
Washington Prescription Blank Order Form - Quill.com Prescription Blank Order Form Quill.com is an...
3
Washington Prescription Blank Order Form Quill.com is an approved vendor for Washington State security prescription blanks. Washington Rx blank security features: • “Void” pantograph if photocopied • Security features printed on front • Microprint signature line • Security watermark on back states “Security Prescriptions” • Chemical-reactant stain appears to make prescription form unusable if chemically altered • The state-approved mortar and pestle watermark Offering our highest standards in state-regulated prescription blanks in accordance with Washington state law, we have met the stringent requirements regarding written prescriptions for controlled substances and stand ready to assist you in meeting your state regulations as quickly and easily as possible. The overview below includes important facts you should know about the law. To order Washington state prescription blanks, simply fill out the order form and then mail, fax or email it to the addresses or fax number below. Our helpful telephone representatives will be happy to answer your questions before you place your written order. Call us toll-free at 800-789-1186. Overview of Requirements Effective July 1, 2010, to prevent unauthorized copying, altering and forgery of prescription forms, every prescription written in the state of Washington by a licensed practitioner must be written on tamper-resistant prescription pads or paper (TRPP) approved by the Pharmacy Board. This includes over-the-counter products dispensed with a prescription. Washington law requires that every prescription include: 1. Two signature lines for prescriber and patient information. 2. The approved seal located in bottom right of prescription form. • Seal consists of a mortar and pestle watermark with the Washington State map centered over the top • State is printed with green thermo-chromic ink that changes from green to yellow when exposed to heat or friction. It goes back to green when cooled. Washington has approved the use of board-approved tamper-resistant paper, with the seal, to be printed in the office. Prescribers are responsible for safeguarding prescription pads and paper from theft. Tamper-resistant prescription paper or pads are not required when: prescriptions are transmitted to the pharmacy electronically, by telephone or by facsimile; prescriptions are written for patients in hospitals (in-patient or out-patient), residents of nursing homes, mental health or correctional facilities; the prescriber writes the order into the patients’ medical or clinical record, the order or prescription is given directly to the pharmacy, and the patient never has the opportunity to handle the written order or prescription. COMPLETE ORDER FORM and SUBMIT TO: FAX: 800-328-0023 • MAIL: Quill Corporation, P.O. Box 94080, Palatine, II 60094 EMAIL: [email protected] If you have any questions, call 800-789-1186 © 2015, Quill Lincolnshire, Inc. 15497
Transcript of Washington Prescription Blank Order Form - Quill.com Prescription Blank Order Form Quill.com is an...

Washington Prescription Blank Order FormQuill.com is an approved vendor for
Washington State security prescription blanks.
Washington Rx blank security features:• “Void” pantograph if photocopied
• Security features printed on front
• Microprint signature line
• Security watermark on back states “Security Prescriptions”
• Chemical-reactant stain appears to make prescription form unusable if chemically altered
• The state-approved mortar and pestle watermark
Offering our highest standards in state-regulated prescription blanks in accordance with Washington state law, we have met the stringent requirements regarding written prescriptions for controlled substances and stand ready to assist you in meeting your state regulations as quickly and easily as possible.
The overview below includes important facts you should know about the law. To order Washington state prescription blanks, simply fi ll out the order form and then mail, fax or email it to the addresses or fax number below. Our helpful telephone representatives will be happy to answer your questions before you place your written order. Call us toll-free at 800-789-1186.
Overview of RequirementsEffective July 1, 2010, to prevent unauthorized copying, altering and forgery of prescription forms, every prescription written in the state of Washington by a licensed practitioner must be written on tamper-resistant prescription pads or paper (TRPP) approved by the Pharmacy Board. This includes over-the-counter products dispensed with a prescription.
Washington law requires that every prescription include:1. Two signature lines for prescriber and patient information.2. The approved seal located in bottom right of prescription form.
• Seal consists of a mortar and pestle watermark with the Washington State map centered over the top
• State is printed with green thermo-chromic ink that changes from green to yellow when exposed to heat or friction. It goes back to green when cooled.
Washington has approved the use of board-approved tamper-resistant paper, with the seal, to be printed in the offi ce. Prescribers are responsible for safeguarding prescription pads and paper from theft.
Tamper-resistant prescription paper or pads are not required when: prescriptions are transmitted to the pharmacy electronically, by telephone or by facsimile; prescriptions are written for patients in hospitals (in-patient or out-patient), residents of nursing homes, mental health or correctional facilities; the prescriber writes the order into the patients’ medical or clinical record, the order or prescription is given directly to the pharmacy, and the patient never has the opportunity to handle the written order or prescription.
