Water reclamation redesign for reducing Cryptosporidium risks at a recreational spray park using...
10
Water reclamation redesign for reducing Cryptosporidium risks at a recreational spray park using stochastic models Mark H. Weir a, *, Maria Tereza Pepe Razzolini b , Joan B. Rose a , Yoshifumi Masago c a Department of Fisheries and Wildlife, Michigan State University, 303 Manly Miles Building, 1405 S. Harrison Rd., East Lansing, MI 48824, USA b School of Public Health, University of Sao Paul, Sao Paulo, Brazil c Department of Civil and Environmental Engineering, Tohoku University, Japan article info Article history: Received 30 November 2010 Received in revised form 22 September 2011 Accepted 24 September 2011 Available online 14 October 2011 Keywords: Risk assessment Monte Carlo Markov chains Water treatment Cryptosporidium abstract Recreational outbreaks associated with sprayparks are well recognized, and may be partly due to the engineering designs used for their water reclamation systems are problematic to control. This work is based on an outbreak of cryptosporidiosis linked to a spraypark in New York State, where it was determined, specifically that the spraypad (the main attraction) was the primary exposure point. We first determined the likely dose the spraypad users were exposed to, then modeled the efficacy of the treatment system and used this to inform a Monte Carlo method to estimate the probability of infection and illness for the users of the spraypad. The current treatment system which consists of; two holding tanks, a dual media filter and chlorine injection as well as two design change recommendations were modeled using three independent Markov chain models. Within the current treatment system design the receiving tank for the treatment train is also connected with a second pipe to the spraypad used to deliver the return (treated) water, this return pipe is acting potentially as a bypass for the treatment train. Based on the risk assessments performed it is recommended that the bypass pipe be removed from the treatment system since in doing so the probability of infection and illness were reduced appreciably. Secondarily including an ozone contactor was shown to slightly reduce the risk further and provide a multiple barrier. ª 2011 Elsevier Ltd. All rights reserved. 1. Introduction 1.1. General overview In recent years, an increase of waterborne outbreaks associ- ated with treated recreational waters has been observed. In the United States from 2005 to 2006, treated water venues were associated with 58 recreational water outbreaks, with 24 outbreaks reported in 2005 and 34 in 2006, resulting in a total of 4167 cases of gastroenteritis (CDC, 2008). According to the CDC, 33 (56.9%) of the 58 outbreaks of gastroenteritis were caused by protozoan parasites and of these 33 outbreaks 31 (93.9%) were identified as being caused by Cryptosporidium (CDC, 2008). Cryptosporidium has been recognized as the most frequent cause of recreational water-associated outbreaks of gastroenteritis, including treated and disinfected venues (CDC, 2007). Causer et al. (2006) reported an outbreak of Cryptosporidium infection at an Illinois recreational waterpark in 2001. From 13 August to 30 September a total of 358 cases were identified * Corresponding author. Tel.: þ1 570 460 8459; fax: þ1 517 353 9807. E-mail address: [email protected] (M.H. Weir). Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/watres water research 45 (2011) 6505 e6514 0043-1354/$ e see front matter ª 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.watres.2011.09.047
-
Upload
mark-h-weir -
Category
Documents
-
view
216 -
download
3
Transcript of Water reclamation redesign for reducing Cryptosporidium risks at a recreational spray park using...
ww.sciencedirect.com
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 4
Available online at w
journal homepage: www.elsevier .com/locate/watres
Water reclamation redesign for reducing Cryptosporidium risksat a recreational spray park using stochastic models
Mark H. Weir a,*, Maria Tereza Pepe Razzolini b, Joan B. Rose a, Yoshifumi Masago c
aDepartment of Fisheries and Wildlife, Michigan State University, 303 Manly Miles Building, 1405 S. Harrison Rd., East Lansing, MI 48824,
USAb School of Public Health, University of Sao Paul, Sao Paulo, BrazilcDepartment of Civil and Environmental Engineering, Tohoku University, Japan
a r t i c l e i n f o
Article history:
Received 30 November 2010
Received in revised form
22 September 2011
Accepted 24 September 2011
Available online 14 October 2011
Keywords:
Risk assessment
Monte Carlo
Markov chains
Water treatment
Cryptosporidium
* Corresponding author. Tel.: þ1 570 460 845E-mail address: [email protected] (M
0043-1354/$ e see front matter ª 2011 Elsevdoi:10.1016/j.watres.2011.09.047
a b s t r a c t
Recreational outbreaks associated with sprayparks are well recognized, and may be partly
due to the engineering designs used for their water reclamation systems are problematic to
control. This work is based on an outbreak of cryptosporidiosis linked to a spraypark in
New York State, where it was determined, specifically that the spraypad (the main
attraction) was the primary exposure point. We first determined the likely dose the
spraypad users were exposed to, then modeled the efficacy of the treatment system and
used this to inform a Monte Carlo method to estimate the probability of infection and
illness for the users of the spraypad. The current treatment system which consists of; two
holding tanks, a dual media filter and chlorine injection as well as two design change
recommendations were modeled using three independent Markov chain models. Within
the current treatment system design the receiving tank for the treatment train is also
connected with a second pipe to the spraypad used to deliver the return (treated) water,
this return pipe is acting potentially as a bypass for the treatment train. Based on the risk
assessments performed it is recommended that the bypass pipe be removed from the
treatment system since in doing so the probability of infection and illness were reduced
appreciably. Secondarily including an ozone contactor was shown to slightly reduce the
risk further and provide a multiple barrier.
ª 2011 Elsevier Ltd. All rights reserved.
1. Introduction CDC, 33 (56.9%) of the 58 outbreaks of gastroenteritis were
1.1. General overview
In recent years, an increase of waterborne outbreaks associ-
ated with treated recreational waters has been observed. In
the United States from 2005 to 2006, treated water venues
were associated with 58 recreational water outbreaks, with 24
outbreaks reported in 2005 and 34 in 2006, resulting in a total
of 4167 cases of gastroenteritis (CDC, 2008). According to the
9; fax: þ1 517 353 9807..H. Weir).
ier Ltd. All rights reserved
caused by protozoan parasites and of these 33 outbreaks 31
(93.9%) were identified as being caused by Cryptosporidium
(CDC, 2008). Cryptosporidium has been recognized as the most
frequent cause of recreational water-associated outbreaks of
gastroenteritis, including treated and disinfected venues
(CDC, 2007).
Causer et al. (2006) reported an outbreak of Cryptosporidium
infection at an Illinois recreational waterpark in 2001. From 13
August to 30 September a total of 358 cases were identified
.

wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 46506
(281 clinical cases and 77 laboratory-confirmed), 77.9% of
them were children (those less than 18 years old). Laboratory
analysis revealed the presence of Cryptosporidium oocysts in
stool specimens from 77 patients, 22 of these specimens
underwent genotypic testing, with ten (45.5%) positive for
Cryptosporidium hominis. Water samples from the toddler/
wading pool and backwash filter system were positive for
Cryptosporidium using USEPAMethod 1622 but all of themwere
PCR negative. According to epidemiological study and envi-
ronmental analysis, the evidence associated attending the
waterpark with the outbreak.
