Vitamin D in Fetal Development: Findings From a Birth Cohort Study · 2020-02-09 · Kun Zhu,...
10
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/269714719 Vitamin D in Fetal Development: Findings From a Birth Cohort Study Article in Pediatrics · December 2014 DOI: 10.1542/peds.2014-1860 · Source: PubMed CITATIONS 55 READS 173 10 authors, including: Some of the authors of this publication are also working on these related projects: Assessing climate resilience of health systems View project Predicting language outcomes View project Prue H Hart University of Western Australia 256 PUBLICATIONS 8,203 CITATIONS SEE PROFILE Robyn Lucas Australian National University 227 PUBLICATIONS 4,705 CITATIONS SEE PROFILE Andrew J O Whitehouse University of Western Australia 209 PUBLICATIONS 4,875 CITATIONS SEE PROFILE Kun Zhu Sir Charles Gairdner Hospital 160 PUBLICATIONS 3,851 CITATIONS SEE PROFILE All content following this page was uploaded by Prue H Hart on 23 December 2014. The user has requested enhancement of the downloaded file.
Transcript of Vitamin D in Fetal Development: Findings From a Birth Cohort Study · 2020-02-09 · Kun Zhu,...

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/269714719
Vitamin D in Fetal Development: Findings From a Birth Cohort Study
Article in Pediatrics · December 2014
DOI: 10.1542/peds.2014-1860 · Source: PubMed
CITATIONS
55READS
173
10 authors, including:
Some of the authors of this publication are also working on these related projects:
Assessing climate resilience of health systems View project
Predicting language outcomes View project
Prue H Hart
University of Western Australia
256 PUBLICATIONS 8,203 CITATIONS
SEE PROFILE
Robyn Lucas
Australian National University
227 PUBLICATIONS 4,705 CITATIONS
SEE PROFILE
Andrew J O Whitehouse
University of Western Australia
209 PUBLICATIONS 4,875 CITATIONS
SEE PROFILE
Kun Zhu
Sir Charles Gairdner Hospital
160 PUBLICATIONS 3,851 CITATIONS
SEE PROFILE
All content following this page was uploaded by Prue H Hart on 23 December 2014.
The user has requested enhancement of the downloaded file.

Vitamin D in Fetal Development:Findings From a Birth Cohort StudyPrue H. Hart, PhDa, Robyn M. Lucas, MBChBa,b, John P. Walsh, MBBSc,d, Graeme R. Zosky, PhDa,e, Andrew J.O. Whitehouse, PhDa,Kun Zhu, PhDc,d, Karina L. Allen, PhDa,f, Merci M. Kusel, MBBSa, Denise Anderson, MBiostata, Jenny A. Mountain, MBAa
abstractBirth cohort studies provide an invaluable resource for studies of the influenceof the fetal environment on health in later life. It is uncertain to what extentmaternal vitamin D status influences fetal development. Using an unselectedcommunity-based cohort of 901 mother-offspring pairs (the Western AustralianPregnancy Cohort [Raine] Study), we examined the relationship betweenmaternal vitamin D deficiency at 18 weeks’ pregnancy and long-term healthoutcomes of offspring who were born in Perth, Western Australia (32° South),in 1989–1991. Vitamin D deficiency (serum 25-hydroxyvitamin D [25(OH)D],50 nmol/L) was present in 36% (323 of 901) of the pregnant women. Afteradjusting for relevant covariates, maternal vitamin D deficiency duringpregnancy was associated with impaired lung development in 6-year-oldoffspring, neurocognitive difficulties at age 10, increased risk of eating disordersin adolescence, and lower peak bone mass at 20 years. In summary, vitamin Dmay have an important, multifaceted role in the development of fetal lungs,brain, and bone. Experimental animal studies support an active contribution ofvitamin D to organ development. Randomized controlled trials of vitamin Dsupplementation in pregnant women with long-term follow-up of offspring areurgently required to examine whether the correction of vitamin D deficiency inpregnant women is beneficial for their offspring and to determine the optimallevel of maternal serum 25(OH)D for fetal development.
