promarkny.files.wordpress.com · Web viewPlease print, fill and fax to: (585) 424-3647. Phone:...
2
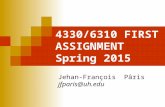
Please print, fill and fax to: (585) 424-3647 Phone: 535-424-4330 gina@promarkny,com [email protected] Long Term Care Proposal Request Agent Name: ____________________________________ Phone Number: ___________ Client Name: ____________________________________Date of Birth: _____________ Spouse Name: ___________________________________ Date of Birth: _____________ Product Requested: NYS Partnership Plan Total Asset 3/6/50 Elimination Period 30day 60day 90/100day Total Asset 4/4/100 Lifetime Pay 10 Pay Dollar for Dollar 1.5/3/50 Premium Mode Annual Semi- Annual Quarterly Monthly Dollar for Dollar 2/2/100 Medications and Additional Health History Both Applying? Non-Partnership Cash Benefit Total Benefit Monthly Payout $100,000 $200,000 $300,000 $500,000 $1,000,000 $3,000 $4,500 $6,000 $7,500 $9,000 $12,000 Inflation Option Elimination Period 30day 60day 90/100day 5% Compound 5% Compound x2 3% Compound 5% Simple None Lifetime Pay 10 Pay Riders Spouse Waiver of Premium Return of Premium Rider Survivor Benefit Rider Shared Care Rider Life Insurance/LTC Benefit Combination Call for details (585) 424-4330
Transcript of promarkny.files.wordpress.com · Web viewPlease print, fill and fax to: (585) 424-3647. Phone:...

Please print, fill and fax to: (585) 424-3647Phone: 535-424-4330 gina@promarkny,com [email protected]
Long Term Care Proposal RequestAgent Name: ____________________________________ Phone Number: ___________
Client Name: ____________________________________ Date of Birth: _____________
Spouse Name: ___________________________________ Date of Birth: _____________
Product Requested:
NYS Partnership PlanTotal Asset3/6/50
Elimination Period30day 60day
90/100dayTotal Asset 4/4/100
Lifetime Pay10 Pay
Dollar for Dollar1.5/3/50
Premium ModeAnnualSemi-AnnualQuarterlyMonthly
Dollar for Dollar2/2/100
Medications and Additional Health History
Medical History: Circle those that apply
Client Tobacco Stroke Diabetes Cancer Heart DiseaseSpou Tobacco Stroke Diabetes Cancer Heart Disease
Both Applying?
Non-Partnership Cash Benefit
Total Benefit Monthly Payout$100,000
$200,000
$300,000
$500,000
$1,000,000
$3,000
$4,500
$6,000
$7,500
$9,000
$12,000Inflation Option Elimination Period
30day 60day90/100day
5% Compound
5% Compound x2
3% Compound
5% Simple
None
Lifetime Pay10 Pay
Riders Spouse Waiver of Premium Return of Premium Rider Survivor Benefit Rider Shared Care Rider
Life Insurance/LTC Benefit Combination
Call for details(585) 424-4330

se