Later, Wheeler et al. (2007) reported an outbreak of cryp-
tosporidiosis at a California waterpark in 2004, where more
than 250 persons were ill due to a common exposure to the
waterpark. Cryptosporidium oocysts were found in stool spec-
imens from 52 persons as well as detected in water samples
from the sand and backwash from the filter. No Cryptospo-
ridium was detected from either the lake or three wells which
supplied the park. According to the authors, both the epide-
miological and environmental investigation supported the
hypothesis that the outbreak was associated with using the
waterslides in the waterpark.
The work presented in this paper is based on a cryptospo-
ridiosis outbreak which occurred at a New York State recrea-
tional spraypark which affected 746 people who reported
gastrointestinal illness after attending the spraypark facility.
In 2005 a formal request submitted by Joan B. Rose via the
freedom of information acts, garnered information and data
on the epidemiology, environmental and engineering inves-
tigation and the engineering designs of the spraypark. After
this information was obtained a quantitative microbial risk
assessment (QMRA) was developed in order to evaluate the
probability of infectiondue to exposure to contaminatedwater
withCryptosporidium oocysts, aswell as evaluate the efficacy of
potential combined treatment retrofits aimed at reducing
recreational risks. The goal of this work was first to evaluate
this outbreak of cryptosporidiosis so as to inform the level of
contamination and exposure for the recreating population at
this spraypark. Second, stochastic models of the water recla-
mation treatment system (and design recommendations)
were used as inputs to theMonte Carlomodel,whichwas used
as the means of modeling the risk of infection and illness.
This risk estimate was then used to examine the effective-
ness of engineering design change(s) for the recreational spray
park to reduce the risk of cryptosporidiosis. Two main design
changes were analyzed, first the removal of the pipe, (which
was likely acting as a bypass) from the treatment system, and
the combination of removing this pipe and adding an ozone
contactor. These redesign options were chosen as likely
responses which would ensure use of the current treatment
system (as the entire system could not be bypassed) and
a potential addition to the treatment trainwhich is specifically
able to inactivate oocysts (ozone contactor). The addition of
chlorinewas continued, however for this analysis chlorination
is considered negligibly effective for Cryptosporidium oocysts.
1.2. Cryptosporidium as an environmental Hazard
Cryptosporidium oocysts are environmentally robust, persis-
tent in water and are resistant to common disinfectants
(Smith and Rose, 1998; WHO, 2002, 2006; Carey et al., 2004).
Cryptosporidium transmission occurs by ingestion of food or
water contaminated by oocysts which are relatively potent
even at low doses compared to other pathogens (Smith and
Rose, 1998; WHO, 2006; Haas et al., 1999). The oocysts are
excreted in the feces of the infected host with levels as high
as 107 oocysts per gram of feces and can be shed for as long
as 50 days after the cessation of diarrhea (Chappell et al.,
1996; CDC, 2007). The cryptosporidiosis symptoms are
persistent diarrhea, fever, abdominal cramps, nausea,
appetite loss and vomiting. Cryptosporidium oocysts in recre-
ational water represents a public health concern, consid-
ering, its high inherent risks and persistence in the water
environment (Rose et al., 2002). In recent years QMRAs have
been undertaken for recreational waters (Ashbolt et al., 2010;
Roser et al., 2006), however for drinking water, the proba-
bility of infection is estimated in addition the probability of
illness so as to develop a conservative public health
approach, by using probability of infection, thereby
addressing the initial state of the disease process capturing
all possible outcomes (Regli et al., 1991). Modeling the risk of
infection is also beneficial when considering the more severe
outcomes groups with greater susceptibility such as children
can incur. Typically a conditional dose response model that
estimates the probability of illness given the probability of
infection, however this is not possible for Cryptosporidium
(Teunis et al., 1999). Despite the inability to apply a condi-
tional probability of illness, a probability of illness given
infection can be developed using the morbidity ratio (illness
given infection) recommended by the United States Envi-
ronmental Protection Agency (EPA) (US EPA, 2006a). There-
fore this work examines both the probability of infection and
probability of illness to recreational users of the spraypark
using both infection and illness for evaluation of risk
reduction potential.
1.3. Outbreak description
As discussed earlier this work is based on an outbreak at
a recreational spraypark. Themain attraction at the spraypark
as with most recreational sites of this type is the spraypad.
The spraypad is a large concrete surface, in this case in the
shape of an oval. The spraypad has numerous water spray
attractions that children play with and around. This location
was determined the primary site of exposure by the New York
State Department of Health (NYSDOH). In order to charac-
terize the outbreak better a case control study and a cohort
study were performed by the NYSDOH. The case control study
was used to describe the overall outbreak; and the data from
the cohort study were used to determine the attack rates to
the spraypark users.
In August 2005, the NYSDOHwas notified of an outbreak of
gastrointestinal illness associated with attending this spray-
park facility. The attendance in August 2005, the time frame of
the outbreak, was approximately 30,000 people.
A total of 746 people reported gastrointestinal (GI) symp-
toms, of these; five were hospitalized, with no deaths re-
ported. The reported symptoms were as follows: diarrhea,
nausea, abdominal cramps, vomiting, fever and appetite loss.
The types of cases were defined as follows:
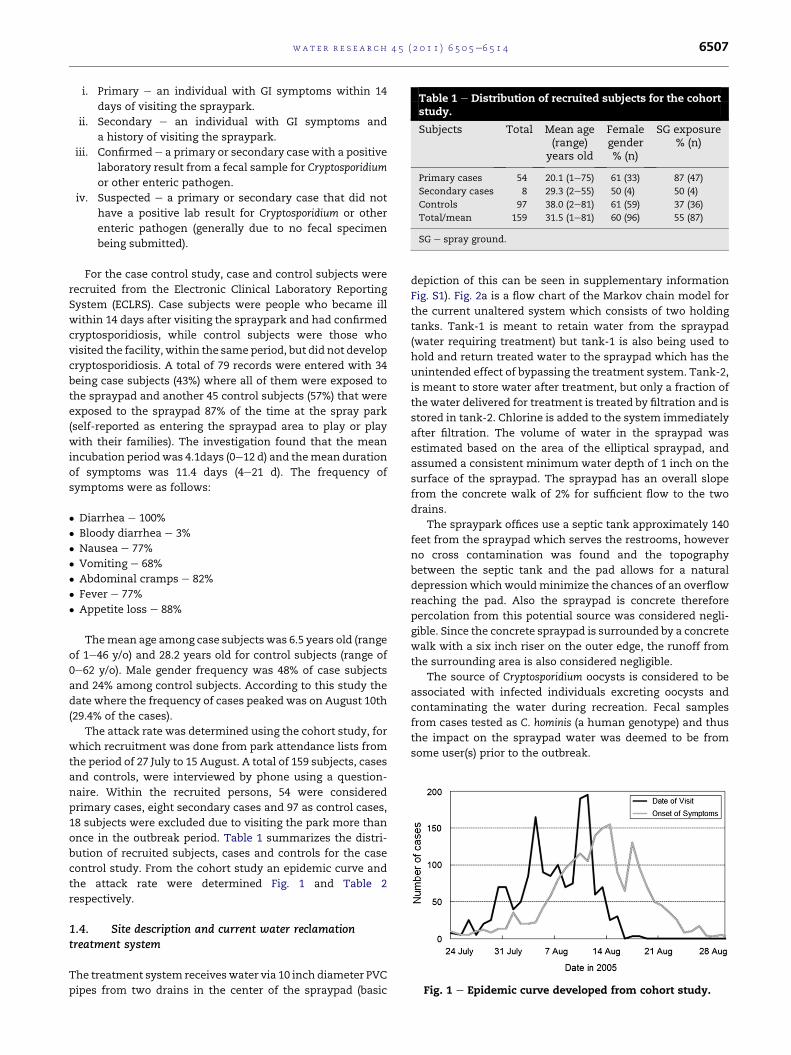
Table 1 e Distribution of recruited subjects for the cohortstudy.