The concept that health and disease inlater life are partly determined in uterowas first introduced by Barker in the1980s when he showed that low birthweight babies are at greater risk ofdeveloping coronary heart disease laterin life.1 The developmental origins ofhealth and disease hypothesis suggeststhat the early environment inpregnancy can determine structural,metabolic, physiologic, and behavioraldevelopment and modify responsepatterns that influence future diseasesusceptibility.2 The evidence forpreprogramming of disease duringfetal life is being explored through theestablishment of cohort studies thatrecruit and study pregnant women andthen monitor their offspring duringchildhood, adolescence, and intoadulthood.
Our studies have concentrated onserum 25-hydroxyvitamin D levels(25(OH)D) during pregnancy as ameasure of vitamin D adequacy and thelong-term implications for the health ofthe offspring. Many reviews supporta need for vitamin D sufficiency inpregnancy but have concentrated onthe benefits associated with reducingadverse pregnancy and birthoutcomes such as gestational diabetes,preeclampsia, bacterial vaginosis, andsmall-for-gestational-age infants.3 Weaddress longer term benefits of vitaminD sufficiency during pregnancy. Wesummarize the outcomes of ourlongitudinal analyses of children bornto women with various levels of serum25(OH)D measured when they were 18weeks pregnant. In accordance withthe guidelines of the Institute of
aTelethon Kids Institute, dSchool of Medicine andPharmacology, and fSchool of Psychology, University ofWestern Australia, Perth, Australia; bCollege of Medicine,Biology and Environment, Australian National University,Canberra, Australia; cDepartment of Endocrinology andDiabetes, Sir Charles Gairdner Hospital, Nedlands,Australia; and eSchool of Medicine, Faculty of Health,University of Tasmania, Hobart, Australia
Dr Hart conceptualized and designed the study,coordinated maternal 25(OH)D measures anddrafted the initial manuscript; Drs Whitehouseand Kusel conceptualized and designed the studyand coordinated maternal 25(OH)D measures; DrLucas and Ms Anderson analyzed ultravioletradiation data; Drs Walsh, Zosky, Whitehouse, Zhu,and Allen lead analyses of maternal vitamin D levelsand their associations with child and adolescenthealth measures; Ms Mountain manages the RaineStudy; and all authors contributed to the writing ofthe report and approved the final manuscript assubmitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1860
DOI: 10.1542/peds.2014-1860
Accepted for publication Oct 2, 2014
Address correspondence to Dr Prue H. Hart,Telethon Kids Institute, University of WesternAustralia, PO Box 855, West Perth 6872, Australia.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2015 by the American Academy ofPediatrics
FINANCIAL DISCLOSURE: The authors have indicatedthey have no financial relationships relevant to thisarticle to disclose.
FUNDING: Raine Study core management fundinghas been provided by the University of WesternAustralia, Telethon Kids Institute, Raine MedicalResearch Foundation, UWA Faculty of Medicine,Dentistry and Health Sciences, Women’s and Infant’sResearch Foundation, Curtin University and EdithCowan University.
POTENTIAL CONFLICT OF INTEREST: The authors haveindicated they have no potential conflicts of interestto disclose.
PEDIATRICS Volume 135, number 1, January 2015 SPECIAL ARTICLE at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

Medicine,4 we define vitamin Ddeficiency as serum 25(OH)D levels,50 nmol/L. We document theextensive impact that vitamin Ddeficiency in pregnancy can have onlung, brain, and bone development assubsequently measured in thechildren during childhood,adolescence, and early adulthood.
THE RAINE PROSPECTIVE BIRTHCOHORT
The Western Australian PregnancyCohort (Raine) Study is an unselected,community-based cohort.Predominantly Caucasian women(∼90%) were recruited atapproximately gestational age 18weeks and delivered their offspringbetween 1989 and 1991 in Perth,Western Australia (32°South).5 Atthis time, vitamin D supplementationin a concentrated form or in food wasrare and not specifically sought fromthe mothers. We analyzedassociations between the mother’sserum 25(OH)D levels at 18 weeks’gestation and longer term outcomesin their offspring in childhood,adolescence, and early adulthood. Ofimportance, the emphasis was onchanges that reflect organdevelopment (eg, lung capacity,language ability, peak bone mass) andthat may predispose, in some cases, toill health later in life. One hundredtwenty-one mother-offspring pairswere consistent across the 5published substudies collated here asa summative review.6–10 Studies wereapproved by the Human Researchethics committees at King EdwardMemorial Hospital, Princess MargaretHospital, and the University ofWestern Australia, Perth, Australia.
