WATER AND ELECTROLYTES DISTURBANCES
71
WATER AND ELECTROLYTES DISTURBANCES niversity of Medicine and Pharmacy, Iasi chool of Medicine NESTHESIA and INTENSIVE CARE onf. Dr. Ioana Grigoras MEDICINE 4 th year English Program Suport de curs
description
University of Medicine and Pharmacy, Iasi School of Medicine ANESTHESIA and INTENSIVE CARE Conf. Dr. Ioana Grigoras. MEDICINE 4 th year English Program Suport de curs. WATER AND ELECTROLYTES DISTURBANCES. PHYSIOLOGY. Body water = 55-60% of body weight Water distribution : - PowerPoint PPT Presentation
Transcript of WATER AND ELECTROLYTES DISTURBANCES
WATER AND ELECTROLYTES DISTURBANCES
University of Medicine and Pharmacy, IasiSchool of MedicineANESTHESIA and INTENSIVE CAREConf. Dr. Ioana Grigoras
MEDICINE4th year
English ProgramSuport de curs
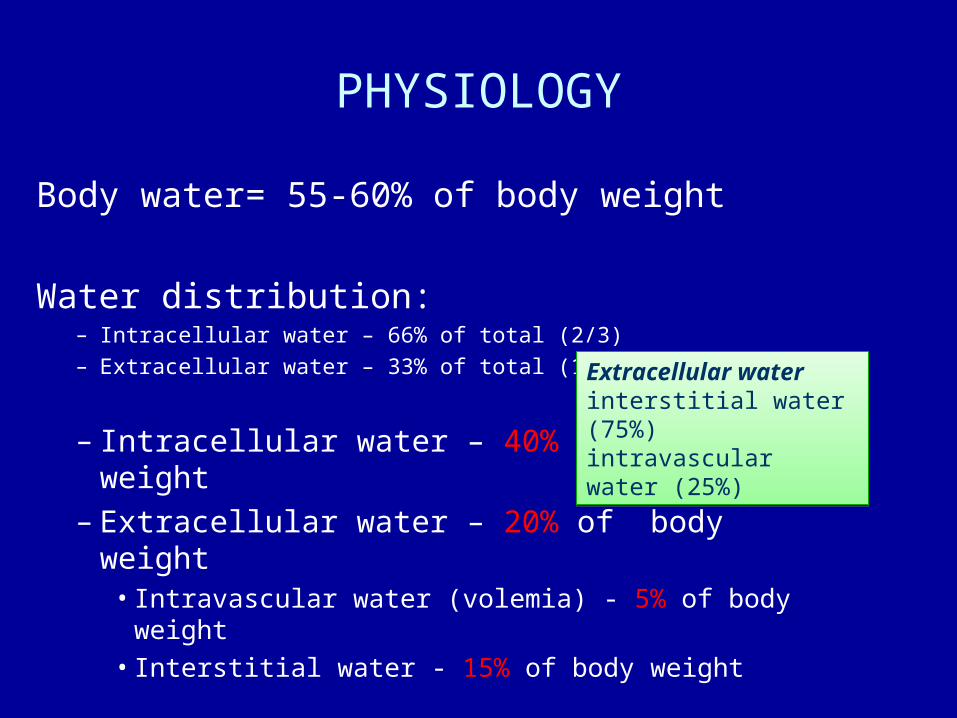
PHYSIOLOGY
Body water= 55-60% of body weight
Water distribution:– Intracellular water – 66% of total (2/3)
– Extracellular water – 33% of total (1/3)
– Intracellular water – 40% of body weight– Extracellular water – 20% of body weight
• Intravascular water (volemia) - 5% of body weight
• Interstitial water - 15% of body weight
Extracellular water interstitial water (75%) intravascular water (25%)
Extracellular water interstitial water (75%) intravascular water (25%)


