-term complications. Some of these complications begin within months of the onset of diabetes, although most tend to develop after a few years. Most of the complications are progressive. The more strictly people with diabetes are able to control the levels of sugar in the blood, the less likely it is that these complications will develop or become worse.
Most complications are the result of problems with blood vessels. High sugar levels over a long time cause narrowing of both the small and large blood vessels. The narrowing reduces blood flow to many parts of the body, leading to problems. There are several causes of blood vessel narrowing. Complex sugar-based substances build up in the walls of small blood vessels, causing them to thicken and leak. Poor control of blood sugar levels also tends to cause the levels of fatty substances in the blood to rise, resulting in atherosclerosis (see Atherosclerosis) and decreased blood flow in the larger blood vessels. Atherosclerosis is between 2 and 6 times more common in people with diabetes than in people who do not have diabetes and tends to occur at younger ages.
Over time, elevated levels of sugar in the blood and poor circulation can harm the heart, brain, legs, eyes, kidneys, nerves, and skin, resulting in angina, heart failure, strokes, leg cramps on walking (claudication), poor vision, kidney failure, damage to nerves (neuropathy), and skin breakdown. Heart attacks and strokes are more common among people with diabetes.
Poor circulation to the skin can lead to ulcers and infections and causes wounds to heal slowly. People with diabetes are particularly likely to have ulcers and infections of the feet and legs. Too often, these wounds heal slowly or not at all, and amputation of the foot or part of the leg may be needed.
People with diabetes often develop bacterial and fungal infections, typically of the skin. When the levels of sugar in the blood are high, white blood cells cannot effectively fight infections. Any infection that develops tends to be more severe.
Did You Know... People who can strictly control
their blood sugar levels may be

able to minimize or delay diabetes complications.
Damage to the blood vessels of the eye can cause loss of vision (diabetic retinopathy—see Retinal Disorders: Diabetic Retinopathy). Laser surgery can seal the leaking blood vessels of the eye and prevent permanent damage to the retina. Therefore, people with diabetes should have yearly eye examinations to check for damage.
The kidneys can malfunction, resulting in kidney failure that may require dialysis or kidney transplantation. Doctors usually check the urine of people with diabetes for abnormally high levels of protein (albumin), which is an early sign of kidney damage. At the earliest sign of kidney complications, people are often given angiotensin-converting enzyme (ACE) inhibitors, drugs that slow the progression of kidney damage.
Damage to nerves can manifest in several ways. If a single nerve malfunctions, an arm or leg may suddenly become weak. If the nerves to the hands, legs, and feet become damaged (diabetic polyneuropathy), sensation may become abnormal, and tingling or burning pain and weakness in the arms and legs may develop (see Peripheral Nerve Disorders: Causes). Damage to the nerves of the skin makes repeated injuries more likely because people cannot sense changes in pressure or temperature.
Long-Term Complications of DiabetesTissue or Organ Affected
What Happens Complications
Blood vessels Fatty material (atherosclerotic plaque) builds up and blocks large or medium-sized arteries in the heart, brain, legs, and penis.
The walls of small blood vessels are damaged so that the vessels do not transfer oxygen to tissues normally, and the vessels may leak.
Poor circulation causes wounds to heal poorly and can lead to heart disorders, strokes, gangrene of the feet and hands, erectile dysfunction (impotence), and infections.
Eyes The small blood vessels of the retina are damaged.
Decreased vision and, ultimately, blindness occur.
Kidney Blood vessels in the kidney thicken.
The kidneys malfunction, and ultimately, kidney failure occurs.

Protein leaks into urine.
Blood is not filtered normally.Nerves Nerves are damaged because
glucose is not metabolized normally and because the blood supply is inadequate.
Legs suddenly or gradually weaken.
People have reduced sensation, tingling, and pain in their hands and feet.
Autonomic nervous system
The nerves that control blood pressure and digestive processes are damaged.
Swings in blood pressure occur.
Swallowing becomes difficult.
Digestive function is altered, and sometimes bouts of diarrhea occur.
Erectile dysfunction develops.Skin Blood flow to the skin is
reduced, and sensation is decreased, resulting in repeated injury.
Sores and deep infections (diabetic ulcers) develop.
Healing is poor.Blood White blood cell function is
impaired.People become more susceptible to infections, especially of the urinary tract and skin.
Connective tissue
Glucose is not metabolized normally, causing tissues to thicken or contract.
Carpal tunnel syndrome and Dupuytren's contracture develop.
The Foot in DiabetesDiabetes causes many changes in the body. The following changes in the feet are common and difficult to treat.
Damage to the nerves (neuropathy) affects sensation to the feet, so that pain is not felt. Irritation and other forms of injury may go unnoticed. An injury may wear through the skin before any pain is felt.
Changes in sensation alter the