Serum 25(OH)D concentration wasmeasured by immunoassay(Immunodiagnostic Systems Ltd,Fountain Hills, AZ); a subset ofsamples was reassayed by using thereference method of isotope-dilutionliquid chromatography/tandem massspectrometry and showed strongagreement (r2 = 0.87) with no
evidence of analytical interference.7
Maternal serum 25(OH)D levels werenormally distributed. Approximately36% (323 of 901) of the pregnantwomen were vitamin D–deficient,which compares favorably with thereported prevalence of vitamin Ddeficiency in pregnancy, which rangesfrom 33% to 98% worldwide.11 Only3% of mothers (29 of 901) weredefined as severely vitamin Ddeficient, that is, 25(OH)D ,25nmol/L, and 18% (162 of 901) hadvitamin D levels .75 nmol/L.
ASSOCIATIONS OF BONE, LUNG, ANDBRAIN DEVELOPMENT WITH SERUM25(OH)D LEVELS
First, maternal vitamin D deficiencyat 18 weeks (which is an importanttime in fetal lung development)12 wasassociated with reduced lung functionin children at 6 years of age.6 In thissubstudy of 260 mother-offspringpairs, there was a significant positiveassociation between maternal serum25(OH)D levels and Z scores forforced vital capacity (FVC). Theeffects on lung measures titrated withvitamin D levels after adjusting forconfounders. Children from motherswho were vitamin D deficient had anestimated mean FVC Z score 0.10lower than children born to motherswho had levels between 50 and75 nmol/L. These children, in turn, hada mean estimated FVC Z score 0.23lower than children born to motherswith 25(OH)D levels .75 nmol/L.6
Maternal vitamin D deficiency at 18weeks also correlated with currentwheeze in 6-year-old offspring(genders combined) and an increasedrisk of asthma in boys.6 There wereno significant associations found withatopy measurements; this studysuggests that an association ofvitamin D deficiency with respiratorydisease is due to an impact on lungdevelopment.6
Second, in consideration of braindevelopment, maternal vitamin Ddeficiency at 18 weeks’ gestation wassignificantly associated with reduced
neurocognitive development in theoffspring, including languageimpairment at ages 5 and 10,7
increased risk of having an eatingdisorder in adolescence,8 and moreautistic-like behaviors in earlyadulthood.9 In the study of languageimpairment in 743 mother-offspringpairs, multivariable regressionanalyses, incorporating a range ofconfounding variables (maternal ageat conception, maternal education,family income, maternal smokingduring pregnancy, offspring parity,season of blood collection), foundthat the risk of pregnant women whohad 25(OH)D levels within the lowestquartile of the distribution(#46 nmol/L) having a child withclinically significant languagedifficulties was increased close totwofold compared with womenwithin the highest quartile of the25(OH)D distribution (.70 nmol/L).7
In a follow-up investigation, 406offspring of mothers with measured25(OH)D levels at 18 weeks’gestation completed the Autism-Spectrum Quotient, a measure ofautistic-like traits in the generalpopulation, in early adulthood.Offspring of mothers with 25(OH)Dlevels ,50 nmol/L were at increasedrisk for high scores ($2 SD above themean) on the Attention Switchingsubscale of this measure, denotingbehaviors consistent with the autismphenotype.9 Finally, eating disordersymptoms were assessed in offspringaged 14, 17, and 20 years in 526white mother-child dyads.8 Usingmultivariate logistic regressionmodels, lower maternal vitamin Dstatus was a significant predictor ofeating disorder risk in femaleoffspring. Having a serum 25(OH)Dlevel in the lowest quartile(,46 nmol/L) was associated witha twofold increase in odds for havingan eating disorder by age 20 years(95% confidence interval [CI] forodds ratio = 1.03–5.27) relative toconcentrations in the highest quartile(.71.4 nmol/L). These results wereobtained after adjusting for
e168 HART et al at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

sociodemographic characteristics,BMI, depressive symptoms, maternaleducation, and season of birth.8 Therewas a nonsignificant increased odds,and suggestion of trend, for thesecond and third 25(OH)D quartiles.
