Vivian W.S. Chan, HBSc; Lisa Manuel, HBSc, BASc;...
21
Knowledge Users: Women’s Health in Women’s Hands Funding: CUHI seed grant, Faculty of Community Services Ryerson University 1 Vivian W.S. Chan, HBSc; 1,2 Lisa Manuel, HBSc, BASc; 3 Souraya Sidani, PhD, RN; 2,3 Enza Gucciardi, PhD 1 University of Toronto, 2 Ryerson University, School of Nutrition, 3 Ryerson University, School of Nursing
-
Upload
nguyenthuy -
Category
Documents
-
view
218 -
download
0
Transcript of Vivian W.S. Chan, HBSc; Lisa Manuel, HBSc, BASc;...
Knowledge Users: Women’s Health in Women’s HandsFunding: CUHI seed grant, Faculty of Community Services Ryerson
University
1Vivian W.S. Chan, HBSc; 1,2Lisa Manuel, HBSc, BASc;
3Souraya Sidani, PhD, RN; 2,3
Enza Gucciardi, PhD 1University of Toronto, 2Ryerson University, School of Nutrition, 3Ryerson University, School of Nursing
Background
Higher rates of diabetes among ethnic minority populations
Black African, Black Caribbean, Hispanic, Latin American, South Asian (Harris et al., 1998; King et al., 1998; Creatore et al., 2010)
Women at greater risk for diabetes complications
Cardiovascular disease, coronary heart disease, stroke, and depressive symptoms (Barrett-Connor, et al., 2004; Huxley, et al., 2006; Tuomilehto, et al., 2001; Gucciardi et al., 2008)
Accessible self-management education is essential for ethnic minorities
People from these cultural groups report poorer glycemic control and limited access to diabetes self-management resources and support (Harris et al., 1999;Karter et al., 2000)
