![I 2018nopr.niscair.res.in/bitstream/123456789/45328/1/VP 66-67... · 2018. 10. 29. · gSa] jhV~ohV djrs gSa vkSj lks'ky ehfM;k ij vius QsojsV cukrs gSaA bl losZ ds vuqlkj] Hkkjr](https://static.fdocuments.in/doc/165x107/60c566281fdb6429c17c96ba/i-66-67-2018-10-29-gsa-jhvohv-djrs-gsa-vksj-lksky-ehfmk-ij-vius-qsojsv.jpg)
vol 13 5 2009 - Revues et...
74
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) Scope The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It presents structured review articles ("cards") on genes, leukaemias, solid tumours, cancer-prone diseases, more traditional review articles on these and also on surrounding topics ("deep insights"), case reports in hematology, and educational items in the various related topics for students in Medicine and in Sciences. Editorial correspondance Jean-Loup Huret Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France tel +33 5 49 44 45 46 or +33 5 49 45 47 67 [email protected] or [email protected] Staff Mohammad Ahmad, Mélanie Arsaban, Mikael Cordon, Isabelle Dabin, Marie-Christine Jacquemot-Perbal, Maureen Labarussias, Anne Malo, Catherine Morel-Pair, Laurent Rassinoux, Sylvie Yau Chun Wan - Senon, Alain Zasadzinski. Philippe Dessen is the Database Director, and Alain Bernheim the Chairman of the on-line version (Gustave Roussy Institute – Villejuif – France). The Atlas of Genetics and Cytogenetics in Oncology and Haematology (ISSN 1768-3262) is published 12 times a year by ARMGHM, a non profit organisation, and by the INstitute for Scientific and Technical Information of the French National Center for Scientific Research (INIST-CNRS) since 2008. The Atlas is hosted by INIST-CNRS (http://www.inist.fr) http://AtlasGeneticsOncology.org © ATLAS - ISSN 1768-3262
Transcript of vol 13 5 2009 - Revues et...

Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5)
Scope
The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It presents structured review articles ("cards") on genes, leukaemias, solid tumours, cancer-prone diseases, more traditional review articles on these and also on surrounding topics ("deep insights"), case reports in hematology, and educational items in the various related topics for students in Medicine and in Sciences.
Editorial correspondance
Jean-Loup Huret Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France tel +33 5 49 44 45 46 or +33 5 49 45 47 67 [email protected] or [email protected]
Staff Mohammad Ahmad, Mélanie Arsaban, Mikael Cordon, Isabelle Dabin, Marie-Christine Jacquemot-Perbal, Maureen Labarussias, Anne Malo, Catherine Morel-Pair, Laurent Rassinoux, Sylvie Yau Chun Wan - Senon, Alain Zasadzinski. Philippe Dessen is the Database Director, and Alain Bernheim the Chairman of the on-line version (Gustave Roussy Institute – Villejuif – France).
The Atlas of Genetics and Cytogenetics in Oncology and Haematology (ISSN 1768-3262) is published 12 times a year by ARMGHM, a non profit organisation, and by the INstitute for Scientific and Technical Information of the French National Center for Scientific Research (INIST-CNRS) since 2008. The Atlas is hosted by INIST-CNRS (http://www.inist.fr)
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

The PDF version of the Atlas of Genetics and Cytogenetics in Oncology and Haematology is a reissue of the original articles published in collaboration with the Institute for Scientific and Technical Information (INstitut de l’Information Scientifique et Technique - INIST) of the French National Center for Scientific Research (CNRS) on its electronic publishing platform I-Revues. Online and PDF versions of the Atlas of Genetics and Cytogenetics in Oncology and Haematology are hosted by INIST-CNRS.
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Scope
The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It presents structured review articles ("cards") on genes, leukaemias, solid tumours, cancer-prone diseases, more traditional review articles on these and also on surrounding topics ("deep insights"), case reports in hematology, and educational items in the various related topics for students in Medicine and in Sciences.
Editorial correspondance
Jean-Loup Huret Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France tel +33 5 49 44 45 46 or +33 5 49 45 47 67 [email protected] or [email protected]
Staff Mohammad Ahmad, Mélanie Arsaban, Mikael Cordon, Isabelle Dabin, Marie-Christine Jacquemot-Perbal, Maureen Labarussias, Anne Malo, Catherine Morel-Pair, Laurent Rassinoux, Sylvie Yau Chun Wan - Senon, Alain Zasadzinski. Philippe Dessen is the Database Director, and Alain Bernheim the Chairman of the on-line version (Gustave Roussy Institute – Villejuif – France).
The Atlas of Genetics and Cytogenetics in Oncology and Haematology (ISSN 1768-3262) is published 12 times a year by ARMGHM, a non profit organisation, and by the INstitute for Scientific and Technical Information of the French National Center for Scientific Research (INIST-CNRS) since 2008. The Atlas is hosted by INIST-CNRS (http://www.inist.fr)
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Editor
Jean-Loup Huret (Poitiers, France)
Editorial Board Sreeparna Banerjee (Ankara, Turkey) Solid Tumours Section Alessandro Beghini (Milan, Italy) Genes Section Anne von Bergh (Rotterdam, The Netherlands) Genes / Leukaemia Sections Judith Bovée (Leiden, The Netherlands) Solid Tumours Section Vasantha Brito-Babapulle (London, UK) Leukaemia Section Charles Buys (Groningen, The Netherlands) Deep Insights Section Anne Marie Capodano (Marseille, France) Solid Tumours Section Fei Chen (Morgantown, West Virginia) Genes / Deep Insights Sections Antonio Cuneo (Ferrara, Italy) Leukaemia Section Paola Dal Cin (Boston, Massachussetts) Genes / Solid Tumours Section Louis Dallaire (Montreal, Canada) Education Section Brigitte Debuire (Villejuif, France) Deep Insights Section François Desangles (Paris, France) Leukaemia / Solid Tumours Sections Enric Domingo-Villanueva (London, UK) Solid Tumours Section Ayse Erson (Ankara, Turkey) Solid Tumours Section Richard Gatti (Los Angeles, California) Cancer-Prone Diseases / Deep Insights Sections Ad Geurts van Kessel (Nijmegen, The Netherlands) Cancer-Prone Diseases Section Oskar Haas (Vienna, Austria) Genes / Leukaemia Sections Anne Hagemeijer (Leuven, Belgium) Deep Insights Section Nyla Heerema (Colombus, Ohio) Leukaemia Section Jim Heighway (Liverpool, UK) Genes / Deep Insights Sections Sakari Knuutila (Helsinki, Finland) Deep Insights Section Lidia Larizza (Milano, Italy) Solid Tumours Section Lisa Lee-Jones (Newcastle, UK) Solid Tumours Section Edmond Ma (Hong Kong, China) Leukaemia Section Roderick McLeod (Braunschweig, Germany) Deep Insights / Education Sections Cristina Mecucci (Perugia, Italy) Genes / Leukaemia Sections Yasmin Mehraein (Homburg, Germany) Cancer-Prone Diseases Section Fredrik Mertens (Lund, Sweden) Solid Tumours Section Konstantin Miller (Hannover, Germany) Education Section Felix Mitelman (Lund, Sweden) Deep Insights Section Hossain Mossafa (Cergy Pontoise, France) Leukaemia Section Stefan Nagel (Braunschweig, Germany) Deep Insights / Education Sections Florence Pedeutour (Nice, France) Genes / Solid Tumours Sections Elizabeth Petty (Ann Harbor, Michigan) Deep Insights Section Susana Raimondi (Memphis, Tennesse) Genes / Leukaemia Section Mariano Rocchi (Bari, Italy) Genes Section Alain Sarasin (Villejuif, France) Cancer-Prone Diseases Section Albert Schinzel (Schwerzenbach, Switzerland) Education Section Clelia Storlazzi (Bari, Italy) Genes Section Sabine Strehl (Vienna, Austria) Genes / Leukaemia Sections Nancy Uhrhammer (Clermont Ferrand, France) Genes / Cancer-Prone Diseases Sections Dan Van Dyke (Rochester, Minnesota) Education Section Roberta Vanni (Montserrato, Italy) Solid Tumours Section Franck Viguié (Paris, France) Leukaemia Section José Luis Vizmanos (Pamplona, Spain) Leukaemia Section Thomas Wan (Hong Kong, China) Genes / Leukaemia Sections

Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Volume 13, Number 5, May 2009
Table of contents
Gene Section
DENR (density-regulated protein) 336 Line S Reinert, Ronald B Gartenhaus
FBXO31 (F-box protein 31) 338 Anthony J Bais
FOXP3 (forkhead box P3) 343 Yang Liu, Lizhong Wang
FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) 348 Deborah A Altomare, Joseph R Testa
GPA33 (glycoprotein A33 (transmembrane)) 354 Tania Tabone, Joan K Heath
KLK5 (Kallikrein-related peptidase 5) 357 George M Yousef, Eleftherios P Diamandis
MIR10B (microRNA 10b) 360 Begum Akman, Ayse Elif Erson
RSPO1 (R-spondin homolog (Xenopus laevis)) 364 Diana Blaydon
UBE2C (ubiquitin-conjugating enzyme E2C) 367 Pierlorenzo Pallante, Maria Teresa Berlingieri, Alfredo Fusco
WNT5A (wingless-type MMTV integration site family, member 5A) 371 Masaru Katoh
Leukaemia Section
Nasal T cell lymphoma 374 Antonio Cuneo, Francesco Cavazzini, Gian Matteo Rigolin
t(14;14)(q11;q32) CEBPE/IGH, inv(14)(q11q32) CEBPE/IGH 376 Jean-Loup Huret
t(14;19)(q32;q13) IGH/CEBPA 378 Jean-Loup Huret
t(2;4)(p22;q12) 381 Jean-Loup Huret
t(5;14)(q35;q32.2) 383 Stefan Nagel, Roderick AF MacLeod
t(8;14)(q11;q32) 388 Jean-Loup Huret

Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Solid Tumour Section
Liver tumors: an overview 391 Munechika Enjoji
Cancer Prone Disease Section
McCune Albright syndrome 395 Margaret Zacharin
Case Report Section
Dic(1;15)(p11;p11) as a non-random abnormality in essential thrombocytemia 399 Olivier Theisen, Steven Richebourg, Jean-Luc Lai, Catherine Roche-Lestienne
Dic(1;15)(p11;p11) as a non-random abnormality in Myelodysplasic syndrome 401 Olivier Theisen, Steven Richebourg, Jean-Luc Lai, Catherine Roche-Lestienne

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 336
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
DENR (density-regulated protein) Line S Reinert, Ronald B Gartenhaus
University of Maryland Greenebaum Cancer Center, 9-011 BRB, 655 West Baltimore Street, Baltimore, MD 21201, USA (LSR, RBG)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/DENRID40295ch12q24.html DOI: 10.4267/2042/44465
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: DRP; DRP1; SMAP-3
HGNC (Hugo): DENR
Location: 12q24.31
DNA/RNA Description The gene encompasses 18583 bp DNA and contains 8 exons (e.g. NCBI: NC_000012).
Transcription 2766 bp mRNA. The 3'-untranslated region (3' UTR) of DENR was found to have a high number of uracyl (U)- and adenine (A)-rich sequences (AREs) (Mazan-Mamczarz and Gartenhaus, 2007).
Protein Description Size: 198 amino acids; 22092 Da.
Expression DENR is expressed in variety of tissues, with the highest quantity in skeletal and cardiac muscle. The protein level of DENR is up regulated in parallel with increasing cell density (Deyo et al., 1998). Very recently, it was found that this up regulation is controlled by the AUF-1 protein which binds to the 3'UTR of DENR mRNA and in a cell density-dependent manner (Mazan-Mamczarz and Gartenhaus, 2007). Furthermore, Oh JJ. et al. showed that DENR expression is increased in association with HER-2 overexpression in ovarian and breast cancers (Oh et al., 1999).
Localisation Predominantly in the cytoplasm of 3T3 cells.
Function Until recently there was little published data regarding DENR function. Reinert et al. showed that the oncogene MCT-1 interacts with DENR in vivo and in vitro. DENR contains a SUI1 domain which is also found in translation initiation factor eIF1, where the SUI1 domain is involved in recognition of the translation initiation codon (Yoon and Donahue, 1992). Interestingly, DENR together with MCT-1 sediment in the translation initiation complex fraction in both human embryonic kidney cell cultures and lymphoid cell lines. This complex was shown to interact with the cap complex and to alter the mRNA translational profile of a subset of cancer-related mRNAs. This supports a model where MCT-1 exerts it ongogenic function, at least in part by recruiting the SUI1 domain containing DENR to the translation initiation complex, thereby modulating the translational profile (Reinert et al., 2006).
Homology The SUI1 domain present in DENR is homologous to the SUI-1 domain found in eIF1. The SUI1 domain contains a secondary structure fold corresponding to that found in a number of ribosomal proteins and RNA-binding domains.
Implicated in Lymphoma oncogene Note The MCT-1 oncogene protein modifies mRNA translational profiles through its interaction with DENR which contains an SUI1 domain involved in

DENR (density-regulated protein) Reinert LS, Gartenhaus RB
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 337
recognition of the translation initiation codon (Yoon and Donahue, 1992; Reinert et.al., 2006).
Ovarian cancer and Breast cancer Disease DENR expression is increased in association with HER-2 overexpression in ovarian and breast cancers (Oh. et al., 1999).
References Yoon HJ, Donahue TF. The suil suppressor locus in Saccharomyces cerevisiae encodes a translation factor that functions during tRNA(iMet) recognition of the start codon. Mol Cell Biol. 1992 Jan;12(1):248-60
Deyo JE, Chiao PJ, Tainsky MA. drp, a novel protein expressed at high cell density but not during growth arrest. DNA Cell Biol. 1998 May;17(5):437-47
Oh JJ, Grosshans DR, Wong SG, Slamon DJ. Identification of differentially expressed genes associated with HER-2/neu overexpression in human breast cancer cells. Nucleic Acids Res. 1999 Oct 15;27(20):4008-17
Reinert LS, Shi B, Nandi S, Mazan-Mamczarz K, Vitolo M, Bachman KE, He H, Gartenhaus RB. MCT-1 protein interacts with the cap complex and modulates messenger RNA translational profiles. Cancer Res. 2006 Sep 15;66(18):8994-9001
Mazan-Mamczarz K, Gartenhaus RB. Post-transcriptional control of the MCT-1-associated protein DENR/DRP by RNA-binding protein AUF1. Cancer Genomics Proteomics. 2007 May-Jun;4(3):233-9
This article should be referenced as such:
Reinert LS, Gartenhaus RB. DENR (density-regulated protein). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):336-337.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 338
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
FBXO31 (F-box protein 31) Anthony J Bais
Immunogene Therapy Surgical Research Division, Boston University School of Medicine, Roger Williams Medical Center, 825 Chalkstone Avenue, Providence, RI 02908, USA (AJB)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/FBXO31ID44280ch16q24.html DOI: 10.4267/2042/44466
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: FBX14; Fbx31; FBX31; FBXO14; DKFZP434B027; DKFZp434J1815; FLJ22477; MGC15419; MGC9527; pp2386
HGNC (Hugo): FBXO31
Location 16q24.2
Local order: Telomere; centromeric to JPH3 and telomeric to FOXL1.
DNA/RNA Description FBXO31 encodes one mRNA transcript, published analyses have not reordered alternative five prime transcript or start sequences. FBXO31 is 3,635-bp in length, composed of 9 exons (1 to 9) spanning approximately 55-kb of genomic DNA, and has an ORF of 1,620-bp encoding a protein of 539 amino acids with a predicted mass of 61-kDa. Alternative five prime transcripts may exist. Homologous mouse cDNA sequences extending further five prime have been used for RT-PCR to identify putative translation start sites and established that alternatively spliced five prime exons result in short and long isoforms. The short isoform is 3,635-bp in length (i.e. approximately with poly A), and is the predicted primary transcript. The long isoform is 3,725-bp in length, contains an additional five prime exon of 87-bp and has an ORF of 1,707-bp encoding a protein of 568 amino acids. An additional smaller isoform of 3,099-bp with an ORF of 1,104-bp and 367 amino acids was predicted in GenBank. FBXO31 contains a moderate density C + G rich region (66% G + G with 9% CpG) spanning approximately
2.48-kb located within and five prime to the 350-bp exon 1. The FBXO31 transcript has and an uncharacteristically short 23-bp five prime untranslated region.
Pseudogene None identified.
Protein Description FBXO31 contains no significant homology to other known proteins apart from a characteristic 40 amino acid F-box domain at the COOH-terminal end. The F-box motif first described in cyclin F consists of approximately 50 amino acids that define an expanding family of eukaryotic proteins. There are currently three subdivisions of the F-box protein family based on the type of carboxy terminal motifs present in the protein sequences. Following proposed patterns the nomenclature adopted by HUGO denotes F-boxes that contain LRRs as FBXL, those containing WD repeats as FBXW, and those lacking all known protein-interaction domains as FBXO. FBXO31 forms part of the FBXO class of F-box proteins. Comparison of FBXO31 with the F-box domain of functionally demonstrated F-box proteins (i.e. Fbx1, Fbx2, Fbw1a, Fbw1b and Fbl1) indicates that FBXO31 matches the F-box consensus more closely than recognized F-box proteins from each of the three classes. Most F-box proteins notated as FBXO do not have recognizable substrate binding domains. In one instance Fbx7 has been shown to contain a proline-rich region that functions with SCF complexes in regulating Cdk1 - cyclin B - phosphorylated hepatoma up-regulated protein (HURP) proteolysis. This proline-rich region has been found in other FBXO proteins.

FBXO31 (F-box protein 31) Bais AJ
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 339
The COOH-terminal end of FBXO31 contains a 175-aa glycine and arginine rich region with possible similar function. FBXO31 contains six minimal D-box (RxxL) motifs. Proteins with RxxL motifs are often degraded via the APC/C (Cdh1) ubiquitin ligase.
Expression FBXO31 is widely expressed as a 3.6-kb transcript at similar levels in breast, testis, ovary, liver, uterus, prostate, colon, stomach, bladder, spinal cord, pancreas, trachea, kidney and thyroid. High expression is found in brain and low expression in bone marrow. FBXO31 is represented by the unigene cluster Hs.567582. cDNA clones from Hs.567582 express in the adrenal gland, blood, colon, germ cells, heart, kidney, liver, lung, muscle, placenta, synovial membrane, tonsil, cervix, lymph tissue, skin, mammary gland, testis, ovary, uterus, prostate, stomach, bladder, spinal cord, pancreas, thyroid and brain.
Localisation Co-immunoprecipitation experiments indicate that the carboxy terminal domain of FBXO31 associates with the Skp1, Roc-1 and Cullin-1 proteins. Immuno-localization studies demonstrate that ectopic expression of FBXO31 causes a change of Skp1 localization from the nucleus to the cytoplasm. The Skp1 protein returns to a nuclear localization when co-expressed with a FBXO31 protein with a deleted F-box domain.
Function FBXO31 is associated with the Skp1, Roc-1 and Cullin-1 proteins through its substrate F-box recognition domain and forms part of an SCF ubiquitination complex. The ubiquitin-dependant proteasome degradation pathway regulates protein abundance and the function of oncogenes, tumor suppressors, transcription factors and other signaling molecules. Ubiquitination begins with the addition of ubiquitin moieties to target proteins and follows a multi-step process, the end point being proteolysis of polyubiquitinated substrates by a 26S multi-protein complex. Ubiquitination of substrates targeted for degradation requires 3 classes of enzymes; the ubiquitin-activating enzymes (E1), the ubiquitin conjugating enzymes (E2) and the ubiquitin ligases (E3). E3 proteins participate in cell cycle progression. SCF complexes (a class of E3 ligases) regulate the G1-S phase transition. A wide variety of SCF targets include G1 phase cyclins, cyclin-dependant kinase inhibitors, DNA replication factors and transcription factors that promote cell cycle progression. F-box containing proteins act as substrate recognition components of the SCF ubiquitin-ligase complexes in the ubiquitin-dependant proteasome degradation pathway. These complexes contain four components; Skp1, Cullin, Rbx-Rocl-Hrtl and an F-box protein. The F-box motif tethers the F-box protein to other
components of the SCF complex by binding the core SCF component Skp1. This motif is generally found in the amino half of the proteins and is often coupled with other protein domains in the variable carboxy terminus of the protein. The most common carboxy terminal domains include leucine-rich repeats (LRRs) and WD-40 domains. Regions rich in glycine and arginine have also been implicated as protein binding domains, although such domains contain a more definitive repeat region than present in FBXO31. F-box SCF ubiquitin ligase complexes are involved in proteolysis pathways critical to diverse cellular functions including muscle atrophy, DNA metabolism, ER-associated degradation, desmin-related myopathy, signal transduction, control of G1-S progression and orderly execution of cell cycle. Skp1, Cul1 and Rbx1 are invariant proteins of the SCF complex while the F-box proteins that bind to Skp1 are the components that impart functional specificity. For instance Skp2 specifically binds phosphorylated p27 resulting in its degradation and control of S phase entry in the cell cycle.
Homology F-box domain containing no other significant homology.
Mutations Note None recorded.
Implicated in Neurodegenerative disorders and cancer Note Aberrant ubiquitin-dependant proteasome degradation in neurodegenerative disorders and cancer. Precedence for disruption in neurodegenerative disorders. The Parkin gene functions as an E3 ubiquitin ligase often mutated in inherited forms of Parkinson's disease. In Alzheimer's disease defective ubiquitination of cerebral proteins has been identified. The Von Hippel-Lindau (VHL) tumor suppressor protein is part of a complex that functions as a ubiquitin-protein ligase E3. VHL associates the ligase complex to target proteins such as HIF1aand VDU1 (VHL interacting deubiquitinating enzyme 1). HIF-a has been shown to regulate genes involved in tumor angiogenesis; VDU1 has deubiquitinating activity. Aberrant ubiquitin-dependant proteasome degradation of SCF-FBXO31 complexes has been proposed as a mechanism for tumor progression. FBXO31 would function as a tumor suppressor by mediating generation of SCF-FBXO31 complexes that compete and balance levels of other SCF complexes normally targeted to degradation proteins required to maintain cell

FBXO31 (F-box protein 31) Bais AJ
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 342
proliferation. An example is SCF complexes resulting in SCF-Skp2 E3 ligases that mediate ubiquitination and subsequent degradation of the CDK-inhibitor p27. Ectopic expression of FBXO31 would lower SCF-Skp2 complexes resulting in increased p27 and inhibition of transition from G1-S phase. This model corroborates with studies showing that high levels of Skp2 were associated with reduced levels of p27 in several cancers.
Abnormal protein None recorded.
Breast cancer, Prostate cancer, and several other cancers Note Loss of heterozygosity (LOH) of 16q22-qter in breast cancer, prostate cancer, and several other cancers. This region is frequently deleted in several human cancers causing loss of heterozygosity. The 16q24.3 region including FBXO31 spans approximately 3-Mb from the marker D16S498 to the telomere and contains at least two smallest regions of overlap (SROs). These SROs are most frequently deleted in early and late stage breast cancer and in prostate cancer. Loss of normal function of FBXO31 may be a key event in the early stage of breast cancer. LOH on the whole 16q22-qter region is frequently detected in breast and prostate cancer. Micro-cell mediated transfer experiments with 16q22-qter fragments (the 360-kb YAC clone 792E1 at D16S476 and D16S498 and the 85-kb BAC clone 346J21 at D16S3048 and D16S3063) have been shown to induce senescence in human and rat breast tumor cell lines. FBXO31 encompasses the 792E1 clone and a partial region of 346J21, has been shown to induce senescence in the breast cancer cell line MCF-7 and is regarded as the cellular senescence gene. FBXO31 is a potential tumor suppressor shown to be down-regulated in breast cancer cell lines relative to normal breast expression and cause G1 phase cell cycle arrest of the MDA-MB-468 cell line. Quantitative gene expression analysis of 78 genes in the 16q24.3 region demonstrated that FBXO31 was one of two genes including CYBA with a moderately aberrant expression profile. Expression of FBXO31 was reduced 100 to 200-fold in MDA-MB-134 and SK-BR-3 and moderately reduced in the other cell lines. 68 other genes displayed normal expression, one displayed significantly aberrant expression (CBFA2T3), six displayed mildly aberrant expression (DPEP1, CDH15, Hs.17074, Hs.189419, SLC7A5 and AA994450), and one gene displayed excessively reduced expression (CA5A). From microarray analysis FBXO31 was one of the 70-gene classifiers down-regulated in association with tumors of a favorable prognosis. The prognostic association between down-regulated FBXO31 and breast tumors corroborates with other studies demonstrating that LOH of chromosome 16q is associated with tumors of favorable prognosis.
Disease 16q22-qter LOH is detected in bilateral breast cancer and ductal lavage, in rare inflammatory breast cancer, and in several other cancers, including central nervous system neuroectodermal ependymoma and primary ependymomas, colorectal liver metastases, gastric tumor cancer, head and neck squamous cell carcinoma, hepatocellular carcinoma, lung tumor, nasopharyngeal tumor, ovarian tumor, rhabdomyosarcoma, and Wilms' tumor. 16q22-qter LOH in ovarian, hepatocellular and particularly breast and prostate cancers, exhibit similar SROs, suggesting common molecular pathways are affected.
References Carter BS, Ewing CM, Ward WS, Treiger BF, Aalders TW, Schalken JA, Epstein JI, Isaacs WB. Allelic loss of chromosomes 16q and 10q in human prostate cancer. Proc Natl Acad Sci U S A. 1990 Nov;87(22):8751-5
Carter BS, Ewing CM, Ward WS, Treiger BF, Aalders TW, Schalken JA, Epstein JI, Isaacs WB. Allelic loss of chromosomes 16q and 10q in human prostate cancer. Proc Natl Acad Sci U S A. 1990 Nov;87(22):8751-5
Tsuda H, Zhang WD, Shimosato Y, Yokota J, Terada M, Sugimura T, Miyamura T, Hirohashi S. Allele loss on chromosome 16 associated with progression of human hepatocellular carcinoma. Proc Natl Acad Sci U S A. 1990 Sep;87(17):6791-4
Zhang WD, Hirohashi S, Tsuda H, Shimosato Y, Yokota J, Terada M, Sugimura T. Frequent loss of heterozygosity on chromosomes 16 and 4 in human hepatocellular carcinoma. Jpn J Cancer Res. 1990 Feb;81(2):108-11
Sato T, Akiyama F, Sakamoto G, Kasumi F, Nakamura Y. Accumulation of genetic alterations and progression of primary breast cancer. Cancer Res. 1991 Nov 1;51(21):5794-9
Thomas GA, Raffel C. Loss of heterozygosity on 6q, 16q, and 17p in human central nervous system primitive neuroectodermal tumors. Cancer Res. 1991 Jan 15;51(2):639-43
Maw MA, Grundy PE, Millow LJ, Eccles MR, Dunn RS, Smith PJ, Feinberg AP, Law DJ, Paterson MC, Telzerow PE. A third Wilms' tumor locus on chromosome 16q. Cancer Res. 1992 Jun 1;52(11):3094-8
Sakai K, Nagahara H, Abe K, Obata H. Loss of heterozygosity on chromosome 16 in hepatocellular carcinoma. J Gastroenterol Hepatol. 1992 May-Jun;7(3):288-92
Bai C, Sen P, Hofmann K, Ma L, Goebl M, Harper JW, Elledge SJ. SKP1 connects cell cycle regulators to the ubiquitin proteolysis machinery through a novel motif, the F-box. Cell. 1996 Jul 26;86(2):263-74
Hochstrasser M. Ubiquitin-dependent protein degradation. Annu Rev Genet. 1996;30:405-39
Suzuki H, Komiya A, Emi M, Kuramochi H, Shiraishi T, Yatani R, Shimazaki J. Three distinct commonly deleted regions of chromosome arm 16q in human primary and metastatic prostate cancers. Genes Chromosomes Cancer. 1996 Dec;17(4):225-33
Godfrey TE, Cher ML, Chhabra V, Jensen RH. Allelic imbalance mapping of chromosome 16 shows two regions of common deletion in prostate adenocarcinoma. Cancer Genet Cytogenet. 1997 Oct 1;98(1):36-42