way people with diabetes carry weight on their feet, concentrating weight in certain areas so that calluses form. Calluses (and dry skin) increase the risk of skin breakdown.
Diabetes can cause poor circulation in the feet, making ulcers more likely to form when the skin is damaged and making the ulcers slower to heal.
Because diabetes can affect the body's ability to fight infections, a foot ulcer, once it forms, easily becomes infected. Because of neuropathy, people may not feel discomfort from the infection until it becomes serious and difficult to treat, leading to gangrene. People with diabetes are more than 30 times more likely to require amputation of a foot or leg than are people without diabetes.
Foot care is critical (see Caring for the Feet ). The feet should be protected from injury, and the skin should be kept moist with a good moisturizer. Shoes should fit properly and not cause areas of irritation. Shoes should have appropriate cushioning to spread out the pressure caused by standing. Going barefoot is ill advised. Regular care from a podiatrist, such as having toenails cut and calluses removed, may also be helpful. Also, sensation and blood flow to the feet should be regularly evaluated by doctors.Diagnosis
The diagnosis of diabetes is made when people have abnormally high levels of sugar in the blood. Blood sugar levels are often checked during a routine physical examination. Checking the levels of sugar in the blood annually is particularly important in older people, because diabetes is so common in later life. People may have diabetes, particularly type 2 diabetes, and not know it. Doctors may also check blood sugar levels in people who have symptoms of diabetes such as increased thirst, urination, or hunger. Doctors may also check

blood sugar levels in people who have disorders that can be complications of diabetes, such as frequent infections, foot ulcers, and yeast infections.
To measure the blood sugar levels, a blood sample is usually taken after people have fasted overnight. However, it is possible to take blood samples after people have eaten. Some elevation of blood sugar levels after eating is normal, but even after a meal the levels should not be very high. Fasting blood sugar levels should never be higher than 126 mg/dL. Even after eating, blood sugar levels should not be higher than 200 mg/dL.
Doctors can also measure the level of a protein in the blood, hemoglobin A1C (also called glycosylated or glycolated or hemoglobin). Glycosylated hemoglobin forms when the blood has been exposed to high blood sugar levels over a period of time. Doctors do not usually use this test to diagnose diabetes, but the test can help confirm the diagnosis when blood sugar levels are not extremely high. The test demonstrates long-term trends in blood sugar levels.
Another kind of blood test, an oral glucose tolerance test, may be done in certain situations, such as in routine screening of pregnant women for gestational diabetes (see Pregnancy Complicated by Disease: Gestational Diabetes) or in older people who have symptoms of diabetes but normal glucose levels when fasting. However, it is not routinely used for testing for diabetes, including in pregnant women at very low risk. In this test, people fast, have a blood sample taken to determine the fasting blood sugar level, and then drink a special solution containing a large, standard amount of glucose. More blood samples are then taken over the next 2 to 3 hours and are tested to determine whether the level of sugar in the blood rises abnormally high.
Did You Know... Many people have type 2
diabetes and are not aware of it.
Treatment
Treatment of diabetes involves diet, exercise, education, and, for most people, drugs. If people with diabetes strictly control blood sugar levels, complications are less likely to develop. The goal of diabetes treatment, therefore, is to keep blood sugar levels within the normal range as much as possible. Treatment of high blood pressure and cholesterol levels can prevent some of the complications of diabetes as well. A low dose of aspirin Some Trade Names BAYERtaken daily is also helpful.
People with diabetes benefit greatly from learning about the disorder,

understanding how diet and exercise affect their blood sugar levels, and knowing how to avoid complications. A nurse trained in diabetes education can provide information about managing diet, exercising, monitoring blood sugar levels, and taking drugs.
People with diabetes should always carry or wear medical identification (such as a bracelet or tag) to alert health care practitioners to the presence of diabetes. This information allows health care practitioners to start life-saving treatment quickly, especially in the case of injury or altered mental status.
Diet management is very important in people with both types of diabetes. Doctors recommend a healthy, balanced diet and efforts to maintain a healthy weight. Some people benefit from meeting with a dietitian to develop an optimal eating plan.
People with type 1 diabetes who are able to maintain a healthy weight may be able to avoid the need for large doses of insulin Some Trade Names HUMULINNOVOLIN. People with type 2 diabetes may be able to avoid the need for all drugs by achieving and maintaining a healthy weight. Some people who have been unsuccessful in losing weight through diet and exercise may take drugs to help them lose weight or may even undergo stomach reduction surgery.
In general, people with diabetes should not eat much sweet food. They should also try to eat meals on a regular schedule. Long periods between eating should be avoided. People with diabetes also tend to have high levels of cholesterol in the blood, so limiting the amount of saturated fat in the diet is important. Drugs may also be needed to help control the level of cholesterol in the blood.
Appropriate amounts of exercise can also help people control their weight and maintain blood sugar levels within the normal range. Because blood sugar levels go down during exercise, people must be alert for symptoms of low blood sugar. Some people need to eat a small amount of food with sugar during prolonged exercise, decrease their insulin dose, or both. People with diabetes should stop smoking and consume only moderate amounts of alcohol (up to one drink per day for women and two for men).
Diabetic ketoacidosis is a medical emergency, because it can cause coma and death. Hospitalization, usually in an intensive care unit, is necessary. Large amounts of fluids are given intravenously along with electrolytes, such as sodium, potassium, chloride, and phosphate, to replace those fluids and electrolytes lost through excessive urination. Insulin Some Trade Names HUMULINNOVOLINis generally given intravenously so that it works quickly and the dose can be adjusted frequently. Blood levels of sugar, ketones, and electrolytes are measured

