VTE: It’s still a killer in Canada Sam Schulman, MD, PhD Dept. of Medicine McMaster University.
54
VTE: It’s still a killer in Canada Sam Schulman, MD, PhD Dept. of Medicine McMaster University
-
Upload
emerald-pitts -
Category
Documents
-
view
217 -
download
1
Transcript of VTE: It’s still a killer in Canada Sam Schulman, MD, PhD Dept. of Medicine McMaster University.

VTE: It’s still a killer in Canada
Sam Schulman, MD, PhD
Dept. of Medicine
McMaster University

Faculty/Presenter DisclosureFaculty/Presenter Disclosure
• Faculty: Dr. Sam Schulman• Program: 51st Annual Scientific
Assembly
• Relationships with commercial interests:– Grants/Research Support: N/A– Speakers Bureau/Honoraria: Boehringer
Ingelheim and Bayer Healthcare for work in study-related committees
– Consulting Fees: N/A– Other: N/A

Disclosure of Commercial Disclosure of Commercial SupportSupport
• This program has received financial support from Boehringer Ingelheim and Bayer Healthcare in the form of Honorarium.
• This program has received in-kind support from N/A
Potential for conflict(s) of interest:– Dr. Sam Schulman has received Honorarium from Bayer
Healthcare and Boehringer Ingelheim whose products are being discussed in this program.
– Bayer Healthcare and Boehringer Ingelheim sell products that will be discussed in this program: rivaroxaban and dabigatran.

Mitigating Potential BiasMitigating Potential Bias
• All treatment alternatives are discussed
Contents
• Case discussion
• Epidemiological data
• Who is at the highest risk
• Extended prophylaxis – when?
• Diagnosis – missing and overinterpreting
• Treatment – a lot easier now
• How long after VTE – a dilemma

Unfortunate case• 65 y.o. male, fell from ladder.• X-rays normal except for L4 burst # on CT• No bleeding, Hgb stable• Sharp back pain, remains bedridden in hospital.
On day 3 urinary problems and weakness in one leg scheduled for decompression laminectomy next day.
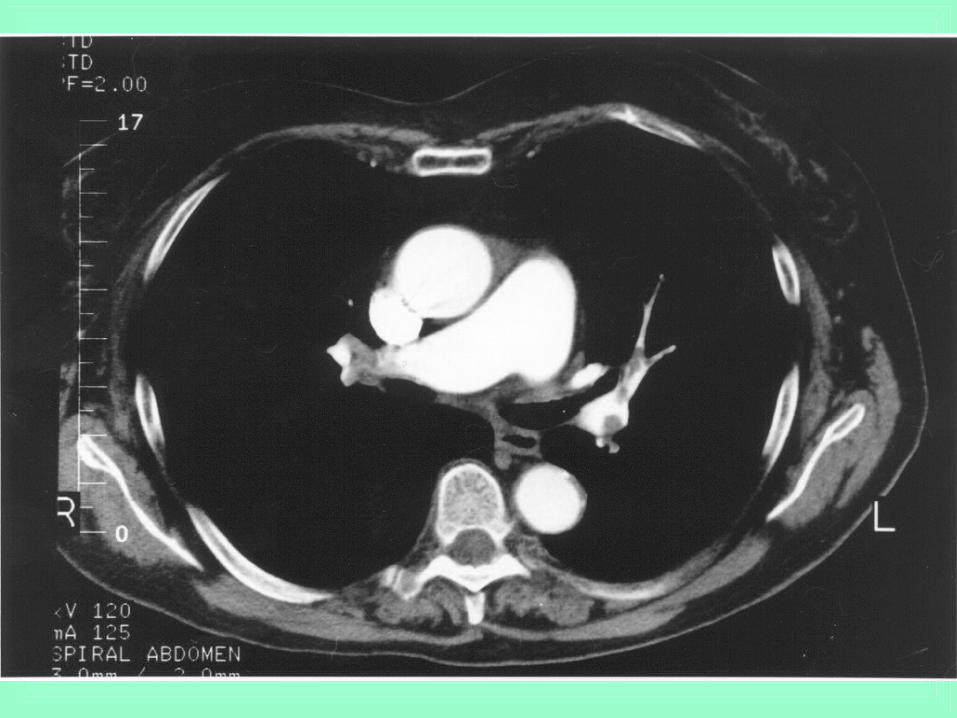
• SaO2 94-98% all the time• Surgery Day 4 in late afternoon. Suspected MI in
recovery arrest. CPR unsuccessful – large PE

