Watchful Waiting in Continuous-Flow Left Ventricular...
9
1 C ontinuous-flow left ventricular assist devices (CF-LVADs) have led to a significant improvement in the survival of patients with end stage heart failure. 1–3 However, CF-LVAD use is complicated by numerous serious adverse events, with bleeding and thrombosis accounting for 51.3% of readmis- sions. 4 Device thrombosis in particular is a feared complica- tion of long-term CF-LVAD support, occurring in ≈10% of patients per year with substantial increase in mortality per the most recent Interagency Registry for Mechanically Assisted Circulatory Support report. 5–7 Significant progress has been made in diagnosis and management of device thrombosis and it has become clear that hemolysis is its hallmark sign. 8–10 Intensification of standard anticoagulation and antiplatelet therapy is the usual first step when hemolysis is observed, yet its efficacy is poorly studied and uncertainty exists as to when escalation of therapy to thrombolysis or possibly device exchange should be pursued. 10,11 See Editorial by Kiernan and Katz See Clinical Perspective Indeed, there currently is no consensus on the appropriate use of medical or surgical interventions for the treatment of hemolysis in Heartmate II CF-LVAD (HM II, Thoratec Corp, Pleasanton, CA) patients. 7,8,10,12 A watchful waiting approach Original Article © 2016 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.115.002896 Background—Management of hemolysis in the setting of suspected device thrombosis in continuous-flow left ventricular assist device patients varies widely, ranging from watchful waiting with intensified antithrombotic therapy to early surgical device exchange. The aim of this study was to compare the outcomes of hemolysis events treated with surgical interventions versus medical management alone. Methods and Results—A retrospective review of Heartmate II continuous-flow left ventricular assist device patients at 2 centers from January 2009 to September 2014 was completed. Patients were categorized as surgical management if hemolysis refractory to intensification of standard antithrombotic therapy was treated surgically. The primary end point was the first occurrence of cerebrovascular accident (CVA) or death. Sixty-four hemolysis events occurred in 49/367 patients implanted with Heartmate II continuous-flow left ventricular assist devices. Of 49 primary hemolysis events, 24 were treated with surgical interventions. After surgical treatment, 1 patient died and 2 experienced CVAs, as compared with 3 deaths and 9 CVAs in the 25 patients who remained on intensified antithrombotic therapy alone. The 1-year freedom from CVA or death was 87.5% and 49.5% in the surgical and medical cohorts, respectively (P=0.027). Resolution of a primary hemolysis event without CVA or death occurred in 21/24 patients treated with surgical interventions and in 13/25 who remained on medical therapy alone. A similar association between treatment and outcome was noted in the 15 recurrent hemolysis events. Conclusions—Hemolysis refractory to intensification of antithrombotic therapy identifies continuous-flow left ventricular assist device patients at major risk for CVA and death. Early device exchange should be considered to minimize these risks. (Circ Heart Fail. 2016;9:e002896. DOI: 10.1161/CIRCHEARTFAILURE.115.002896.) Key Words: analysis ■ heart failure ■ hemolysis ■ hemorrhage ■ thrombosis Received August 29, 2015; accepted March 18, 2016. From the Division of Cardiology, Department of Medicine, Montefiore Medical Center/Albert Einstein College of Medicine, New York, NY (A.P.L., O.S., S.R.P., D.B.S., J.D.N., J.J.S., U.P.J.); Division of Cardiology, Department of Medicine, Columbia University, New York, NY (A.P.L., J.Z.W., C.J.L., J.A.F., V.K.T., P.C.C.); Department of Cardiothoracic Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, New York, NY (D.J.G.); Department of Cardiothoracic Surgery, Columbia University, New York, NY (Y.N., H.T.); and Division of Cardiology, University of Chicago, IL (N.U.). *Drs Levin and Saeed contributed equally to this work. Correspondence to Ulrich P. Jorde, MD, Division of Cardiology, Montefiore Medical Center/Albert Einstein College of Medicine, 3400 Bainbridge Ave, Medical Arts Pavilion – 7th Floor, Bronx, New York 10467. E-mail ujorde@montefiore.org. Watchful Waiting in Continuous-Flow Left Ventricular Assist Device Patients With Ongoing Hemolysis Is Associated With an Increased Risk for Cerebrovascular Accident or Death Allison P. Levin, BA*; Omar Saeed, MD*; Joshua Z. Willey, MD; Charles J. Levin; Justin A. Fried, MD; Snehal R. Patel, MD; Daniel B. Sims, MD; Jenni D. Nguyen, RN, BSN; Julia J. Shin, MD; Veli K. Topkara, MD, MSc; Paolo C. Colombo, MD; Daniel J. Goldstein, MD; Yoshifumi Naka, MD, PhD; Hiroo Takayama, MD, PhD; Nir Uriel, MD, MSc; Ulrich P. Jorde, MD by guest on June 30, 2018 http://circheartfailure.ahajournals.org/ Downloaded from
Transcript of Watchful Waiting in Continuous-Flow Left Ventricular...

1
Continuous-flow left ventricular assist devices (CF-LVADs) have led to a significant improvement in the survival of
patients with end stage heart failure.1–3 However, CF-LVAD use is complicated by numerous serious adverse events, with bleeding and thrombosis accounting for 51.3% of readmis-sions.4 Device thrombosis in particular is a feared complica-tion of long-term CF-LVAD support, occurring in ≈10% of patients per year with substantial increase in mortality per the most recent Interagency Registry for Mechanically Assisted Circulatory Support report.5–7 Significant progress has been made in diagnosis and management of device thrombosis and it has become clear that hemolysis is its hallmark sign.8–10
Intensification of standard anticoagulation and antiplatelet therapy is the usual first step when hemolysis is observed, yet its efficacy is poorly studied and uncertainty exists as to when escalation of therapy to thrombolysis or possibly device exchange should be pursued.10,11
See Editorial by Kiernan and Katz See Clinical Perspective
Indeed, there currently is no consensus on the appropriate use of medical or surgical interventions for the treatment of hemolysis in Heartmate II CF-LVAD (HM II, Thoratec Corp, Pleasanton, CA) patients.7,8,10,12 A watchful waiting approach
Original Article
© 2016 American Heart Association, Inc.
Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.115.002896
Background—Management of hemolysis in the setting of suspected device thrombosis in continuous-flow left ventricular assist device patients varies widely, ranging from watchful waiting with intensified antithrombotic therapy to early surgical device exchange. The aim of this study was to compare the outcomes of hemolysis events treated with surgical interventions versus medical management alone.
Methods and Results—A retrospective review of Heartmate II continuous-flow left ventricular assist device patients at 2 centers from January 2009 to September 2014 was completed. Patients were categorized as surgical management if hemolysis refractory to intensification of standard antithrombotic therapy was treated surgically. The primary end point was the first occurrence of cerebrovascular accident (CVA) or death. Sixty-four hemolysis events occurred in 49/367 patients implanted with Heartmate II continuous-flow left ventricular assist devices. Of 49 primary hemolysis events, 24 were treated with surgical interventions. After surgical treatment, 1 patient died and 2 experienced CVAs, as compared with 3 deaths and 9 CVAs in the 25 patients who remained on intensified antithrombotic therapy alone. The 1-year freedom from CVA or death was 87.5% and 49.5% in the surgical and medical cohorts, respectively (P=0.027). Resolution of a primary hemolysis event without CVA or death occurred in 21/24 patients treated with surgical interventions and in 13/25 who remained on medical therapy alone. A similar association between treatment and outcome was noted in the 15 recurrent hemolysis events.
Conclusions—Hemolysis refractory to intensification of antithrombotic therapy identifies continuous-flow left ventricular assist device patients at major risk for CVA and death. Early device exchange should be considered to minimize these risks. (Circ Heart Fail. 2016;9:e002896. DOI: 10.1161/CIRCHEARTFAILURE.115.002896.)
Key Words: analysis ■ heart failure ■ hemolysis ■ hemorrhage ■ thrombosis
Received August 29, 2015; accepted March 18, 2016.From the Division of Cardiology, Department of Medicine, Montefiore Medical Center/Albert Einstein College of Medicine, New York, NY (A.P.L.,
O.S., S.R.P., D.B.S., J.D.N., J.J.S., U.P.J.); Division of Cardiology, Department of Medicine, Columbia University, New York, NY (A.P.L., J.Z.W., C.J.L., J.A.F., V.K.T., P.C.C.); Department of Cardiothoracic Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, New York, NY (D.J.G.); Department of Cardiothoracic Surgery, Columbia University, New York, NY (Y.N., H.T.); and Division of Cardiology, University of Chicago, IL (N.U.).
*Drs Levin and Saeed contributed equally to this work. Correspondence to Ulrich P. Jorde, MD, Division of Cardiology, Montefiore Medical Center/Albert Einstein College of Medicine, 3400 Bainbridge Ave,
Medical Arts Pavilion – 7th Floor, Bronx, New York 10467. E-mail [email protected].
Watchful Waiting in Continuous-Flow Left Ventricular Assist Device Patients With Ongoing Hemolysis Is
Associated With an Increased Risk for Cerebrovascular Accident or Death
Allison P. Levin, BA*; Omar Saeed, MD*; Joshua Z. Willey, MD; Charles J. Levin; Justin A. Fried, MD; Snehal R. Patel, MD; Daniel B. Sims, MD; Jenni D. Nguyen, RN, BSN;
Julia J. Shin, MD; Veli K. Topkara, MD, MSc; Paolo C. Colombo, MD; Daniel J. Goldstein, MD; Yoshifumi Naka, MD, PhD; Hiroo Takayama, MD, PhD;
Nir Uriel, MD, MSc; Ulrich P. Jorde, MD
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

2 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
observing hemolysis refractory to intensification of standard antithrombotic therapy may be contemplated because of the unknown significance of hemolysis without overt pump or end-organ dysfunction as well as to avoid the upfront risk of death and stroke associated with device exchange.13 On the other hand, surgical intervention has evolved to a less invasive subcostal approach and potentially removes the root cause of future pump dysfunction and embolic events, such as cere-brovascular accidents (CVA).14,15 To determine which strategy in CF-LVAD patients with ongoing hemolysis may provide optimal outcomes, we compared the outcomes of hemolysis events treated with surgical management versus medical man-agement alone in patients implanted with the HM II CF-LVAD at 2 large volume academic medical centers.
Methods
Study PopulationA retrospective chart review of all patients who underwent HM II implantation at either Montefiore Medical Center/Albert Einstein College of Medicine or Columbia University Medical Center be-tween January 2009 and September 2014 was conducted. This study was approved by both institutions’ review boards. Analysis was per-formed on combined deidentified data from the clinical databases at both institutions.
Data CollectionPreoperative clinical information, baseline demographics, and lactate dehydrogenase (LDH) values were collected from electronic medical charts. To exclude postoperative alterations, LDH values ≤14 days af-ter HM II implantation were excluded. A hemolysis event was defined as at least 3 consecutive LDH measurements greater than 700 U/L (2.5× normal value at our laboratories). Recurrent hemolysis events were defined as a repeat increase in LDH to above 2.5× normal on 3 serial measurements after levels had dropped consistently below 400 U/L.9
Hemolysis TreatmentPatient charts were reviewed to identify the strategy used to treat the hemolysis event. Treatments strategies were divided into surgical and medical interventions. Patients were categorized as the surgical group if they underwent a device exchange, bend-relief repair, or an out-flow graft ligation with pump decommissioning (powered off) to treat hemolysis refractory to intensification of standard antithrombotic therapy. Those only treated by intensified antithrombotic therapy and those in whom antithrombotic therapy had remained unchanged after hemolysis had occurred were placed in the medical group. Intensified antithrombotic therapy was defined as at least one but possibly all of the following: Escalation of target partial thromboplastin time to either 80 to 100 or antifactor Xa assay 0.5 to 0.7 on a continuous heparin infusion, target International Normalized Ratio increase to 2.5 to 3.0, an increase in aspirin dosage from 81 mg to 325 mg daily, and the addition of dipyridamole 75 mg three times per day.16
OutcomesThe primary end point was the first occurrence of a composite end point of CVA or death after a primary hemolysis event within 1-year of treatment. The secondary end point was the first occurrence of a composite end point of CVA or death after a recurrent hemolysis event within 1-year of treatment of the initial hemolysis event. Overall ef-fectiveness of therapy after a hemolysis event was measured as the proportion of patients who experienced a resolution of their primary hemolysis events without CVA, death or recurrence. CVAs included ischemic or hemorrhagic events, which were verified through a com-puted tomographic scan reviewed by an independent neurologist.