every few hours. Doctors also measure the blood's acid level. Sometimes, additional treatments are needed to correct a high acid level. However, controlling the levels of sugar in the blood and replacing electrolytes usually allow the body to restore the normal acid-base balance.
Nonketotic hyperglycemic-hyperosmolar coma is treated much like diabetic ketoacidosis. Fluids and electrolytes must be replaced. The levels of sugar in the blood must be restored to normal levels gradually to avoid sudden shifts of fluid into the brain. The blood sugar levels tend to be more easily controlled than in diabetic ketoacidosis, and blood acidity problems are not severe.
Insulin Replacement Therapy
People with type 1 diabetes almost always require insulin Some Trade Names HUMULINNOVOLINtherapy, and many people with type 2 diabetes require it as well. Insulin Some Trade Names HUMULINNOVOLINis injected. It currently cannot be taken by mouth because insulin Some Trade Names HUMULINNOVOLINis destroyed in the stomach. A nasal spray form of insulin Some Trade Names HUMULINNOVOLINwas available but has been discontinued. New forms of insulin Some Trade Names HUMULINNOVOLIN, such as forms that can be taken by mouth or applied to the skin, are being tested.
Insulin
Insulin Some Trade Names HUMULINNOVOLINis injected under the skin into the fat layer, usually in the arm, thigh, or abdominal wall. Small syringes with very thin needles make the injections nearly painless. An air pump device that blows the insulin Some Trade Names HUMULINNOVOLINunder the skin can be used for people who cannot tolerate needles. An insulin Some Trade Names HUMULINNOVOLINpen, which contains a cartridge that holds the insulin Some Trade Names

HUMULINNOVOLIN, is a convenient way for many people to carry insulin Some Trade Names HUMULINNOVOLIN, especially for people who take several injections a day outside the home. Another device is an insulin Some Trade Names HUMULINNOVOLINpump, which pumps insulin Some Trade Names HUMULINNOVOLINcontinuously from a reservoir through a small needle left in the skin. Additional doses of insulin Some Trade Names HUMULINNOVOLINcan be released at programmed times, or release can be triggered as needed. The pump more closely mimics the way the body normally produces insulin Some Trade Names HUMULINNOVOLIN. For some people, the pump offers an added degree of control, whereas others find wearing the pump annoying or develop sores at the needle site.
Insulin Some Trade Names HUMULINNOVOLINis available in three basic forms, divided by speed of onset and duration of action:
Rapid-acting insulin, such as regular insulin Some Trade Names HUMULINNOVOLIN, is fast and short acting. Regular insulin Some Trade Names HUMULINNOVOLINreaches its maximum activity in 2 to 4 hours and works for 6 to 8 hours. Lispro, aspart, and glulisine insulins, special types of regular insulin Some Trade Names HUMULINNOVOLIN, are the fastest of all, reaching maximum activity in about 1 hour and working for 3 to 5 hours. Rapid-acting insulin Some Trade Names HUMULINNOVOLINis often used by people who take several daily injections and is injected 15 to 20 minutes before meals or just after eating.
Intermediate-acting insulin (such as insulin Some Trade Names HUMULINNOVOLINzinc suspension, lente, or isophane insulin Some Trade Names HUMULINNOVOLINsuspension) starts to work in 1 to 3 hours, reaches its maximum activity in 6 to 10 hours, and works for 18 to 26 hours. This type of insulin Some Trade Names HUMULINNOVOLINmay be used in the morning to provide coverage for the first part of the day or in the evening to provide coverage during the night.

Long-acting insulin (such as extended insulin Some Trade Names HUMULINNOVOLINzinc suspension, ultra-lente, or glargine) has very little effect in the first few hours but provides coverage for 20 to 36 hours depending on which of these types is used.
Insulin Some Trade Names HUMULINNOVOLINpreparations are stable at room temperature for months, allowing them to be carried, brought to work, or taken on a trip. Insulin Some Trade Names HUMULINNOVOLINshould not, however, be exposed to extreme temperatures.
The choice of insulin Some Trade Names HUMULINNOVOLINis complex. The following factors are considered before deciding which insulin Some Trade Names HUMULINNOVOLINis best:
How willing and able people are to monitor their blood sugar levels and adjust the insulin Some Trade Names HUMULINNOVOLINdosage
How varied daily activity is How adept people are at learning about and understanding the disorder How stable blood sugar levels are during the day and from day to day
The easiest regimen to follow is a single daily injection of an intermediate-acting insulin Some Trade Names HUMULINNOVOLIN. However, such a regimen provides the least control over blood sugar levels and is, therefore, rarely the best approach. Stricter control may be achieved by combining two insulins—a rapid-acting and an intermediate-acting insulin Some Trade Names HUMULINNOVOLIN—in one morning dose. This combination requires more skill, but it offers people greater opportunity to adjust the blood sugar levels. A second injection of one insulin Some Trade Names HUMULINNOVOLINor both may be taken at dinner or at bedtime. Strictest control is usually achieved by injecting a rapid-acting and an intermediate-acting insulin Some Trade Names
HUMULINNOVOLINin the morning and evening along with several additional injections of rapid-acting insulin Some Trade Names