Third, with respect to development ofbone, the organ historicallyassociated with vitamin D, weexamined total bone mineral contentand bone mineral density by dualenergy x-ray absorptiometry in theadult offspring of 341 mothers.Maternal vitamin D deficiency at 18weeks’ gestation was associated withlower peak bone mass among theirchildren at 20 years of age.10
Specifically, we found a reduction of2.7% in total body bone mineralcontent and 1.7% lower total bodybone mineral density (afteraccounting for season of samplecollection and maternal and offspringfactors) compared with offspring ofvitamin D–sufficient mothers.10 Theresults are consistent with a previousbirth cohort study in which maternalvitamin D status was determined at34 weeks’ gestation and bone mineraldensity measured in the offspring at 9years of age,13 but not with a secondstudy in which maternal vitamin Dstatus was determined at variousstages of pregnancy and the offspringstudied at 9 to 10 years of age.14 Wechose to measure bone mineraldensity in the offspring at 20 years ofage because this represents a time ofskeletal maturity, when the influenceof growth-related confounders isleast.15 Achievement of optimal peakbone mass is considered the bestprotection against age-related boneloss.15 From our results, it isbiologically plausible that maternalvitamin D deficiency in pregnantwomen may influence fracture risk oftheir offspring decades later.
The outcomes in the describedstudies are summarized in Table 1.An analysis of the maternal serum25(OH)D levels of the substudies incomparison with the total cohort forwhom maternal serum 25(OH)D
levels were measured showedsignificantly higher mean 25(OH)Dlevels for participants in the lungfunction studies (60.2 nmol/L, 95%CI 58.0–62.5) and those for languagedevelopment (59.5 nmol/L, 95% CI58.1–60.8) than for the total cohort(57.9 nmol/L). Because this meanmeasure for all mothers for whom25(OH)D was measured was close toinclusion in the 95% CI for levelsmeasured in the substudies, weconcluded that any bias in thosestudied in the substudies was minor.
STUDIES IN EXPERIMENTAL ANIMALS
Is a physiologic role for vitamin D inthe development of fetal lung, brain,and bone biologically plausible?Animal studies suggest that it is andsupport an active involvement byvitamin D in organ development inutero. Studies from our laboratorydetected deficits in lung function andaltered lung structure in 2-week-oldprogeny from vitamin D–deficientfemale mice.16 Vitamin D–deficientrats deliver babies with altered brainstructures consistent with increasedrisk of schizophrenia development.17
Finally, although some animal studieshave suggested that themineralization of the fetal skeleton isindependent of vitamin D,18 othershave observed skeletal mineralizationdefects in fetuses born from vitaminD–deficient or vitamin D receptor–null mothers on normal calciumdiets.19 The caveat is that if theintervention was dietary or micewithout vitamin D receptors wereused, vitamin D deficiency in theanimals was extreme, causing theanimals to be highly (or totally)vitamin D deficient. Nonetheless,
these studies give some support tovitamin D as an important mediatorof optimal lung, brain, and bonedevelopment.
IS VITAMIN D OR EXPOSURE TO UVRADIATION RESPONSIBLE FOR THEOBSERVED ASSOCIATIONS?