PE - mortality
• 10% succumb within 1 h– Usually before arrival at the hospital
• PE – 3rd leading cause of cardiovascular death

Risk factors for VTE• Surgery• Trauma• Immobility, paresis• Malignancy• Cancer therapy • Previous VTE• Increasing age• Pregnancy / postpartum• Estrogens• Selective estrogen
receptor modulators
• Acute medical illness• Heart or respiratory
failure• Inflam. bowel disease• Nephrotic syndrome• Myeloprolif disorders• PNH• Obesity• Smoking• Varicose veins• Central venous catheter• Thrombophilic defect
ACCP Guidelines on Antithrombotic and Thrombolytic Therapy

Cancellation of Sx day after day – not an uncommon phenomenon
• Waiting time for hip# Sx often 3 days• Typical order: ”NPO for surgery in a.m.”,
”Hold heparin”• Heparin or LMWH evening before does not
increase bleeding.• These patients have to receive LMWH qHS• Even neuraxial anesthesia next morning is
OK (10-12 h after last dose)
American Society of Regional Anesthesia and Pain MedicineEvidence-Based Guidelines, 3rd ed., 2010

Postop VTE prophylaxis
• Necessary if patient not mobilizing within 24 h
• Bleeding risk – use mechanical devices
• Otherwise ”chemoprophylaxis” – usually until discharge. Consider extension if patient not mobilizing at that time point
• Use a risk assessment score, e.g. Caprini
Gould MK et al. ACCP Guidelines. CHEST 2012; 141 Suppl: 227-77

Data on incidence of VTE
• Worcester, MA – all medical records 1999 with VTE diagnosis: 104 per 100,0001
• Olmsted County, MN – medical records of all residents with VTE 1966-1990, incl PE on autopsy: 117 per 100,0002
• Sweden – Men born 1913, followed from age 50: 387 per 100,0003
• Bretagne, France – Diagnosis data: 184/100,0004
1. Spencer FA. J Gen Intern Med 20062. Silverstein MD. Arch Intern Med 19983. Hansson PO. Arch Intern Med 19974. Oger E and EPI-GETBO. Thromb Haemost 2000