WATER DISTRIBUTION Variation according to gender
Total Body Water = 0.6 x (kg body weight) - for malesTotal Body Water= 0.5 x (kg body weight) - for females Total Body Water = 0.6 x (kg body weight) - for malesTotal Body Water= 0.5 x (kg body weight) - for females
newborns have the highest percentage of water (75%); older persons and females have relatively less water. newborns have the highest percentage of water (75%); older persons and females have relatively less water.
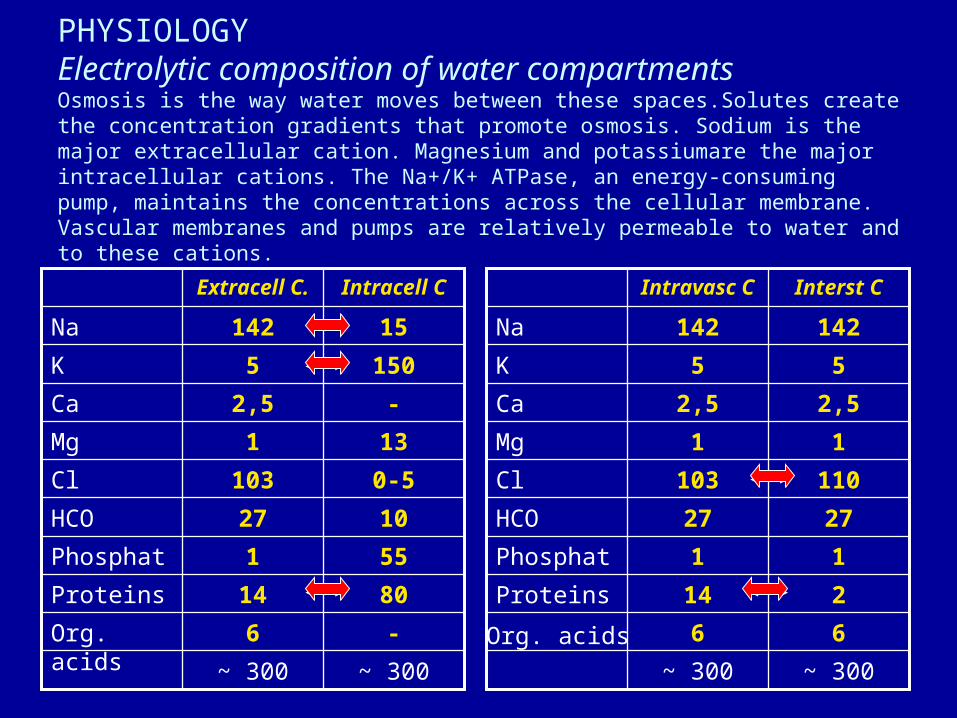
PHYSIOLOGY Electrolytic composition of water compartmentsOsmosis is the way water moves between these spaces.Solutes create the concentration gradients that promote osmosis. Sodium is the major extracellular cation. Magnesium and potassiumare the major intracellular cations. The Na+/K+ ATPase, an energy-consuming pump, maintains the concentrations across the cellular membrane. Vascular membranes and pumps are relatively permeable to water and to these cations.
~ 300~ 300
66
214Proteins
11Phosphat
2727HCO
110103Cl
11Mg
2,52,5Ca
55K
142142Na
Interst CIntravasc C
~ 300~ 300
-6Org. acids
8014Proteins
551Phosphat
1027HCO
0-5103Cl
131Mg
-2,5Ca
1505K
15142Na
Intracell CExtracell C.
Org. acids
WATER AND ELECTROLYTES BALANCE Evaluation
CLINICAL EVALUATION :– History
• Water and salt ingestion• Losses• Thurst
– Skin and mucous membranes examination • Oral mucosae humidity• Skin humidity• Skin colour and temperature• Cutaneous turgor
– Body weight– Respiratory system clinical exam
• Polypneea• Crackles at lung bases
– Clinical examination of peripheral veins– Haemodynamic parameters
• Arterial blood pressure • Pulse wave amplitude• Orthostatic challenge• CVP,...
– Urinary outflow– Evaluation of the counscience level

Clinical evaluation of
the intravascular compartment:– thurst
– BP, heart rate, orthostatic challenge
– central venous pressure
– pulmonary capillary wedge pressure, cardiac output
– organ function:• conscience
• urinary flow
• tissue perfusion
WATER AND ELECTROLYTES BALANCE
Evaluation

Clinical evaluation of
interstitial space:
unreliable– skin and mucous membrane examination
• colour
• humidity
• turgour
• edema
WATER AND ELECTROLYTES BALANCE
Evaluation
Clinical examination of intracellular compartment:
unreliable
– thurst– mental status disturbances– neurological signs
WATER AND ELECTROLYTES BALANCE
Evaluation
LABORATORY EVALUATION– Hematocrit and total proteins
– Blood and urinary electrolytes measurement
– Blood and urinary osmolarity
– ECG
WATER AND ELECTROLYTES BALANCE
Evaluation

OSMOLARITY• Plasma osmolarity =
the sum contributions of all osmotic active substances
• The main plasma osmotic active substances: Na, glucose, ureea
• Plasma osmolarity– measured osmolarity– estimated (calculated) osmolarity
• Calculated osmolarity = Na-mia x 2 + blood glucose/18 +ureea/2,8
Intracellular volume disturbances are the consequences of
effective osmotic pressure variation

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)

