Vocational - WordPress.com€¦ · Web viewLifting, though she coped ... (keyboarding and mouse)...
67
Vocational Medical Assessors Contract Operational Guidelines
Transcript of Vocational - WordPress.com€¦ · Web viewLifting, though she coped ... (keyboarding and mouse)...

Vocational Medical Assessors
Contract
Operational Guidelines
October 2008

Vocational Medical Assessors – Operational Guidelines
This is a living document and will be updated as required.

Vocational Medical Assessors – Operational Guidelines
Contents
Introduction.......................................................................................................................1Role of ACC.....................................................................................................................1Purpose of the guidelines...............................................................................................1Injury and non-injury considerations...............................................................................1Definition of rehabilitation..............................................................................................2Individual rehabilitation plan (IRP)..................................................................................2Discussing recommendations with the client..................................................................3
About Vocational Rehabilitation.........................................................................................3Purpose of vocational rehabilitation...............................................................................3Qualifications required for Occupational Assessors........................................................4Qualifications required for Medical Assessors.................................................................4Key terms used in vocational rehabilitation....................................................................5
The Initial Assessments (IOA and IMA)...............................................................................7Initial Occupational Assessment (IOA)............................................................................7Initial Medical Assessment (IMA)....................................................................................7
Reporting on the Initial Assessments (IOA and IMA)...........................................................8Initial Occupational Assessment (IOA) Report.................................................................8Initial Medical Assessment (IMA) Report.........................................................................9
The Vocational Independence Assessments (VIOA and VIMA)..........................................10Vocational Independence Occupational Assessment (VIOA).........................................10Vocational Independence Medical Assessment (VIMA).................................................10
Reporting on the Vocational Independence Assessments (VIOA and VIMA).....................11Vocational Independence Occupational Assessment (VIOA) Report..............................11Vocational Independence Medical Assessment (VIMA) Report......................................12Medical report quality check by Branch Medical Advisor..............................................12
The Steps in the Medical Assessment Process.................................................................13Step 1 – Background information from ACC..................................................................13Step 2 – Clinical examination........................................................................................14Step 3 – The medical report..........................................................................................14Step 4 – Recommendations..........................................................................................14
Appendices......................................................................................................................16Appendix 1: Relevant Legislation..................................................................................16Appendix 2: Vocational Services...................................................................................22
October 2008

Vocational Medical Assessors – Operational Guidelines
Appendix 3: Vocational Paths.......................................................................................27Maintain employment..............................................................................................27Obtain employment.................................................................................................28Regain or acquire vocational independence............................................................29
Appendix 4: Example - Initial Medical Assessment Report............................................31Appendix 5: Example - Vocational Independence Medical Assessment........................39Appendix 6: Example - Work Type Detail Sheet............................................................46Appendix 7: US Department of Labor Physical Demand Characteristics of Work..........47Appendix 8: Frequently Asked Questions (FAQs)..........................................................48Appendix 9: Flowchart of Client Participation in Vocational Rehabilitation...................50
October 2008
Vocational Medical Assessors – Operational Guidelines
Introduction
Welcome to the Vocational Medical Assessors’ Operational Guidelines. This document gives information on carrying out initial and vocational independence medical assessments for the vocational rehabilitation programme.
It is designed to help ACC-contracted medical assessors: Assess a client’s capacity for vocational rehabilitation, including recommendations for
further treatment or rehabilitation, or Assess whether ACC has completed vocational and medical rehabilitation and the
client has the capacity to work.
Role of ACC
ACC is responsible for determining clients’ eligibility and entitlements in a fast effective way to help them achieve maximum independence. ACC may not take into account the age limits for weekly compensation when deciding whether vocational rehabilitation will be cost effective. All applications for vocational rehabilitation beyond three years and beyond 65 years of age are considered on their merit. Applications for vocational rehabilitation longer than three years are initially received by client service staff who will then complete a submission for consideration by the Team Manager/Branch Manager. The application is then referred to the Customer Service Technical Support Team for consideration and they will make a recommendation which will be sent back to the client service staff member.
Purpose of the guidelines
The purpose of the guidelines is to: Achieve consistency in the approach to assessments and report writing Provide information to assessors about ACC’s rehabilitation model and legislative
framework.
Injury and non-injury considerations
In preparing the IMA and VIMA report the medical assessor must take into account any condition suffered by the client that is not related to their personal injury. This means that the IRP can be prepared taking into account any non-injury factors. Thus the question of medical sustainability must reference any non-injury factors present.
However, it may be that the non-injury factors that were taken into account at the IMA, and considered when developing the IRP, have changed during the course of rehabilitation. It could also be that new non-injury conditions have developed since the IMA was completed. In this case the IRP would be amended. Assessors completing the VIMA need to reference this specifically when commenting on the client’s capacity to undertake work.
Definition of rehabilitation
October 2008 Page 1 of 50

Vocational Medical Assessors – Operational Guidelines
The focus of this guideline is vocational rehabilitation. Other rehabilitation consists of treatment, social rehabilitation, and assorted ancillary
services such as transport.
Treatment includes: Social rehabilitation includes:
Ancillary services include:
Physical rehabilitation Cognitive rehabilitation An examination for the
purpose of providing a certificate to ACC (such as a medical certificate for time off work).
ACC funds the provision of treatment through:
Reimbursing treatment providers for their treatment consultations and procedures, according to the Accident Insurance (Insurer’s Liability to Pay Costs of Treatment) Regulations 1999
Providing bulk funding to the Crown for emergency department, acute inpatient and follow-up medical outpatient services
Buying treatment services (such as elective surgery) under contract
Paying for pharmaceuticals prescribed for ACC covered injuries.
Communication Home help, child care
and attendant care Aids and appliances, eg.
wheelchairs and walking frames
Educational participation Training for
independence programmes
Financial management Health care Hygiene care Mobility Motivation Safety management Sexuality Cognitive tasks of daily
living Modifications to the home
or personal transport.Social rehabilitation helps clients regain as much pre-injury independence as possible in everyday life skills.
Transport to and from rehabilitation appointments
Support people
Rehabilitation aims to help restore to the maximum practicable extent a client’s health, independence, and participation.
Individual rehabilitation plan (IRP)
All clients are required to have an IRP completed if they are likely to need social or vocational rehabilitation for 13 weeks or more following an injury. These plans are negotiated with the client and may include input from employers and the client’s doctor and family. Included in these plans are: Planned assessments. Outcomes for treatment, social, and vocational rehabilitation.These plans are signed by both the client and ACC’s client service staff. Vocational assessments by either the occupational or medical assessor can be included in the plans
October 2008 Page 2 of 50
Vocational Medical Assessors – Operational Guidelines
as well as the agreed rehabilitation that will be arranged for the clients. The assessments are vital to setting goals and planning rehabilitation. IRPs are updated when necessary and form an important agreement between ACC and clients.
Discussing recommendations with the client
The assessment procedure must follow the principles of natural justice. One of these principles is the client’s right to a fair hearing. A client may have a support person present during their assessment. Clients also occasionally request a tape recording of the session. Clients should arrange this with the assessor prior to the assessment. In these cases the medical assessor may also arrange to either retain a copy of the tape or also record the session.
Client commentsWhen the assessor has completed the clinical examination component, they should discuss their findings and the recommendations they are considering with the client and ask them for their comments. It is important that the client has the opportunity to discuss any issues they have concerning their injury and the occupations. Client comments must be included for each work type.
Note: The AC Act requires a copy of the assessment to be given to the client by their client service staff member.
About Vocational Rehabilitation
Purpose of vocational rehabilitation
Vocational rehabilitation is designed to help a client: Maintain or obtain employment, or Regain or acquire vocational independence. See also Part 4 section 80 of the AC Act for the scope of vocational rehabilitation.
If a client needs vocational rehabilitation ACC will provide the entitlements and interventions, and support the client in their employment or their ability to become employed which will help them earn an income and so contribute to an appropriate quality of life for them. The employment must be: Suitable for the client (in terms of their capacity to function) Appropriate for the client’s levels of training, experience, and qualifications.
In practical terms, ACC gives comprehensive vocational rehabilitation services that: Focus on the client’s needs. Address any injury-related barriers to the client’s independence that prevent their
participation in work environments.Additional information for providers is contained on ACC’s website www.acc.co.nz and covers information about injury prevention, levies & cover, and claims.
October 2008 Page 3 of 50

Vocational Medical Assessors – Operational Guidelines
Vocational assessments are required by ACC: Whenever a client is deemed to need vocational rehabilitation as described as
required (Part 4, section 89, AC Act). Where new employment or vocational independence is being considered.
Qualifications required for Occupational Assessors
Section 90 of the AC Act states: “An occupational assessment must be undertaken by an assessor whom the Corporation considers has the appropriate qualifications and experience to do the assessment required in the particular case.”
Each approved assessor must have: A tertiary qualification relevant to vocational rehabilitation (eg. occupational therapy,
rehabilitation, psychology, career counselling, social work, human resource management).
At least two years’ relevant experience in providing vocational rehabilitation services, with demonstrated excellence in service provision and an ability to work effectively with ACC.
Current full membership of a relevant professional association (eg New Zealand Association of Occupational Therapists, Career Practitioners Association of New Zealand, or New Zealand Society of Physiotherapists).
Qualifications required for Medical Assessors
Sections 93-94 of the AC Act set out the required qualifications of medical assessors:
93. Medical assessor(1) A medical assessment must be undertaken by a medical practitioner who is described in subsection (2) or subsection (3).(2) A medical practitioner who provides general medical services must also—
(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) have at least 5 years' experience in general practice; and(c) meet at least 1 of the following criteria:
(i) be a Fellow of the Royal New Zealand College of General Practitioners or hold an equivalent qualification:(ii) be undertaking training towards becoming a Fellow of the Royal New Zealand College of General Practitioners or holding an equivalent qualification(iii) have undertaken relevant advanced training.
(3) A medical practitioner who does not provide general medical services must—(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) be a member of a recognised college.]
94. Assessments when medical assessor unavailable(1) A… medical practitioner who does not qualify under section 93 may undertake a
medical assessment if the Corporation is satisfied that—(a) the circumstances in subsection (2) exist; and
October 2008 Page 4 of 50
Vocational Medical Assessors – Operational Guidelines
(b) the… medical practitioner's qualifications and experience are broadly comparable with the qualifications and experience specified in section 93.
(2) The circumstances are that—(a) a… medical practitioner who does qualify under section 93 is not available to undertake a medical assessment without unreasonable delay or unreasonable inconvenience to the claimant; and(b) the delay or inconvenience would have an adverse effect on providing vocational rehabilitation to the claimant.(3) Sections 95 and 96 apply to a… medical practitioner who qualifies under this section to undertake a medical assessment.
Key terms used in vocational rehabilitation
Independence in employmentThe purpose of vocational rehabilitation is to restore the client’s independence in their employment situation.
‘Medically sustainable’ ability to work The concept of ‘medically sustainable’ is used for the IMA and looks at whether any identified type of work is medically sustainable, ie there are no medical or treatment rehabilitation needs. It also asks if any type of work is likely to be medically sustainable, ie that after appropriate medical or treatment rehabilitation the type of work will become medically sustainable.
Medical assessors will report on medical evidence regarding a client’s ability to engage in work. This allows ACC to make a decision on vocational rehabilitation. Facts on experience, education, or training are not medical, but occupational and ACC will get this information from the occupational assessor Medical assessors must ensure they are giving an opinion that can be medically supported.
Example:A useful test in deciding whether an opinion is in fact a medical one is to put the question in a different way. This could be: if this client wanted to work in one of the types of work specified and came to you to ask advice as to whether you would provide them with medical clearance to do so, would you have a medical reason to advise them that they could not, or should not, do so?
Scope of vocational rehabilitationSee Purpose of vocational rehabilitation on pg 3.
Types of work“Types of work” refers to a broad group of jobs and roles that have a common set of work tasks and functions. For more information see Work type detail sheets in the IOA report section on page 8, and Appendix 6 on page 46 for an example.Vocational assessmentsThere are two types of assessments in the vocational rehabilitation process: initial assessments and vocational independence assessments.
