Watermark Medical ARES Sleep Study · PDF fileWatermark Medical ARES Sleep Study Report....
2
Watermark Medical ARES Sleep Study Report PHYSICIAN INTERPRETATION AND COMMENTS: Findings are consistent with severe, positional obstructive sleep apnea (OSA). CLINICAL HISTORY: 58 year old male presented with: 16.5 inch neck, BMI of 30, an Epworth sleepiness score of 8, no co-morbidities and symptoms of nocturnal snoring and witnessed apneas. Based on the clinical history, the patient has a high pre-test probability of having severe OSA. SLEEP STUDY FINDINGS: Patient underwent a one night Home Sleep Test and by behavioral criteria, slept for approximately 6.5 hours, with a sleep latency of 3 minutes and a sleep efficiency of 92.3%. Severe sleep disordered breathing (AHI=39 ) is noted based on a 4% hypopnea desaturation criteria, predominantly in the supine position (58 events/hour). The patient slept supine 54.8% of the night based on valid sleep time of 6.5 hours and is 3.6 times as likely to have apneas/hypopneas when supine. When considering more subtle measures of sleep disordered breathing, the overall respiratory disturbance index is also severe (RDI=53 ) based on a 1% hypopnea desaturation criteria with confirmation by surrogate arousal indicators. The apneas/hypopneas are accompanied by minimal oxygen desaturation (percent time below 90% SpO2: 4.2%, Min SpO2: 80.1%). The average desaturation across all sleep disordered breathing events is 4.5%. Snoring occurs for 45.6% (30 dB) of the study, 41.4% is very loud. The mean pulse rate is 55 BPM, with very frequent pulse rate variability (72 events with >= 6 BPM increase/decrease per hour). TREATMENT CONSIDERATIONS: Consider nasal continuous positive airway pressure (CPAP ) as the initial treatment choice for severe obstructive sleep apnea. An auto - PAP or an auto - PAP titration study may be appropriate given the ARES predicted CPAP pressure of 11 cm H2O. A mandibular advancement splint (MAS) or referral to an ENT surgeon for modification to the airway should be considered to reduce the risk of mortality caused by severe OSA if the patient prefers an alternative therapy or the CPAP trial is unsuccessful. A Mandibular Advancement Splint (MAS ) will likely provide treatment benefit independent of OSA severity. The patient should avoid sleeping supine ; the non-supine RDI is 2.2 times less severe than the supine RDI. DISEASE MANAGEMENT CONSIDERATIONS: None. Study Review: The raw data of this ARES study has been reviewed, with the report confirmed. Caution:The diagnosis of the Obstructive Sleep Apnea Syndrome must be based on all available clinical data, of which this study is only a part. Thus final diagnosis and treatment recommendations should include information from an examination of the patient by a knowledgeable physician. ARES Traceability: 20110930171725_f410ad0f-87eb-e011-9b04-005056b80e76_N1.ASI; N/A; ARES Sleep Study Report Patient Name Turek, Don Study Ordered by Carson, Thomas E Date of Night 1 09/28/2011 Date of Birth 5/14/1953 Identification Number RACAN2383199 Overall AHI Overall RDI % time < 90% SpO2 Mean SpO2 % time snoring > 30 dB 39 53 4.2 % 94.9 % 45.6 % Signature: Date:
-
Upload
nguyentuyen -
Category
Documents
-
view
220 -
download
3
Transcript of Watermark Medical ARES Sleep Study · PDF fileWatermark Medical ARES Sleep Study Report....

Watermark Medical
ARES Sleep Study Report
PHYSICIAN INTERPRETATION AND COMMENTS: Findings are consistent with severe, positional obstructivesleep apnea (OSA).
CLINICAL HISTORY: 58 year old male presented with: 16.5 inch neck, BMI of 30, an Epworth sleepiness score of 8, noco-morbidities and symptoms of nocturnal snoring and witnessed apneas. Based on the clinical history, the patient has a highpre-test probability of having severe OSA.