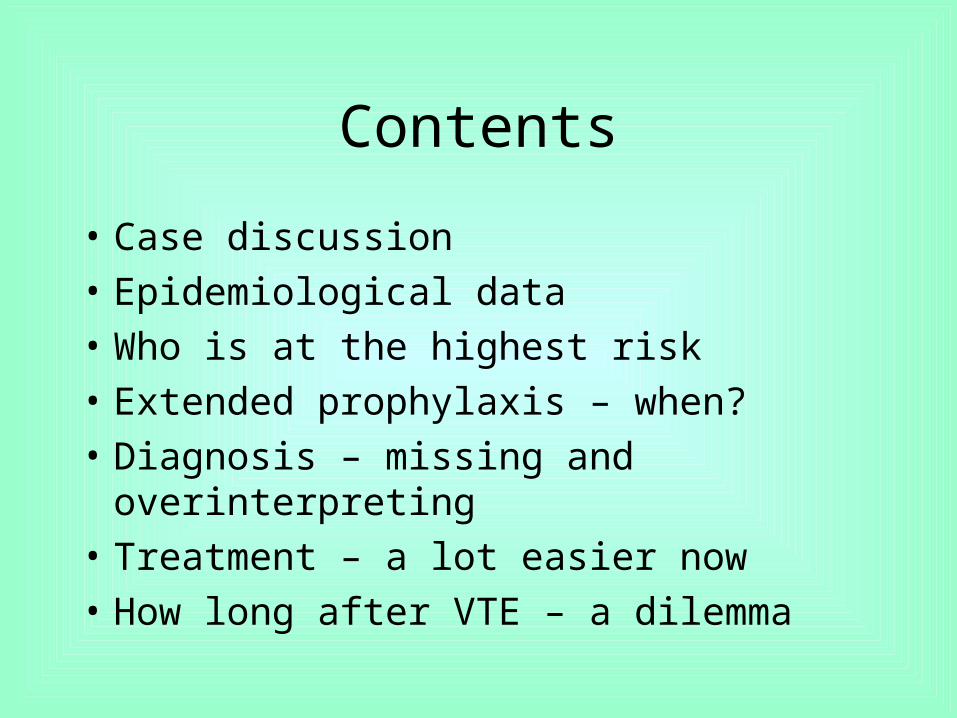
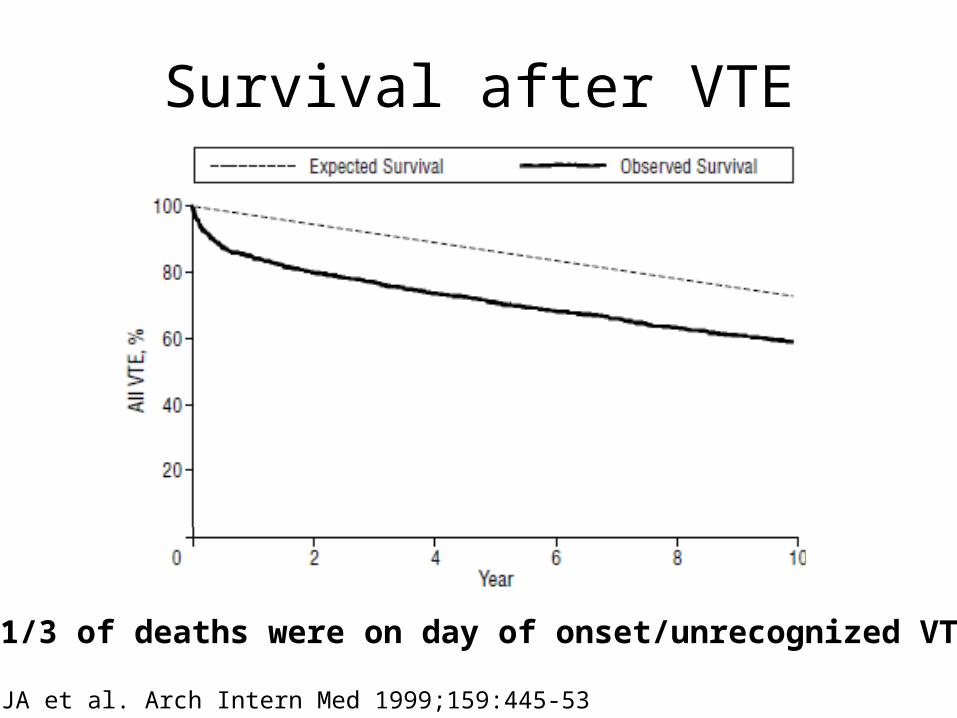
Survival after VTE
• Olmsted County inception cohort
• Followed 1966-1990, n=2218
After 7-day 30-day 1-year
DVT 96.2% 94.5% 85.4%
PE ±DVT
59.1% 55.6% 47.7%
VTE 74.8% 72.0% 63.6%
Risk factors for deathPEAgeBMIPatient location @ onsetMalignancyCHF
More risk factorsNeurologic diseaseChronic lung diseaseRecent SxHormone RxSmoking tobaccoChron renal disease
Heit JA et al. Arch Intern Med 1999;159:445-53
Survival after VTE
Heit JA et al. Arch Intern Med 1999;159:445-53
>1/3 of deaths were on day of onset/unrecognized VTE

Copyright ©2003 American Heart Association
White, R. H. Circulation 2003;107:I-4-I-8
Annual incidence of VTE among residents of Worcester MA 1986, by age and sex
Effect of age

Prevalence of VTE is predicted to double by 2050
VTE = venous thromboembolism
Deitelzweig SB et al. Am J Haematol 2011;86:217–2015
YearVTE cases per 100 000:
2002
2003
2004
2005
2006
2008
2010
2015
2020
2025
2030
2035
2040
2045
2050
317
341
371
401
422
426
432
453
478
505
527
544
556
563
567
Ad
ult
s 1
8 y
ea
rs a
nd
old
er
wit
h V
TE
in
US
A (
mil
lio
ns
)
0
0.5
1
1.5
2
2002 2003 2004 2005 2006 2008 2010 2015 2020 2025 2030 2035 2040 2045 2050

Patients at highest risk
• Recent VTE
• Malignancy
• Spinal cord injury
• Heparin-induced thrombocytopenia

Increased prophylactic dose
• Spinal cord injury
• Burn injury
• Bariatric surgery

