Vol. 5, page 1 SRMConline.com October 2014 Oncology 2014 1/Southside... · Annual Report Vol. 5,...
32
Oncology 2014 October 2014 Annual Report SRMConline.com Vol. 5, page 1 2014 has been a great year for our community. Southside Regional Medical Center (SRMC) has had an excellent oncology program for over three decades, developed years ago by a forward thinking team of oncologists, ultimately leading to the achievement of accreditation with commendation from the American College of Surgeons Commission on Cancer in 2011. SRMC’s Department of Radiation Oncology has been providing state-of-the-art cancer care since September 1989. Building upon this foundation of outstanding community cancer care, on January 6, 2014, SRMC opened up a new 36,000 square foot Medical Arts Pavilion housing SRMC’s oncology program, a brand new women’s imaging center, and obstetrics and gynecology services at 210 Medical Park Boulevard, immediately adjacent to SRMC’s main hospital. The results have far exceeded our expectations. SRMC continues to build and foster relationships with established oncologists including Dr. Butchaia Kondragunta, Dr. Sujatha Yellinedi, and Dr. Nishanth Sukumaran. SRMC has forged new partnerships with leading oncology professionals, including Dr. William Voelski, Dr. Yogesh Gandhi, Dr. Shobha Nalluri, Dr. Attique Samdani, and Dr. Mitchell Machado of Virginia Cancer Institute. Members of our community now have increased options and access to specialized medical care including more availability for clinical trials. SRMC has some of the best people and technology available for the delivery of oncology care. In 2014 our radiation oncology CANCER COMMITTEE CHAIRMAN’S REPORT David R. Penberthy, MD, MBA Board Certified Medical Director of Radiation Oncology Cancer Committee Chairman Southside Regional Medical Center Petersburg, Virginia department commissioned a state-of-the-art Varian TrueBeam™ linear accelerator for the most sophisticated delivery of external beam radiotherapy including intensity modulated radiotherapy (IMRT) and image guided radiotherapy (IGRT). Our department plans to expand our range of services in the near future. With advanced communications abilities in SRMC’s new pavilion, SRMC now has the ability to perform virtual consultations with specialists remotely if necessary. SRMC’s new cancer center allows even closer collaboration amongst our team of dedicated oncology professionals including surgeons, medical oncologists, pathologists, radiologists and many others. SRMC’s new Medical Arts Pavilion is a warm and inviting environment, and with the current services available, it is a major health care resource for our community while simultaneously facilitating SRMC’s mission of providing excellent, compassionate patient care. More than ever, SRMC can better meet our community’s needs. 2014 has been a great year, and I am excited about SRMC’s future and am thrilled to be part of SRMC’s team.
Transcript of Vol. 5, page 1 SRMConline.com October 2014 Oncology 2014 1/Southside... · Annual Report Vol. 5,...

Oncology 2014October 2014
Annual Report
SRMConline.comVol. 5, page 1
2014 has been a great year for our community. Southside Regional Medical Center (SRMC) has had an excellent oncology program for over three decades, developed years ago by a forward thinking team of oncologists, ultimately leading to the achievement of accreditation with commendation from the American College of Surgeons Commission on Cancer in 2011. SRMC’s Department of Radiation Oncology has been providing state-of-the-art cancer care since September 1989. Building upon this foundation of outstanding community cancer care, on January 6, 2014, SRMC opened up a new 36,000 square foot Medical Arts Pavilion housing SRMC’s oncology program, a brand new women’s imaging center, and obstetrics and gynecology services at 210 Medical Park Boulevard, immediately adjacent to SRMC’s main hospital. The results have far exceeded our expectations. SRMC continues to build and foster relationships with established oncologists including Dr. Butchaia Kondragunta, Dr. Sujatha Yellinedi, and Dr. Nishanth Sukumaran. SRMC has forged new partnerships with leading oncology professionals, including Dr. William Voelski, Dr. Yogesh Gandhi, Dr. Shobha Nalluri, Dr. Attique Samdani, and Dr. Mitchell Machado of Virginia Cancer Institute. Members of our community now have increased options and access to specialized medical care including more availability for clinical trials. SRMC has some of the best people and technology available for the delivery of oncology care. In 2014 our radiation oncology
CANCER COMMITTEE CHAIRMAN’S REPORTDavid R. Penberthy, MD, MBABoard CertifiedMedical Director of Radiation OncologyCancer Committee ChairmanSouthside Regional Medical CenterPetersburg, Virginia
department commissioned a state-of-the-art Varian TrueBeam™ linear accelerator for the most sophisticated delivery of external beam radiotherapy including intensity modulated radiotherapy (IMRT) and image guided radiotherapy (IGRT). Our department plans to expand our range of services in the near future. With advanced communications abilities in SRMC’s new pavilion, SRMC now has the ability to perform virtual consultations with specialists remotely if necessary. SRMC’s new cancer center allows even closer collaboration amongst our team of dedicated oncology professionals including surgeons, medical oncologists, pathologists, radiologists and many others. SRMC’s new Medical Arts Pavilion is a warm and inviting environment, and with the current services available, it is a major health care resource for our community while simultaneously facilitating SRMC’s mission of providing excellent, compassionate patient care. More than ever, SRMC can better meet our community’s needs. 2014 has been a great year, and I am excited about SRMC’s future and am thrilled to be part of SRMC’s team.

October 2014Vol. 5, page 2
ANOTHER YEAR OF GROWTHSubmitted by: Faye Flemming RN, BSN, OCN, SRMC Oncology Service Line Director
January 2014 was exceptionally busy with the opening of SRMC’s Medical Arts Pavilion (MAP). Radiation Oncology services moved all of their services to the new cancer center located inside the MAP from their 625 Adams Street location. Radiation therapy patients began treatments on the new state-of-the-art TrueBeam™ Linear Accelerator in January. This new technology is now located within our new Cancer Center on the conveniently located hospital campus.
Within the new Cancer Center you will find a resource center/oncology library, navigation office, support staff, oncology administration, SRMC tumor registry and a large conference room for oncology-related activities. This offers easy access to oncology, women’s and SRMC services for our oncology patients.
SRMC has also been busy obtaining a new certificate of public need (CON) to offer stereotactic radiosurgery (SRS). This has been approved and a second state-of-the-art TrueBeam™ linear accelerator with SRS has been ordered. We hope to have this service available to our patients by the beginning of 2015.
We are also in the process of working with the state and obtaining a CON and equipment for a High Dose Rate Brachytherapy (HDR). We are hoping to begin offering this service to our patients in the first half of 2015.
Virginia Cancer Institute (VCI) opened a Petersburg office on the second floor of the MAP. This addition has added a second oncology practice with easy access to the hospital for our SRMC oncology patients and families. Both Dr. Machado’s SRMC Medical Oncology Practrice and the SRMC Infusion Center closed in January. Dr. Machado is now one of the medical oncologists at VCI’s Petersburg office and he is seeing his patients on SRMC’s campus. SRMC infusion patients are now treated at one of the two medical oncologists’ infusion areas.
I would like to thank all of the multidisciplinary oncology team members, hospital staff, community organizations, patients, and families for continuing to assist us in making our oncology service line the best it can be. Everyone’s time, input, patience and assistance are appreciated!
The Cancer Committee continues to guide us by meeting quarterly to oversee the cancer program and services. It is
TABLE OF CONTENTSPage 1Cancer Committee Chairman’s ReportPages 2-3Another Year of GrowthPage 4Oncology NursingRadiation TherapyPage 5Medical OncologyPage 6Surgery Pathology/LaboratoryPage 7 RadiologyDigestive SolutionsPages 8-9Cancer Committee MembersEndoscopic UltrasoundPage 10-11 Women’s ImagingPage 12Spiritual Care ServicesPages 13-20Halo ProcedureOncology Program OutcomesPage 21Cancer ConferencesPage 22Wound Healing CenterEducationPage 23Care PartnersPage 24Oncology Nurse NavigationCommunity Resources/SupportsPages 25-26Rehabilitation ServicesPages 27-29Creating a Culture of SafetyCase ManagementPage 30Supportive Services for PatientsPage 31What is a Cancer Registry?Cancer Liaison PhysicianPage 32Quality DepartmentSenior Administration

October 2014Vol. 5, page 3
hard to believe it will soon be three years since we received accreditation with commendations for our cancer program from the Commission on Cancer (CoC). We are scheduled for re-accreditation in November 2014.
The Oncology Quality Committee continues to be a very functional multidisciplinary committee. They have developed and overseen completion of our yearly oncology quality plan based on identified priorities relating to the quality of our oncology programs and services. This committee also identifies, discusses and makes recommendations to the Cancer Committee related to any oncology quality items.
Our Oncology Steering Committee has been very busy working on cancer center planning and oncology program additions and improvements. Our navigation, psychosocial and distress management programs continue to grow and receive extremely positive satisfaction results. Continued planning for the development of a more formal palliative care program remains an objective for this committee.
Some of our major accomplishments and projects in 2014 include:• Opening a new Medical Arts Pavilion (MAP) at 210 Medical Park Boulevard housing SRMC’s new
Cancer Center, Woman’s Imaging, Tri-Cities OB/GYN Associates and Virginia Cancer Institute (VCI) on the hospital campus
• Now treating all radiation therapy patients on a new state-of-the-art TrueBeam™ linear accelerator at the new Cancer Center in Suite 100 of the Medical Arts Pavilion
• Now treating all oncology infusion patients at the medical oncologist’s infusion area• Dr. Machado closed his medical oncology practice at SRMC and joined VCI, practicing medical
oncology in their office in the new MAP/Cancer Center• Conducted our second annual head and neck screening with almost 60 attendees screened• Converted to a paperless Electronic Medical Record (EMR) system in radiation oncology• Continues to provide a survivorship and follow-up care plans to our radiation oncology patients at
the end of hospital-based radiation oncology treatment• Continues to provide treatment summaries to radiation oncology patients after completion of treatments • Participates in many local, state and national organizations as board, advisory and other committee
and project team members • Providing oncology-related presentations at local and national meetings and activities • Now participating in the
CoC Rapid Quality Reporting System (RQRS)
• Received a Certificate of Need (CON) to provide stereotactic radiosurgery (SRS) and High Dose Rate Brachytherapy (HDR)
• Completed construction of a second linear accelerator vault and purchased a second TrueBeam™ linear accelerator; this second machine is equipped for sterotactic radiosurgery
TrueBeam™ Linear Accelerator provides an excellent and comfortable patient treatment environment.

