
Washington Update - AHA Physician Alliance · – Tim Walberg • MINNESOTA – Chip Cravaack •...
57
Washington Update The Politics of Health Care Reform: Implications for Physicians March 30, 2011
-
Upload
truonghanh -
Category
Documents
-
view
215 -
download
1
Transcript of Washington Update - AHA Physician Alliance · – Tim Walberg • MINNESOTA – Chip Cravaack •...

Washington Update
The Politics of Health Care Reform: Implications for Physicians
March 30, 2011

Overview
• Political Environment
• Immediate Issues

2012 Presidential• Obama polls improving
– 50% threshold– Tax deal in December– Move to the center– Unhappy base, but no challenger
• Republicans– No clear front runner (historic)– Late starting– Significant divisions

Political leverage…Senate• What’s at stake?
– 33 seats 23 Democrats 10 Republicans
• Democratic vulnerabilities– States where John McCain won in 2008
Joe Manchin (D-WV)…+13 Claire McCaskill (D-MO)…+0.1 Ben Nelson (D-NE)…+14.9 John Tester (D-MT)…+2.3
– States where GOP flipped Senate seats this year Sherrod Brown (D-OH)…Rob Portman (R) Bob Casey (D-PA)…Pat Toomey (R) [Kent Conrad (D-ND)]…Jon Hoeven (R) Herb Kohl (D-WI)…Ron Johnson (R)

Political leverage…House
• FLORIDA– Daniel Webster– Allen West
• ILLINOIS– Robert Dold– Adam Kinzinger– Randy Hultgren– Bobby Schilling– Joe Walsh
• KANSAS– Kevin Yoder
• MICHIGAN– Dan Benishek– Tim Walberg
• MINNESOTA– Chip Cravaack
• NEVADA– Joe Heck
• NEW HAMPSHIRE– Charlie Bass– Frank Guinta
• NEW JERSEY– Jon Runyan
• NEW YORK– Ann Marie Buerkle– Chris Gibson– Richard Hanna– Nan Hayworth
• NORTH CAROLINA– Renee Elmers
• OHIO– Steve Chabot– Steve Stivers
• PENNSYLVANIA– Lou Barletta– Mike Fitzpatrick– Pat Meehan
• TEXAS– Francisco Canseco– Blake Farenthold
• VIRGINIA– Scott Rigell
• WASHINGTON– Jamie Herrera
• WISCONSIN– Sean Duffy– Reid Ribble
31 new GOP (of 62) representatives whorepresent districts won by President Obama

Political leverage…House• 49 congressional districts carried by John McCain
were held by Democrats going into 2010 election– Democrats lost in 37 of those districts
• Remaining focus– Jason Altmire (PA)– Dan Boren (OK)– Ben Chandler (KY)– Mark Critz (PA)– Gabrielle Giffords (AZ)– Tim Holden (PA)– Jim Matheson (UT)– Mike McIntyre (NC)– Colin Peterson (MN)– Nick Rahall (WV)– Mike Ross (AR)– Heath Schuler (NC)

New political environment
• Cut spending
• Roll back ACA
• Regulatory relief
GOP Priorities

Political environment
• Legislative gridlock possible on major issues – Not just Democrats vs. Republicans…
but Republicans vs. Republicans– Still need 60 votes in the Senate– White House holds veto pen
• But grand deal also possible
Key Assumptions

Political environment
• New emphasis on deficit reduction…and zero-sum game on policy adjustments– “Cut-go” versus “pay-go”
Key Assumptions

Political environment• Health care reform
– Defensive strategy to preservepositive elements of reform
– Offensive strategy to: Shape key provisions during
implementation process Make improvements in
priority areas Political challenge

Legislative brinksmanship“Must Do” Measures
• Funding the government – Continuing Resolutions on Appropriations
Vehicle for reducing discretionary spending
• Debt limit extensions– Vehicle for longer term
deficit reduction
• Expiring provisions– Taxes– Medicare physician payment cuts

