Vol. Prinited Simplified, Accurate Method for Antibiotic ... · Simplified, Accurate Methodfor...
8
APPUED MICROBIOLOGY, Mar., 1966 Copyright @ 1966 American Society for Microbiology Vol. 14, No. 2 Prinited in U.S.A. Simplified, Accurate Method for Antibiotic Assay of Clinical Specimens JOHN V. BENNETT, JEAN L. BRODIE, ERNEST J. BENNER, AND WILLIAM M. M. KIRBY Division of Infectious Diseases, Department of Medicine, University of Washington School of Medicine, Seattle, Washington Received for publication 27 September 1965 ABSTRACT BENNETT, JOHN V. (University of Washington School of Medicine, Seattle), JEAN L. BRODIE, ERNEST J. BENNER, AND WILLIAM M. M. KIRBY. Simplified, accurate method for antibiotic assay of clinical specimens. Appl. Microbiol. 14:170-177. 1966.-Large glass plates are used for this modified agar-well diffusion assay method, allowing up to 81 replications on a single plate. With a specially designed agar punch, it is possible to prepare the small agar wells very quickly. The saving in serum resulting from fewer replications of standards with the large plates, and the small volume of the agar wells, makes it economically feasible to use pooled human serum for the standard antibiotic solutions. Methods are described for pre- paring the standard solutions, and for providing controls for the deterioration of standards and unknowns. Procedures for preparing and maintaining the commonly used assay organisms are presented. Serum specimens are tested directly rather than diluting them to a narrow range of antibiotic concentrations. This is possible because of a procedure for calculations that recognizes the curvilinear relationship between zone sizes and antibiotic concentrations. Adaptation of this method to a number of the commonly used antibiotics is described. With this method, it has been possible to test large numbers of clinical specimens in a minimal time, and with accuracy consistently better than 10%. Antibiotic assays performed in laboratories concerned with the commercial production of antibiotics have reached a high stage of sophisti- cation and accuracy. Both cup-plate and turbidi- metric procedures are used, and large supplies of appropriate standard and unknown materials are available in simple solutions. In contrast, assays of antibiotics in specimens from patients, chiefly blood and urine, have sometimes been inaccurate and lacking in standardization for a number of reasons. Variable constituents of body fluids, limited quantities of serum available for stand- ards, lack of control of deterioration, and differ- ences in technical procedures are factors that have led to discrepancies in results of cup-plate assays. The widespread practice of using twofold serial dilutions of serum has added to the prob- lem because of the very large inaccuracies asso- ciated with this method. With both cup-plate and serum dilution methods, the reports from differ- ent clinical investigators are so variable that it is difficult to draw valid conclusions about the actual serum concentrations (micrograms per milliliter) produced by a given dose of an anti- bitotic, or to compare results obtained in different laboratories. After intensive study, we have devised a method of assay permitting the use of pooled human serum for antibiotic standards, utilizing a mini- mum of patients' serum (0.3 ml per sample), and yet providing suitable standardization so that the error is less than =4:10%. The method is an agar-well assay, and the simplicity and accuracy stem from a variety of modifications of procedures previously described (2, 3, 9). In addition, the method of plotting and calculating the results provides new concepts that further simplify the procedure. Standards and test organisms for a number of commonly used antibiotics have been worked out for this method. This procedure is readily adaptable to any laboratory, and its widespread use should greatly improve the re- liability and reproducibility of results obtained by clinical investigators. MATERIALS AND METHODS Preparation and pouring of plates. To make up to 81 uniform replications, a large (14 by 14 inches; 170 on June 5, 2020 by guest http://aem.asm.org/ Downloaded from
Transcript of Vol. Prinited Simplified, Accurate Method for Antibiotic ... · Simplified, Accurate Methodfor...

APPUED MICROBIOLOGY, Mar., 1966Copyright @ 1966 American Society for Microbiology
Vol. 14, No. 2Prinited in U.S.A.
Simplified, Accurate Method for Antibiotic Assay ofClinical Specimens
JOHN V. BENNETT, JEAN L. BRODIE, ERNEST J. BENNER,AND WILLIAM M. M. KIRBY
Division ofInfectious Diseases, Department ofMedicine, University of Washington School of Medicine,Seattle, Washington
Received for publication 27 September 1965
ABSTRACT
BENNETT, JOHN V. (University of Washington School of Medicine, Seattle),JEAN L. BRODIE, ERNEST J. BENNER, AND WILLIAM M. M. KIRBY. Simplified, accuratemethod for antibiotic assay of clinical specimens. Appl. Microbiol. 14:170-177.1966.-Large glass plates are used for this modified agar-well diffusion assay method,allowing up to 81 replications on a single plate. With a specially designed agar
punch, it is possible to prepare the small agar wells very quickly. The saving inserum resulting from fewer replications of standards with the large plates, andthe small volume of the agar wells, makes it economically feasible to use pooledhuman serum for the standard antibiotic solutions. Methods are described for pre-
paring the standard solutions, and for providing controls for the deterioration ofstandards and unknowns. Procedures for preparing and maintaining the commonlyused assay organisms are presented. Serum specimens are tested directly ratherthan diluting them to a narrow range of antibiotic concentrations. This is possiblebecause of a procedure for calculations that recognizes the curvilinear relationshipbetween zone sizes and antibiotic concentrations. Adaptation of this method to a
number of the commonly used antibiotics is described. With this method, it hasbeen possible to test large numbers of clinical specimens in a minimal time, andwith accuracy consistently better than 10%.
