Vocal Fold Lipo Injection: New Potentials from Regenerative … · Department of...
6
Central Annals of Otolaryngology and Rhinology Cite this article: Ribeiro L, Castro E, Ferreira M, Carvalho P, Gomes M, et al. (2015) Vocal Fold Lipo Injection: New Potentials from Regenerative Medicine. Ann Otolaryngol Rhinol 2(4): 1036. *Corresponding author Leandro Ribeiro, Department of Otorhinolaryngology, Vila Nova de Gaia/Espinho Hospital Center, Rua Conceição Fernandes, 4434-502 V. N. Gaia, Portugal, Tel: 351-227-865-100; Fax: 351-227-83020; Email: Submitted: 13 March 2015 Accepted: 13 May 2015 Published: 14 May 2015 Copyright © 2015 Ribeiro et al. OPEN ACCESS Keywords • Vocal fold paralysis • Laryngoplasty • Platelet-rich plasma • Adipose tissue • Adipose-derived stem cell Research Article Vocal Fold Lipo Injection: New Potentials from Regenerative Medicine Leandro Ribeiro 1 *, Eugénia Castro 1 , Manuela Ferreira 1 , Pedro Carvalho 2 , Manuela Gomes 2 and Artur Conde 1 1 Department of Otorhinolaryngology, Vila nova de Gaia/Espinho Hospital Center, Portugal 2 Department of Biomaterials, Biodegradables and Biomimetics, Research Institute- Braga, Portugal Abstract Introduction: Vocal fold lipoinjection (VFLI) has been used in glottal insufficiency rehabilitation, although with inconsistent results due to unpredictable fat resorption. Recent studies demonstrate that platelet-rich plasma (PRP), obtained from autologous venous blood, increases graft stability, stimulating the proliferation of adipose stem cells (ASC). Objective: The objective of this work is to confirm the presence of ASC in the adipose tissue and verify the possible effect of PRP on graft stability and survival. Material and Methods: To this end the abdominal fat samples of two patients with unilateral vocal fold paralysis who had undergone VFLI were analysed by immunofluorescence, using monoclonal antibodies to specific CD markers, and flow cytometry. Simultaneously the authors searched the published literature, chose relevant references and extracted and systematized the data to make a study protocol for application of PRP on VFLI. Results: The authors confirmed the presence of ASC in adipose tissue. Conclusion: PRP should improve graft survival, enhancing de functional and long- term results of VFLI. INTRODUCTION Unilateral vocal fold paralysis and congenital or acquired tissue defects in the superficial layers of them are a frequent cause of severe breathy dysphonia resulting from insufficient vocal fold adduction. The glottic air leak causes a poorly audible voice and fatigue on phonation [1]. Intracordal injection therapy was first described by Brunings [2] in 1911. It has been used in vocal rehabilitation to treat the glottic insufficiency caused by recurrent unilateral laryngeal nerve paralysis, vocal cord atrophy and sulcus vocalis. This procedure is intended to correct position and/or volume of the vocal cord and to attain glottal closure [3]. Various types of materials including silicon, collagen, fascia and fat, have been used with relative success. Autologous fat tissue has been considered to be ideal “filler” for vocal fold augmentation because it is biocompatible, versatile, nonimmunogenic, inexpensive and readily obtainable with low donor site morbidity. Techniques using fat for intracordal injection was first reported by Mikaelian [4] in 1991, and has been used clinically worldwide. Autogenous fat injection laryngoplasty is a simple, inexpensive and safe procedure [5,6] which improves the voice parameters over the short term [5-7]. However, the fat absorption which occurs over the time turns the long-term voice- outcome unpredictable, limiting its role in the modern era [8,9]. Kruschechewsky and colleagues (10) showed an 82% absorption rate of autologous fat graft 12-weeks after vocal fold lipoinjection (VFLI) in a canine model with a vocal fold paralysis. In a similar study with a feline model, Saccogna [11] showed that the injected fat material was stable at 8 months after the injection but not at 12 months. The adipose tissue seems to be a particularly good source of stem cells and it contains more multipotent cells per cc than bone marrow: one gram of adipose tissue yields ~5 × 103 stem cells, which is 100-fold higher than the number of mesenchymal stem cells in one gram of bone marrow [12]. This tissue consists of adipocytes and a heterogenous population of various other cells types, including adipose-derived stem cells (ASC), preadipocytes, endothelial cells, pericytes from blood vessels and fibroblasts [13,14]. ASC, sometimes called MSC [14], are similar to bone marrow-derived stem cell (BMSC) in that they reside in a perivascular location [12] and are capable of maturing
Transcript of Vocal Fold Lipo Injection: New Potentials from Regenerative … · Department of...