October 2014Vol. 5, page 4
ONCOLOGY NURSINGOncology nursing services focus on the physical, psychosocial, spiritual, cultural and educational needs of our patients and their loved ones, and nurses provide these services within our inpatient and outpatient settings. Specially trained oncology nurses complete triage, screenings, assessments, education, care planning, treatments, referrals, emotional support, and follow-up care as they assist physicians throughout the patient’s cancer journey. Nurses assist patients by arranging for “at home” oncology care assistance via home health, private, and hospice agencies of the patient’s choice.
Specially trained chemotherapy/biotherapy nurses attend the ONS chemotherapy/biotherapy certification class. After passing the ONS chemotherapy/biotherapy exam, attending all required SRMC oncology educational offerings and completing observed administration of chemotherapy/biotherapy at SRMC, these nurses are then allowed to administer chemotherapy/biotherapy to our patients.
SRMC strongly encourages our oncology nurses to obtain Oncology Nursing Certification (OCN). Certification is one of the methods utilized at SRMC to assure patients and families their nurse has obtained the knowledge and skill required to competently provide the patient with specialized oncology care. Being an OCN signifies the RN has met or exceeded rigorous criteria for knowledge and experience and has a measured competence in this demanding and ever changing specialty area. To become an OCN, nurses must meet the requirements and then successfully complete the OCN examination. Certification is valid for four years and may be renewed by either passing the examination again or by meeting precisely defined education and practice requirements.
Oncology Nurses attend SRMC’s weekly tumor boards. Their participation in tumor boards adds a nursing, psychosocial and patient/family perspective to our patients’ plan and care. This also gives nurses an opportunity to learn more about their individual patient’s disease and care, specific cancers, clinical trials/research, staging, clinical guidelines, diagnostics, treatment options, palliative care, end-of-life care, survivorship care and other oncology team members’ specialties.
All patients receiving infusion oncology services as an inpatient, such as chemotherapy or biotherapy, are placed on the medical/surgical oncology inpatient unit, 4 East. Lynette Parker RN, BSN is the unit manager for 4 East. Her oncology nurses have received training by SRMC and completion of the Oncology Nursing Society’s Cancer Chemotherapy and Biotherapy Course.
Oncology Nurses are also present in the Radiation Therapy and Oncology Navigation departments. These nurses assist with the care, education and support of our oncology patients by assessing their clinical, physical and psychosocial needs. They then support the patients and oncology team by providing resources, coordination of care, referrals and emotional support.
“Being an OCN signifies the RN has met or exceeded rigorous criteria for knowledge and experience and has a measured competence in a demanding and ever changing specialty area.“

October 2014Vol. 5, page 5
Cancer care at SRMC utilizes a multidisciplinary team approach. Radiation Therapy is one component of that team. Radiation therapy (also known as radiotherapy) is a cancer treatment that uses high doses of radiation to kill cancer cells and stop them from spreading. Radiation therapy can be external beam (when the linear accelerator outside your body aims radiation at cancer cells) or internal (when radiation is put inside your body, in or near the cancer cells). Sometimes people get both forms of radiation therapy. Approximately 60 percent of cancer patients receive radiation therapy as a first or later course of treatment.
Radiation Therapy is used to help cure, stop, or slow the growth of cancer as well as used to help reduce symptoms. Most patients get external beam therapy once a day, five days a week, Monday through Friday. Treatments last for two to 10 weeks, depending on the type of cancer and the goal of treatment.
The center opened with a new Varian TrueBeam™ linear accelerator. We are working to install our second TrueBeam™ with stereotactic capabilities in the fall of 2014. The Radiation Therapy department treated 360 patients in the year 2013. We preformed 6,328 therapy procedures using modern techniques such as 3-D conformal therapy, Intensity Modulated Radiation Therapy (IMRT), Rapid Arc and Image Guided Radiation Therapy (IGRT).
Our radiation oncology team consists of radiation oncologists, physicists, dosimetrists, technicians, nurses, patient navigators, registration staff, registry staff and administrators. They work together to make each patient’s experience as pleasant as possible.
Medical oncology services at SRMC are provided by two groups of private practice medical oncologists. Both practices are located close to SRMC for easy access to both their practices and the hospital. Each physician in these practices is a member of the SRMC multidisciplinary oncology team. They actively participate in cancer conferences (tumor boards), the cancer committee, the steering committee, the oncology quality committee, palliative care, the ethics committee and all aspects of oncology care at SRMC. They work side-by-side with other physicians and staff to assure patients receive the best quality care and that their needs are addressed.
34 Medical Park Boulevard, Suite G • Dr. Butchaiah Kondragunta• Dr. Sujatha Yellinedi• Dr. Nishanth Sukumaran This is located between the hospital and Crater Road, easily accessed from the hospital parking lot.
Physicians in both of these practices provide and/or coordinate consultations, diagnostic care, medical treatments (including, but not limited to chemotherapy, biotherapy, hormonal therapy and transfusion services), symptom management, palliative care, home health care, survivorship care and hospice/end-of-life care.
MEDICAL ONCOLOGY
Virginia Cancer Institute (VCI) Medical Arts Pavilion• Dr. Mitchell Machado• Dr. Yogesh Gandhi• Dr. Shobha Nalluri• Dr. James T. May, III• Dr. Attique SamdaniLocated adjacent to the hospital.
RADIATION THERAPY

October 2014Vol. 5, page 6
SRMC offers our oncology patients both inpatient and outpatient options for required surgical procedures. Our team of surgical specialists assists other oncology physicians in providing the best diagnostic and surgical care possible for our oncology patients. They perform consultative, diagnostic, interventional and surgical procedures and assist with care. Our surgeons often attend our weekly tumor boards and many of their oncology cases are discussed to assure a multidisciplinary approach to our patients’ care.
Surgeons meet with our patients to help determine their diagnosis. Surgeons can obtain specimens (biopsies) from suspected cancer sites to either rule out cancer or provide physicians a pathological diagnosis of cancer. These biopsies can be completed in our operating room suite, endoscopy, same day surgery, woman’s imaging and even in radiology depending on the site and the patient.
We have trained surgeons in the following surgical specialties: general surgery, orthopedics, thoracic surgery, bariatrics, gynecology, cardiovascular, urology, and ENT. You can find information about all SRMC physicians on our website (SRMConline.com) under “Find a Doctor.”
The Department of Pathology at Southside Regional Medical Center, a part of the clinical laboratory, assists other physicians in providing care for patients with cancer by evaluating tissue specimens to establish the diagnosis and extent of disease, to determine the appropriate treatment and to monitor the progress of the patient’s response to treatment. The tissue specimens may be as small as individual cells obtained by needle aspiration and as large as resected organs, such as breast, colon, prostate and lung. Specimens are analyzed under the microscope and a wide array of additional testing is available, some of which is performed at reference laboratories. This includes tests such as hormone receptor content in breast cancers, biomarkers to determine the prognosis and response to specific therapies for many cancers, chromosome analysis (cytogenetics) and laser scanning (flow cytometry) to detect abnormal cells in blood and bone marrow.
The pathologic features of resected specimens are reported in standard formats, using the protocols developed by the College of American Pathologists, in order that the treating doctor is assured of having all relevant information in an easy to read format. All of this information is reported in the hospital’s computer system and thus upon completion of laboratory studies is immediately available to all physicians providing care for a patient. The pathologists provide assistance in the evaluation of cancer patients by performing bone marrow aspirations and biopsies on hospitalized patients and outpatients. They also provide immediate microscopic evaluation of cancer specimens at the time of an operation to determine the extent of surgery required to effectively remove a cancer. The pathologists attend the weekly oncology conferences, presenting photographs of tissue specimens and describing the extent of disease, to assist other physicians in determining the most appropriate therapies.
Our pathology department is a department within the laboratory. The pathologists advise and assist with physician oversight of the lab and related items. The laboratory staff is another important part of the oncology team. They draw blood, complete testing and report findings of patient blood and other bodily excretions.
PATHOLOGY/LABORATORY
SURGERY

October 2014Vol. 5, page 7
The SRMC Radiology Department provides a full array of imaging and interventional services to our oncology inpatients and outpatients. Some of their services we utilize include, but are not limited to: • Computerized Tomography (CT)• PET-CT scanning• Digital Mammography• Radiographs• Ultrasound• Nuclear Medicine (including sentinel node procedures)• Stereotactic breast biopsy• Ultrasonic guided thyroid biopsy• Interventional Radiology (such as insertion & diagnostics of vascular access devices, other
biopsies, other diagnostic procedures and therapeutic procedures)
A radiologist attends every weekly tumor board. Our oncology radiologists include: • Dr. Michele Brenner-Vincent (Medical Director of Radiology and Cancer Committee member)• Dr. Jeffrey Morgan • Dr. Cary Straton • Dr. Craig Rowell
The Digestive Solutions department performed over 5,200 endoscopic procedures in 2013. Our highly trained registered nurses assist physicians with many procedures including endoscopy, colonoscopy, endoscopic ultrasound, gastrostomy tube placement, ERCP, esophageal manometry, liver biopsy, paracentesis and bronchoscopy. The department utilizes state-of-the-
art, high-definition equipment to diagnose and treat many GI disorders as well as pulmonary conditions. In July 2013 we began a new procedure at Southside Regional Medical Center to treat Barrett’s esophagus utilizing a non-surgical ablation treatment to the affected tissue of the esophagus, preventing it from developing into cancerous lesions. Our gastroenterologists continue to utilize our endoscopic ultrasound technology to place fiducial markers in the prostate for radiation treatment. Also in 2013, we introduced a new, relatively painless, treatment for internal hemorrhoids using bipolar energy. This procedure is performed under minimal sedation in an outpatient setting; the procedure is far less painful than traditional banding procedures. Our pulmonologists continue to treat our asthma patients with the bronchothermoplasty procedure and are the only physicians in the central Virginia area doing this remarkable life changing treatment. Our patients have seen remarkable improvement in their asthma symptoms, decreased ER visits and use of rescue inhalers. Digestive Solutions is growing to provide the best treatment options for our patients close to home.Our physicians include:• Dr. Yiping Rao • Dr. Zahid Rashid• Dr. Sanjeev Jairath• Dr. Robert Flynn• Dr. Gregory Lemite, Gastroenterology
• Dr. Robert Davis, Dr. Tahir Allauddin, Dr. Russell Johnson; Pulmonology
• Dr. John Breard, Thoracic Surgery• Dr. T. Datta, Bariatric Surgery• Dr. J. Rayudu, Dr. R. Ross, Dr. B. Smith, Dr. S.
Malik, and Dr. M. Basker, General Surgery
RADIOLOGY