Initial assessments
October 2008 Page 5 of 50
Vocational Medical Assessors – Operational Guidelines
The initial assessment process is for all clients who cannot return to their pre-injury work and require vocational rehabilitation. It is split into two parts: An initial occupational assessment (IOA) to identify the types of work that may be
appropriate for the client. An initial medical assessment (IMA) to determine whether the types of work
identified in the IOA can be medically sustainable for the client.
After these assessments the rehabilitation and treatment agreed to is included in the IRP. If the client’s circumstances change (eg their medical status or their employer’s willingness to help with their rehabilitation), the IRP is modified to reflect the change.
The vocational rehabilitation plan in the IRP will meet the client’s needs and address any injury-related barriers the client has to achieving independence in employment.
Vocational independence assessments The vocational independence assessment process will show whether a client’s rehabilitation has been completed and they are able to obtain/maintain employment or have achieved vocational independence. This assessment confirms that the client has been given comprehensive vocational rehabilitation assistance that has focused on addressing any injury-related barriers to their independence in employment. (See Appendix 1 on pg 16 for relevant legislation references.)
Once the rehabilitation specified in a client’s IRP has been completed, and if the client is receiving weekly compensation, two further assessments may be completed: The vocational independence occupational assessment (VIOA). The vocational independence medical assessment (VIMA).
These assessments will ensure that vocational independence has been achieved.
Vocational independenceVocational independence is achieved when a client has attained their rehabilitation outcome, ie they can do the work they are trained, experienced, or educated in and they can work for 35 hours per week or more.
Vocational pathsThere are three paths to enable the client to return to work or work readiness (see Part 4 section 80 (1) of the AC Act, and Appendix 3 on pg 27). The paths can be noted in the IRP, but this is not required. The three paths are: Maintain employment Obtain employment Regain or acquire vocational independence.
The Initial Assessments (IOA and IMA)
Initial Occupational Assessment (IOA)
The purpose of the IOA is to: Assess the client’s skills, experience and ability to undertake employment
October 2008 Page 6 of 50
Vocational Medical Assessors – Operational Guidelines
Identify suitable types of work for the client based on their education, experience, pre-incapacity earnings, and training
Complete a work type detail sheet for each suitable work type.
Initial Medical Assessment (IMA)
Purpose of the IMAThe purpose of the IMA is to produce a report that ACC uses to determine the client’s vocational rehabilitation needs and direction. It requires the medical assessor to consider the types of work that have been identified in the IOA and give an opinion on whether any of the types of work are, or are likely to be, medically sustainable for the client.
The tasks on the work type detail sheet must be considered against the client’s post-injury condition, and the sheets used with the Department of Labor Physical Demand Characteristics of Work (see Appendix 7 on page 47 for an example) which defines the terms used by occupational assessors and includes the terms occasional, frequent, and constant with the percentages of the workday, as well as physical demands such as sedentary, light, medium, heavy, very heavy, and the typical energy required.
If the type of work is only likely to be sustainable, the report needs to show evidence of the rehabilitation the client will need in order to carry out the identified type(s) of work.
Assessors to list their qualifications As experts it is important that medical assessors specify their qualifications. This should include all qualifications and experience relevant to the type of report they are writing. In terms of the information considered and the history obtained, the assessor should: Identify the documents sent to them by ACC or other sources, eg the client
Note: If the assessor needs more information from ACC, they should request this from the client service staff member who referred the client to them.
Detail who attended the assessment, eg support person or lawyer and what input they had, if any
Identify elements of the history given by, or obtained from, other parties Highlight any relevant inconsistencies in the history and information.
For the examination and clinical findings, medical assessors should: Document the time taken for the assessment Document all the aspects of the examination – it is easy to omit parts of the routine
clinical examination, eg pertinent normal findings Describe all tests performed – detail reduces the potential for later dispute.When commenting on the types of work, medical assessors should: Comment on the adequacy or otherwise of information provided on the tasks involved
in the types of work Focus on the generic aspects of the tasks Give reasons why a type of work is, or is not, medically sustainable – a simple list is
not sufficient Tie the reasoning back to the examination findings, the comments and input of the
client, and the information provided
October 2008 Page 7 of 50

Vocational Medical Assessors – Operational Guidelines
Include comments on the non-injury related conditions, and the impact or otherwise on medical sustainability or the client’s capacity to undertake work
Provide recommendations for treatment/rehabilitation that could assist the client in sustaining a work type, eg pain management, work trial.
The IMA must determine whether the types of work identified by the IOA are, or are likely to be, medically sustainable. This is required under Part 4 section 89 of the AC Act.
See also Qualifications required for Occupational and Medical Assessors on pg 4.
Reporting on the Initial Assessments (IOA and IMA)
Initial Occupational Assessment (IOA) Report
This assessment report identifies: The training skills required for the work types (Unit Group), and the possible individual
jobs the client could do. How the client’s current skills and abilities match these jobs. What further training/skill development may be needed.
Work type detail sheetsA work type detail sheet is completed for each of the work types identified as suitable (providing job details). A copy of this report is forwarded to the initial medical assessor, with the specific work type detail sheets. These sheets have been developed by an occupational assessor for use by assessors and aim to achieve national consistency regarding descriptions of work environments and work functions. The task requirements for these jobs may occasionally vary from the specifications and when this occurs the occupational assessor will detail any variations on the IOA work type detail sheet and the assessment report.1 See Appendix 6 on pg 46 for a work type detail sheet example.
Initial Medical Assessment (IMA) Report
OverviewBefore beginning any report, it is wise to review information that has been provided and assess whether it is adequate or whether there are gaps. If there are gaps or the information is inadequate, request clarification or further information. Do not be tempted to fill gaps with assumptions.
The body of the report should list the information considered when preparing the report, the history and clinical findings gained from the assessment, and the assessor’s opinion on the medical sustainability of each identified type of work.
1 Practitioners without current professional membership of a relevant association must demonstrate their intent to work towards this within a stated timeframe.
October 2008 Page 8 of 50
Vocational Medical Assessors – Operational Guidelines
Medical assessors are legally viewed as expert witnesses. The role of an expert witness encompasses the expectations of honesty, independence, and integrity. Further, the area of expertise is medical, not legal or occupational. Therefore, the medical assessor must constrain their opinions to those of medicine.
Report details The assessor’s report must specify: Relevant details about the client, including details of the client’s injury Relevant details about the clinical examination undertaken by the assessor, including
the methods used and the findings Results of any additional assessments of the client’s condition Information provided to them by ACC Medical reports that have been prepared for ACC Information regarding any non-injury related conditions that may impact on the
client’s ability to work Any other relevant medical reports The report of the occupational assessor – the IOA (including the work type detail
sheets) The clinical findings from their own examination Any other information or comments that the client asks the assessor to consider, that
the assessor decides are relevant.
Part 4 section 89 of the AC Act requires that the IMA contains a determination of whether the types of work identified by the IOA are, or are likely to be, medically sustainable.
The Vocational Independence Assessments (VIOA and VIMA)
Vocational Independence Occupational Assessment (VIOA)
The purpose of the vocational independence occupational assessment is to: Review how the client has progressed since their IOA, and how the vocational
rehabilitation provided to the client has helped. This may include the use of professionally recognised, objective assessment methodologies during the consultation that achieve defensible and recognised findings.
Identify suitable types of work for the client based on their education, experience, pre-incapacity earnings, and training.
October 2008 Page 9 of 50
Vocational Medical Assessors – Operational Guidelines
Vocational Independence Medical Assessment (VIMA)
The purpose of this assessment is to ascertain whether the client can do any, or all, of the work options recommended by the occupational assessor on a full-time basis, ie 35 hours a week or more. See, Part 4, section 108(3) of the AC Act.
The medical assessor also takes into account any comments from the client or their doctor, and may ask for more information, or a further assessment by a specialist, before making a recommendation.
This assessment will ensure that comprehensive vocational rehabilitation, as identified in a client’s IRP, has been completed and that it has focused on the client’s needs and addressed any injury-related barriers to enable the client to either maintain or obtain employment or regain or acquire vocational independence.
ACC can ask for a determination of a client’s vocational independence at any reasonable interval. It is usually completed when the client has finished the vocational rehabilitation set out in their IRP.
The definition of vocational independence in Part 1 section 6 of the AC Act is:“vocational independence, in relation to a claimant, means the claimant’s capacity, as determined under section 107, to engage in work—
(a) for which he or she is suited by reason of experience, education, or training, or any combination of those things; and(b) for 35 hours or more a week”
See also Qualifications required for Occupational and Medical Assessors on pg 4.
Reporting on the Vocational Independence Assessments (VIOA and VIMA)
Vocational Independence Occupational Assessment (VIOA) Report
In identifying such jobs and writing the report, the assessor will: Consider the client’s suitability as at the date of the consultation. Disregard the effects of the client’s injury on the client’s ability to work. The assessor
will not exclude jobs because they believe the client may not be able to perform them due to the client’s injury (this is the role of the vocational independence medical assessor).
Disregard job availability, geographical location, the client’s child care requirements, transportation availability, and the client’s pre-injury occupation – except when prioritising job options.
Identify and prioritise job options that most closely align with the client’s pre-injury
October 2008 Page 10 of 50

Vocational Medical Assessors – Operational Guidelines
occupation, while not limiting the jobs for which the client is suited by reason of experience, education, pre-incapacity earnings, and training.
Be realistic about job choices. Jobs must exist within the current New Zealand labour market and be full-time occupations, ie 35 hours per week or more.
The client is likely to have received a period of rehabilitation and treatment based on the initial assessments and so the VIOA will consider and report on work options that the client is able to perform the ‘next working day’.
The client will be invited to comment, make submissions, and raise any issues or concerns about their experience, education, training, pre-incapacity earnings, or potential job options. However, a client’s disagreement with some or all of the identified jobs because they are not the client’s preference is not a reason for the assessor excluding them from their recommendations. These concerns will be discussed with the client and documented.
The VIOA report includes: The client’s previous work experience The client’s education and training attainments The client’s transferable skills The identified jobs Evidence of having taken into account the client’s earnings before their incapacity,
and evidence that the assessor has used their professional expertise to source earnings information about other job types.
A summary Comments, submissions, issues and/or concerns raised by the client.
A work type detail sheet is prepared specifying the requirements of each job. See Appendix 6 on page 46 for a work type detail sheet example.
Vocational Independence Medical Assessment (VIMA) Report
Assessors to list their qualificationsAs experts it is important that medical assessors specify their qualifications specifically related to the type of report they are writing. See section, Assessors to list their qualifications on page 7.
The VIMA must determine whether the types of work listed in the VIOA are, or are likely to be, medically sustainable. This is required under Part 4 Vocational independence, sections 107-113 of the AC Act.
VIMA report detailsThe assessor must prepare and provide to ACC a report on the medical assessment that specifies: Relevant details about the client, including details of the client’s injury Relevant details about the clinical examination undertaken by the assessor, including
the methods used and the findings
October 2008 Page 11 of 50

Vocational Medical Assessors – Operational Guidelines
Results of any additional assessments of the client’s condition The assessor’s opinion of the client’s vocational independence in relation to the types
of work identified in the occupational assessor’s report Any comments made by the client to the assessor about the client’s injury and
vocational independence related to each of the types of work identified in the occupational assessor’s report
Recommendations about any medical rehabilitation that will help the client to achieve and sustain employment in any of the job options
Any conditions not related to the injury that prevent the client from having vocational independence.
When writing the report medical assessors must take into account: Information provided to them by ACC Medical reports that have been prepared for ACC prior to preparing the IRP Information regarding any non-injury related conditions that may impact on the
client’s ability to work Any other relevant medical reports The report of the occupational assessor – the VIOA (including the work type detail
sheets) The clinical findings from their examination Any other information or comments that the client requests the assessor to consider,
that the assessor decides are relevant.