• Republicans needed to follow-through on campaign promise…and take the vote
• Largely symbolic
• Public remains equally divided
• Will relitigate before 2012 election
Repeal of health care reform

Repeal and Replace• House Votes
–Repeal 245 – 189 (3 Ds)–Replace 253 – 175 (14 Ds)
• Senate Vote – 47- 51 (Party line)

Priorities – To Do (Offense)
Expiring Provisions
Regulatory Relief
ACA FixesACA Implementation
Medical Liability Reform

• FIRST, expiring provisions• SECOND, PPACA implementation
– Rules and regulations– Coverage– Enroll America– Field leadership…performance improvement
• THIRD, PPACA fixes– IPAB exemption for CAH– Readmissions (2013)– Hospital acquired conditions (2015)– 340B expansions– GME (health care workforce) – Disproportionate share reductions (2014)
“To Do List”…5 Areas
Advocacy Agenda 2011 – Key Priorities
To Do List – Key Priorities• FOURTH, liability reform
– The HEALTH Act (H.R. 5)
• FIFTH, regulatory relief– Clinical integration– Misuse of False Claims Act– Recovery audit contractors– Health information technology
Certification Health information exchanges Eligibility for funding Meaningful use/flexibility Multi-campus


• Beyond PPACA repeal− Defunding and blocking implementation– Legal challenges– Potential legislative amendments
1099 reporting Medical device tax (offset) Coverage expansions
Medicaid expansions Individual mandate Employer responsibility
Physician self-referral Comparative effectiveness CMS Center for Innovation
Advocacy Agenda 2011

Defunding• Implementation money ($10-20B/10yr
cost to implement)
• Prevention and Public Health Fund
• Center for Medicare and Medicaid Innovation

Legal challenges• Court decisions currently 3-2
• Florida District Court ruled individual mandate unconstitutional and struck down entire law
• When will it go to the Supreme Court?

President’s FY 2012 Budget
• $62 billion primarily for two year patch on Medicare physician payment reductions
– Funded by specific savings from:
Medicaid Reducing ability of states to use Medicaid provider taxes
in 2015 ($18.3 billion) Rebase/extend Medicaid DSH allotments in 2021 ($4.1
billion) Limit Medicaid DME payment to Medicare levels ($6.4
billion) Pharmaceutical proposals ($12.8 billion) Program “integrity” ($13.9 billion) Program “efficiencies” ($6.4 billion)
Health Care

President’s FY 2012 Budget
• Children’s GME($317 million in FY 2012)
• No major changes to restructure entitlement programs such as Medicare, Medicaid or Social Security
Other Highlights

Potential hospital risks• Indirect medical education adjustment• Medicare bad-debt• IPAB Expansion• Acceleration of PPACA provisions• Elimination of Medicaid provider taxes
Politics of deficit reduction• Initial focus on discretionary funding
– FY 2008 levels– Earmarks
• Medicare and Social Security reform not possible without support from President Obama
– Republicans have no mandate for reform– Polls show most voters opposed– Would alienate seniors in 2012 elections
• Previous GOP efforts have failed withoutDemocratic support:
– Ronald Reagan and Social Security in 1981– Newt Gingrich and Medicare in 1995– George W. Bush and Social Security in 2005
• In addition…other GOP challenges in taking on Medicare:– Were critical of Medicare cuts in ACA– “Death panel” issue
• Significant reforms will not generate short-term savings because of necessary grandfathering requirements
Medicaid• Phase out of additional FMAP
fundingAmerican Recovery and Reinvestment Act of 2009
• “Flexibility:” pressure from governors– Block grants– Maintenance of effort
for eligibility
• Elimination of provider taxes

Politics of deficit reduction
• Democrats– Kent Conrad (ND)*– Dick Durbin (IL)*– Mark Warner (VA)
• Republicans– Mike Crapo (ID)*– Tom Coburn (OK)*– Saxby Chambliss (GA)
Bipartisan Senate Group