Antibiotic assays performed in laboratoriesconcerned with the commercial production ofantibiotics have reached a high stage of sophisti-cation and accuracy. Both cup-plate and turbidi-metric procedures are used, and large supplies ofappropriate standard and unknown materials areavailable in simple solutions. In contrast, assaysof antibiotics in specimens from patients, chieflyblood and urine, have sometimes been inaccurateand lacking in standardization for a number ofreasons. Variable constituents of body fluids,limited quantities of serum available for stand-ards, lack of control of deterioration, and differ-ences in technical procedures are factors thathave led to discrepancies in results of cup-plateassays. The widespread practice of using twofoldserial dilutions of serum has added to the prob-lem because of the very large inaccuracies asso-ciated with this method. With both cup-plate andserum dilution methods, the reports from differ-ent clinical investigators are so variable that it isdifficult to draw valid conclusions about theactual serum concentrations (micrograms permilliliter) produced by a given dose of an anti-
bitotic, or to compare results obtained in differentlaboratories.
After intensive study, we have devised a methodof assay permitting the use of pooled humanserum for antibiotic standards, utilizing a mini-mum of patients' serum (0.3 ml per sample), andyet providing suitable standardization so thatthe error is less than =4:10%. The method is anagar-well assay, and the simplicity and accuracystem from a variety of modifications of procedurespreviously described (2, 3, 9). In addition, themethod of plotting and calculating the resultsprovides new concepts that further simplify theprocedure. Standards and test organisms for anumber of commonly used antibiotics have beenworked out for this method. This procedure isreadily adaptable to any laboratory, and itswidespread use should greatly improve the re-liability and reproducibility of results obtainedby clinical investigators.
MATERIALS AND METHODS
Preparation and pouring of plates. To make up to81 uniform replications, a large (14 by 14 inches;
170
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

ANTIBIOTIC ASSAY OF CLINICAL SPECIMENS
35.6 by 35.6 cm) square piece of plate glass, 0.25inch (0.64 cm) thick and having a flat surface, isused for the assay plates (Fig. 1). Four glass sides areattached to the surface by epoxy resin, two oppositesides rising 1 inch (2.5 cm) and the others 0.75 inch(1.9 cm) above the surface. A 0.25-inch thick plasticcover may then be securely placed over the top of theplate and sealed to prevent drying. The inside diameterof the plate is 12 by 12 inches (30.5 by 30.5 cm).The glass is routinely prepared by swabbing with 70%ethyl alcohol containing 4% concentrated HCI byvolume after washing thoroughly with soap and water,and the inner surface is swabbed with acetone andflamed before use. Autoclaving with streaming steam(100 C) not under pressure is also feasible, providingthat cooling of the glass is allowed to take place verygradually.
The assay agar is prepared by mixing 31 g ofpowder (Difco nutrient agar, 1.5%) with 1,080 ml ofdistilled water in a large flask, placing the flask in aboiling-water bath until the medium is clear, and dis-pensing the medium in four smaller flasks (270 mleach). Evaporation occurs during autoclaving so thatabout 250 ml remain from an original 270 ml. Aftersterilization, flasks containing 250 ml of melted agarare placed in a water bath at 56 C to maintain a liquidstate until poured. To provide a layer which is uni-formly about 2.7 mm deep, 250 ml of seeded agar(see section on Assay organisms) is poured onto an
assay plate which rests on a special pouring surface.This is a large rectangular piece of hardwood 1.5inches (3.8 cm) thick that can be leveled by adjustingfour threaded metal bolts which are attached to thebottom.