Bariatric surgery
• >100,000 procedures in the US
• Incidence of reported VTE 0.1% - 1%, fatal PE 0.2%
• Mainly after discharge
• 95% of US surgeons give prophylaxis
• LMWH, UFH tid or fondaparinux: May add mechanical.
• Higher doses than standard
Consecutive patients 1979-2000Early ambulation & mechanical proph.
Group 1: enoxaparin 30 mg bid (n=92)DVT 5.4%
Group 2: enoxaparin 40 mg bid (n=389)DVT 0.6%
Scholten DJ et al. Obes Surg 2002;12:19-24
Consecutive patients 1979-2000Early ambulation & mechanical proph.
Group 1: enoxaparin 30 mg bid (n=92)DVT 5.4%
Group 2: enoxaparin 40 mg bid (n=389)DVT 0.6%
Scholten DJ et al. Obes Surg 2002;12:19-24

Extended postop prophylaxis,i.e. up to 1 month instead of 1 week
1. High risk of VTE + pelvic/abdominal Sx for cancer (Grade 1B)
a) Results in 13 fewer non-fatal events per 1000 without significant increase in bleeding
2. Major orthopedic surgery (THR, TKR, HFS) – minimum 10-14 d (Grade 1B) and suggest up to 35 d (Grade 2B)
a) Results in 9 fewer non-fatal events per 1000 without significant increase in bleeding
ACCP Guidelines. CHEST 2012; 141 Suppl

Spinal cord injury
• In case of paraplegia:
• Very high risk at least first month
• Continued increased risk 3 months
• Then normalization

Logistics not an excuse now
• LMWH/fondaparinux are parenteral.
• Rivaroxaban 10 mg or dabigatran 150/220 mg once dailyor apixaban 2.5 mg twice dailyare available and approved for THR and TKR
• Effective and safe, cost-effective vs LMWH

The Primary Outcomes – Ortho Sx• RE-MODEL TKR Non-inferior
• RE-MOBILIZE TKR Inferior
• RE-NOVATE THR Non-inferior
• RE-NOVATE II THR Non-inferior
• RECORD 1 THR Superior
• RECORD 2 THR Superior
• RECORD 3 TKR Superior
• RECORD 4 TKR Superior
• ADVANCE 1 TKR Non-inferiority not met
• ADVANCE 2 TKR Superior
• ADVANCE 3 THR Superior
Dabi
Riva
Apixa

Suspected DVT / PE

Typical case
• 36 y.o. lady with pain in the R calf x 3d
• Previously healthy
• Went for a long walk last weekend
• Was on COC for 10 years, stopped at age 28, restarted 3 months ago.
• Physical: Tender calf, no edema or SOB

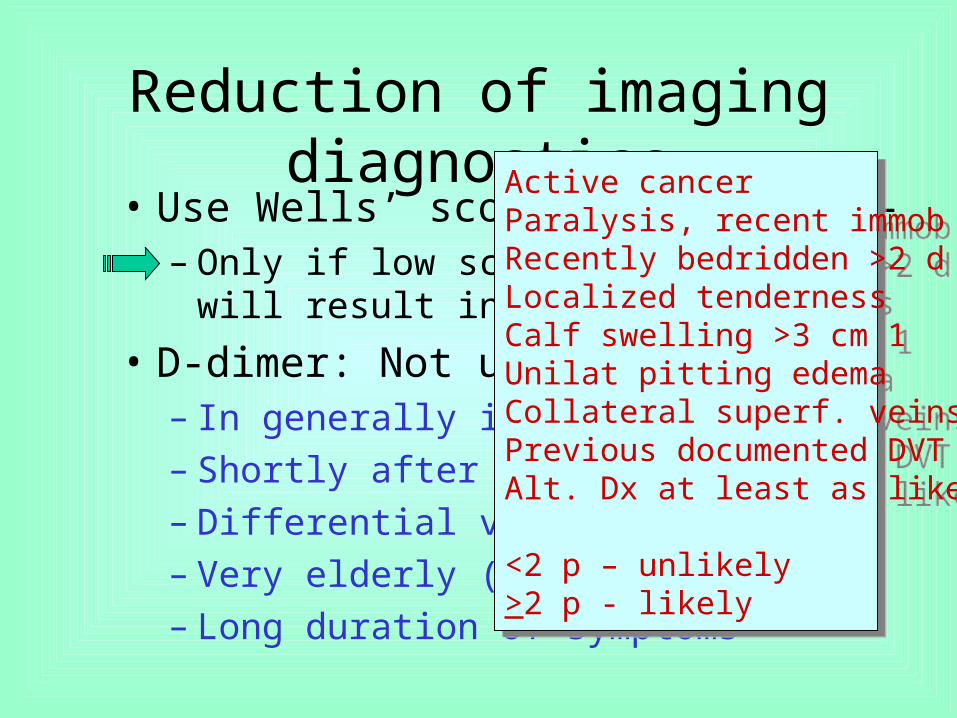
Reduction of imaging diagnostics• Use Wells’ score and D-dimer –
– Only if low score + neg D-dimer will result in No imaging
• D-dimer: Not useful– In generally ill patients– Shortly after surgery– Differential vs cellulitis– Very elderly (>80)– Long duration of symptoms
Active cancer 1Paralysis, recent immob 1Recently bedridden >2 d 1Localized tenderness 1Calf swelling >3 cm 1Unilat pitting edema 1Collateral superf. veins 1Previous documented DVT 1Alt. Dx at least as likely -2
<2 p – unlikely>2 p - likely
Active cancer 1Paralysis, recent immob 1Recently bedridden >2 d 1Localized tenderness 1Calf swelling >3 cm 1Unilat pitting edema 1Collateral superf. veins 1Previous documented DVT 1Alt. Dx at least as likely -2
<2 p – unlikely>2 p - likely