October 2014Vol. 5, page 8
ENDOSCOPIC ULTRASOUND (EUS)
Endoscopic Ultrasound (EUS) is a medical procedure in which endoscopy is combined
with ultrasound to obtain images of the internal organs in the chest and abdomen. It can be used to visualize the walls of these organs, see if it is abnormally thick, suggesting inflammation or malignancy, or to look at adjacent structures. Combined with Doppler imaging, nearby blood vessels can also be evaluated. The procedure is performed by gastroenterologists who have had extensive training.
EUS is performed with the patient sedated. Organs such as the liver, pancreas, and adrenal glands are easily biopsied by a fine needle aspiration (FNA), which can be introduced through the echoendoscope to sample tissue, masses, and any abnormal lymph nodes.
With the scope stationed in the esophagus, EUS can be used for the staging of esophageal and non-small cell lung cancer, as well as for the evaluation of masses, lymph nodes and cysts located within the posterior mediastinum. With FNA, cytology samples can be obtained to stage and/or restage the esophageal or lung cancer. Studies have clearly shown that EUS can prevent unnecessary mediastinoscopies and thoracotomies. In addition, EUS can be utilized to sample suspicious lymph nodes after neoadjuvant therapy in esophageal and lung cancer patients to see if they have been down staged by chemotherapy and would now benefit from surgery.Currently, the EUS study is mandatory in most hospitals for the preoperative
Submitted by: Yiping Rao, MD, Msc, Board Certified, Gastroenterology
CANCER COMMITTEE MEMBERSMEMBERS: Dr. Penberthy, Radiation Oncologist: Cancer Committee Chairperson Dr. Wickizer, CMO, Surgery, ER: Cancer Liaison Physician Dr. Machado, Palliative Care Coordinator Dr. Vincent, Radiology Dr. Summerville, Pathology Dr. Yellinedi, Medical Oncology JoyceDayvault,ChiefQualityOfficer Lori McNulty, Navigation Nurse Lynette Parker, Nurse Manager Judy Slate, Tumor Registry Tonya Grant, Marketing & Outreach Faye Flemming, Oncology Service Line Director
ALTERNATE MEMBERS: Dr. Breard, Surgery Dr. Sukumaran, Medical Oncology Dr. Morgan, Radiology Dr. Siegmund, Pathology Dr. Gandhi, Palliative Care Dr. Ali, Radiation Oncology Cheryl Smith, Oncology Admin Harriet Kelly, Quality Louvenia King, Oncology Nurse Doris Bailey, Navigation Janet Narrow, Registry DEPARTMENTAL COMMITTEE & SUB-COMMITTEE REPRESENTATIVES FROM: Medical Oncology Infusion Inpatient Oncology Senior Administration Nutrition Services Nursing Massey Cancer Center Outreach Radiology Pastoral Care Lab/Pathology Patient Relations American Cancer Society Oncology Administration Palliative care Oncology Navigation Radiation Therapy OB/GYN Marketing/Public Relations Quality Tumor Registry Medical Staff/Physicians Rehab Pharmacy Information Technology

Vol. 5, page 9
staging of gastric cancer, to assess with a good accuracy the tumor depth of wall invasion, the presence of suspicious lymph-nodes and of ascites (predictive of peritoneal involvement).
EUS is highly sensitive for detection of pancreatic cancer (90-95% sensitivity). EUS allows for sampling of pancreatic masses by FNA, thus providing a definitive diagnosis to help direct future therapy. Its role in treatment of patients with pancreatic cancer is promising with studying various chemotherapeutic agents that may be injected into pancreatic tumors under EUS guidance to provide targeted therapy. In patients with pancreatic cancer who have pain due to involvement of the adjacent celiac plexus by their disease, we can perform celiac plexus blockade via EUS to provide longer lasting pain control.
EUS can also be used for imaging of the rectum, colon, and prostate. Staging of rectal cancer by endoscopic ultrasound is straightforward and has been consistently shown to be more accurate than CT or MRI. EUS guided fine needle aspiration may be used to sample lymph nodes during this procedure. Evaluation of the integrity of the anal sphincters may also be done during lower EUS procedures. Radiographic markers (or fiducials) implanted at the prostate tumor site are used as reference points by the system to target the radiation beams. Rectal EUS have provided a safe and reliable technique that may be performed by the gastroenterologist for subsequent prostate localization during radiotherapy.
Experience at Southside Regional Medical Center:From July 2008 through May 2014, four hundred and fifty-six EUS procedures were performed at Southside Regional Medical Center. The most common indications included staging or diagnosis for suspected pancreatico-biliary malignancy, investigating pancreatic cysts, staging of rectal, esophageal, or gastric cancer and evaluating patients with
a dilated common bile duct, pancreatitis, or enlarged lymph nodes in mediastinum. EUS has positively altered the clinical management in many of these patients.
Recently, many cases of EUS guided celiac plexus blockade and prostate fiducial marker placements also were performed without any complications.
It is important to note that EUS has many more indications beyond staging and sampling of malignancy, from evaluating the etiology of pancreatitis to investigating pancreatic cysts. The role of EUS will provide the opportunity for therapeutic interventions in the future. EUS may be used to ablate premalignant pancreatic cysts or to locally treat pancreatic and other GI tract cancer, thus having the greatest clinical impact on these patients.
Yiping Rao, MD, MscBoard Certified Gastroenterology,Internal Medicinewww.virginiaGI.com430 Clairmont Ct, Suite 212Colonial Heights, VA 23834(804) 504-4604
“From July 2008 through May 2014, four hundred and fifty-six EUS procedures were performed at Southside Regional Medical Center.”
October 2014