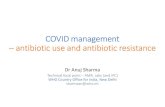
Punching wells in the agar. When the seeded agarhas solidified, wells 5.5 or 4.5 mm in diameter aremade with specially designed agar punches (Fig. 2).Since the agar thickness is 2.7 mm, the approximatevolumes required to fill the wells are 0.06 and 0.04ml, respectively. Both these sizes give suitable zonediameters even with low antibiotic concentrations,and were selected for the ease with which the wellsmay be punched and filled, and the small volumesneeded to fill them. The larger sized wells (5.5 mm)are useful for extending the lower range of concen-trations measurable for antibiotics giving small zonesizes, and the smaller ones are especially useful forpediatric samples; see specific recommendations fordifferent antibiotics and test organisms in Table 1.Larger wells than these are more difficult to punch,no easier to fill, require more solution, and giveunnecessarily larger zone sizes. The tip of the speciallydesigned punch (Fig. 2) is wiped with an alcoholsponge before punching each plate. At the end of aday, the entire punch is briefly flushed with alcoholthrough the nozzle of a squeeze bottle inserted intothe mouthpiece. The excess alcohol is blown out, andthe punch is allowed to dry overnight. Contaminationcan usually be avoided with no other special precau-tions. After the punch is inserted into the agar, it istipped very slightly to break the seal at the glass sur-face. Light suction is applied and maintained as thepunch is lifted from the plate, and the plug of agar isthen easily discharged from the punch by blowinggently on the mouthpiece. With a little practice, 81wells can easily be made in 1 to 2 min, making this amuch more efficient process than placing cylinders ontop of the agar. The agar plugs are removed gently sothat adjacent agar is undisturbed and tears in the agarare rare, making the placement of a drop of meltedagar in the well unnecessary (11). Also, the usual corkbore procedure is less satisfactory, since it requires aseparate step to remove the plug after it is cut. Be-cause of its greater mobility and lack of a need for asuction pump, our instrument is probably more suit-able than an earlier one designed for this purpose (7).The wells are evenly spaced in the agar, their exact
location being determined by placing a paper guide,
Rubber tubingPlastic mouthpiece
IFubber seal
FIG. 1. Photograph of the large glass plate and plas-tic cover. As shown, 81 samples can be assayed simul-taneously.
Steel cylinder4.5 mm. diameter
Beveled cutting edge
tapered gloss tubing, 'Tapered gloss tubing, 1-
FIG. 2. Diagram of the agar punch with which agarcups can be made very rapidly.
VOL. 14, 1966 171
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

TABLE 1. Data concerning assay organisms, cup size, and antibiotic standard concentrations in serum
IntermediateDrug concn(isg or Final concn (Mg or units/ml) (mm) Assay organism
units/mi)
Ampicillin 5 0.25, 0.5, 1, 2, 4 4.5 Bacillus subtilisCephaloridine 20 1, 2, 4, 8, 16 4.5 B. subtilisCloxacillin 60 3, 6, 12, 24. 48 5.5 Sarcina luteaColistin methanesulfonate 10 0.5, 1, 2, 4, 8 5.5 Bordetella bronchisepticaDicloxacillin 60 3, 6, 12, 24, 48 5.5 S. luteaKanamycin 20 1, 2, 4, 8, 16 5.5 B. subtilisCephalothin 12.5 0.625, 1.25, 2.5, 5, 10 4.5 B. subtilisMethicillin 20 1, 2, 4, 8, 16 5.5 B. subtilisNafcillin 7 0.35, 0.7, 1.4, 2.8, 5.6 5.5 S. luteaOxacillin 20 1, 2, 4, 8, 16 5.5 S. luteaPenicillin G 5 0.25, 0.5, 1, 2, 4 4.5 B. subtilisPenicillin V 5 0.25, 0.5, 1, 2, 4 4.5 B. subtilisTetracycline and derivatives 5 0.25, 0.5, 1, 2, 4 5.5 B. cereusVancomycin 10 0.5, 1, 2, 4, 8 5.5 B. subtilis
12 by 12 inches, beneath the glass plate. Dots aremarked on the paper guides at distances of 30, 35, or40 mm, allowing a total of 81, 64, or 49 sites, cor-responding to rows and columns of 9 X 9, 8 X 8,and 7 X 7, respectively. The guides are easily de-signed, and the wells are made over each of the dots.The particular guide which is used depends on thedesired number of replications of unknowns andstandards, the number of unknowns and standards,and the maximal zone sizes expected. In general, 81wells are used for each plate, since for most clinicalmeasurements the zone sizes are not so large as torequire wider spacing.
Filling the wells. The solutions are applied to theplate with fine-tipped capillary pipettes fitted withrubber bulbs. An attempt is made to fill the wells sothat there is a slight meniscus projecting above thesurface of the agar. Slight overflow of solution ontothe surface of the seeded agar does not influence thesize or shape of the zone.