Central Annals of Otolaryngology and Rhinology
Cite this article: Ribeiro L, Castro E, Ferreira M, Carvalho P, Gomes M, et al. (2015) Vocal Fold Lipo Injection: New Potentials from Regenerative Medicine. Ann Otolaryngol Rhinol 2(4): 1036.
*Corresponding authorLeandro Ribeiro, Department of Otorhinolaryngology, Vila Nova de Gaia/Espinho Hospital Center, Rua Conceição Fernandes, 4434-502 V. N. Gaia, Portugal, Tel: 351-227-865-100; Fax: 351-227-83020; Email:
Submitted: 13 March 2015
Accepted: 13 May 2015
Published: 14 May 2015
Copyright© 2015 Ribeiro et al.
OPEN ACCESS
Keywords•Vocal fold paralysis•Laryngoplasty•Platelet-rich plasma•Adipose tissue•Adipose-derived stem cell
Research Article
Vocal Fold Lipo Injection: New Potentials from Regenerative MedicineLeandro Ribeiro1*, Eugénia Castro1, Manuela Ferreira1, Pedro Carvalho2, Manuela Gomes2 and Artur Conde1
1Department of Otorhinolaryngology, Vila nova de Gaia/Espinho Hospital Center, Portugal 2Department of Biomaterials, Biodegradables and Biomimetics, Research Institute- Braga, Portugal
Abstract
Introduction: Vocal fold lipoinjection (VFLI) has been used in glottal insufficiency rehabilitation, although with inconsistent results due to unpredictable fat resorption. Recent studies demonstrate that platelet-rich plasma (PRP), obtained from autologous venous blood, increases graft stability, stimulating the proliferation of adipose stem cells (ASC).
Objective: The objective of this work is to confirm the presence of ASC in the adipose tissue and verify the possible effect of PRP on graft stability and survival.
Material and Methods: To this end the abdominal fat samples of two patients with unilateral vocal fold paralysis who had undergone VFLI were analysed by immunofluorescence, using monoclonal antibodies to specific CD markers, and flow cytometry. Simultaneously the authors searched the published literature, chose relevant references and extracted and systematized the data to make a study protocol for application of PRP on VFLI.
Results: The authors confirmed the presence of ASC in adipose tissue.
Conclusion: PRP should improve graft survival, enhancing de functional and long-term results of VFLI.
INTRODUCTIONUnilateral vocal fold paralysis and congenital or acquired
tissue defects in the superficial layers of them are a frequent cause of severe breathy dysphonia resulting from insufficient vocal fold adduction. The glottic air leak causes a poorly audible voice and fatigue on phonation [1]. Intracordal injection therapy was first described by Brunings [2] in 1911. It has been used in vocal rehabilitation to treat the glottic insufficiency caused by recurrent unilateral laryngeal nerve paralysis, vocal cord atrophy and sulcus vocalis. This procedure is intended to correct position and/or volume of the vocal cord and to attain glottal closure [3]. Various types of materials including silicon, collagen, fascia and fat, have been used with relative success. Autologous fat tissue has been considered to be ideal “filler” for vocal fold augmentation because it is biocompatible, versatile, nonimmunogenic, inexpensive and readily obtainable with low donor site morbidity. Techniques using fat for intracordal injection was first reported by Mikaelian [4] in 1991, and has been used clinically worldwide. Autogenous fat injection laryngoplasty is a simple, inexpensive and safe procedure [5,6] which improves
the voice parameters over the short term [5-7]. However, the fat absorption which occurs over the time turns the long-term voice-outcome unpredictable, limiting its role in the modern era [8,9]. Kruschechewsky and colleagues (10) showed an 82% absorption rate of autologous fat graft 12-weeks after vocal fold lipoinjection (VFLI) in a canine model with a vocal fold paralysis. In a similar study with a feline model, Saccogna [11] showed that the injected fat material was stable at 8 months after the injection but not at 12 months.