Medical report quality check by Branch Medical Advisor
A quality check of the medical assessment report is completed by the branch medical advisor. This quality check ensures that the medical assessor has considered all the information provided by ACC as well as any additional information or comments provided by the client. The quality check also ensures that the medical report details: The client and their injury The clinical examination, the methods used and the clinical findings The results of any additional assessments The assessor’s opinion of the client’s vocational independence for each of the work
types identified in the occupational assessor’s report Discussion with, and comments made by, the client about each of the types of work
identified within the occupational assessor’s report Evidence that the medical assessor has identified the types of work that the client is
able to perform for 35 hours a week or more Any non-injury conditions that prevent the client from having vocational
independence and the rationale for the decision Evidence that any conditions or restrictions attached to the recommendations are
consistent with the requirements on the work type detail sheets provided by the occupational assessor
Any further medical rehabilitation identified during the assessment.
Client service staff or the branch medical advisor may contact the assessor to request clarification of aspects of the report. This may include further clarification, explanation, and correction of oversights. Any requests for changes by the client must be referred to the client service staff member.
October 2008 Page 12 of 50

Vocational Medical Assessors – Operational Guidelines
Steps in the Medical Assessment Process
Step 1 – Background information from ACC
ACC provides the following information to help the medical assessor with their assessment: A summary of the client’s injury claim and medical and occupational rehabilitation.
This will also include any factors that may impact on the assessment, for instance if the client has communication difficulties or has been identified as a potential risk to the assessor.
For VIMAs, the IRP completed by the client service staff member and client. Previous medical and occupational reports requested by ACC as part of the
rehabilitation process The occupational assessor’s report detailing the education, training and experience
the client has in relation to the identified types of work. The report lists all types of work reasonably identified as suitable for the client. It also provides in relation to each type of work the requirements, including any environmental modifications that the assessor identifies as necessary to enable the client to function safely in that type of work.
This information is to help the medical assessor become familiar with the client’s injury and interventions to date, and the types of work deemed suitable by the occupational assessor.
Step 2 – Clinical examination
The medical assessor will take a history, clinically examine and document those organ systems identified as relating to the injury and the impact of the injury in relation to the individual’s capacity to work in the identified occupations. This examination will form the basis of the report. The clinical examination must include recognised testing methodologies that will give defensible, recognised results. These results form the basis of the report and recommendations.
If the client service staff member has requested an assessment and the assessor believes that this should be considered as either a serious injury or complex assessment, the medical assessor should endeavour to discuss this with the client service staff member before proceeding with the assessment. However, if the client service staff member or other decision-maker is unavailable, proceed with the assessment and contact the client service staff member at the earliest opportunity.
Step 3 – The medical report
ACC requires a medical report from the medical assessor that identifies the facts gained from the history and the clinical examination and shows how each recommendation relates to each particular type of work. It is vital that medical assessors are objective and only report or comment on issues that have been identified in reports already provided, or revealed in the assessor’s own history taking and clinical examination of the client.
October 2008 Page 13 of 50
Vocational Medical Assessors – Operational Guidelines
This report should cover three main areas:1. The client’s details, background, and presenting situation.2. The clinical examination, noting the methods used and the findings.3. The assessor’s opinion of the sustainability of work (IMA) and the client’s vocational
independence (VIMA) based on the findings that relate to each type of work identified by the occupational assessor. The medical assessor must give reasons for their decisions, referring to their clinical findings and the specified job tasks, and concisely state the outcome, eg is the client able to do the types of work identified or not?
The written reports should follow the formats given in Appendix 4 (IMA) on pg 31, and Appendix 5 (VIMA) on pg 39.
Step 4 – Recommendations
The occupational assessor will have completed the first section of the medical report. This section will list the types of work that the client has the skills to perform because of their education, experience, or training.
The occupational assessor will have also provided a copy of the relevant work type detail sheets. These sheets provide information on work tasks, work environment, work function/activity, qualifications, and other relevant comments.
The medical assessor then completes the report and sends three copies to ACC. The client service staff member provides one copy of the report to the client, and one to the client’s GP. One copy remains on the client’s file. The report is required by ACC within eight working days of the later of the: Date of clinical examination of the client, or Date the assessor receives any additional information requested by the client service
staff member.
When conducting a VIMA the medical assessor will complete the second section of the recommendation form. The recommendation form represents a summary of both the occupational and medical assessors’ evaluation reports.
The branch medical advisor may review with the client service staff member, any issues arising from the medical assessment reports, specifically: Any further medical treatment/examinations and their relevance Illness-related issues and how these may affect vocational rehabilitation.
Notes: If further information or assessments are required before the medical assessor can
make a recommendation, the medical assessor should contact the client service staff member directly.
The medical assessor may only make one recommendation, showing their rationale, on each other of the occupation recommendations given by the occupational assessor.
October 2008 Page 14 of 50
Vocational Medical Assessors – Operational Guidelines
Further informationIf the medical assessor, having reviewed the background information and completed the clinical examination, requires additional information, they will contact the client service staff member and request the additional information before making recommendations.
October 2008 Page 15 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
APPENDICES
Appendix 1: Relevant Legislation
Accident Compensation Act 2001
Note: Legislation in square brackets is in effect from 1 October 2008.
Part 1 –Interpretation6. Vocational independence, in relation to a claimant, means the claimant’s capacity, as determined under section 107, to engage in work—
(a) for which he or she is suited by reason of experience, education, or training, or any combination of those things; and(b) for 35 hours or more a week
Part 4 - Vocational rehabilitation80. Purpose of vocational rehabilitation(1) The purpose of vocational rehabilitation is to help a claimant to, as appropriate,—
(a) maintain employment; or(b) obtain employment; or(c) regain or acquire vocational independence.
(2) Without limiting subsection (1), the provision of vocational rehabilitation includes the provision of activities for the purpose of maintaining or obtaining employment that is—
(a) suitable for the claimant; and(b) appropriate for the claimant’s levels of training and experience.
85. Corporation liable to provide vocational rehabilitation(1) The Corporation is liable to provide vocational rehabilitation to a claimant who—
(a) has suffered personal injury for which he or she has cover; and(b) is—
(i) entitled to weekly compensation; or(ii) likely, unless he or she has vocational rehabilitation, to be entitled to weekly compensation; or(iii) on parental leave.
[(2) Despite subsection (1)(b)(i), the Corporation is liable to provide vocational rehabilitation to a person who was entitled to weekly compensation and who would, but for clause 52 of Schedule 1 (relationship between weekly compensation and New Zealand superannuation), continue to be entitled to weekly compensation.]
86. Matters to be considered in deciding whether to provide vocational rehabilitation
October 2008 Page 16 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
(1) In deciding whether to provide vocational rehabilitation, the Corporation must have regard to the matters in section 87.(2) In deciding what vocational rehabilitation is appropriate for the claimant to achieve the purpose of vocational rehabilitation under section 80,—
(a) the Corporation must consider whether it is reasonably practicable to return the claimant to the same employment in which the claimant was engaged, and with the employer who was employing the claimant, when the claimant’s incapacity commenced; and(b) if it is not, the Corporation must consider the following matters:
(i) whether it is reasonably practicable to return the claimant to an employment of a different kind with that employer:(ii) whether it is reasonably practicable to return the claimant to the employment in which the claimant was engaged when the claimant’s incapacity commenced, but with a different employer:(iii) whether it is reasonably practicable to return the claimant to a different employment with a different employer, in which the claimant is able to use his or her experience, education, or training:(iv) whether it is reasonably practicable to help the claimant use as many of his or her pre-injury skills as possible to obtain employment.
87. Further matters to be considered in deciding whether to provide vocational rehabilitation(1) In deciding whether to provide vocational rehabilitation, the Corporation must have regard to—
(a) whether the vocational rehabilitation is likely to achieve its purpose under the claimant’s individual rehabilitation plan; and(b) whether the vocational rehabilitation is likely to be cost-effective, having regard to the likelihood that costs of entitlements under this Act will be reduced as a result of the provision of vocational rehabilitation; and(c) whether the vocational rehabilitation is appropriate in the circumstances.
(2) The Corporation is liable to provide the vocational rehabilitation for the minimum period necessary to achieve its purpose, but must not provide any vocational rehabilitation for longer than 3 years (which need not be consecutive).[“(2A) Subsection (2) is subject to subsection (2B).[“(2B) Despite subsection (2), the Corporation may, at its discretion, provide vocational rehabilitation for longer than 3 years if the Corporation considers that—
“(a) the vocational rehabilitation would be likely to achieve its purpose under the claimant’s individual rehabilitation plan; and“(b) the vocational rehabilitation would be likely to be cost effective, having regard to the likelihood that costs of entitlements under this Act will be reduced as a result of the provision of vocational rehabilitation; and“(c) the vocational rehabilitation would be appropriate in the circumstances.
[“(2C) However, despite subsections (1)(b) and (2B)(b), the Corporation must not take into account as a factor against providing vocational rehabilitation that the claimant is, or may become, a person to whom clause 52 of Schedule 1 (relationship betweenweekly compensation and New Zealand superannuation) applies.](3) This section is subject to any regulations made under section 324.88. Vocational rehabilitation may start or resume if circumstances change(1) The Corporation may, at any time, decide whether or not there has been a change of circumstances affecting the claimant’s need for vocational rehabilitation.
October 2008 Page 17 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
(2) If the Corporation decides that there has been such a change, the Corporation and the claimant may agree to the modification of the claimant’s individual rehabilitation plan to reflect the changed circumstances.(3) The Corporation may resume providing vocational rehabilitation under the claimant’s individual rehabilitation plan, with any agreed modifications, to a claimant who—
(a) had vocational rehabilitation; and(b) as a result, obtained employment; but(c) is unable to maintain the employment because of his or her incapacity.
(4) This section is subject to section 87(2) and (3).
89. Assessment of claimant ’s vocational rehabilitation needs An assessment of a claimant’s vocational rehabilitation needs must consist of—
(a) an initial occupational assessment to identify the types of work that may be appropriate for the claimant; and(b) an initial medical assessment to determine whether the types of work identified under paragraph (a) are, or are likely to be, medically sustainable for the claimant.
93. Medical assessor(1) A medical assessment must be undertaken by a medical practitioner who is described in subsection (2) or subsection (3).(2) A medical practitioner who provides general medical services must also—
(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) have at least 5 years' experience in general practice; and(c) meet at least 1 of the following criteria:
(i) be a Fellow of the Royal New Zealand College of General Practitioners or hold an equivalent qualification:(ii) be undertaking training towards becoming a Fellow of the Royal New Zealand College of General Practitioners or holding an equivalent qualification(iii) have undertaken relevant advanced training.
(3) A medical practitioner who does not provide general medical services must—(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) be a member of a recognised college.
94. Assessments when medical assessor unavailable(1) A… medical practitioner who does not qualify under section 93 may undertake a medical assessment if the Corporation is satisfied that—
(a) the circumstances in subsection (2) exist; and(b) the… medical practitioner's qualifications and experience are broadly comparable with the qualifications and experience specified in section 93.
(2) The circumstances are that—(a) a… medical practitioner who does qualify under section 93 is not available to undertake a medical assessment without unreasonable delay or unreasonable inconvenience to the claimant; and
October 2008 Page 18 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
(b) the delay or inconvenience would have an adverse effect on providing vocational rehabilitation to the claimant.
(3) Sections 95 and 96 apply to a… medical practitioner who qualifies under this section to undertake a medical assessment.
95. Conduct of initial medical assessment(1) A medical assessor undertaking an initial medical assessment must take into account—
(a) information provided to the assessor by the Corporation; and(b) any of the following reports, information, or comments provided to the assessor:
(i) medical reports requested by the Corporation before the individual rehabilitation plan was prepared:(ii) any other relevant medical reports; and
(c) the report of the occupational assessor on the initial occupational assessment; and(d) the medical assessor's clinical examination of the claimant; and(e) any other information or comments that the claimant requests the medical assessor to take into account and that the medical assessor decides are relevant.