Ultrasound pitfalls
• Very difficult to tell new from old if no comparison
• If proximal swelling – ask for iliac and inferior v cava veins
• Should do both legs even if unilat spt

Do we have to treat distal DVT?Analysis of 5 studies of sympt calf DVT
without treatment (Rhigini et al 2006): Progression proximally in 25 of 353 (7%)
RCT (N=196):
VKA alone
UFH 5,000 x2
UFH 12,000 x1
Placebo
11% 11% 7% 78%
2.3% 2.3% 0% 25%
Progression0-8 w
9-24 w(ultrasound)
Belcaro G et al. Minerva Med 1997;88:507-14

Calf DVT: Risk factors for progression
• Positive D-dimer
• Extensive calf DVT or close to proximal
• Unprovoked or persistent risk factor
• Active cancer
• History of VTE
• Hospitalized patient
Kearon C et al. ACCP Guidelines. CHEST 2012; 141 Suppl

Practical approach
• Treat if very symptomatic or risk factors for extension (Grade 2C)
• With increasing risk of bleeding – consider not treating – but do serial ultrasound. (Grade 2C)Progression is most common first 2 w.
Kearon C et al. ACCP Guidelines. CHEST 2012; 141 Suppl
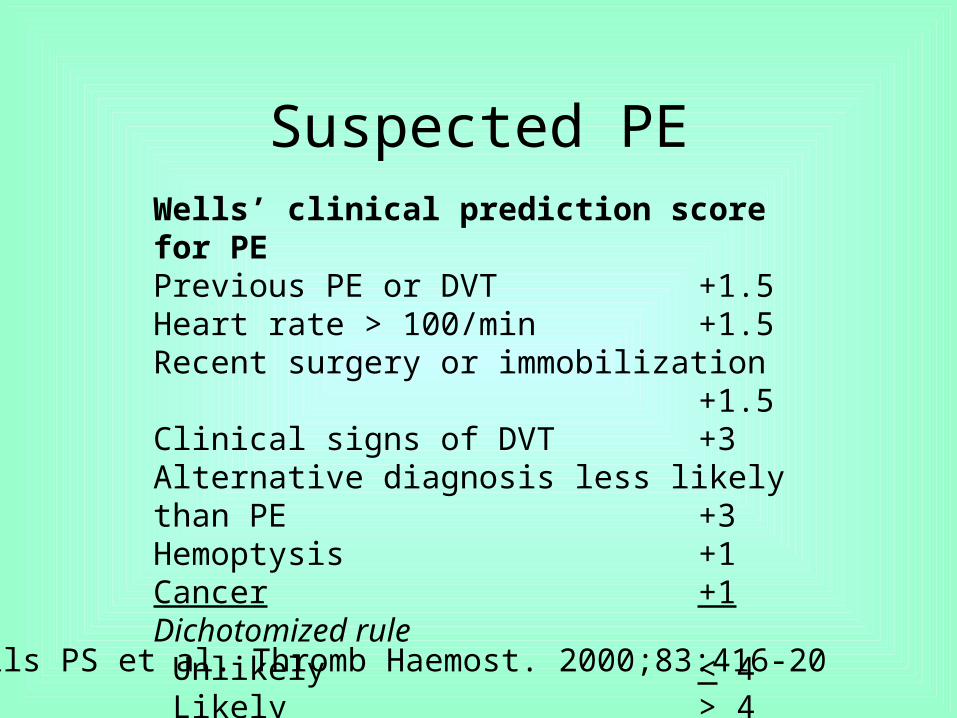
Suspected PEWells’ clinical prediction score for PEPrevious PE or DVT +1.5Heart rate > 100/min +1.5Recent surgery or immobilization +1.5Clinical signs of DVT +3Alternative diagnosis less likely than PE +3Hemoptysis +1Cancer +1Dichotomized rule Unlikely < 4 Likely > 4
Wells PS et al. Thromb Haemost. 2000;83:416-20