Statistical AnalysisContinuous variables are displayed as means±standard deviation or median (Q1 to Q3), for normally distributed and skewed data, respec-tively. Baseline data were compared with t tests for normally distrib-uted continuous variables and χ2 tests for categorical variables with expected frequencies ≥5 for both cohorts. The Mann–Whitney U test and Fisher exact tests were used for non-normally distributed contin-uous variables and categorical values with low expected frequencies, respectively. Cumulative survival free from the primary and second-ary end points at 1-year were shown using Kaplan–Meier curves. The time at risk began at the time of hemolysis onset for the medical group and at the time of surgical intervention for the surgical group. Hazard ratios were calculated using Cox proportional hazards analy-sis. P values of ≤0.05 were considered statistically significant. All statistical analysis was conducted using SE (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
ResultsPatient CharacteristicsDuring the study period, 367 patients underwent HM II implan-tation (Columbia University Medical Center=255, Monte-fiore Medical Center=112). In total, 22,577 LDH values were retrieved (Columbia University Medical Center=13,515, Monte-fiore Medical Center=9062) and screened. Sixty-four hemolysis events were identified in 49 patients, with 13 patients experi-encing more than one event. Detailed demographics by primary event treatment assignment are shown in the Table. Those in the surgical group tended to be older (59±13 versus 51±15 years old,
Table. Patients Characteristics at the Time of Primary Hemolysis Event
Surgical (n=24) Medical (n=25) P Value
Age, y, mean±SD 59.09±13.65 51.7±14.49 0.080
Male, n (%) 20 (48.8) 21 (51.2) 0.263
Body surface area, m2, mean±SD
1.93±0.51 1.96±0.23 0.810
Bridge-to-transplantation, n (%)
12 (41.4) 17 (58.6) 0.337
Ischemic cardiomyopathy, n (%)
10 (47.6) 11 (52.4) 0.556
Diabetes mellitus, n (%) 10 (45.5) 12 (54.6) 0.696
Hypertension, n (%) 12 (42.9) 16 (57.1) 0.469
History of smoking, n (%) 10 (52.6) 9 (47.4) 0.246
Days from implant to hemolysis onset, median (Q1–Q3)
114 (28–313) 86 (29–282) 0.620
Laboratory values at hemolysis onset
Albumin, g/dL 3.7 (3.2–4.2) 4.15 (3.7–8.6) 0.073
Platelet count, 103/mm3
185±62 187±58 0.937
Creatinine, mg/dL 1.62±1.0 1.39±0.86 0.906
AST, U/L 27 (17–67) 46 (22–90) 0.408
ALT, U/L 20.5 (16–27) 46 (22–90) 0.138
LDH, U/L 1074±325 940±294 0.099
ALT indicates alanine transaminase; AST, aspartate aminotransferase; and LDH, lactate dehydrogenase.
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

3 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
P=0.08). Sex distribution, cause of cardiomyopathy, and other baseline demographics did not differ between treatment groups. In the overall cohort, the freedom from hemolysis at 6, 12, and 24 months was 91%, 87%. and 84%, respectively (Figure 1). This represents 0.11 hemolysis events per patient year. Nota-bly, the 1-year freedom from hemolysis among those implanted before March 2011 was 96.1%, as compared with 82.7% among those implanted after this date, corresponding to incidence rates of 0.051 and 0.147, respectively. This significant (P=0.003) increase in 2011 is consistent with contemporary reports.17
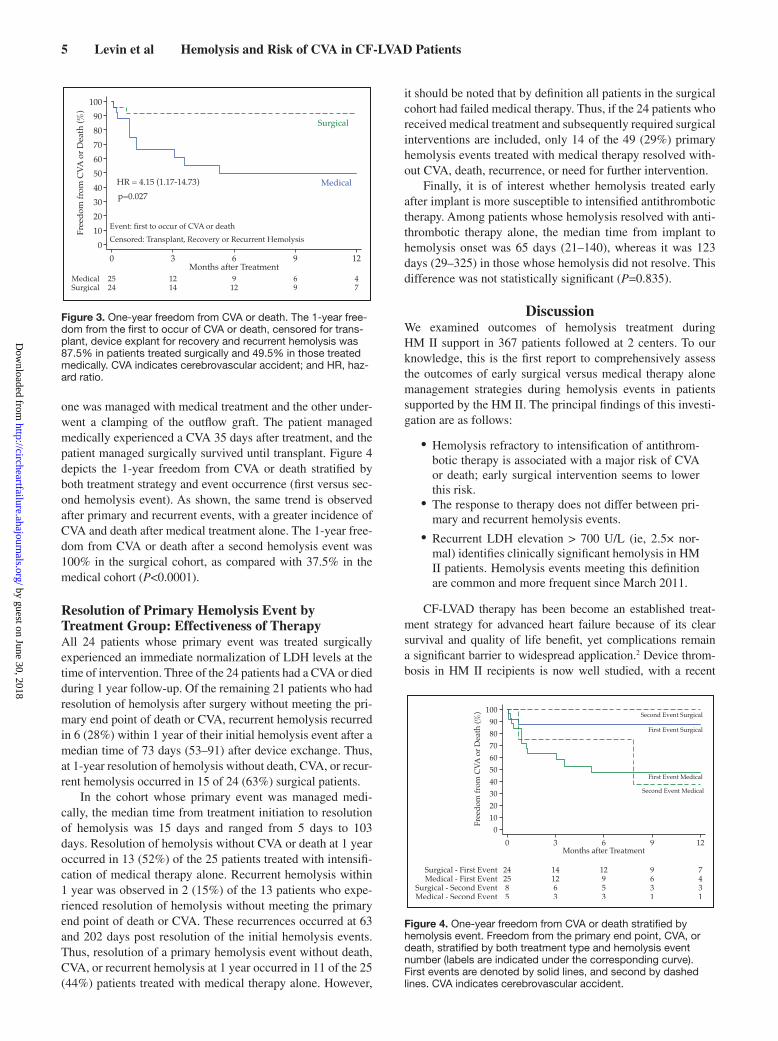
Management of Hemolysis EventsFigure 2 summarizes the various management techniques utilized. Of the 64 events, 33 (52%) were treated surgically. Before surgical treatment, an attempt to maximize antithrom-botic therapy was made in all patients. This included intensi-fication of intravenous heparin in 28 out of 33 events, as well as change in antiplatelet therapy (increase of aspirin dose and addition of intravenous antiplatelet agents) in 14 out of