Although repeated reference is made in the litera-ture to the necessity of randomly applying solutionsto the plate (1, 6), the benefits from this procedureare slight. The greatest single factor making randomi-zation necessary is time, for zone sizes with the samesolution applied repeatedly become smaller as timeelapses. However, it takes more time to apply solutionsrandomly than to apply them in a sequential mannei',which also provides good distribution on the plate.We have found that 81 wells may be filled in 10 minby two technicians. With this scheme, both time andplate variabilities are minimized. In practice, therefore,the solutions are applied in a simple sequential fashiondown the columns, with the sequence being repeatedafter the last solution is reached. For example, tomake 5 replications of each of 5 standards and 11unknowns, the solutions are first labeled with numbers1 to 16, and a diagram is made of the places on a 9 X9 plate where each solution is to be applied (see Fig.3). Solutions 1 to 9 are marked consecutively downthe first column on the left side of the plate with solu-tion no. 1 in the top left corner. Solutions 10 to 16are marked in order down the second column from the
1 10 3 12 5 14 7 16 92 11 4 13 6 15 8 1 103 12 5 14 7 16 9 2 114 13 6 15 8 1 10 3 125 14 7 16 9 2 11 4 136 15 8 1 10 3 12 5 147 16 9 2 11 4 13 6 158 1 10 3 12 5 14 7 169 2 11 4 13 6 15 8 0
FIG. 3. Scheme for sequential addition of solu-tions to the 81 agar cups to give random distribution.
left. Solutions 1 and 2 are then used for the remainingtwo spots at the bottom of this column, with solutions3 to 11 being marked down the third column. Thisprocedure is repeated until all solutions have beenmarked down five times. The wells are then filled inthe sequence indicated in Fig. 3. The solutions areplaced in a rack in clearly marked test tubes, each con-taining a capillary pipette. It is most convenient, butnot essential, for two persons to apply the solutions,each starting on one side and meeting in the middle.
After the wells have been filled, the plastic top isfitted on the plate and tightly sealed in place withnonporous Time Tape on all four sides. This impor-tant step prevents drying along the edges of the plate,and the so-called "edge effect," which is associatedwith distinctly larger zone sizes. Incubation is carriedout at the appropriate temperature (see section onAssay organisms) for 16 to 22 hr. The plates are theninverted, and the zones are read with a caliper throughthe back of the plate to the nearest 0.1 mm. The exactlength of incubation is not critical, but should beabout 16 hr or more to allow clear zones to form.We have also found that assays may be done over theweekend with very little sacrifice of accuracy if theplates are removed from the incubator on Saturdaymoming and refrigerated (4 C) until Monday.
Assay organisms. The test organism of choice forthe assay of a given antibiotic is the one providing thegreatest accuracy with the fewest replications of anunknown (see ANALYSIS OF REsuLTs). The organism
172 BENNETT ET AL. APPL. MICROBIOL.
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

ANTIBIOTIC ASSAY OF CLINICAL SPECIMENS
must also be susceptible enough to permit a clear-cutzone of inhibition with the lowest serum concentrationof antibiotic that is clinically important. It is desirablebut not mandatory for the highest serum concentra-tion of antibiotic expected clinically to produce azone diameter no larger than 30 mm, since this mini-mizes the need to dilute samples, and permits 81replications on each plate.
Using the above criteria, we have found that manycommonly used antibiotics can be assayed satis-factorily with only two test organisms, Sarcina luteaand Bacillus subtilis (see Table 1). Antibiotics in com-mon use which cannot be satisfactorily assayed withthese two test organisms include tetracycline and itsanalogues, and colistin, which are better assayed withBacillus cereus and Bordetella bronchiseptica, respec-tively.We have simplified the usual proceduie for making
a Sarcina suspension (2). Two petri dishes (15 cmin diameter) containing nutrient agar are heavilystreaked with a large loopful of S. lutea ATCC 9341taken from a stock agar slant. After incubation at37 C for 24 hr, the entire growth of Sarcina on thesurface of one plate is scraped off with a wire loopand placed in a flask containing 100 ml of chilledTryptose Phosphate Broth (Difco). The optical den-sity of the suspension is read on a Coleman Juniorspectrophotometer and adjusted to 0.47 at 550 m,by either adding additional organisms from the secondplate or by diluting with Tryptose Phosphate Broth.Unless needed for this purpose, the second plate isdiscarded. The suspension is dispensed in 2-mlamounts in many small vials which are kept in arefrigerator (4 C). Each vial is used once and dis-carded, thus avoiding contamination. A given sus-pension will prove useable for 4 to 6 weeks, and theproblems associated with daily transfers of freshcultures are obviated. For performing assays, 0.7 mlof well-shaken suspension is added to 250 ml ofmelted agar and mixed by swirling just before pour-ing the plate. All assays which use Sarcina are in-cubated at 37 C, since zones are more clear-cut thanat 30 C.