HUMULINNOVOLINduring the day. Adjustments can be made as insulin Some Trade Names HUMULINNOVOLINneeds change. Measuring blood sugar levels at various times during the day helps determine the adjustment. Although this regimen requires the most knowledge of the disorder and attention to the details of treatment, it is considered the best option for most people who are treated with insulin Some Trade Names HUMULINNOVOLIN, especially people with type 1 diabetes.
Some people, especially older people, take the same amount of insulin Some Trade Names HUMULINNOVOLINevery day. Other people adjust the insulin Some Trade Names HUMULINNOVOLINdose daily depending on their diet, exercise, and blood sugar patterns. In addition, insulin Some Trade Names HUMULINNOVOLINneeds may change if people gain or lose weight or experience emotional stress or illness, especially infection.
Over time, some people develop resistance to insulin Some Trade Names HUMULINNOVOLIN. Because the injected insulin Some Trade Names HUMULINNOVOLINis not exactly like the insulin Some Trade Names HUMULINNOVOLINthe body manufactures, the body can produce antibodies to the insulin Some Trade Names HUMULINNOVOLIN. Although this is less common with newer insulin Some Trade Names HUMULINNOVOLINpreparations, these antibodies may interfere with the insulin Some Trade Names HUMULINNOVOLIN's activity, requiring very large doses.
Insulin Some Trade Names HUMULINNOVOLINinjections can affect the skin and underlying tissues. An allergic reaction, which occurs rarely, produces pain and burning, followed by redness, itchiness, and swelling around the injection site for several hours. More commonly, the injections either cause fat deposits, making the skin look lumpy, or destroy fat, causing indentation of the skin. Many people rotate the injection sites, for example, using the thigh one day, the stomach another, and an arm the next, to

avoid these problems.
Insulin Replacement Therapy
Oral Antihyperglycemic Drugs
Oral antihyperglycemic drugs can often lower blood sugar levels adequately in people with type 2 diabetes. However, they are not effective in type 1 diabetes. There are several types. Sulfonylureas (for example, glyburide Some Trade Names DIABETAMICRONASE) and meglitinides (for example, repaglinide Some Trade Names PRANDIN) stimulate the pancreas to produce more insulin Some Trade Names HUMULINNOVOLIN( insulin Some Trade Names HUMULINNOVOLINsecretagogues). Biguanides (for example, metformin Some Trade Names GLUCOPHAGE) and thiazolidinediones (for example, rosiglitazone Some Trade Names AVANDIA) do not affect the release of insulin Some Trade Names HUMULINNOVOLINbut increase the body's response to it ( insulin Some Trade Names HUMULINNOVOLINsensitizers). Doctors may prescribe one of these drugs alone or with a sulfonylurea drug. Another class of drug is the glucosidase inhibitors, such as acarbose Some Trade Names PRECOSE, which work by delaying absorption of glucose in the intestine.
Oral antihyperglycemic drugs are usually prescribed for people with type 2 diabetes if diet and exercise fail to lower the levels of sugar in the blood adequately. The drugs are sometimes taken only once a day, in the morning, although some people need two or three doses. More than one type of oral drug may be used if one is not adequate. If oral antihyperglycemic drugs cannot

control blood sugar levels well enough, insulin Some Trade Names HUMULINNOVOLINinjections alone or in combination with the oral drugs may be needed.
Oral Antihyperglycemic DrugsDrug Number of Daily Doses Selected Side Effects Biguanides Metformin Some Trade Names GLUCOPHAGE
2 to 3 Diarrhea
Increased acidity of body fluids (rare)
Liver failure (rare)Extended-release metformin Some Trade Names GLUCOPHAGE
1 to 2
Sulfonylureas Acetohexamide 1 to 2 Weight gain
Low sodium in blood (hyponatremia) with chlorpropamide Some Trade Names DIABINESE
Chlorpropamide Some Trade Names DIABINESE
1
Glimepiride Some Trade Names AMARYL
1
Glipizide Some Trade Names GLUCOTROL
1 to 2
Glyburide Some Trade Names DIABETAMICRONASE
1 to 2
Micronized glyburide Some Trade Names
1 to 2

DIABETAMICRONASE
Tolazamide 1 to 2 Tolbutamide 1 to 2 Meglitinides Nateglinide Some Trade Names STARLIX
3 Minimal weight gain
Repaglinide Some Trade Names PRANDIN
3
Thiazolidinediones Pioglitazone Some Trade Names ACTOS
1 Weight gain
Fluid retention (edema)
Rosiglitazone Some Trade Names AVANDIA
1 to 2 Weight gain
Fluid retention (edema)
Possible increase in heart attacks
Alpha-glucosidase inhibitors Acarbose Some Trade Names PRECOSE
3 Diarrhea
Abdominal pain
BloatingMiglitol Some Trade Names GLYSET
3
Dipeptidyl peptidase-4 inhibitor Sitagliptin Some Trade Names JANUVIA
1 Headache
Diarrhea
Lung infectionsGlucagon-like peptide agonists Exenatide Some Trade Names BYETTA
2 Nausea
Vomiting
Amylin analog Pramlintide Some Trade 3 Nausea