33 instances. Despite optimization of antithrombotic therapy, these patients had an elevation in their mean creatinine from 1.62±1.0 mg/dL at the onset of hemolysis to 1.96±1.2 mg/dL at the time of surgery (P=0.001). The mean LDH also increased from 1076±337 to 1709±696 IU/L (P<0.001). Surgical treat-ment included 30 device exchanges (9 median sternotomies, 21 subcostal incisions), 2 bend relief repairs, and one ligation of the outflow graft with decommissioning of the pump. Clot was confirmed intraoperatively or after pump disassembly in all patients in whom the device was exchanged. Although there was no set treatment algorithm for surgical intervention throughout the study period, it was generally undertaken after echocardiographic evaluation suggested a flow obstruction and end-organ dysfunction was observed (ie, hypotension and an increase in serum creatinine). The remaining 31 (49%) hemo-lysis events were treated medically; 29 with intensified anti-thrombotic therapy, and 2 (3%) without any change to their baseline regimen as the hemolysis events and their significance went unrecognized at the time of occurrence.12
Figure 1. Freedom from hemolysis. A, Freedom from hemolysis in the overall cohort, censored for transplant, death, and device explant. B, Freedom from hemolysis for patients implanted before March 2011 (dashed line) and after March 2011 (solid line). HR indicates hazard ratio.
A
B
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

4 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
The remaining 31 (49%) hemolysis events were treated medically; 29 with intensified antithrombotic therapy, and 2 (3%) without any change to their baseline regimen as the hemolysis events and their significance went unrecognized at the time of occurrence. The median time from the initial HM II implant to the onset of hemolysis in this group was 86 days (28.5–281.5 days), which was not significantly different from the surgical cohort (P=0.620). In the 29 patients treated with intensified antithrombotic therapy, 26 were treated with heparin in combination with aspirin (81 or 325 mg) or war-farin or both. In addition to heparin, aspirin and warfarin, 1 patient received tirofiban, and another received eptifibatide. One patient was treated with argatroban. In this medically treated group, mean serum creatinine remained unchanged (1.39±0.86–1.25±0.61, P=0.250). Details can be found in Figure 2.
Outcomes of Primary Hemolysis Events by Treatment StrategyOf the 49 primary hemolysis events that occurred at a median time of 108 (28–295) days after implant, 24 patients were man-aged with a surgical approach and the remaining 25 patients were treated only with medical therapy. After 1-year of follow-up from the time of treatment of the initial hemolysis event, the primary end point occurred in 3 of the 24 patients (8%) man-aged surgically, in comparison to 12 of the 25 (48%) patients treated with only medical therapy. This included 1 death and
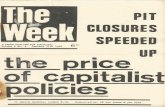
2 CVAs (both ischemic) in the surgical cohort and 3 deaths and 9 CVAs (6 ischemic, 2 hemorrhagic, and 1 hemorrhagic conversion) in the medical cohort. With censoring for recur-rent hemolysis, cardiac transplantation and CF-LVAD explant for recovery, survival free from CVA, or death in the surgi-cally treated patients was 87.5% in comparison to 49.5% in the patients treated with medical therapy only at 1 year. These findings resulted in a hazard ratio of 4.15 (95% confidence interval: 1.17–14.73) for the primary end point of death or CVA in comparing patients managed medically versus those who received a surgical intervention (Figure 3, P=0.027).
Outcomes After Recurrent Hemolysis Events by Treatment StrategyOf the 49 patients who experienced a primary hemolysis event, 13 had at least 1 recurrent hemolysis event. In these 13 patients, 11 patients experienced 2 events and 2 patients experienced 3 events. Thus, a total of 15 recurrent events were observed (13 second events, 2 third events). Of the 13 secondary recurrent events, 8 were managed surgically (all device exchanges) and 5 were managed medically. Among the 8 patients managed sur-gically, after 1 year of follow-up, 1 experienced a third hemo-lysis event, 3 were transplanted, and 4 remained on support. After 1 year of follow-up, in the 5 patients managed with medi-cal treatment alone, 1 experienced a CVA, 1 died, 1 experi-enced a third hemolysis event, 1 was transplanted, and the last remained on support. In the 2 patients with 3 hemolysis events,
Figure 2. Management of hemolysis events. Description of the specific management strategies used to treat all 64 hemolysis events. ASA indicates acetylsalicylic acid.