B. subtilis suspensions are made by adding thecontents of two vials of Subtilis Spore Suspension(Difco) to 100 ml of sterile normal saline and 2.5 mlof solution (Abbott potassium phosphate, 40 meq)containing 0.3825 g of dibasic and 0.0833 g of mono-basic potassium phosphate to give a final pH of 7.4.Samples of 2-ml volume are placed in separate vialsand refrigerated. A suspension will be satisfactoryfor 4 weeks of assay. For 250 ml of agar, 0.8 ml ofsuspension is added, and incubation is carried outat 30 C, since in this instance zone sizes are cleaierat this temperature.A Bordetella bronchiseptica (ATCC 4617) suspen-
sion may be prepared with great simplicity. From a16-hr-old culture in broth, 10 ml is removed anddiluted 1:10 with chilled Tryptose Phosphate Broth.The optical density is then adjusted to 0.10 at 550m,u (Coleman Junior spectrophotometer) by addingeither more culture or chilled broth. This solution isthen dispensed into small vials in 2-ml amounts andkept refrigerated (4 C) until used. A suitable inoculum
is 0.5 ml of well-shaken suspension per 250 ml ofagar. This suspension is satisfactory for at least 4weeks. Incubation temperature for the seeded agaris 37 C.A Bacillus cereus (ATCC 11778) suspension may be
made in the same general manner as that describedfor S. lutea. One drop of a 20-hr broth culture isspread evenly over the surface of a 9-cm petri dishwhich contains blood-agar. After 16 to 20 hr of in-cubation at 30 C, one-half the growth on the platesurface is mechanically scraped off with a wire loopand placed in a bottle containing 100 ml of chilledTryptose Phosphate Broth and mixed by pipette, thenthoroughly shaken. The optical density of the sus-pension is adjusted to 0.30 at 550 m,u on a ColemanJunior spectrophotometer either by adding morebacteria from the remaining half of the plate or byadditional dilution with chilled Tryptose PhosphateBroth. The suspension is dispensed into 2-ml volumesinto several small vials and refrigerated (4 C) untilused. A suitable inoculum is 1.2 ml per 250 ml ofagar. Incubation is carried out at 30 C.We do not use base and seed layers for the four
assay organisms mentioned above, since each of thesetest organisms gives well-defined zones of inhibitionwhen only one agar layer is used. Staphylococcusaureus produces marked "coning" when inoculatedin a single layer of agar 2.7 mm thick, and a seed layeris essential for sharp zones. We have found this or-ganism to be inferior to the others, and rarely use it.
Antibiotic standards. Standard powders of knownpotency are dried if necessary according to directions(4), and convenient amounts are accurately weighedand dissolved in a suitable volume of diluent to givean initial concentration of 1,000 ,g/ml. One inter-mediate solution of lower concentration is prepared(see Table 1), and the final standards are made sepa-rately from the intermediate solution accoiding to thefollowing general scheme:initial solution -* intermediate solution (1,000 ,ug/ml)
_ 1.6 ml + 0.4 ml of diluent0.8 ml + 1.2 ml of diluent0.4 ml + 1.6 ml of diluent0.2 ml + 1.8 ml of diluent
-0.1 ml + 1.9 nl of diluentTo insure maximal accuracy, pipettes are chosen sothat not less than one-half of the total capacity isdelivered (3).
With very highly protein-bound drugs, such asoxacillin and nafcillin, it is necessary to add serumdirectly to the antibiotic powder, since we have foundzone diameters even in 90% serum to be significantlylarger than those in 100% serum. With antibioticswhich are not highly bound to serum proteins, it ispermissible to start with an initial diluent not con-taining protein, e.g., phosphate buffer or TryptosePhosphate Broth. The intermediate solution shouldbe made in serum, with the use of as little of theinitial solution as possible (e.g., 0.1 to 4.9 ml), sothat the final solutions placed in the wells are as nearly100% serum as possible. Serum which is used as adiluent should preferably be pooled from severalhealthy fasting volunteers. Such serum may be col-lected periodically and frozen until used. Competitive
VOL. 14, 1966 173
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

BENNETFT ET AL.
inhibitors of protein binding, if present in the pooledserum but not in an assayed sample, will cause resultsthat are erroneously low with highly serum-boundantibiotics. Many substances possess competitivebinding properties, including salicylates (5), andadditional compounds will undoubtedly be detected.It thus seems advisable that the donors abstain fromall drugs. It is also well to document, by electrophore-sis, the presence of serum components in normalamounts.