The adipose tissue seems to be a particularly good source of stem cells and it contains more multipotent cells per cc than bone marrow: one gram of adipose tissue yields ~5 × 103 stem cells, which is 100-fold higher than the number of mesenchymal stem cells in one gram of bone marrow [12]. This tissue consists of adipocytes and a heterogenous population of various other cells types, including adipose-derived stem cells (ASC), preadipocytes, endothelial cells, pericytes from blood vessels and fibroblasts [13,14]. ASC, sometimes called MSC [14], are similar to bone marrow-derived stem cell (BMSC) in that they reside in a perivascular location [12] and are capable of maturing

Central
Ribeiro et al. (2015)Email:
Ann Otolaryngol Rhinol 2(4): 1036 (2015) 2/6
toward multiple mesodermal tissue types: bone, cartilage, and adipose tissue [12-19]. ASC expression profile has not been firmly established. They are generally considered to be CD45- CD235a- CD31- CD34+. Negativity for CD106 and positivity for CD36 distinguishes ASC from BMSC [12-14].
The plasticity of ASC offers great potential in regenerative medicine and aesthetic surgery [20]. ASC when stimulated by growth factors may have an important role in vocal cord graft survival, enhancing the long-term functional results of VFLI.
The main goal of regenerative medicine is restoring functional and/or structural tissue by using living tissues that will later be integrated in patients [21]. In this process, three basic components are generally present - cells, regulators/growth factors and scaffolds, which may or not be used simultaneously [22-24]. Cell therapy consists of depositing selected living cells in an appropriate scaffold that, when exposed to a specific micro environment will multiply and differentiate in the desired structure [21-23]. Stem cells are assumed as having the highest potential in regenerative medicine. They can be obtained from either embryonic or mature tissues: embryonic stem cells (totipotente) are derived from blastocysts, and therefore can differentiate into any of the germ layers (endoderm, mesoderm or ectoderm) [25,26]; on the other hand, adult stem cells can be collected from certain niches in the body, namely bone marrow, adipose tissue or blood [24], and give rise to specialized cell types of the tissue in which they reside, but can also differentiate into specialized cells of other tissues [16].
Platelet-rich plasma (PRP) is developed from autologous blood and consists of a volume of autologous plasma with a platelet concentration above the baseline and therefore, an increased concentration of platelet growth factors is present as well [27]. Its role in fat grafting survival and its clinical application
is a fast developing area in some medical specialties. It appears that implementation of PRP enhances the fat graft survival.
MATERIALS AND METHODSThe purpose of this article is to:
1-Confirm the presence of ASC in the low abdominal fat;
2-Verify the effect of PRP in the VFLI.
To this end we made a characterization of abdominal fat samples of two patients with unilateral vocal fold paralysis who had undergone VFLI. After isolation and cultivation, cells were harvested using TrypLE Express without phenol red (Invitrogen) [28], washed with PBS three times, and aliquots of 150 x 103 cells were incubated for 20 minutes in the dark with monoclonal antibodies directed against cluster-of-differentiation 29 (CD 29) (eBioscience Cat. No. 14029982), CD34 (BD Biosciences Cat. No.555822), CD45 (BD Cat. No. 555482), CD73 (BD Biosciences Cat. No. 550257), CD90 (BD Biosciences Cat. No. 559869), CD105 (eBioscience Cat. No. 16-1057-82) and SSEA-4 (eBioscience Cat. No. 53-8843). After incubation, cells were washed with PBS supplemented with 1% bovine serum albumin three times and fixed in 1% formaldehyde overnight at 4º C. For each sample, 20 · 103 events were collected on a Becton Dickinson FAC Scalibur flow cytometer using CELL Quest acquisition software (Becton Dickinson) and analyzed using CELL Quest software (Becton Dickinson). This antibody panel was selected, in part, based on the International Society for Cell Therapy (ISCT) and IFATS joint statement article on the criteria for defining adipose-derived stromal/stem cells [29,30].
Simultaneously, we searched the published literature on this topic, chose relevant references, and extracted and systematized the data to make a study protocol for application of PRP on VFLI.
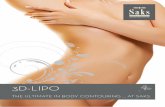
Figure 1 Flow cytometry analysis of patient no. 1.