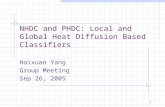
In humans, circulating vitamin D ismainly derived from synthesis in theskin, under the influence of sunlight(specifically shorter wavelength UVradiation), so it remains possible thatsunlight-induced molecules in skin,other than vitamin D, may beresponsible for, or contribute to, thebiological effects observed (eg, nitricoxide, cis-urocanic acid).20 To explorethis, we investigated the relationshipbetween the measured serum 25(OH)Dlevels and the erythemal UVexposure detected at that time in Perth(32°S, 116°E). For erythemal UVexposure, the estimated peak UV levelwas on December 30, and the lowpoint was June 30 (Fig 1A). Formaternal 25(OH)D levels, theestimated peak of the modeled annualdistribution was on February 11 andthe low point on August 13, that is,43 days after the estimated peak ornadir in UV level (Fig 1B). We used thistime lag to measure the correlationbetween erythemal UV exposures andmaternal serum 25(OH)D levels andfound a significant association (r = 0.33;95% CI = 0.27–0.39; P , .0001;Fig 1C). Serum 25(OH) levels couldtherefore provide a measure of theproduction of other moleculesproduced in skin upon sun exposure.Interestingly, in a previous birthcohort study, measures of erythemalUV exposures received by pregnantwomen during the third trimester of
TABLE 1 Summary of the Associations of Organ Development of the Offspring With MaternalSerum 25(OH)D Levels From 5 Separate Studies (N = 901)
Organ Measure Age at Measure n Association
Lung Z scores6 FVC 6 y 260 PositiveBrain Language scores7 5, 10 y 743 Positive
Eating disorder risk8 14, 17, 20 y 526 NegativeAutism-Spectrum Quotient9 Early adulthood 406 Negative
Bone Peak bone mass10 20 y 341 Positive
PEDIATRICS Volume 135, number 1, January 2015 e169 at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

FIGURE 1Square root of the erythemal UV exposure (A) and serum 25(OH)D levels (B) for 871 pregnant women at 18 weeks’ gestation, plotted against the date of blooddraw. Erythemal UV radiation in Perth (32° south, 116° east) was estimated from data from the Total Ozone Mapping Spectrometer aboard the Nimbus-7 satellite(http://iridl.ldeo.colombia.edu/SOURCES/.NASA/.GSFC/.TOMS). For panels A and B, cosinor models in R 3.0.1 showed significant seasonal components (sine andcosine term P values,.025) and are indicated by the solid line. The estimated peak location for erythemal UV exposure was on December 30, which was 43 daysbefore the estimated peak location of serum 25(OH)D levels. In C, erythemal UV exposures 43 days before blood draw significantly correlated with maternal serum25(OH)D levels (r = 0.33; 95% CI 0.27–0.39; P , 0.001). The shading is the 95% confidence region of the fitted linear regression line.
e170 HART et al at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

pregnancy were positively correlatedwith measures of bone mineralcontent, bone area, and area-adjustedbone mineral density in the offspringat 9 to 10 years of age,21 whereasmaternal serum 25(OH)D levels werenot.14 With respect to development ofautoimmune diseases, outcomesattributed to UV-induced vitamin Dmay in fact reflect the actions of otherimmunoregulatory moleculesproduced in skin during exposure toUV irradiation.20
VITAMIN D IN FETAL DEVELOPMENT: ANACTIVE PLAYER OR APPARENT EFFECTSDUE TO CONFOUNDING?
Our observational studies suggest,but do not prove, that vitamin D playsan active role in fetal lung, brain, andbone development. The possibilityremains that the reduced lung, brain,and bone development in theoffspring of vitamin D–deficientmothers may not reflect vitamin Ddeficiency per se but some otherhealth factor in the women that isassociated with maternal vitamin Ddeficiency. To address this, in ouranalyses, we adjusted for a range ofpotentially relevant confoundersincluding maternal age, parity,education and smoking, but it was notpossible to adjust for every possibleconfounder. The possibility remainsthat measures of sufficient serum25(OH)D during pregnancy reflecta healthy lifestyle with much timespent in sunshine. To our knowledge,there have been no studies toinvestigate whether outdoor activityduring pregnancy, or sun-inducedmolecules in skin, can complement theregulatory effects of vitamin D in organdevelopment. Although the studies inthe experimental animals cannotconclude that vitamin D sufficiency isresponsible for optimal organdevelopment during pregnancy, theysupport vitamin D as a contributor todevelopment processes.
It is possible that the offspring’s ownvitamin D status may contribute topostnatal development of their lungs,
brain, and bone. This may be mostrelevant for bone developmentmeasured in 20-year-old offspring.Maternal levels of vitamin D reflecta measure at a distinct time of fetaldevelopment. In contrast, duringchildhood and adolescence, vitamin Dmeasures represent a snapshot ofonly a short time period. Consistentwith this, in the Avon LongitudinalStudy of Parents and Children studyof ∼4000 mother-offspring pairs,14
further inclusion of offspring’scurrent vitamin D status had littleinfluence on associations betweenmaternal vitamin D and bonemeasures in offspring. In the Rainecohort study, serum 25(OH)D levelsin the 6- and 14-year-old offspringwere inversely associated with atopymeasures.22 However, there was nocorrelation between maternal serum25(OH)D measures and atopy of theoffspring at 6 years of age.6
One may think, in the individualstudies reported here, that there mayhave been confounding by aspects ofthe mother’s health. For example,mothers with impaired lung functionmay spend less time outdoors andthus have lower 25(OH)D levels andhave offspring with impaired lungfunction. What is striking with thestudies reported here is the breadthof health outcomes for which anassociation is reported; confoundingby maternal health status as theexplanation for these observedassociations is highly unlikely.
