Vocabularies: Critical Software Infrastructure for
27
Vocabularies: Critical Software Infrastructure for Interoperability and Adoption American Health Information Management Association Workshop Andrew S. Kanter, MD MPH Intelligent Medical Objects, Inc. ©2005 Intelligent Medical Objects, Inc.
Transcript of Vocabularies: Critical Software Infrastructure for

Vocabularies: Critical Software Infrastructurefor Interoperability and AdoptionAmerican Health Information Management Association Workshop
Andrew S. Kanter, MD MPHIntelligent Medical Objects, Inc.
©2005Intelligent Medical Objects, Inc.

IMO©2005AHIMA 2005
Overview
Interoperability and Role of VocabulariesWhere the Money is…
The Interoperability-Adoption tug-of-warStandards—reference terminologiesUsers—interface terminologies
Mapping from Clinical to FinancialManaging the Madness

IMO©2005AHIMA 2005
Interoperability
Definition:In healthcare, interoperability is the ability of different information technology systems and software applications to communicate, to exchange data accurately, effectively, and consistently, and to use the information that has been exchanged.
NAHIT Interoperability Definition. Adapted from the IEEE definition of interoperability, and legal definitions used by the FCC (47 CFR 51.3), in statutes regarding copyright protection (17 USC 1201), and e-government services (44 USC 3601).

IMO©2005AHIMA 2005
HIEI National Net Cost-Benefit
Net return over 10 yr
implementation
Annual Net return after
implementationLevel 2 $141B $22B
Level 3 -$34B $24B
Level 4 $337B $78B
Middleton, Blackford. Deriving Value from IT: Designing for Quality and Patient Safety. www.vipcs.org/conf2004/middleton.pdf

IMO©2005AHIMA 2005 Middleton, Blackford. Deriving Value from IT: Designing for Quality and Patient Safety. www.vipcs.org/conf2004/middleton.pdf

IMO©2005AHIMA 2005
Decision-Support Examples
Interactions Meds-Meds/Nutraceut.Contraindication/Indic. Medications-ProblemsMonitoring Medications-LabsMedical Necessity Procedures-ProblemsCorrect Coding Init. Procedures-ProceduresInteractions Social Hx-Medications

IMO©2005AHIMA 2005
The Interoperability-Adoption Tug-of-War
Interoperability requires standards and limited scopeAdoption favors customization and local preferences producing broad scope

IMO©2005AHIMA 2005
The Standard Terminology Problem
Despite tremendous effort, there is no standard vocabularyDomain-specific vocabulariesICD-9-CM/CPT®/HCPCS/CDTMedications (FDB, Medi-Span™, Multum™)LOINC® for LabsUMLS (Unified Medical Language System)SNOMED® CT
IMO©2005AHIMA 2005
HIPAA-dictated Vocabulary Standards
ICD-9-CM for diseases/problemsICD-P/CPT™/HCPCS for proceduresCDT for dental proceduresNDC for medicationsDRG for inpatient hospitalizations

IMO©2005AHIMA 2005
SNOMED- Solving the Reference Problem
Began in 1965 as a Pathology Nomenclature1998 SNOMED 3.5 had 156,000 terms in 12 different modules2000 SNOMED RT w/190,000 terms and 350,000 relationships2002 SNOMED CT combines with the NHS READ codes and has >800,000 terms2004 SNOMED CT was added to UMLS2006 SNOMED CT goes global?

IMO©2005AHIMA 2005
The User Vocabulary Problem
Like politics, all health care is localDoctors have preferences, and they use them (and want to if you let them)Different doctors have different preferencesDifferent types of users require different vocabularies (doctors, patients, HIM, etc.)

IMO©2005AHIMA 2005
Interface TerminologyPHT = Personal Health Terminology™>160,000 disease/problem termsPreferred mappings from terms to ICD-9 codes (every term has a billable code) and from codes to termsDifferent mappings for coders, clinicians and patients/enrolleesMapped to SNOMED® CT, MeSH, UMLSIncludes context

IMO©2005AHIMA 2005
Capturing the Clinical Intent
Synonyms that allow docs to think like docs—not like billers…
“Transaminitis”“Athlete’s foot”“SVT (Superventricular Tachycardia)”“GERD (Gastroesophageal Reflux Disease)“Crohns”“UC (Ulcerative Colitis)”“Heart block”“Cold sore”“Pink eye”

IMO©2005AHIMA 2005
Weill/Cornell Experience
Production since 6/04Integration of clinical and financial Improved physician acceptanceMore accurate billing (ICD-9/CPT)SNOMED® CT for interoperability