Self-management
Diabetes self-management is critical to preventing further complications
Effective self-management is challenging and complex
Requires a lifelong commitment to lifestyle changes involving adherence to medications, nutrition management, regular self-blood glucose monitoring, and a physically active lifestyle
To improve the delivery of diabetes education, we need to identify and deliver education that works best for them
Study Aim Objective:
To identify effective diabetes self-management education (DSME) components for women of African Caribbean/American, Latin American, and South Asian descent
Research question:
What intervention features are most effective in achieving success in HbA1c, anthropometrics, physical activity, and diet outcomes?
Methodology
Literature search
Keywords for Online Databases: adult, type 2 diabetes mellitus, patient care management, patient education, patient-centered care, ethnic groups, and competency-based education
Key Inclusion Criteria: >70% women with type 2 diabetes (or gender-specific results) from cultural populations of interest, primary intervention studies
with comparison groups
9019 abstracts retrieved, 14 studies included
Methodology (Cont’d)
Quality assessment tool (Hawker, 2002; Effective Public Health Practice Project, 1998)
Looking for clarity, appropriateness, biases in entire article, including study aims, study design, methodology, analyses, and results
Scoring:
Percentage allocated based on the presence of these components in the articles
1 article received a rating of “fair”
and 13 were rated as “good”
Data Analysis
A success analysis was used in place of a meta-analysis (Glazier et al., 2006)
Research interventions were analyzed based on its success of a significant outcome (P-value ≤
0.05)
between the intervention and control groups
Only data measured after the intervention was used in the success calculation
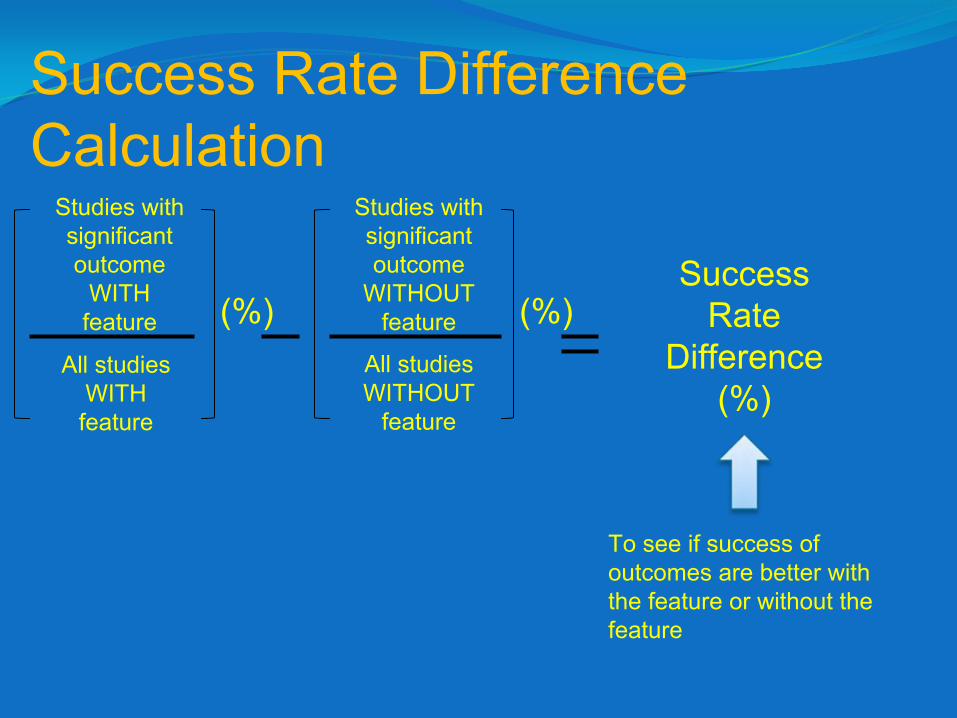
Success Rate Difference Calculation
Success Rate
Difference(%)
To see if success of outcomes are better with the feature or without the feature
Studies with significant outcome
WITH feature
All studies WITH feature
Studies with significant outcome
WITHOUT feature
All studies WITHOUT
feature
(%) (%)
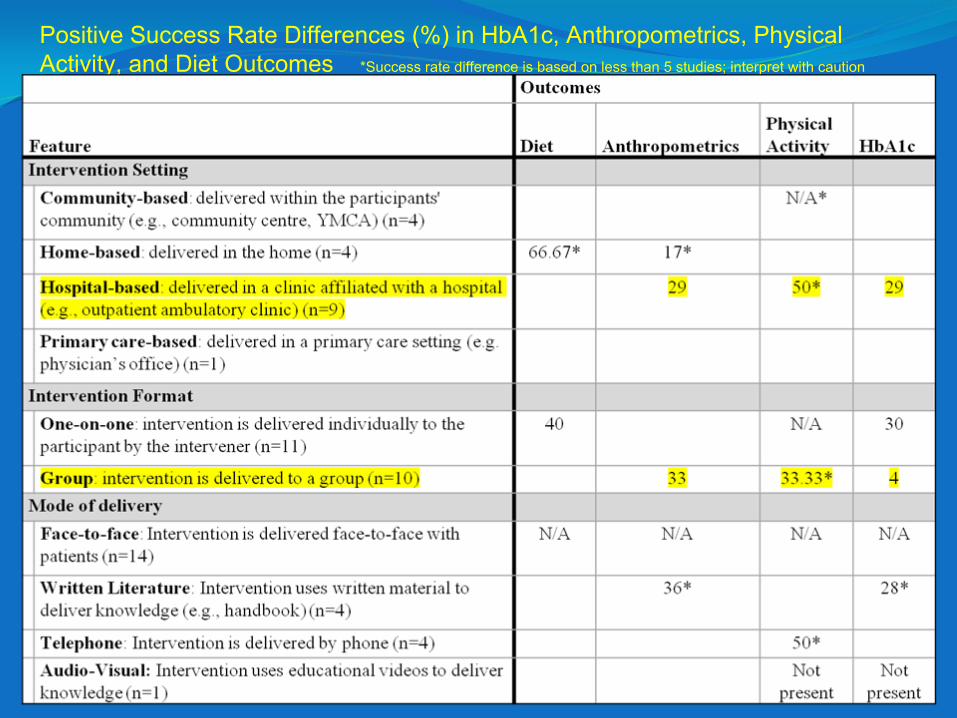
Positive Success Rate Differences (%) in HbA1c, Anthropometrics,
Physical Activity, and Diet Outcomes *Success rate difference is based on less than 5 studies; interpret with caution
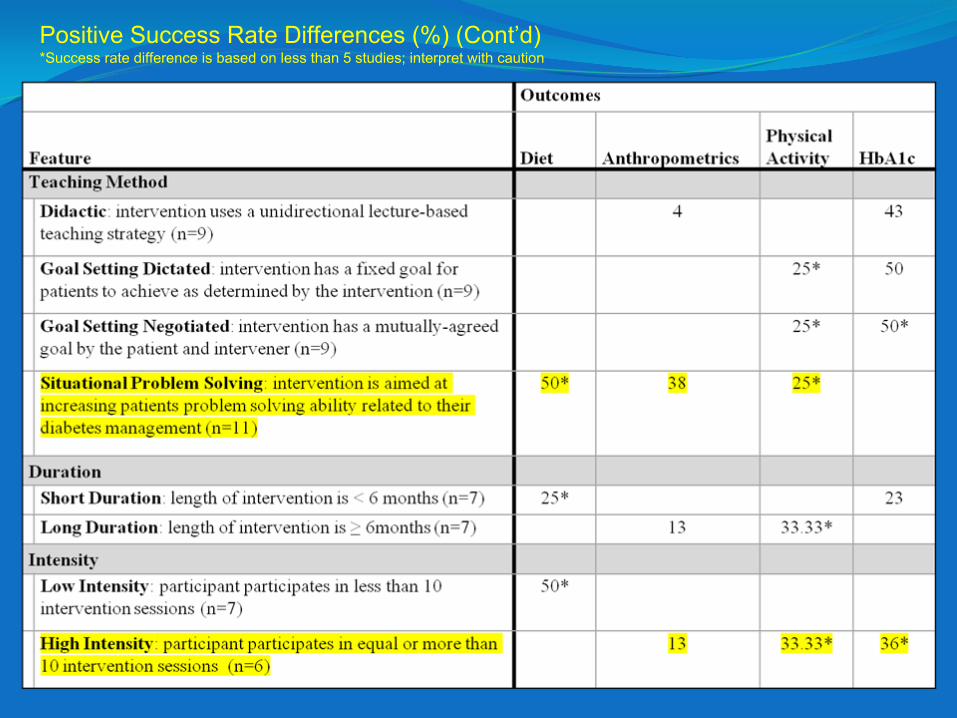
Positive Success Rate Differences (%) (Cont’d) *Success rate difference is based on less than 5 studies; interpret with caution
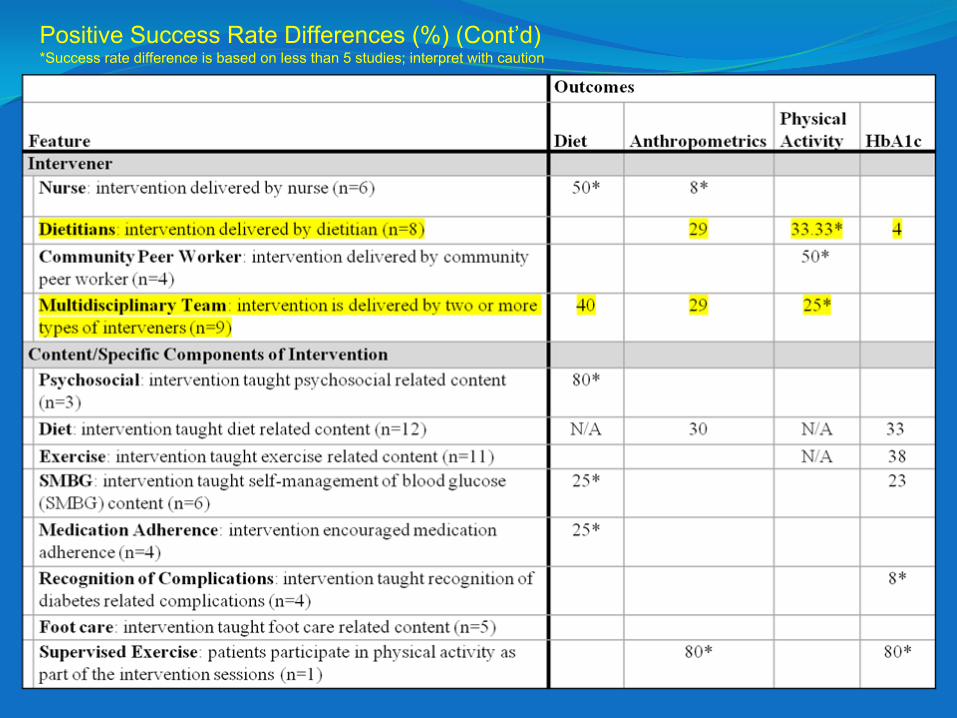
Positive Success Rate Differences (%) (Cont’d) *Success rate difference is based on less than 5 studies; interpret with caution
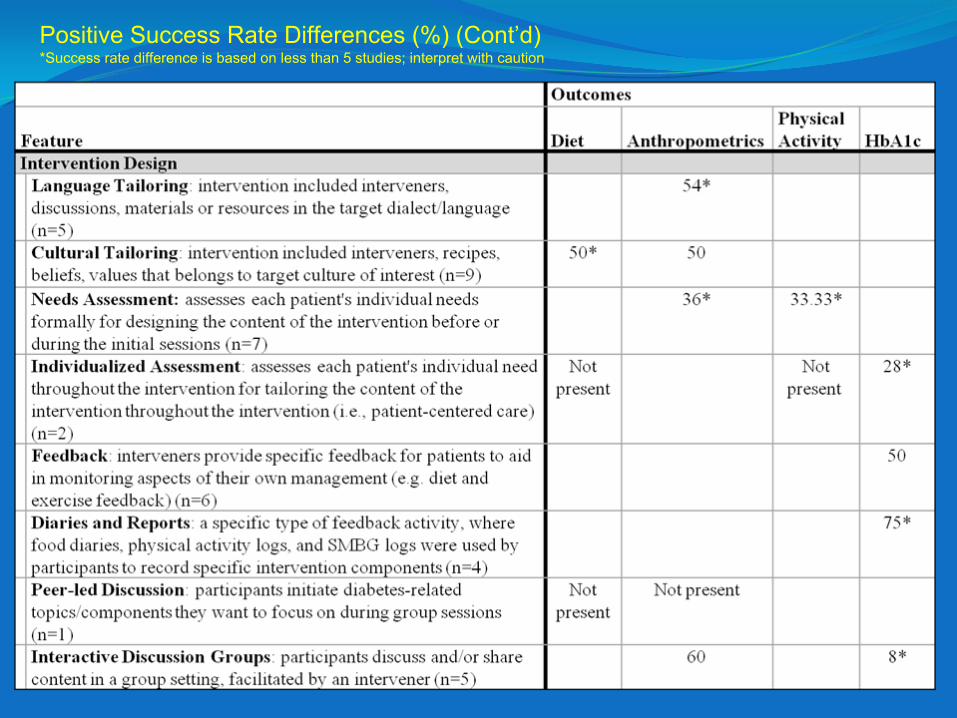