Figure 2 Flow cytometry analysis of patient no. 2.

Central
Ribeiro et al. (2015)Email:
Ann Otolaryngol Rhinol 2(4): 1036 (2015) 3/6
RESULTSThe fat samples analyses (Figures 1,2) confirmed the
presence of a cellular subpopulation, which tested positive for embryonic cell surface marker SSEA-4. The analysis also revealed that the fat samples contained CD105 (endoglin), CD73 (5′ ecto-nucleotidase) and CD90 (Thy-1), which are in agreement with minimal criteria to define human MSCs by “The International Society for Cellular Therapy” [31] and the joint statement for characterization of ASCs from International Federation for Adipose Therapeutics and Science (IFATS) [32].
DISCUSSION
Fat as a source of ASC
Adipose tissue, like the tissue used in VFLI is more than filler. Fat is an ideal source of autologous ASC, particularly in comparison with the traditional bone marrow procurement procedure. Adipose tissue has the advantage of greater accessibility and minimal morbidity involved in its harvest [14,27]. ASC population is adequate for clinical-grade cell manipulation in regenerative medicine of the vocal cords [12,14,16,27]. Although adipose tissue is abundant and easily accessible for autologous tissue replacement, the clinical success of fat grafting is limited by a variable but unpredictable low survival rate [8-11,27].
Cicero and colleagues [16] investigated fat samples harvested from 12 patients affected by breathy dysphonia who had undergone VFLI. After immunocytochemistry analysis and flow cytometry they concluded that “adipose tissue, administered to patients in order to restore glottic competence, contains mesenchymal stem cells”. Specifically, they identified a subpopulation consistent with perivascular/pericyte-like cells, showing that ASC include a multipotential stem cell population that can be associated with cells surrounding blood vessels. They also found SSEA-4 markers for undifferentiated pluripotent human embryonic stem cells, which could explain the high differentiation plasticity of ASC. Zannettino et al [30] have suggested that MSC reside in perivascular niches, which prompts the speculation that perivascular structures (cells and extracellular matrices) may provide signals that balance the maintenance of MSC in an undifferentiated state and their commitment to differentiation.
In this work the authors confirmed the ASCs presence in abdominal fat samples used for vocal fold lipoinjection.
Fat graft survival theories
VFLI is not just a matter of “filling the gap” but of generating a long-term, stable tissue that interacts with adjacent tissue. Problems associated with fat flap transfer, such as resorption are an issue that we need to overcome. This was the goal of this work.
After transplantation approximately 20-80% of fat graft volume is lost [10,15,27]. The reasons behind this poor outcome are unclear. Histologic analysis of fat grafts demonstrates an inflammatory response with acute necrosis, likely associated with reduced fat vascularization [15]. According to other theories, some researchers believe that the preadipocytes and ASC might be the only cell types that survive transplantation, and the variability of these cells between individuals may be one of the
reasons for the observed unpredictability. Maybe preadipocytes and ASC are much more resistant to transfer trauma than adult adipocytes resultant of the differences between metabolic rate and intracellular content of lipids which could explain their survival with much lower nutrition and oxygen [17,33,34]. These cellular elements will, in turn, proliferate and differentiate into mature adipocytes and, depending on environment, into different tissue types.
Platelet-rich plasma enhances fat graft survival
PRP is an autologous blood product formed by selective removal or exchange of either packed red blood cells, leucocyte-rich or platelet-rich layers, or plasma, with a continuous flow blood separator machine [19]. Uses of PRP include providing is an alternative and easily controllable strategy for the local release of multiple endogenous growth factors for tissue regeneration [35,36]. PRP has been used with relatively success and safety in areas such as plastic surgery, maxillofacial surgery and in the treatments of soft tissue ulcers. After activation, PRP releases a pool of growth factors; specifically, PRP releases basic fibroblasts growth factor (b-FGF), insulin-like growth factor-1 (IGF-1), transforming growth factor-β (TGF-β), platelet-derived growth factor (PDGF), epidermal growth factor (EGF) and vascular endothelial growth factor (VEGF) [8,15,27,37]. These growth factors aid in healing by attracting undifferentiated cells into the newly formed matrix, triggering cell division [20] and favoring angiogenesis, therefore enhancing graft survival [15,27,37].