FBXO31 (F-box protein 31) Bais AJ
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 341
Haas AL, Siepmann TJ. Pathways of ubiquitin conjugation. FASEB J. 1997 Dec;11(14):1257-68
Latil A, Cussenot O, Fournier G, Driouch K, Lidereau R. Loss of heterozygosity at chromosome 16q in prostate adenocarcinoma: identification of three independent regions. Cancer Res. 1997 Mar 15;57(6):1058-62
Visser M, Sijmons C, Bras J, Arceci RJ, Godfried M, Valentijn LJ, Voûte PA, Baas F. Allelotype of pediatric rhabdomyosarcoma. Oncogene. 1997 Sep;15(11):1309-14
Baumeister W, Walz J, Zühl F, Seemüller E. The proteasome: paradigm of a self-compartmentalizing protease. Cell. 1998 Feb 6;92(3):367-80
Chou YH, Chung KC, Jeng LB, Chen TC, Liaw YF. Frequent allelic loss on chromosomes 4q and 16q associated with human hepatocellular carcinoma in Taiwan. Cancer Lett. 1998 Jan 16;123(1):1-6
Hershko A, Ciechanover A. The ubiquitin system. Annu Rev Biochem. 1998;67:425-79
Peters JM. SCF and APC: the Yin and Yang of cell cycle regulated proteolysis. Curr Opin Cell Biol. 1998 Dec;10(6):759-68
Sato M, Mori Y, Sakurada A, Fukushige S, Ishikawa Y, Tsuchiya E, Saito Y, Nukiwa T, Fujimura S, Horii A. Identification of a 910-kb region of common allelic loss in chromosome bands 16q24.1-q24.2 in human lung cancer. Genes Chromosomes Cancer. 1998 May;22(1):1-8
Spataro V, Norbury C, Harris AL. The ubiquitin-proteasome pathway in cancer. Br J Cancer. 1998;77(3):448-55
Adeyinka A, Mertens F, Idvall I, Bondeson L, Pandis N. Multiple polysomies in breast carcinomas: preferential gain of chromosomes 1, 5, 6, 7, 12, 16, 17, 18, and 19. Cancer Genet Cytogenet. 1999 Jun;111(2):144-8
Carrano AC, Eytan E, Hershko A, Pagano M. SKP2 is required for ubiquitin-mediated degradation of the CDK inhibitor p27. Nat Cell Biol. 1999 Aug;1(4):193-9
Cenciarelli C, Chiaur DS, Guardavaccaro D, Parks W, Vidal M, Pagano M. Identification of a family of human F-box proteins. Curr Biol. 1999 Oct 21;9(20):1177-9
Iwai K, Yamanaka K, Kamura T, Minato N, Conaway RC, Conaway JW, Klausner RD, Pause A. Identification of the von Hippel-lindau tumor-suppressor protein as part of an active E3 ubiquitin ligase complex. Proc Natl Acad Sci U S A. 1999 Oct 26;96(22):12436-41
Mori Y, Matsunaga M, Abe T, Fukushige S, Miura K, Sunamura M, Shiiba K, Sato M, Nukiwa T, Horii A. Chromosome band 16q24 is frequently deleted in human gastric cancer. Br J Cancer. 1999 May;80(3-4):556-62
Reddy DE, Sandhu AK, DeRiel JK, Athwal RS, Kaur GP. Identification of a gene at 16q24.3 that restores cellular senescence in immortal mammary tumor cells. Oncogene. 1999 Sep 9;18(36):5100-017
Wang X, Gleich L, Pavelic ZP, Li YQ, Gale N, Hunt S, Gluckman JL, Stambrook PJ. Cervical metastases of head and neck squamous cell carcinoma correlate with loss of heterozygosity on chromosome 16q. Int J Oncol. 1999 Mar;14(3):557-61
Winston JT, Koepp DM, Zhu C, Elledge SJ, Harper JW. A family of mammalian F-box proteins. Curr Biol. 1999 Oct 21;9(20):1180-2
Cockman ME, Masson N, Mole DR, Jaakkola P, Chang GW, Clifford SC, Maher ER, Pugh CW, Ratcliffe PJ, Maxwell PH. Hypoxia inducible factor-alpha binding and ubiquitylation by the
von Hippel-Lindau tumor suppressor protein. J Biol Chem. 2000 Aug 18;275(33):25733-41
Friesen WJ, Dreyfuss G. Specific sequences of the Sm and Sm-like (Lsm) proteins mediate their interaction with the spinal muscular atrophy disease gene product (SMN). J Biol Chem. 2000 Aug 25;275(34):26370-5
Gramantieri L, Trerè D, Pession A, Piscaglia F, Masi L, Gaiani S, Mazziotti A, Bolondi L. Allelic imbalance on 16q in small, unifocal hepatocellular carcinoma: correlation with HBV and HCV infections and cellular proliferation rate. Dig Dis Sci. 2000 Feb;45(2):306-11
Kipreos ET, Pagano M. The F-box protein family. Genome Biol. 2000;1(5):REVIEWS3002
Launonen V, Mannermaa A, Stenbäck F, Kosma VM, Puistola U, Huusko P, Anttila M, Bloigu R, Saarikoski S, Kauppila A, Winqvist R. Loss of heterozygosity at chromosomes 3, 6, 8, 11, 16, and 17 in ovarian cancer: correlation to clinicopathological variables. Cancer Genet Cytogenet. 2000 Oct 1;122(1):49-54
López Salon M, Morelli L, Castaño EM, Soto EF, Pasquini JM. Defective ubiquitination of cerebral proteins in Alzheimer's disease. J Neurosci Res. 2000 Oct 15;62(2):302-10
Ohh M, Park CW, Ivan M, Hoffman MA, Kim TY, Huang LE, Pavletich N, Chau V, Kaelin WG. Ubiquitination of hypoxia-inducible factor requires direct binding to the beta-domain of the von Hippel-Lindau protein. Nat Cell Biol. 2000 Jul;2(7):423-7
Reddy DE, Keck CL, Popescu N, Athwal RS, Kaur GP. Identification of a YAC from 16q24 carrying a senescence gene for breast cancer cells. Oncogene. 2000 Jan 13;19(2):217-22
Semenza GL. HIF-1: using two hands to flip the angiogenic switch. Cancer Metastasis Rev. 2000;19(1-2):59-65
Shimura H, Hattori N, Kubo S, Mizuno Y, Asakawa S, Minoshima S, Shimizu N, Iwai K, Chiba T, Tanaka K, Suzuki T. Familial Parkinson disease gene product, parkin, is a ubiquitin-protein ligase. Nat Genet. 2000 Jul;25(3):302-5
Zheng PP, Pang JC, Hui AB, Ng HK. Comparative genomic hybridization detects losses of chromosomes 22 and 16 as the most common recurrent genetic alterations in primary ependymomas. Cancer Genet Cytogenet. 2000 Oct 1;122(1):18-25
Gomes MD, Lecker SH, Jagoe RT, Navon A, Goldberg AL. Atrogin-1, a muscle-specific F-box protein highly expressed during muscle atrophy. Proc Natl Acad Sci U S A. 2001 Dec 4;98(25):14440-5
Yakicier MC, Legoix P, Vaury C, Gressin L, Tubacher E, Capron F, Bayer J, Degott C, Balabaud C, Zucman-Rossi J. Identification of homozygous deletions at chromosome 16q23 in aflatoxin B1 exposed hepatocellular carcinoma. Oncogene. 2001 Aug 23;20(37):5232-8
Yan J, Fang Y, Liang Q, Huang Y, Zeng Y. Novel chromosomal alterations detected in primary nasopharyngeal carcinoma by comparative genomic hybridization. Chin Med J (Engl). 2001 Apr;114(4):418-21
Hansen LL, Jensen LL, Dimitrakakis C, Michalas S, Gilbert F, Barber HR, Overgaard J, Arzimanoglou II.. Allelic imbalance in selected chromosomal regions in ovarian cancer. Cancer Genet Cytogenet 2002 Nov;139:1-8.
Kim J, Kim JH, Lee SH, Kim DH, Kang HY, Bae SH, Pan ZQ, Seo YS. The novel human DNA helicase hFBH1 is an F-box protein. J Biol Chem. 2002 Jul 5;277(27):24530-7
Lerebours F, Bertheau P, Bieche I, Driouch K, De The H, Hacene K, Espie M, Marty M, Lidereau R. Evidence of

FBXO31 (F-box protein 31) Bais AJ
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 342
chromosome regions and gene involvement in inflammatory breast cancer. Int J Cancer. 2002 Dec 20;102(6):618-22
Powell JA, Gardner AE, Bais AJ, Hinze SJ, Baker E, Whitmore S, Crawford J, Kochetkova M, Spendlove HE, Doggett NA, Sutherland GR, Callen DF, Kremmidiotis G. Sequencing, transcript identification, and quantitative gene expression profiling in the breast cancer loss of heterozygosity region 16q24.3 reveal three potential tumor-suppressor genes. Genomics. 2002 Sep;80(3):303-10
Signoretti S, Di Marcotullio L, Richardson A, Ramaswamy S, Isaac B, Rue M, Monti F, Loda M, Pagano M. Oncogenic role of the ubiquitin ligase subunit Skp2 in human breast cancer. J Clin Invest. 2002 Sep;110(5):633-41
van 't Veer LJ, Dai H, van de Vijver MJ, He YD, Hart AA, Mao M, Peterse HL, van der Kooy K, Marton MJ, Witteveen AT, Schreiber GJ, Kerkhoven RM, Roberts C, Linsley PS, Bernards R, Friend SH. Gene expression profiling predicts clinical outcome of breast cancer. Nature. 2002 Jan 31;415(6871):530-6
Yoshida Y, Chiba T, Tokunaga F, Kawasaki H, Iwai K, Suzuki T, Ito Y, Matsuoka K, Yoshida M, Tanaka K, Tai T. E3 ubiquitin ligase that recognizes sugar chains. Nature. 2002 Jul 25;418(6896):438-42
Zur A, Brandeis M. Timing of APC/C substrate degradation is determined by fzy/fzr specificity of destruction boxes. EMBO J. 2002 Sep 2;21(17):4500-10
Bloom J, Pagano M. Deregulated degradation of the cdk inhibitor p27 and malignant transformation. Semin Cancer Biol. 2003 Feb;13(1):41-7
den Engelsman J, Keijsers V, de Jong WW, Boelens WC. The small heat-shock protein alpha B-crystallin promotes FBX4-dependent ubiquitination. J Biol Chem. 2003 Feb 14;278(7):4699-704
Diep CB, Parada LA, Teixeira MR, Eknaes M, Nesland JM, Johansson B, Lothe RA. Genetic profiling of colorectal cancer liver metastases by combined comparative genomic hybridization and G-banding analysis. Genes Chromosomes Cancer. 2003 Feb;36(2):189-97
Matsuyama H, Pan Y, Yoshihiro S, Kudren D, Naito K, Bergerheim US, Ekman P. Clinical significance of chromosome
8p, 10q, and 16q deletions in prostate cancer. Prostate. 2003 Feb 1;54(2):103-11
Reed SI. Ratchets and clocks: the cell cycle, ubiquitylation and protein turnover. Nat Rev Mol Cell Biol. 2003 Nov;4(11):855-64
Safford SD, Goyeau D, Freemerman AJ, Bentley R, Everett ML, Grundy PE, Skinner MA. Fine mapping of Wilms' tumors with 16q loss of heterozygosity localizes the putative tumor suppressor gene to a region of 6.7 megabases. Ann Surg Oncol. 2003 Mar;10(2):136-43
Alkarain A, Jordan R, Slingerland J. p27 deregulation in breast cancer: prognostic significance and implications for therapy. J Mammary Gland Biol Neoplasia. 2004 Jan;9(1):67-80
Bashir T, Dorrello NV, Amador V, Guardavaccaro D, Pagano M. Control of the SCF(Skp2-Cks1) ubiquitin ligase by the APC/C(Cdh1) ubiquitin ligase. Nature. 2004 Mar 11;428(6979):190-3
Hsu JM, Lee YC, Yu CT, Huang CY. Fbx7 functions in the SCF complex regulating Cdk1-cyclin B-phosphorylated hepatoma up-regulated protein (HURP) proteolysis by a proline-rich region. J Biol Chem. 2004 Jul 30;279(31):32592-602
Wang ZC, Lin M, Wei LJ, Li C, Miron A, Lodeiro G, Harris L, Ramaswamy S, Tanenbaum DM, Meyerson M, Iglehart JD, Richardson A. Loss of heterozygosity and its correlation with expression profiles in subclasses of invasive breast cancers. Cancer Res. 2004 Jan 1;64(1):64-71
Härkönen P, Kyllönen AP, Nordling S, Vihko P. Loss of heterozygosity in chromosomal region 16q24.3 associated with progression of prostate cancer. Prostate. 2005 Feb 15;62(3):267-74
Kaur GP, Reddy DE, Zimonjic DB, de Riel JK, Athwal RS. Functional identification of a BAC clone from 16q24 carrying a senescence gene SEN16 for breast cancer cells. Oncogene. 2005 Jan 6;24(1):47-54
Yonekura Y, Yamamoto D, Okugawa H, Tanaka K, Kamiyama Y. Loss of heterozygosity in ductal lavage for breast tumor and the contralateral breast. Oncol Rep. 2005 Apr;13(4):739-43
This article should be referenced as such:
Bais AJ. FBXO31 (F-box protein 31). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):338-342.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 343
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
FOXP3 (forkhead box P3) Yang Liu, Lizhong Wang
Division of Immunotherapy, Department of Surgery Co-leader of Cancer Immunology Program, UMCCC Program of Molecular Mechanism of Diseases University of Michigan BSRB 2059, 109 Zina Pitcher Place, Ann Arbor, MI 48109, USA (YL, LW)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/FOXP3ID44129chXp11.html DOI: 10.4267/2042/44467
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: AIID; DIETER; IPEX; JM2; MGC141961; MGC141963; PIDX; SCURFIN; XPID
HGNC (Hugo): FOXP3
Location: Xp11.23
Local order: Xp telomere 3'- FOXP3 -5' centromere.
The location and orientation of FOXP3 gene on X chromosome. The X-linked gene FOXP3 is a member of the forkhead-box/winged-helix transcription factor family. It was identified during position cloning of Scurfin, a gene responsible for X-linked autoimmune diseases in mice and humans (Chatila et al., 2000; Brunkow et al., 2001; Bennett et al., 2001; Wildin et al., 2001).
Note: ChrX 48994354-49008232 bps.
DNA/RNA Note Some Gene Database only showed 11 coding exons and the first exon is not contained.
Description 12 exons; the first exon, 5' part of exon 2 and 3' part of exon 12 are non-coding.
Transcription 1869 bps mRNA; transcribed in a centromeric to telomeric orientation. Alternative splicing: we have identified two isoforms in both normal breast and prostate cell lines and tissues, but thirteen isoforms were found in breast, prostate, and pancreas cell lines.
Pseudogene None.
Protein Note None.
Description The FOXP3 protein is 431-amino acid long and its molecular weight is 47.25 kilodaltons. It contains four potential functional domains including the repressor, ZF, LZ and fork-head (FKH) domains.

FOXP3 (forkhead box P3) Liu Y, Wang L
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 344
Figure a: Schematic diagram of the FOXP3 gene and protein. ZF: zinc finger domain, LZ: leucine zipper domain, and FKH fork-head domain. Figure b: Alternatively spliced transcript variants encoding different isoforms have been identified. The two isoforms 1 and 2 is shown in the deletion of exon 3 and exon 3 with 5' part of exon 4, respectively. Other splice variant lacking both exons 3 and 8 was also reported (Smith et al., 2006). The repressor domain is localized to the N-terminal region of FOXP3 and is required to repress NFAT-mediated transcriptional activity (Bettelli et al., 2005; Lopes et al., 2006; Wu et al., 2006). The mutant LZ domain impairs both dimerization and suppressive function of FoxP3 in T cells (Chae et al., 2006). The FKH domain is critical for both DNA binding and nuclear localization (Ziegler, 2006). The FKH domain is the most frequent target in immunodysregulation polyendocrinopathy enteropathy X-linked syndrome (IPEX) patients.
Expression FOXP3 locus is transcribed in the regulatory T cell. We used the Rag2 (-/-) and the Rag2 (-/-) mice with the Scurfy (sf) mutation (FoxP3 (sf/Y) or FoxP3 (sf/sf)) to evaluate FoxP3 expression outside of the lymphoid system. Immunohistochemistry and real-time PCR revealed FoxP3 expression in breast epithelial cells, lung respiratory epithelial cells, and prostate epithelial cells, although not in liver, heart, and intestine (Chen et al., 2008). Using mice with a green fluorescence protein open reading frame knocked into the 3' untranslated region of the FoxP3 locus, we showed that the locus is transcribed broadly in epithelial cells of multiple organs (Chen et al., 2008). In human, FOXP3 is expressed in normal human breast epithelial cells but is silenced in most human breast cancers (Zuo et al., 2007b).
Localisation Predominately nuclear. Function Foxp3 is a member of the forkhead/winged-helix family of transcriptional regulators and functions as the master regulator in the development and
function of regulatory T (Treg) cells (Fontenot et al., 2003; Hori et al., 2003; Khattri et al., 2003). Nevertheless, there is still a controversy as to whether defect Treg alone explains the lethal autoimmune diseases observed in the mutant mouse and man (Chang et al., 2005; Godfrey et al., 1991). Moreover, FOXP3 as the first X-linked tumor suppressor directly targets two critical oncogenes HER2/ErbB2 and SKP2 and represses their transcription activity to inhibit cell growth in breast cancer (Zuo et al., 2007a; Zuo et al., 2007b).
Homology FOXP1, FOXP2, and FOXP3 all have the FKH domain and may interact with cytokine gene transactivators NFkappaB and NFAT to regulate several cytokine gene transcription in T cells (Bettelli et al., 2005; Tone et al., 2008; Wu et al., 2006). However, their functional roles are alterative in different T cells.
Mutations Note The somatic mutations but not germline mutations in breast cancer patients.
Germinal In mice, a Foxp3 frameshift mutation in the forkhead domain results in lethality in hemizygous males 16 to 25 days after birth (Brunkow et al., 2001). The mutation in some human IPEX patients is analogous as they cause frameshift and early termination of translation (Chatila, 2000; Brunkow, 2001; Bennett, 2001; Wildin, 2001).
Somatic In breast cancer patients, a total of 27 somatic mutations in all 11 coding exons and intron-exon

FOXP3 (forkhead box P3) Liu Y, Wang L
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 345
Somatic mutation of the FOXP3 gene in breast cancer samples: summary of sequencing data from 65 cases, including 50 formalin-fixed samples and 15 frozen samples. Genomic DNA was isolated from matched normal and cancerous tissues from the same patients and amplified with primers for individual exons and intron-exon boundary regions. Somatic mutations were identified by comparing sequences from normal and cancerous samples from the same patients. The data are from either bulk sequencing of PCR products or from the sequencing of 5-10 clones from PCR products. Only those mutations that were observed in multiple clones were scored. Mutations identified from 50 cases of formalin-fixed samples are marked in black, while those identified from 15 cases of frozen tissue samples are marked in red.
boundary regions have been identified in 36% of 65 patients by PCR (Zuo et al., 2007b). In these mutations, there are 18 nonsynonymous mutations, 3 synonymous mutations and 6 mutations in the intron-exon junction 12 (Zuo et al. 2007b). Interestingly, the mutations are not randomly distributed in FOXP3 gene and the overwhelming majority of the mutations were either in the functional domains or within intron 11 which can affect the forkhead domain sequence (Zuo et al. 2007b).
Implicated in Breast cancer Note None.
Disease In majority of the mammary cancers, Foxp3 allele was inactivated and HER-2/ErbB2 and SKP2 are overexpressed and repressed the HER-2/ErbB2 and SKP2 promoters. Deletion, functionally significant somatic mutations, and down-regulation of the FOXP3 gene are commonly found in human breast cancer
samples and correlated significantly with HER-2/ErbB2 over-expression, regardless of the status of HER-2 amplification. FOXP3 is an X-linked breast cancer suppressor gene and an important regulator of the HER-2/ErbB2 and SKP2 oncogenes in breast cancer development.
Prognosis None
Cytogenetics In fluorescence in situ hybridization (FISH) analysis, the FOXP3 gene is frequently deleted in the breast cancer samples. Out of 223 informative samples, we observed 28 cases (12.6%) with FXOP3 deletion. FOXP3 is likely within the minimal region of deletion in the Xp11 region studied. Although all deletions were heterozygous, the FOXP3 protein was undetectable in 26 out of 28 cases. Thus, it appears that for the majority of the breast cancer samples, LOH alone was sufficient to inactivate the locus, perhaps due to X-chromosomal inactivation. The two cases with both deletion and FOXP3 expression had X polysomy with three and four X chromosomes, respectively.
X-chromosomal deletion pattern in breast cancer. TMA samples were probed with 3 markers for X-chromosome as marked. The deletion of each probe was scored independently and summarized in the colour bars, each bar representing one case. Note that the FOXP3 locus encompasses the minimal deletion in the 10MB area of the X-chromosome. A typical FISH for the CEPX (green) and FOXP3 (orange) probes is shown.

FOXP3 (forkhead box P3) Liu Y, Wang L
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 346
Hybrid/Mutated gene None.
Abnormal protein None
Oncogenesis Mice with the Foxp3 heterozygous mutation spontaneously developed mammary cancer at a high rate (Zuo et al., 2007b). Foxp3 mutation have a comparably higher incidence of human mammary cancer and is likely responsible for the increased rate of breast cancer. Our analysis of human breast cancer samples provides strong support for an important role for the FOXP3 gene in the development of breast cancer (Zuo et al., 2007a; Zuo et al., 2007b). First, FOXP3 is likely the minimal region of deletion in breast cancer. Second, a high proportion of somatic
mutations in the FOXP3 gene are identified in breast cancer and most of the mutations resulted in the non- conservative replacement of amino acids, and the deletions and mutations of the FOXP3 locus corresponded to increased HER-2 and SKP2 levels. Third, approximate 80% breast cancers have a down-regulation of FOXP3 in tumor tissues compared to normal breast tissues. These data indicated that FOXP3 is an X-Linked mammary tumor suppressor gene.
To be noted Note None.
Breakpoints Note None.
Ingenuity Pathway analysis indicated that FoxP3-regulated genes belong to multiple cellular pathways related to the process of cancer development. Most of which are not directly related to FOXP3-mediated repression of ErbB2 (Zuo et al., 2007b). Interestingly, when we used the GeneGo MetaCore knowledgebase to analyze genes that related to ErbB2 signaling pathway, we found that FOXP3 down-regulated 10 genes in this pathway. With the notable exception of b-Myb and c-Myb, the down-regulation is not likely related to FoxP3-mediated ErbB2 repression, as they are not known transcriptional targets of ErbB2. Thus, FOXP3 can suppress ErbB2 signaling and tumor growth by mechanisms other than ErbB2 expression. These data provide a plausible explanation for the tumor suppressor activity of FOXP3 in breast cancer cell lines that do not substantially overexpress HER-2. We also demonstrated that downregulation of SKP2 was critical for FOXP3-mediated growth inhibition in breast cancer cells that do not overexpress ERBB2/HER2 (Zuo et al., 2007a). Our data provide genetic, biochemical, and functional evidence that FOXP3 is a novel transcriptional repressor for the oncogenes HER2/ErbB2 and SKP2 (Zuo et al., 2007b; Zuo et al., 2007a).
References Godfrey VL, Wilkinson JE, Rinchik EM, Russell LB. Fatal lymphoreticular disease in the scurfy (sf) mouse requires T cells that mature in a sf thymic environment: potential model for thymic education. Proc Natl Acad Sci U S A. 1991 Jul 1;88(13):5528-32
Chatila TA, Blaeser F, Ho N, Lederman HM, Voulgaropoulos C, Helms C, Bowcock AM. JM2, encoding a fork head-related
protein, is mutated in X-linked autoimmunity-allergic disregulation syndrome. J Clin Invest. 2000 Dec;106(12):R75-81
Bennett CL, Christie J, Ramsdell F, Brunkow ME, Ferguson PJ, Whitesell L, Kelly TE, Saulsbury FT, Chance PF, Ochs HD. The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat Genet. 2001 Jan;27(1):20-1

FOXP3 (forkhead box P3) Liu Y, Wang L
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 347
Brunkow ME, Jeffery EW, Hjerrild KA, Paeper B, Clark LB, Yasayko SA, Wilkinson JE, Galas D, Ziegler SF, Ramsdell F. Disruption of a new forkhead/winged-helix protein, scurfin, results in the fatal lymphoproliferative disorder of the scurfy mouse. Nat Genet. 2001 Jan;27(1):68-73
Wildin RS, Ramsdell F, Peake J, Faravelli F, Casanova JL, Buist N, Levy-Lahad E, Mazzella M, Goulet O, Perroni L, Bricarelli FD, Byrne G, McEuen M, Proll S, Appleby M, Brunkow ME. X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy syndrome is the human equivalent of mouse scurfy. Nat Genet. 2001 Jan;27(1):18-20
Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat Immunol. 2003 Apr;4(4):330-6
Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the transcription factor Foxp3. Science. 2003 Feb 14;299(5609):1057-61
Khattri R, Cox T, Yasayko SA, Ramsdell F. An essential role for Scurfin in CD4+CD25+ T regulatory cells. Nat Immunol. 2003 Apr;4(4):337-42
Bettelli E, Dastrange M, Oukka M. Foxp3 interacts with nuclear factor of activated T cells and NF-kappa B to repress cytokine gene expression and effector functions of T helper cells. Proc Natl Acad Sci U S A. 2005 Apr 5;102(14):5138-43
Chang X, Gao JX, Jiang Q, Wen J, Seifers N, Su L, Godfrey VL, Zuo T, Zheng P, Liu Y. The Scurfy mutation of FoxP3 in the thymus stroma leads to defective thymopoiesis. J Exp Med. 2005 Oct 17;202(8):1141-51
Chae WJ, Henegariu O, Lee SK, Bothwell AL. The mutant leucine-zipper domain impairs both dimerization and suppressive function of Foxp3 in T cells. Proc Natl Acad Sci U S A. 2006 Jun 20;103(25):9631-6
Lopes JE, Torgerson TR, Schubert LA, Anover SD, Ocheltree EL, Ochs HD, Ziegler SF. Analysis of FOXP3 reveals multiple domains required for its function as a transcriptional repressor. J Immunol. 2006 Sep 1;177(5):3133-42
Smith EL, Finney HM, Nesbitt AM, Ramsdell F, Robinson MK. Splice variants of human FOXP3 are functional inhibitors of human CD4+ T-cell activation. Immunology. 2006 Oct;119(2):203-11
Wu Y, Borde M, Heissmeyer V, Feuerer M, Lapan AD, Stroud JC, Bates DL, Guo L, Han A, Ziegler SF, Mathis D, Benoist C, Chen L, Rao A. FOXP3 controls regulatory T cell function through cooperation with NFAT. Cell. 2006 Jul 28;126(2):375-87
Ziegler SF. FOXP3: of mice and men. Annu Rev Immunol. 2006;24:209-26
Zuo T, Liu R, Zhang H, Chang X, Liu Y, Wang L, Zheng P, Liu Y. FOXP3 is a novel transcriptional repressor for the breast cancer oncogene SKP2. J Clin Invest. 2007 Dec;117(12):3765-73
Zuo T, Wang L, Morrison C, Chang X, Zhang H, Li W, Liu Y, Wang Y, Liu X, Chan MW, Liu JQ, Love R, Liu CG, Godfrey V, Shen R, Huang TH, Yang T, Park BK, Wang CY, Zheng P, Liu Y. FOXP3 is an X-linked breast cancer suppressor gene and an important repressor of the HER-2/ErbB2 oncogene. Cell. 2007 Jun 29;129(7):1275-86
Chen GY, Chen C, Wang L, Chang X, Zheng P, Liu Y. Cutting edge: Broad expression of the FoxP3 locus in epithelial cells: a caution against early interpretation of fatal inflammatory diseases following in vivo depletion of FoxP3-expressing cells. J Immunol. 2008 Apr 15;180(8):5163-6
Tone Y, Furuuchi K, Kojima Y, Tykocinski ML, Greene MI, Tone M. Smad3 and NFAT cooperate to induce Foxp3 expression through its enhancer. Nat Immunol. 2008 Feb;9(2):194-202
This article should be referenced as such:
Liu Y, Wang L. FOXP3 (forkhead box P3). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):343-347.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 348
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Deborah A Altomare, Joseph R Testa
Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111, USA (DAA, JRT)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/FRAP1ID40639ch1p36.html DOI: 10.4267/2042/44468
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: FLJ44809; FRAP; FRAP2; MTOR; RAFT1; RAPT1; mTOR
HGNC (Hugo): MTOR
Location: 1p36.22
Note: EXOSC10 is exosome component 10, ANGPTL7 encodes angiopoietin-like 7, UBIAD1 is UbiA prenyltransferase domain containing 1, PTCHD2 is patched domain containing 2, LOC100128221 is similar to hCG2041787, and SRM encodes spermidine synthase.
DNA/RNA Note A map of the genomic organization of the human FRAP1 gene can be found at http://www.ncbi.nlm.nih.gov/projects/sviewer/?id=NC_000001.9v=11081381..11252951.
Description The FRAP1 gene encompasses approximatively 156 kb and contains 58 exons. The gene resides on the minus strand. Reported location on human chromosome 1 is between 11,089,179-11,245,151 bases in NCBI36 coordinates and 11,089,180-11,245,176 bases in ensemble49 coordinates.
Transcription Transcript length is 8,680 bp.
Pseudogene No human pseudogene known.
Protein Description The amino terminus of FRAP (alias, mTOR) consists of several tandem HEAT (Huntingtin, EF2, A subunit of PP2A, TOR1) repeats) that are implicated in protein-protein interations (Hay and Sonenberg, 2004; Bhaskar and Hay, 2007). Each HEAT repeat contains two alpha helices of approximatively 40 amino acids. The carboxy-terminal half contains two FAT (FRAP, ATM, TRAP) domains. Upstream of the catalytic domain is the FRB (FKBP12-rapamycin binding) domain. The catalytic domain has sequence similarity to the catalytic domain of phosphatidylinositol kinase (PIK), which is homologous to a family of other protein kinases termed PIKK (PIK-related kinase).

FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Altomare DA, Testa JR
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 349
The amino acid residues corresponding to the FRAP1 (alias mTOR) protein domains are reported in pfam (see below) Pfam: PF00454: Phosphatidylinositol 3- and 4-kinase (2181-2431) Pfam: PF02259: FAT domain (1513-1910) Pfam: PF02260: FATC domain (2517-2549) Pfam: PF08771: FKBP12 Rapamycin Binding domain (2015-2114) mTOR also contains a putative negative regulatory (NR) domain between the catalytic domain and FATC. The FATC (FRAP, ATM, TRRAP C-terminal) domain is essential for the kinase activity. The FATC and FAT domains are thought to interact in a way the exposes the catalytic domain. The protein consists of 2549 amino acids, with a predicted molecular weight of 288,891 Da. The ternary complex of human FK506-binding protein (FKBP12), the inhibitor rapamycin, and the FKBP12-rapamycin-binding (FRB) domain of human FRAP has been crystallized at a resolution of 2.7 angstroms (Choi et al., 1996), and then refined at 2.2 angstroms (Liang et al., 1999). Phosphorylation sites of FRAP (alias, mTOR) are reported in http://www.phosphosite.org .
Expression Expressed is found in numerous tissues, with high levels in testis.
Localisation Localization is predominantly cytoplasmic, but the protein is also associated with mitochondrial, endoplasmic reticulum and Golgi membranes (Guertin and Sabatini, 2007). A fraction of protein also may shuttle between the nucleus and cytoplasm.
Function There are more than 2500 articles specifically referring to FRAP1 or mTOR in PubMed. mTOR is central to several key cellular pathways including insulin signaling, regulation of eIF4e and p70S6 kinase, and hypoxia induced factor 1alpha (HIF1alpha) stimulation of vascular endothelial growth factor (VEGF). These pathways affect several processes including cell growth (size), protein translation, ribosome biogenesis, regulation of cell cycle progression, response to nutrients and cellular stress, angiogenesis, cell polarity and cytoskeletal reorganization. mTOR also has been shown to play a role in the regulation of autophagy (Pattingre et al., 2008), an adaptive cellular response to nutrient starvation whereby a cytoplasmic vacuole or autophagosome engulfs cellular macromolecules and organelles for degradation.
mTOR protein exists in two functionally distinct complexes named mTOR complex 1 (mTORC1) and complex 2 (mTORC2) (see figure under "Implicated in"). The regulator of mTORC1 signaling and kinase activity is the ras-like small GTPase Rheb (Ras homologue enriched in brain), which binds directly to the mTOR catalytic domain and enables mTORC1 to attain an active configuration (Avruch et al., 2006). Insulin/IGF stimulates the accumulation of Rheb-GTP through activated AKT and subsequent inhibition of the Rheb-GTPase-activating function of the tuberous sclerosis (TSC1/TSC2) heterodimer. Energy depletion decreases Rheb-GTP through the action of adenosine monophosphate-activated protein kinase (AMPK) to phosphorylate TSC2 and stimulate its Rheb-GTPase activating function and also HIFalpha-mediated transcriptional responses that act upstream of the TSC1/2 complex. Amino-acid depletion inhibits mTORC1 by acting predominantly downstream of the TSC complex, by interfering with the ability of Rheb to bind to mTOR. As shown below, mTORC1 contains the core components mTOR, Raptor (regulatory associated protein of mTOR), and mLST8/GbetaL (G protein beta-subunit-like protein). It is the mTORC1 complex that is characteristically sensitive to inhibition by rapamycin. mTORC1 is a major regulator of ribosomal biogenesis and protein synthesis, largely through the phosphorylation/inactivation of the 4E-BPs (4E-binding proteins) and the phosphorylation/activation of S6K (ribosomal S6 kinase). The binding of S6K1 and 4E-BP1 to raptor requires a TOR signaling (TOS) motif, which contains an essential phenylalanine followed by four alternating acidic and small hydrophobic amino acids (Schalm and Blenis, 2002). Recently, a TOS motif also has been identified in the N terminus of HIF1alpha, which has been shown to interact with Raptor (Land and Tee, 2007). Furthermore, activation of mTOR by Rheb overexpression enhanced HIF1alpha activity and VEGF-A secretion under hypoxic conditions, whereas the mTOR inhibitor rapamycin blocked the pathway. PRAS40 (proline-rich AKT substrate 40 kDa) is a novel mTOR binding partner that mediates AKT signals to mTOR independently of TSC1/TSC2 (Vander Haar et al., 2007). Hence, PRAS40 and Rheb are postulated to co-regulate mTORC1 (Guertin and Sabatini, 2007). PRAS40 binds mTORC1 via Raptor, and is an mTOR phosphorylation substrate (Thedieck et al., 2007). Moreover, PRAS40 binds the mTOR
FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Altomare DA, Testa JR
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 350
kinase domain and its interaction with mTOR is induced under conditions that inhibit mTOR signaling, such as nutrient or serum deprivation or mitochondrial metabolic inhibition (Vander Haar et al., 2007). PRAS40 contains a variant TOS motif and competes with S6K1 and 4E-BP1 by functioning as a direct inhibitor of substrate binding (Oshiro et al., 2007, Wang et al., 2007). mTORC2 contains mTOR, Rictor (rapamycin-insensitive companion of mTOR), SIN1 (SAPK interacting protein) and mLST8/GbetaL. Proline rich protein 5-like (PRR5) protein also binds specifically to mTORC2, via Rictor and/or SIN1 (Thedieck et al., 2007). mTORC2 has been shown to regulate cell-cycle-dependent polarization of the actin cytoskeleton. Although not as sensitive to rapamycin as mTOR1, mTORC2 may be affected by prolonged rapamycin exposure in some cell types (Sarbassov et al., 2006; Zeng et al., 2007). However, the regulation of mTORC2 is largely unknown and does not function downstream of Rheb (Blaskar and Hay, 2007). Direct genetic evidence for the importance of various components of the mTORC1 and/or mTORC2 complexes was provided by targeted disruption studies in mice (Guertin et al., 2006). Mice null for mTOR, as well as those lacking Raptor die early in embryonic development. However, mLST8-null embryos survive until e10.5 and resemble embryos missing Rictor. Collectively, mTORC1 function was found to be essential in early development, mLST8 was required only for mTORC2 signaling, and mTORC2 was found to be a necessary component of the AKT-FOXO and PKCalphaalpha pathways.
Homology Mouse (Mus musculus): Frap1, 99 % amino acid smilarity with Human FRAP1. Rat (Rattus norvegicus): Frap1, 99% amino acid similarity with Human FRAP1. Dog (Canis familiaris): FRAP1, 99% amino acid similarity with Human FRAP1. Worm (Caenorhabditis elegans): B0261.2b, 51% amino acid similarity with Human FRAP1. Fruit fly (Drosophila melanogaster): Tor, 64% amino acid similarity with Human FRAP1.
Mutations Note No mutations are reported to date.
Implicated in Various cancers and hamartoma syndromes Note Activation of mTOR signaling is associated with several hamartoma syndromes, as well as in cancer.
Disease Among the dominantly inherited disorders classified as phakomatoses are tuberous sclerosis 1 and 2, Peutz-Jeghers syndrome, Cowden disease, neurofibromatosis 1 and neurofibromatosis 2, and von-Hippel-Lindau disease (Tucker et al., 2000). These disorders are characterized by scattered hamartomatous or adenomatous "two-hit" lesions that have a low probability of becoming malignant. These particular disorders are caused by germline mutations of certain tumor suppressor genes, i.e., TSC2 / TSC1, LKB1, PTEN, NF1/NF2 and VHL, respectively, encoding proteins that intersect with the AKT/mTOR signaling pathway (Altomare and Testa, 2005). Germline mutations of TSC1 and TSC2 each give rise to the hereditary disorder known as tuberous sclerosis complex (TSC) (Astrinidis and Henske, 2005; Jozwiak et al., 2008). Hamartomas arise in the central nervous system, kidney, heart, lung, and skin, with occasional tumors progressing to malignancy (i.e., renal cell carcinoma). In TSC tumor cells, biallelic inactivation of TSC2 or TSC1 results in constitutive mTOR activity, independent of AKT activation status. Aside from TSC, another rare lung disease known as pulmonary lymphangioleiomyomatosis (LAM) occurs from somatic or genetic mutations of TSC1 or TSC2 that lead to the activation of downstream mTOR (Krymskaya, 2008). These findings have provided rationale for the first rapamycin clinical trial for LAM (Goncharova and Krymskaya, 2008). The LKB1 tumor suppressor/AMPK pathway is an alternate means of inactivating TSC2 and contributing to constitutive mTOR activation (Inoki et al., 2005; Kwiatkowski and Manning, 2005). The kinase controlling AMPK (AMP-activated protein kinase) has been identified as LKB1, which is encoded by the gene inactivated in Peutz-Jeghers syndrome, a disorder characterized by multiple gastrointestinal hamartomatous polyps. There is now experimental evidence that Peutz-Jeghers polyposis could be suppressed by targeting mTOR (Wei et al., 2008). Germline PTEN mutations occur in 80% of patients with Cowden disease, a heritable multiple hamartoma syndrome with a high risk of breast, thyroid and endometrial carcinomas (Gustafson, et al., 2007). Decreased or absent expression of PTEN results in constitutive activation of the AKT/mTOR pathway. Loss-of-function mutations in NF1 contributes to the neurofibromatosis type I familial cancer syndrome, which is characterized by benign neurofibromas and occasional malignant peripheral nerve sheath tumors (MPNSTs), as well as hamartomatous lesions of the eye, myeloid malignancies, gliomas, and pheochromocytomas. The NF1-encoded protein, neurofibromin, functions as a Ras-GAP, and deregulation of Ras due to NF1 inactivation is postulated to contribute to tumor development. Activated Ras signaling to PI3K results in activation of
FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Altomare DA, Testa JR
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 351
the AKT/mTOR pathway (Johannessen et al., 2005). The mTOR inhibitor rapamycin has been shown to suppress the growth of NF1-associated malignancies in a genetically modified mouse model (Johannessen et al., 2008). Like NF1, NF2 also can regulate AKT/mTOR signaling (Scoles, 2008); the NF2-encoded protein, merlin, does so by binding to PIKE (phosphatidylinositol 3-kinase enhancer). Germline inactivation of the von Hippel-Lindau tumor suppressor gene (VHL) causes hamartomatous tumors associated with the von-Hippel-Lindau syndrome. Moreover, most renal cell carcinomas have biallelic alterations in the von VHL gene, resulting in the accumulation of hypoxia-inducible factors 1 and 2 , and downstream targets including vascular endothelial growth factor (VEGF) (Cho et al., 2007). The observed clinical efficacy of mTOR inhibitors in patients with renal cell carcinoma may be mediated in part by the dependence of efficient hypoxia-inducible factor translation.
Hybrid/Mutated gene A schematic model of mTOR signaling depicts various environmental and molecular interactions that influence the pathway. mTOR protein exists in two functionally distinct complexes named mTORC1 and mTORC2. Components are described above, under the Protein Function section. The classical phosphorylation substrates of mTORC1 are S6 kinases and 4E-BP1, although HIF1alpha and PRAS40 also have been shown to have TOR signaling motifs. Because mTOR is shared by both mTORC1 and mTORC2, there may be equilibrium between the two complexes, as well as competition for mTOR (Bhuskar and Hay, 2007). Insulin and other growth factors activate mTORC1 via activation of phosphatidylinositol 3-OH kinase (PI3K) and downstream AKT. Constitutive activation of mTORC1 can occur in the absence of TSC1 or TSC2. Once mTORC1 is activated, it is able to elicit a negative feedback loop to inhibit AKT activity. In opposition, mTORC2 is an activator of AKT, which places this pathway under both positive and negative controls mediated by mTOR. In contrast to growth factor activation of mTORC1, responses to cellular stresses such as energy depletion and amino acid deprivation are mediated by TSC1/2 and/or Rheb (Hay and Sonenberg, 2004; Guertin and Sabatini, 2007). AMPK is activated by reduced intracellular ATP levels
and a concomitant increase in intracellular AMP. Under conditions of energy depletion, TSC2 is phosphorylated and activated by AMPK, thereby inhibiting mTORC1 activity. Amino acid starvation also elicits a decrease in mTORC1 activity through Rheb. Abundant evidence suggests that a deregulation between signaling components in the PI3K-AKT-TSC2-Rheb-mTORC1 pathway is a critical step in tumorigenesis. Tumor suppressor genes involved in predisposition to hamartomatous lesions are discussed above in the Implicated Diseases section.
Human malignant tumors Note Activation of mTOR signaling has been reported in several types of human malignant tumors. Clinical results have been reported for the mTOR inhibitors CCI-799 (Wyeth), RAD001 (Novartis) and AP23573 (Ariad Pharmaceuticals), all rapamycin analogs (Guertin and Sabatini, 2007). Therapeutic response is highly variable, suggesting that biomarkers still are needed for predicting response to rapamycin therapy. To date, some of the best clinical response rates to rapamycin have been observed in patients suffering from Kaposi's sarcoma or mantle-cell lymphoma. Patients with renal cell carcinomas exhibiting a nonclear cell histology also appear to benefit from treatment with mTOR inhibitors (Hanna et al., 2008). Patients with advanced sarcomas are yet another subset of individuals that have benefited from therapeutic mTOR inhibition (Wan and Helman, 2007).
Disease Collectively, there are a number of mechanisms that contribute to the deregulation of the AKT/mTOR pathway in human malignant tumors (Altomare and Testa, 2005; Wan and Helman, 2007). Phospho-AKT immunohistochemical staining is frequently associated with phospho-mTOR staining. mTOR has emerged as a validated therapeutic target in cancer (Abraham and Eng, 2008). Specific to mTOR, mTORC2 activity was found to be elevated in glioma cell lines and primary tumors as compared with normal brain tissue (Masri et al., 2007). Overexpression of Rictor increased mTORC2 activity, anchorage-independent growth in soft agar, S-phase cell cycle distribution, motility, and integrin expression, whereas knockdown of Rictor inhibited these events.

FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Altomare DA, Testa JR
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 352
Xenograft studies also supported a role for increased mTORC2 activity in tumorigenesis and enhanced tumor growth. PKCalpha activity was shown to be dependent of Rictor-expression, consistent with the known regulation of actin organization by mTORC2 via PKCalpha. Collectively, these data suggest that mTORC2 is hyperactivated in gliomas and promotes tumor cell proliferation and invasive potential due to increased complex formation in the presence of overexpressed Rictor.
Prognosis Recent data suggest that inhibition of mTOR results in clinical benefit in patients with poor prognostic features, and in preclinical models this therapeutic effect involves downregulation of HIF1alpha (Hanna et al., 2008).
Huntington disease Note mTOR has been implicated in Huntington disease, an inherited neurodegenerative disorder.
Disease Ravikumar et al. (2004) showed that mTOR is sequestered in polyglutamine aggregates in cell models, transgenic mice, and human brains. Sequestration of mTOR impaired its kinase activity and induced autophagy, a key mechanism for clearance of mutant huntingtin fragments to protect against polyglutamine toxicity. Rapamycin also attenuated huntingtin accumulation and cell death in cell models, and inhibited autophagy. Furthermore, rapamycin protected against neurodegeneration in a fly model, and the rapamycin analog CCI-779 decreased aggregate formation in a mouse model of Huntington disease.
References Choi J, Chen J, Schreiber SL, Clardy J. Structure of the FKBP12-rapamycin complex interacting with the binding domain of human FRAP. Science. 1996 Jul 12;273(5272):239-42
FRAP1 (FK506 binding protein 12-rapamycin associated protein 1) Altomare DA, Testa JR
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 353
Liang J, Choi J, Clardy J. Refined structure of the FKBP12-rapamycin-FRB ternary complex at 2.2 A resolution. Acta Crystallogr D Biol Crystallogr. 1999 Apr;55(Pt 4):736-44
Tucker M, Goldstein A, Dean M, Knudson A. National Cancer Institute Workshop Report: the phakomatoses revisited. J Natl Cancer Inst. 2000 Apr 5;92(7):530-3
Schalm SS, Blenis J. Identification of a conserved motif required for mTOR signaling. Curr Biol. 2002 Apr 16;12(8):632-9
Hay N, Sonenberg N. Upstream and downstream of mTOR. Genes Dev. 2004 Aug 15;18(16):1926-45
Ravikumar B, Vacher C, Berger Z, Davies JE, Luo S, Oroz LG, Scaravilli F, Easton DF, Duden R, O'Kane CJ, Rubinsztein DC. Inhibition of mTOR induces autophagy and reduces toxicity of polyglutamine expansions in fly and mouse models of Huntington disease. Nat Genet. 2004 Jun;36(6):585-95
Altomare DA, Testa JR. Perturbations of the AKT signaling pathway in human cancer. Oncogene. 2005 Nov 14;24(50):7455-64
Astrinidis A, Henske EP. Tuberous sclerosis complex: linking growth and energy signaling pathways with human disease. Oncogene. 2005 Nov 14;24(50):7475-81
Inoki K, Corradetti MN, Guan KL. Dysregulation of the TSC-mTOR pathway in human disease. Nat Genet. 2005 Jan;37(1):19-24
Johannessen CM, Reczek EE, James MF, Brems H, Legius E, Cichowski K. The NF1 tumor suppressor critically regulates TSC2 and mTOR. Proc Natl Acad Sci U S A. 2005 Jun 14;102(24):8573-8
Kwiatkowski DJ, Manning BD. Tuberous sclerosis: a GAP at the crossroads of multiple signaling pathways. Hum Mol Genet. 2005 Oct 15;14 Spec No. 2:R251-8
Avruch J, Hara K, Lin Y, Liu M, Long X, Ortiz-Vega S, Yonezawa K. Insulin and amino-acid regulation of mTOR signaling and kinase activity through the Rheb GTPase. Oncogene. 2006 Oct 16;25(48):6361-72
Guertin DA, Stevens DM, Thoreen CC, Burds AA, Kalaany NY, Moffat J, Brown M, Fitzgerald KJ, Sabatini DM. Ablation in mice of the mTORC components raptor, rictor, or mLST8 reveals that mTORC2 is required for signaling to Akt-FOXO and PKCalpha, but not S6K1. Dev Cell. 2006 Dec;11(6):859-71
Sarbassov DD, Ali SM, Sengupta S, Sheen JH, Hsu PP, Bagley AF, Markhard AL, Sabatini DM. Prolonged rapamycin treatment inhibits mTORC2 assembly and Akt/PKB. Mol Cell. 2006 Apr 21;22(2):159-68
Bhaskar PT, Hay N. The two TORCs and Akt. Dev Cell. 2007 Apr;12(4):487-502
Cho D, Signoretti S, Regan M, Mier JW, Atkins MB. The role of mammalian target of rapamycin inhibitors in the treatment of advanced renal cancer. Clin Cancer Res. 2007 Jan 15;13(2 Pt 2):758s-763s
Guertin DA, Sabatini DM. Defining the role of mTOR in cancer. Cancer Cell. 2007 Jul;12(1):9-22
Gustafson S, Zbuk KM, Scacheri C, Eng C. Cowden syndrome. Semin Oncol. 2007 Oct;34(5):428-34
Land SC, Tee AR. Hypoxia-inducible factor 1alpha is regulated by the mammalian target of rapamycin (mTOR) via an mTOR signaling motif. J Biol Chem. 2007 Jul 13;282(28):20534-43
Masri J, Bernath A, Martin J, Jo OD, Vartanian R, Funk A, Gera J. mTORC2 activity is elevated in gliomas and promotes
growth and cell motility via overexpression of rictor. Cancer Res. 2007 Dec 15;67(24):11712-20
Oshiro N, Takahashi R, Yoshino K, Tanimura K, Nakashima A, Eguchi S, Miyamoto T, Hara K, Takehana K, Avruch J, Kikkawa U, Yonezawa K. The proline-rich Akt substrate of 40 kDa (PRAS40) is a physiological substrate of mammalian target of rapamycin complex 1. J Biol Chem. 2007 Jul 13;282(28):20329-39
Thedieck K, Polak P, Kim ML, Molle KD, Cohen A, Jenö P, Arrieumerlou C, Hall MN. PRAS40 and PRR5-like protein are new mTOR interactors that regulate apoptosis. PLoS One. 2007 Nov 21;2(11):e1217
Vander Haar E, Lee SI, Bandhakavi S, Griffin TJ, Kim DH. Insulin signalling to mTOR mediated by the Akt/PKB substrate PRAS40. Nat Cell Biol. 2007 Mar;9(3):316-23
Wan X, Helman LJ. The biology behind mTOR inhibition in sarcoma. Oncologist. 2007 Aug;12(8):1007-18
Wang L, Harris TE, Roth RA, Lawrence JC Jr. PRAS40 regulates mTORC1 kinase activity by functioning as a direct inhibitor of substrate binding. J Biol Chem. 2007 Jul 6;282(27):20036-44
Zeng Z, Sarbassov dos D, Samudio IJ, Yee KW, Munsell MF, Ellen Jackson C, Giles FJ, Sabatini DM, Andreeff M, Konopleva M. Rapamycin derivatives reduce mTORC2 signaling and inhibit AKT activation in AML. Blood. 2007 Apr 15;109(8):3509-12
Abraham RT, Eng CH. Mammalian target of rapamycin as a therapeutic target in oncology. Expert Opin Ther Targets. 2008 Feb;12(2):209-22
Goncharova EA, Krymskaya VP. Pulmonary lymphangioleiomyomatosis (LAM): progress and current challenges. J Cell Biochem. 2008 Feb 1;103(2):369-82
Hanna SC, Heathcote SA, Kim WY. mTOR pathway in renal cell carcinoma. Expert Rev Anticancer Ther. 2008 Feb;8(2):283-92
Johannessen CM, Johnson BW, Williams SM, Chan AW, Reczek EE, Lynch RC, Rioth MJ, McClatchey A, Ryeom S, Cichowski K. TORC1 is essential for NF1-associated malignancies. Curr Biol. 2008 Jan 8;18(1):56-62
Jozwiak J, Jozwiak S, Wlodarski P. Possible mechanisms of disease development in tuberous sclerosis. Lancet Oncol. 2008 Jan;9(1):73-9
Krymskaya VP. Smooth muscle-like cells in pulmonary lymphangioleiomyomatosis. Proc Am Thorac Soc. 2008 Jan 1;5(1):119-26
Pattingre S, Espert L, Biard-Piechaczyk M, Codogno P. Regulation of macroautophagy by mTOR and Beclin 1 complexes. Biochimie. 2008 Feb;90(2):313-23
Scoles DR. The merlin interacting proteins reveal multiple targets for NF2 therapy. Biochim Biophys Acta. 2008 Jan;1785(1):32-54
Wei C, Amos CI, Zhang N, Wang X, Rashid A, Walker CL, Behringer RR, Frazier ML. Suppression of Peutz-Jeghers polyposis by targeting mammalian target of rapamycin signaling. Clin Cancer Res. 2008 Feb 15;14(4):1167-71
This article should be referenced as such:
Altomare DA, Testa JR. FRAP1 (FK506 binding protein 12-rapamycin associated protein 1). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):348-353.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 354
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
GPA33 (glycoprotein A33 (transmembrane)) Tania Tabone, Joan K Heath
Ludwig Institute for Cancer Research, Melbourne Branch, PO Box 2008, Royal Melbourne Hospital, Parkville, VIC 3050, Australia (TT, JKH)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/GPA33ID40735ch1q23.html DOI: 10.4267/2042/44469
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: A33; MGC129986; MGC129987
HGNC (Hugo): GPA33
Location: 1q24.1
Note: Location of GPA33 on human chromosome 1q24 showing flanking genes to demonstrate synteny to other vertebrates, such as mouse (chromosome 1) and zebrafish (chromosomes 1 and 9). Note that an evolutionary duplication event of the entire zebrafish genome has resulted in the two copies of gpa33 in zebrafish.
DNA/RNA Description The human GPA33 gene comprises 7 exons (all coding) spanning 37,787 bp of genomic DNA.
Transcription 2,793 bp mRNA; 960 bp open reading frame (Heath et al., 1997).
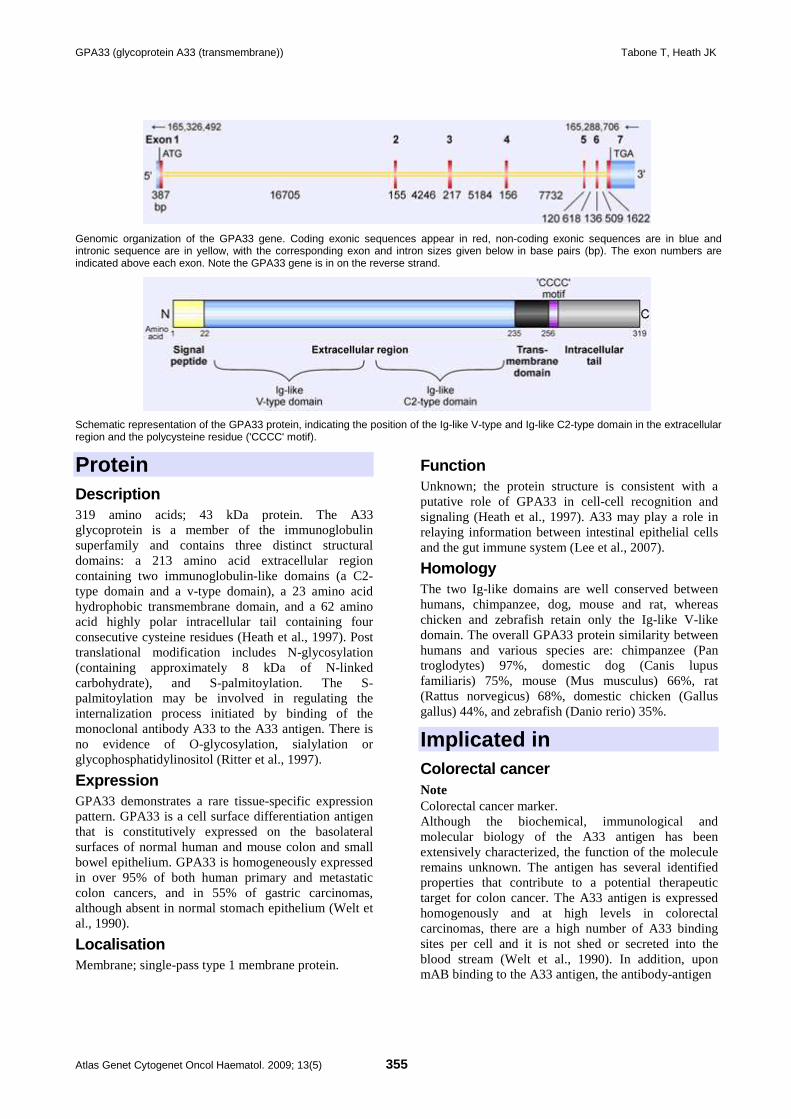
GPA33 (glycoprotein A33 (transmembrane)) Tabone T, Heath JK
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 355
Genomic organization of the GPA33 gene. Coding exonic sequences appear in red, non-coding exonic sequences are in blue and intronic sequence are in yellow, with the corresponding exon and intron sizes given below in base pairs (bp). The exon numbers are indicated above each exon. Note the GPA33 gene is in on the reverse strand.
Schematic representation of the GPA33 protein, indicating the position of the Ig-like V-type and Ig-like C2-type domain in the extracellular region and the polycysteine residue ('CCCC' motif).
Protein Description 319 amino acids; 43 kDa protein. The A33 glycoprotein is a member of the immunoglobulin superfamily and contains three distinct structural domains: a 213 amino acid extracellular region containing two immunoglobulin-like domains (a C2-type domain and a v-type domain), a 23 amino acid hydrophobic transmembrane domain, and a 62 amino acid highly polar intracellular tail containing four consecutive cysteine residues (Heath et al., 1997). Post translational modification includes N-glycosylation (containing approximately 8 kDa of N-linked carbohydrate), and S-palmitoylation. The S-palmitoylation may be involved in regulating the internalization process initiated by binding of the monoclonal antibody A33 to the A33 antigen. There is no evidence of O-glycosylation, sialylation or glycophosphatidylinositol (Ritter et al., 1997).
Expression GPA33 demonstrates a rare tissue-specific expression pattern. GPA33 is a cell surface differentiation antigen that is constitutively expressed on the basolateral surfaces of normal human and mouse colon and small bowel epithelium. GPA33 is homogeneously expressed in over 95% of both human primary and metastatic colon cancers, and in 55% of gastric carcinomas, although absent in normal stomach epithelium (Welt et al., 1990).
Localisation Membrane; single-pass type 1 membrane protein.
Function Unknown; the protein structure is consistent with a putative role of GPA33 in cell-cell recognition and signaling (Heath et al., 1997). A33 may play a role in relaying information between intestinal epithelial cells and the gut immune system (Lee et al., 2007).
Homology The two Ig-like domains are well conserved between humans, chimpanzee, dog, mouse and rat, whereas chicken and zebrafish retain only the Ig-like V-like domain. The overall GPA33 protein similarity between humans and various species are: chimpanzee (Pan troglodytes) 97%, domestic dog (Canis lupus familiaris) 75%, mouse (Mus musculus) 66%, rat (Rattus norvegicus) 68%, domestic chicken (Gallus gallus) 44%, and zebrafish (Danio rerio) 35%.
Implicated in Colorectal cancer Note Colorectal cancer marker. Although the biochemical, immunological and molecular biology of the A33 antigen has been extensively characterized, the function of the molecule remains unknown. The antigen has several identified properties that contribute to a potential therapeutic target for colon cancer. The A33 antigen is expressed homogenously and at high levels in colorectal carcinomas, there are a high number of A33 binding sites per cell and it is not shed or secreted into the blood stream (Welt et al., 1990). In addition, upon mAB binding to the A33 antigen, the antibody-antigen

GPA33 (glycoprotein A33 (transmembrane)) Tabone T, Heath JK
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 356
complex is internalized and sequestered in vesicles (Daghighian et al., 1996). Selective immunological targeting of tumors with monoclonal antibodies (mAb) is an important therapeutic approach in cancer therapy. Clinical imaging and biopsy-based biodistribution studies using radiolabeled murine mAb A33 demonstrated specific targeting to antigen-positive tumor tissues in 95% of colorectal patients with tumor retention for up to six weeks (Welt et al., 1990; Welt et al., 1994). The only normal tissue reported to accumulate the radioisotope was the bowel, with clearance from the normal gastrointestinal tract within one week. Phase I and II therapy trials using 125I- and 131I-labeled murine A33 mAb were shown to have antitumor effects without bowel toxicity, however human anti-mouse antibody development in all patients prevented repeated dosing and led to the development of humanized mAb A33 (huA33). Phase I clinical trials using multiple dose schedules of 125I- and 131I-labled huA33 mAb in patients with colorectal carcinoma have been conducted and have shown safety and possible efficacy, with future trials proposed (Chong et al., 2005; Scott et al., 2005).
References Welt S, Divgi CR, Real FX, Yeh SD, Garin-Chesa P, Finstad CL, Sakamoto J, Cohen A, Sigurdson ER, Kemeny N. Quantitative analysis of antibody localization in human metastatic colon cancer: a phase I study of monoclonal antibody A33. J Clin Oncol. 1990 Nov;8(11):1894-906
Welt S, Divgi CR, Kemeny N, Finn RD, Scott AM, Graham M, Germain JS, Richards EC, Larson SM, Oettgen HF. Phase I/II study of iodine 131-labeled monoclonal antibody A33 in patients with advanced colon cancer. J Clin Oncol. 1994 Aug;12(8):1561-71
Daghighian F, Barendswaard E, Welt S, Humm J, Scott A, Willingham MC, McGuffie E, Old LJ, Larson SM. Enhancement of radiation dose to the nucleus by vesicular internalization of iodine-125-labeled A33 monoclonal antibody. J Nucl Med. 1996 Jun;37(6):1052-7
Heath JK, White SJ, Johnstone CN, Catimel B, Simpson RJ, Moritz RL, Tu GF, Ji H, Whitehead RH, Groenen LC, Scott AM, Ritter G, Cohen L, Welt S, Old LJ, Nice EC, Burgess AW. The human A33 antigen is a transmembrane glycoprotein and a novel member of the immunoglobulin superfamily. Proc Natl Acad Sci U S A. 1997 Jan 21;94(2):469-74
Ritter G, Cohen LS, Nice EC, Catimel B, Burgess AW, Moritz RL, Ji H, Heath JK, White SJ, Welt S, Old LJ, Simpson RJ. Characterization of posttranslational modifications of human A33 antigen, a novel palmitoylated surface glycoprotein of human gastrointestinal epithelium. Biochem Biophys Res Commun. 1997 Jul 30;236(3):682-6
Chong G, Lee FT, Hopkins W, Tebbutt N, Cebon JS, Mountain AJ, Chappell B, Papenfuss A, Schleyer P, U P, Murphy R, Wirth V, Smyth FE, Potasz N, Poon A, Davis ID, Saunder T, O'keefe GJ, Burgess AW, Hoffman EW, Old LJ, Scott AM. Phase I trial of 131I-huA33 in patients with advanced colorectal carcinoma. Clin Cancer Res. 2005 Jul 1;11(13):4818-26
Scott AM, Lee FT, Jones R, Hopkins W, MacGregor D, Cebon JS, Hannah A, Chong G, U P, Papenfuss A, Rigopoulos A, Sturrock S, Murphy R, Wirth V, Murone C, Smyth FE, Knight S, Welt S, Ritter G, Richards E, Nice EC, Burgess AW, Old LJ. A phase I trial of humanized monoclonal antibody A33 in patients with colorectal carcinoma: biodistribution, pharmacokinetics, and quantitative tumor uptake. Clin Cancer Res. 2005 Jul 1;11(13):4810-7
Lee JW, Epardaud M, Sun J, Becker JE, Cheng AC, Yonekura AR, Heath JK, Turley SJ. Peripheral antigen display by lymph node stroma promotes T cell tolerance to intestinal self. Nat Immunol. 2007 Feb;8(2):181-90
This article should be referenced as such:
Tabone T, Heath JK. GPA33 (glycoprotein A33 (transmembrane)). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):354-356.
Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 357
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
KLK5 (Kallikrein-related peptidase 5) George M Yousef, Eleftherios P Diamandis
Department of Laboratory Medicine,St Michael's Hospital,30 Bond Street, Toronto, ON, M5B 1W8, Canada, (GMY), Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, 6th Floor, Room 6-201, Box 32, 60 Murray Street, Toronto, Ontario, Canada, M5T 3L9 (EPD)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/KLK5ID41085ch19q13.html DOI: 10.4267/2042/44470
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: EC 3.4.21; HSCTE; KLK-L2; KLKL2; SCTE
HGNC (Hugo): KLK5
Location: 19q13.41
Local order: Telomere to centromere.
DNA/RNA Description The KLK5 gene is approximately 9.5 kb in length, consisting of 6 exons (5 of them are coding exons) and 5 introns.
Transcription Five alternatively spliced variants have been identified for the KLK5 gene. These variants differ in the number and length of the 5' untranslated exons and/or the last two coding exons. Tissue-specific expression of these variants is regulated by multiple promoters located in the first exon of each isoform. KLK5 splice variants were found to be differentially expressed, at the mRNA level, in ovarian, breast and prostate cancers.
Pseudogene None identified.
Protein Description Full-length KLK5 is formed of 293 amino acids. It is composed of a signal peptide (29 amino acids), followed by an activation peptide (37 amino acids) and the mature chain (227 amino acids), with 4 potential N-linked glycosylation sites. The position of the catalytic
triad of serine proteases is conserved. KLK5 is synthesized as a full-length protein intracellularly. In the secretary pathway, the signal peptide is cleaved and the zymogen is released outside the cells. Upon activation, the propeptide is removed to generate the mature active protein. In serum and ascites fluid, in addition to the free (approximately 40 kDa) form, KLK5 forms complexes with alpha(1)-antitrypsin and alpha(2)-macroglobulin.
Expression At the mRNA level, KLK5 is expressed in a variety of tissues, mainly the testis, brain, breast, thyroid and salivary glands. The KLK5 protein is expressed at higher levels in the skin, salivary gland, testis and female genital organs. KLK5 has also been identified in many biological fluids, including vaginal secretions, breast milk and seminal plasma. Many fetal tissues, including bone, skin, thymus and kidney also express KLK5.
Localisation KLK5 is a secreted protein.
Function KLK5 is a secreted serine protease. The physiological functions of KLK5 are not fully understood. The KLK5 protein was originally identified from a keratinocyte library and was purified from the stratum corneum of the human skin. It was found to have a trypsin-like enzymatic activity with strong preference for Arg over Lys in the P1 position. Evidence exists that it plays a role in skin desquamation. KLK5 can also digest extracellular matrix components, collagens type I, II, III, IV, fibronectin, and laminin, and can potentially release angiostatin from plasminogen, and "cystatin-like domain 3" from low molecular weight kininogen, and fibrinopeptide B and peptide beta15-42 from the B

KLK5 (Kallikrein-related peptidase 5) Yousef GM, Diamandis EP
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 358
beta chain of fibrinogen. The KLK5 protein has been shown to activate another kallikrein, KLK7, and was found to be under steroid hormonal regulation in cancer cell lines. It has been recently shown that KLK5 is differentially expressed in a number of malignancies, including ovarian, breast and prostate cancers, but the mechanisms of its involvement in cancer have yet to be determined.
Homology The human KLK5 protein sequence shares 40-70% homology with other members of the human tissue kallikreins, and 70% identity with that of the mouse orthologue.
Mutations Note No germinal or somatic mutations are identified to be associated with cancer so far.
Implicated in Ovarian cancer Disease Higher KLK5 concentrations were found in the serum of 69% of patients with ovarian cancer. The KLK5 protein was found to be elevated in 55% of ovarian cancer tissues compared to normal. Also, KLK5 mRNA is significantly elevated in ovarian cancer, especially serous type. Ovarian cancer ascites contains higher levels, as compared to benign effusions and ascites from other cancer types. Two KLK5 splice variants are upregulated in ovarian cancer tissues compared to normal.
Prognosis The KLK5 mRNA and protein are markers of unfavorable prognosis in ovarian cancer, being overexpressed in late stage and higher grade tumors, and associated with shorter DFS and OS. In addition, the KLK5 protein was shown to be an independent indicator of poor prognosis in patients with high-grade tumors and optimal debulking success.
Cytogenetics No cytogenetic abnormalities are identified so far.
Hybrid/Mutated gene None identified.
Breast cancer Disease Higher concentrations of KLK5 were found in the serum of 49% of patients with breast cancer. KLK5 splice variant 2 is downregulated in breast cancer compared to normal.
Prognosis The KLK5 mRNA transcript was found to be an indicator of unfavorable prognosis, being
overexpressed in node-positive patients with ER-negative tumors. It is independently associated with decreased DFS and OS, and it is an independent indicator of shorter DFS and OS in node-positive patients.
Cytogenetics No cytogenetic abnormalities are identified so far.
Hybrid/Mutated gene None identified.
Prostate cancer Disease KLK5 mRNA is downregulated in cancer vs normal prostatic tissues.
Prognosis KLK5 mRNA is a favorable prognostic maker, with higher levels associated with low grade tumors and low Gleason score.
Cytogenetics No cytogenetic abnormalities are identified so far.
Hybrid/Mutated gene None identified.
Testicular cancer Disease KLK5 mRNA is downregulated in cancer vs normal testicular tissues.
Prognosis KLK5 mRNA is a marker of favorable prognosis, overexpressed in smaller, early stage non-seminomas.
Cytogenetics No cytogenetic abnormalities are identified so far.
Hybrid/Mutated gene None identified.
Non-small cell lung carcinoma Disease Serum KLK5 levels are lower in lung cancer compared to normal and can be used as part of a multiparametric panel for diagnosis.
Prognosis None identified.
Cytogenetics No cytogenetic abnormalities are identified so far.
Hybrid/Mutated gene None identified.
Urinary bladder carcinoma Disease None identified.
Prognosis Increased expression of KLK5 was frequently observed in invasive tumors (pT2-pT4) compared with superficial tumors (pTa, pT1).