SLEEP STUDY FINDINGS: Patient underwent a one night Home Sleep Test and by behavioral criteria, slept forapproximately 6.5 hours, with a sleep latency of 3 minutes and a sleep efficiency of 92.3%. Severe sleep disordered breathing(AHI=39) is noted based on a 4% hypopnea desaturation criteria, predominantly in the supine position (58 events/hour). Thepatient slept supine 54.8% of the night based on valid sleep time of 6.5 hours and is 3.6 times as likely to haveapneas/hypopneas when supine. When considering more subtle measures of sleep disordered breathing, the overall respiratorydisturbance index is also severe (RDI=53) based on a 1% hypopnea desaturation criteria with confirmation by surrogatearousal indicators. The apneas/hypopneas are accompanied by minimal oxygen desaturation (percent time below 90% SpO2:4.2%, Min SpO2: 80.1%). The average desaturation across all sleep disordered breathing events is 4.5%. Snoring occurs for45.6% (30 dB) of the study, 41.4% is very loud. The mean pulse rate is 55 BPM, with very frequent pulse rate variability (72events with >= 6 BPM increase/decrease per hour).
TREATMENT CONSIDERATIONS: Consider nasal continuous positive airway pressure (CPAP) as the initialtreatment choice for severe obstructive sleep apnea. An auto-PAP or an auto-PAP titration study may be appropriategiven the ARES predicted CPAP pressure of 11 cm H2O. A mandibular advancement splint (MAS) or referral to an ENTsurgeon for modification to the airway should be considered to reduce the risk of mortality caused by severe OSA if the patientprefers an alternative therapy or the CPAP trial is unsuccessful. A Mandibular Advancement Splint (MAS) will likelyprovide treatment benefit independent of OSA severity. The patient should avoid sleeping supine; the non-supine RDI is2.2 times less severe than the supine RDI.
DISEASE MANAGEMENT CONSIDERATIONS: None.
Study Review: The raw data of this ARES study has been reviewed, with the report confirmed. Caution:The diagnosis of the ObstructiveSleep Apnea Syndrome must be based on all available clinical data, of which this study is only a part. Thus final diagnosis and treatmentrecommendations should include information from an examination of the patient by a knowledgeable physician.