October 2014Vol. 5, page 10
healthy woman
beau
tiful
beautiful
beautiful
beautiful
beautiful
sistersi
ster
sister
sister
sister
friend
friend
friend
frie
nd
wife
wife
wifewife
wife
wife
wife
wife
daughter
woman
woman
mother
mother
mother
mother
mother
specialists
specialists
fam
ily
surgery
surgerysurgery
surgery
surgery
surg
ery
surgery
healing
healing
healing
healing
healing
healing
healing
wellness
wellness
hope
hope
hope
hope
hope
hope hope
hope
hope
awareness
awareness
awareness
awareness
awareness
awar
enes
s
awareness
awareness
awarenessmammogram
gynecology
gynecology
gynecology
imagingob/gyn
ob/gyn
ob/gyn
ob/gyn
ob/gyn
strong
strong
strong
strong
strongstrong strong
advanced
adva
nced
motivation
motivation
mot
ivat
ion
motivation
motivation
motivation
motivation
cour
age
courage
courage
courage
treat
trea
t
treattreat
treat
treat
treat
treat
treat
treat
care
care
care
care
care
care
care
care
care
preventionp
revention
prevention
prevention
diagnose
diagnose
diagnose
quality
quality
quality
quality
quality
quality
quality
quality
210 Medical Park Boulevard • Suite 225Petersburg, Virginia 23805
p: 804.765.5379 • f: 804.765.5525
The new Women’s Imaging Center, located in the Medical Arts Pavilion on the campus of Southside Regional Medical Center, provides advanced, fully digital imaging and diagnosis for women of all ages. The new imaging center, staffed by radiologists and technologists who are specially trained in women’s health, promotes clinical excellence and compassionate care. The services provided by SRMC’s Women’s Imaging include:
Screening Mammogram
Diagnostic Mammogram
Breast Ultrasound
Bone Density Screening (DEXA scan)
Breast Biopsies
A screening mammogram is an image of the breast(s), used to detect and diagnose breast disease. Screening mammography is used as a preventative measure for women who have no symptoms of breast disease.
A diagnostic mammogram is an image of the breast(s) performed on patients that are having breast symptoms, have implants or have had previous breast cancer. Diagnostic mammograms are used when an abnormality is found during a screening mammogram. Indications for a diagnostic mammogram include, but are not limited to:
Breast ultrasound is a very common exam using sound waves to produce the image (no radiation exposure). Ultrasound is most typically performed as a supplemental exam to mammography. Indications for breast ultrasound include but are not limited to:
If a significant abnormality is found on the diagnostic mammogram, ultrasound or clinical breast examination, a breast biopsy is often recommended. A biopsy involves the removal of a small sample of breast tissue that is sent to a pathologist for examination. Types of breast biopsies include:
• Evaluation of a palpable mass or thickening – used to distinguish solid and cystic lesions. • Evaluation of a finding on mammography, CT scan, or Breast MRI. • Evaluation of focal symptoms in pregnant women and patients under age 30 (to avoid radiation exposure to the breast).
• Breast lump/mass• Focal breast pain• Skin thickening • Onset of inverted nipple
• Stereotactic breast biopsies• Cyst Aspirations
• Ultrasound guided core biopsies• Needle localization
• Nipple discharge• Previous breast cancer• Follow up from screening mammogram
N
95
Wagner Rd.
South Crater Rd.
Med
ical Park Blvd
.
OB UltrasoundAn ultrasound is a test that uses sound waves to produce an image of the fetus inside the uterus. This type of ultrasound is sometimes referred to as a sonogram. It is non-invasive and poses no risk to either mother or baby. Ultrasounds are often requested by your primary obstetrician to check gestational dating and to examine the fetus for normal growth and development.
GYN UltrasoundGynecologic ultrasonography is a test that uses sound waves to produce an image of the female pelvic organs (specifically the uterus, ovaries and the fallopian tubes) as well as the bladder and the adnexa.
A bone density test determines if you have osteoporosis — a disease that causes bones to become more fragile and more likely to break. A bone density test makes it possible to know your risk of breaking bones before the fact. Additionally, a bone density test uses images to measure how many grams of calcium and other bone minerals are packed into a segment of bone. The bones that are most commonly tested are located in the spine, hip and forearm.
October 2014Vol. 5, page 11
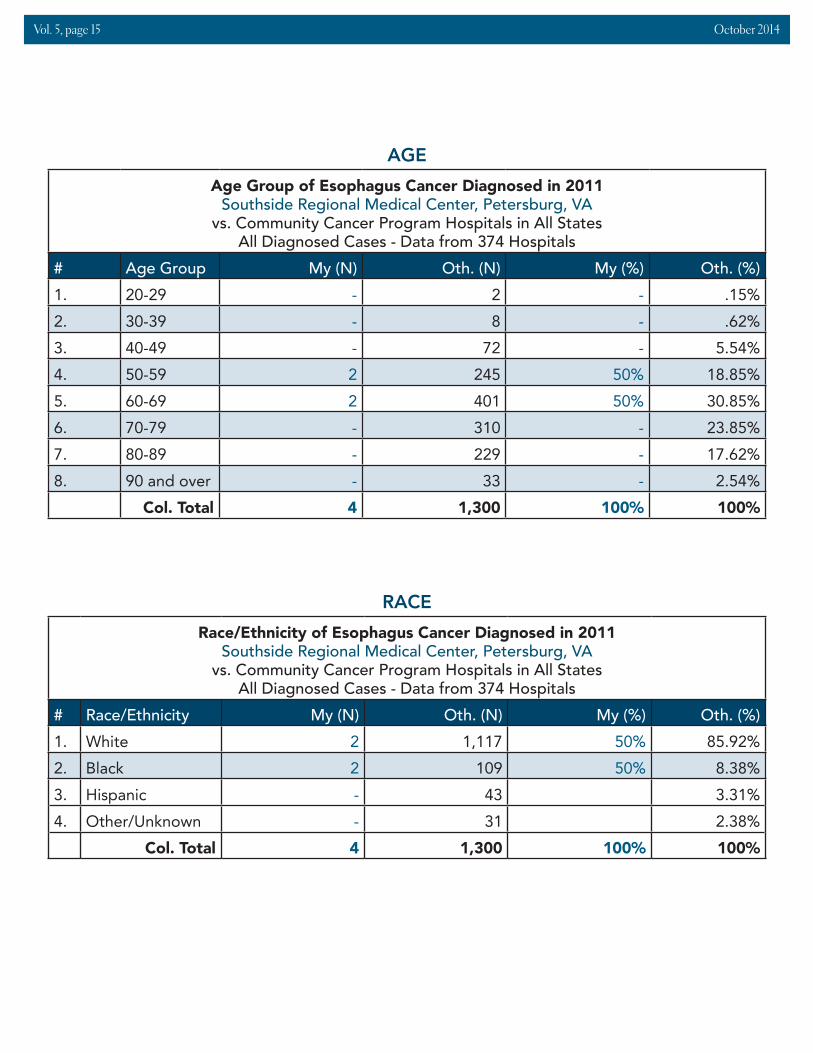
The new Women’s Imaging Center, located in the Medical Arts Pavilion on the campus of Southside Regional Medical Center, provides advanced, fully digital imaging and diagnosis for women of all ages. Radiologists and technologists who are specially trained in women’s health staff our imaging center. Services are performed in a warm and inviting environment that promotes clinical excellence and compassionate care. The Women’s Imaging team works closely with the oncology department and oncology team members to provide screening, preventative, diagnostic and follow-up procedures and information to our oncology patients. The Women’s Imaging Center provides the following services:
Screening MammogramA screening mammogram is an image of the breast(s), used to detect and diagnose breast disease. Screening mammography is used as a preventative measure for women who have no symptoms of breast disease.
Diagnostic MammogramA diagnostic mammogram is an image of the breast(s) performed on patients that are having breast symptoms, have implants or have had previous breast cancer. Diagnostic mammograms are used when an abnormality is found during a screening mammogram. Indications for a diagnostic mammogram include, but are not limited to:• Breast lump/mass• Nipple discharge• Focal breast pain • Previous breast cancer• Skin thickening • Follow-up from screening mammogram• Onset of inverted nipple
Breast UltrasoundBreast ultrasound is a very common exam using sound waves to produce the image (no radiation exposure). Ultrasound is most typically performed as a supplemental exam to mammography. Indications for breast ultrasound include but are not limited to:• Evaluation of a palpable mass or thickening - used to distinguish solid and cystic lesions.• Evaluation of a finding on mammography, CT scan, or breast MRI.• Evaluation of focal symptoms in pregnant women and patients under age 30 (to avoid radiation
exposure to the breast)
Breast BiopsiesIf a significant abnormality is found using diagnostic mammogram, ultrasound or clinical breast examination, a breast biopsy is often recommended. A biopsy involves the removal of a small sample of breast tissue that is sent to a pathologist for examination. Types of breast biopsies include:• Stereotactic breast biopsies • Ultrasound guided core biopsies• Cyst aspirations • Needle localization
WOMEN’S IMAGING CENTER
Mammography equipment
Stereotactic equipment

October 2014Vol. 5, page 12
HALO PROCEDUREYiping Rao, MD, Msc, Board Certified, Gastroenterology
A new procedure available at SRMC is treating Barrett’s esophagus which is a pre-cancerous tissue in the lining of the esophagus. The procedure, known as endoscopic radiofrequency ablation therapy, is an outpatient procedure that takes approximately 30 minutes. Dr. Yiping Rao, a gastroenterologist practicing at SRMC, has been trained in the new therapy which removes pre-cancerous
cells from the esophagus with a targeted procedure, leaving behind healthy cells to regenerate. “The main purpose of the ablation procedure is to ablate, or remove the abnormal lining thus allowing the tissue to regenerate and normal tissue to grow back,” said Dr. Rao.
“The main purpose of the ablation procedure is to ablate, or remove the abnormal lining thus allowing the tissue to regenerate and normal tissue to grow back.”
Spiritual Care Services continues to have a supporting role in caring for the emotional and spiritual needs of cancer patients, their families, and Cancer Center staff. The Director of Spiritual Care Services and SRMC’s team of 33 trained volunteer chaplains visit cancer patients upon referral from Nurse Navigator, Lori McNulty, and inpatient referrals from unit staff. The Director of Spiritual Care Services also serves on the Oncology Steering Committee and is a resource speaker during Cancer Support Group meetings. Our chaplain team is respectful of diversity and the religious preferences and practices of others. Our goal is to offer hope that supports healing and coping through active listening, reflective conversations, prayer, spiritual counseling, inter-faith referrals, and by providing Bibles and other inspirational writings, as well as, care notes that relate to the unique needs of cancer patients and families. Spiritual Care Services and allied partners promote the wellness and wholeness of our oncology patients. Don Phelps, M.S. in Patient Counseling, D. Min.Director of Spiritual Care Services
SPIRITUAL CARE SERVICES
GYN UltrasoundGynecologic ultrasonography is a test that uses sound waves to produce an image of the female pelvic organs (specifically the uterus, ovaries and the fallopian tubes), as well as, the bladder and the adnexa.
Bone Density Screening (DEXA scan)A bone density test determines if you have osteoporosis — a disease that causes bones to become more fragile and more likely to break. A bone density test makes it possible to determine your risk of breaking bones before the fact. Additionally, a bone density test uses images to measure how many grams of calcium and other bone minerals are packed into a segment of bone. The bones that are most commonly tested are located in the spine, hip and forearm.

October 2014Vol. 5, page 13
2014 SRMC ONCOLOGY PROGRAM OUTCOMES
Rapid Quality Reporting System (RQRS) as of June 30, 2014:
According to a recent news release, those suffering from Barrett’s esophagus have a 200% greater risk of developing esophageal cancer than the average person. The five year esophageal cancer survival rate is less than 15%. This non-surgical endoscopic option can eliminate Barrett’s and help restore peace of mind for patients rather than the traditional annual endoscopy with biopsy and “wait and see” mentality previously practiced.
The procedure involves the insertion of a catheter into the esophagus where the radiofrequency therapy is delivered directly to the area affected. The physician delivers a rapid burst of high frequency energy which cauterizes a very thin layer of the abnormal esophagus. The entire procedure is done under sedation with the guide of an endoscope. No incisions are made, the recovery period is short and patients go home that same day.
2014 ONCOLOGY QUALITY SCORECARD
MEASURE DEFINITION GOAL 2014 RESULTS
Pain assessed and intensity documented (QOPI Core Measure #3, 4a & 6)
Pain assessment documentation (includes documentation of no pain) for each rad onc consult and on treatment visit: rad onc 95% 97%
Patient Sat. Rad Onc
Patients with "Would recommend radiation therapy services" 95% 100%
Patient Sat. Nurse Navigator
Patients with " Would recommend radiation therapy services" 95% 100%