(2) The medical assessor must also take into account any condition suffered by the claimant that is not related to the claimant's personal injury.(3) The Corporation must provide to a medical assessor all information the Corporation has that is relevant to an initial medical assessment.
96. Report on initial medical assessment(1) The medical assessor must prepare and provide to the Corporation a report on the initial medical assessment.(2) The report must—
(a) contain the determination required by section 89(b); and(b) take into account the matters referred to in section 95.
(3) The Corporation must provide a copy of the report to the claimant.
Part 4 - Vocational independence107. Corporation to determine vocational independence(1) The Corporation may determine the vocational independence of—
(a) a claimant who is receiving weekly compensation:(b) a claimant who may have an entitlement to weekly compensation.
(2) The Corporation determines a claimant's vocational independence by requiring the claimant to participate in an assessment carried out—
(a) for the purpose in subsection (3); and(b) in accordance with sections 108 to 110 and clauses 24 to 29 of Schedule 1; and(c) at the Corporation's expense.
(3) The purpose of the assessment is to ensure that comprehensive vocational rehabilitation, as identified in a claimant's individual rehabilitation plan, has been completed and that it has focused on the claimant's needs, and addressed any injury-related barriers, to enable the claimant—
(a) to maintain or obtain employment; or(b) to regain or acquire vocational independence.
October 2008 Page 19 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
108. Assessment of claimant's vocational independence(1) An assessment of a claimant's vocational independence must consist of—
(a )an occupational assessment under clause 25 of Schedule 1; and(b) a medical assessment under clause 28 of Schedule 1.
(2) The purpose of an occupational assessment is to—(a) consider the progress and outcomes of vocational rehabilitation carried out under the claimant's individual rehabilitation plan; and(b) consider whether the types of work (whether available or not) identified in the claimant's individual rehabilitation plan are still suitable for the claimant because they match the skills that the claimant has gained through education, training, or experience.
(3) The purpose of a medical assessment is to provide an opinion for the Corporation as to whether, having regard to the claimant's personal injury, the claimant has the capacity to undertake any type of work identified in the occupational assessment and reflected in the claimant's individual rehabilitation plan.
109. When claimant's vocational independence to be assessed(1) The Corporation may determine the claimant's vocational independence at such reasonable intervals as the Corporation considers appropriate.(2) However, the Corporation must determine the claimant's vocational independence again if—
(a) the Corporation has previously determined that the claimant had—(i) vocational independence under this section; or(ii) a capacity for work under section 89 of the Accident Insurance Act 1998; or(iii) a capacity for work under section 51 of the Accident Rehabilitation and Compensation Insurance Act 1992; and
(b) the Corporation believes, or has reasonable grounds for believing, that the claimant's vocational independence or capacity for work may have deteriorated due to the injuries that were assessed in the previous vocational independence or capacity for work assessment.
(3) The claimant may give the Corporation information to assist the Corporation to reach a belief under subsection (2)(b).
Schedule 1 - Vocational rehabilitation27. Medical assessor(1) A medical assessment must be undertaken by a medical practitioner who is described in subclause (2) or subclause (3).(2) A medical practitioner who provides general medical services must also—
(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) have at least 5 years' experience in general practice; and(c) meet at least 1 of the following criteria:
(i) be a Fellow of the Royal New Zealand College of General Practitioners or hold an equivalent qualification:(ii) be undertaking training towards becoming a Fellow of the Royal New Zealand College of General Practitioners or holding an equivalent qualification:(iii) have undertaken relevant advanced training.
(3) A person who does not provide general medical services must also—
October 2008 Page 20 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
(a) have an interest, and proven work experience, in disability management in the workplace or in occupational rehabilitation; and(b) be a member of a recognised college.
28. Conduct of medical assessment(1) A medical assessor undertaking a medical assessment as part of an assessment of a claimant's vocational independence under section 108 must take into account—
(a) information provided to the assessor by the Corporation; and(b) any individual rehabilitation plan for the claimant; and(c) any of the following medical reports provided to the assessor:
(i) medical reports requested by the Corporation before the individual rehabilitation plan was prepared:(ii) medical reports received during the claimant's rehabilitation; and
(d) the report of the occupational assessor under clause 26; and(e) the medical assessor's clinical examination of the claimant; and(f) any other information or comments that the claimant requests the medical assessor to take into account and that the medical assessor decides are relevant.
(2) The Corporation must provide to a medical assessor all information the Corporation has that is relevant to a medical assessment.
29. Report on medical assessment(1) The medical assessor must prepare and provide to the Corporation a report on the medical assessment specifying—
(a) relevant details about the claimant, including details of the claimant's injury; and(b) relevant details about the clinical examination of the claimant undertaken by the assessor, including the methods used and the assessor's findings from the examination; and(c) the results of any additional assessments of the claimant's condition; and(d) the assessor's opinion of the claimant's vocational independence in relation to each of the types of work identified in the occupational assessor's report; and(e) any comments made by the claimant to the assessor relating to the claimant's injury and vocational independence in relation to each of the types of work identified in the occupational assessor's report.
(2) The report must also identify any conditions that—(a) prevent the claimant from having vocational independence; and(b) are not related to the claimant's injury.
(3) The Corporation must provide a copy of the report to the claimant.
October 2008 Page 21 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
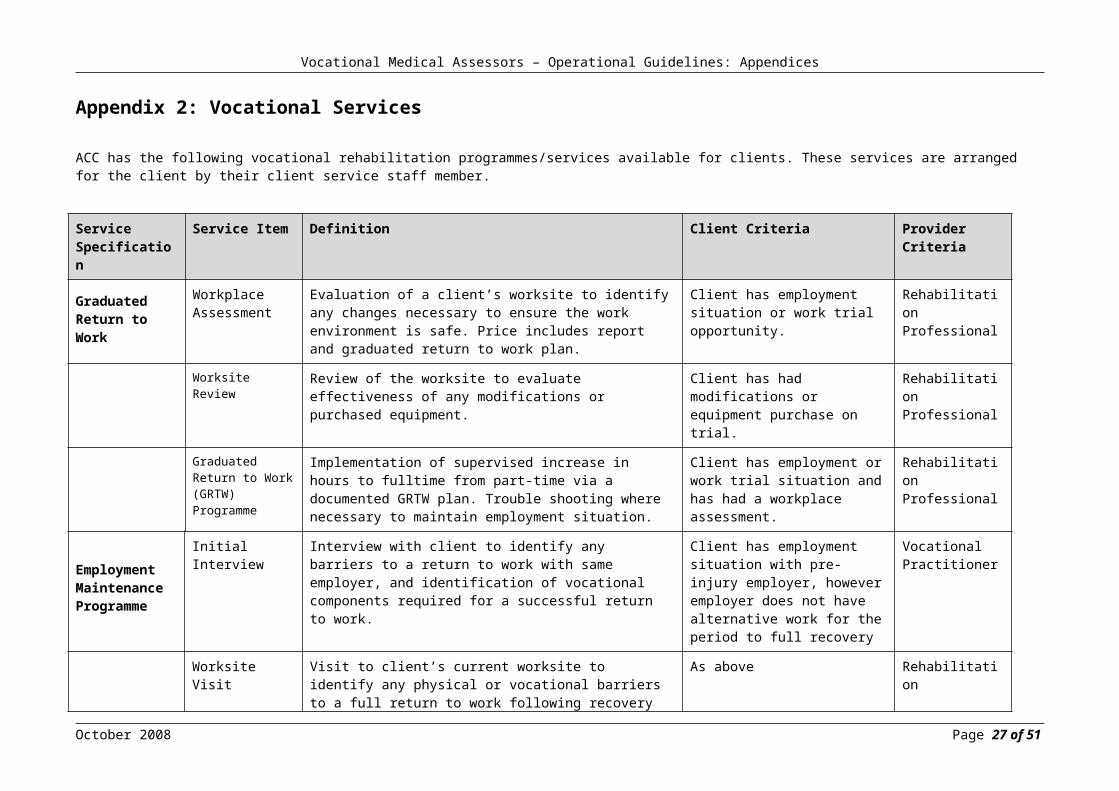
Appendix 2: Vocational Services
ACC has the following vocational rehabilitation programmes/services available for clients. These services are arranged for the client by their client service staff member.
Service Specification
Service Item Definition Client Criteria Provider Criteria
Graduated Return to Work
Workplace Assessment
Evaluation of a client’s worksite to identify any changes necessary to ensure the work environment is safe. Price includes report and graduated return to work plan.
Client has employment situation or work trial opportunity.
Rehabilitation Professional
Worksite Review Review of the worksite to evaluate effectiveness of any modifications or purchased equipment.
Client has had modifications or equipment purchase on trial.
Rehabilitation Professional
Graduated Return to Work (GRTW) Programme
Implementation of supervised increase in hours to fulltime from part-time via a documented GRTW plan. Trouble shooting where necessary to maintain employment situation.
Client has employment or work trial situation and has had a workplace assessment.
Rehabilitation Professional
Employment Maintenance Programme
Initial Interview Interview with client to identify any barriers to a return to work with same employer, and identification of vocational components required for a successful return to work.
Client has employment situation with pre-injury employer, however employer does not have alternative work for the period to full recovery
Vocational Practitioner
Worksite Visit Visit to client’s current worksite to identify any physical or vocational barriers to a full return to work following recovery from injury.
As above Rehabilitation Professional
Individual Programme Plan
A time-framed individual return to work plan that outlines individual and group components for client to participate in over the required number of weeks for a successful return to work.
As above Vocational Practitioner
October 2008 Page 22 of 51

Vocational Medical Assessors – Operational Guidelines: Appendices
Service Specification
Service Item Definition Client Criteria Provider Criteria
Employment Maintenance Programme - continued
Key Provider Monitoring
Includes:a) weekly meeting or phone call with/to client to monitor programme progress and ensure on track; andb) report on achievement, or not, of programme goals, ie. Employment maintenance; andc) a 3-week follow-up phone call to employer, client and client service staff member confirming durable return to work.
As above Vocational Practitioner
Rehabilitation Modules
Group modules addressing aspects of injury prevention and injury management.
As above Rehabilitation Professional
Vocational Modules
Group modules addressing employer and employee responsibilities for return to work.
As above Vocational Practitioner
Functional Capacity Evaluation (FCE)
Full FCE Assessment of a client’s ability to sustain physical performance in response to a range of physical demands reliably and safely.
Client has yet to obtain employment or work trial situation (therefore baseline functioning needs to be established).
Rehabilitation Professional
Task-Specific Evaluation
Assessment of client’s ability to sustain specified tasks reliably and safely.
Client has employment situation or work trial opportunity, however GP needs confirmation via an FCE that client can attempt the work.
Rehabilitation Professional
Occupational Assessment
Initial Assessment
Assessment of client’s existing education, training experience and will take into account a client’s earnings before the client’s incapacity Identification of suitable work types on ACC work type detail sheets.
Client has yet to obtain employment or work trial situation.
Occupational Assessor
Service Service Item Definition Client Criteria Provider
October 2008 Page 23 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Specification Criteria
Occupational Assessment - continued
Reassessment Reassessment as above, in situations where the client service staff member indicates this is required.
As above As above
Curriculum Vitae (CV) Preparation
Individualised CV to emphasise marketable qualities and skills.