All Hemolysis Events
(n=64)
Surgical Treatment (n=33)
Exchange
(n=30)
Bend-Relief Repair (n=2)
Ligation of Outflow Graft
(n=1)
Medical Treatment (n=31)
Intensified Anticoagulation
(n=29)
Heparin/ASA/Warfarin
(n=25)
Heparin/ASA/Warfirin/Tirofiban
(n=1)
Heparin/ASA/Eptifibatide
(n=1)
Argatroban
(n=1)
Baseline Anticoagulation Regimen
(n=2)
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
5 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
one was managed with medical treatment and the other under-went a clamping of the outflow graft. The patient managed medically experienced a CVA 35 days after treatment, and the patient managed surgically survived until transplant. Figure 4 depicts the 1-year freedom from CVA or death stratified by both treatment strategy and event occurrence (first versus sec-ond hemolysis event). As shown, the same trend is observed after primary and recurrent events, with a greater incidence of CVA and death after medical treatment alone. The 1-year free-dom from CVA or death after a second hemolysis event was 100% in the surgical cohort, as compared with 37.5% in the medical cohort (P<0.0001).
Resolution of Primary Hemolysis Event by Treatment Group: Effectiveness of TherapyAll 24 patients whose primary event was treated surgically experienced an immediate normalization of LDH levels at the time of intervention. Three of the 24 patients had a CVA or died during 1 year follow-up. Of the remaining 21 patients who had resolution of hemolysis after surgery without meeting the pri-mary end point of death or CVA, recurrent hemolysis recurred in 6 (28%) within 1 year of their initial hemolysis event after a median time of 73 days (53–91) after device exchange. Thus, at 1-year resolution of hemolysis without death, CVA, or recur-rent hemolysis occurred in 15 of 24 (63%) surgical patients.
In the cohort whose primary event was managed medi-cally, the median time from treatment initiation to resolution of hemolysis was 15 days and ranged from 5 days to 103 days. Resolution of hemolysis without CVA or death at 1 year occurred in 13 (52%) of the 25 patients treated with intensifi-cation of medical therapy alone. Recurrent hemolysis within 1 year was observed in 2 (15%) of the 13 patients who expe-rienced resolution of hemolysis without meeting the primary end point of death or CVA. These recurrences occurred at 63 and 202 days post resolution of the initial hemolysis events. Thus, resolution of a primary hemolysis event without death, CVA, or recurrent hemolysis at 1 year occurred in 11 of the 25 (44%) patients treated with medical therapy alone. However,
it should be noted that by definition all patients in the surgical cohort had failed medical therapy. Thus, if the 24 patients who received medical treatment and subsequently required surgical interventions are included, only 14 of the 49 (29%) primary hemolysis events treated with medical therapy resolved with-out CVA, death, recurrence, or need for further intervention.
Finally, it is of interest whether hemolysis treated early after implant is more susceptible to intensified antithrombotic therapy. Among patients whose hemolysis resolved with anti-thrombotic therapy alone, the median time from implant to hemolysis onset was 65 days (21–140), whereas it was 123 days (29–325) in those whose hemolysis did not resolve. This difference was not statistically significant (P=0.835).
DiscussionWe examined outcomes of hemolysis treatment during HM II support in 367 patients followed at 2 centers. To our knowledge, this is the first report to comprehensively assess the outcomes of early surgical versus medical therapy alone management strategies during hemolysis events in patients supported by the HM II. The principal findings of this investi-gation are as follows:
•Hemolysis refractory to intensification of antithrom-botic therapy is associated with a major risk of CVA or death; early surgical intervention seems to lower this risk.
•The response to therapy does not differ between pri-mary and recurrent hemolysis events.
•Recurrent LDH elevation > 700 U/L (ie, 2.5× nor-mal) identifies clinically significant hemolysis in HM II patients. Hemolysis events meeting this definition are common and more frequent since March 2011.
CF-LVAD therapy has been become an established treat-ment strategy for advanced heart failure because of its clear survival and quality of life benefit, yet complications remain a significant barrier to widespread application.2 Device throm-bosis in HM II recipients is now well studied, with a recent
Figure 3. One-year freedom from CVA or death. The 1-year free-dom from the first to occur of CVA or death, censored for trans-plant, device explant for recovery and recurrent hemolysis was 87.5% in patients treated surgically and 49.5% in those treated medically. CVA indicates cerebrovascular accident; and HR, haz-ard ratio.
Figure 4. One-year freedom from CVA or death stratified by hemolysis event. Freedom from the primary end point, CVA, or death, stratified by both treatment type and hemolysis event number (labels are indicated under the corresponding curve). First events are denoted by solid lines, and second by dashed lines. CVA indicates cerebrovascular accident.
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
6 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
report by Starling et al7 demonstrating a significant increase in its frequency after March 2011. Interestingly, our observation of increased frequency of hemolysis is entirely consistent with their report, yet such a finding may not have been evident using historical cutoffs for hemolysis (plasma free hemoglobin > 40 mg/dL).2,17 We used an LDH level of 700 U/L (2.5× normal) to define hemolysis events, as such an elevation has previously been shown to provide high sensitivity and specificity for the diagnosis of device thrombosis.12,18 Our current data further support that such LDH elevations are meaningful and we think this in and of itself is an important observation.
Several recent reports indicate excellent outcomes with early surgical device exchange in patients who developed hemolysis as well as end-organ dysfunction.14,15,19 In the absence of guideline recommendations and expert consen-sus statements, it must be emphasized that current published management practices all reserve pump exchange for hemo-dynamically significant pump thrombosis.11 Despite this,
patients with hemolysis and no evidence of end-organ dys-function may experience embolic complications including devastating CVAs.10,17,20
In this context, it is important to note that the surgical technique for HM II device exchange has evolved. Recently reported favorable safety profiles and long-term outcomes after subcostal device exchange may provide added reas-surance for lowering thresholds for early surgical interven-tion.14 On the other hand, 28% of patients in our series had a recurrence of hemolysis after an initial successful surgical exchange. This may indicate the presence of patient related–risk factors of thrombus formation that remain unchanged after device replacement, but could also result from left-over throm-bus in outflow graft or inflow cannula not removed during device exchange. We do not think the latter to be the case for our surgically exchanged patients, as hemolysis cleared after exchange in all patients and screening for residual thrombus in the outflow graft and inflow cannula was routinely performed.