October 2014Vol. 5, page 14
Gender of Esophagus Cancer Diagnosed in 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 374 Hospitals
# Gender My (N) Oth. (N) My (%) Oth. (%)1. Male 3 1,018 75% 78.31%2. Female 1 282 25% 21.69%
Col. Total 4 1,300 100% 100%
GENDER
Assessment and Evaluation of Treatment planning: Esophageal Cancers Patients
Percentage of July 2012 - June 2013 SRMC registry patients treated at SRMC for a new diagnosis of esophageal cancer whose diagnostic work up and treatment adhere to NCCN guidelines compliant compliant
QI Coordinator study #1: Head and Neck Radiation Therapy Patients’ Nutritional Status While Receiving Radiation Therapy
Participate in the ACOS RQRS program and report findings complete complete
RQRS
Participate in the ACOS RQRS program andreportfindings
Above the average for all programs
Refer to graph on page 13
Pathology report data
Percentage pathology reports including 100% CAP guidelines’ data 95% 99%
Pathology report synoptic format
Percentage pathology reports in synoptic format 95% 100%
SUMMARY: We have met our goals for all of our outcome measures as of June 30, 2014. Though wemetourgoals,weidentifiedonepotentialareaforimprovement: 1. Increasing physician pain assessment documentation in our MD consult note to 100%.RECOMMENDATIONS: 1. Review audit results with staff and physicians 2. Brainstorm with physicians on methods to increase their consultation note pain documentation
2011 Tumor Registry Esophageal Cancer Statistics: SRMC Compared to All US Community Cancer Programs
MEASURE DEFINITION GOAL 2014 RESULTS
October 2014Vol. 5, page 15
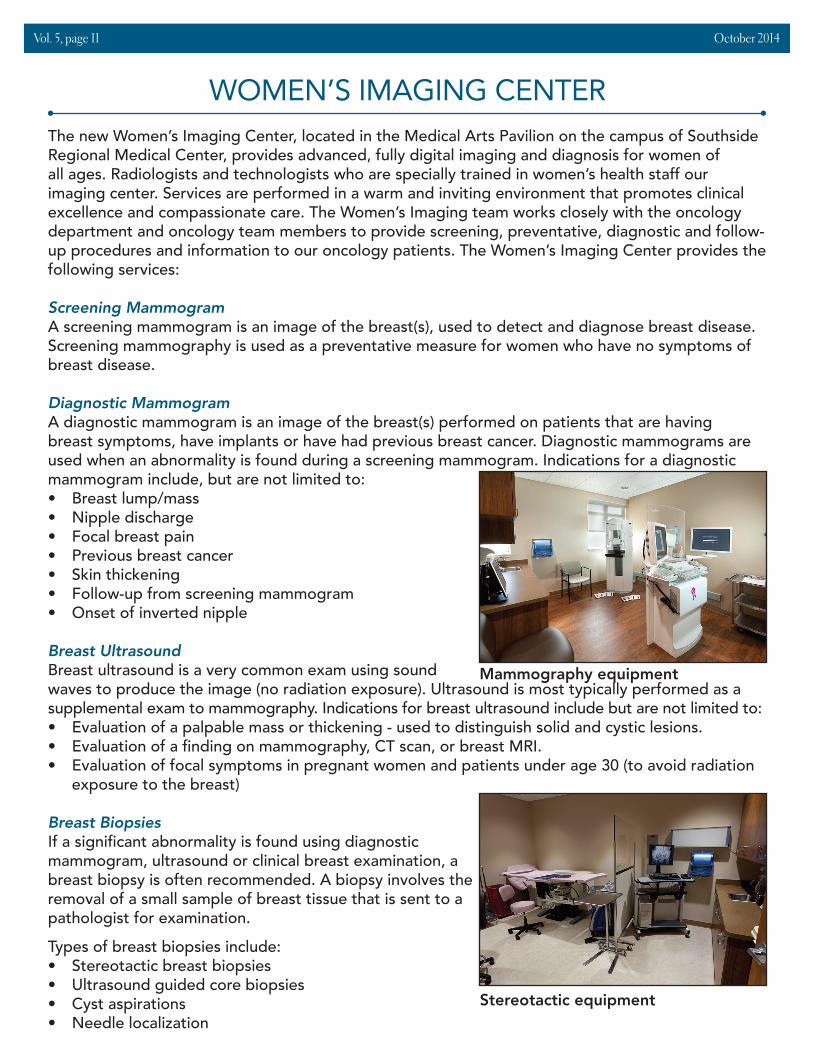
Race/Ethnicity of Esophagus Cancer Diagnosed in 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 374 Hospitals
# Race/Ethnicity My (N) Oth. (N) My (%) Oth. (%)1. White 2 1,117 50% 85.92%2. Black 2 109 50% 8.38%3. Hispanic - 43 3.31%4. Other/Unknown - 31 2.38%
Col. Total 4 1,300 100% 100%
RACE
Age Group of Esophagus Cancer Diagnosed in 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 374 Hospitals
# Age Group My (N) Oth. (N) My (%) Oth. (%)1. 20-29 - 2 - .15%2. 30-39 - 8 - .62%3. 40-49 - 72 - 5.54%4. 50-59 2 245 50% 18.85%5. 60-69 2 401 50% 30.85%6. 70-79 - 310 - 23.85%7. 80-89 - 229 - 17.62%8. 90 and over - 33 - 2.54%
Col. Total 4 1,300 100% 100%
AGE

October 2014Vol. 5, page 16
Household Income of Esophagus Cancer Diagnosed in 2008, 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 412 Hospitals
# Household Income My (N) Oth. (N) My (%) Oth. (%)1. < $28,000 1 236 8.33% 9.25%2. $28,000 - $32,999 6 411 50% 16.11%3. $33,000 - $38,999 - 551 - 21.59%4. $39,000 - $48,999 4 598 33.33% 23.43%5. $49,000 + 1 589 8.33% 23.08%6. Unknown - 167 - 6.54%
Col. Total 12 2,552 100% 100%
INCOME
Histology of Esophagus Cancer Diagnosed in 2008, 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 412 Hospitals
# Histology My (N) Oth. (N) My (%) Oth. (%)1. Carcinoma, NOS - 83 - 3.25%2. Squamous Cell Carcinoma, NOS 8 683 66.67% 26.76%3. Adenocarcinoma, NOS 3 1,493 25% 58.5%4. OtherSpecifiedTypes 1 293 8.33% 11.48%
Col. Total 12 2,552 100% 100%
HISTOLOGY
Insurance Status of Esophagus Cancer Diagnosed in 2008, 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 412 Hospitals
# Insurance Status My (N) Oth. (N) My (%) Oth. (%)1. Not Insured 1 99 8.33% 3.88%2. Private/Managed 1 685 8.33% 26.84%3. Medicaid 1 212 8.33% 8.31%4. Medicare 9 1,428 75% 55.96%5. Other Government - 73 - 2.86%
6.Insurance Status Unknown - 55 - 2.16%
Col. Total 12 2,552 100% 100%
INSURANCE STATUS

October 2014Vol. 5, page 17
First Course Treatment of Esophagus Cancer Diagnosed in 2008, 2011Southside Regional Medical Center, Petersburg, VA
vs. Community Cancer Program Hospitals in All StatesAll Diagnosed Cases - Data from 412 Hospitals
# Histology My (N) Oth. (N) My (%) Oth. (%)1. Surgery Only - 105 - 4.11%2. Radiation Only 1 219 8.33% 8.58%3. Radiation and Chemotherapy 7 883 58.33% 34.6%4. Chemotherapy Only 1 321 8.33% 12.58%
5.Surgery, Radiation and Chemotherapy 1 248 8.33% 9.72%
6. OtherSpecifiedTherapy - 79 - 3.1%7. No First Course RX 2 697 16.67% 27.31%
Col. Total 12 2,552 100% 100%
FIRST COURSE OF TREATMENT
2014 Study Results
Quality Coordinator Study: Head and Neck Cancer Patient’s Nutrition
Topic: 1. Percent of weight loss in SRMC head and neck cancer patients from the first day of their first treatment course to last day of their first treatment course 2. Percent of patients who received a speech therapy consult 3. Percent of patients who received a nutrition consult
Reasoning: Head and neck cancer patients are at high risk for weight loss and nutritional difficulties during their treatment course. These can both negatively impact their outcomes. Screenings and preventative care can assist with decreasing these issues.
Methodology: Complete audits of the above data for all SRMC radiation therapy patients with a diagnosis of head and neck cancer receiving first course radiation therapy for a new diagnosis during 2013. Compare data and outcomes to benchmarks and guidelines.
National Guidelines: NCCN Guidelines
Benchmark Comparison: NCCN Guidelines

October 2014Vol. 5, page 18
Summary of DataDiagnosis Total Weight Loss Dysphagia Consult (Y/N) Nutrition Consult (Y/N)
Base tongue 6% Y YOropharynx 6% N Y
Parotid 1% N YTongue 10% Y YGlottis 8% Y YGlottis * Y YGlottis 8% Y YGlottis * Y Y
Base tongue * Y Y*treatment not complete at
time of audit 78% 100%Performance Improvement Recommendations: • Include nutritionist and dysphagia clinic consults as SRMC standard of care pre-first course
radiation therapy for all newly diagnosed esophageal patients. Update process to assure 100% referrals for both consults for all head and neck patients prior to the start of radiation therapy as first course of treatment.
• Create a standard patient education resource to be given to all new esophageal and other head and neck patients to assist with nutritional education prior to the start of radiation therapy.
Monitoring of Study Effectiveness: This study was effective in demonstrating that our esophageal patients do lose weight during treatment, the need for obtaining nutrition and dysphagia consults and the need for physician support for these consults and support. It also brought attention to the need to create a standard process and tool for head and neck cancer patient education about nutrition.
Quality Improvements Implemented: • Processes updated to include a nutrition and speech therapy consult on all radiation therapy
patients with head and neck cancers prior to start of treatment• A patient education handout entitled “Diet and Cancer Treatment” is now included in all head
and neck cancer patients’ cancer center packet. Patients and families use this tool to complete education requirements prior to the start of radiation therapy and PRN.
Quality Coordinator Study: Lung Cancer Molecular Testing at SRMCTopic: 1. SRMC Registry lung cancer patient statistics 2. Processes for obtaining lung cancer diagnostic specimens 3. Epidermal Growth Factor Receptor and Anaplastic Lymphoma Kinase testing of lung cancer pathology specimens
Reasoning: Lung cancer is SRMC’s number one occurring cancer site diagnosis. Lung cancer has a high mortality rate and is routinely diagnosed at later stages than other cancers. Due to many recent medical advances, the diagnosis, treatment and care of lung cancer continues to change. Many gene mutations have been identified, along with diagnostic tests and treatment directly related
October 2014Vol. 5, page 19
to these mutations, especially in adenocarcinoma. These tests and treatments can be costly, but are necessary to provide the most appropriate available treatment for patients. Because of these advances and continued changes in this field of medicine, it is difficult for every provider and practice/facility to remain up-to-date on the newest changes in quality, most cost-effective diagnostic and treatment choices for their patients with lung cancer.
To assist with improving the overall quality of lung cancer care nationally by providing its members with easy access to education, assessments and program planning tools and resources, the Association of Community Cancer Centers (ACCC) offered a few of its members the opportunity to participate in a Molecular Testing for Lung Cancer: Learning Labs for Process Improvement Project. SRMC applied to participate in this project and has been accepted.
Once this project is completed, the results will be shared with other cancer programs to assist
Criteria: All SRMC Cancer Registry patients with a primary diagnosis of lung cancer from November 1, 2012 through October 31, 2013.
Methodology: SRMC completed the following items:1. Created a multidisciplinary team to participate in this project2. Completed baseline data collection for all SRMC Cancer Registry patients diagnosed at
with a primary lung cancer from November 1, 2012 through October 31, 20133. Completed an initial survey4. Arranged and hosted a two-and-a-half hour interdisciplinary learning lab to include
education about molecular testing, review of submitted data, identified barriers to molecular testing, and potential areas for improvement
ACCC assisted by:1. Coordinating the project2. Providing resources and tools3. Overseeing the project4. Reviewing and assisting with interpretation of data and presented this to the team5. Presenting the learning lab and encouraging active participation of our team6. Facilitating team brainstorming to identify potential areas for improvement and
interpretation of the data7. Providing a summary of the learning lab possible improvements8. Serving as a resource to assist with the improvement implementation9. Sharing experiences from the project with all ACCC members and assisting them in
completing their own similar projects
National Guidelines: • National Comprehensive Cancer Network (NCCN)• College of American Pathologists (CAP)• American College of Surgeons (ACOS)• National Quality Forum (NQF)• Quality Oncology Practice Initiative (QOPI)