Our strategy• Hospitals have already made a significant contribution
to achieving savings in the Medicare and Medicaid programs
• Ideas: savings and revenueopportunities
– Liability reform– “Real” comparative effectiveness– Care at the end of life– Administrative simplification– Junk food taxes– Other revenues– Beneficiary cost-sharing restructuring– Adjusting retirement age
• Coalitions to help lawmakers make some of these tough choices
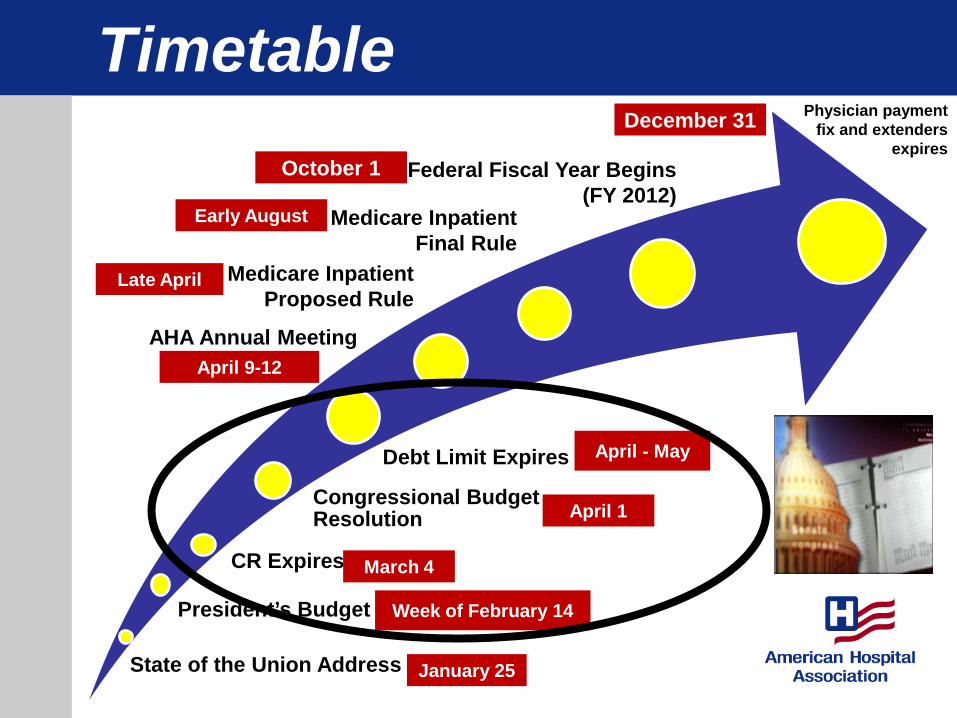
Timetable
State of the Union Address
Congressional Budget Resolution
CR Expires
Debt Limit Expires
President’s Budget
Physician paymentfix and extenders
expires
January 25
Week of February 14
March 4
April 1
December 31
April - May
Medicare InpatientProposed Rule
Late April
AHA Annual MeetingApril 9-12
Medicare InpatientFinal Rule
Early August
Federal Fiscal Year Begins (FY 2012)
October 1

Washington Update
Physician Leadership ForumMarch 30, 2011

The Politics of Health Care Reform: Implications for Physicians
March 30, 2011
Key Physician Issues for 2011• Changes Beginning Jan 1• Physician Quality Reporting• EHR & eRx Incentive Programs
Mandatory Payment Reforms• Hospital Value-Based Purchasing• Readmissions• Hospital-Acquired Conditions
Voluntary Programs• ACOs, Bundling & Medical Homes
Today’s Agenda

Key Physician Issues
Changes Effective January 1, 2011• Physician payment update
– No cuts for 2011– 29.5% reduction beginning Jan. 1, 2012
• Medicare 10% bonus payment– Primary care physicians – General surgeons providing care in HPSAs
• PAs allowed to order SNF services

