
Vulval Dermatology - parksideprimaryfirst.co.uk · Painful vulval conditions ... Erosive LP of...
51
Vulval Dermatology
Transcript of Vulval Dermatology - parksideprimaryfirst.co.uk · Painful vulval conditions ... Erosive LP of...

Vulval Dermatology
Lichen sclerosus
Lichen planus
Eczema / lichen simplex
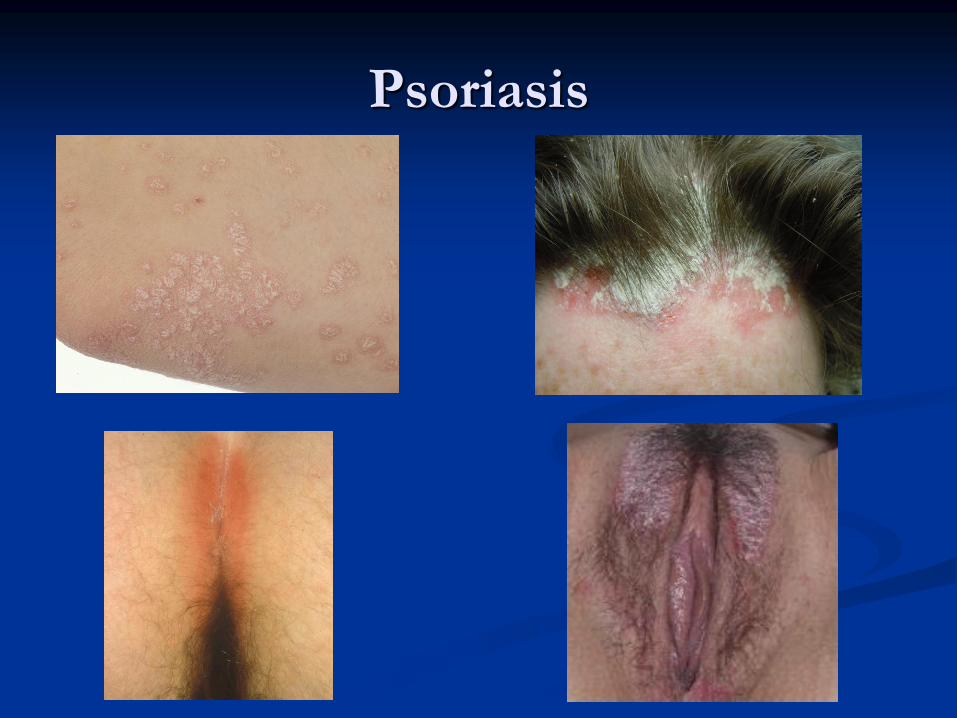
Psoriasis
Sebopsoriasis
Painful vulval conditions
Vulvovaginitis in children
Incidental lesions
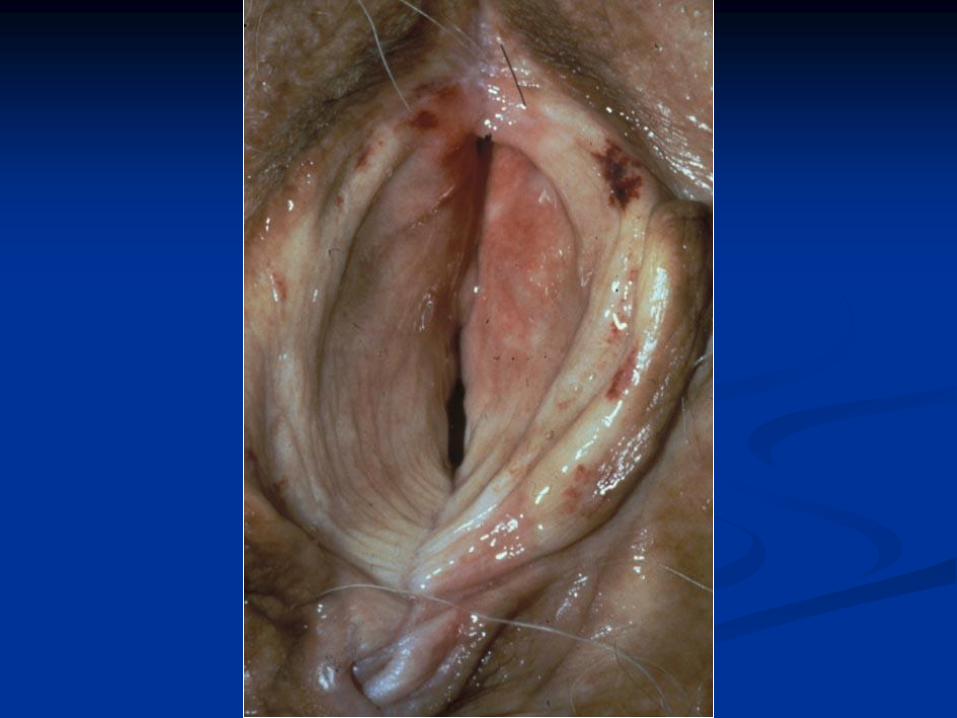
Lichen sclerosus
Onset 45 to 60 years but can occur in childhood
(Up to 15% onset before 13 years)
In children onset 3 to 6 years
Pruritus common but may be asymptomatic
May be sore +/- dyspareunia
Occasionally spontaneous resolution occurs,
particularly in girls around the menarche (25%)