The above dilution scheme, returning to the inter-mediate solution for each standard, avoids errorsthat can result from having the potency of some ofthe standards dependent on each other. It also pro-vides standards with twofold variations in concen-tration. For example, if the intermediate concentra-tion is 20 ug/ml, then the standards will be 16, 8, 4,2, and 1 ,ug/ml. When any set of standards is madeaccording to the proposed scheme and plotted on logpaper, the linear distance between successive standardswill be equal, thus allowing the log of concentrationto be converted to a simple arithmetic scale, whichgreatly facilitates statistical analysis of results.When accurate and valid serum determinations
are desired from patients with serious metabolicdisturbances, such as uremia, diabetic ketoacidosis,cirrhosis, etc., it is advisable to make the antibioticstandards in the patient's own control serum obtainedbefore the antibiotic is administered. A general schemefor this, which requires a total of only 4.5 ml of con-trol serum and results in standards which are 90%patient's serum and 10% pooled normal serum, fol-lows:initial solution -* intermediate solution (1,000 ,ug/ml)~1.6 +0.4SS 0.1 +0.9 PS
-40.8 + 1.2S-0.1 +0.9 PS-0.4+ 1.6S -0.1 + 0.9PS-0.2+ 1.8S-0.1 +0.9PS
-*0.1 + 1.9 S 0.1 +0.9PSwhere S equals milliliters of pooled normal serum andPS equals milliliters of patient's control serum. Itshould be noted that, to obtain the same standardconcentrations as with the first dilution scheme, theintermediate concentration here needs to be 10 timesas potent. For this special procedure in which thepatient's serum is used for standards as well as un-knowns, an assay of five serum samples with appro-priate standards requires only 6 ml of patient's serum,a considerable saving as compared with the volumesneeded for the conventional cylinder-plate assayprocedure in which small plates are used.
Deterioration. Deterioration of antibiotics in clini-cal serum samples may lead to erroneously low assayvalues. To compensate for deterioration, the standardsmay be made when the samples are collected and bothsubjected to the same conditions until assay. Whensequential samples are collected over long time pe-riods, the standards may be frozen and each sampletreated in the same manner as soon as possible aftercollection.
ANALYSIS OF RESuLTSThe routine achievement of better than 10%
accuracy is a reasonable goal for antibiotic
assay of serum specimens, and may be defined as a95% certainty that a reported concentration iswithin 410% of the true concentration of thesample. Greater accuracy would be possible withmore replications of each unknown, but the workinvolved would be far too burdensome for smalllaboratories if more than six replications wereused routinely.Our methods of analysis employed a 16-fold dif-
ference in the potency of standards, a deliberatebreak from the traditional assay procedure whichlimits the standard concentrations to a narrowrange, representing a portion of the dose-responsecurve that does not depart significantly from astraight line. With this wider range, the dose-response relationship is a curve described by apolynomial regression of the form y = a + bx+ cx2.Method 1. After the zone diameters have been
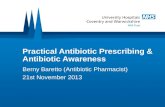
read and the six replications of each of the fivestandards have been averaged, five points areconstructed on two-cycle semilogarithmic graphpaper, plotting the mean zone diameters ofinhibition against the log of the antibiotic con-centration of each standard. These five points arethen joined together by straight lines (Fig. 4).To determine the concentration of an unknown,its mean diameter of inhibition is then convertedto concentration by extrapolation from the graph.The errors resulting from use of straight linesconnecting the five points, rather than a truecurve, are minor, since this series of straight lines
48-
\ 24-
°~12-
(.3
t 6-(.3
Q_ 3--Q
10 14 18 22Zone size in mm
26 30
FIG. 4. Demonstration of the curvilinear relation-ship between zone sizes and antibiotic concentrations,which applies for all antibiotics tested.
174 APPL. MICROBIOL.
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

ANTIBIOTIC ASSAY OF CLINICAL SPECIMENS
quite closely approximates a curve. In actualpractice, we rarely use method 1, since method 2is more accurate and involves little extra work.Method 2. The accuracy of estimating the con-
centration of the unknowns can be increased byapplying some fairly simple calculations to deter-mine the "best fitting curve" for the standard,instead of using the slightly less accurate "curve"described above. With the use of any ordinarycalculator that will accumulate products, and alittle practice, the best fitting curve can be deter-mined in 10 min or less by the method of leastsquares. This is the method ordinarily used inassaying chlnical specimens.A simplified means for deriving the values of
a, b, and c from the polynomial regression, y =
a + bx + cx2, has been determined by one of us(J.V.B.) from a more general solution to suchproblems (8). With the five concentrations pre-pared as described under Antibiotic standards,the standards can be coded into a simple linearscale of 1, 2, 3, 4, 5. To proceed, with an examplefrom a dicloxacillin standard curve, the fivestandards (3, 6, 12, 24, and 48 ,ug/ml) which are
to be plotted on the abscissa of the graph (xvalues) are coded numerically, and the cor-responding mean zone diameters are listed nextto them (y values), as illustrated in Table 2. Thezone diameters are added to give Ey which meansthe sum (E) of the individual diameters (y). Thefourth column above is then calculated by mul-tiplying the individual numbers under x and y,and these individual products are then totaledto give the sum Exy. With a calculator, of course,the individual products are automatically ac-
cumulated; they have been written down underxy to illustrate how the values would appear if acalculator was not being used. Next, the valuesfor x2y are determined in the same way and areadded to give the sum Ex2y. Before returning tothe general formula, another set of equations ap-plying to a curve with five points at equal dis-tances must be solved, with the values now avail-able being used to determine a, b, and c, which
represent three variables that are a part of thegeneral formula.
