Viva Voce for Normal Pregnancy
40
Viva voce for normal pregnancy case H.NEHA FINAL YR MBBS Roll 57 Under the guidance of Prof.Dr.M.S.Vishwan athan
-
Upload
jeyakumar-meyyappan -
Category
Documents
-
view
61 -
download
2
description
just a rapid review of normal pregnancy
Transcript of Viva Voce for Normal Pregnancy

Viva voce for normal pregnancy case
H.NEHAFINAL YR MBBS
Roll 57
Under the guidance of Prof.Dr.M.S.Vishwanathan

GOOOOD MORNING

OBJECTIVESHISTORY TAKING
EXAMINATION
IMMUNISATION

HISTORY TAKING

What is the importance of age in pregnancy?
Teenage and >35yrs preg have adverse outcomes
Problems with teenage:› Medical problems: Anemia,malnutrition,pre-
eclampsia› Obetetric problems:fetal
malpresentation,CPD,preterm delivery Problems with pts >35 yrs:
› Fetal : chromosomal abnormalities- downs syndrome,IUGR,malposition,postdated
› Maternal : obesity,PIH,GDM,prolonged labour,lactational failure


When is patient said to be a booked case according to RCH programme?
•1st:20 wks or as soon as she becomes pregnant
•2nd:32 wks or once in 2nd trimester
•3rd:36 wks or once in last trimester
Atleast 3 ANC:
NOTE: A registered pt is not the same as booked case. Registration is done with ANM in a subcentre.

Number of ANC visits ideally?
Once every 4 wks in 1st trimesterOnce every 2 wks in 2nd trimesterOnce every week in 3rd trimester

What does gravity and parity denote?
Gravida: denotes a past/present pregnancy irrespective of gestational age and outcome
Parity: denotes a previous pregnancy beyond the period of viability(>28 wks) irrespective of the outcome

Who is grandmultipara and what are the problems associated with it?
Grand multipara:Birth to atleast 4 viable children Associated prob:
› Malpresentation due to pendulous abdomen› Pronounced lordosis:increases pelvic inclination and
non engagement of fetal head at term› Medical probs: anemia,PIH,GDM› Multiple pregnancy › Placenta previa › Osteomalacic changes leading to contracted pelvis
due to calcium deficiency› Ruptured uterus› PPH

Are EDD and gestational age synonymous? Justify your answer
No it is not synonymous
EDD- depends on last menstrual period
Gestational age-depends on the conception date

What is EDD,conception date,gestational age, menstrual age
EDD: expected date of delivery is the date estimated based on LMP to approx know the due date of birth. It is calculated using
naegele’s formula and modified
naegele’s formula
Conception date: it is the date
when the egg is fertilised. In
normal cycle it is two wks later than the LMP.
Gestational age: “amount of time
the baby is actually
developing” so it is counted from two weeks after
the LMP
Menstrual age: number of
weeks passed from the 1st day
of LMP

How is EDD calculated?
Naegele’s formula: for regular cycles
1st day of LMP+9 mnths +7 days
Modified naegele’s: for irregular cycles
For longer cycles: add the extra days to get
EDD
Eg. Woman with 45 days
cycle and LMP-3.1.12
EDD- 3.1.12+9mnths+7days=10.
10.12 now add the extra
number of days-15 to the
EDD CORRECTED
EDD: 10.10.12+15days=25.10.12
For shorter cycles: subtract the shorter
days to get EDD
Eg. Woman with 20 days
cycle and LMP-3.1.12
EDD-3.1.12+9mnths+7days=10.
10.12 now subtract the shorter days-10 from the
EDD CORRECTED
EDD:10.10.12-10
days=30.11.12

How to determine the reliability of EDD?
Pt should not be using OCP’S
Last three periods should be regular
Clinical history,examination,USG-all correlate with the EDD

To daughters A couple made a deal the night of their Marriage to NOT open the door of
their room to anybody who comes knocking in the morning for any reason! In the morning the parents of the husband came & knocked on the door, the husband & the wife were looking at each other & as they agreed before, they didn't open the door. After a while the parents of the bride came knocking at the door to check on them, the couple were looking at each other, then the bride dropped a tear & started crying she said: "I cannot keep them knocking & not open the door, I miss them already" The husband didn't say anything & he let her open the door for her parents. Years & years passed & the couple had 5 children, the first ones were boys & the 5th was a little girl, when she was born the father was extremely happy that Almighty blessed him with her, & he threw a Huge Party for her in Grand style, people were so amazed with his joy & his happiness that they asked him, why are you so happy with her more than you were before with her elder brothers? He answered simply: "She is the one who will open the door for me" Baby girls are the comfort of the eyes of their father! They hold the key to their mothers hearts! Daughters are really unique. They care for their parents even after they are married

. Its rightly said, "A son is a son till he gets a Wife, a daughter is a daughter all her Life!"