SOBERING LESSONS FROM STUDIESIN ADULTS DETERMINING THEREQUIREMENTS FOR VITAMIN DFOR BETTER HEALTH
During the past decade, there havebeen frequent reports fromobservational studies of inverseassociations between serum 25(OH)Dlevels and multiple health outcomes.In turn, randomized controlled trialsof vitamin D for risk or progression ofconditions such as cancer,cardiovascular disease, acuterespiratory infections, diabetes, andother autoimmune conditions were
established. Meta-analyses of trials ofvitamin D supplementation forvarious conditions have givenequivocal results,3,23,24 with a recentmeta-analysis suggesting that vitaminD may have, at best, a 15% benefiteffect on the risk of myocardialinfarction or ischemic heart disease,stroke or cerebrovascular disease,cancer, and total fracture.25 There areseveral possible explanations for thelack of efficacy of supplementationwith vitamin D in clinical trials. Theseinclude inadequate vitamin D dosage,recruitment of participants who werenot vitamin D deficient (in which caseno benefit of supplementation wouldbe expected), insufficient power inthe trials to detect a treatment effect,recruitment of individuals whosedisease process was too advanced tobe reversed, inadequate treatmentduration, or that other co-regulatorsare necessary for vitamin D to work(eg, calcium, serum binding proteins).Alternatively, vitamin D may bea confounder in the observationalstudies: higher 25(OH)D levels maybe simply a surrogate of a generallyhealthier lifestyle, disease may causelow levels of 25(OH)D throughreduced sunlight exposure or alteredmetabolism (reverse causality),26 orsun exposure may have beneficialhealth effects that are both vitamin Ddependent and independent and thatwill only be partially replicated byvitamin D supplementation.
Importantly, some negative effects onhealth have occurred at high levels ofserum 25(OH)D, including increasedfalls and fractures in older peoplegiven a large annual dose of 500 000IU vitamin D.23 A nonlinear, U-shapedassociation has been reportedbetween vitamin D levels and acutecoronary syndrome and mortality, aswell as for other conditions.27
CONCLUSIONS
Despite clear concerns about drawingstrong conclusions fromobservational data that do notconfirm that vitamin D is
PEDIATRICS Volume 135, number 1, January 2015 e171 at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

mechanistically involved, from theanalyses of children in ourcommunity cohort and the supportiveexperimental animal studies,pregnancy may be a time of particularsensitivity to vitamin D deficiency.This study of mother-offspring pairsis important because the motherswere not selected for anypredisposing condition, and theirserum 25(OH)D levels were notskewed to particularly high or lowlevels as can be contrived in animalstudies. Approximately 900 mother-offspring pairs were sufficient to findassociations of bone, lung, and braindevelopment with maternal serum25(OH)D levels. This study wasperformed in Perth, WesternAustralia, a city of mild winters. Yetthe variations in serum 25(OH)Dlevels were sufficient to see theseassociations with organ developmentand, we propose, predictors of variedhealth outcomes in later life. Ofimportance, in this cohort,associations of maternal serum25(OH)D levels with lung function,indices of neurodevelopment andmental health, and peak bone masswere detected and suggest thatsufficient vitamin D is permissive foroptimal development of multipleorgans, not just bone as would behistorically proposed.