VOLUME CONTRACTION

CLASSIFICATION OF HYPOVOLEMIC SHOCK
Class I Class II Class III Class IV
Blood loss- ml < 750ml 750-1500ml 1500-2000ml >2000ml
Blood loss-% <15% 15-30% 30-40% >40%
Pulse rate <100/min < 100/min 120-140/min >140/min
BP N N
Plus wave amplitude
N
Capillary refill N + + +
Respiratory rate 14-20/min 20-30/min 30-40/min >40/min
Urinary output >30ml/oră Oliguria Oligoanuria Anuria
Mental status Mild anxiety Anxiety Confused Lethargy
PRINCIPLES of TREATMENT• Treatment of causative disease • STOP THE LOSSES• Volume replacement
• Volume replacement– Routes of volume administration
– Solutions for volume replacement
– Rhythm of administration
– Monitorization of volume replacement efficiency
WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
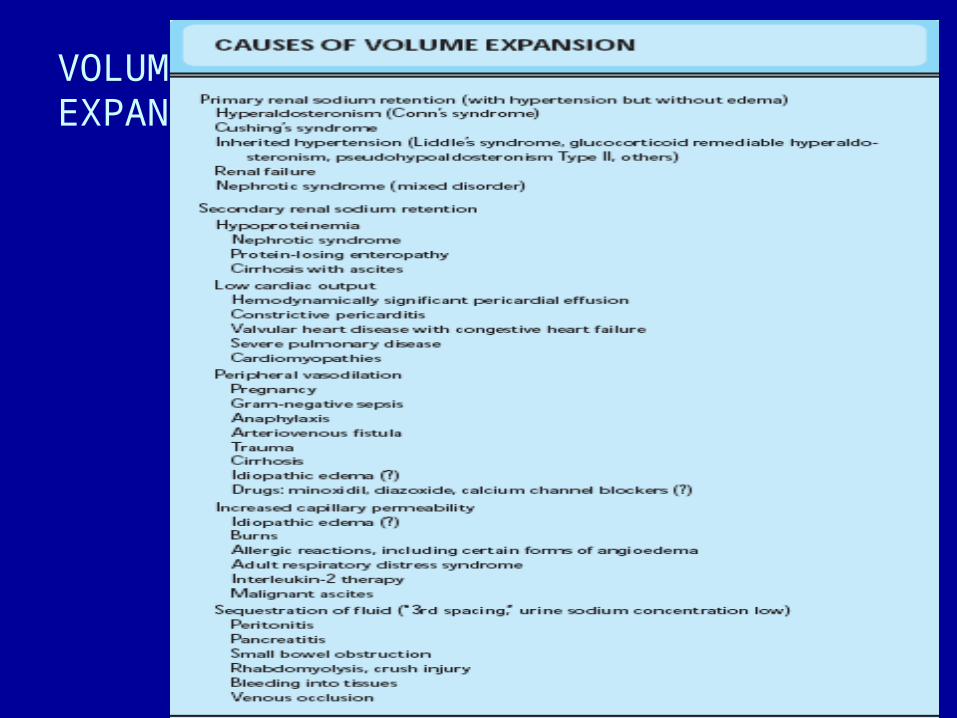
VOLUMEEXPANTION

VOLUME EXPANTION
VOLUME EXPANTION
PRINCIPLES of TREATMENT
• Treatment of causative disease
• Limitation of water intake
• Diuretics

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
SODIUM DISTURBANCES
• Plasma sodium concentration =
extracellular water – sodium ratio
• Na-mia is not a predictor of intravascular volume