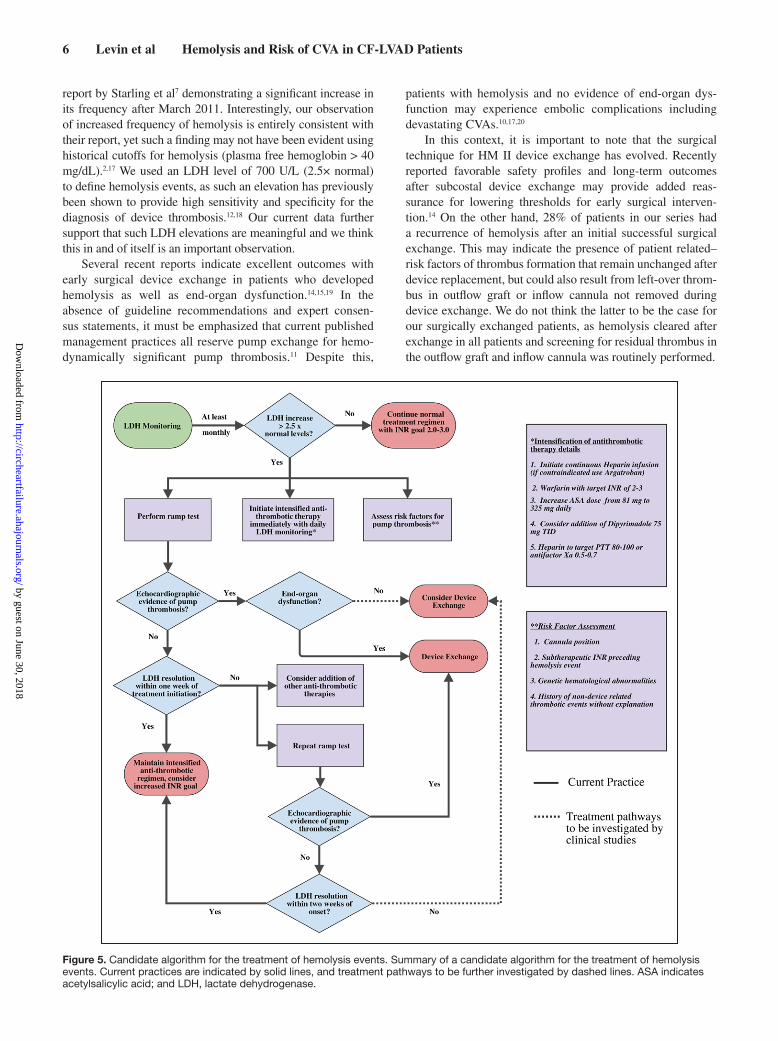
Figure 5. Candidate algorithm for the treatment of hemolysis events. Summary of a candidate algorithm for the treatment of hemolysis events. Current practices are indicated by solid lines, and treatment pathways to be further investigated by dashed lines. ASA indicates acetylsalicylic acid; and LDH, lactate dehydrogenase.
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

7 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
There are several limitations to the current investigation that need to be considered. First, this is a retrospective anal-ysis with all its inherent limitations. For example, no proto-coled inflow cannula position assessments were performed to establish that medical therapy would be futile and only device exchange could resolve hemolysis. Second, even though patients in the medical therapy arm were grouped together, the actual medical regimens were somewhat heterogeneous. Thus, the efficacy of specific antithrombotic regimen in comparison to surgical intervention remains uncertain. Third, our medical therapy approach did not include true thrombolytic therapy and eptifibatide as this has been shown to be associated with a high risk of intracranial bleeding in HM II patients.21 Fourth, the histological make up of thrombus, such as fresh versus chronic clot may alter management strategy and clot histology was not verified in this analysis. In this context, it should be noted that the time to detection of the hemolysis event in each group was similar. Fifth, the true clinical applicability of our results to recurrent events may be limited by the relatively low absolute number of recurrent events. Nevertheless, we decided to strat-ify our analysis by primary versus recurrent because it would be inaccurate, both statistically and clinically, to perform a combined analysis because of the inherent rise in baseline haz-ard for recurrent events. In addition, our overall relatively low sample size and event rate prohibits highly rigorous statistical conclusions. Finally, the influence of center-specific surgical experience, perioperative care, and outpatient management strategies may limit the generalizability of our results.
Given the differences in outcomes based on treatment approach, we do not think that the cited limitations are suf-ficient to significantly undermine our principal observation: There is a high risk of CVA and death during ongoing obser-vation of hemolysis refractory to intensification of antithrom-botic therapy. Our data are consistent with observations most recently made in the Interagency Registry for Mechanically Assisted Circulatory Support database by Katz et al6 who reported increased morbidity and mortality after hemolysis. Of note, we report substantially lower freedom from hemolysis rates (87% versus 95%) than Katz et al6 because of different
definitions of hemolysis (plasma-free hemoglobin 40 mg/dL versus LDH 2.5× normal). This finding is in keeping with data from Cowger et al8 who previously reported that the traditional plasma-free hemoglobin 40 definition will grossly (by ≈50%) underestimate the incidence of hemolysis compared with LDH 2.5× normal. They further suggested that low level hemolysis may ultimately lead to high level hemolysis in HM II. Clearly, the key question at this time is what degree of hemolysis is clinically relevant as well as how and when it should be treated.