Physician Quality ReportingPhysician Quality Reporting System (PQRS)• ACA extends the voluntary pay-for-reporting
initiative (formerly PQRI) – Bonus payment as a percentage of total
allowable Medicare charges• 2011 = 1.0%• 2012, 2013 and 2014 = 0.5%• 2015 = negative 1.5% [non-participating physicians]• 2016 = negative 2.0% [non-participating physicians]
New for CY 2011– Report on 3 measures (or a measure set) for 50%
(down from 80%) of eligible cases– New Group Practice Reporting Option (GPRO) II– 0.5% bonus for participation in a qualified
Maintenance of Certification (MOC) program

Physician Resource Use • Confidential feedback reports to
physicians (or groups) on per-capita resource use & quality of care measures– Currently, 12,000 physicians in 12
markets– ACA expands to all physicians, and
requires comparison of resource use to other physicians
– Beginning 2013, ACA requires public reporting of physician performance
Physician Quality Reporting (Cont.)

Physician Quality Reporting (Cont.)
Value-Based Payment Modifier– Budget neutral– Identify specific quality and cost measures by 2012– Rulemaking in 2013– Initial performance period in 2014– Implementation in 2015 for specific physicians and
groups of physicians– Phased up to all physicians by 2017

Electronic Health RecordsBeginning 2011, EPs are eligible for either a:• Medicare incentive payment (up to $44,000)
• 75% of Medicare charges for covered professional services subject to an annual cap
• Penalties for those who are not meaningful users beginning in 2015 (1.0% in 2015, 2.0% in 2016, 3.0% in 2017 and beyond, but HHS option to increase to 5.0% penalty if less than 75% EPs meet MU)
Or• Medicaid incentive payment (up to $63,750)
• Optional and administered by states (12 to date)• To qualify, 30%+ encounters are Medicaid• No penalties

EP Meaningful Use Definition
1. CPOE for medications2. Drug-drug/drug-allergy checks3. Electronic prescriptions 4. Record demographics5. Structured problem list6. Structured medication list7. Structured medication allergy list8. Record and chart changes in vital signs9. Record smoking status10. 1 clinical decision support rule 11. Report 6 clinical quality measures (3 core)12. Electronic health info to patients13. Provide visit summary14. Exchange key clinical information (capability)15. Protect electronic health information
16. Drug-formulary checks17. Incorporate structured clinical-lab data18. Generate patient lists by condition19. Generate patient reminders/follow-up20. Patient access to health information21. Identify patient-specific education resources22. Medication reconciliation23. Summary care record transitioned or referred
patients
24. Submit data to immunization registries25. Submit syndromic surveillance data
25 Objectives of Meaningful Use 20 Objectives Required in Stage 11. CPOE for Medications2. Drug-drug/drug-allergy checks3. Electronic prescriptions4. Record demographics5. Structured problem list6. Structured medication list7. Structured medication allergy list8. Record and chart changes in vital signs9. Record smoking status10. 1 clinical decision support rule 11. Report clinical quality measures12. Electronic health info to patients13. Electronic copy of discharge instructions14. Exchange key clinical information (capability)15. Protect electronic health information
15 Core Objectives Required of
All EPs
16. Option 117. Option 218. Option 319. Option 4
Choose 5 from
Menu Set20. Public Health Reporting Option 5

Electronic Prescribing - eRx• MIPPA provided EPs incentive payments
for e-prescribing, beginning CY 2009
• For 2011/2012: 1.0% bonus if report on one eRx measure for at least 25 unique e-prescribing events (2013 = 0.5% bonus)
• Penalties for non-participation– 2012 = 1.0%, 2013 = 1.5%, 2014 = 2.0%
• To avoid 2012 penalty, must report 10 e-prescribing events by June 30, 2011

Complex Interactions
• PQRS program incentive (1.0%) regardless EHR or eRX incentive programs.
• Medicaid EHR + eRx (1.0%)
• Medicare EHR, then may not receive eRxbonus… but will receive eRx penalty
Continue to report the eRx measures even if participating in EHR program