October 2014Vol. 5, page 20
Summary of Findings
Total Pts. = 90%
Input%
Input I IIA IIB IIIA IIIB IV%
FNA%
Core%
InadequatePlace of Diagnosis 71% 29% - - - - - - - - -Stage at Diagnosis
for Pts. with Adenocarcinoma - - 7 3 0 13 20 57 - - -
Percent with EGFR and ALK Completed
by Stage - - 100 100 n/a 100 67 41 - - -Biopsies Performed by an Interventional
Radiologist - - - - - - - - 75% 25% <1
Biopsies Performed by a Pulmonologist - - - - - - - - - - 80-85%
1. Discussion of the possible reasons for the exceptionally high percent of lung cancer patients being diagnosed in the inpatient setting revealed the following potential community barriers and issues: economy, culture, being a part of the “tobacco belt,” high number of the community members with no PCP who utilize SRMC ER as their “PCP,” uninsured/underinsured, history of later stage for diagnosis of most cancers, increased mortality rates for all cancers, history of a poor community health status and the lack of a lung screening program.
2. We were unable to determine the reasons why the tests were not performed from the path reports, as well as, if this was discussed with the referring physician from the registry and basic chart review. Further investigation revealed the following reasons for non testing: one patient with end of life care only (not beneficial to obtain), two pathology reports not from SRMC (unable to access reason for not obtaining result and unable to affect an improved outcome for these patients), three path specimens that were pleural fluid only (no tissue and inadequate for molecular testing) and three were tissue from an FNA with no order for testing.
3. Core needle biopsies are generally preferred for better results.
4. We found that the pathology specimens obtained by pulmonolgists that were inadequate for diagnosis were primarily bronchial washings, brushings and biopsy with forceps specimens. Also, a pathologist or technician is not routinely on-site during the procedure to obtain these specimens and assess for tissue adequacy.
Performance Improvements Completed:
1. Improved our reflex molecular testing pathway for lung adenocarcinoma, with 100% compliance to date
2. Improved tracking, measurement and documentation of molecular testing for advanced Non Small Cell Lung Cancer
3. Add a note to the template for lung cancer patients’ pathology reports that can be utilized to

October 2014Vol. 5, page 21
CANCER CONFERENCES (TUMOR BOARD MEETINGS)Submitted by: Mohammed Ali, MD, Radiation Oncology
During the last three years, I have seen a steady growth in the attendance of our tumor board meetings. This is certainly a testament of the interest of different disciplines involved and also the hard work of the staff to select and sort out cases for presentation. These weekly meetings help to decide the best course of action for the treatment of our patients at SRMC.
The overall atmosphere of these meetings is pleasant, open to discussion, and congenial to welcome to discussion relevant to these cases. This also provides a platform for discussion of newly published data in medical journals. The tumor board meetings also provide a venue for discussion of a range of services and their interplay from the diagnosis to the complex treatment which includes the supportive and/or terminal care if needed, i.e., hospice. On occasions patients may need some financial help or other kinds of assistance for their treatments, and the tumor board helps identify these issues and determine how we may help.
According to recently published data* 11.2 million cancer survivors are living in the United States, and 450,000 are of reproductive age. The tumor board focuses not only on the survival following the aggressive treatment by surgery, chemo, and radiation therapy, but also the quality of life issue both in the young and the not-so-young patients.
These weekly sessions include interactive discussion regarding treatment toxicity, both short and long term, in an effort to minimize toxicity and improve long term functional outcomes. Overall, there is a close interaction between the disciplines for the betterment of patients undergoing treatment for a variety of cancer diagnoses and their management.* Pro-Journal, Professional Radiation Oncology/American Society of Radiation Oncology 2012, Volume 2, pages 242-247
state when the managing physician and the pathologist have discussed the need for these tests and it has been decided that the test results are not needed for this patient.
2015 Potential Performance Improvement: The Cancer Committee will choose at least one goal and one quality measure to monitor in 2015 from the following:1. Establish consensus on how physicians will manage inpatients diagnosed with Non Small Cell
Lung Cancer and require molecular testing including addressing the “14-day rule”2. Improve chart documentation and consider adding some of the National Quality Forum or
American Society of Clinical Oncology related measures to our registry data fields3. Choose one or more of the related quality measures from Quality Oncology Practice Initiative
(#81, 84, 85, 88 or 89) and/or National Quality Forum (#0386, 0455, 0457, 2020, 0383 or 0208) to study in 2015
4. Develop an approved process for decision making on how potential lung cancer patients will get biopsied and who will complete this procedure
5. Implement strategies to decrease the number of lung cancer patients diagnosed as inpatients6. Implement strategies to assist with diagnosis of lung cancers at earlier stages
Monitoring of Study Effectiveness: Very effective in educating the multidisciplinary team, increasing participation by all team members in quality improvement related to molecular testing and identifying our use of molecular testing in lung cancer diagnosis and potential areas for improvements. Status: Completed.

October 2014Vol. 5, page 22
More than 1.6 million people will be diagnosed with cancer this year, and about half of all cancer patients undergo radiation therapy. After beating cancer, some patients who undergo radiation therapy discover a hidden complication that may not come to light until years after they concluded treatments. According to the American Cancer Society, serious radiation complications can occur in up to five percent of patients who receive therapeutic radiation.
Radionecrosis occurs when the body is unable to supply enough oxygen to the affected area of the patient’s body. Hyperbaric oxygen therapy, available at Southside Regional Wound Healing Center, increases the amount of oxygen to the wounds, allowing them to heal from the inside. “Hyperbaric oxygen therapy is the only therapy known to reverse the vascular compromise responsible for late radiation effects,” says Scott Covington, MD, FACS, CHWS, Executive Vice President, Medical Affairs for Healogics, a network of wound care centers around the world that specialize in treating radiation injuries. “There are no alternative therapies that correct the problems these patients have, although narcotics and antidepressants have been used to control the pain with limited success and significant side effects. Nothing is a cure-all, but hyperbaric oxygen therapy offers 60 to 80 percent of patients either improvement or complete resolution of the injury.”
The Wound Healing Center at SRMC, managed by Healogics, provides specialized treatment for chronic or non-healing wounds, including those caused by the late effects of radiation. The physicians and clinicians at the Wound Healing Center have access to state-of-the-art treatments available, including hyperbaric oxygen therapy, debridement, dressing selection, and patient education.
WOUND HEALING CENTER
EDUCATIONEducation is entwined into all aspects of the SRMC Oncology program. The Education Department is an active participant of the oncology steering, cancer and quality committees. They assist with assessment, planning and implementation of educational programs and the provision of educational material.
SRMC supports oncology-specific continuing education for health care providers—physicians, nurses and technologists. The multidisciplinary Tumor Board meets every Wednesday and provides one continuing medical education (CME) credit for each. During the past year, the Cancer Committee has provided a platform for a variety of presentations on “Palliative Care,” “Speech &