a = 4.6Ey + 0.5Ex2y - 3.3Exy
b187Exy - 3Ex2y - 23.Ey7
Ex2y + 7Ey - 6Exy14
Once obtained, a, b, and c are solutions for thegeneral formula, y = a + bx + cx2, and whenapplied to the present example yield the follow-ing: y = 6.2660 + 5.6814 x - 0.2585 x2. The codenumbers for x (1, 2, 3, 4, 5) are now substitutedinto the general formula to obtain zone sizes foreach standard concentration that are predictedby this best fitting curve. For comparison, theobserved mean zone sizes and the predicted valuesare shown below in columns 2 and 3 of Table 3.A simple check is then made to learn whether thevariables a, b, and c have been correctly deter-mined; deviations between observed and pre-dicted values should total zero (see column 4,Table 3), and usually do, although rounding offof the final figures for the predicted mean zonesizes can cause a discrepancy of a few hundredthsof a millimeter. The final steps of method 2 areto plot the five predicted mean zone sizes for the
TABLE 3. Illustration of the "best fitting curve"and comparison of predicted and observed
zone sizes
Coded Observed Predicted Difference betweenconcn mean zone mean zone observed zones
mm mm mm
1 11.68 11.69 -.012 16.62 16.59 +.033 20.96 20.98 - .024 24.86 24.86 .005 28.21 28.21 .00
Total = 0.00
TABLE 2. Example of how to apply observed zone sizes and standard antibioticconcentrations to the initial calculations
x ~~~~~yActual concn Coded Mean zone (mm) xy |Xry
concn produced by x
,ug/mi3 1 11.68 11.68 11.686 2 16.62 33.24 66.4812 3 20.96 62.88 188.6424 4 24.86 99.44 397.7648 5 28.21 141.05 705.25
Ey = 102.33 Exy = 348.29 Ex2y = 1,369.81
VoL. 14, 1966 175
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

BENNETT ET AL.
standards on two-cycle semilogarithmic graphpaper and then connect these points with a seriesof straight lines. The antibiotic concentration ofan unknown is then determined by extrapolationfrom the graph.Method 3. This method is even more accurate
than method 2, but is laborious, and is usedchiefly when extreme accuracy is needed. Withthe values of a, b, and c in the general formula,y = a + bx + cx2, having been solved by method2, it is then possible to solve the quadratic equa-tion for x (concentration) rather than y (meanzone sizes). To do this, we have derived thefollowing formula from the data of Smith (10):
+/b2_4ac +4cy- b2c
The procedure is the same as for method 2 upthrough the determination of values for a, b, andc. For a given unknown, the mean zone diameterrepresented by y is simply inserted into this lastformula, and the equation is solved for x. Thefigure obtained for x is in the coded scale (1 to5), and may be simply decoded as follows:
actual concentration = lowest standard
antilog (0.3010x)concentration X 2
In contrast to the other two methods, the con-centration of an unknown has been directly de-termined in this last method without recourse tograph paper.
Estimate of accuracy as obtained by method 3.A formal mathematical dissertation on tolerancelimits for inverse estimation of x from y, withthe use of a polynomial regression, is beyond thescope of this paper, and the reader is referredelsewhere (12). Such tolerance limits have beencalculated for several antibiotics for predictingthe concentration of an unknown at the midpointof the curve, with the assumptions that "s" wasclosely approximated by the standard deviationand that six replications were made of each offive standards. The equations were ultimatelysolved for the number of replications of an un-known needed when the recommended assaysystems are used, as shown in Table 4.
Estimates of accuracy based on tolerance limitsare somewhat larger than 95% confidence limits;thus, the accuracies in Table 4 are conservativeestimates. Table 4 is intended as a guide for theplanning of an assay, and is not intended as asubstitute for accuracy determinations of theactual assay data. If 1 to 3% accuracy is desired,additional replications of the standards are gen-
TABLE 4. Number of replications of an unknownneeded to produce varying accuracies, as calcu-lated by method 3 for a number of antibiotics
AccuracyAntibiotic Avg
:4:3% ±5% 47% 410% 4±20%
mm
Cephalothin .... > 100 10 4 2 1 .29Dicloxacillin >100 12 5 2 1 .38Cephaloridine. . > 100 32 9 4 1 .32Methicillin .. . 48 7 3 1 1 .25Nafcillin ....... > 100 17 6 3 1 .47Oxacillin ....... > 100 47 13 5 1 .50Penicillin G. ... > 100 13 5 2 1 .22Cloxacillin ... . > 100 9 4 2 1 .33Ampicillin ...... 47 7 3 2 1 .21
erally needed. Note that five or fewer replicationsof each of these drugs will yield at least 10%accuracy, thus confirming the feasibility of thisassay goal for routine work.The detailed steps required in the actual as-
sessment of accuracy are too tedious to be ap-plied to every assay. However, since the fit ofthe data to a polynomial regression is usuallyremarkably good, a rough practical estimate ofaccuracy may be obtained by simply determiningthe 95% confidence limits for the mean zonediameter produced by an unknown, extrapolatingthe concentrations from the standard curve whichcorrespond to these zone sizes, and then trans-lating the difference from the mean value in eitherdirection into per cent.