Valu
e-B
ased
Pu
rcha
sing
Rea
dmis
sion
s
Hea
lthca
re-A
cqui
red
Con
ditio
ns
Mandatory Programs
Inpatient PPS Fiscal Year2013
Fiscal Year2014
Fiscal Year2015
Hospital Value-Based Purchasing
MB – 1.0 Potential for Earn
Back
MB – 1.25 Potential for Earn
Back
MB – 1.5 Potential for Earn
Back
Readmissions
MB –Hosp-
specific amount
capped at 1.0
MB – Hosp-specific amount
capped at 2.0
MB – Hosp-specific amount
capped at 3.0
Hospital Acquired Conditions
MB – 1.0For Bottom
Quartile Hospitals
Mandatory Payment Reforms

Hospital Value-Based Purchasing
Payment incentives begin FY 2013
Applies only to PPS hospitals– critical access hospitals are excluded
Also excluded: hospitals determined to have too few patient cases or applicable measures
Funding generated by reducing MS-DRG payments:– 1.0 percent in FY 2013...2.0 percent in FY 2017
and beyond.

VBP Quality MeasuresCMS Proposed Rule – Jan. 7, 2011
Quality Measures: • For FY 2013, 18 total measures
– 17 process measures– HCAHPS patient experiences with care
• For FY 2014, 20 additional measures– 3 mortality measures– 9 ARHQ patient safety measures– 8 HACs
• For FY 2013, performance measured July 1, 2011 – March 31, 2012

Scoring Hospitals’ PerformanceCMS proposal:• Minimum threshold levels
– Need 10 cases in each measure; 4 measures total• Higher of attainment or improvement for each measure• Weighting: process = 70%/ HCAHPS 30%• Linear scale to translate performance score into
incentive payment• Program budget neutral...some
hospitals receive more than withheld, others less

ReadmissionsBeginning FY 2013, penalizes IPPS hospitals with high rates of potentially preventable Medicare readmissions
– Heart attack, heart failure, pneumonia (Secretary may expand in future years)
– Payment penalty is capped at 1.0 percent of total Medicare payments growing to 3.0 percent in 2015
– Statute says CMS must exclude “unrelated readmissions, such as planned readmissions or transfers.”

Readmissions
Hospital-Acquired Conditions Deficit Reduction Act of 2006
• In FY 2008, Secretary must stop paying the higher MS-DRG payment for 8 selected hospital-acquired conditions:• foreign object after surgery• Air embolism• Blood incompatibility• pressure ulcer stages III and IV• Falls and trauma• Vascular catheter-assoc infections• Catheter-assoc UTI

Hospital-Acquired Conditions
ACA requirements: • Applies only to PPS hospitals – critical access
hospitals are excluded • Payment penalty begin FY 2015• 8 measures• Hospitals in bottom-quartile of a national HAC
rate receive 1% cut to all Medicare discharges• Prior to 2015, Secretary will collect and
confidentially share hospital HAC rates – HAC rates released to individual hospitals in March– Will be available 3/31 (cms.gov) & 4/21 (hospital
compare)

Valu
e-B
ased
Pu
rcha
sing
Rea
dmis
sion
s
Hea
lthca
re-A
cqui
red
Con
ditio
ns
Mandatory
Voluntary Programs
Clinical Integration / Health Information Technology
Voluntary
Med
ical
Hom
es
Bun
dled
Pay
men
t
Acco
unta
ble
Car
e O
rgan
izat
ions

ACOs - Statutory Requirements
• Legal structure to receive/distribute savings• Serve minimum of 5,000 beneficiaries• 3-year commitment to participate• Defined process to report quality/cost data• Medicare beneficiaries assigned to ACOs can
continue to choose any providers (no “lock-in”)• Shared savings if ACO savings and quality
targets are achieved, after adjusting for random variation
• Option to use additional risk models including partial capitation
• PGP demo participants may convert and ACOs working with other payers get preference

AHA Policy on ACOs• Regulations must allow flexibility in terms of ACO
structure and governance• Must have real-time data• Quality measures must be reasonable and
attainable… evolve towards assessing care coordination and utilization
• Transparent calculation of expenditures and performance evaluation
• Methods to engage small and rural providers – Formation of regional networks, telemedicine
services; HIT connections• Waive barriers to clinical integration• Acknowledge up-front capital costs

ACO Rules
• Lots of Gossip!!– 1,000 pages +– Interim Final Rule (versus proposed)– DOJ, FTC, OIG, IRS language– Program limited to small number of players– Potentially down-side risk – Due out this Thursday?!