As above Vocational Practitioner
Vocational Independence Assessment
Assessment of the progress and outcomes of a client’s vocational rehabilitation, consideration of whether the types of work identified in the IOA are still suitable and assessment of whether any new types of work are now suitable
Client is work ready, has yet to obtain full employment, and has completed the vocational rehabilitation requirements as per their IRP
Occupational Assessor
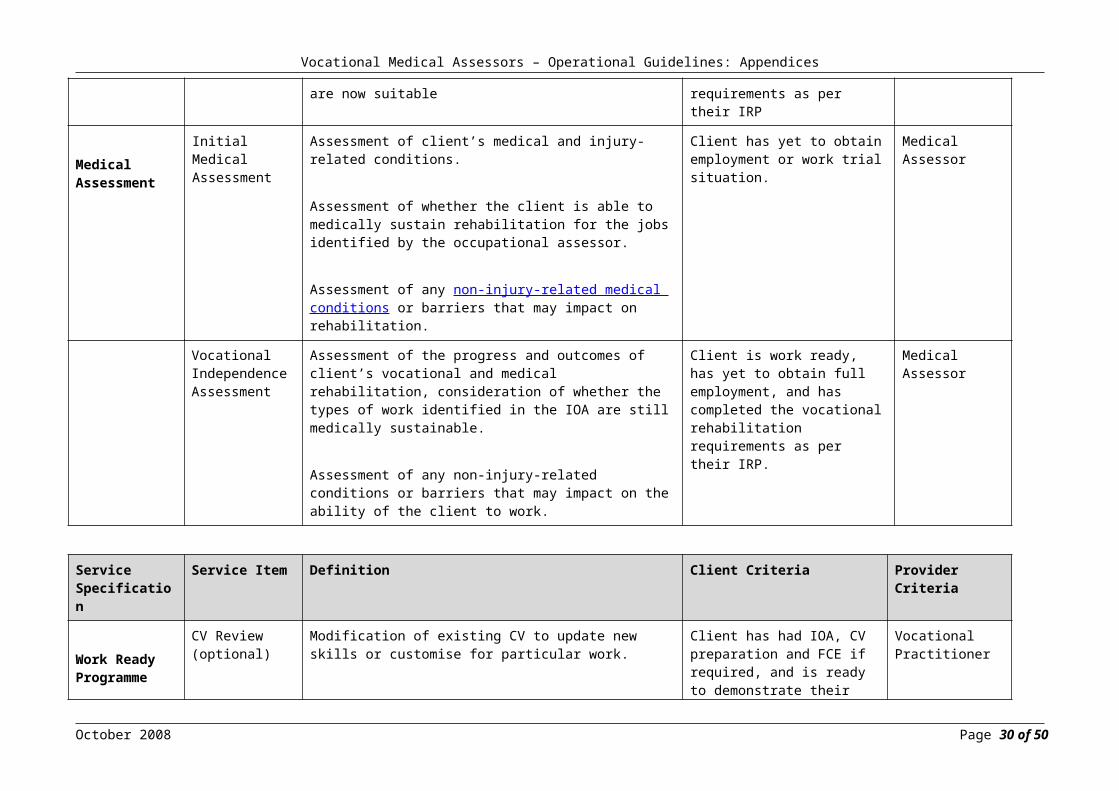
Medical Assessment
Initial Medical Assessment
Assessment of client’s medical and injury-related conditions.
Assessment of whether the client is able to medically sustain rehabilitation for the jobs identified by the occupational assessor.
Assessment of any non-injury-related medical conditions or barriers that may impact on rehabilitation.
Client has yet to obtain employment or work trial situation.
Medical Assessor
Vocational Independence Assessment
Assessment of the progress and outcomes of client’s vocational and medical rehabilitation, consideration of whether the types of work identified in the IOA are still medically sustainable.
Assessment of any non-injury-related conditions or barriers that may impact on the ability of the client to work.
Client is work ready, has yet to obtain full employment, and has completed the vocational rehabilitation requirements as per their IRP.
Medical Assessor
Service Specification
Service Item Definition Client Criteria Provider Criteria
October 2008 Page 24 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Work Ready Programme
CV Review (optional)
Modification of existing CV to update new skills or customise for particular work.
Client has had IOA, CV preparation and FCE if required, and is ready to demonstrate their work readiness, as indicated by Medical Certificate (ACC18).
Vocational Practitioner
Work Trial Unpaid work trial of between 3 and 6 weeks duration with close monitoring.
As above Vocational Practitioner
Work Ready Outcome
Work trial completed with close monitoring. Client has demonstrated they have no outstanding barriers to achieve a return to work.
As above As above
Work Preparation Programme
Initial Interview An initial interview of 30 minutes duration is conducted prior to the commencement of the programme. The interview is conducted by an occupational assessor and will identify the client’s suitability for the programme; determine appropriate individual rehabilitative components; and report any contraindications to the client service staff member.
Client no longer has pre-injury employment, has had IOA and requires work preparation as part of their IRP.
Occupational Assessor
Group Programme
A 6 week programme running 9am-1pm each weekday, which includes vocational, physical, and psychological modules. Payment is for a group programme, which requires a minimum of 6 clients in each course. Fee includes providing reports on weekly attendance, progress, and completion, as well as a detailed 6 week group programme plan.
As above Multidisciplinary including Registered Psychologist
Individual Work Preparation Programme
A detailed programme running 9am-1pm each weekday, for up to 6 weeks, which includes vocational, physical and psychological modules specific to the individual client, identified in the initial interview.
As above As above
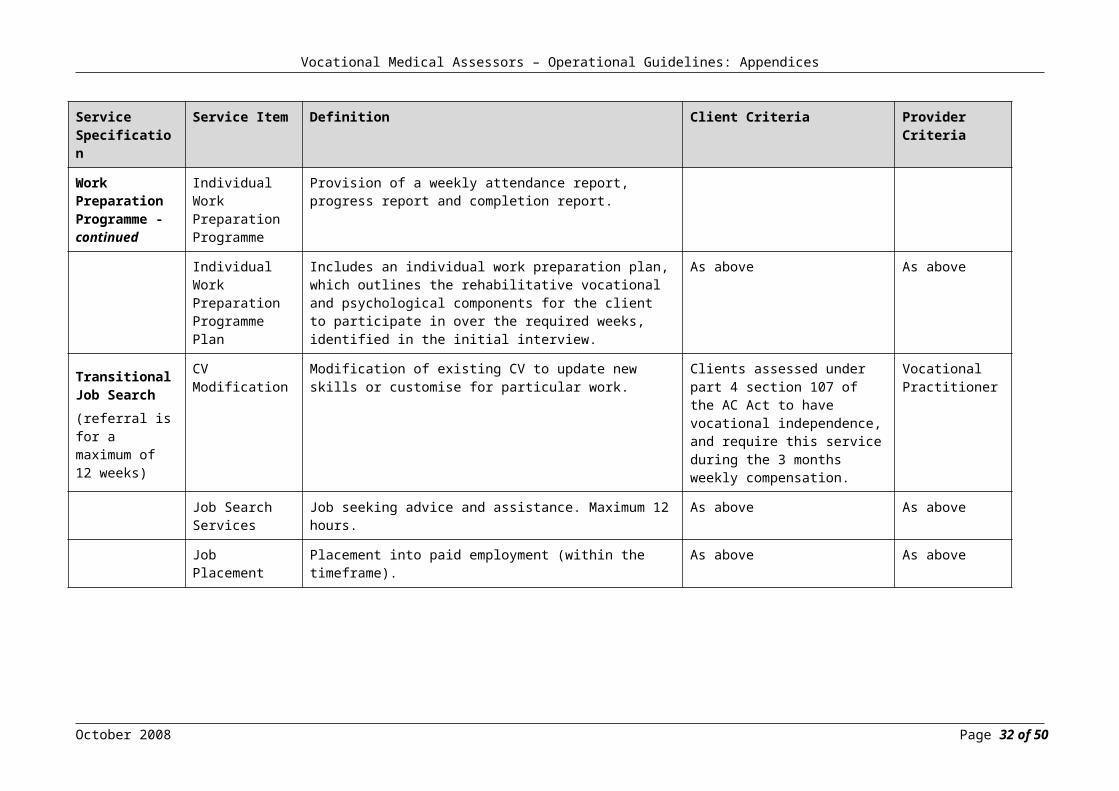
Service Specification
Service Item Definition Client Criteria Provider Criteria
Work Preparation
Individual Work
Provision of a weekly attendance report, progress
October 2008 Page 25 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
Programme - continued
Preparation Programme
report and completion report.
Individual Work Preparation Programme Plan
Includes an individual work preparation plan, which outlines the rehabilitative vocational and psychological components for the client to participate in over the required weeks, identified in the initial interview.
As above As above
Transitional Job Search(referral is for a maximum of 12 weeks)
CV Modification
Modification of existing CV to update new skills or customise for particular work.
Clients assessed under part 4 section 107 of the AC Act to have vocational independence, and require this service during the 3 months weekly compensation.
Vocational Practitioner
Job Search Services
Job seeking advice and assistance. Maximum 12 hours.
As above As above
Job Placement Placement into paid employment (within the timeframe).
As above As above
October 2008 Page 26 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 3 - Vocational Paths
Maintain employment
General aimThe focus of this path is to restore the client’s capacity to continue working with their current employer in either the same type of work or a different one. Rehabilitation through this path aims to both: Ensure the client maintains their existing job Return them to their pre-injury level of work activity, in both the type of tasks and the
number of hours they work.
If the client is unlikely to return to their pre-injury level of work activity, the next preference is to consider appropriate alternative types of work with the same employer. If there are no ‘light duties’ available, but the job remains open, the client is referred to an ‘employment maintenance programme’.
Suitable clients for maintaining employmentSuitable clients for this path have the following features: There is a suitable job to which they can return The client is physically able, now or potentially, to resume their pre-injury work and
medical advice must confirm this The employer can either keep the pre-injury job open for them or provide alternative
suitable work The client will be able to return to the number of hours they worked before the injury,
or can build up to that within a specified timeframe.
Suitable interventions for maintaining employmentTo help the client achieve the rehabilitation outcome of maintaining employment, the following vocational assistance may be considered: Workplace assessment Work ready programme Making modifications to the workplace or purchasing vocational equipment Modifying their duties Employing a provider to monitor and support the client’s gradual return to work Providing an activity-based programme Obtaining the provider’s confirmation of the suitability of any alternative work and
transport.
Note:This assistance may be provided concurrently.
Employer’s involvement
October 2008 Page 27 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
When working toward maintaining a client’s previous employment, Part 4 section 71 of the AC Act requires the employer to help the client with their rehabilitation as per the IRP. The employer is included as an integral member of the rehabilitation team, as early as possible in the process.
The more interested and involved the employer is in maintaining the client’s employment the sooner the client is likely to achieve the rehabilitation outcome. An employer who is involved and provides support for a client in the workplace can also save much time and cost in hiring and training replacement staff.
If this path is selected, the client service staff member must advise both the employer and the client in writing of the decision to return the client to their pre-injury job.
Obtain employment
The second preferred path is to help a client gain appropriate employment even if that is with a different employer. Working toward this outcome includes the client making a reasonable effort to actually obtain work.
General aimThe focus of this path is to restore the client’s ability to work in either: The same type of work for a different employer, or A different type of work for a different employer, which uses their pre-injury
experience, education, or training and is suitable for the status of their injury.
Note: Remember that a different type of work must be at a similar level to their previous type of work.
Suitable clients for obtaining employmentSuitable candidates for this path are those clients who have lost their pre-injury job and: Are able to work, or can build up to, 35 hours or more a week Have sufficient education, training, or experience to reasonably expect to find suitable
work Can gain those skills with some assistance.
Suitable interventionsTo help the client achieve employment with a different employer, the following assistance will be considered by the client service staff member: Initial Occupational Assessment (IOA), with CV preparation Initial Medical Assessment (IMA).
Other services that are provided by ACC include: Functional capacity evaluation
October 2008 Page 28 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Short training course Return to work programme Work hardening programme. Comprehensive pain assessment (if pain is a barrier to returning to work). See Pain
Management Services - Operational Guidelines, pg 29 Functional Reactivation Programme (see Pain Management Services - Operational
Guidelines, pg 14).
Notes: Graduated return to work plans must specify a timeframe to return to full-time work
hours Any of the above programmes and interventions may be provided concurrently Alternative types of work should be specified if they can achieve the return to work
outcome within the specified timeframe and the role uses the client’s existing experience, education, or training
The IMA confirms that the type of work is suitable for the client.
Regain or acquire vocational independence
ACC provides rehabilitation assistance to give the client the support and training they need to be able to seek and undertake appropriate work. Previously, this option was called ‘acquire a capacity for work’, ‘work readiness’, or combinations of these terms.