Names SYMLIN
Low blood sugar levelsMonitoring Treatment
Monitoring blood sugar levels is an essential part of diabetes care. People with diabetes must adjust their diet, exercise, and take drugs to control blood sugar levels. Monitoring blood sugar levels provides the information needed to make those adjustments. Waiting until symptoms of low or high blood sugar levels develop is a recipe for disaster.
Many things cause blood sugar levels to change:
Diet Exercise Stress Illness Drug Time of day
The blood sugar levels may jump after people eat foods they did not realize were high in carbohydrates. Exercise may cause the levels of sugar in the blood to fall low, requiring that additional sugar be eaten. Emotional stress, an infection, and many drugs tend to increase blood sugar levels. Blood sugar levels increase in many people in the early morning hours because of the normal release of hormones (growth hormone and corticosteroids), a reaction called the dawn phenomenon. And blood sugar may shoot too high if the body releases sugar in response to low blood sugar levels (Somogyi effect).
Blood sugar levels can be measured easily at home or anywhere. Most blood sugar monitoring devices use a drop of blood obtained by pricking the tip of the finger with a small lancet. The lancet holds a tiny needle that can be jabbed into the finger or placed in a spring-loaded device that easily and quickly pierces the skin. Most people find the pricking nearly painless. Then, a drop of blood is placed on a reagent strip. In response to sugar, the reagent strip undergoes some chemical changes. A machine reads the changes in the test strip and reports the result on a digital display. Most of these machines time the reaction and read the result automatically. Some devices allow the blood sample to be obtained from other sites, such as the palm, forearm, upper arm, thigh, or calf. The machines are smaller than a deck of cards.
A newer device reads blood sugar through the skin without needing a sample of blood. The device is worn like a wristwatch and can measure the level of sugar in the blood every 15 minutes. Alarms on the device can be set to sound when blood sugar levels drop too low or climb too high. Disadvantages of this device are that it must be calibrated periodically with a blood test, it may irritate the

skin, and it is somewhat large. Other devices can monitor glucose continuously. However, these devices are not routinely used, as they are expensive and have not been shown to be better than glucose meters. In certain circumstances, these devices are less reliable, such as in severe hypoglycemia.
Most people with diabetes should keep a record of their blood sugar levels and report them to their doctors or nurses for advice in adjusting the dose of insulin Some Trade Names HUMULINNOVOLINor the oral antihyperglycemic drug. Many people can learn to adjust the insulin Some Trade Names HUMULINNOVOLINdose on their own as necessary.
Spotlight on AgingOlder people need to follow the same general principles of diabetes management—education, diet, exercise, and drugs—as younger people. However, risking hypoglycemia by strictly controlling blood sugar levels may not be beneficial for people with a short life expectancy, such as those with advanced cancer. Also, managing diabetes can be more difficult for older people. Poor eyesight may make it hard for them to read glucose meters and dose scales on insulin Some Trade Names HUMULINNOVOLINsyringes. They may have problems manipulating the syringe because they have arthritis or Parkinson's disease or have had a stroke. When older people have hypoglycemia, their symptoms may be less obvious. If they have hypoglycemia but have difficulty communicating, dementia or both, they may not be able to let anyone know they are having symptoms.
Education: In addition to learning about diabetes itself, older people may have to learn how to fit management of diabetes in with their management of other disorders. Learning about how to avoid complications, such as dehydration, skin breakdown, and circulation problems, and to manage factors that can contribute to diabetes, such as high blood pressure and high cholesterol levels, is especially important. Such problems become more common as people age, whether they have diabetes or not.
Diet: Many older people have difficulty following a healthy, balanced diet that can control blood sugar levels and weight. Changing long-held food preferences and dietary habits may be hard. Some older people have other disorders that can be affected by diet and may not understand how to integrate the dietary

recommendations for their various disorders.
Some older people cannot control what they eat because someone else is cooking for them―at home or in a nursing home or other institution. When people with diabetes do not do their own cooking, the people who shop and prepare meals for them must also understand the diet that is needed. Older people and their caregivers usually benefit from meeting with a dietitian to develop a healthy, feasible eating plan.
Exercise: Older people may have a difficult time adding exercise to their daily life, particularly if they have not been active or if they have a disorder that limits their movement, such as arthritis. However, they may be able to add exercise to their usual routine. For example, they can walk instead of drive or climb the stairs instead of take the elevator. Also, many community organizations offer exercise programs designed for older people.
Drugs: Taking the drugs used to treat diabetes, particularly insulin Some Trade Names HUMULINNOVOLIN, may be difficult for some older people. For those with vision problems or other problems that make accurately filling a syringe difficult, a caregiver can prepare the syringes ahead of time and store them in the refrigerator. People whose insulin Some Trade Names HUMULINNOVOLINdose is stable may purchase pre-filled syringes. Prefilled insulin Some Trade Names HUMULINNOVOLINpen devices may be easier for people with physical limitations to use. Some of these devices have large numbers and easy-to-turn dials.
Monitoring blood sugar levels: Poor vision, limited manual dexterity due to arthritis, tremor, or stroke, or other physical limitations may make monitoring blood sugar levels more difficult for older people. However, special monitors are available. Some have large numerical displays that are easier to read. Some provide audible instructions and results. Some monitors read blood sugar levels through the skin and do not require a blood sample. People can consult a diabetes educator to determine which meter is most appropriate.
Complications of treatment: The most common complication of treating high blood sugar levels is low blood sugar levels. The risk is greatest for older people who are frail, who are sick enough to require frequent hospital admissions, or who are taking several drugs. Of all available drugs to treat diabetes, long-acting sulfonylurea drugs are most likely to cause low blood sugar levels in older people. When they take these drugs, they are also more likely to have serious symptoms, such as fainting and falling, and to have diffculty thinking or using