Subjects Total Mean age(range)
years old
Femalegender% (n)
SG exposure% (n)
Primary cases 54 20.1 (1e75) 61 (33) 87 (47)
Secondary cases 8 29.3 (2e55) 50 (4) 50 (4)
Controls 97 38.0 (2e81) 61 (59) 37 (36)
Total/mean 159 31.5 (1e81) 60 (96) 55 (87)
SG e spray ground.
Fig. 1 e Epidemic curve developed from cohort study.
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 4 6507
i. Primary e an individual with GI symptoms within 14
days of visiting the spraypark.
ii. Secondary e an individual with GI symptoms and
a history of visiting the spraypark.
iii. Confirmede a primary or secondary case with a positive
laboratory result from a fecal sample for Cryptosporidium
or other enteric pathogen.
iv. Suspected e a primary or secondary case that did not
have a positive lab result for Cryptosporidium or other
enteric pathogen (generally due to no fecal specimen
being submitted).
For the case control study, case and control subjects were
recruited from the Electronic Clinical Laboratory Reporting
System (ECLRS). Case subjects were people who became ill
within 14 days after visiting the spraypark and had confirmed
cryptosporidiosis, while control subjects were those who
visited the facility, within the same period, but did not develop
cryptosporidiosis. A total of 79 records were entered with 34
being case subjects (43%) where all of them were exposed to
the spraypad and another 45 control subjects (57%) that were
exposed to the spraypad 87% of the time at the spray park
(self-reported as entering the spraypad area to play or play
with their families). The investigation found that the mean
incubation periodwas 4.1days (0e12 d) and themean duration
of symptoms was 11.4 days (4e21 d). The frequency of
symptoms were as follows:
� Diarrhea e 100%
� Bloody diarrhea e 3%
� Nausea e 77%
� Vomiting e 68%
� Abdominal cramps e 82%
� Fever e 77%
� Appetite loss e 88%
Themean age among case subjects was 6.5 years old (range
of 1e46 y/o) and 28.2 years old for control subjects (range of
0e62 y/o). Male gender frequency was 48% of case subjects
and 24% among control subjects. According to this study the
date where the frequency of cases peaked was on August 10th
(29.4% of the cases).
The attack rate was determined using the cohort study, for
which recruitment was done from park attendance lists from
the period of 27 July to 15 August. A total of 159 subjects, cases
and controls, were interviewed by phone using a question-
naire. Within the recruited persons, 54 were considered
primary cases, eight secondary cases and 97 as control cases,
18 subjects were excluded due to visiting the park more than
once in the outbreak period. Table 1 summarizes the distri-
bution of recruited subjects, cases and controls for the case
control study. From the cohort study an epidemic curve and
the attack rate were determined Fig. 1 and Table 2
respectively.
1.4. Site description and current water reclamationtreatment system
The treatment system receiveswater via 10 inch diameter PVC
pipes from two drains in the center of the spraypad (basic
depiction of this can be seen in supplementary information
Fig. S1). Fig. 2a is a flow chart of the Markov chain model for
the current unaltered system which consists of two holding
tanks. Tank-1 is meant to retain water from the spraypad
(water requiring treatment) but tank-1 is also being used to
hold and return treated water to the spraypad which has the
unintended effect of bypassing the treatment system. Tank-2,
is meant to store water after treatment, but only a fraction of
the water delivered for treatment is treated by filtration and is
stored in tank-2. Chlorine is added to the system immediately
after filtration. The volume of water in the spraypad was
estimated based on the area of the elliptical spraypad, and
assumed a consistent minimum water depth of 1 inch on the
surface of the spraypad. The spraypad has an overall slope
from the concrete walk of 2% for sufficient flow to the two
drains.
The spraypark offices use a septic tank approximately 140
feet from the spraypad which serves the restrooms, however
no cross contamination was found and the topography
between the septic tank and the pad allows for a natural
depressionwhich wouldminimize the chances of an overflow
reaching the pad. Also the spraypad is concrete therefore
percolation from this potential source was considered negli-
gible. Since the concrete spraypad is surrounded by a concrete
walk with a six inch riser on the outer edge, the runoff from
the surrounding area is also considered negligible.
The source of Cryptosporidium oocysts is considered to be
associated with infected individuals excreting oocysts and
contaminating the water during recreation. Fecal samples
from cases tested as C. hominis (a human genotype) and thus
the impact on the spraypad water was deemed to be from
some user(s) prior to the outbreak.
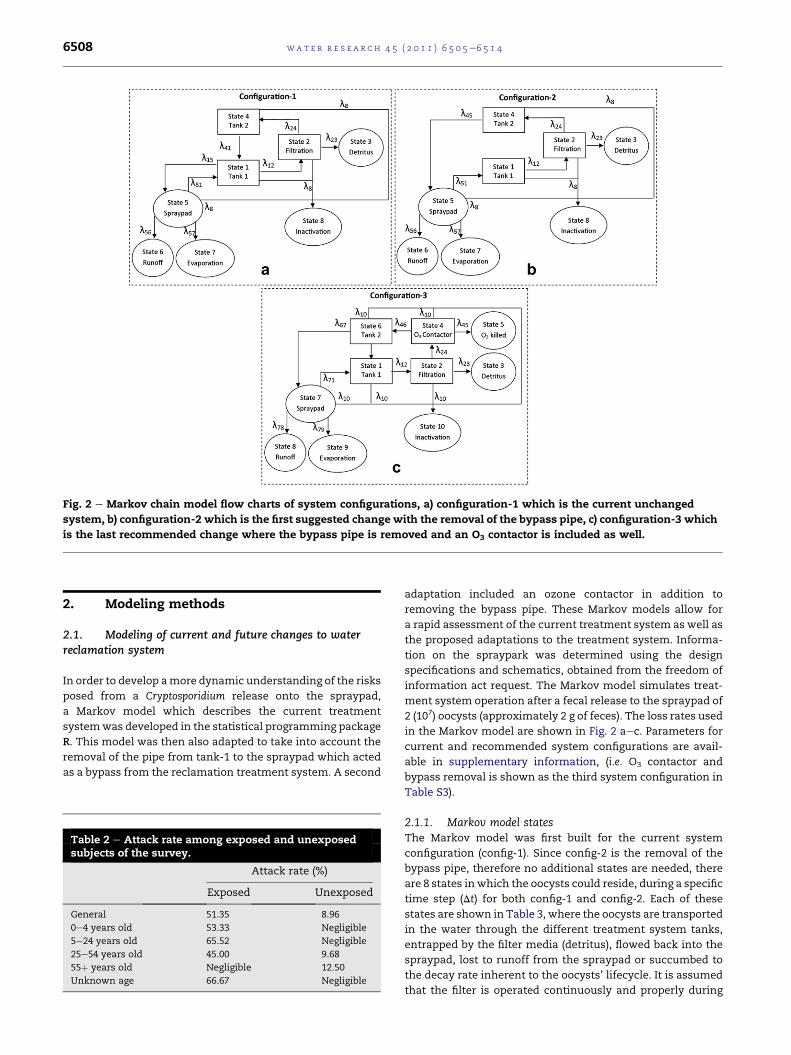
Fig. 2 e Markov chain model flow charts of system configurations, a) configuration-1 which is the current unchanged
system, b) configuration-2 which is the first suggested change with the removal of the bypass pipe, c) configuration-3 which
is the last recommended change where the bypass pipe is removed and an O3 contactor is included as well.