KLK5 (Kallikrein-related peptidase 5) Yousef GM, Diamandis EP
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 359
Cytogenetics Copy number gain was observed in transitional cell carcinoma.
Hybrid/Mutated gene None identified.
Breakpoints Note None identified.
References Kim H, Scorilas A, Katsaros D, Yousef GM, Massobrio M, Fracchioli S, Piccinno R, Gordini G, Diamandis EP. Human kallikrein gene 5 (KLK5) expression is an indicator of poor prognosis in ovarian cancer. Br J Cancer. 2001 Mar 2;84(5):643-50
Yousef GM, Obiezu CV, Jung K, Stephan C, Scorilas A, Diamandis EP. Differential expression of Kallikrein gene 5 in cancerous and normal testicular tissues. Urology. 2002 Oct;60(4):714-8
Yousef GM, Scorilas A, Chang A, Rendl L, Diamandis M, Jung K, Diamandis EP. Down-regulation of the human kallikrein gene 5 (KLK5) in prostate cancer tissues. Prostate. 2002 May 1;51(2):126-32
Yousef GM, Scorilas A, Kyriakopoulou LG, Rendl L, Diamandis M, Ponzone R, Biglia N, Giai M, Roagna R, Sismondi P, Diamandis EP. Human kallikrein gene 5 (KLK5) expression by quantitative PCR: an independent indicator of poor prognosis in breast cancer. Clin Chem. 2002 Aug;48(8):1241-50
Dong Y, Kaushal A, Brattsand M, Nicklin J, Clements JA. Differential splicing of KLK5 and KLK7 in epithelial ovarian cancer produces novel variants with potential as cancer biomarkers. Clin Cancer Res. 2003 May;9(5):1710-20
Yousef GM, Kapadia C, Polymeris ME, Borgono C, Hutchinson S, Wasney GA, Soosaipillai A, Diamandis EP. The human kallikrein protein 5 (hK5) is enzymatically active, glycosylated and forms complexes with two protease inhibitors in ovarian cancer fluids. Biochim Biophys Acta. 2003 Jul 28;1628(2):88-96
Yousef GM, Polymeris ME, Grass L, Soosaipillai A, Chan PC, Scorilas A, Borgoño C, Harbeck N, Schmalfeldt B, Dorn J, Schmitt M, Diamandis EP. Human kallikrein 5: a potential novel serum biomarker for breast and ovarian cancer. Cancer Res. 2003 Jul 15;63(14):3958-65
Yousef GM, Polymeris ME, Yacoub GM, Scorilas A, Soosaipillai A, Popalis C, Fracchioli S, Katsaros D, Diamandis EP. Parallel overexpression of seven kallikrein genes in ovarian cancer. Cancer Res. 2003 May 1;63(9):2223-7
Kurlender L, Yousef GM, Memari N, Robb JD, Michael IP, Borgoño C, Katsaros D, Stephan C, Jung K, Diamandis EP. Differential expression of a human kallikrein 5 (KLK5) splice variant in ovarian and prostate cancer. Tumour Biol. 2004 May-Jun;25(3):149-56
Yousef GM, White NM, Kurlender L, Michael I, Memari N, Robb JD, Katsaros D, Stephan C, Jung K, Diamandis EP. The kallikrein gene 5 splice variant 2 is a new biomarker for breast and ovarian cancer. Tumour Biol. 2004 Sep-Dec;25(5-6):221-7
Yousef GM, Yacoub GM, Polymeris ME, Popalis C, Soosaipillai A, Diamandis EP. Kallikrein gene downregulation in breast cancer. Br J Cancer. 2004 Jan 12;90(1):167-72
Michael IP, Sotiropoulou G, Pampalakis G, Magklara A, Ghosh M, Wasney G, Diamandis EP. Biochemical and enzymatic characterization of human kallikrein 5 (hK5), a novel serine protease potentially involved in cancer progression. J Biol Chem. 2005 Apr 15;280(15):14628-35
Planque C, de Monte M, Guyetant S, Rollin J, Desmazes C, Panel V, Lemarié E, Courty Y. KLK5 and KLK7, two members of the human tissue kallikrein family, are differentially expressed in lung cancer. Biochem Biophys Res Commun. 2005 Apr 22;329(4):1260-6
Prezas P, Arlt MJ, Viktorov P, Soosaipillai A, Holzscheiter L, Schmitt M, Talieri M, Diamandis EP, Krüger A, Magdolen V. Overexpression of the human tissue kallikrein genes KLK4, 5, 6, and 7 increases the malignant phenotype of ovarian cancer cells. Biol Chem. 2006 Jun;387(6):807-11
Shaw JL, Diamandis EP. Distribution of 15 human kallikreins in tissues and biological fluids. Clin Chem. 2007 Aug;53(8):1423-32
Shinoda Y, Kozaki K, Imoto I, Obara W, Tsuda H, Mizutani Y, Shuin T, Fujioka T, Miki T, Inazawa J. Association of KLK5 overexpression with invasiveness of urinary bladder carcinoma cells. Cancer Sci. 2007 Jul;98(7):1078-86
Planque C, Li L, Zheng Y, Soosaipillai A, Reckamp K, Chia D, Diamandis EP, Goodglick L. A multiparametric serum kallikrein panel for diagnosis of non-small cell lung carcinoma. Clin Cancer Res. 2008 Mar 1;14(5):1355-62
This article should be referenced as such:
Yousef GM, Diamandis EP. KLK5 (Kallikrein-related peptidase 5). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):357-359.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 360
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
MIR10B (microRNA 10b) Begum Akman, Ayse Elif Erson
Department of Biology, Office 141, Laboratory, B-56, Middle East Technical University, Ankara 06531, Turkey (BA, AEE)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/MIRN10BID44292ch2q31.html DOI: 10.4267/2042/44471
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: MIRN10B (microRNA 10b): MIR10B; hsa-mir-10b; mir-10b
HGNC (Hugo): MIR10B
Location: 2q31.1
Local order: Based on Mapviewer Genes on Sequence, genes flanking MIRN10B oriented from centromere to telomere on 2q31.1 are:
HOXD11; Homeobox 11, 2q31.1
HOXD 10; Homeobox 10, 2q31.1
HOXD 9; Homeobox 9, 2q31.1
HOXD 8; Homeobox 8, 2q31.1
MIRN10B; microRNA 10b, 2q31.1
HOXD 4; Homeobox 4, 2q31.1
HOXD 3; Homeobox3, 2q31.1
MTX2; Metaxin 2, 2q31.1.
DNA/RNA
Stem-loop structure of mir-10b.
Description In human, microRNA-10 gene has been duplicated. It is now present in the form of two variants as miR-10a and miR-10b located on different chromosomes. miR-10a is located between HOX4B and HOX5B on 17q21, while miR-10b is located between HOXD4 and HOXD8 on 2q31.1. It is believed that, there is a strong correlation between the specific miRs and HOX genes. MIRN10B maps
to the HOXD cluster on 2q31.1. HOX genes are a family of transcription factor genes that play crucial roles during normal development and in oncogenesis. HOXD4 expression is deregulated in a variety of solid and hematopoietic cancers.
Transcription miRNAs are generally transcribed by RNA polymerase II. There is limited information on how miRNA gene expression is regulated due to lack of basic information of their gene structures. Screening of miRNA putative promoter regions (miPPRs) revealed miPPR-10b for MIRN10B. TWIST1, a metastasis-promoting transcription factor, has been shown to induce miR-10b via binding to the most proximal E-box upstream of the miR-10b hairpin region. This E-box was in the miPPR-10b. Pri-miRNA (primary) mir-10b: The primary miRNA transcripts are called pri-miRNAs. They contain cap structures and poly(A) tails. If transcribed by RNA polymerase II, primary transcript of mir-10b is not known yet. Pre-miRNA (precursor) mir-10b: pri-miRNA transcripts are processed by microprocessor complex consisting nuclear RNase enzyme Drosha and the double-stranded RNA binding protein Pasha to generate pre-miRNAs. The precursor mir-10b is 110 nucleotides long. Pre-miR-10b is transferred from nucleus to cytoplasm. Sequence: 5'-CCAGAGGUUGUAACGUUGUCUAUAUA UACCCUGUAGAACCGAAUUUGUGUGGUAUCCGUAUAGUCACAGAUUCGAUUCUAGGGGAAUAUAUGGUCGAUGCAAAAACUUCA-3' Mature miR-10b: In the cytoplasm, pre-miRNA molecules are processed into mature miRNA by RNA-

MIR10B (microRNA 10b) Akman B, Erson AE
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 361
induced silencing complex (RISC). Mature miR-10b is 23 nucleotides long. Sequence: 5'-UACCCUGUAGAACCGAAUUUGUG-3'
Pseudogene No reported pseudogenes.
Protein Note MicroRNAs are not translated into amino acids.
Mutations Note Gene mutations have not been described.
Implicated in Colorectal neoplasia Disease Possible changes in microRNA levels; including miR-10b, was investigated during colorectal tumorigenesis. There was not a significant down-regulation of microRNA 10b in colon tumors to suggest a potential role in colorectal tumorigenesis.
Breast Cancer Disease 76 breast cancers and 10 normal breast samples were analyzed by microRNA microarray and Northern Blotting to identify miRNAs whose expression is deregulated notably in cancer versus normal breast tissues. According to these results; miR-10b was one of the microRNAs which were down-regulated.
Oncogenesis Tumor invasion and Metastasis: Although miR-10b was downregulated in nonmetastatic breast cancers in comparison with normal breast tissue, this miRNA was over-expressed in about 50% of metastatic breast cancers. Ectopic expression of miR-10b had no effect on proliferation, but an increase in transwell migration and Matrigel invasion was observed. In vivo ectopic expression of miR-10b conferred invasive properties on otherwise non-invasive breast cancer cells. Although control tumors could not invade surrounding tissues and exhibited poor vascularization, miR-10b over-expressing tumors exhibited an invasive behavior and
were highly vascularized. miR-10b promoted metastasis in non-metastatic breast cancer cells. Lung micro-metastasis was detected in miR-10b over-expressing cells while there were no intravasating cells or lung metastases in control tumors. It was shown that miR-10b expression was induced by transcription factor TWIST allowing miR-10b to inhibit translation of the mRNA encoding homeobox D10 (Figure 2). This resulted in increased expression of a well-characterized prometastatic gene, RHOC (ras homolog gene family member C), thus leading to migration, tumor invasion, and metastasis.
Glioblastoma Disease miR-10b was one of the over-expressed miRNAs in glioblastomas compared to peripheral tissues. According to the microarray studies on glioblastomas, an excess of 1.97- to 13.6-fold increase was observed in 5 in out of 9 samples. This data was further confirmed by Northern blotting. miR-10b was stated to be a candidate oncogene microRNA as it was significantly upregulated in glioblastomas.
Acute Myeloid Leukemia (AML) Disease Role of microRNAs in the biology of NPMc+ (nucleophosmin) AML was investigated in 85 adult de novo AML patients. Microarray studies characterized these patients for subcellular localization/mutation status of NPM1 and FLT3 mutations. A strong microRNA expression pattern was identified which differentiated NPMc+ mutated from the cytoplasmic-negative (NPM1 unmutated) cases. According to this pattern, miRNA-10b together with miRNA-10a, let-7 and miR-29 family members were up-regulated. These data was further confirmed by qRT-PCR in 44 AML patients (randomly chosen from the initial cohort). According to the overall results, it was remarkable that miRNA-10b and miRNA-10a expression levels clearly differentiated NPMc+ vs. NPMc- cases.
Central Nervous System (CNS) tumors Disease Although, miRNA-10b was not specifically expressed in brain tissue, it was one of the 5 microRNAs which were highly expressed in CNS tumor-derived cell lines compared to normal brain tissue.
Regulation and function of miR-10b in breast cancer metastasis.
MIR10B (microRNA 10b) Akman B, Erson AE
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 362
Hepatocellular adenomas (HCAs) and Hepatocellular Carcinomas (HCCs) Disease Expression of miRNAs was analyzed in a series of 46 malignant and benign hepatocellular tumors compared to 4 normal liver tissues. The most significant deregulated miRNAs were further analyzed in a second series of 43 tumors and 16 non-tumor liver tissues including cirrhosis and chronic hepatitis of various etiologies. miRNA-10b was found to be overexpressed in HCC when compared to benign tumors and non-tumor liver tissues.
Protein synthesis inhibition Disease The apolipoprotein B mRNA-editing enzyme catalytic polypeptide-like 3G (APOBEC3G or A3G) and other APOBEC family members were shown to induce protein synthesis by miRNAs such as miR-10b in 293T and HeLa cells. miRNA microarray results suggested overexpression of miR-10b in 293T cells. Luciferase assay showed A3G effects on miRNA mediated translational repression. A3G facilitates recruitment of miRNA-targeted mRNA to polysomes to synthesize more proteins and drives dissociation of miRNA-targeted mRNA from P-bodies.
Megakaryocytopoiesis Disease In order to discover regulatory pathways during megakaryocytic differentiation, microRNA expression profiling was performed for in vitro differentiated megakaryocytes derived from CD34+ hematopoietic progenitors. According to the PAM (predictive analysis of microarray), miR-10b was one of the microRNAs which were identified to be involved in megakaryocytic differentiation. Downregulation of miR-10b was shown by microarrays. But Northern blot analysis and q-RT-PCR results showed that miR-10a and miR-130a were the most significantly down-regulated among the examined miRNAs.
Adipogenesis Disease miR-10b was shown to be up-regulated during 3T3-L1 pre-adipocyte differentiation. It was stated that this up-regulation may not be related to an actual differentiation process and may be induced by growth arrest and/or hormonal stimulation.
References Meazza R, Faiella A, Corsetti MT, Airoldi I, Ferrini S, Boncinelli E, Corte G. Expression of HOXC4 homeoprotein in the nucleus of activated human lymphocytes. Blood. 1995 Apr 15;85(8):2084-90
Manohar CF, Salwen HR, Furtado MR, Cohn SL. Up-regulation of HOXC6, HOXD1, and HOXD8 homeobox gene expression in human neuroblastoma cells following chemical induction of differentiation. Tumour Biol. 1996;17(1):34-47
Bernstein E, Caudy AA, Hammond SM, Hannon GJ. Role for a bidentate ribonuclease in the initiation step of RNA interference. Nature. 2001 Jan 18;409(6818):363-6
Lagos-Quintana M, Rauhut R, Meyer J, Borkhardt A, Tuschl T. New microRNAs from mouse and human. RNA. 2003 Feb;9(2):175-9
Michael MZ, O' Connor SM, van Holst Pellekaan NG, Young GP, James RJ. Reduced accumulation of specific microRNAs in colorectal neoplasia. Mol Cancer Res. 2003 Oct;1(12):882-91
Calin GA, Sevignani C, Dumitru CD, Hyslop T, Noch E, Yendamuri S, Shimizu M, Rattan S, Bullrich F, Negrini M, Croce CM. Human microRNA genes are frequently located at fragile sites and genomic regions involved in cancers. Proc Natl Acad Sci U S A. 2004 Mar 2;101(9):2999-3004
Denli AM, Tops BB, Plasterk RH, Ketting RF, Hannon GJ. Processing of primary microRNAs by the Microprocessor complex. Nature. 2004 Nov 11;432(7014):231-5
Lee Y, Kim M, Han J, Yeom KH, Lee S, Baek SH, Kim VN. MicroRNA genes are transcribed by RNA polymerase II. EMBO J. 2004 Oct 13;23(20):4051-60
Ciafrè SA, Galardi S, Mangiola A, Ferracin M, Liu CG, Sabatino G, Negrini M, Maira G, Croce CM, Farace MG. Extensive modulation of a set of microRNAs in primary glioblastoma. Biochem Biophys Res Commun. 2005 Sep 9;334(4):1351-8
Iorio MV, Ferracin M, Liu CG, Veronese A, Spizzo R, Sabbioni S, Magri E, Pedriali M, Fabbri M, Campiglio M, Ménard S, Palazzo JP, Rosenberg A, Musiani P, Volinia S, Nenci I, Calin GA, Querzoli P, Negrini M, Croce CM. MicroRNA gene expression deregulation in human breast cancer. Cancer Res. 2005 Aug 15;65(16):7065-70
Zeng Y, Yi R, Cullen BR. Recognition and cleavage of primary microRNA precursors by the nuclear processing enzyme Drosha. EMBO J. 2005 Jan 12;24(1):138-48
Garzon R, Pichiorri F, Palumbo T, Iuliano R, Cimmino A, Aqeilan R, Volinia S, Bhatt D, Alder H, Marcucci G, Calin GA, Liu CG, Bloomfield CD, Andreeff M, Croce CM. MicroRNA fingerprints during human megakaryocytopoiesis. Proc Natl Acad Sci U S A. 2006 Mar 28;103(13):5078-83
Kajimoto K, Naraba H, Iwai N. MicroRNA and 3T3-L1 pre-adipocyte differentiation. RNA. 2006 Sep;12(9):1626-32
Debernardi S, Skoulakis S, Molloy G, Chaplin T, Dixon-McIver A, Young BD. MicroRNA miR-181a correlates with morphological sub-class of acute myeloid leukaemia and the expression of its target genes in global genome-wide analysis. Leukemia. 2007 May;21(5):912-6
Gaur A, Jewell DA, Liang Y, Ridzon D, Moore JH, Chen C, Ambros VR, Israel MA. Characterization of microRNA expression levels and their biological correlates in human cancer cell lines. Cancer Res. 2007 Mar 15;67(6):2456-68
Huang J, Liang Z, Yang B, Tian H, Ma J, Zhang H. Derepression of microRNA-mediated protein translation inhibition by apolipoprotein B mRNA-editing enzyme catalytic polypeptide-like 3G (APOBEC3G) and its family members. J Biol Chem. 2007 Nov 16;282(46):33632-40
Lui WO, Pourmand N, Patterson BK, Fire A. Patterns of known and novel small RNAs in human cervical cancer. Cancer Res. 2007 Jul 1;67(13):6031-43
Ma L, Teruya-Feldstein J, Weinberg RA. Tumour invasion and metastasis initiated by microRNA-10b in breast cancer. Nature. 2007 Oct 11;449(7163):682-8

MIR10B (microRNA 10b) Akman B, Erson AE
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 363
Fujita S, Iba H. Putative promoter regions of miRNA genes involved in evolutionarily conserved regulatory systems among vertebrates. Bioinformatics. 2008 Feb 1;24(3):303-8
Garzon R, Garofalo M, Martelli MP, Briesewitz R, Wang L, Fernandez-Cymering C, Volinia S, Liu CG, Schnittger S, Haferlach T, Liso A, Diverio D, Mancini M, Meloni G, Foa R, Martelli MF, Mecucci C, Croce CM, Falini B. Distinctive microRNA signature of acute myeloid leukemia bearing cytoplasmic mutated nucleophosmin. Proc Natl Acad Sci U S A. 2008 Mar 11;105(10):3945-50
Ladeiro Y, Couchy G, Balabaud C, Bioulac-Sage P, Pelletier L, Rebouissou S, Zucman-Rossi J. MicroRNA profiling in
hepatocellular tumors is associated with clinical features and oncogene/tumor suppressor gene mutations. Hepatology. 2008 Jun;47(6):1955-63
Ma L, Weinberg RA. MicroRNAs in malignant progression. Cell Cycle. 2008 Mar 1;7(5):570-2
Negrini M, Calin GA. Breast cancer metastasis: a microRNA story. Breast Cancer Res. 2008;10(2):203
This article should be referenced as such:
Akman B, Erson AE. MIR10B (microRNA 10b). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):360-363.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 364
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
RSPO1 (R-spondin homolog (Xenopus laevis)) Diana Blaydon
Centre for Cutaneous Research, Institute of Cell and Molecular Sciences, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, 4 Newark Street, Whitechapel, London E1 2AT, United Kingdom (DB)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/RSPO1ID44137ch1p34.html DOI: 10.4267/2042/44472
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: FLJ40906; R-spondin1; RP11-566C13; RSPONDIN; hRspo1
HGNC (Hugo): RSPO1
Location: 1p34.3
DNA/RNA Description 8 exons, 5 coding exons, 24 kb of genomic DNA.
Transcription mRNA about 2.5 kb, 263 residues in full-length translated protein, which contains an N-terminal signal peptide, followed by two cysteine-rich furin-like domains, one thrombospondin type 1 domain (TSP1 domain) and a putative C-terminal nuclear localization signal domain. Three alternatively spliced isoforms have been identified: one lacking the signal peptide encoded by exon 4, one lacking the thrombospondin domain encoded exon 7 and the third has an alternative 5' UTR.
Pseudogene None known.
Protein Description Secreted ligand with an N-terminal signal peptide, two cysteine-rich furin-like domains, one thrombospondin type 1 domain (TSP1) and a putative C-terminal nuclear localization signal domain.
Expression R-spondin1 expression is seen in a number of organs and appears to coincide with expression of genes that form part of the Wnt signaling pathway. In the developing mouse Rspo1 transcripts are undetectable at E7, dramatically increased by E11 and significantly reduced again by E17. Rspo1 expression is predominantly found in mesenchymal cells in a number of developing organs, including the forebrain, dorsal neural tube (roof plate), whisker follicles, kidney, mammary gland, small intestine, the long bones and vertebrae (Nam et al., 2007). Rspo1 expression is also detected in the mesenchyme underlying the developing dermis, while in adult skin, expression is restricted to the dermal papilla of the hair (Parma et al., 2006). Similarly, in humans, RSPO1 expression is detected in the small intestine, kidney, prostate, adrenal gland and pancreas (Kim et al., 2005). Expression of RSPO1 is detected in cultured primary human fibroblasts but not in cultured keratinocytes, indicating that R-spondin1 may be acting as a paracrine signaling molecule.
Localisation Secreted.
Function R-spondin1 is implicated in the Wnt signaling pathway where it seems to act as an enhancer of Wnt signaling. R-spondin1 appears to antagonize Dickkopf1 action, an inhibitor of the Wnt signaling pathway, by binding to the receptor Kremen1 and inhibiting the internalization of LRP6, a Wnt signaling co-receptor (Binnerts et al., 2007).

RSPO1 (R-spondin homolog (Xenopus laevis)) Blaydon D
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 365
Homology There are 3 paralogs of human RSPO1: RSPO2, RSPO3 and RSPO4. Orthologs have been identified in: mouse, chicken, dog, cow and chimpanzee.
Mutations Germinal To date, three homozygous RSPO1 mutations have been identified: a single base pair insertion, 896insG, a 2752 bp deletion that includes exon 4 (the first coding exon) and 286+1G>A, a splice site mutation. 896insG and the 2752 bp deletion were identified in two families exhibiting palmoplantar hyperkeratosis with a predisposition to squamous cell carcinoma of the skin and XX sex reversal. 896insG leads to a frameshift and stop codon after 10 amino acids resulting in the abolition of all normal isoforms of RSPO1. While the 2752 bp deletion allows production of a shorter form of RSPO1 mRNA, that may translate to a shorter protein lacking the signal peptide and first furin-like domain (Parma et al., 2006). The splice site mutation 286+1G>A was identified in a 46,XX female with true hermaphroditism, palmoplantar keratoderma, congenital bilateral corneal opacities, onychodystrophy and hearing impairment. 286+1G>A leads to aberrant splicing of the mRNA and skipping of the second coding exon in all RSPO1 isoforms and a predicted shortened R-spondin1 protein that lacks the entire first furin-like domain and the first two residues of the second furin-like repeat (Tomaselli et al., 2007).
Implicated in Palmoplantar hyperkeratosis with a predisposition to squamous cell carcinoma of the skin and XX sex reversal Note Two families.
Disease Mutations in the RSPO1 gene have been implicated in an autosomal recessive syndrome identified in an Italian family spanning three generations (Micali et al., 2005). The syndrome is characterized by: sclerodactyly, non-epidermolytic palmar plantar keratoderma (PPK) associated with multiple cutaneous squamous cell carcinomas, dental anomlies and early tooth loss due to chronic periodontal disease (in three out of five brothers), hypogenitalism with hypospadias, gynecomastia (in one brother), altered plasma sex hormone levels in the two brothers with abnormal genitalia and hypertriglyceridemia. Four out of the five affected brothers had an abnormal XX karyotype that was associated with the genital abnormalities. None of
the five sisters, or their offspring, were affected. The squamous cell carcinoma lesions found in these patients first developed in the hyperkeratotic skin of the hands and feet (PPK) and then metastasized to other parts of the body, indicating that a single gene is responsible for both the PPK and predisposition to SCC (Radi et al., 2005). However, the sex reversal can be considered to be non-penetrant in affected XY individuals. In this extended Italian family there are eleven 46,XX individuals in two sibships, all of the affected individuals have a male phenotype (two 46,XY and four 46,XX), while none of the seven genetic females with a female phenotype show any sign of the PPK/SCC phenotype or sexual ambiguity. This indicates that a single gene defect underlies both the PPK/SCC and sex reversal, rather than two independent mutations. The family is informative for linkage analysis for the PPK trait and allows linkage exclusion for the sex reversal trait. Linkage analysis performed on this family detected positive LOD scores for two markers at 1p34-p35. Furthermore, an additional affected individual, also from Southern Italy, who presented with XX sex reversal, PPK and SCC, also showed linkage to 1p34, but with a different haplotype (Parma et al., 2006). Sequencing identified two homozygous RSPO1 mutations in the two families. A single nucleotide insertion in codon 36 results in a frame-shift and stop codon after ten amino acid residues, predicted to lead to abolition of all RSPO1 isoforms. However, the second mutation, a 2752 bp deletion including exon 4, leads to a shorter mRNA that may translate to a putative, shorter protein lacking the signal peptide and first furin domain. In situ hybridization analysis has identified expression of mRspo1 in the urogenital ridge at E10.5, with sex-specific differences appearing at E12.5 inline with an increase in the somatic cells of the XX gonad. Furthermore, qPCR detected no differences in mRspo1 levels between XX and XY gonads at E10.5 and E11.5, by E12.5, however, there is a clear increase of expression in XX gonads which is five-fold higher than XY gonads by E14.5. Therefore, there is a sex-specific regulation of R spondin1 at a crucial time in sex determination (Parma et al., 2006). What is more, in the XX sex reversal patients, functional testes are present, but the individuals are sterile, indicating that R-spondin1 is not required for testis differentiation and function (Parma et al., 2006). RT-PCR has shown that RSPO1 is not expressed in cultured keratinocytes, but it is expressed in fibroblasts. Furthermore, plantar keratinocytes from an affected individual did not differentiate in organotypic culture. Together, this data suggests that R-spondin1 might act as a paracrine signal from fibroblasts to keratinocytes, regulating keratinocyte proliferation and differentiation (Parma et al., 2006).