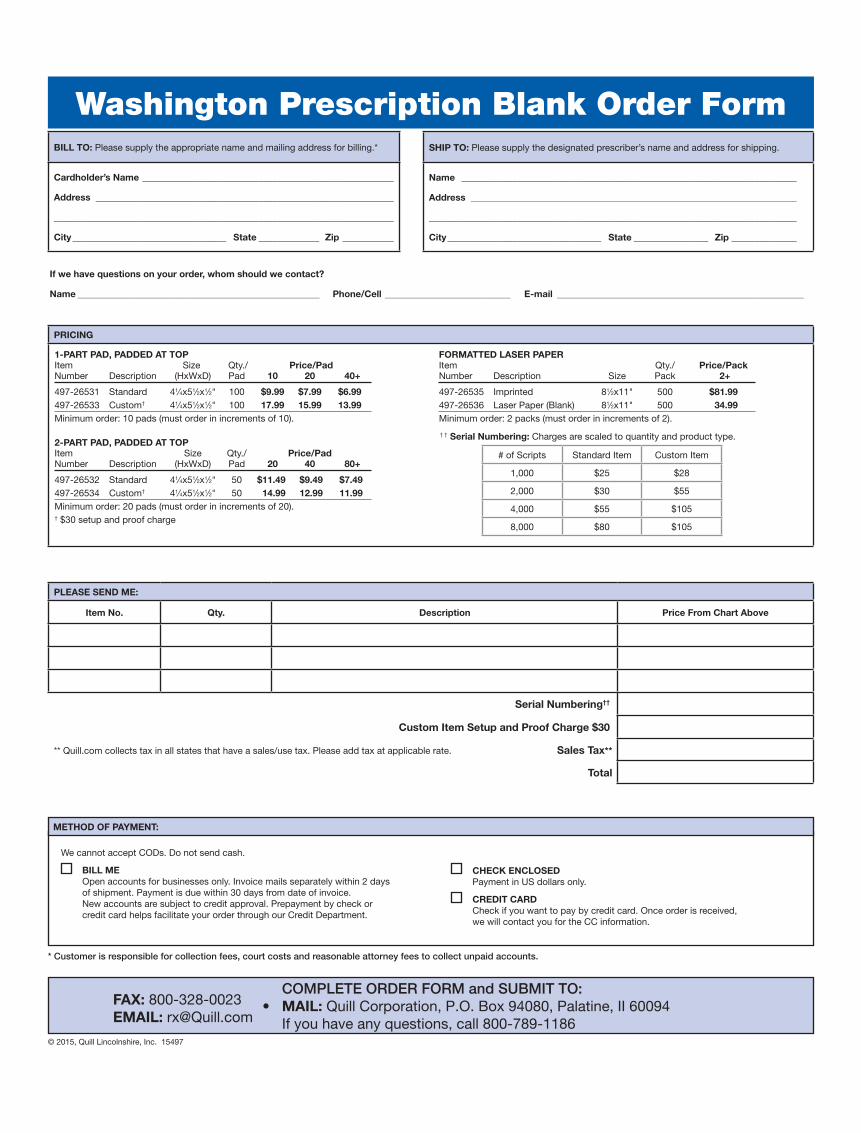
COMPLETE ORDER FORM and SUBMIT TO: FAX: 800-328-0023 • MAIL: Quill Corporation, P.O. Box 94080, Palatine, II 60094 EMAIL: [email protected] If you have any questions, call 800-789-1186© 2015, Quill Lincolnshire, Inc. 15497
Wash
ingto
n P
resc
ripti
on B
lank O
rder
Form
COMPLETE ORDER FORM and SUBMIT TO: FAX: 800-328-0023 • MAIL: Quill Corporation, P.O. Box 94080, Palatine, II 60094EMAIL: [email protected] If you have any questions, call 800-789-1186
Washington Prescription Blank Order FormBILL TO: Please supply the appropriate name and mailing address for billing.*
Cardholder’s Name ______________________________________________________
Address ________________________________________________________________
_________________________________________________________________________
City _________________________________ State _____________ Zip ___________
SHIP TO: Please supply the designated prescriber’s name and address for shipping.
Name ________________________________________________________________________
Address ______________________________________________________________________
_______________________________________________________________________________
City _________________________________ State ________________ Zip ______________
PRICING
1-PART PAD, PADDED AT TOPItem Size Qty./ Price/PadNumber Description (HxWxD) Pad 10 20 40+
497-26531 Standard 41⁄4x51⁄2x1⁄2" 100 $9.99 $7.99 $6.99497-26533 Custom† 41⁄4x51⁄2x1⁄2" 100 17.99 15.99 13.99Minimum order: 10 pads (must order in increments of 10).
2-PART PAD, PADDED AT TOPItem Size Qty./ Price/Pad Number Description (HxWxD) Pad 20 40 80+
497-26532 Standard 41⁄4x51⁄2x1⁄2" 50 $11.49 $9.49 $7.49497-26534 Custom† 41⁄4x51⁄2x1⁄2" 50 14.99 12.99 11.99Minimum order: 20 pads (must order in increments of 20). † $30 setup and proof charge
FORMATTED LASER PAPERItem Qty./ Price/PackNumber Description Size Pack 2+
497-26535 Imprinted 81⁄2x11" 500 $81.99497-26536 Laser Paper (Blank) 81⁄2x11" 500 34.99Minimum order: 2 packs (must order in increments of 2).