parts of the body due to low blood sugar levels.Although urine can also be tested for the presence of sugar, checking urine is not a good way to monitor treatment or adjust therapy. Urine testing can be misleading because the amount of sugar in the urine may not reflect the current level of sugar in the blood. Blood sugar levels can get very low or reasonably high without any change in the sugar levels in the urine.
Doctors can monitor treatment using a blood test called hemoglobin A1C. When the blood sugar levels are high, changes occur in hemoglobin, the protein that carries oxygen in the blood. These changes are in direct proportion to the blood sugar levels over an extended period. Thus, unlike the blood sugar measurement, which reveals the level at a particular moment, the hemoglobin A1C measurement demonstrates whether the blood sugar levels have been controlled over the previous few months. People with diabetes aim for a hemoglobin A1C level of less than 7%. Achieving this level is difficult, but the lower the hemoglobin A1C level, the less likely people are to have complications. Levels above 9% show poor control, and levels above 12% show very poor control. Most doctors who specialize in diabetes care recommend that hemoglobin A1C be measured every 3 to 6 months. Fructosamine, an amino acid that has bonded with glucose, is also useful for measuring blood sugar control over a period of a few weeks.
Monitoring and Preventing Complications
At the time of diagnosis and then at least yearly, people are monitored for the presence of diabetes complications, such as kidney, eye, and nerve damage. Worsening of complications can be prevented or delayed by strict blood sugar control or by early drug treatment. Risk factors for heart problems, such as increased blood pressure and high cholesterol levels, are evaluated at each doctor visit and are treated with drugs if necessary. Another common problem in people with diabetes is gum disease (gingivitis), and regular visits to the dentist for cleaning and preventive care are important.
Hypoglycemia: Keeping blood sugar levels from getting too high is difficult. The main difficulty with trying to strictly control the levels of sugar in the blood is that low blood sugar levels (hypoglycemia) may occur (see Hypoglycemia). Recognizing the presence of low blood sugar is important because treatment of hypoglycemia is an emergency. Symptoms may include hunger pangs, racing heart beat, shakiness, sweating, and inability to think clearly. Sugar must get into the body within minutes to prevent permanent harm and relieve symptoms. Most of the time, people can eat sugar. Almost any form of sugar will do, although glucose works more quickly than table sugar (typical table sugar is sucrose). Many people with diabetes carry glucose tablets or foil packets of a glucose-containing liquid. Other options are to drink a glass of milk (which contains lactose, a type of sugar), sugar water, or fruit juice or to eat a piece of cake, some fruit, or another sweet food. In more serious situations, it may be necessary for

emergency medical practitioners to inject glucose into a vein.
Another treatment for hypoglycemia involves the use of glucagon. Glucagon can be injected into the muscle and causes the liver to release large amounts of glucose within minutes. Small transportable kits containing a syringe filled with glucagon are available for people with diabetes to use in emergency situations.
Experimental Treatments
Experimental treatments are also showing promise for the treatment of type 1 diabetes. In one such treatment, insulin-producing cells are transplanted into body organs. This procedure is not yet routinely done, however, because immunosuppressant drugs must be given to prevent the body from rejecting the transplanted cells. Newer techniques may make suppression of the immune system unnecessary.
Diabetes Mellitus Case StudyPosted by: Admin
May 15, 2008 · 48 Comments · Email This Post · Print This Post
INTRODUCTION:
Diabetes mellitus is a condition in which the pancreas no longer produces enough insulin or cells stop responding to the insulin that is produced, so that glucose in the blood cannot be absorbed into the cells of the body. Symptoms include frequent urination, lethargy, excessive thirst, and hunger. The treatment includes changes in diet, oral medications, and in some cases, daily injections of insulin.
The most common form of diabetes is Type II, It is sometimes called age-onset or adult-onset diabetes, and this form of diabetes occurs most often in people who are overweight and who do not exercise. Type II is considered a milder form of diabetes because of its slow onset (sometimes developing over the course of several years) and because it usually can be controlled with diet and oral medication. The consequences of uncontrolled and untreated Type II diabetes, however, are the just as serious as those for Type I. This form is also called noninsulin-dependent diabetes, a term that is somewhat misleading. Many people with Type II diabetes can