SODIUM DISTURBANCES
WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
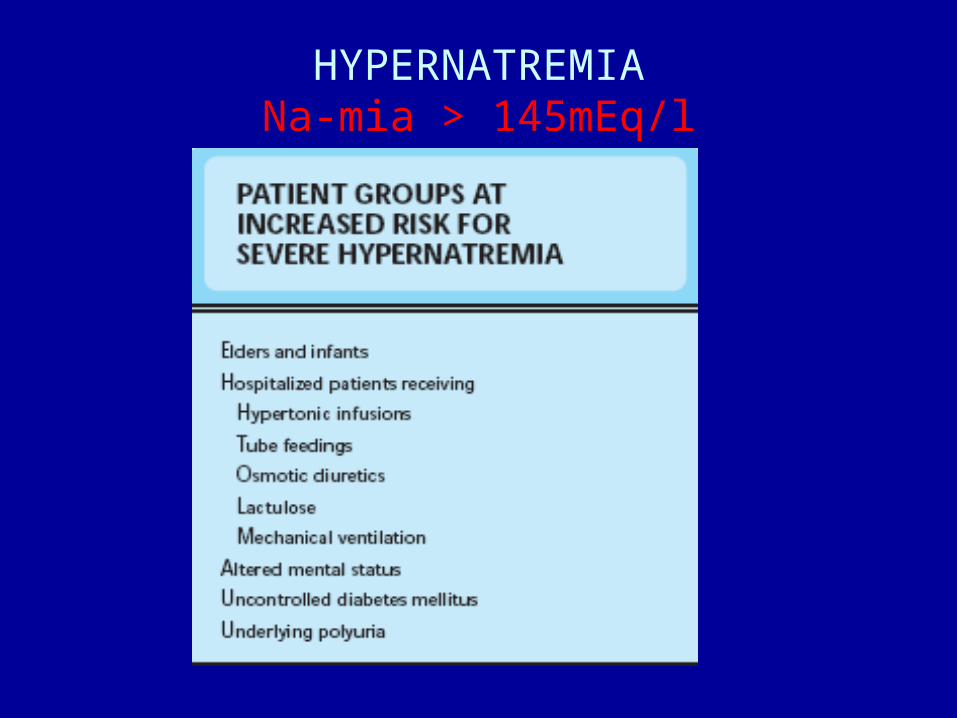
HYPERNATREMIANa-mia > 145mEq/l
• Physiological effects– Extracellular hyperosmolarity– Water movement out of the cell– Preservation of extracellular volume despite losses– Intracellular volume contraction
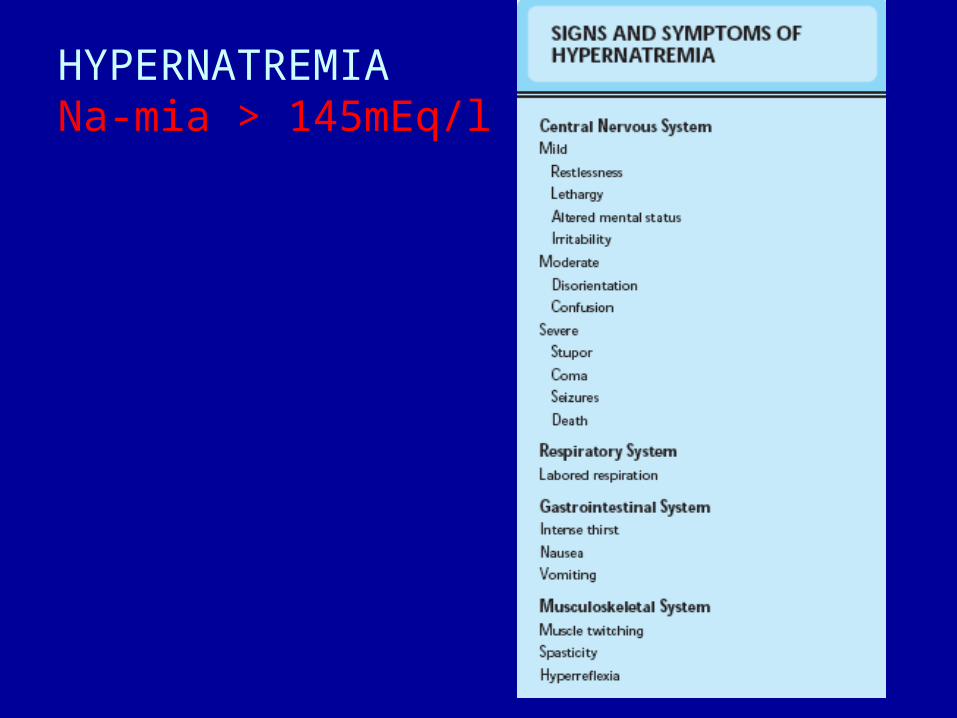
HYPERNATREMIANa-mia > 145mEq/l
HYPERNATREMIANa-mia > 145mEq/l
• Clinical picture– Clinical signs of intracellular volume contraction –
neurological signs– Restlessness, iritability, letargia, hyporeflexia,
coma, convultions– High mortality, neurological sequelae
HYPERNATREMIANa-mia > 145mEq/l

HYPERNATREMIANa-mia > 145mEq/l
• Treatment – Water administration in order to correct
hyperosmolarity– When clinical signs of extracellular volume
contraction (hypovolemia) are present, isotonic solution should be given untill correction of intravascular volume
– Calculation of water deficit0,6 x kg x (Na actual / 140 – 1)
– Speed of correction in chronic hyper Na Na - 0,5-1mEq/hour

HYPERNATREMIANa-mia > 145mEq/l
CLASSIFICATION– HYPOVOLEMIC
• Water and Na deficit• Deficit of water > Na • Body total amount of Na
False hypernatremia– ISOVOLEMIC
• Water deficit • Body total amount of Na - normal
– HYPERVOLEMIC• Water and Na excess• Excess of Na > water • Body total amount of Na ↑
True hypernatremia

HYPOVOLEMIC HYPERNATREMIA Total body Na
MECHANISM- Water and Na deficit; deficit of water > Na; body total amount of Na
CAUSES– Extrarenal losses
• Skin losses (profuse sweating)• Digestive losses (cholera, infant diarrheea)
– Renal losses• osmotic diuresis• excess of diuretics• polyuria
DIAGNOSTIC– Clinical signs of extracellular volume contraction – Na urinary < 10mEq/l – extrarenal losses– Na urinary > 20mEq/l – renal losses
TREATMENT– Water and sodium administrationin isotonic proportions until correction of
hypovolemia; hypotonic solution (NaCl 0,45%)

ISOVOLEMIC HYPERNATREMIA total body Na normal
MECHANISM– water deficit; total body Na normal
CAUSES– Extrarenal losses
• Skin losses (profuse sweating)• Respiratory losses (tachypnea, mechanical ventilation)
– Renal losses • Central diabetes insipidus • Nephrogenic diabetes insipidus • Hypodipsia (decreased water intake)
DIAGNOSTIC– Signs: fever, oliguria, azotemia, drowsiness, coma, convultions– hypotension (late finding)– variable urinary Na
TREATMENT– Increased water intake (NaCl 0,45%,)

ISOVOLEMIC HYPERNATREMIA

ISOVOLEMIC HYPERNATREMIA

HYPERVOLEMIC HYPERNATREMIA total body Na ↑
MECHANISM– water excess; total body Na ↑
CAUSES– excess administration of hypertonic saline (NaCl 7,5%)
– Na bicarbonate administration
– Salt water drowning
DIAGNOSTIC– Signs of extracellular volume expansion
– Signs of intracellular volume contraction
TREATMENT– Diuretics
– Increased water intake