Positive Success Rate Differences (%) (Cont’d) *Success rate difference is based on less than 5 studies; interpret with caution
Recurring Trends Across Three Outcomes
HbA1c, Anthropometrics, and Physical Activity:
Hospital-based intervention setting
Group intervention format
Highly intense intervention (equal or more than 10 sessions)
Incorporating dietitians as an intervener
Recurring Trends Across Three Outcomes
Anthropometrics, Physical Activity, and Diet:
Situational problem solving teaching method
Incorporating multidisciplinary team as interveners
Physiological Outcomes
For HbA1c and Anthropometrics:
Written literature as a mode of delivery
Didactic teaching method
Diet content taught in intervention
Supervised exercise in intervention
Interactive discussion groups in intervention
Behavioural Outcomes
For Physical Activity and Diet:
Negotiated goal setting teaching method
Particular features of interest
Community peer workers and physical activity
Psychosocial content and diet
Limitations
Limited number of studies are included in this literature review due to our inclusion criteria
Only American data; No Canadian data
Not enough studies to do a stratified analysis of success rates between cultures
No South Asian intervention research met our inclusion criteria
Discussion
The recurring successful features across the outcomes may be the future focus for DSME intervention designs
To what extent should programs be flexible? Should we be individualizing or mainstreaming interventions based on specific features?