Based on the available evidence, and further supported by this investigation, an LDH level>2.5× normal should be inter-vened on. Furthermore, the current data provide the strongest evidence to date that a management strategy of early device exchange should be considered in patients with refractory hemo-lysis. Finally, given the high incidence of complications during a watchful waiting approach, with nearly half the patients dying or experiencing CVA in the first 6 months post medical therapy alone, one might argue that exchange should be undertaken based on hemolysis parameters/treatment response alone and before the development of end-organ dysfunction or heart failure. Furthermore, the observation that these serious adverse events occurred in the medical cohort despite an absence of worsening end-organ dysfunction provides additional support for the use of surgical interventions before end-organ dysfunction. Figure 5 depicts a candidate algorithm for the treatment of hemolysis in light of our observations, and Figure 6 summarizes the old, cur-rent, and proposed paradigms for the management of hemolysis.
ConclusionsHemolysis (defined as LDH elevation>2.5× normal) refractory to intensification of antithrombotic therapy identifies HM II patients at major risk for CVA and death. Early device exchange should be considered to minimize these risks. To validate our findings and to improve on current treatment algorithms, pro-spective studies in larger populations are urgently needed.
DisclosuresDrs Naka, Goldstein, Uriel, and Jorde are consultants for both Thoratec and Heartware. The other authors report no conflicts.
Figure 6. Summary of shifts in the paradigm for the treatment of hemolysis. Description of the shift in the paradigm for the monitoring and treatment of hemolysis, as well as a proposed paradigm. LDH indicates lactate dehydrogenase; and pfHgb plasma-free hemoglobin.
No LDH monitoring
Clinical Hemolysis
Overt pump Dysfunction
Device exchange
Clinical LDH monitoring ± Abnormal ramp testDevice
exchangeSevere hemolysis
(Hematuria, anemia,pfHgb > 40 mg/dl)
Any end-organ Dysfunction
Substantial Refractory Hemolysis(LDH > 2.5 x normal)
± Abnormal ramp testConsider Device
exchange
Old Paradigm
Current Paradigm
Proposed Paradigm
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

8 Levin et al Hemolysis and Risk of CVA in CF-LVAD Patients
References 1. Slaughter MS, Pagani FD, McGee EC, Birks EJ, Cotts WG, Gregoric I,
Howard Frazier O, Icenogle T, Najjar SS, Boyce SW, Acker MA, John R, Hathaway DR, Najarian KB, Aaronson KD; HeartWare Bridge to Transplant ADVANCE Trial Investigators. HeartWare ventricular as-sist system for bridge to transplant: combined results of the bridge to transplant and continued access protocol trial. J Heart Lung Transplant. 2013;32:675–683. doi: 10.1016/j.healun.2013.04.004.
2. Jorde UP, Kushwaha SS, Tatooles AJ, Naka Y, Bhat G, Long JW, Horstmanshof DA, Kormos RL, Teuteberg JJ, Slaughter MS, Birks EJ, Farrar DJ, Park SJ; HeartMate II Clinical Investigators. Results of the destination therapy post-food and drug administration approval study with a continuous flow left ventricular assist device: a prospective study using the INTERMACS registry (Interagency Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol. 2014;63:1751–1757. doi: 10.1016/j.jacc.2014.01.053.
3. Park SJ, Milano CA, Tatooles AJ, Rogers JG, Adamson RM, Steidley DE, Ewald GA, Sundareswaran KS, Farrar DJ, Slaughter MS; HeartMate II Clinical Investigators. Outcomes in advanced heart failure patients with left ventricular assist devices for destination therapy. Circ Heart Fail. 2012;5:241–248. doi: 10.1161/CIRCHEARTFAILURE.111.963991.
4. Hasin T, Marmor Y, Kremers W, Topilsky Y, Severson CJ, Schirger JA, Boilson BA, Clavell AL, Rodeheffer RJ, Frantz RP, Edwards BS, Pereira NL, Stulak JM, Joyce L, Daly R, Park SJ, Kushwaha SS. Readmissions after implantation of axial flow left ventricular assist device. J Am Coll Cardiol. 2013;61:153–163. doi: 10.1016/j.jacc.2012.09.041.
5. Kirklin JK, Naftel DC, Pagani FD, Kormos RL, Stevenson LW, Blume ED, Miller MA, Baldwin JT, Timothy Baldwin J, Young JB. Sixth INTERMACS annual report: a 10,000-patient database. J Heart Lung Transplant. 2014;33:555–564. doi: 10.1016/j.healun.2014.04.010.
6. Katz JN, Jensen BC, Chang PP, Myers SL, Pagani FD, Kirklin JK. A multicenter analysis of clinical hemolysis in patients supported with durable, long-term left ventricular assist device therapy. J Heart Lung Transplant. 2015;34:701–709. doi: 10.1016/j.healun.2014.10.002.
7. Starling RC, Moazami N, Silvestry SC, Ewald G, Rogers JG, Milano CA, Rame JE, Acker MA, Blackstone EH, Ehrlinger J, Thuita L, Mountis MM, Soltesz EG, Lytle BW, Smedira NG. Unexpected abrupt increase in left ventricular assist device thrombosis. N Engl J Med. 2014;370:33–40. doi: 10.1056/NEJMoa1313385.
8. Cowger JA, Romano MA, Shah P, Shah N, Mehta V, Haft JW, Aaronson KD, Pagani FD. Hemolysis: a harbinger of adverse outcome after left ventricular assist device implant. J Heart Lung Transplant. 2014;33:35–43. doi: 10.1016/j.healun.2013.08.021.
9. Uriel N, Han J, Morrison KA, Nahumi N, Yuzefpolskaya M, Garan AR, Duong J, Colombo PC, Takayama H, Thomas S, Naka Y, Jorde UP. Device thrombosis in HeartMate II continuous-flow left ventricular assist devices: a multifactorial phenomenon. J Heart Lung Transplant. 2014;33:51–59. doi: 10.1016/j.healun.2013.10.005.
10. Mehra MR, Stewart GC, Uber PA. The vexing problem of thrombosis in long-term mechanical circulatory support. J Heart Lung Transplant. 2014;33:1–11. doi: 10.1016/j.healun.2013.12.002.