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 46508
2. Modeling methods
2.1. Modeling of current and future changes to waterreclamation system
In order to develop amore dynamic understanding of the risks
posed from a Cryptosporidium release onto the spraypad,
a Markov model which describes the current treatment
systemwas developed in the statistical programming package
R. This model was then also adapted to take into account the
removal of the pipe from tank-1 to the spraypad which acted
as a bypass from the reclamation treatment system. A second
Table 2 e Attack rate among exposed and unexposedsubjects of the survey.
Attack rate (%)
Exposed Unexposed
General 51.35 8.96
0e4 years old 53.33 Negligible
5e24 years old 65.52 Negligible
25e54 years old 45.00 9.68
55þ years old Negligible 12.50
Unknown age 66.67 Negligible
adaptation included an ozone contactor in addition to
removing the bypass pipe. These Markov models allow for
a rapid assessment of the current treatment system as well as
the proposed adaptations to the treatment system. Informa-
tion on the spraypark was determined using the design
specifications and schematics, obtained from the freedom of
information act request. The Markov model simulates treat-
ment system operation after a fecal release to the spraypad of
2 (107) oocysts (approximately 2 g of feces). The loss rates used
in the Markov model are shown in Fig. 2 aec. Parameters for
current and recommended system configurations are avail-
able in supplementary information, (i.e. O3 contactor and
bypass removal is shown as the third system configuration in
Table S3).
2.1.1. Markov model statesThe Markov model was first built for the current system
configuration (config-1). Since config-2 is the removal of the
bypass pipe, therefore no additional states are needed, there
are 8 states inwhich the oocysts could reside, during a specific
time step (Dt) for both config-1 and config-2. Each of these
states are shown in Table 3, where the oocysts are transported
in the water through the different treatment system tanks,
entrapped by the filter media (detritus), flowed back into the
spraypad, lost to runoff from the spraypad or succumbed to
the decay rate inherent to the oocysts’ lifecycle. It is assumed
that the filter is operated continuously and properly during

Table 3 e State numbers for treatment system all threeconfigurations (current system configuration andremoval of bypass and removal of bypass with O3
contactor included).
Configurations 1 and 2 Configuration 3
Statenumber
Systemlocation
Statenumber
Systemlocation
State 1 Tank 1 State 1 Tank 1
State 2 Filtration system State 2 Filtration system
State 3 Detritus from filter State 3 Detritus from filter
State 4 Tank 2 State 4 O3 contactor
State 5 Spraypad surface State 5 Cysts inactivated by O3
State 6 Water lost to runoff State 6 Tank 2
State 7 Water lost to
evaporation
State 7 Spraypad surface
State 8 Oocyst death State 8 Water lost to runoff
State 9 Water lost to
evaporation
State 10 Oocyst death
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 4 6509
the season with a sufficient schmutzdecke developed for
removal of oocysts (Schuler et al., 1991), schmutzdecke being
the complex biological layer formed at the top of a filter,
essentially the main treatment layer of the filter.
In config-3 an O3 contactor is included in the original
treatment train, along with the removal of the bypass pipe as
was done in config-2. Therefore there are 10 states for config-3
(Table 3). Inactivation of the oocysts by O3 was accounted for
as an additional loss mechanism removing oocysts. For all
three configurations inactivation due to chlorine is considered
negligible due to the resistance of Cryptosporidium to chlorine.
2.1.2. Transition probabilities and loss ratesThe term pij is the probability that oocysts in state i will move
to state j during time step Dt. The overall rate at which oocysts
are transported from state i is determined with the sum of the
loss rates for removal from state i, denoted with li. Thus the
probability that oocysts will remain in state i ( pii) within the
time step (Dt), is determined with an exponential survival
probability as seen in equation (1) (Nicas and Sun, 2006; Ross,
2007).
pii ¼ expð�li$DtÞ (1)
In turn the probability of oocysts moving from state i to state j
(equation (2)) is defined as the loss rate from state i to state j
(lij) divided by the sum of the loss rates from state i (li). This
allows for the determination of the unconditional probability
that the oocysts in state i moved to state j during Dt, which is
the complement of the probability of the oocysts in state i
multiplied by the conditional probability (Nicas and Sun, 2006;
Ross, 2007).
pij ¼lij
li$�1� pii
�(2)
Therefore the loss rates are first determined in order to
complete the transition probabilities. Since the decay rate of
oocysts are in units of time�1, all loss rates are first order as
well.
The three system configurations used are displayed in
Fig. 2aec for config-1, 2 and 3 respectively. As described above
the (l’s) in the figures are the loss rates of oocysts associated
with moving from one state to another.
The oocysts are delivered through the treatment system
with a volumetric flow rate (Q), and the associated losses are
experienced in the volumes (V) of the compartments, repre-
sented by states in theMarkov chain. The volumetric flow rate
from one state to another (i.e. tank-1 to the filtration tank) is
divided by the volume of the current state which determines
the loss of oocysts from the first state (tank-1) during trans-
port to the next state (current state is symbolized by x) as
shown in equation (3). Therefore in the example of moving
from tank-1 to the filtration tank, the current state volume (Vx)
would be that of tank-1.
lx/y ¼ Qx/y=Vx(3)
The oocysts are also lost during the treatment step(s)
(filtration and ozonation), which is driven by the treatment
efficiency (Elmeko, 2003; Hijnen et al., 2004; Mazounie et al.,
2000), again assuming a schmutzdecke presence for filtra-
tion (Schuler et al., 1991). Equation (4) shows a generalization
of oocyst losses due to treatment. This general form is used
for filtration using a treatment efficiency (h), for filtration
obtained from Schuler et al. (1991) and the O3 contactor
inactivation efficiency for a 2 mg/L dose and contact time of
1 min (Corona-Vaszuez et al., 2002). As can be seen in
equation (4), the physical transport through the treatment
step was considered as well as reduction of oocysts in the
water from treatment, this gave an overall reduction as the
water was transported through the treatment options, rep-
resented as states in the Markov chain. In this general form
a represents the current treatment system state that the
oocysts reside in, they then in turn are transported and
treated in state b.
la/b ¼ Qa/b=Va��Qa/b=Va$hb
�(4)
There are three losses considered constant through the
Markov models, being the decay rate as well as runoff and
evaporation from the spraypad. It is estimated by the spray-
parkmanagers that there is typically a 5% loss ofwater per day
from runoff as well as evaporation (first order loss rate of;
0.0000026 h�1). Decay of Cryptosporidium parvum in neutral
water was considered as well, typical value of 0.000363 h�1
from Robertson et al. (1992) and considered constant for the
simulation. The other loss rate functional forms can be seen in
the supplemental information.