Extra-genital lichen sclerosus
Affects 10% of woman with vulval LS
94% of patients with extra-genital LS will have
genital involvement
Most common on the trunk, particularly flexures
Pruritus uncommon, usually asymptomatic
Atrophic (cigarette paper) skin and bruising
common



Treatment of lichen sclerosus of
vulva
Dermovate ointment nightly 1 month then
alternate nights one month
Soap substitute
Children
Betnovate or Elocon nightly for 2 to 4 weeks
Eumovate ointment for maintenance

Lichen planus

Lichen planopilaris
Post menopausal frontal
fibrosing alopecia Pterygium




Treatment
Dermovate ointment nightly 2 – 4 weeks
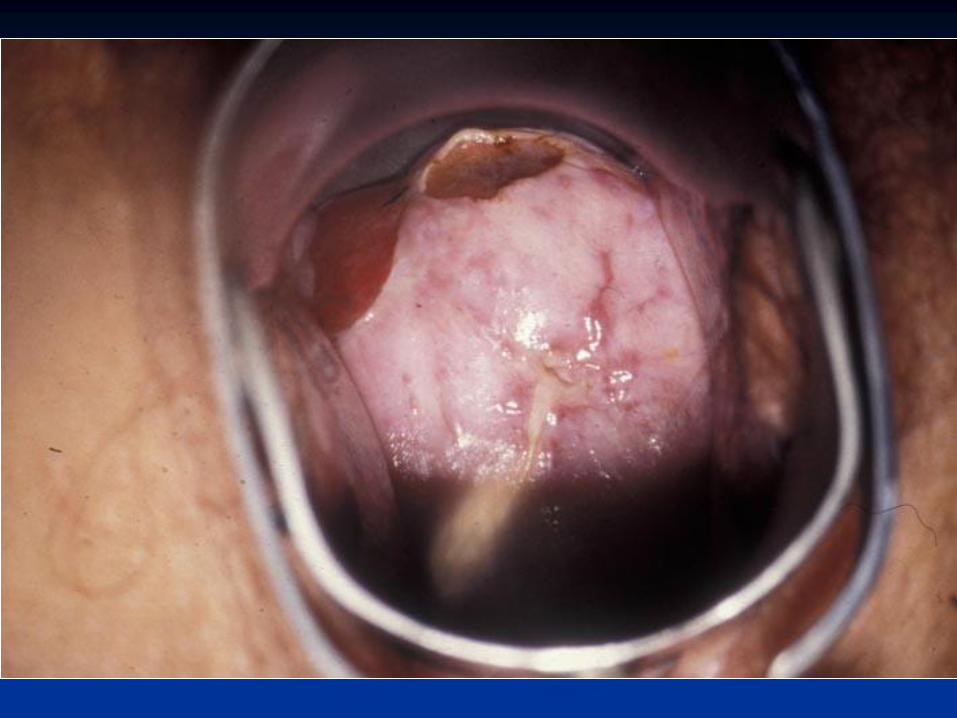
Vulvovaginal-gingival lichen
planus
Erosive LP of vulva and vagina with a
desquamating gingivitis
Chronic and painful
Discharge, dysuria, dyspareunia, post coital
bleeding
Vaginal stenosis


Treatment of VVG-LP
Dermovate nightly 2-4 weeks
Steroid foams or suppositories
Oral steroids, acitretin, methotrexate, ciclosporin and azathioprine

Eczema
Atopic eczema
Lichen simplex
Contact dermatitis
Seborrhoeic eczema/sebopsoriasis



Eczema treatment
Soap substitute
Eumovate ointment nightly
(to increase to Betnovate if more severe)



Lichen simplex treatment
Soap substitute
Betnovate ointment nightly for 2 weeks then 1
week as necessary; maximum of 1 week in 3
+/- Hydroxyzine at night initially


Contact irritant or allergic
dermatitis
Irritants – urinary incontinence, vigorous
cleaning
Allergies – fragrances, preservatives, rubber.
BUT contact allergy of the vulva is rare without
involvement of perianal skin