General aimThe focus of this path is to: Remove any obstacles or barriers that prevent the client from doing any type of work
for which they have skills, education, or experience Help the client use as many of their pre-injury skills as possible in obtaining
employment.
A different type of work must be at a similar level to the client’s previous type of work, and the IMA must confirm that the type of work is suitable for the client.
Suitable clientsClients who may best follow this path include those: Who have suitable education, experience, or training to work in other types of work Who are not likely to achieve independence in employment within a reasonable
period, for any reason For whom previous help to try to achieve independence in their employment has been
unsuccessful Who are able to work 35 hours or more per week, or will be able to build up to that, in
suitable types of work.
Suitable interventions for regaining or acquiring vocational independenceTo help the client regain or acquire vocational independence, consider the following assistance against the decision-making criteria outlined in Part 4 section 87 of the AC Act: IOA, with or without CV preparation
October 2008 Page 29 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
IMA.
Other interventions that may be used include: Functional capacity evaluation Work ready programme Work hardening programme Short training courses Comprehensive pain assessment (if pain is a barrier to returning to work). See Pain
Management Services - Operational Guidelines, pg 29 Functional Reactivation Programme (see Pain Management Services - Operational
Guidelines, pg 14).
Note: Remember to provide all types of assistance concurrently, wherever possible.
October 2008 Page 30 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 4: Example - Initial Medical Assessment Report
11 July 2003
Assessor detailsDr ABC123 Main St
Relevant qualificationsMBChB, Dip Occ Med, FRNZCG P
Referred byClient service staff member YNew Branch
PhFaxEmail
Accident Compensation Corporation
Appointment detailsDate of Examination: 5/7/2002 Time: 10amDuration of Appointment: 75 minutesDate Requested by ACC: 1/7/2002
Client detailsMrs “S”Date of Birth: dd/mm/1949
InjuriesThe injuries as outlined on your referral letter are these: Date of Injury
15/6/97 Nature of Injury
“Occupational Overuse Injury” – bilateral medial epicondylitis Claim Number
A1234567/004
October 2008 Page 31 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
List of medical documentation received including results of diagnostic procedures
No. Date Document Type Provider
1 05/07/2002 Referral for Initial Medical Assessment Client service staff
2 14/05/2002 Initial Occupational Assessment Report Career Services3 22/05/2002 Work Ready Programme Completion Report Workbridge4 19/04/2002 Return to Work Monitoring Ergowise5 23/04/2002 Work Trial Completion Report Workbridge6 15/03/2002 Pain Management Programme ADHB7 25/05/2001 Occupational Physician Report Dr OccPhys18 17/05/2001 MRI Report Mercy MRI9 27/02/2001 Occupational Physician Report Dr OccPhys210 22/02/2001 Radiology Report ARG11 16/06/2001 Orthopaedic Surgeon Report Dr Ortho112 12/05/2000 Physiotherapy Feedback Pro Rehab13 28/07/1998 Occupational Physician Report Dr OccPhys214 10/08/1997 Physiotherapy Report HMC15 14/04/1997 ACC Form: Client Questionnaire Client16 14/03/1997 ACC Form: Medical Practitioner Questionnaire Dr GP1
History of the injury“S” was injured when she was working on a six-month contract managing a motel in Anytown. Her duties involved the full range of motel duties, which included cleaning, making beds, laundry, office work, and general maintenance.
In December 1996 she developed pain in the right elbow, which was placed in a sling. This resulted in an extra loading on the left arm. At the same time she was stressed by the break-up of her marriage in February 1997. She developed bilateral elbow pain. She employed a cleaner to help.
In July 1997 she went overseas and entered another contract to manage a motel in another country for 10 months, returning to New Zealand when her mother died. In October 1998 she bought the rights to sell lollies, until April 2000. This involved sorting and packing lollies into 5-6kg boxes, taking them from the car boot, opening heavy doors in the industrial area and making up to 40 calls per day. She had to stop because of the limitations of elbow function, namely bending, and she required her elderly father to take care of her. She has had several work trials, the last of which was completed in April 2002, at a motel.
October 2008 Page 32 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
She has just started a computer course, and this aggravated both her elbows after two days of typing.
Current state“S” reports pain in both elbows, over the bony prominence of the lateral aspect of the elbow. This is described as dull and intermittent and is rated as a grade 6 out of 10, using a Visual Analogue Scale (10 being the worst).
“S” reports no other symptoms including numbness or tingling, headaches, bowel disturbance, or dysmenorrhoea. Mood is unchanged, and there are no signs of endogenous depression.
She has difficulty getting off to sleep, which may take up to 90 minutes, and she feels she could do with eight hours’ sleep rather than the six hours she is getting at present. The sleep disturbance is not due to her elbows. No daytime sleep is required and daytime alertness is normal.
Current treatment and medicationIn the past “S” has had physiotherapy which loosened the tightness in her arms, acupuncture which worked for a short period, massage which didn’t seem to ease the pain, a rehabilitation programme with work trials which flared up the pain, and a pain management programme which she states was the best for her and has got her where she is today. The programme was run by the Regional Pain Service, in January this year for one month, and she is due for her six-monthly review on 12/7/02.
She has received three steroid injections on the right and two on the left. Past medications included Vioxx, Tramol, Diclofenac, Paradex, Nurofen and topical agents Antiflamme and Bee Pollen.
“S” is currently taking Betaloc CR, two tablets daily and Amizide one tablet daily for hypertension. She has been on this medication for six years. She notices that her fingers go white and cold if she goes outside on a cold winter’s day.
Vocational history“S” was at school until the age of 15 and started full-time employment as she was offered a good office job halfway through the fifth form.
“S” is right handed and was working as a motel manager up to the accident, and was successfully able to work until April 2000.
The work is believed by “S” to be related to the current health problems. Her symptoms are related to activity and the type of work, are activity dependent, and ease with rest.
The past history of occupations include: Accounts assistant between 1994 and 1996 Motel manager between 1997 and 1998 Self-employed, 1998-2000.Psychosocial history“S” lives with her father in his home because of the lack of personal finance. “S”
October 2008 Page 33 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
consumes no alcohol per week and is a non-smoker. Stress is present because of her limited financial resources. She would like to be independent and support herself and live alone. Activities of daily living that are affected and limited by the accident include all of the similar activities that were involved at the motel.
Exercise is performed regularly for 30 minutes three times per week. Her gym membership of three months expired at the end of June; she was attending five to six times per week.
Leisure activities that are affected and limited by the accident include recreation, eg walking, playing board games with family, and playing golf since April 2000.
Past medical historyThe past medical history includes: In 1968 she was involved in a car accident, travelling at a speed of 50 kilometres per
hour. She sustained a fracture of the right wrist, possibly the left clavicle and rib, with puncture of the lungs and a lower back injury.
Hypertension diagnosed in 1997.
There are no known drug, food, or chemical allergies.
Past surgical historyThere is no significant surgical history of note.
Family historyThere is no significant family history of note.
Examination findings“S” was a co-operative patient in no obvious distress, and arrived alone at the assessment. Her blood pressure was 134/86, weight 61.4kg, height 161cm, giving a BMI of 23. There was no abnormality of the chest or clavicle.
Elbows There was no significant deformity or effusion of the elbows. There was no obvious wasting noted of the arms and forearms. There was some
prominence of the lateral epicondyle with an element of fat atrophy, however no depigmentation was noted.
The left elbow lacked 10 degrees of full extension, with pronation and supination being normal bilaterally.
There was discomfort over both lateral epicondyles of the elbow to palpation, the left being worse than the right.
There was no crepitus on movement. Strength testing of the muscles around the elbow was 5/5, except wrist extension
resistance which was slightly weaker on the left and aggravating the elbow pain and normal on the right.
Reflexes of the biceps were 1/3, the triceps were 1/3, the supinator were 1/3, and symmetrical.
Sensation was normal.
October 2008 Page 34 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
Wrist There was no significant deformity or effusion of the right wrist, and it was not
obvious where there may have been a fracture. There was no obvious wasting noted of the forearm or hand muscles. There was no significant discomfort of the wrist to palpation. There was no crepitus on movement. Tinel’s sign was negative.
Lumbosacral Spin Gait was normal and heel and toe walking was normal. The Trendelenberg and the Romberg’s tests were normal. Flexion of the lumbar spine was possible to the mid-shins. Extension was normal. Lateral flexion was normal and symmetrical. Thoraco-lumbar rotation was within normal limits and symmetrical. There was tenderness overlying the lumbosacral junction and bilaterally over the
sacro-iliac joints without significant paravertebral muscle spasm. There were tender points over the buttocks and the right medial knee. Straight leg raising was 70 degrees on the right and 70 degrees on the left. Sciatic stretches were negative. Femoral stretches were negative. Reflexes of the knee were 2/3, the ankles were 1/3, and symmetrical, and the plantars
were down going. Sensation was normal. Power was 5/5 and symmetrical.
InvestigationsThe investigations performed so far included:
17/05/2001 MRI Report Normal22/02/2001 Radiology Report Normal
DiagnosisBased on all of the above, the current diagnosis is: Bilateral tennis elbow Hypertension.
Medical rehabilitationAs noted above, the main current issue relates to pain from her elbows. Previous involvement with the pain programme at the Regional Pain Service was very helpful. It would be important that she attend the planned six-monthly review with this service.
Her hypertension is well controlled on medication. This does not present a barrier to rehabilitation but it is preferable for vocational rehabilitation to avoid outdoor work with significant exposure to the cold.Discussion and opinionThe diagnosis is bilateral epicondylitis with ongoing pain. This has been successfully managed through attendance at the pain programme at the Regional Pain Service. Because of the continuing elbow problem, the physical restrictions would include:
October 2008 Page 35 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Lifting, though she coped comfortably with up to 5-6kg of lollies Carrying, with the limit of 9kg Repetition that involves force, vibration, or lifting.
Because of the hypertension with treatment by a beta blocker (Betaloc CR), outdoor work is ideally avoided.
Work typesEach of the work types identified by the vocational assessor has been considered below in conjunction with the medical examination and the suitability of each for “S”.
It is my opinion that the following types of work are currently medically sustainable for “S”
1. Work type – “Debt Collector” 599311In my opinion this work type is suitable because according to the relevant work type detail sheet the functional demands of the work type, eg walking, driving, and sitting, are all medically sustainable.
Specifically, there is a good variation in postures needed with the mix of sedentary work and moving about. More than very light lifting is unlikely as detailed for this work type. Repetitive work is not required.
The outdoor aspect of this work is not likely to be a problem as there is not significant exposure to cold. There is no medical reason to advise that outdoor work must not be undertaken. The possible development of white and cold fingers is of nuisance value only.
“S” agrees with this, however she thought she may need to get ear phones because of the difficulty of holding the phone, but she is happy in this role having had past experience.
2. Work type – “Supply and Distribution Manager” 133611In my opinion this work type is suitable because the functional demands of the work type, such as sitting, standing, moving, and mental activities are all medically sustainable as detailed in the work type detail sheet.
Specifically there is a good variation in postures needed with the mix of sedentary work and moving about. The work is typically in an office environment indoors. Stretching, bending, twisting, climbing, and lifting are unlikely to be required. Repetitive movements are unlikely to be necessary unless significant keyboarding is required.
“S” agrees with this.3. Work type – “Conference and Event Organiser” 149311
In my opinion this work type is suitable because the functional demands of the work type, such as sitting, driving, and mental activities are all medically sustainable and are detailed in the work type detail sheet.
Specifically there is a good variation in postures needed with the mix of sedentary
October 2008 Page 36 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
work and moving about. The work is typically in an office environment and indoors. Stretching, bending, twisting, climbing, and lifting are unlikely to be required. Repetitive movements are unlikely to be necessary unless significant keyboarding is required.
“S” agrees with this, however the issue is that she doesn’t have the “pizzazz” which she believes is normally part of this role.