2.1.3. Markov matrixThe loss rates described above allow for the determination of
transition probabilities as described in equations (1) and (2).
These transition probabilities are used to build the Markov
matrix, which is the operational component of the Markov
chain model. For config-1 and config-2 an 8 � 8 matrix was is
for the eight states, and config-3 is a 10� 10 matrix represents
the ten states for this configuration. As discussed earlier pij is
the probability that an oocyst in state-i transitions to state-j,

wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 46510
therefore, p12 is the probability of an oocyst in state-1 tran-
sitioning to state-2, and so forth for each row. Therefore each
of the rows represents each of the states andmovement along
the columns of the matrix represents transitioning from that
state to another.
2.1.4. Code and model verification for Markov modelsSince this is a stochastic system, in this case a discrete time
Markov chain is utilized to model the efficacy of the current
and recommended treatment options. Two verification steps
which included general code verification, which is performed
in two steps, first by using an additional researcher uncon-
nected to the project to visually inspect the code, checking for
errors and a line-by-line debugging of the code. Line-by-line
debugging is accomplished by evaluating each of the lines
(or in the case of loops, individual loops) independently, to
confirm that the intended and required result is gained from
executing that line of code (or that loop).
The second type of verification which is possible for this
type of stochastic model is a check of conservation of mass.
This was performed, where 500 oocysts are entered into each
of the compartments of the model individually and the
outputs from the compartments (states) are accounted for, the
sum total of oocysts lost from the states equals the original
amount going in. Therefore using the filter state as an
example the oocysts can be lost due to entrapment as detritus,
lost to decay or flow through the filter and these three loss
mechanisms are the onlymeans of oocysts being lost from the
filter state. This verification test ensures that oocysts are not
being generated in the states. Then a final conservation of
mass verification is performed, where the entire system is
executed (all states, the entire model executed) and conser-
vation of mass is monitored, again where 500 oocyst were
introduced to the systems and each of the pathways account
for the loss of all 500 oocysts, therefore, mass is not created
and only those loss mechanisms for the states are removing
the oocysts from the individual states.
Both of these verification steps were performed and
passed. The external check and debugging of the code passed
andwas verified by the researcher external to this project. The
checks for conservation of mass passed as well, where for
each of the removalmechanisms of themodel, the principle of
conservation of mass held for individual states as well as the
entire model.
2.2. Risk assessment
QMRA is a means of determining the probability of infection
due to exposure to water contaminated with Cryptosporidium
oocysts. The exposure volume was defined using data from
Dufour et al. (2006) as an assumed constant value of 0.108 L/
exposure.
The dose response relationship for probability of infection
(Pi) due to ingestion of Cryptosporidium oocysts was used as
described by the exponential dose response model shown in
equation (5) (Haas et al., 1996). The k parameter used in this
analysis was optimized from human volunteer studies as
recommended in US EPA (2006b), with an optimal value of k
being 0.0907 and bounded on a 95% confidence interval of
0.0074 and 0.3044.
Pi ¼ 1� expð�k$dÞ (5)
If it is desired to estimate the dose from an observed proba-
bility of infection, equation (5) can be rewritten to solve for
dose, since the k parameter is based on human feeding trials
where the observed probability of infection was recorded.
However, since attack rate (AR) was an estimate of the prob-
ability of illness equation (5) will not be as accurate as a dose
response model specific for illness. This could be accom-
plished through a dose responsemodel of probability of illness
conditional on probability of infection. However for Crypto-
sporidium Teunis et al. (1999) in their work developing this type
of conditional dose response model, it was determined that
due to the decreasing trend with dose of the proportion of
infected hosts who became ill such a conditional dose
response model could not be developed. So as to develop
a probability of illness (Pill) via the dose responsemodel which
models probability of infection, the recommended morbidity
ratio (MR) of 0.50 from the US EPA (US EPA, 2006a) is multiplied
by the dose responsemodel in equation (5) (equation (6)). Then
to obtain a dose estimate for the outbreak in question Pill is
substituted with AR after equation (6) is rewritten to solve for
dose (equation (7)).
Pill ¼ ½1� expð�k$doseÞ�$MR (6)
d ¼ ln
��Pill � 1�MR
�.k (7)
The Markov model was executed to simulate 3 h of treatment
system operation after a bolus fecal release of 2(107) oocysts
(approximately 2 g of feces) (Chappell et al., 1996; CDC, 2007).
Thus the scenario being considered is 3 h of spraypad use after
the fecal release. It is assumed that for a trip to the spraypark
which lasts typically five to 6 h that this would give a good
depiction of howmuch the spraypad is used. The Monte Carlo
method models the risks to the users of the spraypad after
a fecal release, using equation (5) to determine the risk of
infection (Pi) from oocyst exposure and equation (6) to esti-
mate the risk of illness (Pill). The Monte Carlo method is
a means of developing a distribution of model results after
repeated random sampling from probability distributions
which describe uncertain variables.
The numerical output of oocyst concentrations from the
Markov models are used to fit probability distributions in
MATLAB for the Monte Carlo model to address the user’s
exposure to oocysts for the QMRA after simulating 3 h of
spraypad use which includes an assumed bolus fecal release
of 2 (107) Cryptosporidium oocysts. The KolmogoroveSmirnov
test statistic was used to determine the goodness of fit for the
distributions. Table 4 shows the probability distributions used
in the Monte Carlo model, which is executed for 10,000 itera-
tions in MATLAB and summarizes the probability distribu-
tions used in this study to estimate the probability of
Cryptosporidium infection (Pi) and illness (Pill) given the
morbidity ratio (US EPA, 2006a). Fitting the probability distri-
butions around the numerical results from the Markov chain
model addresses the first uncertain variable (the concentra-
tion of oocysts for each of the configurations), the second
uncertain variable, the dose response parameter is described
with a triangular distribution, based on the optimal value,

Table 4 e Probability distributions and parameters for the Monte Carlo model.