INTERPRETATION
Although meta-analyses suggest thatvitamin D has relatively minor effectson adult health,3,23–25 it remainspossible (and indeed likely) thatvitamin D may have an importantdevelopmental role in the fetusduring pregnancy. Confirmation ofthis will require carefully plannedtrials of vitamin D supplementation invitamin D–deficient pregnant womenin which outcome measures shouldinclude assessment of respiratory,brain, and skeletal development inthe offspring. This will not be an easytask and will require significantresources because many of thedevelopmental outcomes will not be
evident for many years and severalfunding cycles. An unresolved issue iswhat concentration of maternalserum 25(OH)D is sufficient orindeed optimal in pregnancy. Theissue is complicated by thesuboptimal performance and lack ofharmonization of assays for serum25(OH)D.28 Reference methods suchas liquid chromatography/tandemmass spectrometry are increasinglyused but are expensive and laborintensive. Some practitionersadvocate high doses of vitamin D of4000 IU per day during pregnancy,and in a combined analysis of2 randomized vitamin Dsupplementation trials in pregnantwomen, 4000 IU/day was associatedwith lower risk of hypovitaminosis Dand maternal comorbidities ofpregnancy than control and 2000IU/day groups.29 Whatever thesupplementation dose, one mustensure that 25(OH)D levels aremonitored because excessive levelsof serum vitamin D during pregnancyhave been associated withincreased prevalence ofschizophrenia,30 and this U-shapedcurve may be relevant fordevelopment of other conditions.Despite the uncertainty of theoptimal level, our results in childrenof unselected healthy mothershighlight the impact of sufficientvitamin D on development of lungs,brain, and bone of the fetus. Until wehave better data includingrandomized controlled trials ofvitamin D supplementation ofpregnant women and comprehensiveassessment of the offspring,maintaining a 25(OH)D level of .50nmol/L in pregnant women must beconsidered a reasonable target.
ACKNOWLEDGMENTS
We gratefully acknowledge theRaine Study participants and theirfamilies, and the Raine Study teamfor cohort coordination and datacollection. We acknowledge theUniversity of Western Australia
(UWA), Telethon Kids Institute,Raine Medical Research Foundation,UWA Faculty of Medicine, Dentistryand Health Sciences, Women’s andInfant’s Research Foundation,Curtin University and Edith CowanUniversity for providing RaineStudy core management funding.The funding sources had no role ininterpretation of the data.
REFERENCES1. Barker DJP, Winter PD, Osmond C,
Margetts B, Simmonds SJ. Weight ininfancy and death from ischaemic heartdisease. Lancet. 1989;2(8663):577–580
2. Prescott SL. Early-life environmentaldeterminants of allergic diseases andthe wider pandemic of inflammatorynoncommunicable diseases. J AllergyClin Immunol. 2013;131(1):23–30 doi:10.1016/j.jaci.2012.11.019
3. Theodoratou E, Tzoulaki I, Zgaga L,Ioannidis JPA. Vitamin D and multiplehealth outcomes: umbrella review ofsystematic reviews and meta-analyses ofobservational studies and randomisedtrials. BMJ. 2014;348:g2035 doi:10.1136/bmj.g2035
4. Ross AC, Manson JE, Abrams SA, et al.The 2011 report on dietary referenceintakes for calcium and vitamin D fromthe Institute of Medicine: what cliniciansneed to know. J Clin Endocrinol Metab.2011;96(1):53–58 doi:10.1210/jc.2010-2704
5. Newnham JP, Evans SF, Michael CA,Stanley FJ, Landau LI. Effects of frequentultrasound during pregnancy:a randomised controlled trial. Lancet.1993;342(8876):887–891
6. Zosky GR, Hart PH, Whitehouse AJO,et al. Vitamin D deficiency at 16 to 20weeks’ gestation is associated withimpaired lung function and asthma at6 years of age. Ann Am Thorac Soc.2014;11(4):571–577 doi:10.1513/AnnalsATS.201312-423OC