October 2014Vol. 5, page 23
WOUND HEALING CENTER
SRMC is proud to offer our “Care Partners” program to any oncology inpatient and their loved ones. This innovative program is designed to involve loved ones in the day-to-day care of hospitalized patients. The primary goal of Care Partners is to increase the confidence and skill of loved ones who will be caring for patients once they are discharged. In working with the hospital staff, loved ones feel like they are a part of the team and gain satisfaction from helping their loved ones. They also better understand the care required once the patient is discharged. Care Partners also gain a feeling of experience, which can greatly decrease the anxiety often involved with caring for patients at home.
Care Partners can assist with their loved ones’ care by working with the staff on a wide range of care items. It can be as general as assisting with a bath, changing linens or ordering a meal. Or it can be as specific as assisting staff
with turning, tube feeding or even ostomy or wound care.
Two of the most wonderful “side effects” of the Care Partners program are communication and touch. Care Partners provides a setting for:
• a son who has never assisted his mother with denture-cleaning
• a husband who has not brushed his wife’s hair• a grandson who has never positioned
pillows and watched “Wheel of Fortune” with his grandfather
• a daughter who can’t remember the last time she and her mother touched as she stands before her with a bottle of lotion
A patient referral to Care Partners provides a lovely opportunity to encourage, teach and support those willing to help their loved during a hospital stay. The results can be life-changing for families. Patients may be referred by hospital staff, physicians, family, friends or self-referred.
To refer a patient or to obtain more information about Care Partners, please call Lisa Mason at 804-765-5683.
“Two of the most wonderful ‘side effects’ of the Care
Partners program arecommunication and touch.”
Swallowing Therapy for Oncology Patients,” and “HPV and Cancer.” SRMC also sponsored CME presentations on “Current Treatment Strategies for Chronic Mylogenous Leukemia” and “Prostate Cancer Update.”
SRMC also supports oncology nursing certification. Certified Oncology Nurses are clinical experts, dedicated to providing the best, evidenced-based care. These oncology-certified nurses provide continuing education for additional oncology nursing staff. Furthermore, all SRMC oncology nurses complete an Oncology Nursing Society and Oncology Nursing Certification Corporation Chemotherapy Biotherapy Certificate Course. This course equips nurses with the knowledge needed to safely administer chemotherapy and biotherapy agents to our patients.
Patient education is incorporated into the daily care of our oncology patients. An education center is located in the Cancer Center providing all patients access to the most up-to-date technologies and evidence-based treatment modalities available. Educating patients and their families is an integral part of their care at SRMC.
October 2014Vol. 5, page 24
ONCOLOGY NURSE NAVIGATION PROGRAM
Oncology navigation is the process of guiding patients through the continuum of care from pre-diagnosis through treatment and then survivorship. The Oncology Nurse Navigator is a RN with oncology expertise who assists patients, families and their health care providers by identifying patient and family needs; providing psychosocial and emotional support; assisting with navigating the health care systems and processes; assisting with understanding and connecting with referral resources; overcoming disparities and barriers; advocating for the patient and family; assisting with coordination of care and communication between providers; and understanding the options available for meeting their needs.
The oncology navigation services are available free of charge to all SRMC patients and families, as well as, any non-SRMC community member. Issues the navigator may assist with include, but are not limited to: education, emotions, insurance, cost of care, medications, finances, transportation, symptom management, pain control, palliative care, access to care, quality of life, healthy living, home care assistance, legal assistance, healthy living/wellness, nutrition, fertility, genetics, decreasing and/or preventing suffering, end of life planning, survivorship planning, spirituality and community support. This assistance may be on site or by referral process off site as necessary to meet the patient’s needs.
Our SRMC navigation program began with the hiring of our first nurse navigator in January of 2012. Since then, we have been honored to assist over 600 patients. We are eager to see continued growth in the years to come. These patients and their families have received support emotionally, spiritually, financially, and physically.
Many of these navigation patients have received financial counseling assisting them in receiving financial assistance from local and national organizations such as: American Cancer Society, Breast Cancer Society, Livestrong Camp Kesem, Prince George Christian Church, United Way, reduced rates for medications, SRMC Cancer Center fund donated by The Hospital Guild, local churches, Cancer Care, Ostogroup, Hollister, First Baptist in Hopewell and Head and Neck Cancer Alliance. The outpouring of support deserves a special thank-you to every agency, group and individual who has helped SRMC to relieve some of these patients’ stress by meeting their individual needs.
Since we have moved into the new Cancer Treatment Center, located in the Medical Arts Pavilion, we have held monthly cancer support groups. This group meets on the second Wednesday of each month from 11:00 a.m. – 12:00 noon. Care Advantage provides lunch, thus an RSVP is very helpful but not required. We welcome patients and their families whether they are in active treatment or completed treatment. We have had focused groups on nutrition, spiritual care, exercise and activity provided by the YMCA, and self-care and coping from Crater Community Hospice. We will continue to offer this group and expand as needed for any future growth.
We continue to provide our patients with a survivorship care plan after they complete their treatments. This is provided during their first follow-up visit to the radiation therapy department after completion of their treatment plan. During this visit, a radiation oncology nurse and the physicians educate the patients on recommended guidelines for managing their follow-up care
COMMUNITY RESOURCES AND SUPPORTS

as well as education on what to expect in the following months after treatment completion. The oncologist and the oncology nurse review these guidelines with the patient and then provide a personal individualized copy of the guidelines and education for their personal records.
We have also partnered with the Petersburg YMCA to enable them to bring a Livestrong Survivorship program to Petersburg in 2013. This program has been expanded for 2014 and is now called Return to Wellness. It is a small group personal training program for individuals with medical barriers preventing exercise. The cost is $20.00 per person for six weeks. For more information on this program feel free to contact Ben Buckley at 804-733-9333 or contact the Petersburg YMCA:
120 N. Madison St, Petersburg, VA 23803. This program is structured to assist our cancer patients back to a healthy lifestyle and increase their strength for day-to-day activities. If there is ever a concern for covering this cost, please contact Lori McNulty at 804-765-5095.
The new year will bring with it continued change for our patients and our oncology program. In 2015, we will continue to grow and plan new venues to assist even more patients and families to meet their needs. We are here to help meet our patients’ families’ and communities’ needs and to improve their access to resources within the hospital and the community. Our goal will continue to be focused on assisting those experiencing the effects of cancer at anytime throughout their journey.
Physical rehabilitation compliments oncology care and helps to complete the circle of holistic care provided to the patient. Rehabilitation should be considered before sending patients to fitness gyms to exercise because many times patients have physical impairments that may be overlooked that would prevent them from obtaining maximal benefit from performing general exercise. Rehabilitation aims to help cancer survivors get back to living and enjoying their life as normal as possible after they have completed their oncology treatment. Our rehabilitation department is able to follow-up with patients inside of the hospital and at two convenient outpatient clinics located in Petersburg and Colonial Heights.
Physical TherapyPhysical therapy is used to help treat many of the impairments cancer survivors may experience as a result of the disease process and treatment process. Physical therapy can be beneficial to treat the following impairments:• Balance deficits• Weakness and deconditioning• Joint pain • Range of motion return following conditions such as breast, head and neck cancers• Incontinence• Falls• Chemotherapy-induced peripheral neuropathy• Muscle pain• Orthotic and prosthetic consultation• Assistive devices• Women’s health issues
REHABILITATION SERVICES
October 2014Vol. 5, page 25

Lymphedema Therapy:Lymphedema occurs when the lymphatic system is damaged or blocked. Protein-rich fluid builds up in the soft body tissues and causes swelling. Secondary lymphedema is a common problem that may be caused by damage to the lymphatic system due to cancer and cancer treatment.
Possible signs of lymphedema include:• Swelling of the arm or leg including the fingers and toes• Full or heavy feeling in the arm or leg• Tight feeling in the skin• Thickening of the skin• Tightness of clothing, shoes, watches, rings• Itching• Loss of hair
Unfortunately, there is no cure for lymphedema, but it can be managed with Complete Decongestive Therapy (CDT). The goal of CDT is to reduce the swelling and maintain that reduction with the application of compression therapy.
It is important to treat lymphedema to reduce the risk of infection, reduce pain, and improve range of motion. Treatment also helps prevent skin changes and skin ulcerations. Patients who have had breast cancer, ovarian or uterine cancer are especially good candidates for lymphedema treatment.
Occupational Therapy Individuals may benefit from occupational therapy intervention if they are actively receiving treatment for cancer or if they are working on rebuilding their lives after the completion of treatment. People who are challenged with cancer may experience difficulty in being able to perform routine tasks in their daily personal or work life. An occupational therapist can help in the following areas:
• Relaxation and energy conservation techniques • Improving ability to perform functional activities • Exercises to help with task improvement while using hands and arms • Bed mobility • Recommending different positions to decrease pain and improve comfort while sleeping• Adaptive equipment to assist with activities of daily living• Safe mobility • Higher level thinking activities such as safety in the kitchen, creating a grocery list, or following
a daily medication schedule• Memory problems, limited attention, problem solving skills and limited judgment abilities as
result of radiation or chemotherapy treatments
Occupational therapy can address occupational performance for individuals with cancer of various stages in the disease process. Treatment may be started in an acute care setting or the outpatient setting to improve performance.
Speech Language PathologyHead, neck and lung cancer patients frequently have voice and swallowing disorders that may benefit from speech therapy treatment. Patients who have undergone radiation treatment may have some of the following signs and symptoms and may benefit from speech therapy:
October 2014Vol. 5, page 26

• Sore throat• Dry mouth• Acid reflux• Sensitive mouth• Mouth sores • Decreased taste• Fatigue • Breathing difficulties from swelling and dysphagia • Silent aspiration • Poor intake
Myofascial release and electrical stimulation are effective treatment methods in this population when appropriate. Voice treatment for improved vocal quality and efficacy of communication is also necessary for many of these patients following treatment of laryngeal cancer. Patients with a laryngectomy often benefit from speech treatment for use of an electrolarynx, esophageal speech, or tracheoesophageal puncture (TEP) for communication as well as dysphagia treatment when appropriate. For more information, please call us: Colonial Heights: 804-526-1352; Petersburg: 804-765-6660.
CREATING A CULTURE OF SAFETY
‘Patient Safety,’ ‘Risk Management’ and ‘Medical Error’: If you’re like most people those seem like problems for hospital administration to deal with, ultimately to be solved by making sure that the nurses, pharmacists and technicians just follow the rules. In Oncology, some of our high-risk services include chemotherapy and biotherapy administration, radiation therapy treatments, planning and symptom management and side effect prevention. As Oncology providers, we need to keep our patients safe from harm while undergoing any of the above treatments or services.
Risk Management serves as a resource for patient safety and risk management. Sandy Underhill, Director of Risk Management, and Kimberly Overton, Risk Management Coordinator, review reported safety events, produce trending reports, lead the Patient Safety Committee and assist all hospital departments
October 2014Vol. 5, page 27
in identifying and mitigating the risk of patient harm. According to Underhill, “We have pledged to make our organization a safe place to work and receive safe and trusted health care. Our mission is to advance patient safety, reduce uncertainty and maximize value through management of risk.”
Stemming from the work that produced the 1998 “To Err is Human” study, in which an estimate of more than 100,000 deaths per year were attributed to ‘Medical Error,’ an entire new area of basic science has been added to the study of medicine. Safety Engineering, Risk Science, and Medical Management (or Health Care Management) now focuses the same rigor of research on saving lives and preventing injury or morbidity from error as we were taught in laboratory and practice to use against oncologic or congenital diseases.