Uncertainparameter
Scenario Distribution Distribution parameters KolmogrozeSmirnoztest p-value
r unitless NA Triangular 0.00467 (CI95%b: 0.00195; 0.0097) NA, assumed distribution
Cryptosporidium
concentrationa
Filtration w/o bypass
(current system)
Gamma Scale: 7392 0.0061
Shape: 0.432
Cryptosporidium
concentrationa
Filtration w/o bypass Gamma Scale: 6212 0.0075
Shape: 0.442
Cryptosporidium
concentrationa
Filtration þ O3 Gamma Scale: 6110 0.0055
Shape: 0.465
a Data for fitting these distributions from the Markov chain models.
b 95% confidence interval.
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 4 6511
lower and upper 95th confidence intervals of k from the
exponential model fit to human feeding studies (US EPA,
2006a) and the third uncertain variable is MR using a trian-
gular distribution using the likeliest, maximumandminimum
levels (US EPA, 2006b).
The dose for equation (5) is determined by multiplying the
concentration of oocysts sampled from the probability
distributions by the volume of water ingested by spraypad
users.
3. Results
Using equation (7), the likeliest morbidity ratio of 0.5 (US EPA,
2006a) and the attack rates in Table 2, this analysis estimates
that the population was exposed to an average dose of 12
oocysts (95th confidence interval of 4e149 oocysts).
Rather than using the estimated risk levels as a compar-
ison to current standards, considering they are associated
with highly credible gastrointestinal illness (HCGI) the overall
risk reductions were highlighted. It can be surmised
however, that since attractions like these are targeted toward
children a very low risk of infection or illness, given their
greater susceptibility, would be considered acceptable by
parents and park owners, however no known studies have
highlighted what acceptable risks might be for such
waterparks.
Fig. 3a and d shows the Monte Carlo simulation results for
Pi and Pill respectively to the population exposed to water
contaminated with Cryptosporidium oocysts with the current
treatment system (config-1). An overall risk to the exposed
population is bimodal and skewed slightly to the higher risk
levels with a low probability of experiencing an infection risk
of less than 0.10 (approximately 18% chance). Infection risks
equal to or greater than 0.9 did occur with a 60% probability
of occurrence, for Cryptosporidium. There is also a 15%
probability of incurring a probability of illness of 0e0.025,
and a 60% probability of incurring a probability of illness of
0.5. This demonstrates the untenable original configuration
with respect to Cryptosporidium risks with respect to the
original configuration. This is attributed to the percentage of
water that received no treatment via the bypass of the filter.
These risk estimates do not include risks from other patho-
gens since risk from Cryptosporidium is being highlighted
here.
When the bypass was eliminated from the water recla-
mation system and all the water was filtered, the overall risk
levels were reduced, Fig. 3b and e for showing Pi and Pillrespectively for config-2. As can be seen there is a 30% prob-
ability of experiencing an infection risk within the range of
0.00e0.01. The high risk level (>w0.9 for infection and >w0.35
for illness) was then reduced to a 44% probability of occurring.
When removing the bypass and including an O3 contactor
(Fig. 3c and f for Pi and Pill respectively for config-3), there was
approximately a 37% probability of the risk being at or less
than 0.01 for infection and 0.025 for illness and a 32% proba-
bility of experiencing a high risk of greater than 0.9 or 0.5 for Piand Pill respectively.
A sensitivity analysis is performed to determine which
uncertain variable is driving the risk. In all conditions
assessed, the greatest contributor to the risk for the exposed
population is the concentration of oocysts (Fig. 4a and b for
illness and infection respectively). The sensitivity analyses for
the other configurations were essentially the same, showing
the concentration of oocysts being the primary contributor to
the estimated risk and associated uncertainty. Thus it can be
recommended that at minimum the removal of the bypass
pipe would be necessary to reduce the risks associated with
waterborne disease. While inclusion of the ozone contactor
reduced the risks further and to an even greater degree from
the unaltered configuration, this was not as a sufficiently
appreciable risk reduction from the simpler retrofit (configu-
ration 2) and may not be justified with the higher costs from
both installation and operation associated with the third
configuration.
4. Discussion
This study addressed an important public health problem,
recreational waterborne disease. Swimming venues that use
chlorine are now known to be at risk from Cryptosporidium
and filtration or other types of disinfection including UV or
ozone are needed to control the parasite. According to the
CDC, recreational illnesses are on the rise. Between 2005 and
2006, 78 outbreaks were reported in 31 states, which is the
largest number of outbreaks ever in a two-year period with
4500 people affected (CDC, 2008). There are over 1000
waterpark facilities in North America (city pools with
waterpark features, independently-owned outdoor and
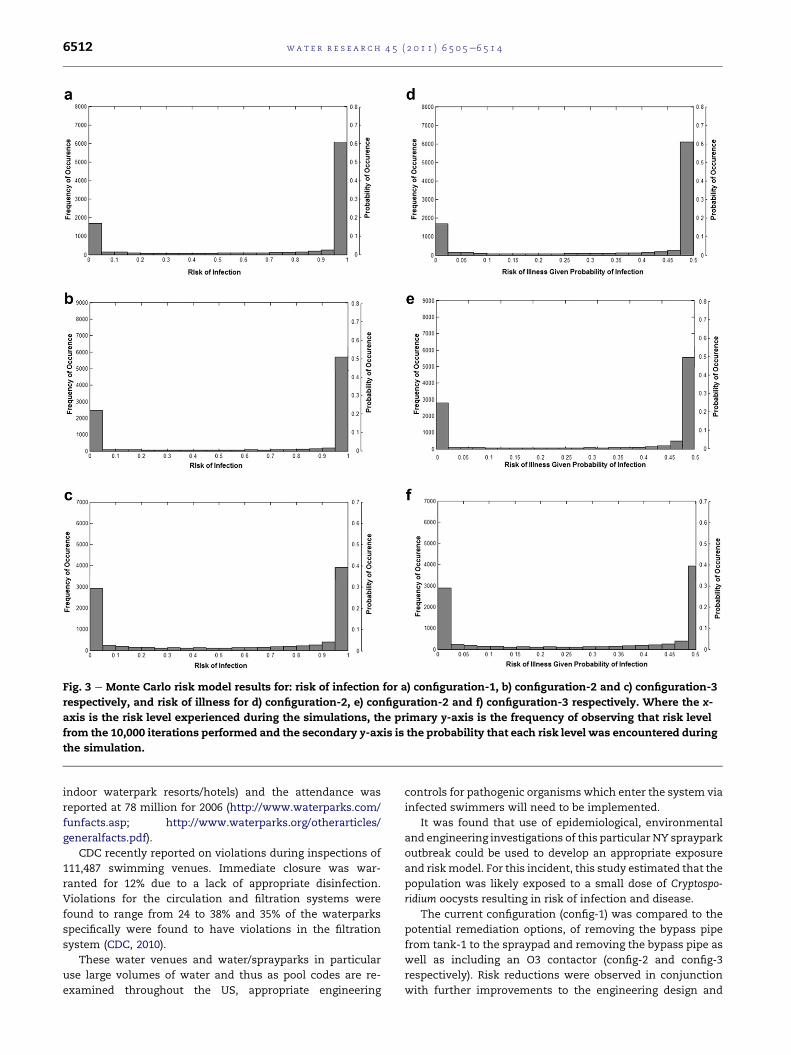
Fig. 3 e Monte Carlo risk model results for: risk of infection for a) configuration-1, b) configuration-2 and c) configuration-3
respectively, and risk of illness for d) configuration-2, e) configuration-2 and f) configuration-3 respectively. Where the x-
axis is the risk level experienced during the simulations, the primary y-axis is the frequency of observing that risk level
from the 10,000 iterations performed and the secondary y-axis is the probability that each risk level was encountered during
the simulation.