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
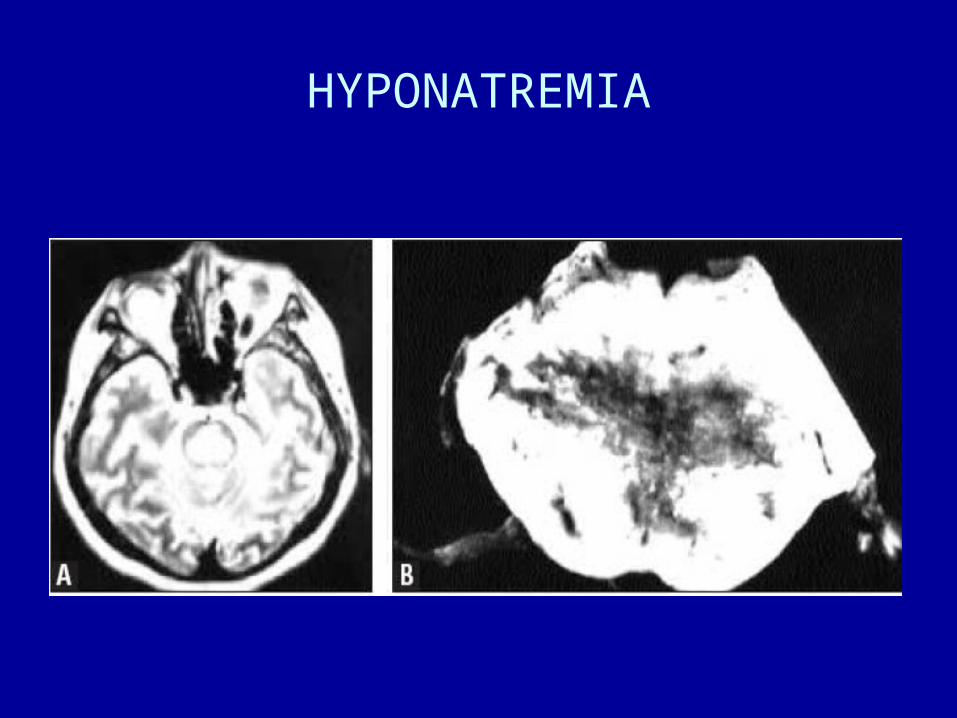
HYPONATREMIANa-mia < 135mEq/l
• Physiological effects– Extracellular hypoosmolarity– Water movement towards the cell– Signs of intracellular volume expansion

HYPONATREMIANa-mia < 135mEq/l
• Clinical picture– Dominated by neurological signs (cerebral edema)– Letargy, apatia, drowsiness, anorexia, nausea,
agitation, hyporeflexia, hypothermia, convulsions– Signs severity depends upon:
• severity of hypoNa-miei (Na < 120mEq/l)
• speed of hypoNa-mia occurrence (acute/chronic)

HYPONATREMIA

Speed of hypoNa-mia occurrence

HYPONATREMIA
• Treatment – Correction of extracellular osmolarity and water
excess removal– Speed of correction depens upon:
• severity of hypoNa-mia• prezence/absence of symptoms• speed of occurrence (acute/chronic)
– Rapid correction of chronic hypoNa-mia – pontine mielinolysis (irreversible sequelae)
– In the prezence of symptoms, rapid correction until Na-mie 120mEq/l, than slow correction


HYPONATREMIA
HYPONATREMIA
HYPONATREMIANa-mia < 135mEq/l
CLASSIFICATION– Hypovolemic
• Water and Na deficit• Deficit of Na > water• Total body Na
True hyponatremia
– Isovolemic • Water excess of extracellular compartment• Total body Na - normal
Dilutional hyponatremia / Pseudohyponatremia
– Hypervolemic• Water and Na excess• Excess of water > Na• Total body Na ↑
Dilutional hyponatremia
HYPOVOLEMIC HYPONATREMIA total body Na
MECHANISM– water and Na deficit; deficit of Na > water; total body Na
CAUSES– Extrarenal losses
• Digestive losses (vomiting, diarrheea)• Skin losses (profuse sweating)• Third space formation (pancreatitis, burns, crush syndrome, intestinal
oclusions, etc.)– Renal losses
• osmotic diuresis, excess of diuretics, polyuria
DIAGNOSTIC• Signs of extracellular volume contraction (hypovolemia)• Na urinary < 10mEq/l – extrarenal losses• Na urinary > 20mEq/l – renal losses
TREATMENT– Correction of extracellular volume– Isotonic solutions

ISOVOLEMIC HYPONATREMIA total body Na normal
MECHANISM– water excess of the extracellular space; total body Na normal
CAUSES– Syndrome of inappropiate antidiuretic hormone secretion (SIADH)
– Fear, excitement, pain, drugs, surgical procedures
– Hyperosmolar states (hyperglycemia, intoxications)
DIAGNOSTIC– Extracellular water excess; no clinical signs
– Na urinary > 20mEq/l
TREATMENT– Water restriction