What is the importance of fever with rash in first trimester?
The most worried viral infection is RUBELLA› C/F:
Mild febrile illness Generalised maculopapular rash Arthralgias Arthritis Lymphadenopathy(suboccipital,postauricular,cer
vical) Conjuncitivitis
› May lead to congenital rubella syndrome › Incubation period: 12 to 23 days

What is the significance of UTI in pregnancy?
May lead to:
•Preterm delivery•LBW babies•Pre-eclampsia•Anemia

What is quickening?when does it occur for primi and multi?
It is the perception of fetal movements by pregnant woman
Primi:18-20 wks Multi:2 wks earlier than primi

Recommendation of IFA?
60 mg of elemental iron and 500 mcg of folic acid for 100 days starting in the second half of pregnancy
Folic acid 500 mcg to be started pre-conceptionaly

In women with previously affected children(neural tube defects) what is the dose of folic acid?
4 mg/day

What is the normal weight gain in singleton pregnancy?
It depends on BMI of the ptBMI (pre-pregnancy)
Recommended weight gain(kg)
Low <19.8 12.5-18
Normal 19.8-26 11.5-16
High 26-29 7-11.5
Obese >29 7
Wt gain for twins is 16 -20 kg


How much spacing is required between pregnancies?
Minimum of three years to replenish iron stores of 1000mg

Diet and rest recommendation in normal pregnant woman?
Diet:
Pregnancy-extra 300kcal/day and
10 gm/day protein
Lactation-extra 600 kcal/day and
20 gm/day protein
Rest: 10 hours/day(8 hrs in night and 2 hrs in noon)

EXAMINATION

Leopolds maneuvre??Leopold’s maneuvers
#1 – Correct dextrorotation of the uterus with the back of one hand
and delineate the fundus
with the other to determine gestational age and/or appropriate
size.
#2 – Run hands down
maternal abdomen on either side of
fetus to determine fetal lie,
identifying small parts and fetal
spine
#3 – Firmly grasp upper and lower
poles of fetus by placing fingers at
uterine fundus and above
symphysis to determine
presentation and fetal size.
#4 – Move hands in
bilaterally from anterior superior iliac
crests to determine
whether or not the presenting
part of the fetus is
engaged in maternal pelvis.
Head regarded as unengaged if
examiner’s hands are see to
converge below fetal head.


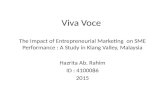
What is Partogram? the partogram is a graphical
representation of the changes that occur in labour, including cervical dilatation, fetal heart rate, maternal pulse,blood pressure, and temperature; it also shows a numerical record of features such as urine output and the volume and type of intravenous infusions (including oxytocin drips) .
So it helps to identify deviations from normal in any of these variables.

Records of the findings at successive vaginal examination (should be done every 4 hours) are plotted on a graph , showing the dilatation of the cervix in cm against time in hours .
Friedman who introduced the idea of partogram had described two phases of labour :-
1- latent phase : from the onset of labour until the cervix 3 cm dilated which may last 3 to 7 hours in a primigravida .
2- active phase : during which the dilatation from 3 to 10 cm (1cm/h), so the slope of partogram curve will be steeper in this phase .

Latent (a) and active (b) phase of labour in a multiparous and a primiparous woman, as shown on partogram

Monitoring for fetal well-being

What is the abdominal girth at term?
90-100 cms


IMMUNIZATION

When should TT be given?
1st dose- as early as possible
2nd dose- one month after the
first dose
Booster dose only if previously
vaccinated within 3 yrs

How is Rh-isoimmunization given?
1st dose: anti-D
immunoglobulin
prophylactically to
all D-negative mother
at 28 wks
2nd dose: after
delivery within
72 hours if
the infant id D-
positive
NOTE: 2nd dose is given cause
the half life of
immmunoglobulin is 24 hrs and
it persists
for 6 wks

What do you mean by neonatal(NNT)high risk,control,elimination areas
NNT high risk areas:• Incidence: <1/1000• TT 2nd dose
coverage:<70%• Attended
deliveries:<50%
NNT control areas:• Incidence:
>1/1000• TT 2nd dose
coverage:70%-89%
• Attended deliveries:50%-74%
NNT elimination areas:• Incidence:<0.1/1
000• TT 2nd dose
coverage:>90%• Attended
deliveries:>75%

When is rubella vaccine given during pregnancy?
It is not given during pregnancy
•MMR should be given in childhood itself.if not immunised it is given atleast 3 mnths prior to conception
•MMR not given in pregnency cause it is live attenuated vaccine