4. Work type – “Sales Assistant” 621111In my opinion this work type is suitable because the functional demands of the work type such as standing, processing, lifting and passing, stretching and twisting, and mental activities are all medically sustainable.
This work type is indoors and the physical demands are in the sedentary to light work range. There is frequent standing required but this is not an issue from a medical perspective for “S”. The position is also sustainable provided that constant repetitive hand and finger activities are not associated with this position.
This work type is classified as sedentary to light physical demand meaning up to 9kg may be involved. This is within her physical ability.
“S” agrees with this, but raises the issue that she was told by her friend that she may have to lift heavy objects, and also the fact that she has had 21 job rejections.
It is my opinion that the following types of work are likely to be medically sustainable for “S” after medical rehabilitation as detailed earlier in my report.
5. Work type – “Accounts Clerk” 551111In my opinion this work type, particularly the repetitive arm, hand, and finger movements, is doubtful in her current situation as exemplified by the aggravation by the current computer course, but may be considered once her rehabilitation is completed. Participation in the pain management rehabilitation programme review is likely to result in her gaining the ability to manage computer use. There is no medical reason to advise against the use of a computer.
“S” agrees with this, however wonders how she would get on with computers, because she can be in agony after spending only 15 minutes sending e-mail.
6. Work type – “Bookkeeper” 551211As in 5 above.
It is my opinion that the following occupation is not medically sustainable for “S”.
7. Work type – “Domestic Housekeeper” 811412In my opinion this work type is unsuitable because the functional demands of the work type are not medically sustainable.
October 2008 Page 37 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
This work type is indoors and the physical demands are in the light to medium work range. The work type detail sheet confirms that there may be constant walking, twisting of the neck and mental activities in this position. There may also be occasional carrying or lifting or moving of various items such as furniture, which “S” will not be able to manage with her injury.
“S” agrees with this.
ConclusionOf the seven work types identified to be suitable for “S” by the vocational assessor, it is my opinion that “S” has currently the physical capacity to perform four of these as detailed above as being medically sustainable.
Two of the work types are likely to be medically sustainable after further rehabilitation at the Regional Pain Service. One of the work types, “Housekeeping” is not medically sustainable.
This conclusion has been discussed by me with “S”, who agrees but would like to think that she could one day return to work as a motel manager. However, she realises that the housekeeping role that can be involved makes this difficult.
Yours sincerelyDr ABC
I hereby certify that in giving this assessment, I have undertaken reasonable actions in the circumstances to give effect to the rights, and comply with the duties, in the current Code of Health and Disability Consumer Rights. This includes Right 5 [Right to Effective Communication], Right 6 [Right to be Fully Informed] and Right 7 [Right to Make an Informed Choice and Give Informed Consent].
October 2008 Page 38 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 5: Example - Vocational Independence Medical Assessment
Dr Very GoodMBChB, MRCGP, Dip Obs, FRNZCGP, Dip Occ Med
THE CLINIC TEL 00 112-4567123 MAIN FAX 00 112-4568ANYTOWN
Vocational independence medical assessment of:
Name: Mrs ABAddress: 246 Other Ave
Anytown
Claim No: Z234567/000
Vocational independence medical assessment issued at the request of Mary Poppins, Client service staff, Anytown Office.
Date of Assessment: 10/09/2003Date of Birth: 23/10/1965Occupation at Injury: Bank TellerEmployer: BankDuration of Employment: 5 yearsDate of Accident / Injury: 15/12/1991Date of Work Cessation: 01/04/1992
Thank you for referring Mrs AB for a vocational independence medical assessment.
I have discussed with her the purpose of the assessment. Mrs AB indicated that she understood the process as this has also been explained by her client service staff member.
I have reviewed the following list of referral documents: Vocational Independence Occupational Assessment report by AB, 12/4/03 Vocational Independence Assessment: File Summary, Team Review and Quality Check Initial Medical Assessment by Dr AB, 20/8/02 IN4A by Dr AB, 27/4/02 Medical Certificate Vocational Independence Assessment: Client Questionnaire Vocational Independence Assessment: General Practitioner Questionnaire Ultrasound R) shoulder, 17/2/2001; X-ray R) shoulder and hand, 14/12/2000; NM R)
shoulder, 21/6/2002
October 2008 Page 39 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Report by Mr Bones, 4/2/2003 Report by Dr GS, Rheumatologist Reports by Dr XV, Occupational Physician Reports by Dr YZ, Occupational Physician Reports by Dr SS, Rheumatologist First Medical Certificate Advice of injury form Report by HH, Physiotherapist GP clinical notes, 11/11/1997 – 6/9/2003 A CV Reports by LJ, Management Consultants Work preparation programme Individual rehabilitation plan Client Consent for Collection and Release of Information Initial Occupational Assessment report by CF Initial Medical Assessment report by Dr EE.
The following details of interview are those as obtained from Mrs AB.
BackgroundAdequate information has been received for this vocational independence medical assessment. It does not conflict with her own history as related to me, which follows.
History of injury, treatment and progressMrs AB was working at a bank in 1992. She had two jobs. In the day she worked as a teller between 11am and 3pm, and at night she worked as a re-check computer operator between 5pm and 11pm or 12pm. She was using her index and middle fingers a lot in her work. She was carrying big bundles of cheques, putting them through the computer, carrying them in trays, and pigeon-holing them to the relevant banks. She developed soreness of her right shoulder, right arm, right hand, and the right side of her neck.
She attended many different types of physical treatment but found they didn’t really help. She seems initially to have been diagnosed with OOS of the right arm. Ultimately she was put off work in 1994. Despite stopping work she has continued to have some symptoms. These have been maximal around the right shoulder and have settled somewhat down in the arm.
Treatment summaryShe has attended physiotherapy, acupuncture, massage, and other physical therapies, which have not really helped much. She has had injections to her right shoulder and to the elbow and neck but these did not help. She used to take a lot of Paracetamol to assist but again doesn’t feel it really helped. She has seen numerous specialists over time, including Dr SS - Rheumatologist, Dr TW - Occupational Physician, Dr ED - Occupational Physician, Dr UO - Rheumatologist, and Mr Bones - Orthopaedic Surgeon. X-rays of the right shoulder and hand dated 19/12/2000 were normal.Right shoulder ultrasound of 15/2/2001 demonstrated some mild thickening of the subacromial bursa but the tendons of the rotator cuff appeared unremarkable. MRI of the right shoulder on 21/5/2002 suggested tendinosis of the supraspinatus, but in addition there was slightly unusual fluid signal at the myotendinous junction at the junction of
October 2008 Page 40 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
supra and infraspinatus, suggesting there may be a small interstitial tear.
Most recently she has seen Mr Bones, who indicates that the diagnosis is a right supraspinatus tendonitis and associated subacromial bursitis impingement. Because of the time course of matters he did not recommend surgery. He did recommend some specific shoulder exercises. These were shown to Mrs AB by her physio. She attended the physio for a total of 10 sessions and now continues to do the exercises at home herself, having learnt what to do. She has found that her shoulder pain has decreased and she is more confident in using her shoulder.
She takes Diclofenac only when pain is particularly bad, which is only about once a month since she started the shoulder exercises recommended by Mr Bones.
Present positionMrs AB indicates she has lived with symptoms for so long now that she has got used to them. However, her pain is only about once a month since starting the regular shoulder exercises, mainly from the right shoulder region, and she tends to point to the superior aspect of the shoulder in the acromio clavicular area when saying this. She describes the pain as a muscle pulling pain. She takes Diclofenac for it only when it is particularly bad, but it helps quite swiftly. Down her arm she feels her symptoms have improved, but there is still some soreness that she notes if she has been busy doing something. Activities that can aggravate pain include stretching up for cleaning, hanging washing, and dusting. Vacuuming, washing dishes and making beds can also make matters worse. She finds that attempting to massage the shoulder or pushing on it actually hurts and doesn’t help. She doesn’t find that heat or other therapies make a difference. The only thing that she isolates as assisting is the medication when pain is really bad.
Sleep can be disturbed if she rolls onto her right side, as it then hurts. She can drive. She feels that using a computer causes an unpleasant sensation of electricity and so she avoids its use. Often when she performs excessive activity with the right arm she does not notice problems while doing so, but will notice increased pain when she sits down and rests afterwards.
Past history of illnessMrs AB has non-insulin dependent diabetes for which she takes Diamicron and Atacand to gain control. She had modest hypercholesterolemia, obesity, raised feffitin, liver function abnormalities, and had an elevated white cell count and associated lymphocytosis when seen by Prof HA, the physician at the Diabetic Clinic. Once the diagnosis of diabetes was made the other problems apparently settled. She has lost weight since this time also. Ultrasound of the liver showed mild fatty changes. A liver biopsy has been taken but was normal. She has suffered with recurrent headaches of the fronto-temporal region, particularly of the R) side of her head. She gets these about twice a week. Sometimes she will use Brufen for them. She does not recall any other major past history.
Occupational historyMrs AB was born in Australia and moved to New Zealand in 1969. She worked as an accounts clerk at a printing factory for two years. She was an accounts clerk in a government department for a year. She was a bank teller for a bank for two years. She was an accounts clerk for six months. She worked in another bank as a bank officer for five years. She left the work there in 1993 because of R) shoulder pain and has not worked since then.
General health (medical, personal, recreation)
October 2008 Page 41 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Mrs AB is married. She has two children, aged 16 and 6. She smokes 10 cigarettes per day. She does not drink alcohol. She indicates she used to be quite sporty, but doesn’t do any regular exercise now. She maintains interests in the church. Her husband is a minister and she is involved in Bible studies etc. She reads a lot and does crosswords.
PainMrs AB describes some muscle pulling pain, which used to be present all of the time around the right shoulder joint but is now only probably once a month. At times, however, she can still suffer with soreness affecting the right neck and the right upper arm, and a strange sensation of the right hand.
ExaminationA pleasant woman with normal gait, posture, and handshake. She appeared to sit through the interview in comfort. Movements of fingers, thumbs, and wrists were fully normal. There was slight reduction in full left elbow flexion from a childhood fracture, restricting flexion on the left elbow to 100. Movements of the left shoulder were normal. Movements of the right shoulder were limited to 150of abduction, 150of flexion, 50of internal rotation, and normal ranges of adduction, extension, and external rotation.
The circumference of the right upper arm was 0.5cm greater than that of the left upper arm. The circumference of the right forearm was 0.5cm greater than that of the left forearm. Reflexes were present and normal (biceps, triceps, and supinator).
Two-point sensation was normal on the digits of both hands. The colour of both hands and arms was normal. Pulses were present and normal at both wrists. There was no scarring or evident deformity of the right arm. She was tender to pressure along the joint line of the right shoulder, but not over the AC joint. There was slight tenderness to palpation into the muscles of the right upper arm; the elbow was non-tender. There was slight tenderness to palpation of the right wrist and hand generally.
Movements of the neck were full in all directions, but lateral flexion to the left did cause soreness on the right-hand side. There are notable scars on the anterior chest including one with what appears to be keloid formation from a mole removal when she was younger. Phalens and Tinel’s tests were negative. She appeared in general to be well.
General Weight: 75kg BMI: 29 Height: 160cm Vision: She does wear spectacles Mobility: Appeared fully normal Hearing: Appeared normal through our interview Other: She is right handed.
Summary of diagnostic investigationsX-rays of the right shoulder and hand dated 19/12/2000 were normal.
15/2/2001 demonstrated some mild thickening of the subacromial bursa, but the tendons of the rotator cuff appeared unremarkable.
MRI of the right shoulder on 21/6/2002 suggested tendinosis of the supraspinatus, but in
October 2008 Page 42 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
addition there was slightly unusual fluid signal at the myotendinous junction at the junction of supra and infraspinatus, suggesting there may be a small interstitial tear.