ISOVOLEMIC HYPONATREMIA

HYPERVOLEMIC HYPONATREMIA total body Na ↑
MECHANISM– Excess of water and Na; excess of water > Na; total body Na ↑
CAUSES– Edematous syndromes (cardiac failure, liver cirhosis, nephrotic
syndrome)– Acute and chronic renal failure
DIAGNOSTIC– Signs of extracellular volume expansion (edema)– Na urinary < 10mEq/l in edematous syndromes– Na urinar > 20mEq/l in renal failure
TREATMENT– Water (and salt) restriction

WATER AND ELECTROLYTES DISTURBANCES
Classification (Shires şi Baxter)
• Volume disturbances• Volume contraction• Volume expansion
• Concentration disturbances• Hyponatremia• Hypernatremia• Other hyperosmolar states
• Composition disturbances• Hypo/hyperpotasemia• Hypo/hypercalcemia• Hypo/hypermagnesemia• Hypo/hyperphosphatemia• Hydrogen ion disturbances (acid-base disturbances)
POTASIUM• Body K distribution
• 98% intracellular – 150-160mEq/l• 2% extracellular – 3,5-5mEq/l
The main intracellular cation• Intracellular functions
» Cell volume regulation» Intracellular pH regulation» Proteins and glycogen synthesis» Cell grow regulation» Cell enzymes activation» Rest potential of cell membrane
The main function membrane potential

Hypokalemia (<3.5mEq/L)
• Pathophysiology – – Decrease in K+ causes decreased excitability
of cells, therefore cells are less responsive to normal stimuli

POTASIUM DISTURBANCES
• Factors which influence K intercompartmental distribution:
– Serum K
– pH: acidosis or alcalosis
– Hyperosmolarity
– Hormons: insulin and catecholamines
• Factors which influence K urinnary excretion:– Serum K level
– Aldosteron
– Urinay flow
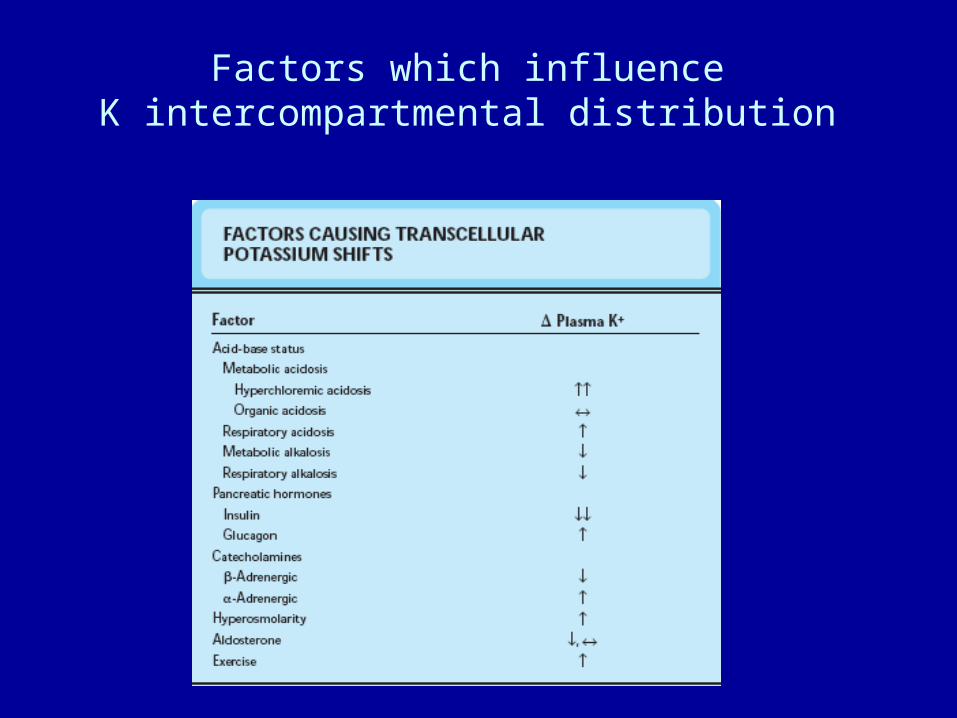
Factors which influence K intercompartmental distribution
POTASIUM
Intercompartmental K movements according to pH
– Acidosis → extracellular H+ ↑ → H+ moves into cell
K+ moves out of cell
hyperpotasemia
– Alcalosis → extracellular H+ → H+ moves out of cell K+ moves into cell
hypopotasemia

HYPERPOTASEMIA
• Frequent causes of pseudohyperpotasemia:– Blood drawing: thin needles, intense negative
pressure (erythrocytes hemolysis, K release), garou, fist “pumping” (K muscle release), blood storage (erythrocytes K release);
– Leucocytosis / thrombocytosis - hyperpotasemia;