Clinical probability assessment
Low or intermediate High
D-dimer
Below cut-off Above cut-off
CUS 1 or MDCTA 2
Negative 3 Positive
No anticoagulant therapy Anticoagulant therapy

Can my PE-patient in ER go home?
• Pulmonary Embolism Severity Index (PESI)– Age 1 p / yr SBP <100 30 p– Male sex 10 p Pulse >110 20 p– Cancer 30 p RR>30 20 p– CHF 10 p Temp <36 20 p– Chron lung dis. 10 p SaO2 <90% 20 p mental status 60 p
Aujesky D et al. Am J Resp Crit Care Med 2005;172:1041–6 External validation in: J Intern Med 2007;261:597-604
85 p or less = low risk of fatal PE – NPV = 99%
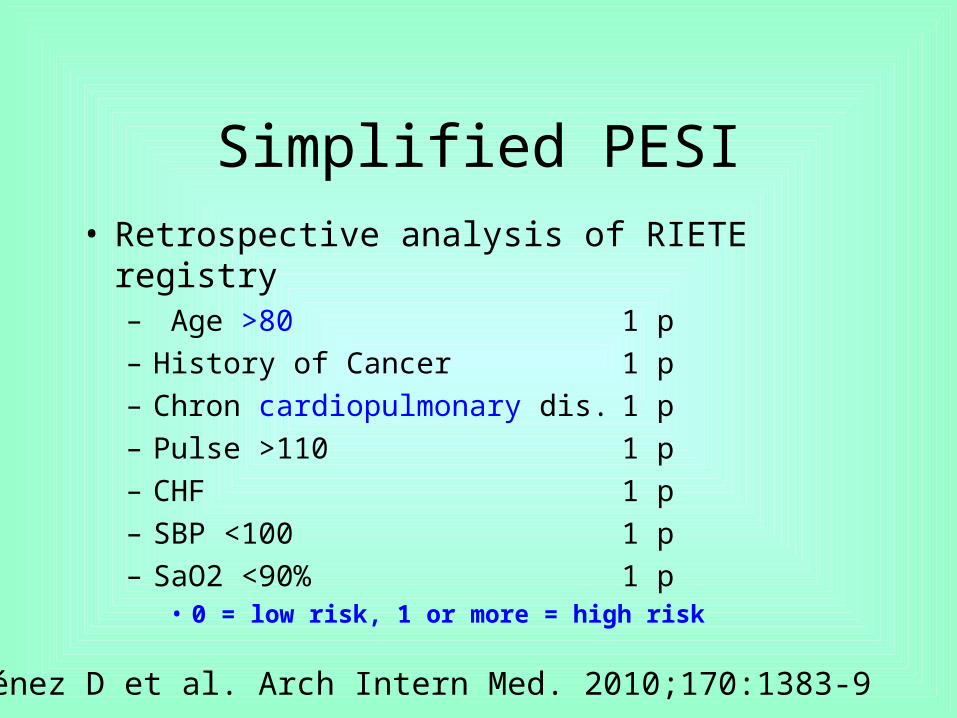
Simplified PESI• Retrospective analysis of RIETE registry
– Age >80 1 p– History of Cancer 1 p– Chron cardiopulmonary dis. 1 p– Pulse >110 1 p– CHF 1 p– SBP <100 1 p– SaO2 <90% 1 p
• 0 = low risk, 1 or more = high risk
Jiménez D et al. Arch Intern Med. 2010;170:1383-9