control the condition with diet and oral medications, however, insulin injections are sometimes necessary if treatment with diet and oral medication is not working.
The causes of diabetes mellitus are unclear, however, there seem to be both hereditary (genetic factors passed on in families) and environmental factors involved. Research has shown that some people who develop diabetes have common genetic markers. In Type I diabetes, the immune system, the body’s defense system against infection, is believed to be triggered by a virus or another microorganism that destroys cells in the pancreas that produce insulin. In Type II diabetes, age, obesity, and family history of diabetes play a role.
In Type II diabetes, the pancreas may produce enough insulin, however, cells have become resistant to the insulin produced and it may not work as effectively. Symptoms of Type II diabetes can begin so gradually that a person may not know that he or she has it. Early signs are lethargy, extreme thirst, and frequent urination. Other symptoms may include sudden weight loss, slow wound healing, urinary tract infections, gum disease, or blurred vision. It is not unusual for Type II diabetes to be detected while a patient is seeing a doctor about another health concern that is actually being caused by the yet undiagnosed diabetes.
Individuals who are at high risk of developing Type II diabetes mellitus include people who:
are obese (more than 20% above their ideal body weight) have a relative with diabetes mellitus belong to a high-risk ethnic population (African-American, Native American, Hispanic,
or Native Hawaiian) have been diagnosed with gestational diabetes or have delivered a baby weighing more
than 9 lbs (4 kg) have high blood pressure (140/90 mmHg or above) have a high density lipoprotein cholesterol level less than or equal to 35 mg/dL and/or a
triglyceride level greater than or equal to 250 mg/dL have had impaired glucose tolerance or impaired fasting glucose on previous testing
Diabetes mellitus is a common chronic disease requiring lifelong behavioral and lifestyle changes. It is best managed with a team approach to empower the client to successfully manage the disease. As part of the team the, the nurse plans, organizes, and coordinates care among the various health disciplines involved; provides care and education and promotes the client’s health and well being. Diabetes is a major public health worldwide. Its complications cause many devastating health problems.
ANATOMY AND PHYSIOLOGY:
Every cell in the human body needs energy in order to function. The body’s primary energy source is glucose, a simple sugar resulting from the digestion of foods containing carbohydrates (sugars and starches). Glucose from the digested food circulates in the blood as a ready energy source for any cells that need it. Insulin is a hormone or chemical produced by cells in the pancreas, an organ located behind the stomach. Insulin bonds to a receptor site on the outside of cell and acts like a key to open a doorway into the cell through which glucose can enter. Some of

the glucose can be converted to concentrated energy sources like glycogen or fatty acids and saved for later use. When there is not enough insulin produced or when the doorway no longer recognizes the insulin key, glucose stays in the blood rather entering the cells.
PATHOPHYSIOLOGY:

Image Source: www.caninsulin.com/Pathophysiology-algorithm.htm
DIAGNOSTIC TEST:
Several blood tests are used to measure blood glucose levels, the primary test for diagnosing diabetes. Additional tests can determine the type of diabetes and its severity.
Random blood glucose test — for a random blood glucose test, blood can be drawn at any time throughout the day, regardless of when the person last ate. A random blood glucose level of 200 mg/dL (11.1 mmol/L) or higher in persons who have symptoms of high blood glucose (see “Symptoms” above) suggests a diagnosis of diabetes.
Fasting blood glucose test — fasting blood glucose testing involves measuring blood glucose after not eating or drinking for 8 to 12 hours (usually overnight). A normal

fasting blood glucose level is less than 100 mg/dL. A fasting blood glucose of 126 mg/dL (7.0 mmol/L) or higher indicates diabetes. The test is done by taking a small sample of blood from a vein or fingertip. It must be repeated on another day to confirm that it remains abnormally high (see “Criteria for diagnosis” below).
Hemoglobin A1C test (A1C) — The A1C blood test measures the average blood glucose level during the past two to three months. It is used to monitor blood glucose control in people with known diabetes, but is not normally used to diagnose diabetes. Normal values for A1C are 4 to 6 percent (show figure 3). The test is done by taking a small sample of blood from a vein or fingertip.
Oral glucose tolerance test — Oral glucose tolerance testing (OGTT) is the most sensitive test for diagnosing diabetes and pre-diabetes. However, the OGTT is not routinely recommended because it is inconvenient compared to a fasting blood glucose test.
The standard OGTT includes a fasting blood glucose test. The person then drinks a 75 gram liquid glucose solution (which tastes very sweet, and is usually cola or orange-flavored). Two hours later, a second blood glucose level is measured.
Oral glucose tolerance testing is routinely performed at 24 to 28 weeks of pregnancy to screen for gestational diabetes; this requires drinking a 50 gram glucose solution with a blood glucose level drawn one hour later. For women who have an abnormally elevated blood glucose level, a second OGTT is performed on another day after drinking a 100 gram glucose solution. The blood glucose level is measured before, and at one, two, and three hours after drinking the solution.
MEDICATIONS:
When diet, exercise and maintaining a healthy weight aren’t enough, you may need the help of medication. Medications used to treat diabetes include insulin. Everyone with type 1 diabetes and some people with type 2 diabetes must take insulin every day to replace what their pancreas is unable to produce. Unfortunately, insulin can’t be taken in pill form because enzymes in your stomach break it down so that it becomes ineffective. For that reason, many people inject themselves with insulin using a syringe or an insulin pen injector,a device that looks like a pen, except the cartridge is filled with insulin. Others may use an insulin pump, which provides a continuous supply of insulin, eliminating the need for daily shots.
The most widely used form of insulin is synthetic human insulin, which is chemically identical to human insulin but manufactured in a laboratory. Unfortunately, synthetic human insulin isn’t perfect. One of its chief failings is that it doesn’t mimic the way natural insulin is secreted. But newer types of insulin, known as insulin analogs, more closely resemble the way natural insulin acts in your body. Among these are lispro (Humalog), insulin aspart (NovoLog) and glargine (Lantus).
A number of drug options exist for treating type 2 diabetes, including:

· Sulfonylurea drugs. These medications stimulate your pancreas to produce and release more insulin. For them to be effective, your pancreas must produce some insulin on its own. Second-generation sulfonylureas such as glipizide (Glucotrol, Glucotrol XL), glyburide (DiaBeta, Glynase PresTab, Micronase) and glimepiride (Amaryl) are prescribed most often. The most common side effect of sulfonylureas is low blood sugar, especially during the first four months of therapy. You’re at much greater risk of low blood sugar if you have impaired liver or kidney function.
· Meglitinides. These medications, such as repaglinide (Prandin), have effects similar to sulfonylureas, but you’re not as likely to develop low blood sugar. Meglitinides work quickly, and the results fade rapidly.
· Biguanides. Metformin (Glucophage, Glucophage XR) is the only drug in this class available in the United States. It works by inhibiting the production and release of glucose from your liver, which means you need less insulin to transport blood sugar into your cells. One advantage of metformin is that is tends to cause less weight gain than do other diabetes medications. Possible side effects include a metallic taste in your mouth, loss of appetite, nausea or vomiting, abdominal bloating, or pain, gas and diarrhea. These effects usually decrease over time and are less likely to occur if you take the medication with food. A rare but serious side effect is lactic acidosis, which results when lactic acid builds up in your body. Symptoms include tiredness, weakness, muscle aches, dizziness and drowsiness. Lactic acidosis is especially likely to occur if you mix this medication with alcohol or have impaired kidney function.
· Alpha-glucosidase inhibitors. These drugs block the action of enzymes in your digestive tract that break down carbohydrates. That means sugar is absorbed into your bloodstream more slowly, which helps prevent the rapid rise in blood sugar that usually occurs right after a meal. Drugs in this class include acarbose (Precose) and miglitol (Glyset). Although safe and effective, alpha-glucosidase inhibitors can cause abdominal bloating, gas and diarrhea. If taken in high doses, they may also cause reversible liver damage.
· Thiazolidinediones. These drugs make your body tissues more sensitive to insulin and keep your liver from overproducing glucose. Side effects of thiazolidinediones, such as rosiglitazone (Avandia) and pioglitazone hydrochloride (Actos), include swelling, weight gain and fatigue. A far more serious potential side effect is liver damage. The thiazolidinedione troglitzeone (Rezulin) was taken off the market in March 2000 because it caused liver failure. If your doctor prescribes these drugs, it’s important to have your liver checked every two months during the first year of therapy. Contact your doctor immediately if you experience any of the signs and symptoms of liver damage, such as nausea and vomiting, abdominal pain, loss of appetite, dark urine, or yellowing of your skin and the whites of your eyes (jaundice). These may not always be related to diabetes medications, but your doctor will need to investigate all possible causes.
· Drug combinations. By combining drugs from different classes, you may be able to control your blood sugar in several different ways. Each class of oral medication can be combined with drugs from any other class. Most doctors prescribe two drugs in combination, although sometimes three drugs may be prescribed. Newer medications, such as Glucovance, which contains both glyburide and metformin, combine different oral drugs in a single tablet.

NURSING INTERVENTIONS:
Advice patient about the importance of an individualized meal plan in meeting weekly weight loss goals and assist with compliance.
Assess patients for cognitive or sensory impairments, which may interfere with the ability to accurately administer insulin.
Demonstrate and explain thoroughly the procedure for insulin self-injection. Help patient to achieve mastery of technique by taking step by step approach.
Review dosage and time of injections in relation to meals, activity, and bedtime based on patients individualized insulin regimen.
Instruct patient in the importance of accuracy of insulin preparation and meal timing to avoid hypoglycemia.
Explain the importance of exercise in maintaining or reducing weight. Advise patient to assess blood glucose level before strenuous activity and to eat
carbohydrate snack before exercising to avoid hypoglycemia. Assess feet and legs for skin temperature, sensation, soft tissues injuries, corns, calluses,
dryness, hair distribution, pulses and deep tendon reflexes. Maintain skin integrity by protecting feet from breakdown. Advice patient who smokes to stop smoking or reduce if possible, to reduce
vasoconstriction and enhance peripheral flow.


