HYPERPOTASEMIACAUSES
– Increased K+ intake• enteral intake• parenterală intake
– K+ movement out of the cells• Metabolic acidosis• Hyperglycemia• Excessive excercise• Hypercatabolism• Drugs: β-blockers, succinilcholine, digitalis
– Decreased urinnary K+ ellimination• Hypovolemia• Hypoaldosteronism• Renal failure• Drugs: spironolactone, AINS, heparine

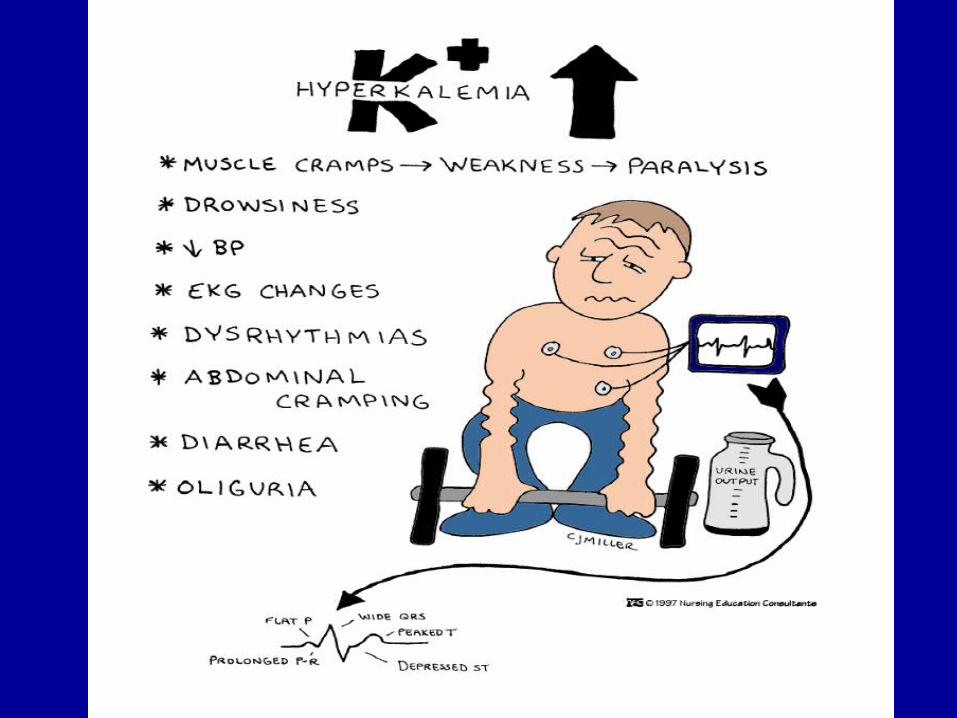
HYPERPOTASEMIA
CLINICAL PICTURE– Muscle signs
• paresthesia
• muscle weakness
• paralysis
– Cardiac signs• EKG signs
• Rhythm disturbances
• Dyastolic cardiac arrest

HYPERPOTASEMIA

HYPERPOTASEMIA
• mild/moderate (K+= 6-8mEq/l) – no clinical signs– limited ECG changes (peaked T waves, no changes of P or
QRS)– need for monitoring and treatment.
• severe (K+= >8mEq/l) – severe signs– severe ECG changes (peaked high T waves, no p waves,
wide QRS complexes)– need for emergency ECG monitoring and emwergency
treatment – risk of cardiac arrest.

HYPERPOTASEMIA
• ECG changes in hyperpotasemia:
• K+= 6-7mEq/l - peaked high T waves
• K+ =8-9mEq/l - absent P wave
• K+ =10mEq/l - wide QRS complex
• K+= 10-11mEq/l – biphasic QRST
• K+ =10-12mEq/l – ventricular fibrillation / dyastolic stillstand

ECG changes in hyperK-mie
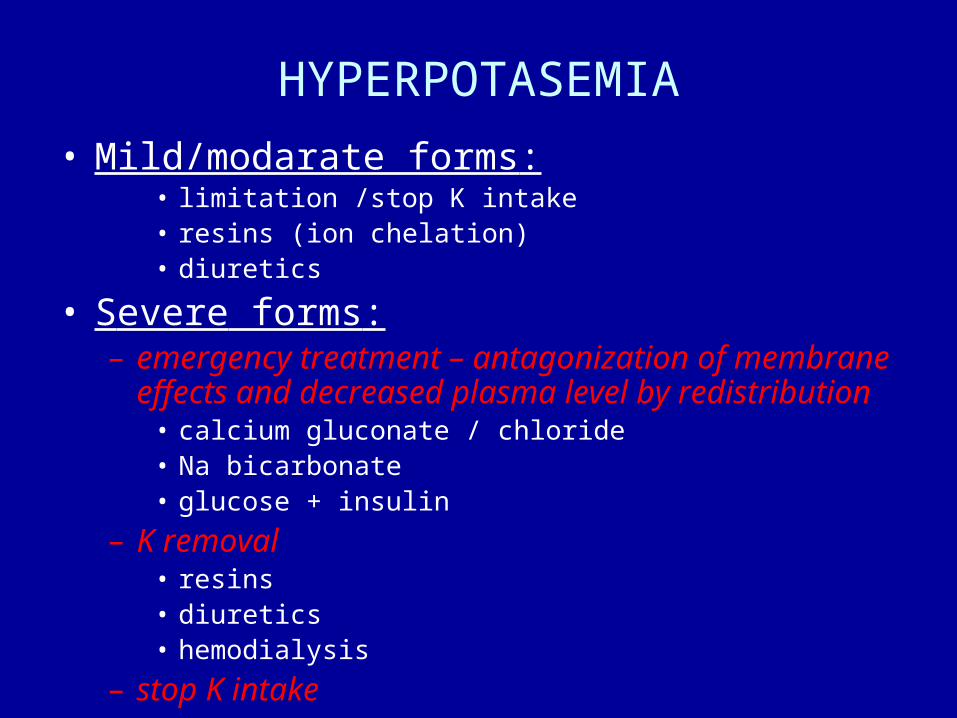
HYPERPOTASEMIA
• Mild/modarate forms:• limitation /stop K intake • resins (ion chelation)• diuretics
• Severe forms:– emergency treatment – antagonization of membrane effects
and decreased plasma level by redistribution• calcium gluconate / chloride • Na bicarbonate• glucose + insulin
– K removal• resins• diuretics• hemodialysis
– stop K intake