Agurs-Collins, T.D., Kumanyika, S.K., Ten Have, T.R., & Adams-Campell L.L. (1997(. A randomized controlled trial of weight reduction and exercise for diabetes management in older African-American subjects. Diabetes Care, 20(10), 1503-1511.
Anderson, R.M., Funnell, M.M., Arnold, M.S., Barr, P.A., Edwards, G.J., & Fitzgerald, J.T. (2000). Assessing the cultural relevance of an education program urban African Americans with diabetes. Diabetes Educator, 26(2), 280-
289.
Anderson-Loftin, W., Barnett, S., Bunn, P., Sullivan, P., Hussey, J., & Tavakoli, A. (2005). Soul food light: Culturally competent diabetes education. Diabetes Educator, 31(4), 555-563.
Barrett-Connor, E., Giardina, E.G., Gitt, A.K., Gudat, U., Steinberg, H.O., & Tschoepe, D. (2004). Women and heart disease: the role of diabetes and hyperglycemia. Arch Intern Med, 164(9), 934-42.
Brown, S.A., Blozis, S.A., Kouzekanani, K., Garcia, A.A., Winchell, M., & Hanis, C.L. (2005). Dosage effects of diabetes self-management education for Mexican-Americans. Diabetes Care, 28(3), 527-532.
Corkery, E., Palmer, C., Foley, M.E., Schechter, C.B., Frisher, L., & Roman, S.H. (1997). Effect of a bicultural community health worker on completion of diabetes education in a Hispanic population. Diabetes Care, 20(3), 254-257.
Creatore, M.I., Moineddin, R., Booth, G., Manuel, D.H., DesMeules, M., McDermott, S., & Glazier, R.H. (2010). Age-
and sex-
related prevalence of diabetes mellitus among immigrants to Ontario, Canada. Canadian Medical Association Journal, 1-9.
Effective Public Health Practice Project. (1998). Quality Assessment Tool For Quantitative Studies. Retrieved November 2009 from
http://www.ephpp.ca/index.html. Corresponding article of interest: Thomas, B.H., Ciliska, D., Dobbins, M., & Micucci, S. (2004). A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews on Evidence-Based Nursing, 1(3), 176-184.
Elshaw, E.B., Young, E.A., Saunders, M., Mcgurn, W.C., & Lopez, L.C. (1994). Utilizing a 24-hour dietary recall and culturally specific diabetes education in Mexican Americans with diabetes. Diabetes Educator, 20(3), 228-235.
Gary, T.L., Bone, L.R., Hill, M.N., Levine, D.M., McGuire, M., Saudek, C., & Brancati, F.L. (2003). Randomized controlled trial of the effects of nurse case manager and community health worker interventions on risk factors for diabetes-related complications in urban African Americans. Preventive Medicine, 37, 23-32.
Glazier, R.H., Kennie, N.R., Bajcar, J., & Willson, K. (2006). A
systematic review of interventions to improve diabetes care in socially disadvantaged populations. Diabetes Care, 29(7), 1675-1688.