Simplified PESI result
Jiménez D et al. Arch Intern Med. 2010;170:1383-9

Initial standard anticoagulation• Generally same treatment for DVT and PE (=VTE):
– UFH iv – weight adjusted (bolus 80 U/kg, infusion at 18 U/kg/h)*
– UFH s.c. 250 U/kg bid *
– UFH s.c. 17,500 U bid *
– UFH s.c. 333 U/kg 1st dose, then 250 U/kg bid without monitoring
– LMWH s.c. without monitoring
– Fondaparinux s.c. 7.5 ±2.5 mg daily
– Rivaroxaban 15 mg p.o. BID x 3 w, then 20 mg q.d. – LU-code 444
* Monitored to keep anti-Xa at 0.3-0.7 IU/mL – at 6 h for s.c. 1B

FIDO-Study
Copyright restrictions may apply.
Kearon, C. et al. JAMA 2006;296:935-942.
Clinical Outcomes During the Study Period
UFH 250 U/kg bid vs LMWH 100 IU/kg bid
Event UFH LMWH
Recurrence 3.8% 3.4%
Maj Bleed 1.7% 3.4%
Any Bleed 8.3% 8.5%
Death 5.2% 6.3%
Event UFH LMWH
Recurrence 3.8% 3.4%
Maj Bleed 1.7% 3.4%
Any Bleed 8.3% 8.5%
Death 5.2% 6.3%

UFH sc in renal failure
• Increased risk of bleeding with any anticoagulant – NOACS, warfarin, LMWH, heparin
• Lack of good studies but reduce dose for– NOACS, LMWH and UFH
• UFH sc protocol @ Hamilton for CrCl <30– 1st dose 250 IU per kg– Then 200 IU per kg q 12 h.

EINSTEIN-DVTObjectively confirmed DVT without symptomatic PE
EINSTEIN-PEObjectively confirmed PE with or without symptomatic DVT
R
Predefined treatment period of 3, 6, 12 months
Rivaroxaban15 mg twice daily
Rivaroxaban20mg once daily
Randomisation
Eligible patients
N~2900
N~3300
Enoxaparin twice daily for at least 5 days, plus VKA target INR 2.5(INR range 2–3)Day 1 Day 21 Day 30
after last dose
DVT=deep vein thrombosis; INR=international normalised ratio; LMWH=low molecular weight heparinPE=pulmonary embolism; VKA=vitamin K antagonist
Oral Factor Xa inhibitor, rivaroxaban: EINSTEIN-DVT/PE

Rivaroxaban – a new optionEinstein DVT
Bauersachs R et al.NEJM 2010; 363: 2499-510
Major or clinically relevant bleeding in 8.1% per group
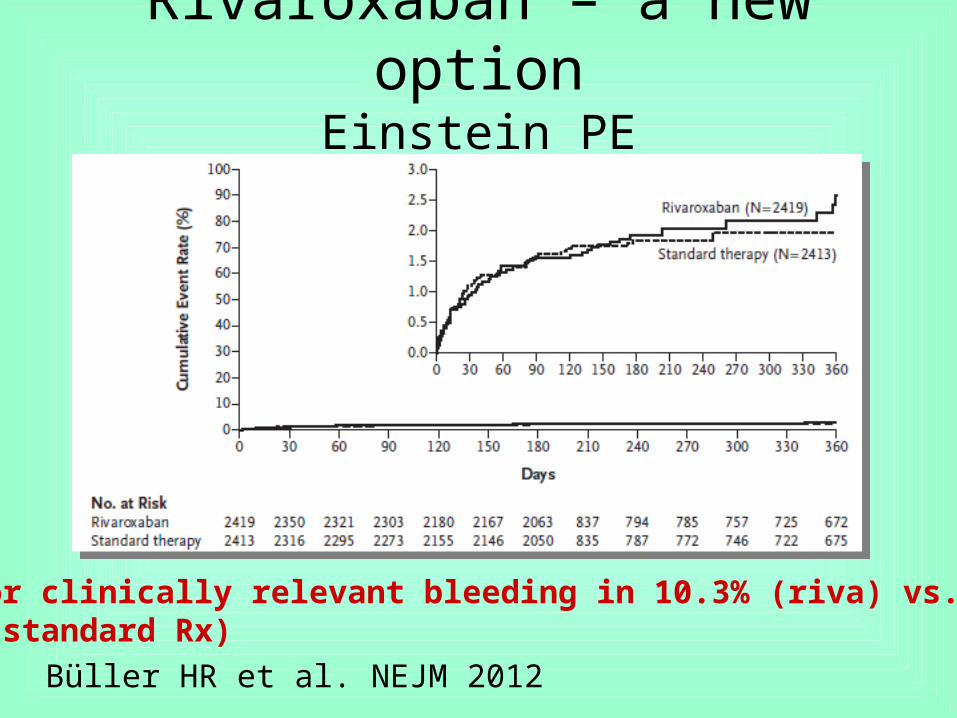
Rivaroxaban – a new optionEinstein PE
Major or clinically relevant bleeding in 10.3% (riva) vs. 11.4% (standard Rx)
Büller HR et al. NEJM 2012