Cervelli [20] observed that PRP (with insulin) had a positive effect on adipogenic differentiation of human ASCs, preventing its proliferative arrest and/or apoptosis. In another study, the same author used several PRP concentrations in patients with: (group A) soft tissue defects associated with signs of aging, (group B) chronic venous lower extremity ulcers, and (group C) hemifacial atrophy. He concluded that the PRP stimulates adipose tissue growth, its differentiation from ASC and early development of a neoangiogenic microcapillary network in an effect dose-dependent [19]. In a study with rabbits, Fraga [27] observed that PRP increases the number of viable adipocytes and blood vessels, while diminishing the necrotic areas and fibrosis, and enhancing free fat graft survival. Gentile P. and colleagues [38] compared the effects of fat alone and fat with PRP on patients with burns sequels and post-traumatic scars. They observed 69% maintenance of contour restoration after 1 year compared with that of the control group (39% maintenance). In another studying using a rabbit model, Rodríguez-Flores et al [39] observed that the infiltration of fat tissue and PRP in the upper lip generates a lower inflammatory reaction and less formation of oil cysts than the infiltration of isolated fat. In another study, Salgarello M [40] reported to have found no positive effect of PRP on breast graft survival. The same was reported by Por YC et al [41] in a study using mice models. Conversely, Willemsen [42] concluded that the procedure was safe and is associated with a low complication rate.
PRP preparation (Figure 3)
PRP is a volume of plasma fraction of autologous blood having platelet concentrations above baseline whole-blood values due to processing and concentration [27,43]. Traditionally, it is used in various surgical fields to enhance soft-tissue and bone healing by delivering supra-physiological concentrations of autologous

Central
Ribeiro et al. (2015)Email:
Ann Otolaryngol Rhinol 2(4): 1036 (2015) 4/6
platelets to the site of tissue damage. These preparations may provide a good cellular source of various growth factors and cytokines, and help modulate tissue response to injury [42]. Activated platelets, upon contact with exposed endothelium within wounds or damaged tissues, are known to release key wound healing factors including PDFG, TGF, VEGF, IGF, and EGF [8,15,27,37,44]. Although PRP seems to be used more frequently in routine medical practice, there are few robust and controlled clinical trials, which help to establish precise clinical protocols [43].
There are a number of commercially standard kits that produces relatively small volumes of PRP. These include GPS (Biomet, Warsaw, IN), the PCCS (Implast Innovations, Inc., Palm Beach Gardens, FL), the Symphony II (DePuy, Warsaw, IN), the SmartPReP (Harvest Technologies Corp., Norwell) and Magellan (Medtronic, Minneapolis, MN) [45,46]. In this work, the authors used one of the available commercial PRP production kits- Gravitational Platelet Separation System (GPS System, Biomet). The system consists of a disposable GPS tube that is used with a bench-top centrifuge. According to the manufacturer, the final product of PRP will contain over 90% of the available platelets in the blood sample.
Preparation can be performed in the operating room during the actual surgical intervention and takes approximately 30 minutes. First, 6 ml (1 ml=1 cm3=1 cc) of Anticoagulant Citrate Dextrose Solution (ACD-A) is drawn into a 60 ml syringe, followed by 54 ml of whole blood. The sample is gently agitated to mix the anticoagulant thoroughly with the whole blood.
The sample is then transferred to the platelet separator, which is then subjected to centrifugation protocol (3200 rotation per minute, 15 minutes). Following centrifugation, the blood sample is separated in different blood fractions. Separation of blood fractions is due to differences in the density of the blood components: the red blood cells form a red-colored fraction on the bottom of the tube separated through a buoy from the buffy coat, a whitish layer forms that is rich in white blood cells, platelets and the platelet-poor plasma, which contains autologous fibrinogen and is poor in platelets, forms on the top. In the next step PRP is extracted from the syringe and is mixed with augmentation material (see below).
Fat preparation (Figure4)
In the Hospital’s Department, the fat graft used in VFLI is obtained from the paraumbilical zone. Having placed the patient
Figure 3 PRP preparation.
Figure 4 Fat preparation.