Fragrance ++

Seborrhoeic eczema
Psoriasis

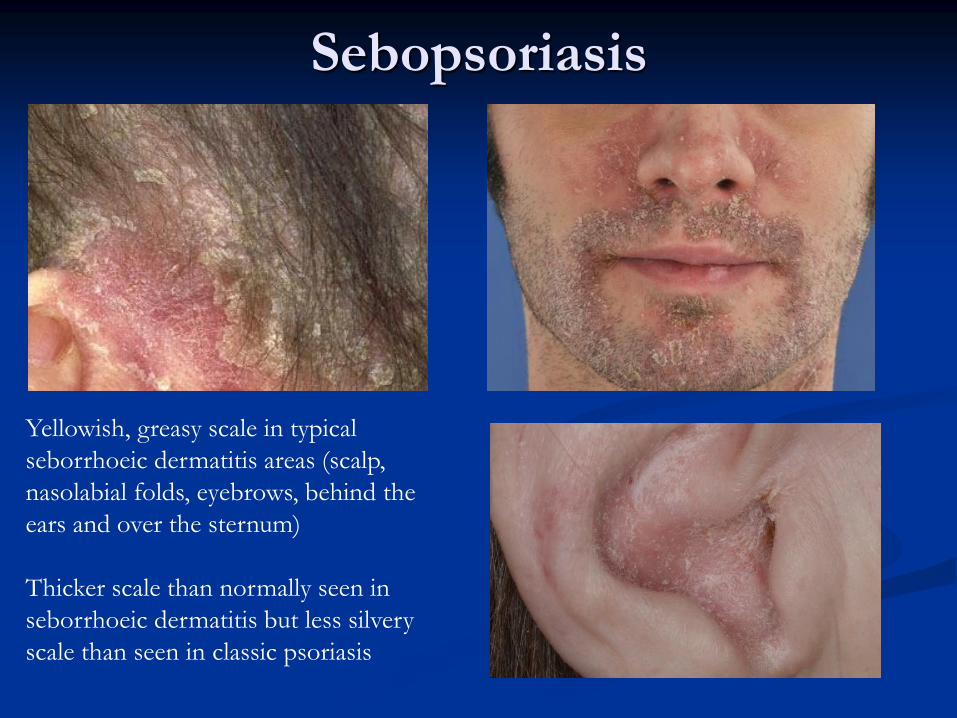
Sebopsoriasis
An overlap between seborrhoeic dermatitis and
psoriasis and has features of both conditions
Yellowish, greasy scale in typical seborrhoeic
dermatitis areas (scalp, nasolabial folds,
eyebrows, behind the ears and over the sternum)
Thicker scale than normally seen in seborrhoeic
dermatitis but less silvery scale than seen in
classic psoriasis
Sebopsoriasis
Yellowish, greasy scale in typical
seborrhoeic dermatitis areas (scalp,
nasolabial folds, eyebrows, behind the
ears and over the sternum)
Thicker scale than normally seen in
seborrhoeic dermatitis but less silvery
scale than seen in classic psoriasis

Treatment of genital or
sebopsoriasis psoriasis
Trimovate cream nightly for 1 to 2 weeks and
then for 3 nights as necessary
Warn patients it may stain clothing
Vulval pain syndromes
Dysaesthetic vulvodynia
Pain is diffuse, constant and spontaneous
Vestibulodynia
Localised pain triggered by touch
Vulval pain syndromes
Dysaesthetic vulvodynia
Post menopausal women
Depression
Vestibulodynia
Younger patients
Dyspareunia
Onset during stressful time
Anxiety common
o/e Tenderness in vestibule +/- erythema

Vulval pain syndromes - Treatment
Unrushed and sympathetic consultation
Soap substitutes and avoid irritants
5% lidocaine ointment PRN
Amitriptyline 10mg nocte increasing by 10mg
per week
Pregabalin, gabapentin, carbamazepine
Psychological help if necessary

Vulvovaginitis in children
Commonest gynaecological problem in prepubertal girls
Itching and soreness
Discharge
Dysuria
Redness of the introitus
Excoriation
Discharge
Swab introitus
Gp A Beta haemolytic streptococcus
Candida
Sexually transmitted infections
Threadworms

Vulvovaginitis
Up to 75% no cause
Avoid soaps, shower gels etc – use aqueous or
Diprobase cream
Avoid other irritants
Barrier creams eg Epaderm
Mild/moderate topical steroid