Bundled Payment – Statute
National, voluntary pilot programsGoal is to improve coordination, quality and
efficiencySecretary will select 10 conditions (mix
chronic/acute, med/surg) Applies to hospitals (IPPS, OPPS, LTACHs),
doctors, and post-acute (IRFs, SNF, HHA)Secretary can waive statutory provisions to
better allow clinical integrationBegins 2013, for 5 years (but if successful,
Secretary to expand scope and duration indefinitely

• Approach to providing comprehensive primary care in a coordinated manner
• ACA grants for capitated payments to primary care providers organized into interdisciplinary teams.– Provide/coordinate preventive, chronic
and acute care services
• Multi-Payer Advanced Primary Care Initiative
• Hospitals play supportive role? – Convene physicians / Serve as a catalyst– Offer capital and IT infrastructure– Provide staff resources, management expertise
Patient-Centered Medical Home
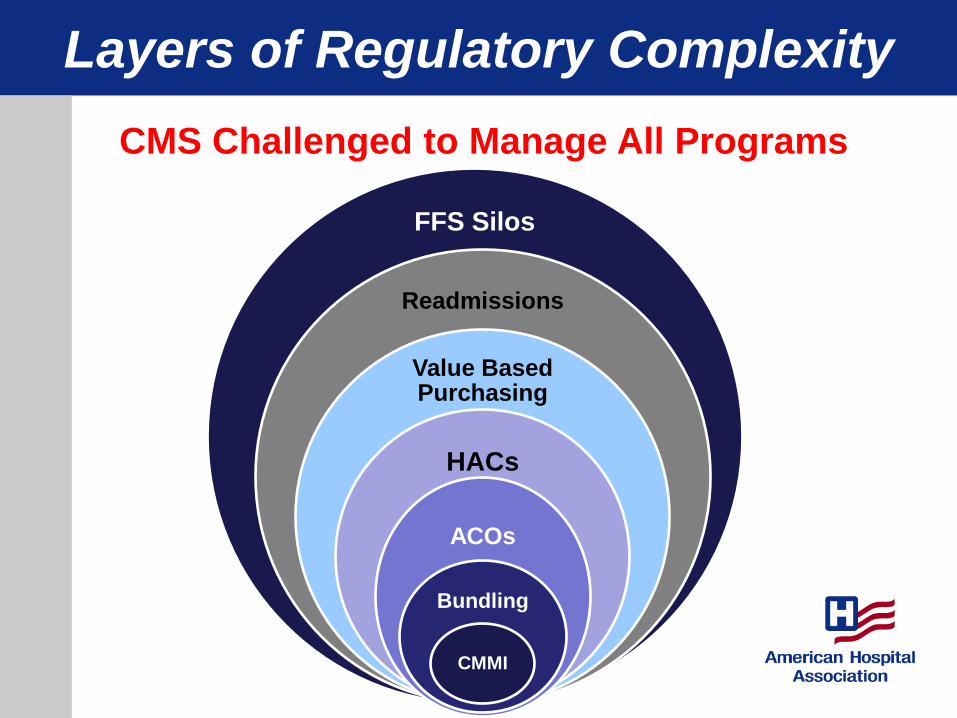
Layers of Regulatory Complexity
FFS Silos
Readmissions
Value Based Purchasing
HACs
ACOs
Bundling
CMMI
CMS Challenged to Manage All Programs

26
Physicians & Hospitals will be:
• More Integrated
• More Accountable
• More At-Risk

The Politics of Health Care Reform: Implications for Physicians
March 30, 2011












![[Alfredo Guinta] Origami Masters](https://static.fdocuments.in/doc/165x107/577cc0fa1a28aba71191cd2d/alfredo-guinta-origami-masters.jpg)