11. Goldstein DJ, John R, Salerno C, Silvestry S, Moazami N, Horstmanshof D, Adamson R, Boyle A, Zucker M, Rogers J, Russell S, Long J, Pagani F, Jorde U. Algorithm for the diagnosis and management of suspected pump thrombus. J Heart Lung Transplant. 2013;32:667–670. doi: 10.1016/j.healun.2013.05.002.
12. Uriel N, Morrison KA, Garan AR, Kato TS, Yuzefpolskaya M, Latif F, Restaino SW, Mancini DM, Flannery M, Takayama H, John R, Colombo PC, Naka Y, Jorde UP. Development of a novel echocardiography ramp test for speed optimization and diagnosis of device thrombosis in contin-uous-flow left ventricular assist devices: the Columbia ramp study. J Am Coll Cardiol. 2012;60:1764–1775. doi: 10.1016/j.jacc.2012.07.052.
13. Kirklin JK, Naftel DC, Kormos RL, Pagani FD, Myers SL, Stevenson LW, Acker MA, Goldstein DL, Silvestry SC, Milano CA, Baldwin JT, Timothy Baldwin J, Pinney S, Eduardo Rame J, Miller MA. Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) analysis of pump thrombosis in the HeartMate II left ventricular assist device. J Heart Lung Transplant. 2014;33:12–22. doi: 10.1016/j.healun.2013.11.001.
14. Ota T, Yerebakan H, Akashi H, Takayama H, Uriel N, Colombo PC, Jorde UP, Naka Y. Continuous-flow left ventricular assist device ex-change: clinical outcomes. J Heart Lung Transplant. 2014;33:65–70. doi: 10.1016/j.healun.2013.07.003.
15. Levin AP, Uriel N, Takayama H, Mody KP, Ota T, Yuzefpolskaya M, Colombo PC, Garan AR, Dionizovik-Dimanovski M, Sladen RN, Naka Y, Jorde UP. Device exchange in HeartMate II recipients: long-term out-comes and risk of thrombosis recurrence. ASAIO J. 2015;61:144–149. doi: 10.1097/MAT.0000000000000170.
16. Adatya S, Uriel N, Yarmohammadi H, Holley CT, Feng A, Roy SS, Reding MT, John R, Eckman P, Zantek ND. Anti-factor Xa and acti-vated partial thromboplastin time measurements for heparin monitoring in mechanical circulatory support. J AM COLL CARDIOL. Heart Fail. 2015;3:314–322. doi: 10.1016/j.jchf.2014.11.009.
17. Shah P, Mehta VM, Cowger JA, Aaronson KD, Pagani FD. Diagnosis of hemolysis and device thrombosis with lactate dehydrogenase during left ventricular assist device support. J Heart Lung Transplant. 2014;33:102–104. doi: 10.1016/j.healun.2013.07.013.
18. Shah P, Mehta VM, Cowger JA, Haft JW, Romano MA, Aaronson KD, Pagani FD. Lactate dehydrogenase is superior to serum free hemoglobin as a marker of pump thrombosis in left ventricular assist devices. J Heart Lung Transplant. 2013;32:S37.
19. Stulak JM, Cowger J, Haft JW, Romano MA, Aaronson KD, Pagani FD. Device exchange after primary left ventricular assist device implanta-tion: indications and outcomes. Ann Thorac Surg. 2013;95:1262–7; dis-cussion 1267. doi: 10.1016/j.athoracsur.2012.08.031.
20. Cowger J, Pagani FD, Haft JW, Romano MA, Aaronson KD, Kolias TJ. The development of aortic insufficiency in left ventricular assist device-supported patients. Circ Heart Fail. 2010;3:668–674. doi: 10.1161/CIRCHEARTFAILURE.109.917765.
21. Tellor BR, Smith JR, Prasad SM, Joseph SM, Silvestry SC. The use of eptifibatide for suspected pump thrombus or thrombosis in patients with left ventricular assist devices. J Heart Lung Transplant. 2014;33:94–101. doi: 10.1016/j.healun.2013.11.002.
CLINICAL PERSPECTIVEThe management of hemolysis, the hallmark sign of device thrombosis in Heartmate II continuous-flow left ventricular assist device patients, ranges from a watchful waiting approach with intensified antithrombotic therapy to early surgical manage-ment via device exchange. Considerable variability in the decision to escalate treatment from a medical to surgical approach exists, driven by the lack of data directly comparing the risks of adverse events with each approach. Using data from 2 large academic centers, we retrospectively compared the outcomes of hemolysis events treated with surgical management versus medical management alone in patients implanted with the Heartmate II continuous-flow left ventricular assist device, includ-ing the rate of stroke, recurrent thrombosis, and death. We found that hemolysis refractory to intensification of antithrom-botic therapy identifies Heartmate II patients at major risk of cerebrovascular accident and death. Early device exchange, especially with the development of the noninvasive subcostal approach, was not associated with significant postoperative morbidity and should be considered soon after the identification of hemolysis refractory to medial therapy.
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Daniel J. Goldstein, Yoshifumi Naka, Hiroo Takayama, Nir Uriel and Ulrich P. JordePatel, Daniel B. Sims, Jenni D. Nguyen, Julia J. Shin, Veli K. Topkara, Paolo C. Colombo,
Allison P. Levin, Omar Saeed, Joshua Z. Willey, Charles J. Levin, Justin A. Fried, Snehal R.Death
orOngoing Hemolysis Is Associated With an Increased Risk for Cerebrovascular Accident Watchful Waiting in Continuous-Flow Left Ventricular Assist Device Patients With
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2016 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation: Heart Failure
doi: 10.1161/CIRCHEARTFAILURE.115.0028962016;9:Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/9/5/e002896World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information isthe Editorial Office. Once the online version of the published article for which permission is being requested
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculation: Heart Failurein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from