And finally…
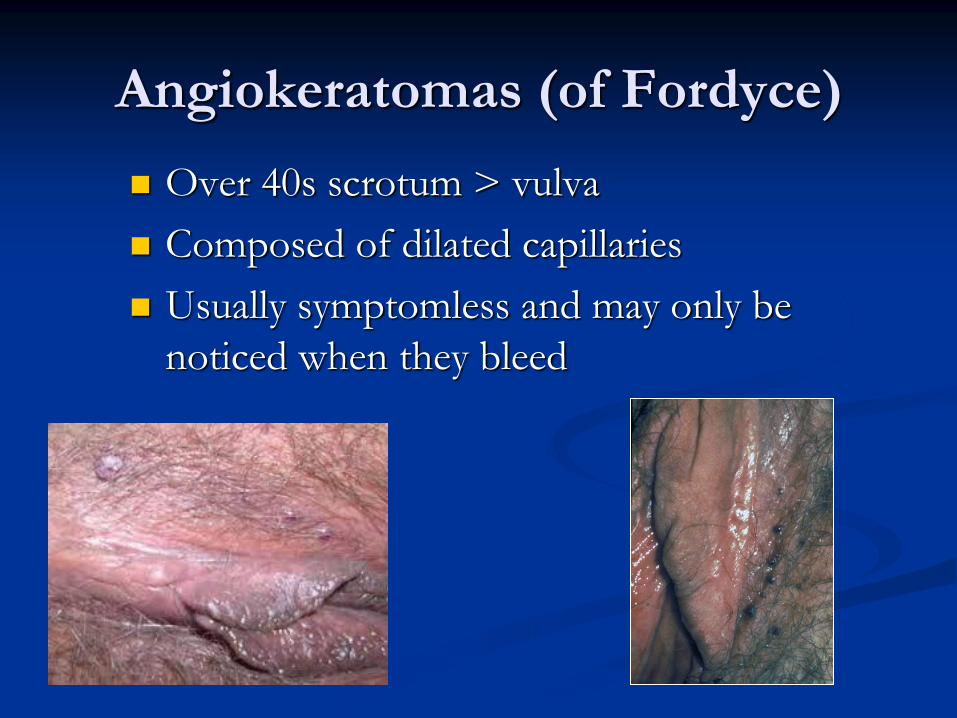
Angiokeratomas (of Fordyce)
Over 40s scrotum > vulva
Composed of dilated capillaries
Usually symptomless and may only be
noticed when they bleed
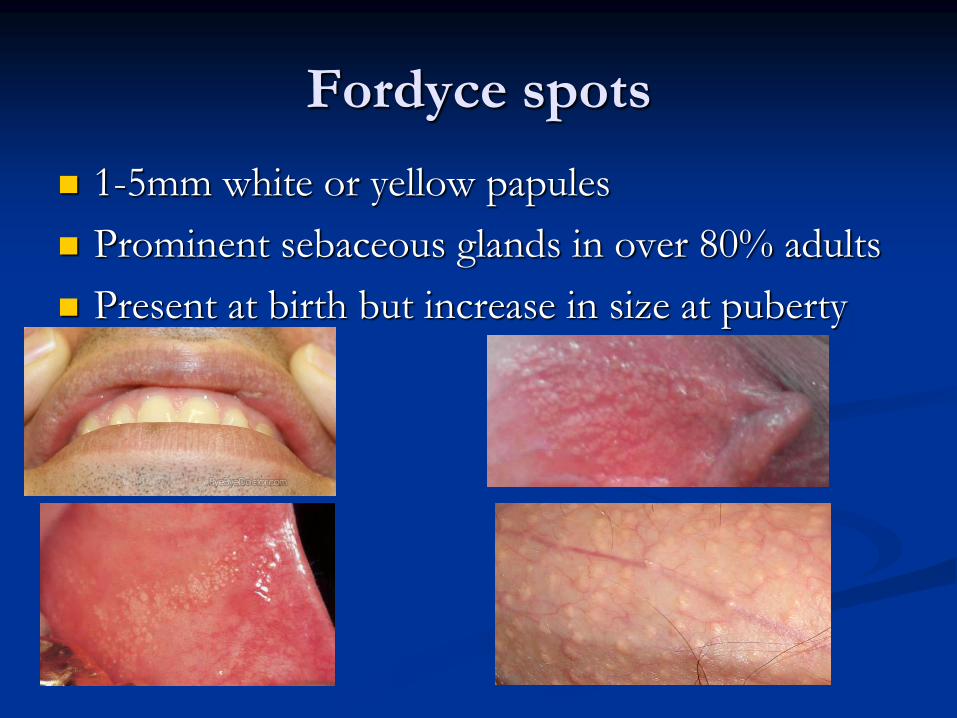
Fordyce spots
1-5mm white or yellow papules
Prominent sebaceous glands in over 80% adults
Present at birth but increase in size at puberty



