Discussion and opinionMrs AB has been diagnosed with right supraspinatus tendonitis and associated subacromial bursitis and impingement by Mr Bones, having undergone MRI scanning. This will be the prime diagnosis for the main site in which she gets symptoms now. Tenderness, although slight of the wrist and hand, would not be explainable by this and one would therefore think that there has perhaps been more than one diagnosis here. I would imagine that she perhaps has a resolving pain syndrome of the right upper limb, and we see the residual sign of this. As stated, the main focus for pain now, however, is the right shoulder and the MRI has demonstrated pathology here confirmed in Mr Bones’ report.
The referral to an orthopaedic surgeon that was recommended in the IMA report of Dr EE has clearly resulted in a considerable improvement in her shoulder pain and condition in general. She has learnt to do the shoulder exercises and does these on a regular basis at home as she has found that they have been very helpful.
No further treatment or rehabilitation initiatives are indicated at this time.
The main restriction therefore would be in excessive or heavy shoulder usage and this would relate to heavy lifting or stretching up or across on the work type detail sheets. There may well still be, however, some residual restriction of persistent and excessive repetitive motion of the hands in tasks such as keyboarding.
Work capacity
Mrs AB has the physical capability to work for 35 hours or more as:
42213 ReceptionistHeavy lifting and stretching up or across are not featured in the work type detail sheets. Repetitive movements are intermittent and hand tools are commonly used. This seems very reasonable. Although computers would be used she would not have to do great tomes on them at a time and the job description is well mixed. Walking and sitting are featured, as are mental activities. Again, given Mrs AB’s restrictions, she has the physical capability to do this job. She indicates she has never done this work and it sounds like it could be a good challenge.
She finds the prospect of computer keying and typing quite scary.
42111 CashierHeavy lifting and stretching up or across are not featured on the work type detail sheet. Repetitive movements and the use of hand tools are frequent to constant and are necessary for operating electronic tills and cash handling.
The position generally requires contact with the public in such a way that one is not actually typing consistently throughout, and in my opinion I feel that she would cope in this role.
She indicated that yes, she supposed there wouldn’t be anything wrong
October 2008 Page 43 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
with doing this type of work. She thought this might be possible.
42113 Ticket IssuerHeavy lifting and stretching up or across are not featured on the work type detail sheet. Although repetitive movements and the use of hand tools are common, the position generally requires contact with the public in such a way that one is not actually typing consistently throughout, and as such I feel that she would cope in this role.
She indicated that yes, she supposed there wouldn’t be anything wrong with doing this type of work.
Mrs AB does not have the capacity to work as a:
552111 Bank WorkerSitting is the most common position in this work type detail sheet. Repetitive movements are intermittent and hand tools are commonly used. She might end up having to do too much in the way of consistent computer input, but in other roles would not.
She indicates that she would like to do this work, but knows that she wouldn’t be able to due to her experiences in the early 90s.
531111 General ClerkHeavy lifting is indicated to be uncommon in the work type detail sheet. Sitting is the common position. Repetitive arm, hand, and finger movements (keyboarding and mouse) are constant for data-entry and data and word processing tasks. The use of minor office hand tools such as pens, calculators, and staplers, as well as telephones will also be occasional to frequent.
She thinks she might like to do this, but wonders about how much computer use and how she would go answering the phone and whether this would be possible for her.
551111 Accounts ClerkThe work type detail sheet has common repetitive movements and the use of hand tools. Sitting is the common position. It would depend on the particular position, but the excess hand and computer usage might become a problem.
She indicates she used to do this and she liked to do it, but she doesn’t think she would manage the computer use now.
551112 Cost ClerkCommon repetitive movements and hand tool usage are features of this work type detail sheet. Sitting is the common position. The job description would indicate a more consistent computer usage and this might well then be a problem.
She felt this was similar to the accounting and bookkeeping clerk one and the computer use might be a problem.
551211 BookkeeperCommon repetitive movements and hand tool usage. Sitting is the common position. The work type detail sheet indicates a more consistent computer usage and this might well then be a problem.
October 2008 Page 44 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
She felt this was similar to the accounting, office clerk, and bookkeeping clerk ones and the computer use might be a problem.
631111 Checkout OperatorHeavy lifting is indicated to be uncommon in the work type detail sheet, but lifting is required albeit perhaps not heavy on a very repetitive basis. The repetitive movements and use of hand tools are indicated to be common. Twisting the body or neck is indicated to be common. Stretching up or across is not featured although this would seem to probably be a feature normally. Overall it is something I would not suggest.
She agreed that packing goods would be a problem for her and did not think this would be a good idea.
She was pleasant and co-operative to interview. She presents as a likable, cheerful person, who would probably be an asset to many workplace settings. I hope that she finds suitable work in the near future. I wish her all the best in general for the future.
TimeInterview commenced at 9.30amFinished at 10.50amcc ACC Client service staffcc GP
October 2008 Page 45 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 6: Example – Work Type Detail Sheet
Fishing Hand - 899212
Description:
Catches fish and shellfish using nets, pots, lines and traps in ocean and inland waters.Work Tasks (may include any combination of the following):
Attaches gear and fastens towing cables to nets; casts and lowers nets, pots, lines and traps into water; prepares lines, attaches running gear and bait, and sets lines into position; hauls in fishing gear and removes fish and other marine life; sorts, cleans, preserves, stows and refrigerates catch.
Work Environment: Works on fishing boats or varying sizes carrying out a full range of deck and other on-
board fishing-related tasks. Works in almost all weather and sea conditions. Occasionally to frequently works with ropes.Work Function/Activity2: Medium to heavy physical demand levels. Stands and walks about the deck of vessel to move ropes, lower pots and nets, clean-
up, and complete general on-board tasks. Uses upper limbs and body to stretch up and across occasionally when lowering fishing
equipment, working winches or brining catch on board. Bends occasionally to frequently. Occasionally to frequently squats or crouches when inspecting catch. Occasionally to frequently twists the body or neck. Frequently lifts and carries equipment, catch and other on-board supplies and
materials. Repetitive hand and arm movements are required occasionally when processing fish
and working ropes and winches. Driving is not required. Uses a range of hand (or power) equipment such as winches, cleats and boat hooks. Frequently climbs on and off vessel and may climb on superstructure or rigging for some
tasks. Mental activities necessary include practical technical and organisational skills. Further Comments:
There are limited opportunities for flexibility of movement.Entry Requirements:
Nil.
2 This document is based on ANZSCO, 2006 (code 899212). Other sources of information that may have been consulted are industry contacts, employers, newspapers and internet-based sources. For physical demand level definitions see Matheson, L.N. (1996). Functional Capacity Evaluation.
October 2008 Page 46 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 7: US Department of Labor Physical Demand Characteristics of Work
OverviewThe 37.02 US Department of Labor Physical Demand Characteristics of Work chart, lists the occupational requirements for physical exertion.
Parameters Amount of weight moved at work Relative frequency that activity occurs during workday (occasional, frequent or
constant).
Physical demand level
Occasional(0-33% of the workday)
Frequent(34-66% of the workday)
Constant(67-100% of the workday)
Typical energy required
Sedentary 10lbs (4.5 kilos)
negligible negligible 1.5-2.1 METS
Light 20lbs (9 kilos) 10lbs (4.5 kilos) and/or walk and/or stand with operation of controls
negligible and/or operate controls while seated
2.2-3.5 METS
Medium 20-50lbs (9-22.7 kilos)
10-25lbs (4.5-11.4 kilos)
10lbs (4.5 kilos)
3.6-6.3 METS
Heavy 50-100lbs (22.7-45.4 kilos)
25-50lbs (11.4-22.7 kilos)
10-20lbs (4.5-9 kilos)
6.4-7.5 METS
Very heavy > 100lbs (45.4 kilos)
> 50lbs (> 22.7 kilos)
20lbs (> 9 kilos)
> 7.5 METS
Where Operation of controls includes pushing and/or pulling of arm and/or leg controls Operating controls while seated includes pushing and/or pulling of arm and/or leg
controls.
ReferenceMatheson LN. Chapter 18: Functional Capacity Evaluation. pages 168-188. In: Demeter SL, Andersson GBJ, Smith GM. Disability Evaluation. Mosby. American Medical Association. 1996.
Appendix 8: Frequently Asked Questions (FAQs)
October 2008 Page 47 of 50

Vocational Medical Assessors – Operational Guidelines: Appendices
How do I take into account non-accident conditions when writing my report?
When completing an IMA report the assessor identifies types of work that are currently medically sustainable or are likely to be medically sustainable following rehabilitation. In doing this, the assessor must consider both the ACC covered injury and non-ACC covered conditions. Types of work that are likely to be sustainable only after treatment or rehabilitation will need a recommendation for treatment or rehabilitation recommendation. This will be limited to the needs of the ACC covered injury and the impact on the client’s vocational rehabilitation. However, it must also take into account the non-covered conditions. For example, if a client has ischaemic heart disease and gets angina on exertion, and had as the covered injury a fractured femur, the rehabilitation recommended would only be looking at helping with the sequelae of the fracture of the femur but, due to the heart condition, the recommendation would likely rule out any work types that were not sedentary or light as given by the work type detail sheet.
What if I consider that the medical diagnosis provided by ACC is wrong?
The basis of good rehabilitation or treatment is a good diagnosis. Assessors will receive medical reports that ACC has been sent and on which the cover decision will be based. If as an assessor you conclude that the diagnosis or characterisation of the injuries in these reports is incorrect, you need to indicate this in the ‘Discussion and Opinion’ section of your report. Your recommendations must be based on your own diagnosis. On receiving such an assessment ACC will need to examine whether the different diagnosis given by you means that ACC needs to re-examine the issue of cover for the client. It is not your role as a vocational medical assessor to look at the question of cover. Your role is to look at the question of vocational rehabilitation and the capacity for work of the client with the conditions as assessed by you.
What is the definition of heavy lifting?
See Appendix 7 for definitions of ‘heavy’, ‘very heavy’, ‘medium’, ‘light’ and ‘sedentary’.
What do I do if the IOA doesn’t seem correct?
If this is identified before the medical assessment, please contact the client service staff member who sent the referral and advise of your concerns.
If you identify it at the time of the actual appointment with the client, proceed with the assessment as usual and contact the client service staff member before completing the report.
If there is any change, the client can always be contacted for comment after the assessment or a follow-up can be arranged if the changes are major.
What is meant by “Sedentary to light work. Frequently standing at sales counter for most of the period employed” in the 52111 Sales Assistant Work
October 2008 Page 48 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
Type Detail Sheet from the occupational assessor?
‘Sedentary to light work’ refers to the requirement to lift negligible to 4.5 kilos and/ or walk and/or stand with the operation of controls. ‘Frequent’ refers to 34 – 66% of the work day. In this case the typical energy required is 1.5 – 3.5 Mets. One Met is the amount of expended energy equal to 3.5ml (kg – min) oxygen consumption. See also, ‘Appendix 7 - US Department of Labor Physical Demand Characteristics of Work’.
Why are 35 hours stipulated?
This is the number of hours that are required by the legislation. The AC Act defines vocational independence as being the capacity to work in a type of employment for 35 hours or more per week.
Who do I contact if I have questions about a vocational medical assessment?
You should in the first instance contact the ACC client service staff member who sent you the referral. ACC has staff who are knowledgeable about vocational rehabilitation from both a medical perspective and a rehabilitation perspective and the client service staff member can put you in contact with the appropriate person if required.
Are there any national guidelines on doing assessments for ACC?
Please see the New Zealand Medical Council’s statement on “Non-Treating Doctors Performing Medical Assessments of Patients for Third Parties”.
This is held on their website: Medical Council of NZ under Publications and guidance > Good Medical Practice - Professionalism.
Why can’t I: Add vocational comments to the IMA/VIMA when I have an occupational
qualification? Add new jobs to the IMA/VIMA? Add tasks if I know the job and disagree with the occupational assessor?
Medical assessors are the experts in the medical area and need to limit their comments to this field. This is required by the AC Act and relevant case law.
October 2008 Page 49 of 50
Vocational Medical Assessors – Operational Guidelines: Appendices
Appendix 9: Flowchart of Client Participation in Vocational Rehabilitation
October 2008 Page 50 of 50