DIscussioNPrincipal advantages of the assay system de-
scribed here are the high degree of accuracy pos-sible with a minimal expenditure of time andmaterials. Most of the refinements have beenused before in one form or another, but to ourknowledge they have not previously been com-bined to achieve this efficient and accurate pro-cedure.- Our direct use of the curvilinear rela-tionship and our method of analyzing the resultsdoes appear to be unique, and represents a dis-tinct departure from traditional methods.Use of a large assay plate permits testing of a
great many samples under uniform conditions,giving a high degree of accuracy and reproduci-bility, and minimizes the number of replicationsas compared with small plates. A simple punchwhich we have designed permits the speedy prep-aration of a large number of agar wells, and theoptimal diameter for using minimal amounts ofserum and yet providing suitable assay charac-
176 APPL. MICROBIOL.
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from

ANTIBIOTIC ASSAY OF CLINICAL SPECIMENS
teristics has been selected. The most appropriateassay organisms for the commonly tested anti-biotics have been determined, and proceduresfor preparing standardized suspensions useful forseveral weeks are described. Attention has beendevoted to preparing accurate standard antibioticsolutions, and to providing controls for thedeterioration of standards and unknowns. Acombination of these advantages has made itpossible to test large numbers of unknowns inminimal time, and with accuracy consistentlybetter than 10% for the unknowns.Another way in which our method greatly
simplifies the actual assay procedure is that theunknowns are tested directly rather than dilutingthem to a narrow range of antibiotic concentra-tions. This is possible because the relationshipbetween antibiotic concentration and zone sizesis nearly perfectly described by a polynomialregression over large differences in potency.With this curvilinear relationship, a 16-folddifference in the potency of the five standards isemployed, and a special formula has been de-vised to determine the best fitting curve. Thus,the whole range of serum concentrations usuallyencountered clinically can in most instances beassayed directly, without dilution, and with ahigh degree of accuracy. An alternative to thisprocedure is the attempted transformation of thecurve to a straight line by use of zones squaredversus concentration, but this is much less satis-factory since the range of the standards oftenneeds to be decreased, and at best there is alwaysa residual curve which leads to systematic errors.The method is equally useful for urine and
other body fluids, but the emphasis has been onserum, since it has presented the greatest difficul-ties, and is the most important for critical com-parisons of antibiotic concentrations.
ACKNOWLEDGMENTSThis investigation was supported by Public Health
Service Grant 2TIA114606 from the National In-stitute of Allergy and Infectious Diseases.
LITERATURE CITED1. FINNEY, D. J. 1961. Principles and planning of
bio-assay. J. Hyg. Epidemiol. Microbiol. Im-munol. (Prague) 5:224-240.
2. GROVE, D. C., AND W. A. RANDALL. 1955. Assaymethods of antibiotics, a laboratory manual.Antibiot. Monographs No. 2.
3. KAVANAGH, F. 1960. A commentary on micro-biological assaying. Advan. Appl. Microbiol.2:65-93.
4. KIRSHBAUM, A., AND D. S. MASTERSON, JR. 1964.Official antibiotic reference standards. Anti-microbial Agents and Chemotherapy-1963,p. 447-450.
5. KUNIN, C. M. 1965. Inhibitors of penicillin bind-ing to serum proteins. J. Lab. Clin. Med. 65:416-431.
6. LEES, K. A., AND J. P. R. TOOTHILL. 1955. Micro-biological assay on large plates. Analyst 80:95-123.
7. MARTIN, G. VON. 1955. A simple apparatus forpunching out of agar plates for antibiotic andvitamin tests. Pharmazie 10:602.
8. MOORE, F. J., F. B. CRAMER, AND R. G. KNOWLES.1951. Statistics for medical students and in-vestigators in the clinical and biological sci-ences. The Blakiston Co., Philadelphia.
9. SIMPsoN, J. S. 1963. Microbiological assay usinglarge plate methods, p. 87-124. In FrederickKavanagh led.], Analytical microbiology.Academic Press, Inc., New York.
10. SMITH, C. A. B. 1954. Biomathematics, the prin-ciples of mathematics for students of biologicalscience, 3rd. ed. Charles Griffin and Co. Ltd.,London.
11. VESmRDAL, J. 1946. The agar cup method for theestimation of penicillin. Acta Pharmacol.Toxicol. 2:9-21.
12. WILLIAMS, E. J. 1959. Regression analysis. JohnWiley & Sons, Inc., New York.
VOL. 14, 1966 177
on June 5, 2020 by guesthttp://aem
.asm.org/
Dow
nloaded from