RSPO1 (R-spondin homolog (Xenopus laevis)) Blaydon D
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 366
Syndromic true hermaphroditism with palmoplantar keratoderma, congenital bilateral corneal opacities, onychodystrophy and hearing impairment Note One patient.
References Kim KA, Kakitani M, Zhao J, Oshima T, Tang T, Binnerts M, Liu Y, Boyle B, Park E, Emtage P, Funk WD, Tomizuka K. Mitogenic influence of human R-spondin1 on the intestinal epithelium. Science. 2005 Aug 19;309(5738):1256-9
Micali G, Nasca MR, Innocenzi D, Frasin LA, Radi O, Parma P, Camerino G, Schwartz RA. Association of palmoplantar keratoderma, cutaneous squamous cell carcinoma, dental anomalies, and hypogenitalism in four siblings with 46,XX karyotype: a new syndrome. J Am Acad Dermatol. 2005 Nov;53(5 Suppl 1):S234-9
Radi O, Parma P, Imbeaud S, Nasca MR, Uccellatore F, Maraschio P, Tiepolo L, Micali G, Camerino G. XX sex reversal, palmoplantar keratoderma, and predisposition to squamous cell carcinoma: genetic analysis in one family. Am J Med Genet A. 2005 Oct 15;138A(3):241-6
Parma P, Radi O, Vidal V, Chaboissier MC, Dellambra E, Valentini S, Guerra L, Schedl A, Camerino G. R-spondin1 is
essential in sex determination, skin differentiation and malignancy. Nat Genet. 2006 Nov;38(11):1304-9
Binnerts ME, Kim KA, Bright JM, Patel SM, Tran K, Zhou M, Leung JM, Liu Y, Lomas WE 3rd, Dixon M, Hazell SA, Wagle M, Nie WS, Tomasevic N, Williams J, Zhan X, Levy MD, Funk WD, Abo A. R-Spondin1 regulates Wnt signaling by inhibiting internalization of LRP6. Proc Natl Acad Sci U S A. 2007 Sep 11;104(37):14700-5
Nam JS, Turcotte TJ, Yoon JK. Dynamic expression of R-spondin family genes in mouse development. Gene Expr Patterns. 2007 Jan;7(3):306-12
Wei Q, Yokota C, Semenov MV, Doble B, Woodgett J, He X. R-spondin1 is a high affinity ligand for LRP6 and induces LRP6 phosphorylation and beta-catenin signaling. J Biol Chem. 2007 May 25;282(21):15903-11
Zhao J, de Vera J, Narushima S, Beck EX, Palencia S, Shinkawa P, Kim KA, Liu Y, Levy MD, Berg DJ, Abo A, Funk WD. R-spondin1, a novel intestinotrophic mitogen, ameliorates experimental colitis in mice. Gastroenterology. 2007 Apr;132(4):1331-43
Tomaselli S, Megiorni F, De Bernardo C, Felici A, Marrocco G, Maggiulli G, Grammatico B, Remotti D, Saccucci P, Valentini F, Mazzilli MC, Majore S, Grammatico P. Syndromic true hermaphroditism due to an R-spondin1 (RSPO1) homozygous mutation. Hum Mutat. 2008 Feb;29(2):220-6
This article should be referenced as such:
Blaydon D. RSPO1 (R-spondin homolog (Xenopus laevis)). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):364-366.
Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 367
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
UBE2C (ubiquitin-conjugating enzyme E2C) Pierlorenzo Pallante, Maria Teresa Berlingieri, Alfredo Fusco
Istituto di Endocrinologia ed Oncologia Sperimentale del CNR c/o Dipartimento di Biologia e Patologia Cellulare e Molecolare, Facolta di Medicina e Chirurgia, Universita degli Studi di Napoli "Federico II", via Pansini 5, 80131 Napoli, Italy (PP, MTB, AF)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/UBE2CID44079ch20q13.html DOI: 10.4267/2042/44473
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: UBCH10; UBE2C-PEN; UbcH10; dJ447F3.2; LOC11065
HGNC (Hugo): UBE2C
Location: 20q13.12
Local order: CENTROMERE---WFDC3-DNTTIP1-UBE2C-TNNC2-SNX21-ACOT8---TELOMERE.
Note: UbcH10 catalyzes the covalent attachment of ubiquitin to target proteins. It is required for the destruction of mitotic cyclins.
DNA/RNA Description UBE2C is located on chromosome 20, at 20q13.12 according to Entrez Gene. In AceView, it covers 4.40 kb, from 43874623 to 43879017 on the direct strand.
Transcription There are 6 representative transcripts annotated in RefSeq database, but, according to AceView, Homo sapiens cDNA sequences in GenBank support at least 13 spliced variants. Isoform 1, the longest isoform, is composed of 6 coding exons of varying lengths, separated by introns: NM_007019.2 (mRNA-ubiquitin-conjugating enzyme E2C): mRNA product length: 823.
Protein Description The UbcH10 gene encodes a member of the E2 ubiquitin-conjugating enzyme family that is involved in the ubiquitin dependent proteolysis. In this pathway, ubiquitin-activating enzyme (E1), ubiquitin-conjugating enzyme (E2), together with ubiquitin ligase (E3), catalyze the covalent attachment of ubiquitin to target proteins, targeting them for degradation mediated by the 26S proteasome. The full-length UbcH10 contains 179 residues for a 19.6 kDa weight. It belongs to the class III Ubc proteins that are characterized by an NH2-terminal extension followed by the "core" Ubc fold. Like all E2 enzymes, UbcH10 contains an active site cysteine residue (position 114) that is crucial for the formation of the ubiquitin-thiolester. Alteration of this residue C(114)S strongly inhibits ubiquitination of cyclin A and Cyclin B confering a dominant-negative phenotype. Levels of UbcH10 are modulated by autoubiquitination. This process is dependent on a motif, the "destruction box" [Arg-X-X-Leu-X-X-(Leu/Ile)-X-Asp] recognized by the mitotic-specific ubiquitination machinery. A study suggests that a destruction box is present in the UbcH10 sequence and includes residues 129-132 (Arg-Thr-Ile-Leu). Interestingly an SNP is reported for the residue 129 (refSNP ID: rs7352110, alleles A/G, Arg>Gly).

UBE2C (ubiquitin-conjugating enzyme E2C) Pallate P, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 368
This would be important since any change in the putative destruction box could stabilize UbcH10 against destruction.
Expression UbcH10 mRNA and protein are expressed at low levels in most adult normal tissues. In contrast, UbcH10 mRNA and protein are highly expressed in tumor tissues. Moreover, UbcH10 protein levels fluctuate during the cell cycle being abundant during M and early G1 phases, but decreasing in late G1, S and G2 phases.
Localisation Nucleoplasm. Cytosol.
Function UbcH10 is crucial for cell cycle progression during the G2/M phase, since its function is required for the destruction of mitotic cyclins and other mitosis-related substrates. UbcH10 interacts with the multiprotein complex APC (anaphase-promoting complex), which has E3 ubiquitin ligase activity, and targets for destruction substrates from the preceding mitosis (cyclin A, cyclin B, securin, geminin). Once these target proteins have been degraded, UbcH10 adds ubiquitins to itself, triggering its own destruction. As a result, the absence of UbcH10 allows the accumulation of cyclin A, which in turn contributes to the APC inactivation, providing a molecular switch that allows cells to proceed from cell division to a new round of DNA duplication. Hence, the function of UbcH10 is strictly linked to the progression of cell cycle through the M phase and the coupling of mitosis to S-phase entry via autonomous regulation of the anaphase-promoting complex.
Implicated in Human cancers Note Several studies suggest a possible use of UbcH10 investigation (together with other molecular markers) in early detection of cancer. Other studies suggest that inhibition of UbcH10 could have a therapeutic potential in cancer treatment.
Disease UbcH10 overexpression was reported in a number of human cancer cell lines and primary tumors and expression data strongly support an association between high UbcH10 expression and a poor tumor differentiation. Expression studies have also shown a correlation between UbcH10 overexpression and the proliferation status since there is a good association with the proliferation marker Ki-67/MIB1. It was found overexpressed in lung carcinoma ( squamous and adenocarcinoma, poorly versus well differentiated), bladder carcinoma (grade 3 versus grade 2), prostate carcinoma (metastatic versus primary), gastric adenocarcinoma cervical, esophageal adenocarcinoma (adenocarcinoma versus Barrett's metaplasia), breast cancer (grade 3 versus grade 1, malignant versus benign neoplastic lesions), brain (astrocytomas versus low-grade tumors or normal controls), medulloblastoma, ovarian carcinoma (grade 3 versus grade 1 and 2), thyroid carcinoma (poorly versus well differentiated), adrenocortical gland, Wilms tumor (relapsed versus relapse-free) hepatocellular carcinoma (correlation with higher frequencies of invasion to capsular formation, invasion to portal vein and tumor de-differentiation). Several expression analysis and functional studies have also shown that UbcH10 resulted up-regulated in experimental model of carcinogenesis, that its overexpression leads to the acquisition of a malignant phenotype and that its knockdown successfully resulted in growth arrest.
Prognosis It was seen that UbcH10 overexpression is a negative predictor of clinical outcome in patients affected by ovarian and hepatocellular carcinoma. Therefore, UbcH10 has been suggested as a helpful prognostic indicator for ovarian and hepatocellular carcinoma patients.
Oncogenesis 20q13.1 chromosomal region is frequently associated with genomic amplification in different malignant neoplasias and amplification of UbcH10 locus has been reported in the case of gastroesophageal carcinomas, colorectal carcinomas with liver metastases, cervical cancers, ovarian carcinomas, gliomas and culture cell lines obtained from anaplastic thyroid carcinomas.

UBE2C (ubiquitin-conjugating enzyme E2C) Pallate P, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 369
References Yu H, King RW, Peters JM, Kirschner MW. Identification of a novel ubiquitin-conjugating enzyme involved in mitotic cyclin degradation. Curr Biol. 1996 Apr 1;6(4):455-66
Townsley FM, Aristarkhov A, Beck S, Hershko A, Ruderman JV. Dominant-negative cyclin-selective ubiquitin carrier protein E2-C/UbcH10 blocks cells in metaphase. Proc Natl Acad Sci U S A. 1997 Mar 18;94(6):2362-7
Tang Z, Li B, Bharadwaj R, Zhu H, Ozkan E, Hakala K, Deisenhofer J, Yu H. APC2 Cullin protein and APC11 RING protein comprise the minimal ubiquitin ligase module of the anaphase-promoting complex. Mol Biol Cell. 2001 Dec;12(12):3839-51
Criqui MC, de Almeida Engler J, Camasses A, Capron A, Parmentier Y, Inzé D, Genschik P. Molecular characterization of plant ubiquitin-conjugating enzymes belonging to the UbcP4/E2-C/UBCx/UbcH10 gene family. Plant Physiol. 2002 Nov;130(3):1230-40
Lin Y, Hwang WC, Basavappa R. Structural and functional analysis of the human mitotic-specific ubiquitin-conjugating enzyme, UbcH10. J Biol Chem. 2002 Jun 14;277(24):21913-21
Okamoto Y, Ozaki T, Miyazaki K, Aoyama M, Miyazaki M, Nakagawara A. UbcH10 is the cancer-related E2 ubiquitin-conjugating enzyme. Cancer Res. 2003 Jul 15;63(14):4167-73
Dairkee SH, Ji Y, Ben Y, Moore DH, Meng Z, Jeffrey SS. A molecular 'signature' of primary breast cancer cultures; patterns resembling tumor tissue. BMC Genomics. 2004 Jul 19;5(1):47
Rape M, Kirschner MW. Autonomous regulation of the anaphase-promoting complex couples mitosis to S-phase entry. Nature. 2004 Dec 2;432(7017):588-95
Wagner KW, Sapinoso LM, El-Rifai W, Frierson HF, Butz N, Mestan J, Hofmann F, Deveraux QL, Hampton GM. Overexpression, genomic amplification and therapeutic potential of inhibiting the UbcH10 ubiquitin conjugase in human carcinomas of diverse anatomic origin. Oncogene. 2004 Aug 26;23(39):6621-9
Bredel M, Bredel C, Juric D, Harsh GR, Vogel H, Recht LD, Sikic BI. Functional network analysis reveals extended gliomagenesis pathway maps and three novel MYC-interacting genes in human gliomas. Cancer Res. 2005 Oct 1;65(19):8679-89
Israeli O, Goldring-Aviram A, Rienstein S, Ben-Baruch G, Korach J, Goldman B, Friedman E. In silico chromosomal clustering of genes displaying altered expression patterns in ovarian cancer. Cancer Genet Cytogenet. 2005 Jul 1;160(1):35-42
Kobirumaki F, Miyauchi Y, Fukami K, Tanaka H. A novel UbcH10-binding protein facilitates the ubiquitinylation of cyclin B in vitro. J Biochem. 2005 Feb;137(2):133-9
Pallante P, Berlingieri MT, Troncone G, Kruhoffer M, Orntoft TF, Viglietto G, Caleo A, Migliaccio I, Decaussin-Petrucci M, Santoro M, Palombini L, Fusco A. UbcH10 overexpression may represent a marker of anaplastic thyroid carcinomas. Br J Cancer. 2005 Aug 22;93(4):464-71
Chen CC, Chang TW, Chen FM, Hou MF, Hung SY, Chong IW, Lee SC, Zhou TH, Lin SR. Combination of multiple mRNA markers (PTTG1, Survivin, UbcH10 and TK1) in the diagnosis of Taiwanese patients with breast cancer by membrane array. Oncology. 2006;70(6):438-46
de Gramont A, Ganier O, Cohen-Fix O. Before and after the spindle assembly checkpoint--an APC/C point of view. Cell Cycle. 2006 Sep;5(18):2168-71
Lin J, Raoof DA, Wang Z, Lin MY, Thomas DG, Greenson JK, Giordano TJ, Orringer MB, Chang AC, Beer DG, Lin L. Expression and effect of inhibition of the ubiquitin-conjugating enzyme E2C on esophageal adenocarcinoma. Neoplasia. 2006 Dec;8(12):1062-71
Peters JM. The anaphase promoting complex/cyclosome: a machine designed to destroy. Nat Rev Mol Cell Biol. 2006 Sep;7(9):644-56
Rape M, Reddy SK, Kirschner MW. The processivity of multiubiquitination by the APC determines the order of substrate degradation. Cell. 2006 Jan 13;124(1):89-103
Takahashi Y, Ishii Y, Nishida Y, Ikarashi M, Nagata T, Nakamura T, Yamamori S, Asai S. Detection of aberrations of ubiquitin-conjugating enzyme E2C gene (UBE2C) in advanced colon cancer with liver metastases by DNA microarray and two-color FISH. Cancer Genet Cytogenet. 2006 Jul 1;168(1):30-5
Zirn B, Hartmann O, Samans B, Krause M, Wittmann S, Mertens F, Graf N, Eilers M, Gessler M. Expression profiling of Wilms tumors reveals new candidate genes for different clinical parameters. Int J Cancer. 2006 Apr 15;118(8):1954-62
Berlingieri MT, Pallante P, Guida M, Nappi C, Masciullo V, Scambia G, Ferraro A, Leone V, Sboner A, Barbareschi M, Ferro A, Troncone G, Fusco A. UbcH10 expression may be a useful tool in the prognosis of ovarian carcinomas. Oncogene. 2007 Mar 29;26(14):2136-40
Berlingieri MT, Pallante P, Sboner A, Barbareschi M, Bianco M, Ferraro A, Mansueto G, Borbone E, Guerriero E, Troncone G, Fusco A. UbcH10 is overexpressed in malignant breast carcinomas. Eur J Cancer. 2007 Dec;43(18):2729-35
Ieta K, Ojima E, Tanaka F, Nakamura Y, Haraguchi N, Mimori K, Inoue H, Kuwano H, Mori M. Identification of overexpressed genes in hepatocellular carcinoma, with special reference to ubiquitin-conjugating enzyme E2C gene expression. Int J Cancer. 2007 Jul 1;121(1):33-8
Lee JJ, Foukakis T, Hashemi J, Grimelius L, Heldin NE, Wallin G, Rudduck C, Lui WO, Höög A, Larsson C. Molecular cytogenetic profiles of novel and established human anaplastic thyroid carcinoma models. Thyroid. 2007 Apr;17(4):289-301
Narayan G, Bourdon V, Chaganti S, Arias-Pulido H, Nandula SV, Rao PH, Gissmann L, Dürst M, Schneider A, Pothuri B, Mansukhani M, Basso K, Chaganti RS, Murty VV. Gene dosage alterations revealed by cDNA microarray analysis in cervical cancer: identification of candidate amplified and overexpressed genes. Genes Chromosomes Cancer. 2007 Apr;46(4):373-84
Reddy SK, Rape M, Margansky WA, Kirschner MW. Ubiquitination by the anaphase-promoting complex drives spindle checkpoint inactivation. Nature. 2007 Apr 19;446(7138):921-5
Stegmeier F, Rape M, Draviam VM, Nalepa G, Sowa ME, Ang XL, McDonald ER 3rd, Li MZ, Hannon GJ, Sorger PK, Kirschner MW, Harper JW, Elledge SJ. Anaphase initiation
is regulated by antagonistic ubiquitination and deubiquitination activities. Nature. 2007 Apr 19;446(7138):876-81
Walker G, MacLeod K, Williams AR, Cameron DA, Smyth JF, Langdon SP. Estrogen-regulated gene expression predicts response to endocrine therapy in patients with ovarian cancer. Gynecol Oncol. 2007 Sep;106(3):461-8
Campone M, Campion L, Roché H, Gouraud W, Charbonnel C, Magrangeas F, Minvielle S, Genève J, Martin AL, Bataille R, Jézéquel P. Prediction of metastatic relapse in node-positive breast cancer: establishment of a clinicogenomic model after

UBE2C (ubiquitin-conjugating enzyme E2C) Pallate P, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 370
FEC100 adjuvant regimen. Breast Cancer Res Treat. 2008 Jun;109(3):491-501
Jiang L, Huang CG, Lu YC, Luo C, Hu GH, Liu HM, Chen JX, Han HX. Expression of ubiquitin-conjugating enzyme E2C/UbcH10 in astrocytic tumors. Brain Res. 2008 Mar 27;1201:161-6
This article should be referenced as such:
Pallate P, Berlingieri MT, Fusco A. UBE2C (ubiquitin-conjugating enzyme E2C). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):367-370.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 371
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
WNT5A (wingless-type MMTV integration site family, member 5A) Masaru Katoh
Genetics and Cell Biology Section, National Cancer Center Research Institute, 5-1-1 Tsukiji, Chuo-ku, Tokyo 104-0045, Japan (MK)
Published in Atlas Database: June 2008
Online updated version : http://AtlasGeneticsOncology.org/Genes/WNT5AID42825ch3p14.html DOI: 10.4267/2042/44474
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: WNT-5A
HGNC (Hugo): WNT5A
Location: 3p14.3
Local order: CACNA2D3 - WNT5A - ERC2.
Note: WNT family ligand. WNT family members with conserved 22 or 24 Cys residues are secreted-type glycoproteins, which are implicated in embryogenesis and carcinogenesis. Nineteen WNT family genes exist within the human genome.
DNA/RNA Note WNT5A gene at chromosome 3p14.3 and WNT5B gene at chromosome 12p13.33 are paralogs within the human genome.
Description WNT5A gene consists of 5 exons. First methionine is located in exon 1, while stop codon in exon 5. dbSNP rs655731, located within exon 5 of the human WNT5A gene, is a synonymous SNP corresponding to codon 263.
Transcription WNT5A is preferentially upregulated in gastric cancer, and melanoma, but downregulated in breast cancer,
colorectal cancer, and acute lymphocytic leukemia. Wnt5a is upregulated by IL6 family cytokines through gp130 in cultured cardiomyocytes, by TGFbeta in mammary epithelial cells, and by TNFalpha in gastric cancer cells. WNT5A upregulation in primary tumor is in part due to stromal expression based on tumor-stromal interaction, while WNT5A downregulation in primary tumor is in part due to epigenetic silencing induced by promoter CpG hypermethylation.
Protein Description Mature WNT5A protein with conserved Cys residues is a secreted-type glycoprotein.
Expression WNT5A mRNA is relatively abundantly expressed in salivary gland, bladder, uterus, placenta, and fetal kidney.
Localisation Naive WNT5A protein is synthesized in the endoplasmic reticulum. Mature WNT5A protein with lipid modifications and glycosylations enters the trans-Golgi network for secretion from the cell surface.
Schematic representation of WNT5A gene.

WNT5A (wingless-type MMTV integration site family, member 5A) Katoh M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 372
Function WNT5A signals are transduced to the canonical and non-canonical WNT signaling cascades. WNT5A signaling through Frizzled-4 (FZD4) or FZD5 receptor and LRP5 or LRP6 co-receptor leads to the stabilization and nuclear accumulation of beta-catenin for the transcriptional activation of target genes, such as MYC, CCND1, and FGF20. On the other hand, WNT5A signaling through Frizzled family receptor or ROR1 or ROR2 co-receptor leads to the activation of the non-canonical WNT signaling cascades, such as DAG - PKC, IP3 - NFAT, or IP3 - NLK signaling cascades. WNT5A-PKC signaling promotes invasion and metastasis of tumors through SNAI1 (Snail)-mediated epithelial-to-mesenchymal transition (EMT), while WNT5A-NLK signaling suppresses carcinogenesis through inhibition of the canonical WNT signaling cascade. Expression of WNT5A is associated with metastatic or aggressive phenotype in gastric cancer, melanoma, and osteosarcoma, but is associated with non-aggressive or better prognostic phenotype in breast cancer, colorectal cancer, and acute lymphocytic leukemia. Together these facts indicate that WNT5A induces oncogenic as well as tumor suppressive functions in a context-dependent manner.
Homology Human WNT5A shows 98.7% total amino-acid identity with rodent Wnt5a, indicating that mammalian WNT5A orthologs are highly conserved. Among 19 WNT family members, WNT5A is most homologous to WNT5B.
Mutations Note WNT5A gene is located at human chromosome 3p14.3 around the susceptible locus of Zimmermann-Laband Syndrome; however, mutation of WNT5A gene has not been detected.
Germinal Wnt5a knockout mice show smaller somites and shortened presomitic mesoderm, abnormalities in the lungs with the foreshortened trachea, dysplasia of genitals, and ventricular septal defects.
Implicated in Melanoma Prognosis Poor prognosis.
Gastric cancer Prognosis Poor prognosis.
Osteosarcoma Prognosis
Poor prognosis
Breast cancer Prognosis Better prognosis.
Colorectal cancer Prognosis Better prognosis.
Acute lymphocytic leukemia Prognosis Better prognosis.
References Clark CC, Cohen I, Eichstetter I, Cannizzaro LA, McPherson JD, Wasmuth JJ, Iozzo RV. Molecular cloning of the human proto-oncogene Wnt-5A and mapping of the gene (WNT5A) to chromosome 3p14-p21. Genomics. 1993 Nov;18(2):249-60
Dealy CN, Roth A, Ferrari D, Brown AM, Kosher RA. Wnt-5a and Wnt-7a are expressed in the developing chick limb bud in a manner suggesting roles in pattern formation along the proximodistal and dorsoventral axes. Mech Dev. 1993 Oct;43(2-3):175-86
Moon RT, Campbell RM, Christian JL, McGrew LL, Shih J, Fraser S. Xwnt-5A: a maternal Wnt that affects morphogenetic movements after overexpression in embryos of Xenopus laevis. Development. 1993 Sep;119(1):97-111
Wong GT, Gavin BJ, McMahon AP. Differential transformation of mammary epithelial cells by Wnt genes. Mol Cell Biol. 1994 Sep;14(9):6278-86
Iozzo RV, Eichstetter I, Danielson KG. Aberrant expression of the growth factor Wnt-5A in human malignancy. Cancer Res. 1995 Aug 15;55(16):3495-9
Lejeune S, Huguet EL, Hamby A, Poulsom R, Harris AL. Wnt5a cloning, expression, and up-regulation in human primary breast cancers. Clin Cancer Res. 1995 Feb;1(2):215-22
Austin TW, Solar GP, Ziegler FC, Liem L, Matthews W. A role for the Wnt gene family in hematopoiesis: expansion of multilineage progenitor cells. Blood. 1997 May 15;89(10):3624-35
Bui TD, Zhang L, Rees MC, Bicknell R, Harris AL. Expression and hormone regulation of Wnt2, 3, 4, 5a, 7a, 7b and 10b in normal human endometrium and endometrial carcinoma. Br J Cancer. 1997;75(8):1131-6
He X, Saint-Jeannet JP, Wang Y, Nathans J, Dawid I, Varmus H. A member of the Frizzled protein family mediating axis induction by Wnt-5A. Science. 1997 Mar 14;275(5306):1652-4
Slusarski DC, Yang-Snyder J, Busa WB, Moon RT. Modulation of embryonic intracellular Ca2+ signaling by Wnt-5A. Dev Biol. 1997 Feb 1;182(1):114-20
He TC, Sparks AB, Rago C, Hermeking H, Zawel L, da Costa LT, Morin PJ, Vogelstein B, Kinzler KW. Identification of c-MYC as a target of the APC pathway. Science. 1998 Sep 4;281(5382):1509-12
Tetsu O, McCormick F. Beta-catenin regulates expression of cyclin D1 in colon carcinoma cells. Nature. 1999 Apr 1;398(6726):422-6
Yamaguchi TP, Bradley A, McMahon AP, Jones S. A Wnt5a pathway underlies outgrowth of multiple structures in the vertebrate embryo. Development. 1999 Mar;126(6):1211-23

WNT5A (wingless-type MMTV integration site family, member 5A) Katoh M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 373
Jönsson M, Dejmek J, Bendahl PO, Andersson T. Loss of Wnt-5a protein is associated with early relapse in invasive ductal breast carcinomas. Cancer Res. 2002 Jan 15;62(2):409-16
Saitoh T, Katoh M. Expression and regulation of WNT5A and WNT5B in human cancer: up-regulation of WNT5A by TNFalpha in MKN45 cells and up-regulation of WNT5B by beta-estradiol in MCF-7 cells. Int J Mol Med. 2002 Sep;10(3):345-9
Saitoh T, Mine T, Katoh M. Frequent up-regulation of WNT5A mRNA in primary gastric cancer. Int J Mol Med. 2002 May;9(5):515-9
Weeraratna AT, Jiang Y, Hostetter G, Rosenblatt K, Duray P, Bittner M, Trent JM. Wnt5a signaling directly affects cell motility and invasion of metastatic melanoma. Cancer Cell. 2002 Apr;1(3):279-88
Carr KM, Bittner M, Trent JM. Gene-expression profiling in human cutaneous melanoma. Oncogene. 2003 May 19;22(20):3076-80
Oishi I, Suzuki H, Onishi N, Takada R, Kani S, Ohkawara B, Koshida I, Suzuki K, Yamada G, Schwabe GC, Mundlos S, Shibuya H, Takada S, Minami Y. The receptor tyrosine kinase Ror2 is involved in non-canonical Wnt5a/JNK signalling pathway. Genes Cells. 2003 Jul;8(7):645-54
Fujio Y, Matsuda T, Oshima Y, Maeda M, Mohri T, Ito T, Takatani T, Hirata M, Nakaoka Y, Kimura R, Kishimoto T, Azuma J. Signals through gp130 upregulate Wnt5a and contribute to cell adhesion in cardiac myocytes. FEBS Lett. 2004 Aug 27;573(1-3):202-6
Chamorro MN, Schwartz DR, Vonica A, Brivanlou AH, Cho KR, Varmus HE. FGF-20 and DKK1 are transcriptional targets of beta-catenin and FGF-20 is implicated in cancer and development. EMBO J. 2005 Jan 12;24(1):73-84
Gregorieff A, Pinto D, Begthel H, Destrée O, Kielman M, Clevers H. Expression pattern of Wnt signaling components in the adult intestine. Gastroenterology. 2005 Aug;129(2):626-38
Katoh M. WNT/PCP signaling pathway and human cancer (review). Oncol Rep. 2005 Dec;14(6):1583-8
Katoh M, Katoh M. Comparative genomics on Wnt5a and Wnt5b genes. Int J Mol Med. 2005 Apr;15(4):749-53
Dejmek J, Säfholm A, Kamp Nielsen C, Andersson T, Leandersson K. Wnt-5a/Ca2+-induced NFAT activity is counteracted by Wnt-5a/Yes-Cdc42-casein kinase 1alpha signaling in human mammary epithelial cells. Mol Cell Biol. 2006 Aug;26(16):6024-36
Mikels AJ, Nusse R. Purified Wnt5a protein activates or inhibits beta-catenin-TCF signaling depending on receptor context. PLoS Biol. 2006 Apr;4(4):e115
Pukrop T, Klemm F, Hagemann T, Gradl D, Schulz M, Siemes S, Trümper L, Binder C. Wnt 5a signaling is critical for macrophage-induced invasion of breast cancer cell lines. Proc Natl Acad Sci U S A. 2006 Apr 4;103(14):5454-9
Dissanayake SK, Wade M, Johnson CE, O'Connell MP, Leotlela PD, French AD, Shah KV, Hewitt KJ, Rosenthal DT, Indig FE, Jiang Y, Nickoloff BJ, Taub DD, Trent JM, Moon RT, Bittner M, Weeraratna AT. The Wnt5A/protein kinase C pathway mediates motility in melanoma cells via the inhibition of metastasis suppressors and initiation of an epithelial to mesenchymal transition. J Biol Chem. 2007 Jun 8;282(23):17259-71
Katoh M, Katoh M. STAT3-induced WNT5A signaling loop in embryonic stem cells, adult normal tissues, chronic persistent inflammation, rheumatoid arthritis and cancer (Review). Int J Mol Med. 2007 Feb;19(2):273-8
Roarty K, Serra R. Wnt5a is required for proper mammary gland development and TGF-beta-mediated inhibition of ductal growth. Development. 2007 Nov;134(21):3929-39
Zuidervaart W, Pavey S, van Nieuwpoort FA, Packer L, Out C, Maat W, Jager MJ, Gruis NA, Hayward NK. Expression of Wnt5a and its downstream effector beta-catenin in uveal melanoma. Melanoma Res. 2007 Dec;17(6):380-6
Cheng CW, Yeh JC, Fan TP, Smith SK, Charnock-Jones DS. Wnt5a-mediated non-canonical Wnt signalling regulates human endothelial cell proliferation and migration. Biochem Biophys Res Commun. 2008 Jan 11;365(2):285-90
Fukuda T, Chen L, Endo T, Tang L, Lu D, Castro JE, Widhopf GF 2nd, Rassenti LZ, Cantwell MJ, Prussak CE, Carson DA, Kipps TJ. Antisera induced by infusions of autologous Ad-CD154-leukemia B cells identify ROR1 as an oncofetal antigen and receptor for Wnt5a. Proc Natl Acad Sci U S A. 2008 Feb 26;105(8):3047-52
Pilarsky C, Ammerpohl O, Sipos B, Dahl E, Hartmann A, Wellmann A, Braunschweig T, Löhr M, Jesnowski R, Friess H, Wente MN, Kristiansen G, Jahnke B, Denz A, Rückert F, Schackert HK, Klöppel G, Kalthoff H, Saeger HD, Grützmann R. Activation of Wnt signalling in stroma from pancreatic cancer identified by gene expression profiling. J Cell Mol Med. 2008 Dec;12(6B):2823-35
Witze ES, Litman ES, Argast GM, Moon RT, Ahn NG. Wnt5a control of cell polarity and directional movement by polarized redistribution of adhesion receptors. Science. 2008 Apr 18;320(5874):365-9
Ying J, Li H, Yu J, Ng KM, Poon FF, Wong SC, Chan AT, Sung JJ, Tao Q. WNT5A exhibits tumor-suppressive activity through antagonizing the Wnt/beta-catenin signaling, and is frequently methylated in colorectal cancer. Clin Cancer Res. 2008 Jan 1;14(1):55-61
This article should be referenced as such:
Katoh M. WNT5A (wingless-type MMTV integration site family, member 5A). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):371-373.