IMO©2005AHIMA 2005
It is easier for me to find appropriate clinical terms.
0%
10%
20%
30%
40%
50%
Resp
onse
Per
cent
age
"Stro
ngly disa
gree"
"Disa
gree"
"Neu
tral/n
o opinion"
"Agree
""S
trongly
agree
"
Percentage
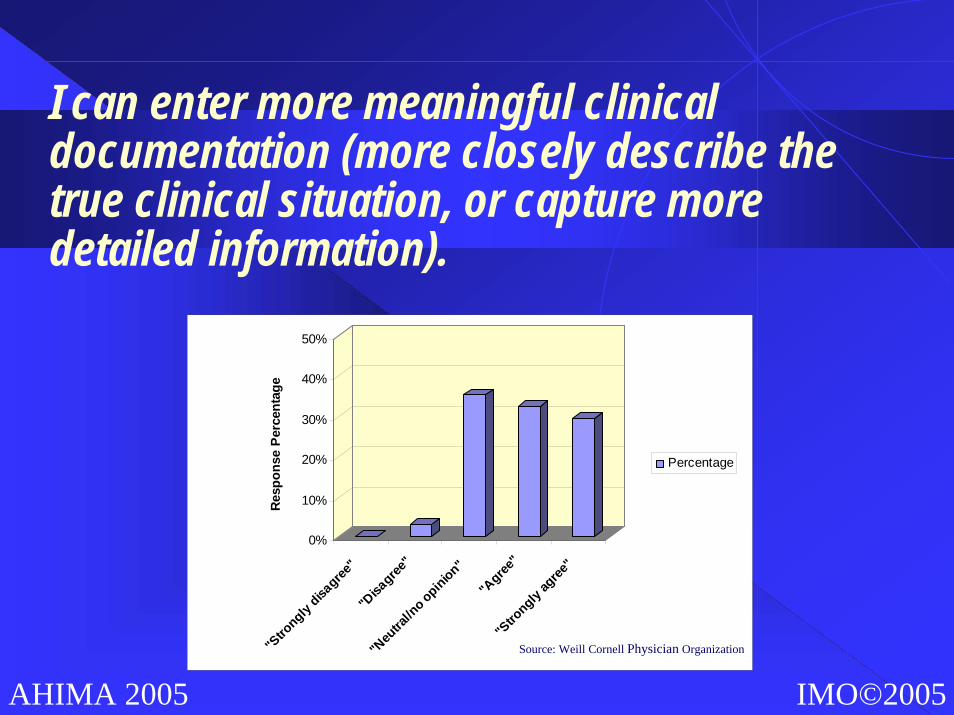
Source: Weill Cornell Physician Organization
IMO©2005AHIMA 2005
I can enter more meaningful clinical documentation (more closely describe the true clinical situation, or capture more detailed information).
0%
10%
20%
30%
40%
50%
Resp
onse
Per
cent
age
"Stro
ngly disa
gree"
"Disa
gree"
"Neu
tral/n
o opinion"
"Agree
""S
trongly
agree
"
Percentage
Source: Weill Cornell Physician Organization

IMO©2005AHIMA 2005
I spend less time searching for and/or documenting diagnoses/problems in EpicCare.
0%
10%
20%
30%
40%
50%
Res
pons
e P
erce
ntag
e
"Stro
ngly disa
gree"
"Disa
gree"
"Neu
tral/n
o opinion""A
gree"
"Stro
ngly ag
ree"
Percentage
Source: Weill Cornell Physician Organization

IMO©2005AHIMA 2005
I am more satisfied with EpicCare.
0%
10%
20%
30%
40%
50%
Resp
onse
Per
cent
age
"Stro
ngly disa
gree"
"Disa
gree"
"Neu
tral/n
o opinion"
"Agree
""S
trongly
agree
"
Percentage
Source: Weill Cornell Physician Organization

IMO©2005AHIMA 2005
Getting from Clinical to Financial
Not going to replace HIM professionalsClinical concepts do not always have all the “context” required for codingEven having more than one code per concept can be a problemRules-based systems on the horizon but harder to implement and maintainNeed oversight and validation for the maps

IMO©2005AHIMA 2005
Mapping from Clinical to Financial
Interface Terms
AmyotrophicLateral Sclerosis
ALS
Lou Gehrig’sDisease
Concept LevelTerminology
AmyotrophicLateral Sclerosis
SNOMED® CTReference
Terminology
AmyotrophicLateral Sclerosis
86044005
ICD-9-CMCoding
AmyotrophicLateral Sclerosis
335.20

IMO©2005AHIMA 2005
Mapping from Clinical to Financial
SNOMED® CTReference
Terminology
Hemiparesis
20022000
ICD-9-CMCoding
Unspecified Hemiplegiaand Hemiparesis AffectingDominant Side, LE CVA
438.21
Unspecified Hemiplegiaand Hemiparesis Affecting
Nondominant Side, LE CVA
438.22
Clinical Context:Dominant or Nots/p CVA or Not?
?

IMO©2005AHIMA 2005
Mapping from Clinical to Financial
Interface Terms
Hemiparesis due to CVA, Dominant Side
Hemiparesis AffectingDominant Side, Late Effectof CerebrovascularDisease
Concept LevelTerminology
HemiparesisAffecting
Dominant Side, Late Effect of
CerebrovascularDisease
SNOMED® CTReference
Terminology
Hemiparesis
20022000
Clinical Context:Explicit
ICD-9-CMCoding
Unspecified Hemiplegiaand Hemiparesis AffectingDominant Side, LE CVA
438.21
Unspecified Hemiplegiaand Hemiparesis Affecting
Nondominant Side, LE CVA
438.22

IMO©2005AHIMA 2005
Managing the Madness
Clinical users are not happy with administrative terms and have preferencesManaging all the dictionaries is hard workFocus on more frequent regulatory releases means more updates and more workGrace periods disappearingConsequences of failure higherOutsourcing makes sense
IMO©2005AHIMA 2005
Conclusions
Application Interoperability ROI requires both standards and flexibility in vocabulariesIt’s the data, data, data…Do not underestimate the work if you are going to take it on yourselfGet ready by having a terminology strategy now

IMO©2005AHIMA 2005
Intelligent Medical Objects, Inc.
Homepage: http://www.e-imo.comEmail: [email protected]

IMO©2005AHIMA 2005
Business Intelligence

Clinical Vocabulary Mapping Methods Institute Saturday, October 15, 2005