From our colleagues in this new research we can indeed identify that the nursing team is responsible for 39% of errors occurring in a hospital that threaten patients and yield bad outcomes not caused by the patients’ presenting condition. Nurses are responsible for 78% of all patient encounters, treatments, transports, and medications. Physicians are responsible for the remaining 22% of the patient’s encounters in the hospital, and are responsible for another 31% of medical errors, and physician errors are more likely to be fatal.
Scientists in disciplines in which even a single error can precipitate results which are fatal to persons and/or entire organizations, costly in dollars, life and time, have developed the multidisciplinary study of processes to mitigate error with the goal of zero such events of preventable failure or harm. Organizations who make these processes into mandated operational practice are working to be “High Reliability Organizations” (HRO). Since the late 1960s, the air travel, nuclear, automotive, and structural engineering industries have made great strides in this study resulting in overall improvement in their risk profiles on the order of 82-98% (the latter signified by the aerospace and nuclear industries). During that time the hospital medicine error rate has remained essentially unchanged.
As leaders in providing patient care within SRMC, the extent to which we become a high reliability organization, a safe place for our patients to heal, is in our hands. Our colleagues have learned that “hard wiring” a few personal disciplines, like the ones we used to master our profession, will make all the difference. When we endeavor to collaborate as colleagues with similar processes, practices and disciplines, our patients benefit as their risk of error and injury are greatly reduced. With a joint focus on patient safety, all stakeholders in the health care industry benefit.
Southside Regional Medical Center High Reliability Team and Daily Safety Huddle
The High Reliability team consists of the Chief Executive Officer, Assistant Chief Executive Officer, Chief Operating Officer, Chief Quality Officer, Assistant Chief Nursing Officer, Chief Medical Officer, Community Cares Champion and Risk Management. The team is responsible for monitoring the facility’s safety metrics, and
training leaders to deliver error prevention tools quarterly. They are also responsible for monitoring compliance with the error prevention education, collecting and sharing best practices, rounding with purpose, and celebrating staff and physicians who have prevented harm using various error prevention tools.
Daily Safety Huddles are conducted at 9:00 a.m. with all department directors in attendance to maintain awareness of operations and to give direction about priority and responsibility for resolution of any known or potential safety issues. “SAFETY FIRST” is the first item on ALL meeting agendas regardless of the meeting topic.
Safety Error Prevention Tools
In order to “hard wire” a culture of safety it is necessary to implement tools that are easy to remember and create safe behaviors at every level of the organization. The SAFE error prevention tool has been introduced into the SRMC safety culture and provides simple techniques which form the foundation of the
Daily Safety Huddle Agenda
1. Look Back - Identify significant safety or quality issues from the last 24 hours/last shift
2. Look ahead - Identify anticipated safety or quality issues in next 24 hours/next shift
3. Follow up on Start-the-Clock Safety Critical Issues
October 2014Vol. 5, page 28

The Case Management Department is available to assist any oncology patient who is hospitalized and has complex discharge planning needs. They work with the patient’s insurance provider to support the hospitalization. If the inter-disciplinary team recommends an inpatient to receive further assistance, equipment or care after discharge, the assigned case manager will assist with the coordination of these services. The case managers will work with the patient and family to arrange services such as home care, hospice care, palliative care, durable medical equipment, acute rehab and/or skilled nursing home placement. Every unit in the hospital has a case manager assigned to assist them with the coordination of discharge needs. Any patient or family can request for a hospitalized patient to receive a case management visit by asking the physician or nurse.
CASE MANAGEMENT DEPARTMENT
October 2014Vol. 5, page 29
High Reliability Culture. These tools were developed as part of an evidenced based analysis from other high reliability organizations and have proven to be effective in reducing errors.
When errors and mistakes result in harm, we fail in our promise, and we fail those we serve. Harm turns health to hurt. Our patients take it for granted that we will heal without harm. We cannot take it for granted. In our journey to deliver quality care, the only acceptable goal is zero events of harm. To be a leader, we need to deliver healing without harm reliably – each time, every time.

As our patients come to our center, they have much more to deal with than just the diagnosis of cancer. Our mission is to help our patients meet as many of their needs as possible. We help take care of them and their family while we treat their cancer.
SRMC has a provided a Community Resource Center (oncology resource library) within
the lobby area of our new Cancer Center at 210 Medical Park Blvd, Petersburg, VA. This resource area is open to our patients and the public. The Resource Center offers both general and disease specific information about cancer, cancer care, cancer prevention, cancer screening and wellness. There is also a computer for use in searching for cancer related information. Our patient navigation and registration staff are also available to assist in finding specific information, offer additional support and resource referrals and/or to answer any questions. Patients, families, friends and community members are encouraged to stop in anytime Monday-Friday from 8:00 a.m. - 4:30 p.m.
SRMC’s oncology department also offers and refers patients and loved ones to support groups that assist them in their cancer journey. Whether patients and families attend one or all of the support meetings, support groups can be very beneficial in assisting patients and families to cope with their disease. The following support groups are available in our area and have provided a great resource to our patients and the community:
A partnership with Good Neighbor Counseling Services has
given our patients access to increased services. With this partnership, we have a social work intern on site two days a week assisting with
support groups and distress screenings. This partnership enables us to reach more patients and families and assist them with gathering resources and making resource referrals during their time of need. Good Neighbor Counseling Services provides individual and family counseling at their office in Colonial Heights through referrals.
We have also started to host the American Cancer Society’s
program Look Good Feel Better as of this past May. This is a workshop for women offered while in active treatment to help them combat the appearance-related side effects of cancer treatment. It is a volunteer-based workshop that is hands-on with makeup, skin care, nail care, and tips on dealing with hair loss. Each woman receives a free makeup kit to use during the workshop and take home with her once she completes this session. Our patients have truly enjoyed each Cancer Support Group and Look Good Feel Better session. If you would like more information about these groups, please call Lori McNulty (804-765-5095) or Faye Flemming (804-765-5884) anytime.
YMCA Return to Wellness program is a small group personal training program for individuals with medical barriers preventing exercise. This is a six-week program and the cost is $20 per person. This is offered at the Petersburg YMCA 120 N. Madison Street, Petersburg, VA 23803. Please contact the YMCA at 804-733-9333. The goal of this program is to improve energy levels and improve flexibility and endurance.
Tri-Cities Pink Challengers Breast Cancer Support Group started in our area after a group of ladies had been given the opportunity to reflect on their cancer journey as a research project with VCU. After this project they wanted to continue meeting and open their group to other breast
SUPPORTIVE SERVICES FOR ONCOLOGY PATIENTSOctober 2014Vol. 5, page 30

cancer survivors. This group currently meets at the Petersburg YMCA at 120 N. Madison Street, Petersburg, VA 23803 on the third Thursday of the month from 6:00 – 8:00 p.m. In partnering with the YMCA, the group is able to offer exercise programs every other month and educational opportunities on the opposite months.
The Cancer Registry is a specialized database that contains the systematic collection of reportable malignancies. This includes cancers and benign/borderline brain and central nervous system tumors, which are diagnosed and/or treated at the hospital. Complete diagnosis, staging and treatment are captured as part of a compiled summary of each patient’s disease process. In a hospital, a Certified Tumor Registrar (CTR) is responsible for entering cases into the Cancer Registry. A CTR works with a Registry Clerk who initially reviews cases for reportability, and places their demographic information in the registry until they are ready to be reviewed by the CTR. The clerk helps retrieve treatment information and performs follow up on patients yearly. Patient follow up provides valuable recurrence and survival information. The cancer registry works with hospital administrators and physicians by supplying data reports to help access local area cancer needs, quality measure, etc. Lastly, cancer data reporting is required by both the American College of Surgeons, Commission on Cancer and the Virginia State Cancer Registry. Data submitted to these agencies is used in a variety of ways for statistical and epidemiologic purposes.
WHAT IS A CANCER REGISTRY?
The SRMC Cancer Committee along with the American Commission on Cancer (COC) appoints a Cancer Liaison Physician (CLP) to serve as a member of the cancer committee. Each CLP serves a three-year term, but may be reappointed indefinitely. These physicians help to oversee the clinically related items for cancer programs and cancer committees. Their primary responsibility is to lead the cancer program’s efforts to evaluate, interpret and report oncology related performance, with special emphasis on SRMC’s tumor registry and National Cancer Data Base (NCDB) data. This is completed on a quarterly basis. The CLP also reports CoC activities to the multidisciplinary team and serves as an SRMC liaison with the American Cancer Society (ACS).
Dr. Boyd Wickizer, Chief Medical Officer, serves as SRMC’s present CLP. This is his second term in that position. He also leads the Oncology Quality Committee along with our Chief of Quality Officer, Joyce Dayvault. This committee evaluates our oncology program and identifies areas for growth in a multidisciplinary setting. Dr. Wickizer also is a member of our Oncology Steering Committee and attends committee meetings to assist with brainstorming and planning of our oncology service line.
CANCER LIAISON PHYSICIAN
October 2014Vol. 5, page 31
We hope this information is helpful. Please call our nurse navigator, Lori McNulty, at 804-765-5095 for any additional information on these programs.

The SRMC Quality Department is a very important part of the oncology team. The Chief Quality Officer (CQO) oversees the Quality, Infection Control and Medical Staff Office Departments and staff as well as all hospital-wide quality and accreditation and regulatory requirements. The CQO is a member of the Cancer Committee, assists Dr Wickizer in leading our Oncology Quality Committee, and serves as our Cancer Committee Quality Coordinator. Quality department staff attend oncology steering committee meetings; lead our quality studies, projects and initiatives; work with other staff to oversee oncology and other accreditations; and assist all oncology team members and departments in ensuring high quality cancer care.
Each year, the oncology quality coordinator oversees several quality related studies to access our oncology programs, services and care. These are reported to the Cancer Committee and the results are published yearly in our annual report. Our Quality Department also remains up-to-date on all local, state and national regulations to assure compliance within our program.
SENIOR ADMINISTRATIONThe SRMC Administrative Team, including the SRMC Board of Trustees and the Corporate Leadership Team, takes an active role in overseeing the SRMC Oncology Service Line and the development of oncology services to meet community defined needs. This includes developing relationships with area providers of oncology services such as Radiation Oncologists, Medical Oncologists, Pathologists, Radiologists, Surgeons, Primary Care and other Physician Specialists to ensure all physicians have the tools they need to provide high quality accessible oncology care to their patients. The Senior Team also manages financial resources needed to hire the appropriate staff, purchase equipment, contract with vendors for services and expand and enhance facilities.
This past year SRMC dedicated over eight million dollars in capital to build our new SRMC Cancer Center in the Medical Arts Pavilion and equip it with some of the most advanced cancer treatment equipment available. In 2014, there is an additional $3.5 million planned to further enhance the equipment offerings to provide a truly comprehensive cancer center. In collaboration with the Oncology Service Line Director, the administrative team also helps to develop and expand services to compliment the oncology service line such as the nurse navigation program, support groups, and community outreach. It is an exciting time for SRMC and for the community it serves.
October 2014Vol. 5, page 32
THE SRMC QUALITY DEPARTMENT
210 Medical Park Boulevard • Suite 100 • Petersburg, VA 23805 • (804) 765-5850 • SRMConline.com