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 374
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Nasal T cell lymphoma Antonio Cuneo, Francesco Cavazzini, Gian Matteo Rigolin
Hematology Section, Dept. Of Biomedical Sciences, University of Ferrara, Ferrara Italy (AC, FC, GMR)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/NasalTCellLymphomID2100.html DOI: 10.4267/2042/44475
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Alias: Angiocentric T-cell lymphoma; Polymorphic reticulosis; Lethal midline granuloma
Clinics and pathology Disease Extranodal NH/T-cell lymphoma, nasal type.
Phenotype/cell stem origin This lymphoma derives form the transformation of NK lymphocytes and, less frequently, T-lymphocytes.
Epidemiology It is seen most frequently in China, Japan, Korea and other Asian countries and in Central America.
Clinics Middle aged adults are most frequently affected, with slight male predominance. The disease involves the nasal cavity and may spread to the pharynx, palate and larinx. Less frequently, orbital and cranial nerve involvement was described. Spreading to the skin, soft tissue and gastrointestinal tract may occur. Bone marrow involvement is unusual at presentation. Hemophagocytic syndrome was described in some cases. The tumor is locally invasive and destructive (Liang et al., 2006).
Pathology The cellular infiltrate is polymorphic, typically associated with an angioinvase growth pattern, with consequent angiodestruction, ischemia and tissue necrosis. Neoplastic cells are CD56 positive, with negativity for surface CD3. The TCR gene is usually germline, even though some cases with a clonally rearranged TCR were reported (Yoon et al., 1999).
Epstein-Barr virus infection in this lymphoma was well documented by molecular methods (Chiang et al., 1997).
Treatment Combination regimens such as CHOP or other aggressive schedules followed by local radiotherapy are the mainstay of treatment. Autologous bone marrow transplantation has been used.
Prognosis Prognosis is severe, with less than 50% of the patients achieving durable complete response after intensive chemotherapy and local radiotherapy. The disseminated forms of the disease are almost uniformly fatal.
Cytogenetics Cytogenetics morphological Three out of seven cases studied by Wong et al (1997), including one nasal, one extranasal and one leukaemic form, showed a common region of deletion at 6q21-q25, suggesting that this may be a nonrandom chromosomal aberration. Other non-random abnormalities include +X, i(1q), i(7q), +8, del(13q), del(17p), i(17q), and 11q23 rearrangement (Wong et al., 1999).
Cytogenetics molecular P73 gene methylation was described in 94% of the cases; other methylated genes included hMLH1 (63%), p16 (63%), p15 (48%), and RAR beta (47%) (Siu et al., 2002). P53 gene overexpression was documented (Quintanilla-Martinez et al., 1999). Comparative genomic hybridization studies identified del(6q), del(13q),del (17p), del (1p), del(12q), and partial gain of Xp, 2p, 10q as recurrent abnormalities (Siu et al., 1999; Ko et al., 2001). Some of these

Nasal T cell lymphoma Cuneo A, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 375
abnormalities (i.e. 17p deletion and 1p deletion) may be associated the aggressive leukemic variant of the disease (Nakashima et al., 2005). Genome-wide array-based comparative genomic hybridization identified recurrent regions of imbalances: gain of 2q and loss of 6q16-27,11q22-23, 5p14, 5q34, 1p36, 2p16, 4q12, 4q31 (Nakashima et al., 2005).
References Chiang AK, Chan AC, Srivastava G, Ho FC. Nasal T/natural killer (NK)-cell lymphomas are derived from Epstein-Barr virus-infected cytotoxic lymphocytes of both NK- and T-cell lineage. Int J Cancer. 1997 Nov 4;73(3):332-8
Wong KF, Chan JK, Kwong YL. Identification of del(6)(q21q25) as a recurring chromosomal abnormality in putative NK cell lymphoma/leukaemia. Br J Haematol. 1997 Sep;98(4):922-6
Quintanilla-Martinez L, Franklin JL, Guerrero I, Krenacs L, Naresh KN, Rama-Rao C, Bhatia K, Raffeld M, Magrath IT. Histological and immunophenotypic profile of nasal NK/T cell lymphomas from Peru: high prevalence of p53 overexpression. Hum Pathol. 1999 Jul;30(7):849-55
Siu LL, Wong KF, Chan JK, Kwong YL. Comparative genomic hybridization analysis of natural killer cell lymphoma/leukemia. Recognition of consistent patterns of genetic alterations. Am J Pathol. 1999 Nov;155(5):1419-25
Wong KF, Zhang YM, Chan JK. Cytogenetic abnormalities in natural killer cell lymphoma/leukaemia--is there a consistent pattern? Leuk Lymphoma. 1999 Jul;34(3-4):241-50
Yoon TY, Lee HT, Chang SH. Nasal-type T/natural killer cell angiocentric lymphoma, Epstein-Barr virus-associated, and showing clonal T-cell receptor gamma gene rearrangement. Br J Dermatol. 1999 Mar;140(3):505-8
Ko YH, Choi KE, Han JH, Kim JM, Ree HJ. Comparative genomic hybridization study of nasal-type NK/T-cell lymphoma. Cytometry. 2001 Apr 15;46(2):85-91
Siu LL, Chan JK, Wong KF, Kwong YL. Specific patterns of gene methylation in natural killer cell lymphomas : p73 is consistently involved. Am J Pathol. 2002 Jan;160(1):59-66
Nakashima Y, Tagawa H, Suzuki R, Karnan S, Karube K, Ohshima K, Muta K, Nawata H, Morishima Y, Nakamura S, Seto M. Genome-wide array-based comparative genomic hybridization of natural killer cell lymphoma/leukemia: different genomic alteration patterns of aggressive NK-cell leukemia and extranodal Nk/T-cell lymphoma, nasal type. Genes Chromosomes Cancer. 2005 Nov;44(3):247-55
Liang RL.. Nasal T7NK-cell lymphoma. In: Canellos GP, Lister TA, Young BD: The Lymphomas 2nd edition. Sanuders Elsevier, Philadelphia, 2006, pp 451-455
This article should be referenced as such:
Cuneo A, Cavazzini F, Rigolin GM. Nasal T cell lymphoma. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):374-375.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 376
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(14;14)(q11;q32) CEBPE/IGH, inv(14)(q11q32) CEBPE/IGH Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t1414q11q32CEBPEIGHID1438.html DOI: 10.4267/2042/44476
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note This chromosome anomaly should not be confused with the t(14;14)(q11;q32)/inv(14)(q11q32) found in T-cell diseases, which implicates TCR alpha or TCR delta (14q11) and TCL1A (14q32).
Clinics and pathology Disease CD10+ acute lymphoblastic leukaemia (B-ALL).
Epidemiology Only 4 cases to date of t(14;14)(q11;q32)/inv(14)(q11q32) with CEBPE and IGH involvements (Akasaka et al., 2007). Five other cases of t(14;14)(q11;q32)/inv(14)(q11q32) in B-cell leukemias are known (Denny et al., 1986; Speleman et al., 1991; Chervinsky et al., 1995; Wong et al., 1995; Thomas et al., 2001), but without proof that CEBPE was involved. As a matter of fact, a t(4;11)(q21;q23) was found in 2 of these cases, and a t(8;14)(q24;q32) in another case; this latter group is certainly heterogeneous.
Clinics The four patients were male patients, aged 15, 25, 45, and 45 years, with a WBC under 50 x 109/l. Survival is available only for two cases: 19 mths+ and 48 months+, resembling the relatively fair survival of
patients with a t(8;14)(q11;q32) CEBPD/IGH translocation. One case was a Down syndrome patient; this may not be anecdotical, since more than 1/4 of t(8;14)(q11;q32) case are also Down syndrome patients.
Genes involved and proteins CEBPE Location 14q11
Protein DNA-binding protein. CCAAT enhancer-binding protein (CEBP) transcription factors are a family of 6 multifunctional basic leucine zipper (bZIP) transcription factors. The 5 other CEBPs are: CEBPA (19q13), CEBPB (20q13), CEBPD (8q11), CEBPG (19q13), all four equally implicated in leukemias, and DDIT3/CHOP/CEBP zeta (12q13), so far known to be involved in solid tumours (liposarcoma). These transcription factors play a key role in cellular differentiation, in particular in the control of myeloid differentiation. CEBPE is composed of an N-term transactivation domain, a negative regulatory domain, a DNA-binding basic motif, and a leucine-zipper domain in C-term (Ramji et al., 2002; Nerlov et al., 2007).
IgH Location 14q32

t(14;14)(q11;q32) CEBPE/IGH, inv(14)(q11q32) CEBPE/IGH Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 377
Result of the chromosomal anomaly Fusion protein Oncogenesis Overexpression of the CEBP gene.
References Denny CT, Hollis GF, Hecht F, Morgan R, Link MP, Smith SD, Kirsch IR. Common mechanism of chromosome inversion in B- and T-cell tumors: relevance to lymphoid development. Science. 1986 Oct 10;234(4773):197-200
Speleman F, Mangelschots K, Vercruyssen M, Dal Cin P, Aventin A, Offner F, Laureys G, Van den Berghe H, Leroy J. Analysis of whole-arm translocations in malignant blood cells by nonisotopic in situ hybridization. Cytogenet Cell Genet. 1991;56(1):14-7
Chervinsky DS, Grossi M, Kakati S, Block AW, Aplan PD. Concurrent presence of inv(14)(q11q32) and t(4;11)(q21;q23) in pre-B acute lymphoblastic leukemia. Genes Chromosomes Cancer. 1995 Mar;12(3):229-36
Wong KF, Kwong YL, Wong TK. Inversion 14q in acute lymphoblastic leukemia of B-lineage. Cancer Genet Cytogenet. 1995 Mar;80(1):72-4
Thomas X, Olteanu N, Charrin C, Lhéritier V, Magaud JP, Fiere D. Acute lymphoblastic leukemia in the elderly: The Edouard Herriot Hospital experience. Am J Hematol. 2001 Jun;67(2):73-83
Ramji DP, Foka P. CCAAT/enhancer-binding proteins: structure, function and regulation. Biochem J. 2002 Aug 1;365(Pt 3):561-75
Akasaka T, Balasas T, Russell LJ, Sugimoto KJ, Majid A, Walewska R, Karran EL, Brown DG, Cain K, Harder L, Gesk S, Martin-Subero JI, Atherton MG, Brüggemann M, Calasanz MJ, Davies T, Haas OA, Hagemeijer A, Kempski H, Lessard M, Lillington DM, Moore S, Nguyen-Khac F, Radford-Weiss I, Schoch C, Struski S, Talley P, Welham MJ, Worley H, Strefford JC, Harrison CJ, Siebert R, Dyer MJ. Five members of the CEBP transcription factor family are targeted by recurrent IGH translocations in B-cell precursor acute lymphoblastic leukemia (BCP-ALL). Blood. 2007 Apr 15;109(8):3451-61
Nerlov C. The C/EBP family of transcription factors: a paradigm for interaction between gene expression and proliferation control. Trends Cell Biol. 2007 Jul;17(7):318-24
This article should be referenced as such:
Huret JL. t(14;14)(q11;q32) CEBPE/IGH, inv(14)(q11q32) CEBPE/IGH. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):376-377.

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 378
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(14;19)(q32;q13) IGH/CEBPA Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t1419q32q13ALLID1335.html DOI: 10.4267/2042/44477
This article is an update of : Moorman AV, Robinson HM. t(14;19)(q32;q13) in acute lymphoblastic leukaemia. Atlas Genet Cytogenet Oncol Haematol 2004;8(4):326-327. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note This abnormality is cytogenetically identical but molecularly distinct from the t(14;19)(q32;q13) seen in chronic lymphoid leukaemia (CLL) and other chronic B-cell lymphoproliferative disorders, which results in the juxtaposition of BCL3 with IGH on the der(14) and subsequent over expression of the BCL3 protein.
G-banded metaphase showing the t(14;19)(q32;q13). The derivative chromosomes 14 and 19 are arrowed (bottom) G-banded karyogram showing the t(14;19)(q32;q13) and a add(15q) (top).
Clinics and pathology Disease Acute lymphoblastic leukaemia (ALL).
Phenotype/cell stem origin B-lineage immunophenotype and FAB L1, mostly CD10+: B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
Epidemiology Rare, with only 28 cases reported to date (Heerema et al., 1985; Prigogina et al., 1988; Pui et al., 1993; Andreasson et al., 2000; Robinson et al., 2004; Chapiro et al., 2006; Akasaka et al., 2007). The estimated incidence in childhood and adult ALL is <1%. Among the reported cases there appears to be a female pre-dominance (9M/19F) which is unusual for ALL. The age range of patients is 5 to 76 years with a median of 19 years. This abnormality is most often found in adolescents and young adults.
Clinics Typically, patients with this abnormality have low white cell count of 9/L, but 10% of patients present with a WBC above 50 x 109/L.
Prognosis It is difficult to assess the true prognosis of patients with this abnormality given its rarity, however initial data suggest that the prognosis is better than expected for patients of a similar age (see Figure 2).

t(14;19)(q32;q13) IGH/CEBPA Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 379
Cytogenetics Note This balanced translocation can usually be identified by G-banding alone. The breakpoint on chromosome 14 is consistently given as 14q32; however the breakpoint on chromosome 19 has, in the past, been more variably attributed, from q11 to q13. It is to be noted, however, that the gene involved on chromosome 19, CEBPA, lies at 38,482,776 bp from pter, very close to the q12 band limit.
Cytogenetics morphological The t(14;19) has been described as the sole abnormality in 12 out of 28 cases, and is more frequently accompanied by additional structural and/or numerical abnormalities; +21 (acquired) was found in three cases, +6 in two cases. A t(9;22)(q34;q11) was found in one case, a trisomy 8 in one case. This abnormality has been reported in a single case with Down syndrome. In a closely related translocation, the t(8;14)(q11;q32) with CEBPD/IGH involvement, more than 1/4 of cases were Down syndrome patients.
Genes involved and proteins Note The involvement of the IGH gene located at 14q32 has been demonstrated via FISH using the LSI IGH Dual Colour Break Apart Rearrangement Probe in all cases tested. Metaphase and interphase FISH using probes flanking the BCL3 gene have ruled out the involved of this gene; thus distinguishing it from the cytogenetically identical translocation t(14;19)(q32;q13) seen in CLL and other chronic B-cell lymphoproliferative disorders.
IgH Location 14q32
CEBPA Location 19q13
Note Alternatively, CEBPG can be involved instead of CEBPA (one case so far described). It is unknown if they bear the same prognosis, as they differ in their N-term.
DNA/RNA CEBPA is a single-exon gene, CEBPG also.
Protein DNA-binding protein. CCAAT enhancer-binding protein (CEBP) transcription factors are a family of 6 multifunctional basic leucine zipper (bZIP) transcription factors. The 4 other CEBPs are: CEBPB (20q13), CEBPD (8q11), CEBPE (8q11), all three equally implicated in leukemias, and DDIT3/CHOP/CEBP zeta (12q13), so far known to be involved in solid tumours (liposarcoma). These transcription factors play a key role in cellular differentiation, in particular in the control of myeloid differentiation. CEBPA is composed of an N-term transactivation domain, a negative regulatory domain, a DNA-binding basic motif, and a leucine-zipper domain in C-term. CEBPA mRNA is translated into two major proteins, p42CEBPA and p30CEBPA. The 30 kDa protein lacks the transactivating domain, and inhibits DNA binding and transactivation by p42CEBPA. CEBPA is essential for the lineage specific differentiation of myelocytic haematopoietic precursors into mature neutrophils. CEBPG only contains a DNA-binding basic motif, and a leucine-zipper domain (Ramji et al., 2002; Nerlov et al., 2007).
Germinal mutations CEBPA has been found mutated in a familial acute myeloid leukemia (Smith et al., 2004).
Somatic mutations 10% of acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS) cases exhibit a mutation in CEBPA, It seems to bear a good prognosis
Result of the chromosomal anomaly Fusion protein Oncogenesis Overexpression of the CEBP gene.
References Heerema NA, Palmer CG, Baehner RL. Karyotypic and clinical findings in a consecutive series of children with acute lymphocytic leukemia. Cancer Genet Cytogenet. 1985 Jun;17(2):165-79
Prigogina EL, Puchkova GP, Mayakova SA. Nonrandom chromosomal abnormalities in acute lymphoblastic leukemia of childhood. Cancer Genet Cytogenet. 1988 Jun;32(2):183-203

t(14;19)(q32;q13) IGH/CEBPA Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 380
Pui CH, Raimondi SC, Borowitz MJ, Land VJ, Behm FG, Pullen DJ, Hancock ML, Shuster JJ, Steuber CP, Crist WM. Immunophenotypes and karyotypes of leukemic cells in children with Down syndrome and acute lymphoblastic leukemia. J Clin Oncol. 1993 Jul;11(7):1361-7
Andreasson P, Höglund M, Békássy AN, Garwicz S, Heldrup J, Mitelman F, Johansson B. Cytogenetic and FISH studies of a single center consecutive series of 152 childhood acute lymphoblastic leukemias. Eur J Haematol. 2000 Jul;65(1):40-51
Ramji DP, Foka P. CCAAT/enhancer-binding proteins: structure, function and regulation. Biochem J. 2002 Aug 1;365(Pt 3):561-75
Robinson HM, Taylor KE, Jalali GR, Cheung KL, Harrison CJ, Moorman AV. t(14;19)(q32;q13): a recurrent translocation in B-cell precursor acute lymphoblastic leukemia. Genes Chromosomes Cancer. 2004 Jan;39(1):88-92
Smith ML, Cavenagh JD, Lister TA, Fitzgibbon J. Mutation of CEBPA in familial acute myeloid leukemia. N Engl J Med. 2004 Dec 2;351(23):2403-7
Chapiro E, Russell L, Radford-Weiss I, Bastard C, Lessard M, Struski S, Cave H, Fert-Ferrer S, Barin C, Maarek O, Della-
Valle V, Strefford JC, Berger R, Harrison CJ, Bernard OA, Nguyen-Khac F. Overexpression of CEBPA resulting from the translocation t(14;19)(q32;q13) of human precursor B acute lymphoblastic leukemia. Blood. 2006 Nov 15;108(10):3560-3
Akasaka T, Balasas T, Russell LJ, Sugimoto KJ, Majid A, Walewska R, Karran EL, Brown DG, Cain K, Harder L, Gesk S, Martin-Subero JI, Atherton MG, Brüggemann M, Calasanz MJ, Davies T, Haas OA, Hagemeijer A, Kempski H, Lessard M, Lillington DM, Moore S, Nguyen-Khac F, Radford-Weiss I, Schoch C, Struski S, Talley P, Welham MJ, Worley H, Strefford JC, Harrison CJ, Siebert R, Dyer MJ. Five members of the CEBP transcription factor family are targeted by recurrent IGH translocations in B-cell precursor acute lymphoblastic leukemia (BCP-ALL). Blood. 2007 Apr 15;109(8):3451-61
Nerlov C. The C/EBP family of transcription factors: a paradigm for interaction between gene expression and proliferation control. Trends Cell Biol. 2007 Jul;17(7):318-24
This article should be referenced as such:
Huret JL. t(14;19)(q32;q13) IGH/CEBPA. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):378-380.

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 381
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(2;4)(p22;q12) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t0204p22q12ID2136.html DOI: 10.4267/2042/44478
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Myeloproliferative disease with eosinophilia
Epidemiology Only one case to date, a 64 year old male patient.
Prognosis The patient remained in complete remission for 24 months of treatment with imatinib, but refused any more treatment, althoughthere was no side effect. Elevated eosinophil counts were again detected 14 months after end of treatment.
Genes involved and proteins STRN Location 2p22.2
Protein Composed of a caveolin-binding domain, a coiled-coil domain, a calmodulin-binding domain, and at least 6 WD-repeats. Striatin (STRN) binds many proteins, and forms multi-protein complexes. It is a scaffolding protein; striatin contains a caveolin-binding consensus motif, and binds caveolin-1, the major protein involved in caveolae and lipid rafts. Striatin is also involved in signaling and trafficking in a Ca2+ dependant manner, exhibiting a dual role in endocytic process and signaling.
PDGFRA Location 4q12
Protein Composed of an extracellular domain (the immunoglobulin-like motifs), a transmembrane domain, with an inhibitory juxtamembrane WW-like domain (Irusta et al., 2002), and an intracellular domain (kinase domain); receptor tyrosine kinase; forms homodimer, and heterodimer with PDGFRB; dimerization induces kinase domain activation, leading to the activation of intracellular signalling pathways (Kawagishi et al., 1995).
Somatic mutations Hybrid genes between various partners and PDFRGA occur in chronic myeloid leukaemia-like diseases with eosinophilia, mostly chronic eosinophilic leukemia (CEL), a clonal hypereosinophilic syndrome. PDGFRA partners known so far are: STRN (2p24), herein described (Curtis et al., 2007), FIP1L1 (4q12) (Cools et al., 2003; Pardanani et al., 2004), CDK5RAP2 (9q33) (Walz et al., 2006), KIF5B (10p11) (Score et al., 2006), ETV6 (12p13) (Curtis et al., 2007), and BCR (22q11) (Baxter et al., 2002). Mutations of platelet-derived growth factor receptor-alpha (PDGFRA) are observed in a subset of gastrointestinal stromal tumors (GISTs) (Heinrich et al., 2003). Tumours with PDGFRA involvement are responsive to imatinib therapy (Cools et al., 2003; Debiec-Rychter et al., 2004).
Result of the chromosomal anomaly Hybrid gene Transcript 5' STRN-3' PDGFRA; Fusion between STRN intron 6

t(2;4)(p22;q12) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 382
and a truncated PDGFRA exon 12; reciprocal product not found -> in frame fusion between STRN exon 6 and PDGFRA exon 12.
Fusion protein Description The N-term STRN - C-term PDGFRA fusion protein retains the caveolin-binding domain, the coiled-coil domain, and the calmodulin-binding domain, but not the WD-repeats of STRN, fused to a truncated WW-like domain and the kinase domain of PDGFRA; the coiled-coil domain from STRN may act as a dimerization motif that could constitutively activate PDGFRA tyrosine kinase.
References Kawagishi J, Kumabe T, Yoshimoto T, Yamamoto T. Structure, organization, and transcription units of the human alpha-platelet-derived growth factor receptor gene, PDGFRA. Genomics. 1995 Nov 20;30(2):224-32
Couet J, Li S, Okamoto T, Ikezu T, Lisanti MP. Identification of peptide and protein ligands for the caveolin-scaffolding domain. Implications for the interaction of caveolin with caveolae-associated proteins. J Biol Chem. 1997 Mar 7;272(10):6525-33
Gaillard S, Bartoli M, Castets F, Monneron A. Striatin, a calmodulin-dependent scaffolding protein, directly binds caveolin-1. FEBS Lett. 2001 Nov 9;508(1):49-52
Baxter EJ, Hochhaus A, Bolufer P, Reiter A, Fernandez JM, Senent L, Cervera J, Moscardo F, Sanz MA, Cross NC. The t(4;22)(q12;q11) in atypical chronic myeloid leukaemia fuses BCR to PDGFRA. Hum Mol Genet. 2002 Jun 1;11(12):1391-7
Irusta PM, Luo Y, Bakht O, Lai CC, Smith SO, DiMaio D. Definition of an inhibitory juxtamembrane WW-like domain in the platelet-derived growth factor beta receptor. J Biol Chem. 2002 Oct 11;277(41):38627-34
Cools J, DeAngelo DJ, Gotlib J, Stover EH, Legare RD, Cortes J, Kutok J, Clark J, Galinsky I, Griffin JD, Cross NC, Tefferi A, Malone J, Alam R, Schrier SL, Schmid J, Rose M, Vandenberghe P, Verhoef G, Boogaerts M, Wlodarska I, Kantarjian H, Marynen P, Coutre SE, Stone R, Gilliland DG. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic
hypereosinophilic syndrome. N Engl J Med. 2003 Mar 27;348(13):1201-14
Heinrich MC, Corless CL, Duensing A, McGreevey L, Chen CJ, Joseph N, Singer S, Griffith DJ, Haley A, Town A, Demetri GD, Fletcher CD, Fletcher JA. PDGFRA activating mutations in gastrointestinal stromal tumors. Science. 2003 Jan 31;299(5607):708-10
Debiec-Rychter M, Dumez H, Judson I, Wasag B, Verweij J, Brown M, Dimitrijevic S, Sciot R, Stul M, Vranck H, Scurr M, Hagemeijer A, van Glabbeke M, van Oosterom AT. Use of c-KIT/PDGFRA mutational analysis to predict the clinical response to imatinib in patients with advanced gastrointestinal stromal tumours entered on phase I and II studies of the EORTC Soft Tissue and Bone Sarcoma Group. Eur J Cancer. 2004 Mar;40(5):689-95
Pardanani A, Brockman SR, Paternoster SF, Flynn HC, Ketterling RP, Lasho TL, Ho CL, Li CY, Dewald GW, Tefferi A. FIP1L1-PDGFRA fusion: prevalence and clinicopathologic correlates in 89 consecutive patients with moderate to severe eosinophilia. Blood. 2004 Nov 15;104(10):3038-45
Benoist M, Gaillard S, Castets F. The striatin family: a new signaling platform in dendritic spines. J Physiol Paris. 2006 Mar-May;99(2-3):146-53
Score J, Curtis C, Waghorn K, Stalder M, Jotterand M, Grand FH, Cross NC. Identification of a novel imatinib responsive KIF5B-PDGFRA fusion gene following screening for PDGFRA overexpression in patients with hypereosinophilia. Leukemia. 2006 May;20(5):827-32
Walz C, Curtis C, Schnittger S, Schultheis B, Metzgeroth G, Schoch C, Lengfelder E, Erben P, Müller MC, Haferlach T, Hochhaus A, Hehlmann R, Cross NC, Reiter A. Transient response to imatinib in a chronic eosinophilic leukemia associated with ins(9;4)(q33;q12q25) and a CDK5RAP2-PDGFRA fusion gene. Genes Chromosomes Cancer. 2006 Oct;45(10):950-6
Curtis CE, Grand FH, Musto P, Clark A, Murphy J, Perla G, Minervini MM, Stewart J, Reiter A, Cross NC. Two novel imatinib-responsive PDGFRA fusion genes in chronic eosinophilic leukaemia. Br J Haematol. 2007 Jul;138(1):77-81
This article should be referenced as such:
Huret JL. t(2;4)(p22;q12). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):381-382.

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 383
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(5;14)(q35;q32.2) Stefan Nagel, Roderick AF MacLeod
DSMZ - German Collection of Microorganisms and Cell Cultures, Dept of Human & (SN), Animal Cell Cultures, Inhoffenstr. 7b, 38124, Braunschweig, Germany (RAFM)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t0514q35q32ID1386.html DOI: 10.4267/2042/44479
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease T cell acute lymphoblastic leukemia (T-ALL)
Phenotype/cell stem origin Cortical T cell leukemia (CD1a+, CD10+).
Epidemiology Restricted to T-ALL. Relatively frequent in pediatric T-
ALL (approximatively 20%); less frequent in adult T-ALL.
Cytology FAB nomenclature: L1 or L2 ALL.
Prognosis TLX3 expression - presumably due to t(5;14)(q35.1;q32) or its congeners - has been reported to confer poor prognosis.
Cytogenetics
G-banding of t(5;14)(q35;q32.2) in a pediatric T-ALL leukemia cell line (CCRF-CEM) illustrating the cryptic nature of this rearrangement. Hence normal and rearranged homologs are indistinguishable by G-banding, as are standard and rare variant t(5;14) subtypes. In chromosome painting images only a minority of cells in even superior preparations show the t(5;14).

t(5;14)(q35;q32.2) Nagel S, MacLeod RAF
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 384
Cytogenetics morphological t(5;14), like other cryptic chromosomal aberrations, was discovered relatively recently and most subsequent studies have focused on molecular and clinical aspects of this entity to the exclusion of cytogenetics. This gap is aggravated by the uniquely large breakpoint cluster region (bcr) of the 14q32 partner gene, BCL11B (alias CTIP2, RIT1). Hence, detailed documentation of this interesting rearrangement is largely based on data obtained using t(5;14) T-ALL cell lines which hitherto all carry submicroscopic insertions, both ins(5;14) and ins(14;5), instead of conventional reciprocal translocations. If verified in patient material, detailed analysis of such configurations may reveal neighboring genes or regulators inimical to the oncogenic activity of t(5;14), and therefore excluded by the more selective insertional rearrangements.
Cytogenetics molecular The proximities of the 14q32.2, and of both standard and variant 5q35 breakpoints to their respective telomeres, impairs FISH detection using chromosome painting probes except in optimal preparations. The tendency of t(5;14) to involve microinsertions (in both directions), together with the sheer magnitude of the BCL11B bcr, impedes detection by specific BAC/PAC combinations.
Probes The widespread involvement of cryptic rearrangements, notably microinsertions, plus the sheer length of the 14q32.2 breakpoint cluster complicates diagnostic probe design. Sensitive molecular cytogenetic diagnosis requires a BAC contig-battery covering bcr at both 5q35 and 14q32. Given the ectopic - all or none - nature of TLX3 expression in affected cells, screening t(5;14) is probably better performed by RT-PCR.
Variants A microscopically synonymous variant, t(5;14)(q35.2;q32.2), whereby the closely related and neighboring NKX2-5 is juxtaposed to BCL11B, has proved frustratingly difficult to identify clinically despite occurring in two widely used T-ALL cell lines, CCRF-CEM and PEER. NKX2-5 is ectopically activated in t(5;14)(q35.2;q11.2) where it is juxtaposed with TRAD. The diagnostic caveats for the standard translocation also apply: detection of variant t(5;14) by RT-PCR is likely to pose fewer technical difficulties than cytogenetic detection by FISH.
Genes involved and proteins Note The breakpoints at 14q32.2 are located in the
downstream region of BCL11B and are widely distributed along an almost unprecedentedly long stretch of about 1 Mbp in extent. So far there is no hint of deregulation of BCL11B by t(5;14)(q35;32). The t(5;14) aberration results in the juxtaposition of either TLX3 or NKX2-5 homeobox genes with enhancer elements located downstream of BCL11B inside a "genomic desert" region. TLX3 and NKX2-5 are located at 5q35.1 and 5q35.2, respectively, about 2 Mbp apart. The centromeric neighbour of TLX3, RANBP17, may undergo truncation by the translocation, although this may not be significant as RANBP17 is not expressed in T-cells. While both, TLX3 and NKX2-5 have been described to be activated by translocations involving the T-cell receptor genes, aberrations targeting NKX2-5 seem to be very rare in T-ALL. Together with TLX1/HOX11 both homeobox genes, TLX3 and NKX2-5, are members of the NK-like family of homeobox genes, implicating similar activities in T-cell leukemogenesis. However, differences in the prognostic outcome may indicate functional differences between TLX1 and TLX3. A couple of dysregulated targets of these NK-like homeobox genes have been described, including PP2A for TLX1 and MEF2C for NKX2-5. Physiologically, TLX3 and NKX2-5 are involved in organogenesis of the spleen. Additionally, TLX3 is expressed in neuronal cells of the periphery and NKX2-5 in the heart. Therefore, their expression in T-cells is ectopic and serves as a solid diagnostic marker detectable by (quantitiative) RT-PCR. However, no standard assay for TLX3, as described for other mutated genes in leukemia/lymphoma by BIOMED, has been published so far.
TLX3 Location 5q35.1
Note Alias: HOX11L2.
Protein Homeodomain; member of the NK-like family of homeobox genes.
NKX2-5 Location 5q35.2
Note Alias: CSX.
Protein Homeodomain; member of the NK-like family of homeobox genes.

t(5;14)(q35;q32.2) Nagel S, MacLeod RAF
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 385
Upper image depicts results of chromosome painting in an above average T-ALL cell (CCRF-CEM) with t(5;14) and concurrent ins(14;5). Note absence of visible signs betraying reciprocal exchange. Chromosome painting was performed using Cambio probes (Cambridge, UK) for chromosomes 5 (TexasRed), and 14 (Cy3). Middle image depicts standard t(5;14)(q35.1;q32.2) as represented by ins(5;14)(q35.1;q32.2q32.2) in cell line DND-41 which activates TLX3 transcription by juxtaposition with part of the noncoding region of BCL11B (clones shown below). Insert shows fiber-FISH confirming the regions juxtaposed. Lower image summarizes breakpoint data for t(5;14)(q35;q32) in T-ALL at three loci: TLX3 (standard translocation), NKX2-5 (variant translocation), and BCL11B (both translocations). Patient and cell line breakpoints are shown red and blue, respectively, together with insertion data from cell line DND-41. The NKX2-5 patient breakpoint included for comparison is from a t(5;14)(q35.2;q11.2) patient where TRAD is the activating partner. Coordinates are given in Mbp. Note the circa 1 Mbp 14q32.2 bcr which effectively covers the 3'-BCL11B regulatory region, while TLX3 breakpoints cover a "modest" 90 Kbp. NKX2-5 cases are too rare to allow bcr delineation.