ARES Traceability: 20110930171725_f410ad0f-87eb-e011-9b04-005056b80e76_N1.ASI; N/A;
ARES Sleep Study Report
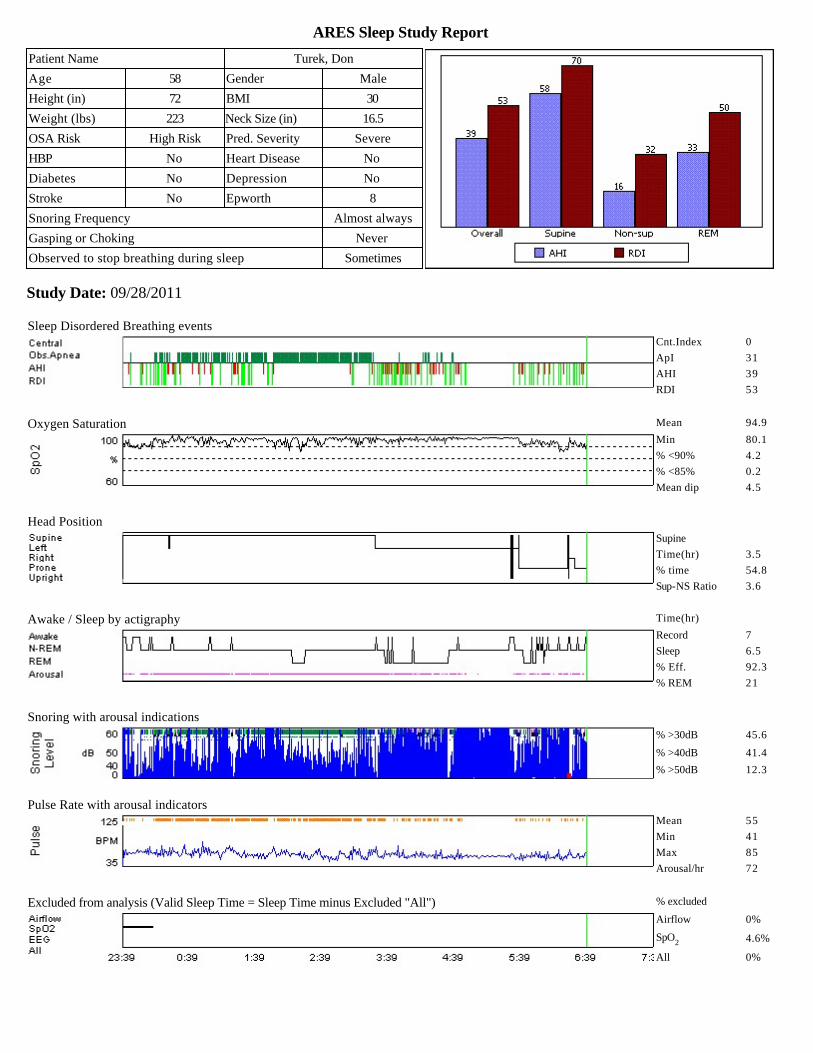
Study Date: 09/28/2011
Patient Name Turek, Don Study Ordered by Carson, Thomas E
Date of Night 1 09/28/2011 Date of Birth 5/14/1953
Identification Number RACAN2383199
Overall AHI Overall RDI % time < 90% SpO2 Mean SpO2 % time snoring > 30 dB
39 53 4.2 % 94.9 % 45.6 %
Signature: Date:
Patient Name Turek, Don
Age 58 Gender Male
Height (in) 72 BMI 30
Weight (lbs) 223 Neck Size (in) 16.5
OSA Risk High Risk Pred. Severity Severe
HBP No Heart Disease No
Diabetes No Depression No
Stroke No Epworth 8
Snoring Frequency Almost always
Gasping or Choking Never
Observed to stop breathing during sleep Sometimes
Sleep Disordered Breathing eventsCnt.Index 0
ApI 31
AHI 39
RDI 53
Oxygen Saturation Mean 94.9
Min 80.1
% <90% 4.2
% <85% 0.2
Mean dip 4.5
Head PositionSupine
Time(hr) 3.5
% time 54.8
Sup-NS Ratio 3.6
Awake / Sleep by actigraphy Time(hr)
Record 7
Sleep 6.5
% Eff. 92.3
% REM 21
Snoring with arousal indications
% >30dB 45.6
% >40dB 41.4
% >50dB 12.3
Pulse Rate with arousal indicatorsMean 55
Min 41
Max 85
Arousal/hr 72
Excluded from analysis (Valid Sleep Time = Sleep Time minus Excluded "All") % excluded
Airflow 0%
SpO2 4.6%
All 0%
Brandon M Womack
Rectangle
Brandon M Womack
Rectangle
Brandon M Womack
Text Box
Severe OSA Sample Report - Type II Device: Minimum 7 Channels Presented by Advanced Diagnostic
Watermark Medical
ARES Sleep Study Report
PHYSICIAN INTERPRETATION AND COMMENTS: Findings are consistent with severe, positional obstructivesleep apnea (OSA).
CLINICAL HISTORY: 58 year old male presented with: 16.5 inch neck, BMI of 30, an Epworth sleepiness score of 8, noco-morbidities and symptoms of nocturnal snoring and witnessed apneas. Based on the clinical history, the patient has a highpre-test probability of having severe OSA.