Central
Ribeiro et al. (2015)Email:
Ann Otolaryngol Rhinol 2(4): 1036 (2015) 5/6
under general endotracheal anesthesia with a fine tube, a 1-2 cm incision is made. Then, small amounts of fat are harvested and transferred “en bloc” to a small dish with dexametasone (4 mg/ml) and regular insulin 100 U (the combination of insulin and dexametasone are theorized to stabilized the lipocyte cell membranes, which improves cell survival during the transplantation process). Then, the fat is manually fragmented, filtered and washed-out with saline solution in order to remove free fatty acids, serum and blood which induce an intense inflammatory response that diminishes the graft survival.
Injection of solution (fat with PRP)
The fat is mixed with PRP (Figure 5) at the rate of 1:4 (according to Fathi et al [47]). The solution is then loaded into a Bruning syringe with a long 18-gauge needle. The handle of the Brunning syringe is advanced until fat is just coming out of the syringe tip. A Hollinger`s laryngoscope is then inserted in order to expose the vocal folds. Next, the solution is injected lateral to vocal processes and profoundly on the paraglottic space of the affected vocal fold. The solution is injected until a bilateral over injection is achieved. At conclusion, the injection site is closed with a CO2 laser, minimizing the risk of graft extrusion.
Postoperative care
After VCLI, the authors emphasize strict vocal rest for 2 days and general rest for 2 weeks. Theoretically, rest minimizes the risk of implant extrusion and enhances graft survival. The patients receive intra- and post-operative corticosteroid treatments in order to minimize the risk of airway obstruction, antibiotic ciprofloxacin (500 mg 2 id) and esomeprazole (20 mg 2id).
CONCLUSIONFat grafts used in VFLI, though still in the treatment`s infancy,
offer great potential as a therapeutic strategy. In this work the authors confirmed the presence of multipotent stem cells in adipose tissue which, when stimulated with appropriate growth factors (like the growth factors present in PRP), should improve
graft survival and enhance the functional and long-term results of VFLI. Studies in vivo are needed in order to confirm the validity of the presented technique.
ACKNOWLEDGEMENTSTo Alex Vagonis (Pre-medical Student at the University of
Virginia) for grammatical correction.
REFERENCES1. Cantarella G, Baracca G, Forti S, Gaffuri M, Mazzola RF. Outcomes of
structural fat grafting for paralytic and non-paralytic dysphonia. Acta Otorhinolaryngol Ital. 2011; 31: 154-160.
2. Brunings W. Ubereineneue Behande lungs Methodeder Rekurrens-lamung.Verhandl Ver Deutch Laryngol 1911; 18: 93-98.
3. Tamura E, Fukuda H, Tabata Y. Intracordal injection technique: materials and injection site. Tokai J Exp Clin Med. 2008; 33: 119-123.
4. Mikaelian DO, Lowry LD, Sataloff RT. Lipoinjection for unilateral vocal cord paralysis. Laryngoscope. 1991; 101: 465-468.
5. Hsiung MW, Lin YS, Su WF, Wang HW. Autogenous fat injection for vocal fold atrophy. Eur Arch Otorhinolaryngol. 2003; 260: 469-474.
6. Havas TE, Priestley KJ. Autologous fat injection laryngoplasty for unilateral vocal fold paralysis. ANZ J Surg. 2003; 73: 938-943.
7. Umeno H, Chitose S, Sato K, Nakashima T. Comparative study of framework surgery and fat injection laryngoplasty. J Laryngol Otol Suppl. 2009; 35-41.
8. McCulloch TM, Andrews BT, Hoffman HT, Graham SM, Karnell MP, Minnick C. Long-term follow-up of fat injection laryngoplasty for unilateral vocal cord paralysis. Laryngoscope. 2002; 112: 1235-1238.
9. Laccourreye O, Papon JF, Kania R, Crevier-Buchman L, Brasnu D, Hans S. Intracordal injection of autologous fat in patients with unilateral laryngeal nerve paralysis: long-term results from the patient`s perspective. Laryngoscope 2003; 113: 541-545.
10. Kruschewsky Lde S, De Mello-Filho FV, Dos Santos AC, Rosen CA. Autologous fat graft absorption in unilateral paralyzed canine vocal folds. Laryngoscope. 2007; 117: 96-100.