t(5;14)(q35;q32.2) Nagel S, MacLeod RAF
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 386
Result of the chromosomal anomaly Hybrid gene
Figure 1 shows RT-PCR analysis of genes involved in t(5;14)(q35;q32) in T-ALL cell lines PEER and CCRF-CEM, both expressing NKX2-5 instead of TLX3. Figure 2 shows expression array data converted into a heat-map and demonstrate gene activities in five T-ALL cell lines: ALL-SIL (TRAD/TLX1), CCRF-CEM (NKX2-5/BCL11B), HPB-ALL (TLX3/BCL11B), PEER (NKX2-5/BCL11B), JURKAT (negative control). Red indicates high, green low, and black medium expression level. Note expression of homeobox genes is restricted to presence of corresponding translocation.
Fusion protein Description No fusion protein, but ectopic expression of either TLX3 or NKX2-5.
Oncogenesis Due to the chromosomal translocation, transcription factor binding sites for PU.1 and HMGA1, located near 5'-TLX3/NKX2-5 (5q35) and 3'-BCL11B (14q32.2), respectively, are juxtaposed. PU.1 and HMGA1 proteins are thus able to interact across the boundaries of the juxtaposed regions and form enhanceosomal complexes mediating transcriptional activity. Furthermore, BCL11B enhancer regions at 14q32 aggregate with acetylated histones recruited to open chromatin at DNaseI hypersensitive sites and contact the nuclear matrix - a region favorable to transcription. Altogether, these data indicate the existence of potent enhancer regions at 14q32 downstream of BCL11B responsible for homeobox gene activation in
partipicipant translocations. The precise physiological mechanism(s) underlying the normal activity of presumptive BCL11B enhancers awaits clarification: although these enhancers may be involved in the developmental control of BCL11B activity - a gene demanding exquisite regulation in T-cells - little supporting data are as yet available.
References Bernard OA, Busson-LeConiat M, Ballerini P, Mauchauffé M, Della Valle V, Monni R, Nguyen Khac F, Mercher T, Penard-Lacronique V, Pasturaud P, Gressin L, Heilig R, Daniel MT, Lessard M, Berger R. A new recurrent and specific cryptic translocation, t(5;14)(q35;q32), is associated with expression of the Hox11L2 gene in T acute lymphoblastic leukemia. Leukemia. 2001 Oct;15(10):1495-504
Satterwhite E, Sonoki T, Willis TG, Harder L, Nowak R, Arriola EL, Liu H, Price HP, Gesk S, Steinemann D, Schlegelberger B, Oscier DG, Siebert R, Tucker PW, Dyer MJ. The BCL11 gene family: involvement of BCL11A in lymphoid malignancies. Blood. 2001 Dec 1;98(12):3413-20
MacLeod RA, Nagel S, Kaufmann M, Janssen JW, Drexler HG. Activation of HOX11L2 by juxtaposition with 3'-BCL11B in an acute lymphoblastic leukemia cell line (HPB-ALL) with t(5;14)(q35;q32.2). Genes Chromosomes Cancer. 2003 May;37(1):84-91
Nagel S, Kaufmann M, Drexler HG, MacLeod RA. The cardiac homeobox gene NKX2-5 is deregulated by juxtaposition with BCL11B in pediatric T-ALL cell lines via a novel t(5;14)(q35.1;q32.2). Cancer Res. 2003 Sep 1;63(17):5329-34
Cavé H, Suciu S, Preudhomme C, Poppe B, Robert A, Uyttebroeck A, Malet M, Boutard P, Benoit Y, Mauvieux L, Lutz P, Méchinaud F, Grardel N, Mazingue F, Dupont M, Margueritte G, Pages MP, Bertrand Y, Plouvier E, Brunie G, Bastard C, Plantaz D, Vande Velde I, Hagemeijer A, Speleman F, Lessard M, Otten J, Vilmer E, Dastugue N. Clinical significance of HOX11L2 expression linked to t(5;14)(q35;q32), of HOX11 expression, and of SIL-TAL fusion in childhood T-cell malignancies: results of EORTC studies 58881 and 58951. Blood. 2004 Jan 15;103(2):442-50
MacLeod RA, Nagel S, Drexler HG. BCL11B rearrangements probably target T-cell neoplasia rather than acute myelocytic leukemia. Cancer Genet Cytogenet. 2004 Aug;153(1):88-9
Su XY, Busson M, Della Valle V, Ballerini P, Dastugue N, Talmant P, Ferrando AA, Baudry-Bluteau D, Romana S, Berger R, Bernard OA. Various types of rearrangements target TLX3 locus in T-cell acute lymphoblastic leukemia. Genes Chromosomes Cancer. 2004 Nov;41(3):243-9
Gottardo NG, Jacoby PA, Sather HN, Reaman GH, Baker DL, Kees UR. Significance of HOX11L2/TLX3 expression in children with T-cell acute lymphoblastic leukemia treated on Children's Cancer Group protocols. Leukemia. 2005 Sep;19(9):1705-8
Nagel S, Scherr M, Kel A, Hornischer K, Crawford GE, Kaufmann M, Meyer C, Drexler HG, MacLeod RAF.. Inhibition of TLX3 and NKX2-5 in t(5;14)(q35;q32) T-ALL after Blocking Remote 3'-BCL11B Enhancer Sequences with Matching DNA Oligos Reveals Coregulation by PU.1 and HMGA1. Blood , 2006; 108: 2212.
Su X, Drabkin H, Clappier E, Morgado E, Busson M, Romana S, Soulier J, Berger R, Bernard OA, Lavau C. Transforming potential of the T-cell acute lymphoblastic leukemia-associated homeobox genes HOXA13, TLX1, and TLX3. Genes Chromosomes Cancer. 2006 Sep;45(9):846-55

t(5;14)(q35;q32.2) Nagel S, MacLeod RAF
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 387
Su XY, Della-Valle V, Andre-Schmutz I, Lemercier C, Radford-Weiss I, Ballerini P, Lessard M, Lafage-Pochitaloff M, Mugneret F, Berger R, Romana SP, Bernard OA, Penard-Lacronique V. HOX11L2/TLX3 is transcriptionally activated through T-cell regulatory elements downstream of BCL11B as a result of the t(5;14)(q35;q32). Blood. 2006 Dec 15;108(13):4198-201
van Grotel M, Meijerink JP, Beverloo HB, Langerak AW, Buys-Gladdines JG, Schneider P, Poulsen TS, den Boer ML, Horstmann M, Kamps WA, Veerman AJ, van Wering ER, van Noesel MM, Pieters R. The outcome of molecular-cytogenetic subgroups in pediatric T-cell acute lymphoblastic leukemia: a retrospective study of patients treated according to DCOG or COALL protocols. Haematologica. 2006 Sep;91(9):1212-21
Nagel S, Scherr M, Kel A, Hornischer K, Crawford GE, Kaufmann M, Meyer C, Drexler HG, MacLeod RA. Activation of TLX3 and NKX2-5 in t(5;14)(q35;q32) T-cell acute lymphoblastic leukemia by remote 3'-BCL11B enhancers and coregulation by PU.1 and HMGA1. Cancer Res. 2007 Feb 15;67(4):1461-71
Nagel S, Meyer C, Quentmeier H, Kaufmann M, Drexler HG, MacLeod RA. MEF2C is activated by multiple mechanisms in a subset of T-acute lymphoblastic leukemia cell lines. Leukemia. 2008 Mar;22(3):600-7
van Grotel M, Meijerink JP, van Wering ER, Langerak AW, Beverloo HB, Buijs-Gladdines JG, Burger NB, Passier M, van Lieshout EM, Kamps WA, Veerman AJ, van Noesel MM, Pieters R. Prognostic significance of molecular-cytogenetic abnormalities in pediatric T-ALL is not explained by immunophenotypic differences. Leukemia. 2008 Jan;22(1):124-31
Van Vlierberghe P, Homminga I, Zuurbier L, Gladdines-Buijs J, van Wering ER, Horstmann M, Beverloo HB, Pieters R, Meijerink JP. Cooperative genetic defects in TLX3 rearranged pediatric T-ALL. Leukemia. 2008 Apr;22(4):762-70
This article should be referenced as such:
Nagel S, MacLeod RAF. t(5;14)(q35;q32.2). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):383-387.

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 388
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(8;14)(q11;q32) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t0814ID1112.html DOI: 10.4267/2042/44480
This article is an update of : Huret JL. t(8;14)(q11;q32). Atlas Genet Cytogenet Oncol Haematol 2005;9(3):256-258. Huret JL. t(8;14)(q11;q32). Atlas Genet Cytogenet Oncol Haematol 1999;3(4):196-197. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity
- 8, + der(14) t(8;14)(q11;q32) G banding (left) - Courtesy Gitte Birk Kerndrup and Steen Rosthoj; der(14) t(8;14)(q11;q32) R-banding - Courtesy Pascale Cornillet-Lefebvre and Stephanie Struski (top), and with a constitutional trisomy 21 (bottom) - Courtesy Petr Balicek, Jana Rabasova, and Jiri Hak. More iconography can be found in the Case Report section (see below).
Clinics and pathology Disease CD10+ acute lymphoblastic leukemia (ALL) in most cases; chronic myelogenous leukemia (CML) very rarely; one case of histiocyte-rich B-cell lymphoma.
Etiology Strikingly, more than 1/4 of cases are Down syndrome patients.
Epidemiology At least 52 cases to date (see Ref. below); the t(8;14)(q11;q32) represents about 1/1 000 cases of childhood leukemias; median age is 11 years (range 3-49), with 10% above 20 years; unbalanced sex ratio (29M/18F).
Clinics Organomegaly is not frequent, central nervous system (CNS) involvement was not noted; WBC was < 50 X 109/l in most cases.

t(8;14)(q11;q32) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 389
Prognosis Prognosis is likely to be not bad, although a long follow up is missing in about half of the cases (see Figure 2).
Cytogenetics Cytogenetics morphological Sole (acquired) anomaly in 1/3 of cases; accompany a t(9;22)(q34;q11) in 20% of cases; unbalanced form with a der(14) t(8;14) in 15% of cases, indicating that the crucial event is likely to lie on der(14). One case was a three way translocation t(2;14;8).
Additional anomalies t(8;14) may be found with t(9;22) (see above); t(8;14) is accompanied by an acquired (not constitutional) +21 in 10% of cases; +X, +8, and del(13q) are also recurrently found with t(8;14).
Genes involved and proteins CEBPD Location 8q11
Protein DNA-binding protein. CCAAT enhancer-binding protein (CEBP) transcription factors are a family of 6 multifunctional basic leucine zipper (bZIP) transcription factors. The 5 other CEBPs are: CEBPA (19q13), CEBPB (20q13), CEBPE (14q11), CEBPG (19q13), all four equally implicated in leukemias, and DDIT3/CHOP/CEBP zeta (12q13), so far known to be involved in solid tumours (liposarcoma). These transcription factors play a key role in cellular differentiation, in particular in the control of myeloid differentiation. CEBPD is composed of a N-term transactivation domain, a DNA-binding basic motif, and a leucine-zipper domain in C-term (Ramji et al., 2002; Nerlov et al., 2007).
IgH Location 14q32
Result of the chromosomal anomaly Fusion protein Oncogenesis Overexpression of the CEBP gene.
To be noted Case Report A case of pre-B ALL with t(8;14)(q11;q32). A case of Down syndrome with acute lymphoblastic leukemia and t(8;14)(q11;q32). A new case of t(8;14)(q11;q32) in an acute lymphoblastic leukemia.
References Hayata I, Sakurai M, Kakati S, Sandberg AA. Chromosomes and causation of human cancer and leukemia. XVI. Banding studies of chronic myelocytic leukemia, including five unusual Ph11 translocations. Cancer. 1975 Oct;36(4):1177-91
Kardon NB, Slepowitz G, Kochen JA. Childhood acute lymphoblastic leukemia associated with an unusual 8;14 translocation. Cancer Genet Cytogenet. 1982 Aug;6(4):339-43
Carroll AJ, Castleberry RP, Crist WM. Lack of association between abnormalities of the chromosome 9 short arm and either "lymphomatous" features or T cell phenotype in childhood acute lymphocytic leukemia. Blood. 1987 Mar;69(3):735-8
Crist W, Carroll A, Shuster J, Jackson J, Head D, Borowitz M, Behm F, Link M, Steuber P, Ragab A. Philadelphia chromosome positive childhood acute lymphoblastic leukemia: clinical and cytogenetic characteristics and treatment outcome. A Pediatric Oncology Group study. Blood. 1990 Aug 1;76(3):489-94
Hayashi Y, Pui CH, Behm FG, Fuchs AH, Raimondi SC, Kitchingman GR, Mirro J Jr, Williams DL. 14q32 translocations are associated with mixed-lineage expression in childhood acute leukemia. Blood. 1990 Jul 1;76(1):150-6
Hu N, Bian ML, Le Beau MM, Rowley JD. Cytogenetic analysis of 51 patients with chronic myeloid leukemia. Chin Med J (Engl). 1990 Oct;103(10):831-9
Wodzinski MA, Watmore AE, Lilleyman JS, Potter AM. Chromosomes in childhood acute lymphoblastic leukaemia: karyotypic patterns in disease subtypes. J Clin Pathol. 1991 Jan;44(1):48-51
Pui CH, Carroll AJ, Raimondi SC, Schell MJ, Head DR, Shuster JJ, Crist WM, Borowitz MJ, Link MP, Behm FG. Isochromosomes in childhood acute lymphoblastic leukemia: a collaborative study of 83 cases. Blood. 1992 May 1;79(9):2384-91
Pui CH, Raimondi SC, Borowitz MJ, Land VJ, Behm FG, Pullen DJ, Hancock ML, Shuster JJ, Steuber CP, Crist WM. Immunophenotypes and karyotypes of leukemic cells in children with Down syndrome and acute lymphoblastic leukemia. J Clin Oncol. 1993 Jul;11(7):1361-7

t(8;14)(q11;q32) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 390
Secker-Walker LM, Hawkins JM, Prentice HG, Mackie PH, Heerema NA, Provisor AJ. Two Down syndrome patients with an acquired translocation, t(8;14)(q11;q32), in early B-lineage acute lymphoblastic leukemia. Cancer Genet Cytogenet. 1993 Oct 15;70(2):148-50
Testoni N, Zaccaria A, Martinelli G, Pelliconi S, Buzzi M, Farabegoli P, Panzica G, Tura S. t(8;14)(q11;q32) in acute lymphoid leukemia: description of two cases. Cancer Genet Cytogenet. 1993 May;67(1):55-8
Shearer P, Parham D, Kovnar E, Kun L, Rao B, Lobe T, Pratt C. Neurofibromatosis type I and malignancy: review of 32 pediatric cases treated at a single institution. Med Pediatr Oncol. 1994;22(2):78-83
Litz CE, Davies S, Brunning RD, Kueck B, Parkin JL, Gajl Peczalska K, Arthur DC. Acute leukemia and the transient myeloproliferative disorder associated with Down syndrome: morphologic, immunophenotypic and cytogenetic manifestations. Leukemia. 1995 Sep;9(9):1432-9
Schoch C, Rieder H, Stollmann-Gibbels B, Freund M, Tischler HJ, Silling-Engelhardt G, Fonatsch C. 17p anomalies in lymphoid malignancies: diagnostic and prognostic implications. Leuk Lymphoma. 1995 Apr;17(3-4):271-9
Lee AC, Chan LC, Kwong KW. Down syndrome, acute lymphoblastic leukemia, and t(8;14)(q11;q32) Cancer Genet Cytogenet. 1996 May;88(1):92
Sun T, Susin M, Tomao FA, Brody J, Koduru P, Hajdu SI. Histiocyte-rich B-cell lymphoma. Hum Pathol. 1997 Nov;28(11):1321-4
Forrest DL, Nevill TJ, Horsman DE, Brockington DA, Fung HC, Toze CL, Conneally EA, Hogge DE, Sutherland HJ, Nantel SH, Shepherd JD, Barnett MJ. Bone marrow transplantation for adults with acute leukaemia and 11q23 chromosomal abnormalities. Br J Haematol. 1998 Dec;103(3):630-8
Whitehead VM, Vuchich MJ, Cooley LD, Lauer SJ, Mahoney DH, Shuster JJ, Payment C, Koch PA, Akabutu JJ, Bowen T, Kamen BA, Ravindranath Y, Emami A, Look AT, Beardsley GP, Pullen DJ, Camitta B. Accumulation of methotrexate polyglutamates, ploidy and trisomies of both chromosomes 4 and 10 in lymphoblasts from children with B-progenitor cell acute lymphoblastic leukemia: a Pediatric Oncology Group Study. Leuk Lymphoma. 1998 Nov;31(5-6):507-19
Andreasson P, Höglund M, Békássy AN, Garwicz S, Heldrup J, Mitelman F, Johansson B. Cytogenetic and FISH studies of a single center consecutive series of 152 childhood acute lymphoblastic leukemias. Eur J Haematol. 2000 Jul;65(1):40-51
Heerema NA, Sather HN, Sensel MG, Lee MK, Hutchinson RJ, Nachman JB, Reaman GH, Lange BJ, Steinherz PG, Bostrom BC, Gaynon PS, Uckun FM. Abnormalities of chromosome
bands 13q12 to 13q14 in childhood acute lymphoblastic leukemia. J Clin Oncol. 2000 Nov 15;18(22):3837-44
Kaleem Z, Shuster JJ, Carroll AJ, Borowitz MJ, Pullen DJ, Camitta BM, Zutter MM, Watson MS. Acute lymphoblastic leukemia with an unusual t(8;14)(q11.2;q32): a Pediatric Oncology Group Study. Leukemia. 2000 Feb;14(2):238-40
Balicek P, Rabasova J, Hak J.. A case of Down syndrome with acute lymphoblastic leukemia and t(8;14)(q11;q32). Atlas Genet Cytogenet Oncol Haematol. June 2001.
Byatt SA, Cheung KL, Lillington DM, Mazzullo H, Martineau M, Bennett C, Roberts K, Harewood L, Sumption N, Humphreys M, Burrett J, Harrison CJ. Three further cases of t(8;14)(q11.2;q32) in acute lymphoblastic leukemia. Leukemia. 2001 Aug;15(8):1304-5
Kerndrup GB, Rosthoj S. A case of pre-B ALL with t(8;14)(q11;q32). Atlas Genet Cytogenet Oncol Haematol. June 2001.
Mathew S, Rao PH, Dalton J, Downing JR, Raimondi SC. Multicolor spectral karyotyping identifies novel translocations in childhood acute lymphoblastic leukemia. Leukemia. 2001 Mar;15(3):468-72
Ramji DP, Foka P. CCAAT/enhancer-binding proteins: structure, function and regulation. Biochem J. 2002 Aug 1;365(Pt 3):561-75
Moore S, Suttle J, Bain S, Story C, Rice M. Acute lymphoblastic leukemia characterized by t(8;14)(q11.2;q32). Cancer Genet Cytogenet. 2003 Feb;141(1):1-4
Quilichini B, Zattara H, Casalonga F, BastideAlliez LA, Curtillet C, Fossat C, Michel G.. A new case of t(8;14)(q11;q32) in an acute lymphoblastic leukemia. Atlas Genet Cytogenet Oncol Haematol. May 2003 .
Akasaka T, Balasas T, Russell LJ, Sugimoto KJ, Majid A, Walewska R, Karran EL, Brown DG, Cain K, Harder L, Gesk S, Martin-Subero JI, Atherton MG, Brüggemann M, Calasanz MJ, Davies T, Haas OA, Hagemeijer A, Kempski H, Lessard M, Lillington DM, Moore S, Nguyen-Khac F, Radford-Weiss I, Schoch C, Struski S, Talley P, Welham MJ, Worley H, Strefford JC, Harrison CJ, Siebert R, Dyer MJ. Five members of the CEBP transcription factor family are targeted by recurrent IGH translocations in B-cell precursor acute lymphoblastic leukemia (BCP-ALL). Blood. 2007 Apr 15;109(8):3451-61
Nerlov C. The C/EBP family of transcription factors: a paradigm for interaction between gene expression and proliferation control. Trends Cell Biol. 2007 Jul;17(7):318-24
This article should be referenced as such:
Huret JL. t(8;14)(q11;q32). Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):388-390.

Solid Tumour Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 391
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Liver tumors: an overview Munechika Enjoji
Department of Clinical Pharmacology, Faculty of Pharmaceutical Sciences, Fukuoka University, 8-19-1 Nanakuma, Johnan-ku, Fukuoka 814-0180, Japan (ME)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Tumors/LiverOverviewID5273.html DOI: 10.4267/2042/44481
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Classification WHO histological classification of the liver and intrahepatic bile ducts.
Epithelial tumors Benign:
Hepatocellular adenoma Focal nodular hyperplasia Intrahepatic bile duct adenoma Intrahepatic bile duct cystadenoma Biliary papillomatosis
Malignant: Hepatocellular carcinoma Intrahepatic cholangiocarcinoma Bile duct cystadenocarcinoma Combined hepatocellular and cholangiocarcinoma Hepatoblastoma Undifferentiated carcinoma
Non-epithelial tumors Benign:
Angiomyolipoma Lymphangioma and lymphangiomatosis Hemangioma Infantile hemangioendothelioma
Malignant: Epithelioid hemangioendothelioma Angiosarcoma Embryonal sarcoma Rhabdomyosarcoma Others
Miscellaneous tumors Solitary fibrous tumor Teratoma York sac tumor Carcinosarcoma Rhabdoid tumor
Others
Hematopoietic and lymphoid tumors
Secondary tumors
Epithelial abnormalities Liver cell dysplasia Dysplastic nodules Bile duct abnormalities
Miscellaneous lesions Mesenchymal hamartoma Nodular transformation Inflammatory pseudotumor
Clinics and pathology Disease Benign tumors Hepatic hemangioma: Hemangioma is the most common benign tumor of the liver and is more frequent in women. Many cases are discovered incidentally and the reported incidence is 2-20%. Tumor size may be associated with pregnancy and estrogen levels. Hepatic hemangioma is usually asymptomatic, and rarely grows or bleeds. Surgical excision is required in some symptomatic cases. No genetic alterations heave been reported. Focal nodular hyperplasia (FNH): FNH is the second most frequent benign tumor of the liver and occurs mainly in women (80-90%). In a hyperplastic lesion, all of the normal liver constituents are present but in an abnormally organized pattern. Underlying congenital arteriovenous malformation, oral contraceptives, and some medicines such as azathioprine are considered to be pathogenic factors. FNH has no malignant potential but a combination of various imaging techniques may be needed for correct diagnosis. FNHs exhibit few chromosomal abnormalities. Strong immunostaining of

Liver tumors: an overview Enjoji M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 392
ras oncogene p21 has been reported and epithelial cells of the ductular proliferation were bcl-2-positive. Hepatocellular adenoma: Adenomas occur almost exclusively in younger women. Evidence is accumulating that the intake of oral contraceptives is associated with the occurrence of hepatocellular adenoma. Most are asymptomatic and found by chance at the time of a scan. Prognosis is relatively good. Occasionally, hepatocellular adenomas can be complicated by bleeding either spontaneously or following trauma. The risk of evolution to hepatocellular carcinoma is small. Hepatic adenomas exhibit few chromosomal abnormalities. In one study, nuclear accumulation of β-catenin was reported in 46% of hepatic adenomas, which indicates activation of the Wnt signaling pathway. In another report, truncated forms of β-catenin were detected. Uneven and relatively weak p21 reactions were noted in hepatic adenomas. Angiomyolipoma: Angiomyolipoma is a relatively rare tumor and is composed of fatty cells, blood vessels, and smooth muscle cells in varying proportions. Thick-walled blood vessels are usually arranged in an island-like formation. Malignant degeneration has not been reported. In one report, of 15 hepatic angiomyolipoma samples tested, all were KIT (CD117), transmembrane growth factor receptor, positive. Bile duct cystadenoma: Hepatic cystadenoma is a rare multilocular cystic tumor probably occurs as a result of congenital bile duct malformations. It is seen more frequently in women and usually arises from ducts near the hilum of the liver. Owing to its trend towards malignant degeneration, surgical resection may be recommended. No cytogenetic alterations have been reported.
Malignant tumors Hepatocellular carcinoma (HCC): HCC is the most frequently observed and clinically important primary hepatic neoplasm. It occurs more commonly in men than women and its geographical distribution varies considerably. In areas with high incidence, chronic infection with HBV or HCV is a well-known underlying cause. A frequent association with chronic liver disease/cirrhosis has also been reported. a-fetoprotein and PIVKA-II are the most commonly used tumor-associated markers. It has been reported that chromosomal aberrations on 1p, 6q, 8p/q, and 13p occur almost exclusively in HCCs. Overexpression of c-myc oncogene and a-prothymosin was also reported. An uneven and comparatively weak ras p21 immunohistochemical reaction was noted in HCC. The frequency of p53 mutations varies among different geographic areas. In recent reports, expression of nuclear Jun activation binding protein 1 (Jab1) was observed in 57% of HCCs, and MDM mutations and GAGE-1, GAGE-2 expression were also commonly observed in HCC specimens. In an immunohistochemical evaluation of HCC specimens,
altered expression of bcl-2 and human Mut S homologue-2 (hMSH2) proteins was observed during hepatocarcinogenesis. c-erbB-2 oncopeptide was immunohistochemically detected in HCCs although the percentage of samples positive for c-erbB-2 was low. Intrahepatic cholangiocarcinoma: Intrahepatic cholangiocarcinoma (CC), the second most prevalent intrahepatic primary cancer, arises from the intrahepatic bile duct epithelium. It occurs primarily in the middle-aged and elderly patients with no obvious sex differences. Its incidence varies widely between geographic regions: the highest incidence is reported in Southeast Asia. Opisthorchis viverrini-induced CCs are common in Thailand. Liver fluke infection, carcinogenic nitroso-compounds, hepatolithiasis, and primary sclerosing cholangitis are high-risk factors for intrahepatic CC. CA19-9, CEA, and CA125 are well studied as tumor-associated markers. In intrahepatic CCs, loss of heterozygosity (LOH) at chromosomal loci 3p13-p21, 5q35-qter, 8p22, 17p13, and 18q has been reported. The reported mutation rates of K-ras, which is converted to an active oncogene by point mutations, in intrahepatic CCs vary widely; for example, a mutation rate of 50-56% has been reported in Japanese patients versus 0-8% in Thai patients. Inactivation of p53 by mis-sense or non-sense mutations and by loss of chromosome 17p induces disruption of critical growth-regulating mechanisms and may have a crucial role in carcinogenesis. It has been reported that the p53 mutation and loss of chromosome 17p was present in 11-37% and 38% of intrahepatic CCs, respectively. Alterations of the tumor suppressor gene, p16INK4A, were found to be frequent in a study of intrahepatic CCs. Therefore, the p16 gene may be crucial for intrahepatic biliary carcinogenesis and progression. Amplification and overexpression of proto-oncogene c-erbB-2 are frequently seen in cancers of the biliary tract. Combined hepatocellular and cholangiocarcinoma: Combined hepatocellular and cholangiocarcinoma (combined tumors) is a more aggressive malignancy with a poorer prognosis than ordinary HCC. Its reported frequency varies widely; but a rate of 1.0-6.5% has been observed among patients with primary liver cancer. Statistically, combined tumors occur predominantly in men, with a mean age of onset in the sixth decade. In Asian cases, a high incidence of HBV or HCV infection and frequent association of cirrhosis have been reported. LOH at 4q, 8p, 13q, 16q, and 17p is frequently seen in combined tumors similar to that in HCC. LOH at 3p and 14q are reported to be specific in CCs and combined tumors in contrast to HCCs. Mutations of the K-ras gene have been reported to be common in CC but rarely in HCC. The reported incidence of p53 mutation is 10-29% in combined tumors. Hepatoblastoma: Hepatoblastoma, the most common hepatic tumor in children, is arises in the endodermal

Liver tumors: an overview Enjoji M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 393
liver epithelium and displays various histological patterns. The incidence is twice as high in boys than girls. Key markers include elevation or non-decreasing expression of a-fetoprotein, hepatomegaly, and weight loss. It is strongly associated with familial adenomatous polyposis probably owing to altered expression of the adenomatous polyposis coli (APC) gene. The most common genetic aberrations are extra copies of chromosomes 1q, 2q, 4q, 7q, 8, 17q, and 20, and LOH for 11p. It has been reported that p53 mutations contribute to hepatoblastoma. Bile duct cystadenocarcinoma: Hepatic cystadenocarcinoma is a rare multilocular tumor containing mucinous fluid. However, it is uncertain whether the incidence differs between sexes. After curative resection, the prognosis is good. In an immunohistochemical study of hepatic cystadenocarcinomas, p53, c-erbB-2, and bcl-2 were focally expressed in the tumor epithelium.
References Radosevich JA, Gould KA, Koukoulis GK, Haines GK, Rosen ST, Lee I, Gould VE. Immunolocalization of ras oncogene p21 in human liver diseases. Ultrastruct Pathol. 1993 Jan-Feb;17(1):1-8
Charlotte F, L'Herminé A, Martin N, Geleyn Y, Nollet M, Gaulard P, Zafrani ES. Immunohistochemical detection of bcl-2 protein in normal and pathological human liver. Am J Pathol. 1994 Mar;144(3):460-5
Watanabe M, Asaka M, Tanaka J, Kurosawa M, Kasai M, Miyazaki T. Point mutation of K-ras gene codon 12 in biliary tract tumors. Gastroenterology. 1994 Oct;107(4):1147-53
Yoshida S, Todoroki T, Ichikawa Y, Hanai S, Suzuki H, Hori M, Fukao K, Miwa M, Uchida K. Mutations of p16Ink4/CDKN2 and p15Ink4B/MTS2 genes in biliary tract cancers. Cancer Res. 1995 Jul 1;55(13):2756-60
Imai Y, Oda H, Arai M, Shimizu S, Nakatsuru Y, Inoue T, Ishikawa T. Mutational analysis of the p53 and K-ras genes and allelotype study of the Rb-1 gene for investigating the pathogenesis of combined hapatocellular-cholangiocellular carcinomas. Jpn J Cancer Res. 1996 Oct;87(10):1056-62
Weihing RR, Shintaku IP, Geller SA, Petrovic LM. Hepatobiliary and pancreatic mucinous cystadenocarcinomas with mesenchymal stroma: analysis of estrogen receptors/progesterone receptors and expression of tumor-associated antigens. Mod Pathol. 1997 Apr;10(4):372-9
Wu CG, Habib NA, Mitry RR, Reitsma PH, van Deventer SJ, Chamuleau RA. Overexpression of hepatic prothymosin alpha, a novel marker for human hepatocellular carcinoma. Br J Cancer. 1997;76(9):1199-204
Shrestha ML, Miyake H, Kikutsuji T, Tashiro S. Prognostic significance of Ki-67 and p53 antigen expression in carcinomas of bile duct and gallbladder. J Med Invest. 1998 Aug;45(1-4):95-102
Terada T, Ashida K, Endo K, Horie S, Maeta H, Matsunaga Y, Takashima K, Ohta T, Kitamura Y. c-erbB-2 protein is expressed in hepatolithiasis and cholangiocarcinoma. Histopathology. 1998 Oct;33(4):325-31
Kang YK, Kim WH, Lee HW, Lee HK, Kim YI. Mutation of p53 and K-ras, and loss of heterozygosity of APC in intrahepatic cholangiocarcinoma. Lab Invest. 1999 Apr;79(4):477-83
Schlott T, Ahrens K, Ruschenburg I, Reimer S, Hartmann H, Droese M. Different gene expression of MDM2, GAGE-1, -2 and FHIT in hepatocellular carcinoma and focal nodular hyperplasia. Br J Cancer. 1999 Apr;80(1-2):73-8
Fujii H, Zhu XG, Matsumoto T, Inagaki M, Tokusashi Y, Miyokawa N, Fukusato T, Uekusa T, Takagaki T, Kadowaki N, Shirai T. Genetic classification of combined hepatocellular-cholangiocarcinoma. Hum Pathol. 2000 Sep;31(9):1011-7
Hirohashi S, et al.. Tumors of the liver and intrahepatic bile ducts. in "WHO classification tumors of the digestive system" Hamilton SR and Aaltonen LA (2000) Eds. The IARC Press. REVIEW
Tannapfel A, Benicke M, Katalinic A, Uhlmann D, Köckerling F, Hauss J, Wittekind C. Frequency of p16(INK4A) alterations and K-ras mutations in intrahepatic cholangiocarcinoma of the liver. Gut. 2000 Nov;47(5):721-7
Cong WM, Bakker A, Swalsky PA, Raja S, Woods J, Thomas S, Demetris AJ, Finkelstein SD. Multiple genetic alterations involved in the tumorigenesis of human cholangiocarcinoma: a molecular genetic and clinicopathological study. J Cancer Res Clin Oncol. 2001;127(3):187-92
Chen YW, Jeng YM, Yeh SH, Chen PJ. P53 gene and Wnt signaling in benign neoplasms: beta-catenin mutations in hepatic adenoma but not in focal nodular hyperplasia. Hepatology. 2002 Oct;36(4 Pt 1):927-35
Makhlouf HR, Remotti HE, Ishak KG. Expression of KIT (CD117) in angiomyolipoma. Am J Surg Pathol. 2002 Apr;26(4):493-7
Torbenson M, Lee JH, Choti M, Gage W, Abraham SC, Montgomery E, Boitnott J, Wu TT. Hepatic adenomas: analysis of sex steroid receptor status and the Wnt signaling pathway. Mod Pathol. 2002 Mar;15(3):189-96
Altimari A, Fiorentino M, Gabusi E, Gruppioni E, Corti B, D'Errico A, Grigioni WF. Investigation of ErbB1 and ErbB2 expression for therapeutic targeting in primary liver tumours. Dig Liver Dis. 2003 May;35(5):332-8
Schnater JM, Köhler SE, Lamers WH, von Schweinitz D, Aronson DC. Where do we stand with hepatoblastoma? A review. Cancer. 2003 Aug 15;98(4):668-78
Terracciano L, Tornillo L. Cytogenetic alterations in liver cell tumors as detected by comparative genomic hybridization. Pathologica. 2003 Apr;95(2):71-82
Cazals-Hatem D, Rebouissou S, Bioulac-Sage P, Bluteau O, Blanché H, Franco D, Monges G, Belghiti J, Sa Cunha A, Laurent-Puig P, Degott C, Zucman-Rossi J. Clinical and molecular analysis of combined hepatocellular-cholangiocarcinomas. J Hepatol. 2004 Aug;41(2):292-8
Hussein MR. Alterations of p53, Bcl-2, and hMSH2 protein expression in the cirrhotic, macroregenerative, dysplastic nodules and hepatocellular carcinomas in Upper Egypt. Liver Int. 2004 Dec;24(6):552-60
Raidl M, Pirker C, Schulte-Hermann R, Aubele M, Kandioler-Eckersberger D, Wrba F, Micksche M, Berger W, Grasl-Kraupp B. Multiple chromosomal abnormalities in human liver (pre)neoplasia. J Hepatol. 2004 Apr;40(4):660-8
Nagata T, Nakamura M, Shichino H, Chin M, Sugito K, Ikeda T, Koshinaga T, Fukuzawa M, Inoue M, Mugishima H. Cytogenetic abnormalities in hepatoblastoma: report of two new cases and review of the literature suggesting imbalance of chromosomal regions on chromosomes 1, 4, and 12. Cancer Genet Cytogenet. 2005 Jan 1;156(1):8-13
Aishima S, Kuroda Y, Asayama Y, Taguchi K, Nishihara Y, Taketomi A, Tsuneyoshi M. Prognostic impact of

Liver tumors: an overview Enjoji M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 394
cholangiocellular and sarcomatous components in combined hepatocellular and cholangiocarcinoma. Hum Pathol. 2006 Mar;37(3):283-91
Patel T. Cholangiocarcinoma. Nat Clin Pract Gastroenterol Hepatol. 2006 Jan;3(1):33-42
Tischoff I, Wittekind C, Tannapfel A. Role of epigenetic alterations in cholangiocarcinoma. J Hepatobiliary Pancreat Surg. 2006;13(4):274-9
Berg JP, Zhou Q, Breuhahn K, Schirmacher P, Patil MA, Chen X, Schäfer N, Höller TT, Fischer HP, Büttner R, Gütgemann I. Inverse expression of Jun activation domain binding protein 1 and cell cycle inhibitor p27Kip1: influence on proliferation in
hepatocellular carcinoma. Hum Pathol. 2007 Nov;38(11):1621-7
Curia MC, Zuckermann M, De Lellis L, Catalano T, Lattanzio R, Aceto G, Veschi S, Cama A, Otte JB, Piantelli M, Mariani-Costantini R, Cetta F, Battista P. Sporadic childhood hepatoblastomas show activation of beta-catenin, mismatch repair defects and p53 mutations. Mod Pathol. 2008 Jan;21(1):7-14
This article should be referenced as such:
Enjoji M. Liver tumors: an overview. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):391-394.