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 46512
indoor waterpark resorts/hotels) and the attendance was
reported at 78 million for 2006 (http://www.waterparks.com/
funfacts.asp; http://www.waterparks.org/otherarticles/
generalfacts.pdf).
CDC recently reported on violations during inspections of
111,487 swimming venues. Immediate closure was war-
ranted for 12% due to a lack of appropriate disinfection.
Violations for the circulation and filtration systems were
found to range from 24 to 38% and 35% of the waterparks
specifically were found to have violations in the filtration
system (CDC, 2010).
These water venues and water/sprayparks in particular
use large volumes of water and thus as pool codes are re-
examined throughout the US, appropriate engineering
controls for pathogenic organisms which enter the system via
infected swimmers will need to be implemented.
It was found that use of epidemiological, environmental
and engineering investigations of this particular NY spraypark
outbreak could be used to develop an appropriate exposure
and riskmodel. For this incident, this study estimated that the
population was likely exposed to a small dose of Cryptospo-
ridium oocysts resulting in risk of infection and disease.
The current configuration (config-1) was compared to the
potential remediation options, of removing the bypass pipe
from tank-1 to the spraypad and removing the bypass pipe as
well as including an O3 contactor (config-2 and config-3
respectively). Risk reductions were observed in conjunction
with further improvements to the engineering design and
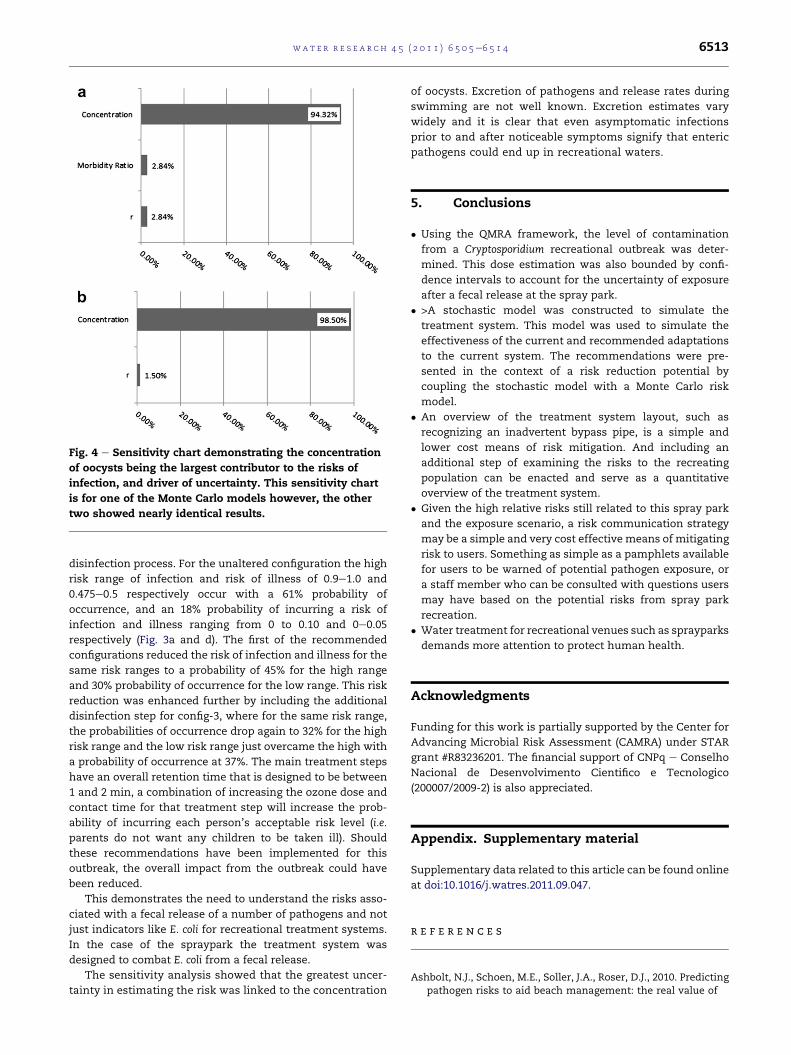
Fig. 4 e Sensitivity chart demonstrating the concentration
of oocysts being the largest contributor to the risks of
infection, and driver of uncertainty. This sensitivity chart
is for one of the Monte Carlo models however, the other
two showed nearly identical results.
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 4 6513
disinfection process. For the unaltered configuration the high
risk range of infection and risk of illness of 0.9e1.0 and
0.475e0.5 respectively occur with a 61% probability of
occurrence, and an 18% probability of incurring a risk of
infection and illness ranging from 0 to 0.10 and 0e0.05
respectively (Fig. 3a and d). The first of the recommended
configurations reduced the risk of infection and illness for the
same risk ranges to a probability of 45% for the high range
and 30% probability of occurrence for the low range. This risk
reduction was enhanced further by including the additional
disinfection step for config-3, where for the same risk range,
the probabilities of occurrence drop again to 32% for the high
risk range and the low risk range just overcame the high with
a probability of occurrence at 37%. The main treatment steps
have an overall retention time that is designed to be between
1 and 2 min, a combination of increasing the ozone dose and
contact time for that treatment step will increase the prob-
ability of incurring each person’s acceptable risk level (i.e.
parents do not want any children to be taken ill). Should
these recommendations have been implemented for this
outbreak, the overall impact from the outbreak could have
been reduced.
This demonstrates the need to understand the risks asso-
ciated with a fecal release of a number of pathogens and not
just indicators like E. coli for recreational treatment systems.
In the case of the spraypark the treatment system was
designed to combat E. coli from a fecal release.
The sensitivity analysis showed that the greatest uncer-
tainty in estimating the risk was linked to the concentration
of oocysts. Excretion of pathogens and release rates during
swimming are not well known. Excretion estimates vary
widely and it is clear that even asymptomatic infections
prior to and after noticeable symptoms signify that enteric
pathogens could end up in recreational waters.
5. Conclusions
� Using the QMRA framework, the level of contamination
from a Cryptosporidium recreational outbreak was deter-
mined. This dose estimation was also bounded by confi-
dence intervals to account for the uncertainty of exposure
after a fecal release at the spray park.
� >A stochastic model was constructed to simulate the
treatment system. This model was used to simulate the
effectiveness of the current and recommended adaptations
to the current system. The recommendations were pre-
sented in the context of a risk reduction potential by
coupling the stochastic model with a Monte Carlo risk
model.
� An overview of the treatment system layout, such as
recognizing an inadvertent bypass pipe, is a simple and
lower cost means of risk mitigation. And including an
additional step of examining the risks to the recreating
population can be enacted and serve as a quantitative
overview of the treatment system.