PLEASE SEND ME:
Item No. Qty. Description Price From Chart Above
Serial Numbering††
Custom Item Setup and Proof Charge $30
** Quill.com collects tax in all states that have a sales/use tax. Please add tax at applicable rate. Sales Tax**
Total
† † Serial Numbering: Charges are scaled to quantity and product type.
# of Scripts Standard Item Custom Item
1,000 $25 $28
2,000 $30 $55
4,000 $55 $105
8,000 $80 $105
If we have questions on your order, whom should we contact?
Name ____________________________________________________ Phone/Cell ___________________________ E-mail _____________________________________________________
© 2015, Quill Lincolnshire, Inc. 15497
METHOD OF PAYMENT:
We cannot accept CODs. Do not send cash.
BILL ME Open accounts for businesses only. Invoice mails separately within 2 days of shipment. Payment is due within 30 days from date of invoice.
New accounts are subject to credit approval. Prepayment by check or credit card helps facilitate your order through our Credit Department.
CHECK ENCLOSED Payment in US dollars only.
CREDIT CARD Check if you want to pay by credit card. Once order is received,
we will contact you for the CC information.
* Customer is responsible for collection fees, court costs and reasonable attorney fees to collect unpaid accounts.

IMP
OR
TAN
T: T
he in
form
atio
n re
que
sted
bel
ow m
ust
be
fille
d o
ut in
ord
er fo
r us
to
pro
cess
you
r or
der
.
• Li
cens
e nu
mb
er is
req
uire
d fo
r p
rinte
r va
lidat
ion.
Pre
-prin
ting
the
num
ber
on
your
bla
nks
is o
ptio
nal
•
DE
A n
umb
er is
op
tiona
l. If
pro
vid
ed, w
e w
ill p
re-p
rint
the
num
ber
on
your
Rx
bla
nks
PR
ES
CR
IBE
R IN
FOR
MA
TIO
N: I
nfor
mat
ion
liste
d b
elow
will
be
pre
-prin
ted
on
the
pad
s.
Nam
eD
egre
eLi
cens
e #
(Op
tiona
l)D
EA
#(O
ptio
nal)
Thank Y
ou
for
Your
Ord
er
OP
TIO
NS: re
view
sam
ple
for
addit
ional opti
ons
ava
ilable
Lab
elin
g In
fo:
Bla
nk R
efill
NR
1 2
3 4
5
Refi
ll __
_ tim
es R
EFI
LL -
0 -
1 -
2 -
3 -
4 -
PR
N S
pan
ish
Che
ck B
ox V
oid
Aft
er _
____
____
__P
atie
nt In
fo:
DO
B M
/FB
od
y P
rint
: Q
uant
ity C
heck
Box
es P
re-p
rint
regu
lar
non-
sche
dul
ed p
resc
riptio
n
info
rmat
ion.
Ple
ase
pro
vid
e te
xt a
nd la
yout
. S
eria
l Num
ber
ing
Sta
rtin
g #
____
____
____
____
_N
ote:
Cha
rges
ap
ply
to
this
op
tion.
Ple
ase
refe
r to
pric
e ch
art.
CLI
NIC
NA
ME
/AD
DR
ES
S/P
HO
NE
INFO
RM
AT
ION
: Ple
ase
det
ail w
hat
you
wan
t p
re-p
rinte
d o
nly
(or
atta
ch a
sam
ple
).
LIC
EN
SE
# R
equi
red
fo
r P
rint
er V
alid
atio
n(in
clud
ing
bla
nk la
ser
pap
er):
Des
igna
ted
Pre
scri
ber
Nam
e:Li
cens
e #
Wash
ingto
n P
resc
ripti
on B
lank O
rder
Form
SE
ND
FR
EE
PR
OO
F T
O: (
char
ges
ap
ply
to
cus
tom
item
s o
nly)
Fax
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
E-m
ail
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
C
OM
PLE
TE
OR
DE
R F
OR
M a
nd S
UB
MIT
TO
:
FAX
: 800
-328
-002
3 •
MA
IL: Q
uill
Cor
por
atio
n, P
.O. B
ox 9
4080
, Pal
atin
e, II
600
94
EM
AIL
: rx@
Qui
ll.co
m
If
you
have
any
que
stio
ns, c
all 8
00-7
89-1
186
© 2
015,
Qui
ll Li
ncol
nshi
re, I
nc.
1549
7
If we have questions on your order, whom should we contact?
Name ____________________________________________________ Phone/Cell ___________________________ E-mail _____________________________________________________


