Cancer Prone Disease Section Review
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 395
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
McCune Albright syndrome Margaret Zacharin
The Royal Children's Hospital, Parkville, Victoria 3052, Australia (MZ)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Kprones/McCuneAlbrightID10093.html DOI: 10.4267/2042/44482
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note McCune Albright syndrome is characterized by the triad of polyostotic fibrous dysplasia, pigmentary skin lesions and endocrinopathy.
Inheritance MAS is not inherited. It is a sporadic genetic disorder, caused by a mutation in the GNAS gene encoding the alpha subunit of the stimulatory G protein (GSalpha), cyclic AMP protein kinase dependent cellular signaling pathway involving G protein coupled receptors. An arginine or occasionally serine, leucine or glycine to histidine transposition at residue 201 attenuates GTpase activity. This results in constitutive activation of adenylyl cyclase. The somatic mutation occurs in early embryogenesis, resulting in widespread tissue distribution of abnormalities. The post zygotic mutation is responsible for the mosaic pattern of tissue distribution and the extreme variability of clinical changes, varying from multi system disease to almost unrecognized disorders with single organ involvement. Increased adenylate cyclase activity in bone from clinical fibrous dysplastic lesions is caused by expression of Cfos proto-oncogene in bone. Recent identification of increased fibroblast growth factor (FGF23) activity in fibrous dysplastic lesions has linked the bony abnormalities to a recognized marker of bone metabolism.
Clinics Phenotype and clinics The phenotype of MAS is extremely varied, ranging from multisystem disease, to minimal single organs being affected.
Fibrous dysplasia is the characteristic lesion seen in MAS, the bone lesion being of marrow stromal cells of osteogenic lineage, with increasing cyclic AMP up regulating osteogenic cells to osteoblasts within the fibrous dysplastic cells, compared to normal woven bone. Cartilaginous islands with woven bone and immature mesenchymal cells are found in the lesions, with resultant increased bone fragility in affected areas. Lesions may be polyostotic, panostotic or monostotic, with increased risk for long bone fractures, shepherd's crook deformity of proximal long bones and spinal compression fractures. Osteomalacia complicates 50% of fibrous dysplasia bone lesions, due to increased FGF23 activity resulting in phosphaturia. Café au lait marks with a coast of Maine appearance follow a dermatomal distribution along the lines of Blaschko. The activating GSalpha mutation in skin involves tyrosinase gene activation in affected melanocytes. Similar pigmentation is seen in oral mucosa. Endocrinopathies The endocrine events most commonly seen are gonadotrophin independent precocious puberty, thyrotoxicosis and Cushing syndrome. Gonadotrophin independent precocious puberty in girls is seen in at least 30%, presenting with premature thelarche. Progress is often intermittent and characterized by suppressed gonadotrophins and elevated oestrogen levels, confirming the ovarian source of the disorder. Ovarian cysts are commonly seen. Continuous oestrogen production may result in long term continuing menstrual abnormalities and infertility. Male precocious puberty is less common, seen in 15%. Macro-orchidism without precocity is more common and may be unilateral or bilateral, often with excess Sertoli cell hyperactivity. Testicular microlithiasis is present in 62% compared with a normal population microlithiasis rate of 5%.

McCune Albright syndrome Zacharin M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 396
Thyroid disease has been described in association with nodular and diffuse goitres, single toxic adenoma and hyperthyroidism with T3 toxicosis, with an overall prevalence of 30%. Thyroid cancer has only rarely been described. Clinical difficulty in detection of hyperthyroidism in the presence of a hyperdynamic circulation due to polyostotic fibrous dysplasia is significant, with biochemical evaluation prior to surgery suggested to reduce the risk of thyroid storm. Acromegaly is reported in up to 21% of affected patients, the pattern of disease varying from the common isolated form and often being co-secretory without adenoma formation. GS alpha mutations in these lesions have been demonstrated on the maternal allele. Cushing syndrome Macro nodular adrenocortical hyperplasia is the typical feature, with various outcomes reported, from spontaneous resolution to a severe neonatal presentation. Upper gastrointestinal polyps are now identified in association with MAS, with the typical hamartomatous appearance similar to Peutz Jegher syndrome polyps. These may be in association with oral melanotic pigmentation or independent of pigmentary changes. Overlap in clinical features between disorders associated with multiple endocrine disease such as Carney complex and Peutz Jegher syndrome is evident. Phosphaturia with associated hypophosphataemia may require oral phosphate and calcitriol. No outcome data has been reported. Surgical removal of FD lesions has been observed to decrease phosphate wasting.
Neoplastic risk Café au lait skin lesions are benign Fibrous dysplastic lesions can undergo malignant sarcomatous transformation, most commonly in cranio-facial bones. Other rare sarcomas include angiosarcoma, liposclerosing myxoma and chondrosarcoma. Of those patients who have developed sarcoma within FD lesions, 46% had received prior radiation treatment in the affected field (for acromegaly).NB Increased sensitivity of FD lesions to metaplasia after radiation has cause for concern for treatment planning strategies Thyroid cancer has only rarely been reported. Testicular Sertoli and Leydig cell tumours have both been described, but are rare. Ovarian hyperfunction is associated with ovarian cysts but are benign. Long term excess oestrogen secretion might increase the risk for breast cancer, particularly in the presence of growth hormone excess. Growth hormone excess with acromegaly is benign but care is required with treatment planning strategies in view of excess radiation risk in an area affected with fibrous dysplasia.
Treatment Fibrous dysplasia can be treated with bisphosphonates. These drugs are well tolerated and
reduce bone pain and bone turnover. Overall impact on the course of the disease is unclear, with minimal reduction in long term fracture risk and variable reports of possible reduction in lesional size in adults. Bisphosphonate use in children has not been shown to arrest uncontrolled expansion of dysplastic lesions in long bones or to change histomorphology in treated children or adolescents. Dental extractions and restorations do not exacerbate FD lesions. Surgical interventions using a combined approach, involving medullary rodding and bisphosphonate have been shown to improve surgical outcomes.Optic canal decompression in fibrous dysplasia of the sphenoid should be confined to surgical intervention for uncontrolled compression of visual or other nerve pathways. Precocious puberty in girls. Treatment is complex with escape from effect of aromatase inhibitors. Selective oestrogen receptor modulators have been reported to be effective but with similar escape phenomena. Secondary activation of the hypothalamic pituitary ovarian axis in response to persistent oestrogen exposure may require addition of GRNH analogue. Surgery for removal of a cystic ovary or laparoscopic cystectomy has been occasionally effective. Oophorectomy is not recommended as fertility is potentially normal. Precocious puberty in boys. Aromatase inhibitors or androgen blockade have been utilized with variable outcome. GNRH analogues may be required for secondary activation of the hypothalamic pituitary axis. Acromegaly. Management is difficult due to lack of a discrete lesion, limited access due to sphenoid wing fibrous dysplasia and radiation risk to dysplastic areas. Somatostatin and dopamine agonists have been used with variable outcomes.
Prognosis Morbidity is most commonly related to complications of polyostotic fibrous dysplasia and the need for orthopaedic intervention. Multiple lower limb fractures and bilateral hip shepherd's crook deformity frequently result in limited locomotion in adulthood, for severely affected individuals. Endocrinopathies are amenable to intervention, but management strategies are limited by effectiveness of medical interventions and radiation related risk. Excess mortality risk is related to malignancy risk and occasionally to high output cardiac failure or cardiomyopathy.
Genes involved and proteins GNAS Alias gsp oncogene
Location 20q13

McCune Albright syndrome Zacharin M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 397
Note Mutations of gsp are readily identified in lesional tissue from affected individuals with enhanced detection by multiple rounds of nested PCR and by including a peptide nucleic acid (PNA) in the PCR to block amplification of wild type GNAS targets. Peripheral Blood gsp detection is similarly enhanced, using PNA clamping. Protein expression: The GNAS locus is under complex imprinting control. GNAS encodes GS alpha expressed from maternal and paternal alleles in most tissues, with preferential expression of the maternal allele in kidney, thyroid and pituitary somatotrophs. Transcripts upstream from Exon 1 are expressed only from the paternal allele. Other transcripts 38 kb upstream from exon 1 encode 2 proteins, XLalphas and ALEX and a transcript 52 kb upstream of exon 1, encode distinct proteins that may affect signal transduction. The latter is expressed exclusively from the maternal allele, encoding a neurosecretory protein, NESP55. Gsalpha expression from the maternal allele will result in pathophysiological abnormality in tissues where that allele is expressed, but paternally expressed GNAS alleles may also result in endocrine dysfunction. Imprinting suppressing expression of paternal GNAS allele in some patients may result in a more severe phenotype. Mutations occurring later in embryogenesis are likely to give rise to fewer mutant cells and a milder phenotype.
References Bajpai A, Zacharin M. Gastrointestinal polyps in McCune Albright syndrome: Expanding the spectrum of a well known disorder Submitted for publication
PRAY LG. Sexual precocity in females; report of two cases, with arrest of precocity in the McCune-Albright syndrome after removal of a cystic ovary. Pediatrics. 1951 Nov;8(5):684-92
GORLIN RJ, CHAUDHRY AP. Oral melanotic pigmentation in polyostotic fibrous dysplasia, Albright's syndrome. Oral Surg Oral Med Oral Pathol. 1957 Aug;10(8):857-62
Bowerman JE. Polyostotic fibrous dysplasia with oral melanotic pigmentation. Br J Oral Surg. 1969 Mar;6(3):188-91
Danon M, Robboy SJ, Kim S, Scully R, Crawford JD. Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr. 1975 Dec;87(6 Pt 1):917-21
Dent CE, Gertner JM. Hypophosphataemic osteomalacia in fibrous dysplasia. Q J Med. 1976 Jul;45(179):411-20
Joishy SK, Morrow LB. McCune-Albright syndrome associated with a functioning pituitary chromophobe adenoma. J Pediatr. 1976 Jul;89(1):73-5
Foster CM, Ross JL, Shawker T, Pescovitz OH, Loriaux DL, Cutler GB Jr, Comite F. Absence of pubertal gonadotropin secretion in girls with McCune-Albright syndrome. J Clin Endocrinol Metab. 1984 Jun;58(6):1161-5
Wierman ME, Beardsworth DE, Mansfield MJ, Badger TM, Crawford JD, Crigler JF Jr, Bode HH, et al. Puberty without
gonadotropins. A unique mechanism of sexual development. N Engl J Med. 1985 Jan 10;312(2):65-72
Laue L, Kenigsberg D, Pescovitz OH, Hench KD, Barnes KM, Loriaux DL, Cutler GB Jr. Treatment of familial male precocious puberty with spironolactone and testolactone. N Engl J Med. 1989 Feb 23;320(8):496-502
Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E, Spiegel AM. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N Engl J Med. 1991 Dec 12;325(24):1688-95
Yoshimoto M, Nakayama M, Baba T, Uehara Y, Niikawa N, Ito M, Tsuji Y. A case of neonatal McCune-Albright syndrome with Cushing syndrome and hyperthyroidism. Acta Paediatr Scand. 1991 Oct;80(10):984-7
Lawless ST, Reeves G, Bowen JR. The development of thyroid storm in a child with McCune-Albright syndrome after orthopedic surgery. Am J Dis Child. 1992 Sep;146(9):1099-102
Schwindinger WF, Francomano CA, Levine MA. Identification of a mutation in the gene encoding the alpha subunit of the stimulatory G protein of adenylyl cyclase in McCune-Albright syndrome. Proc Natl Acad Sci U S A. 1992 Jun 1;89(11):5152-6
Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 7-1993. A six-year-old boy with multiple bone lesions, repeated fractures, and sexual precocity. N Engl J Med. 1993 Feb 18;328(7):496-502
Feuillan PP, Jones J, Cutler GB Jr. Long-term testolactone therapy for precocious puberty in girls with the McCune-Albright syndrome. J Clin Endocrinol Metab. 1993 Sep;77(3):647-51
Boston BA, Mandel S, LaFranchi S, Bliziotes M. Activating mutation in the stimulatory guanine nucleotide-binding protein in an infant with Cushing's syndrome and nodular adrenal hyperplasia. J Clin Endocrinol Metab. 1994 Sep;79(3):890-3
Michiels FM, Caillou B, Talbot M, Dessarps-Freichey F, Maunoury MT, Schlumberger M, Mercken L, et al. Oncogenic potential of guanine nucleotide stimulatory factor alpha subunit in thyroid glands of transgenic mice. Proc Natl Acad Sci U S A. 1994 Oct 25;91(22):10488-92
Shenker A, Weinstein LS, Sweet DE, Spiegel AM. An activating Gs alpha mutation is present in fibrous dysplasia of bone in the McCune-Albright syndrome. J Clin Endocrinol Metab. 1994 Sep;79(3):750-5
Candeliere GA, Glorieux FH, Prud'homme J, St-Arnaud R. Increased expression of the c-fos proto-oncogene in bone from patients with fibrous dysplasia. N Engl J Med. 1995 Jun 8;332(23):1546-51
Ringel MD, Schwindinger WF, Levine MA. Clinical implications of genetic defects in G proteins. The molecular basis of McCune-Albright syndrome and Albright hereditary osteodystrophy. Medicine (Baltimore). 1996 Jul;75(4):171-84
Yamamoto T, Ozono K, Kasayama S, Yoh K, Hiroshima K, Takagi M, Matsumoto S, Michigami T, Yamaoka K, Kishimoto T, Okada S. Increased IL-6-production by cells isolated from the fibrous bone dysplasia tissues in patients with McCune-Albright syndrome. J Clin Invest. 1996 Jul 1;98(1):30-5
Riminucci M, Fisher LW, Shenker A, Spiegel AM, Bianco P, Gehron Robey P. Fibrous dysplasia of bone in the McCune-Albright syndrome: abnormalities in bone formation. Am J Pathol. 1997 Dec;151(6):1587-600
Hayward BE, Kamiya M, Strain L, Moran V, Campbell R, Hayashizaki Y, Bonthron DT. The human GNAS1 gene is imprinted and encodes distinct paternally and biallelically

McCune Albright syndrome Zacharin M
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 398
expressed G proteins. Proc Natl Acad Sci U S A. 1998 Aug 18;95(17):10038-43
Kim IS, Kim ER, Nam HJ, Chin MO, Moon YH, Oh MR, Yeo UC, Song SM, Kim JS, Uhm MR, Beck NS, Jin DK. Activating mutation of GS alpha in McCune-Albright syndrome causes skin pigmentation by tyrosinase gene activation on affected melanocytes. Horm Res. 1999;52(5):235-40
Kirk JM, Brain CE, Carson DJ, Hyde JC, Grant DB. Cushing's syndrome caused by nodular adrenal hyperplasia in children with McCune-Albright syndrome. J Pediatr. 1999 Jun;134(6):789-92
Bianco P, Riminucci M, Majolagbe A, Kuznetsov SA, Collins MT, Mankani MH, Corsi A, Bone HG, et al. Mutations of the GNAS1 gene, stromal cell dysfunction, and osteomalacic changes in non-McCune-Albright fibrous dysplasia of bone. J Bone Miner Res. 2000 Jan;15(1):120-8
Cast JE, Nelson WM, Early AS, Biyani S, Cooksey G, Warnock NG, Breen DJ. Testicular microlithiasis: prevalence and tumor risk in a population referred for scrotal sonography. AJR Am J Roentgenol. 2000 Dec;175(6):1703-6
Chapurlat RD, Meunier PJ. Fibrous dysplasia of bone. Baillieres Best Pract Res Clin Rheumatol. 2000 Jun;14(2):385-98
Collins MT, Shenker A. MCune Albright syndrome: new insights. Curr Opin Endocrinol Diabetes 2000; 6: 119-125.
Coutant R, Lumbroso S, Rey R, Lahlou N, Venara M, Rouleau S, Sultan C, Limal JM. Macroorchidism due to autonomous hyperfunction of Sertoli cells and G(s)alpha gene mutation: an unusual expression of McCune-Albright syndrome in a prepubertal boy. J Clin Endocrinol Metab. 2001 Apr;86(4):1778-81
Laven JS, Lumbroso S, Sultan C, Fauser BC. Dynamics of ovarian function in an adult woman with McCune--Albright syndrome. J Clin Endocrinol Metab. 2001 Jun;86(6):2625-30
Peterson AC, Bauman JM, Light DE, McMann LP, Costabile RA. The prevalence of testicular microlithiasis in an asymptomatic population of men 18 to 35 years old. J Urol. 2001 Dec;166(6):2061-4
Lee JS, FitzGibbon E, Butman JA, Dufresne CR, Kushner H, Wientroub S, Robey PG, Collins MT. Normal vision despite narrowing of the optic canal in fibrous dysplasia. N Engl J Med. 2002 Nov 21;347(21):1670-6
Riminucci M, Collins MT, Lala R, Corsi A, Matarazzo P, Gehron Robey P, Bianco P. An R201H activating mutation of the GNAS1 (Gsalpha) gene in a corticotroph pituitary adenoma. Mol Pathol. 2002 Feb;55(1):58-60
Akintoye SO, Lee JS, Feimster T, Booher S, Brahim J, Kingman A, Riminucci M, Robey PG, Collins MT. Dental characteristics of fibrous dysplasia and McCune-Albright syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003 Sep;96(3):275-82
Collins MT, Sarlis NJ, Merino MJ, Monroe J, Crawford SE, Krakoff JA, Guthrie LC, Bonat S, Robey PG, Shenker A. Thyroid carcinoma in the McCune-Albright syndrome: contributory role of activating Gs alpha mutations. J Clin Endocrinol Metab. 2003 Sep;88(9):4413-7
Fragoso MC, Domenice S, Latronico AC, Martin RM, Pereira MA, Zerbini MC, Lucon AM, Mendonca BB. Cushing's syndrome secondary to adrenocorticotropin-independent macronodular adrenocortical hyperplasia due to activating mutations of GNAS1 gene. J Clin Endocrinol Metab. 2003 May;88(5):2147-51
Matsuba A, Ogose A, Tokunaga K, Kawashima H, Hotta T, Urakawa S, Umezu H, Higuchi T, Endo N. Activating Gs alpha mutation at the Arg201 codon in liposclerosing myxofibrous tumor. Hum Pathol. 2003 Nov;34(11):1204-9
Plotkin H, Rauch F, Zeitlin L, Munns C, Travers R, Glorieux FH. Effect of pamidronate treatment in children with polyostotic fibrous dysplasia of bone. J Clin Endocrinol Metab. 2003 Oct;88(10):4569-75
Huston TL, Simmons RM. Ductal carcinoma in situ in a 27-year-old woman with McCune-Albright syndrome. Breast J. 2004 Sep-Oct;10(5):440-2
Leet AI, Chebli C, Kushner H, Chen CC, Kelly MH, Brillante BA, Robey PG, Bianco P, Wientroub S, Collins MT. Fracture incidence in polyostotic fibrous dysplasia and the McCune-Albright syndrome. J Bone Miner Res. 2004 Apr;19(4):571-7
Matarazzo P, Lala R, Andreo M, Einaudi S, Altare F, Viora E, Buzi F, De Luca F, De Sanctis V, Rigon F, Wasniewska M, de Sanctis L, de Sanctis C. McCune-Albright syndrome: persistence of autonomous ovarian hyperfunction during adolescence and early adult age. J Pediatr Endocrinol Metab. 2006 May;19 Suppl 2:607-17
Metzler M, Luedecke DK, Saeger W, Grueters A, Haberl H, Kiess W, Repp R, Rascher W, Doetsch J. Low prevalence of Gs alpha mutations in śomatotroph adenomas of children and adolescents. Cancer Genet Cytogenet. 2006 Apr 15;166(2):146-51
Wasniewska M, Matarazzo P, Weber G, Russo G, Zampolli M, Salzano G, Zirilli G, Bertelloni S. Clinical presentation of McCune-Albright syndrome in males. J Pediatr Endocrinol Metab. 2006 May;19 Suppl 2:619-22
Mieszczak J, Lowe ES, Plourde P, Eugster EA. The aromatase inhibitor anastrozole is ineffective in the treatment of precocious puberty in girls with McCune-Albright syndrome. J Clin Endocrinol Metab. 2008 Jul;93(7):2751-4
This article should be referenced as such:
Zacharin M. McCune Albright syndrome. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):395-398.

Case Report Section Paper co-edited with the European LeukemiaNet
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 399
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Dic(1;15)(p11;p11) as a non-random abnormality in essential thrombocytemia Olivier Theisen, Steven Richebourg, Jean-Luc Lai, Catherine Roche-Lestienne
Laboratoire de Genetique Medicale, Hopital Jeanne de Flandre, CHRU de Lille, France (OT), Institut de Recherche sur le Cancer, Centre JP Aubert, Unite Inserm 837, Lille, France (SR), Institut de Recherche sur le Cancer, Centre JP Aubert, Unite Inserm 837, Lille, France (JLL, CRL)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Reports/dic115inETRocheID100036.html DOI: 10.4267/2042/44483
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics Age and sex 74 years old female patient.
Previous history No preleukemia; No previous malignancy; No inborn condition of note.
Organomegaly No hepatomegaly, no splenomegaly, no enlarged lymph nodes, no central nervous system involvement.
Blood WBC: 16.4X 109/l HB: 16.3g/dl Platelets: 872X 109/l Blasts: 0%
Cyto-Pathology Classification Cytology: -
Immunophenotype: -
Rearranged Ig Tcr: - Pathology: MPD
Electron microscopy: - Diagnosis: Essential Thrombocytemia
Survival Date of diagnosis: 03-1997
Treatment: Hydroxyurea
Complete remission: no Treatment related death: no Relapse: no Status: Death. Last follow up: 02-2008
Survival: 131 months
Karyotype Sample: Bone marrow
Culture time: 48h
Banding: GTG
Results 46,XX,[3]/46,XX,-15,+dic(1;15)(p11;p11)[10]
Karyotype at Relapse: NA
Other molecular cytogenetics technics: NA
Other Molecular Studies Technics: NA
Other Findings Note: NA
Karyotype at diagnosis presenting the dic(1;15)(p11;p11) as sole abnormality.

Dic(1;15)(p11;p11) as a non-random abnormality in essential thrombocytemia Theisen O, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 400
Comments This is an additional MPD case presenting this recurrent abnormality, with 11 years survival. However the death is not related to the disease (cardiac failure) in this case.
This article should be referenced as such:
Theisen O, Richebourg S, Lai JL, Roche-Lestienne C. Dic(1;15)(p11;p11) as a non-random abnormality in essential thrombocytemia. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):399-400.

Case Report Section Paper co-edited with the European LeukemiaNet
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 401
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Dic(1;15)(p11;p11) as a non-random abnormality in Myelodysplasic syndrome Olivier Theisen, Steven Richebourg, Jean-Luc Lai, Catherine Roche-Lestienne
Laboratoire de Genetique Medicale, Hopital Jeanne de Flandre, CHRU de Lille, France (OT), Institut de Recherche sur le Cancer, Centre JP Aubert, Unite Inserm 837, Lille, France (SR), Institut de Recherche sur le Cancer, Centre JP Aubert, Unite Inserm 837, Lille, France (JLL, CRL)
Published in Atlas Database: May 2008
Online updated version : http://AtlasGeneticsOncology.org/Reports/dic115inMyelodRocheID100037.html DOI: 10.4267/2042/44484
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2009 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics Age and sex 76 female patient.
Previous history No preleukemia; No previous malignancy; No inborn condition of note.
Organomegaly No hepatomegaly, no splenomegaly, no enlarged lymph nodes, no central nervous system involvement.
Blood WBC: 6.7X 109/l HB: 7.5g/dl Platelets: 450X 109/l Blasts: 0% Bone marrow: 52 ringed sideroblast (Perls staining).
Cyto-Pathology Classification Cytology: -
Immunophenotype: -
Rearranged Ig Tcr: -
Electron microscopy: - Diagnosis: Myelodysplastic syndrome (MDS): refractory anemia with ringed sideroblast (RARS).
Survival Date of diagnosis: 05-1994
Treatment: Norethandrolone Complete remission was obtained. Treatment related death: no Relapse: no Status: Death. Last follow up: 04-1997
Survival: 37 months
Karyotype Sample: Bone marrow
Culture time: 48h
Banding: RHG
Results 46,XX,[3]/47,XX,+8[3]/47,XX,+8,-15,+dic(1;15)(p11;p11)[8]
Other molecular cytogenetics technics: NA
Other Molecular Studies Technics: NA
Other Findings Note: NA
Comments This is an MDS case presenting this recurrent abnormality, with a 3 years survival. In this case the death is not related to disease (non-small cell lung carcinoma).

Dic(1;15)(p11;p11) as a non-random abnormality in Myelodysplasic syndrome Theisen O, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 402
This article should be referenced as such:
Theisen O, Richebourg S, Lai JL, Roche-Lestienne C. Dic(1;15)(p11;p11) as a non-random abnormality in Myelodysplasic syndrome. Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5):401-402.
Partial karyotype at diagnosis presenting the dic(1;15)(p11;p11) associated with trisomy 8.

Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Instructions to Authors Manuscripts submitted to the Atlas must be submitted solely to the Atlas. Iconography is most welcome: there is no space restriction. The Atlas publishes "cards", "deep insights", "case reports", and "educational items". Cards are structured review articles. Detailed instructions for these structured reviews can be found at: http://AtlasGeneticsOncology.org/Forms/Gene_Form.html for reviews on genes, http://AtlasGeneticsOncology.org/Forms/Leukaemia_Form.html for reviews on leukaemias, http://AtlasGeneticsOncology.org/Forms/SolidTumour_Form.html for reviews on solid tumours, http://AtlasGeneticsOncology.org/Forms/CancerProne_Form.html for reviews on cancer-prone diseases. According to the length of the paper, cards are divided, into "reviews" (texts exceeding 2000 words), "mini reviews" (between), and "short communications" (texts below 400 words). The latter category m ay not be accepted for indexing by bibliographic databases. Deep Insights are written as traditional papers, made of paragraphs with headings, at the author's convenience. No length restriction. Case Reports in haematological malignancies are dedicated to recurrent -but rare- chromosomes abnormalities in leukaemias/lymphomas. Cases of interest shall be: 1- recurrent (i.e. the chromosome anomaly has already been described in at least 1 case), 2- rare (previously described in less than 20 cases), 3- with well documented clinics and laboratory findings, and 4- with iconography of chromosomes. It is mandatory to use the specific "Submission form for Case reports": see http://AtlasGeneticsOncology.org/Reports/Case_Report_Submission.html. Educational Items must be didactic, give full information and be accompanied with iconography. Translations into French, German, Italian, and Spanish are welcome.
Subscription: The Atlas is FREE!
Corporate patronage, sponsorship and advertising Enquiries should be addressed to [email protected].
Rules, Copyright Notice and Disclaimer Conflicts of Interest: Authors must state explicitly whether potential conflicts do or do not exist. Reviewers must disclose to editors any conflicts of interest that could bias their opinions of the manuscript. The editor and the editorial board members must disclose any potential conflict. Privacy and Confidentiality – Iconography: Patients have a right to privacy. Identifying details should be omitted. If complete anonymity is difficult to achieve, informed consent should be obtained. Property: As "cards" are to evolve with further improvements and updates from various contributors, the property of the cards belongs to the editor, and modifications will be made without authorization from the previous contributor (who may, nonetheless, be asked for refereeing); contributors are listed in an edit history manner. Authors keep the rights to use further the content of their papers published in the Atlas, provided that the source is cited. Copyright: The information in the Atlas of Genetics and Cytogenetics in Oncology and Haematology is issued for general distribution. All rights are reserved. The information presented is protected under international conventions and under national laws on copyright and neighbouring rights. Commercial use is totally forbidden. Information extracted from the Atlas may be reviewed, reproduced or translated for research or private study but not for sale or for use in conjunction with commercial purposes. Any use of information from the Atlas should be accompanied by an acknowledgment of the Atlas as the source, citing the uniform resource locator (URL) of the article and/or the article reference, according to the Vancouver convention. Reference to any specific commercial products, process, or service by trade name, trademark, manufacturer, or otherwise, does not necessarily constitute or imply its endorsement, recommendation, or favouring. The views and opinions of contributors and authors expressed herein do not necessarily state or reflect those of the Atlas editorial staff or of the web site holder, and shall not be used for advertising or product endorsement purposes. The Atlas does not make any warranty, express or implied, including the warranties of merchantability and fitness for a particular purpose, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of any information, and shall not be liable whatsoever for any damages incurred as a result of its use. In particular, information presented in the Atlas is only for research purpose, and shall not be used for diagnosis or treatment purposes. No responsibility is assumed for any injury and/or damage to persons or property for any use or operation of any methods products, instructions or ideas contained in the material herein. See also: "Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication - Updated October 2004": http://www.icmje.org.
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Dic(1;15)(p11;p11) as a non-random abnormality in Myelodysplasic syndrome Theisen O, et al.
Atlas Genet Cytogenet Oncol Haematol. 2009; 13(5) 404


