11. Saccogna PW, Werning JW, Setrakian S, Strauss M. Lipoinjection in the paralyzed feline vocal fold: study of graft survival. Otolaryngol Head Neck Surg. 1997; 117: 465-470.
12. Casadei A, Epis R, Ferroni L, Tocco I, Gardin C, Bressan E, et al. Adipose tissue regeneration: a state of the art. J Biomed Biotechnol. 2012; 2012: 462543.
13. Kokai LE, Marra K, Rubin JP. Adipose stem cells: biology and clinical applications for tissue repair and regeneration. Transl Res. 2014; 163: 399-408.
14. Cawthorn WP, Scheller EL, MacDougald OA. Adipose tissue stem cells meet preadipocyte commitment: going back to the future. J Lipid Res. 2012; 53: 227-246.
15. Jin R, Zhang L, Zhang YG. Does platelet-rich plasma enhance the survival of grafted fat? An update review. Int J Clin Exp Med. 2013; 6: 252-258.
16. Lo Cicero V, Montelatici E, Cantarella G, Mazzola R, Sambataro G, Rebulla P, et al. Do mesenchymal stem cells play a role in vocal fold fat graft survival? Cell Prolif. 2008; 41: 460-473.
17. Coleman SR. Structural fat grafting: more than a permanent filler. Plast Reconstr Surg. 2006; 118: 108S-120S.
18. Albano JJ, Alexander RW. Autologous fat grafting as a mesenchymal
Figure 5 The addition of PRP to the fat.

Central
Ribeiro et al. (2015)Email:
Ann Otolaryngol Rhinol 2(4): 1036 (2015) 6/6
Ribeiro L, Castro E, Ferreira M, Carvalho P, Gomes M, et al. (2015) Vocal Fold Lipo Injection: New Potentials from Regenerative Medicine. Ann Otolaryngol Rhinol 2(4): 1036.
Cite this article
stem cell source and living bioscaffold in a patellar tendon tear. Clin J Sport Med. 2011; 21: 359-361.
19. Cervelli V, Bocchini I, Di Pasquali C, De Angelis B, Cervelli G, Curcio CB, et al. platelet rich lipotransfert: our experience and current state of art in the combined use of fat and PRP. Biomed Res Int. 2013; 2013: 434191.
20. Cervelli V, Scioli MG, Gentile P, Doldo E, Bonanno E, Spagnoli LG, et al. Platelet-rich plasma greatly potentiates insulin-induced adipogenic differentiation of human adipose-derived stem cells through a serine/threonine kinase Akt-dependent mechanism and promotes clinical fat graft maintenance. Stem Cells Transl Med. 2012; 1: 206-220.
21. Saxena A. Tissue Engineering. J Indian AssocPediatrSurg 2005; 10: 14-19.
22. Sivayoham E, Saunders R, Derby B, Woolford T. Current concepts and advances in the application of tissue engineering in otorhinolaryngology and head and neck surgery. J Laryngol Otol. 2013; 127: 114-120.
23. Hirano S. Tissue Engineering for Voice Disorder. JMAJ 2011; 139: 827-830.
24. Rebecca S. Bartlett, Susan L. Thibeault. Bioengineering the Vocal Fold: A Review of Mesenchymal Stem Cell Applications. Advances in Biomimetics. Prof. Marko Cavrak (Ed.) 2011; ISBN: 978-953.
25. Thomson JA, Itskovitz-Eldor J, Shapiro SS, Waknitz MA, Swiergiel JJ, Marshall VS, et al. Embryonic stem cell lines derived from human blastocysts. Science. 1998; 282: 1145-1147.
26. Mazzola RF, Cantarella G, Torretta S, Sbarbati A, Lazzari L, Pignataro L. Autologous fat injection to face and neck: from soft tissue augmentation to regenerative medicine. Acta Otorhinolaryngol Ital. 2011; 31: 59-69.
27. Pires Fraga MF, Nishio RT, Ishikawa RS, Perin LF, Helene A Jr, Malheiros CA. Increased survival of free fat grafts with platelet-rich plasma in rabbits. J Plast Reconstr Aesthet Surg. 2010; 63: e818-822.
28. Carvalho PP, Wu X, Yu G, Dietrich M, Dias IR, Gomes ME, et al. Use of animal protein-free products for passaging adherent human adipose-derived stromal/stem cells. Cytotherapy. 2011; 13: 594-597.