� Given the high relative risks still related to this spray park
and the exposure scenario, a risk communication strategy
may be a simple and very cost effective means of mitigating
risk to users. Something as simple as a pamphlets available
for users to be warned of potential pathogen exposure, or
a staff member who can be consulted with questions users
may have based on the potential risks from spray park
recreation.
� Water treatment for recreational venues such as sprayparks
demands more attention to protect human health.
Acknowledgments
Funding for this work is partially supported by the Center for
Advancing Microbial Risk Assessment (CAMRA) under STAR
grant #R83236201. The financial support of CNPq e Conselho
Nacional de Desenvolvimento Cientifico e Tecnologico
(200007/2009-2) is also appreciated.
Appendix. Supplementary material
Supplementary data related to this article can be found online
at doi:10.1016/j.watres.2011.09.047.
r e f e r e n c e s
Ashbolt, N.J., Schoen, M.E., Soller, J.A., Roser, D.J., 2010. Predictingpathogen risks to aid beach management: the real value of
wat e r r e s e a r c h 4 5 ( 2 0 1 1 ) 6 5 0 5e6 5 1 46514
quantitative microbial risk assessment (QMRA). WaterResearch 44, 4692e4703.
Carey, C.M., Lee, H., Trevors, J.T., 2004. Biology, persistence anddetection of Cryptosporidium parvum and Cryptosporidiumhominis oocyst. Water Research 38, 818e862.
Causer, L.M., Handzel, T., Welch, P., Carr, M., Culp, D., Lucht, R.,Mudahar,K., Robinson,D.,Neavar, E., Fenton,S., Rose,C., Craig,L.,Arrowood,M.,Wahlquist, S.,Xiao,L., Lee,Y.-M.,Mirel, L., Levy,D., Beach, M.J., Poquete, G., Dworkin, M.S., 2006. An outbreak ofCryptosporidium hominis infection at an Illinois recreationalwaterpark. Epidemiology and Infection 134, 147e156.
Chappell, C.L., Okhuysen, P.C., Sterling, C.R., DuPont, H.L., 1996.Cryptosporidium parvum: intensity of infection and oocystexcretion patterns in healthy volunteers. Journal of InfectiousDiseases 173, 232e236.
CDC-Centers for Disease Control and Prevention, 2007.2003e2005. Morbidity and Mortality Weekly ReportSurveillance Summaries 56 (SS-07), 1e10.
CDC-Centers for Disease Control and Prevention, 2008.Surveillance for waterborne disease and outbreaks associatedwith recreational water use and other aquatic facility-associated health events e United States, 2005e2006.Morbidity and Mortality Weekly Report 57 (SS-09), 1e70.
CDC-Centers for Disease Control and Prevention, May 21, 2010.Violations identified from routine swimming pool inspectionsd selected states and counties, United States, 2008. Morbidityand Mortality Weekly Report 59 (No. 19), 582e587.
Corona-Vaszuez, B., Samuelson, A., Rennecker, J.L., Marinas, B.J.,2002. Inactivation of Cryptosporidium parvum oocysts withozone and free chlorine. Water Research 36, 4053e4063.
Dufour, A.P., Evans, O., Behymer, T.D., Cantu, R., 2006. Wateringestion during swimming activities in a pool: a pilot study.Journal of Water and Health 04 (4), 425e430.
Elmeko, M.B., 2003. Removal of viable and inactivatedCryptosporidium by dual- and tri-media filtration. WaterResearch 37, 2998e3008.
Haas, C.N., Crockett, C.S., Rose, J.B., Gerba, C.P., Fazil, A.M., 1996.Assessing the risk posed by oocysts in drinking water. Journalof American Water Works Association 88 (9), 131e136.
Haas, C.N., Rose, J.B., Gerba, C.P., 1999. Quantitative MicrobialRisk Assessment. John Wiley and Sons, New York, NY.
Hijnen, W.A.M., Schijven, J.F., Bonne, P., Visser, A., Medema, G.J.,2004. Elimination of viruses, bacteria and protozoan oocystsby slow sand filtration. Water Science and Technology 50 (1),147e154.
Mazounie, P., Bernozeau, F., Alla, P., 2000. Removal ofcryptosporidiosis by high rate contact filtration: the
performance of the prospect water filtration plant during theSydney water crisis. Water Science and Technology 41 (7),93e101.
Nicas, M., Sun, G., 2006. An integrated model of infection riskin a health-care environment. Risk Analysis 26 (4),1085e1096.
Regli, S., Rose, J.B., Haas, C.N., Ferba, C.P., 1991. Modeling the riskfrom Giardia and viruses in drinking water. Journal ofAmerican Water Works Association 83 (11), 76e84.
Robertson, L.J., Campbell, A.T., Smith, H.V., 1992. Survival ofCryptosporidium parvum oocysts under various environmentalpressures. Applied Environmental Microbiology 58 (11),3494e3500.
Rose, J.B., Huffman, D.E., Gennacaro, A., 2002. Risk a control ofwaterborne cryptosporidiosis. FEMS Microbiology Review 26,113e123.
Roser, D.J., Davies, C.M., Ashbolt, N.J., Morison, P., 2006. Microbialexposure assessment of an urban recreational lake: a casestudy of the application of new risk-based guidelines. WaterScience and Technology 54 (3), 245e252.
Ross, S.M., 2007. Introduction to Probability Models. AcademicPress, Burlington, MA.
Schuler, P.F., Ghosh, M.M., Gopalan, P., 1991. Slow sanddiatomaceous earth filtration of cysts and other particulates.Water Research 25 (8), 995e1005.
Smith, H.V., Rose, J.B., 1998. Waterborne cryptosporidiosis:current status. Parasitology Today 14 (1), 14e22.
Teunis, P.F., Nagelkerke, N.J., Haas, C.N., 1999. Dose-responsemodels for infectious gastroenteritis. Risk Analysis 19,1251e1260.
US EPA Office of Water, 2006a. Economic Analysis for the FinalLong Term 2 Enhanced Surface Water Treatment Rule EPA815-R-06-001.
US EPA Office of Water, 2006b. EPA 815-R-06-001. Appendices tothe Economic Analysis for the Final Long Term 2 EnhancedSurface Water Treatment Rule, vol. II (H e U).
Wheeler, C., Vugia, D.J., Thomas, G., Beach, M.J., Carnes, S.,Maier, T., Gorman, J., Xiao, L., Arrowood, M.J., Gilliss, D.,Werner, S.B., 2007. Outbreak of cryptosporidiosis at a Californiawaterpark: employee and patron roles and the long roadtowards prevention. Epidemiology and Infection 135, 302e310.
WHO e World Health Organization, 2002. Guidelines for drinking-water quality. In: Addendum Microbiological Agents inDrinking-water, second ed. WHO, Geneva.
WHO eWorld Health Organization, 2006. Guidelines for Drinking-water Quality. First Addendum to 3rd ed. Vol. 1 e
Recommendations. WHO, Geneva.