Caveats for rivaroxaban
• Not for severe renal dysfunction (calc CrCl <30 mL/min)
• Few of the study patients hade extensive DVT or large PE. These patients might benefit from intial parenteral Rx.
• Dose change at 3 weeks (15 mg BID 20 mg q.d.)
• Dose with food – more reliable absorption

Standard duration of anticoagulation is now 3 m.
Schulman S et al. N Engl J Med 1995; 332: 1661-5Kearon C et al. N Engl J Med 1999; 340: 901-6
6 months? 27 months?
1A

WODIT
Months
0 3 6 9 12 15 18 21 24 27 30 33 36
Cum
ulat
ive
Haz
ard
0.00
0.05
0.10
0.15
0.20
0.25
0.30
3 months 1 year
Months
0 3 6 9 12 15 18 21 24 27 30 33 36
Cum
ulat
ive
Haz
ard
0.00
0.05
0.10
0.15
0.20
0.25
0.30
3 months 1 year
Agnelli et al. NEJM 2001

Recurrent DVT after stopping
• Patients with unprovoked DVT– 3 months Rx – 10% first year after (WODIT)
– 6 months Rx – 10% first year after (DURAC)
– 12 months Rx – 10% first year after (WODIT)
– 24 months Rx – 10% first year after (LAFIT)
• No difference 3 vs 6 months in patients with proximal DVT or PE in DOTAVK
Pinede et al: Circulation; May 27, 2001 (DOTAVK)

PE as a risk factor
HAZARD OF VTE (OFF TREATMENT)
PE at baseline NoYes
0
10
20
30
40
50
60
Time since qualifying VTE (months)
0 10 20 30 40 50
Pinede et al. ASH 2003
A meta-analysis on individual dataN=2474

Decision on long-term at 3 m
• Long-term treatment for– Unprovoked VTE– Second episode– Cancer
• Unless bleeding risk or adequate monitoring unavailable
1B

Suggestions for duration of VKA
• Proximal DVT and permanent risk or PE
3 m 6 m 12 m 24 m Indefinitely
Bleeding, Poorcompliance
Old ageNeeds ASAFemale?
Mildthrombophilicdefect /Second VTE
Third VTE or more,Severe thrombophilia,Severe venous insuff.,Pulmonary hypertension
Patient preferences

Or …
• Provoked and small DVT or small PE: 3 m
• Unprovoked small DVT: 3 m
• Unprovoked extensive DVT: 6 m
• Unprovoked extensive PE: 1 y

Elevated D-dimer
0
10
20
30
40
0 1 2 3 4
Years of follow-up
Pro
ba
bili
ty o
fre
cu
rre
nc
e (
%) EichingerH
EichingerNPalareti(idiop)HPalareti(idiop)NPalareti(thr-philia)HPalareti(thr-philia)NCosmiHCosmiN
0
10
20
30
40
0 1 2 3 4
Years of follow-up
Pro
ba
bili
ty o
fre
cu
rre
nc
e (
%) EichingerH
EichingerNPalareti(idiop)HPalareti(idiop)NPalareti(thr-philia)HPalareti(thr-philia)NCosmiHCosmiN

Management strategy – unprovoked VTE
Dx
0 3-6 m +1 m
D-dimer
Pos
Neg Pos 8.9%/yr
Neg Neg 3.5%/yr
Verhovsek M. Ann Intern Med. 2008;149:481-90

D-dimer in males
• Several studies indicate that males have despite normalization of D-dimer a higher risk of recurrence.

Conclusions
• Several risk scores and risk stratification tools are available and should be used
• Diagnostic algorithm for DVT/PE is helpful• Many options for treatment of VTE exist• Decide at 3-6 months regarding stopping or
indefinite anticoagulation• Extended postoperative prophylaxis after THR,
TKR, HFS and abdominal/pelvic Sx for cancer