HYPOPOTASEMIA
CAUSES– Normal total K – changes of intercompartmental distribution
• Respiratorie / metabolic alcalosis
– Low total K • Deceased intake
• Poor nutrition (alcoholics)
• Digestive losses– Vomiting, gastric fistulae, naso-gastric tube, …
– Diarrheea, laxatives
• Renal losses– Excess of mineralocorticoids – primary/secondary
– Diuretics
– Osmotic diuresis

HYPOPOTASEMIACLINICAL PICTURE
Changes of membrane potential • Neuro-muscle effects
– Parestesia– Muscle weakness– Hyporeflexia– Paralitic ileus
• Cardio-vascular effects – Changes of cardiac excitability– ECG changes– Enhancement of digoxin toxicity – Rhythm disturbances– HTA
• Vegetative effects– orthostatic hTA
• Hepatic effects– Aggravation of encephalopathy in liver cirhosis patients
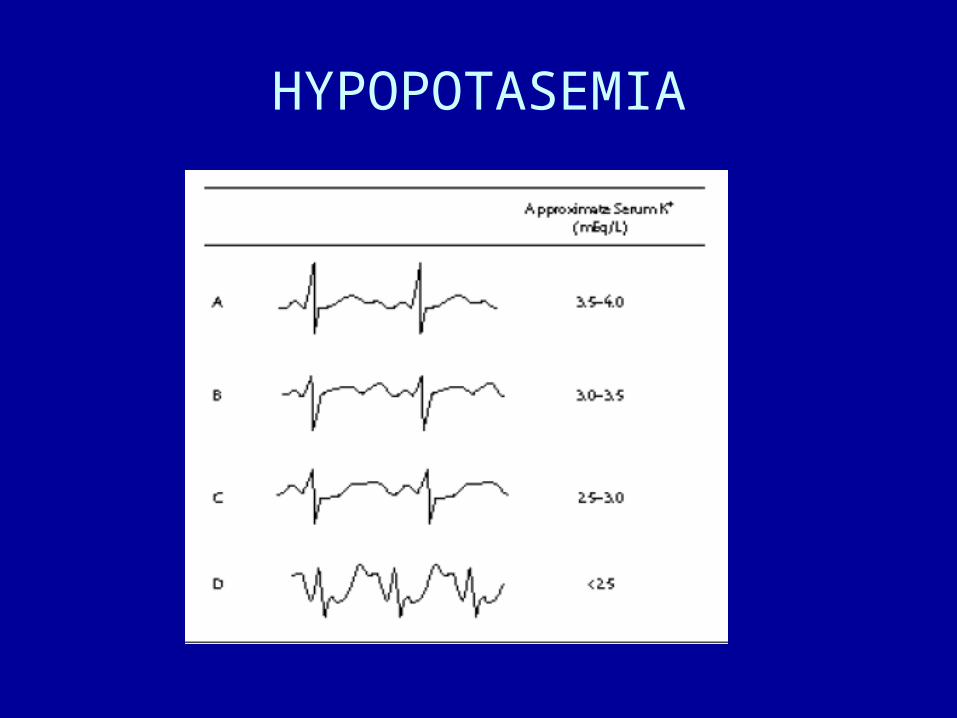
HYPOPOTASEMIA
ECG ABNORMALITIES• Flat T wave
• U wave
• wide QRS complex
• ST depresion
• Atrial and ventricular rhythm disturbances
HYPOPOTASEMIA

HYPOPOTASEMIA
PROPHYLAXIS• Administration of K daily needs – 1mEq/kg day
TREATMENT• Correction of causative disease• K amount– depends upon severity of hypo-K
– K-mia > 3mEq/l – oral
– K-mia 2-3mEq/l – 10-20mEq/h
– K-mia < 2mEq/l – 20mEq iv + than 20mEq/h
ECG monitoring - mandatory