Gucciardi, E., Wang ,S.C., DeMelo, M., Amaral, L., & Stewart, D.E.. (2008). Characteristics of men and women with diabetes: observations during patients' initial visit to a diabetes education centre. Can Fam Physician, 54(2):219-27.
Harris, M.I., Eastman, R.C., Cowie, C.C., Flegal, K.M., & Eberhardt, M.S. (1999). Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care, 22(3), 403-408.
Harris, M.I., Flegal, K.M., Cowie, C.C., Eberhardt, M.S., Goldstein, D.E., Little, R.R., et al. (1998). Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988-1994. Diabetes Care, 21(4), 518-524.
Hawker S., Payne, S., Kerr C., Hardey, M., & Powell, J. (2002). Appraising the Evidence: Reviewing Disparate Data Systematically. Qualitative Health Research, 12, 1284-
1299.
Huxley, R., Barzi, F., & Woodward ,M. (2006). Excess risk of fatal coronary heart disease associated with diabetes in men and women: meta-analysis of 37 prospective cohort studies. BMJ, 332(7533):73-8.
Jaber, L.A., Halapy, H., Fernet, M., Tummalapalli, S., & Diwakaran, H. (1996). Evaluation of a pharmaceutical care model on diabetes management. Annals of Pharmacotherapy, 30(3), 238-243.
Karter A.J., Ferrara A., Darbinian J.A., Ackerson L.M., Selby J.V. (2000). Self-monitoring of blood glucose: language and financial barriers in a managed care population with diabetes. Diabetes Care, 23(4), 477-83.
Keyserling, T.C., Samuel-Hodge, C.D., Ammerman, A.S., Ainsowrth, B.E., Heriques-Roldan, C.F., Elasy, T.A., Skelly, A.H., Johnston, L.F., & Bangdiwala, S.I. (2002). A romandized trial of an intervention improve self-care behaviors of African-American women with type 2 diabetes. Diabetes Care, 25(9), 1576-1583.
King, H., Aubert, R.E., & Herman, W.H. (1998). Global burden of diabetes, 1995-2025: prevalence, numerical estimates, and projections. Diabetes Care, 21(9), 1414-1431.
Mayer-Davis, E.J., D’Antonio A.M., Smith, S.M., Kirkner, G., Martin, S.L., Parra-Medina, D., & Schultz, R. (2004). Pounds off with empowerment (POWER): A clinical trial of weight management strategies for black and white adults with diabetes who live in medically underserved rural communities. American Journal of Public Health, 94(10), 1736-1742.
McNabb, W.L., Quinn, M.T., & Rosing, L. (1993). Weight loss program for inner-city black women with non-insulin-dependent diabetes mellitus: PATHWAYS. Journal of American Dietetic Association, 73(1), 75-77.
Skelly, A.H., Carlson, J., Leeman, J., Holditch-Davis, D., & Soward, A. (2005). Symptom-focused management for African American women with type 2 diabetes: A pilot study. Applied Nursing Research, 18(4), 213-220.
Smith, D.E., Heckenmeyer, C.M., Kratt, P.P., & Mason, D.A. (1997). Motivational interviewing to improve adherence to a behavioral weight-control program for older obese women with NIDDM: A pilot study. Diabetes Care, 20(1), 52-4.
Sohal, P.S. (2008). Prevention and management of diabetes in South Asians. Canadian Journal of Diabetes, 32(3), 206-210.
Tuomilehto ,J., Lindstrom, J., Eriksson, J.G., Valle, T.T., Hamalainen, H., Ilanne-Parikka, P., et al. (2001). Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance 25. N Engl J Med , 344(18):1343-50.
West, D.S., DiLillo, V., Bursac, Z., Gore, S.A., Greene, P.G. (2007). Motivational interviewing improves weight loss in women with type 2 diabetes. Diabetes Care, 30(5), 1081-1087.