SLEEP STUDY FINDINGS: Patient underwent a one night Home Sleep Test and by behavioral criteria, slept forapproximately 6.5 hours, with a sleep latency of 3 minutes and a sleep efficiency of 92.3%. Severe sleep disordered breathing(AHI=39) is noted based on a 4% hypopnea desaturation criteria, predominantly in the supine position (58 events/hour). Thepatient slept supine 54.8% of the night based on valid sleep time of 6.5 hours and is 3.6 times as likely to haveapneas/hypopneas when supine. When considering more subtle measures of sleep disordered breathing, the overall respiratorydisturbance index is also severe (RDI=53) based on a 1% hypopnea desaturation criteria with confirmation by surrogatearousal indicators. The apneas/hypopneas are accompanied by minimal oxygen desaturation (percent time below 90% SpO2:4.2%, Min SpO2: 80.1%). The average desaturation across all sleep disordered breathing events is 4.5%. Snoring occurs for45.6% (30 dB) of the study, 41.4% is very loud. The mean pulse rate is 55 BPM, with very frequent pulse rate variability (72events with >= 6 BPM increase/decrease per hour).
TREATMENT CONSIDERATIONS: Consider nasal continuous positive airway pressure (CPAP) as the initialtreatment choice for severe obstructive sleep apnea. An auto-PAP or an auto-PAP titration study may be appropriategiven the ARES predicted CPAP pressure of 11 cm H2O. A mandibular advancement splint (MAS) or referral to an ENTsurgeon for modification to the airway should be considered to reduce the risk of mortality caused by severe OSA if the patientprefers an alternative therapy or the CPAP trial is unsuccessful. A Mandibular Advancement Splint (MAS) will likelyprovide treatment benefit independent of OSA severity. The patient should avoid sleeping supine; the non-supine RDI is2.2 times less severe than the supine RDI.
DISEASE MANAGEMENT CONSIDERATIONS: None.
Study Review: The raw data of this ARES study has been reviewed, with the report confirmed. Caution:The diagnosis of the ObstructiveSleep Apnea Syndrome must be based on all available clinical data, of which this study is only a part. Thus final diagnosis and treatmentrecommendations should include information from an examination of the patient by a knowledgeable physician.
ARES Traceability: 20110930171725_f410ad0f-87eb-e011-9b04-005056b80e76_N1.ASI; N/A;
ARES Sleep Study Report
Study Date: 09/28/2011
Patient Name Turek, Don Study Ordered by Carson, Thomas E
Date of Night 1 09/28/2011 Date of Birth 5/14/1953
Identification Number RACAN2383199
Overall AHI Overall RDI % time < 90% SpO2 Mean SpO2 % time snoring > 30 dB
39 53 4.2 % 94.9 % 45.6 %
Signature: Date:
Patient Name Turek, Don
Age 58 Gender Male
Height (in) 72 BMI 30
Weight (lbs) 223 Neck Size (in) 16.5
OSA Risk High Risk Pred. Severity Severe
HBP No Heart Disease No
Diabetes No Depression No
Stroke No Epworth 8
Snoring Frequency Almost always
Gasping or Choking Never
Observed to stop breathing during sleep Sometimes
Sleep Disordered Breathing eventsCnt.Index 0
ApI 31
AHI 39
RDI 53
Oxygen Saturation Mean 94.9
Min 80.1
% <90% 4.2
% <85% 0.2
Mean dip 4.5
Head PositionSupine
Time(hr) 3.5
% time 54.8
Sup-NS Ratio 3.6
Awake / Sleep by actigraphy Time(hr)
Record 7
Sleep 6.5
% Eff. 92.3
% REM 21
Snoring with arousal indications
% >30dB 45.6
% >40dB 41.4
% >50dB 12.3
Pulse Rate with arousal indicatorsMean 55
Min 41
Max 85
Arousal/hr 72
Excluded from analysis (Valid Sleep Time = Sleep Time minus Excluded "All") % excluded
Airflow 0%
SpO2 4.6%
All 0%
Brandon M Womack
Rectangle