29. Kumai Y, Kobler JB, Park H, Lopez-Guerra G, Karajanagi S, Herrera VL, et al. Crosstalk between adipose-derived stem/stromal cells and vocal fold fibroblasts in vitro. Laryngoscope. 2009; 119: 799-805.
30. Zannettino AC, Paton S, Arthur A, Khor F, Itescu S, Gimble JM, et al. Multipotential human adipose-derived stromal stem cells exhibit a perivascular phenotype in vitro and in vivo. J Cell Physiol. 2008; 214: 413-421.
31. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006; 8: 315-317.
32. Bourin P, Bunnell BA, Casteilla L, Dominici M, Katz AJ, March KL et al. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: a joint statement of the International Federation for Adipose
Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013; 15: 641-648.
33. Von Heimburg D, Hemmrich K, Haydarlioglu S, Staiger H, Pallua N. Comparison of viable cell yield from excised versus aspirated adipose tissue. Cells Tissues Organs. 2004; 178: 87-92.
34. Wolter TP, Von Heimburg D, Stoffels I, Groeger A, Pallua N. Cryopreservation of mature human adipocytes: in vitro measurement of viability. Ann Plast Surg. 2005; 55: 408-413.
35. Chen FM, Zhang M, Wu ZF. Toward delivery of multiple growth factors in tissue engineering. Biomaterials. 2010; 31: 6279-6308.
36. Nurden AT, Nurden P, Sanchez M, Andia I, Anitua E. Platelets and wound healing. Front Biosci. 2008; 13: 3532-3548.
37. Keyhan SO, Hemmat S, Badri AA, Abdeshahzadeh A, Khiabani K. Use of platelet-rich fibrin and platelet-rich plasma in combination with fat graft: which is more effective during facial lipostructure? J Oral Maxillofac Surg. 2013; 71: 610-621.
38. Gentile P, De Angelis B, Pasin M, Cervelli G, Curcio CB, Floris M et al. Adipose-derived stromal vascular fraction cells and platelet-rich plasma: basic and clinical evaluation for cell-based therapies in patients with scars on the face. J Craniofac Surg. 2014; 25: 267-272.
39. Rodríguez-Flores J, Palomar-Gallego MA, Enguita-Valls AB, Rodríguez-Peralto JL, Torres J. Influence of platelet-rich plasma on the histologic characteristics of the autologous fat graft to the upper lip of rabbits. Aesthetic Plast Surg. 2011; 35: 480-486.
40. Salgarello M, Visconti G, Rusciani A. Breast fat grafting with platelet-rich plasma: a comparative clinical study and current state of the art. Plast Reconstr Surg. 2011; 127: 2176-2185.
41. Por YC, Yeow VK, Louri N, Lim TK, Kee I, Song IC. Platelet-rich plasma has no effect on increasing free fat graft survival in the nude mouse. J Plast Reconstr Aesthet Surg. 2009; 62: 1030-1034.
42. Willemsen JC, Lindenblatt N, Stevens HP. Results and long-term patient satisfaction after gluteal augmentation with platelet-rich plasma-enriched autologous fat. Eur J Plast Surg. 2013; 36: 777-782.
43. Akhundov K, Pietramaggiori G, Waselle L, Darwiche S, Guerid S, Scaletta C, et al. Development of a cost-effective method for platelet-rich plasma (PRP) preparation for topical wound healing. Ann Burns Fire Disasters. 2012; 25: 207-213.
44. Landesberg R, Roy M, Glickman RS. Quantification of growth factor levels using a simplified method of platelet-rich plasma gel preparation. J Oral Maxillofac Surg. 2000; 58: 297-300.
45. Kevy SV, Jacobson MS. Comparison of methods for point of care preparation of autologous platelet gel. J Extra Corpor Technol. 2004; 36: 28-35.
46. Marlovits S, Mousavi M, Gäbler C, Erdös J, Vécsei V. A new simplified technique for producing platelet-rich plasma: a short technical note. Eur Spine J. 2004; 13 Suppl 1: S102-106.
47. Fathi H, Fereyduni F. Treatment results of combined platelet-rich plasma and fat injection in patients with velopharyngeal insufficiency. Tehran Univ Med J 2013; 71: 445-451.