7. Whitehouse AJ, Holt BJ, Serralha M, HoltPG, Kusel MM, Hart PH. Maternal serumvitamin D levels during pregnancy andoffspring neurocognitive development.Pediatrics. 2012;129(3):485–493 doi:10.1542/peds.2011-2644
8. Allen KL, Byrne SM, Kusel MM, Hart PH,Whitehouse AJ. Maternal vitamin D levels
e172 HART et al at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

during pregnancy and offspring eatingdisorder risk in adolescence. Int J EatDisord. 2013;46(7):669–676 doi:10.1002/eat.22147
9. Whitehouse AJ, Holt BJ, Serralha M, HoltPG, Hart PH, Kusel MM. Maternal vitaminD levels and the autism phenotypeamong offspring. J Autism Dev Disord.2013;43(7):1495–1504 doi:10.1007/s10803-012-1676-8
10. Zhu K, Whitehouse AJ, Hart PH, et al.Maternal vitamin D status duringpregnancy and bone mass in offspring at20 years of age: a prospective cohortstudy. J Bone Miner Res. 2014;29(5):1088–1095 doi:10.1002/jbmr.2138
11. Dawodu A, Akinbi H. Vitamin D nutritionin pregnancy: current opinion. Int JWomens Health. 2013;5:333–343 doi:10.2147/IJWH.S34032
12. Merkus PJ, ten Have-Opbroek AA, QuanjerPH. Human lung growth: a review.Pediatr Pulmonol. 1996;21(6):383–397
13. Javaid MK, Crozier SR, Harvey NC, et al;Princess Anne Hospital Study Group.Maternal vitamin D status duringpregnancy and childhood bone mass atage 9 years: a longitudinal study. Lancet.2006;367(9504):36–43
14. Lawlor DA, Wills AK, Fraser A, Sayers A,Fraser WD, Tobias JH. Association ofmaternal vitamin D status duringpregnancy with bone-mineral content inoffspring: a prospective cohort study.Lancet. 2013;381(9884):2176–2183 doi:10.1016/S0140-6736(12)62203-X
15. Heaney RP, Abrams S, Dawson-Hughes B,et al. Peak bone mass. Osteoporos Int.2000;11(12):985–1009
16. Zosky GR, Berry LJ, Elliot JG, James AL,Gorman S, Hart PH. Vitamin D
deficiency causes deficits in lungfunction and alters lung structure. AmJ Respir Crit Care Med. 2011;183(10):1336–1343 doi:10.1164/rccm.201010-1596OC
17. Kesby JP, Eyles DW, Burne TH, McGrath JJ.The effects of vitamin D on braindevelopment and adult brain function. MolCell Endocrinol. 2011;347(1–2):121–127doi:10.1016/j.mce.2011.05.014
18. Karras SN, Anagnostis P, Bili E, et al.Maternal vitamin D status in pregnancyand offspring bone development: theunmet needs of vitamin D era.Osteoporos Int. 2014;25(3):795–805 doi:10.1007/s00198-013-2468-5
19. Bouillon R, Carmeliet G, Verlinden L, et al.Vitamin D and human health: lessonsfrom vitamin D receptor null mice.Endocr Rev. 2008;29(6):726–776 doi:10.1210/er.2008-0004
20. Hart PH, Gorman S, Finlay-Jones JJ.Modulation of the immune system by UVradiation: more than just the effects ofvitamin D? Nat Rev Immunol. 2011;11(9):584–596 doi:10.1038/nri3045
21. Sayers A, Tobias JH. Estimated maternalultraviolet B exposure levels inpregnancy influence skeletaldevelopment of the child. J ClinEndocrinol Metab. 2009;94(3):765–771doi:10.1210/jc.2008-2146
22. Hollams EM, Hart PH, Holt BJ, et al.Vitamin D and atopy and asthmaphenotypes in children: a longitudinalcohort study. Eur Respir J. 2011;38(6):1320–1327 doi:10.1183/09031936.00029011
23. Reid IR, Bolland MJ, Grey A. Effects ofvitamin D supplements on bone mineraldensity: a systematic review and meta-
analysis. Lancet. 2014;383(9912):146–155doi:10.1016/S0140-6736(13)61647-5
24. Chowdhury R, Kunutsor S, Vitezova A,et al. Vitamin D and risk of cause specificdeath: systematic review and meta-analysis of observational cohort andrandomised intervention studies. BMJ2014;348:g1903
25. Bolland MJ, Grey A, Gamble GD, Reid IR.The effect of vitamin D supplementationon skeletal, vascular, or cancer outcomes:a trial sequential meta-analysis. LancetDiabetes Endocrinol. 2014;2(4):307–320doi:10.1016/S2213-8587(13)70212-2
26. Autier P, Boniol M, Pizot C, Mullie P.Vitamin D status and ill health:a systematic review. Lancet DiabetesEndocrinol. 2014;2(1):76–89 doi:10.1016/S2213-8587(13)70165-7
27. Rosen CJ, Taylor CL. Commonmisconceptions about vitaminD—implications for clinicians. Nat RevEndocrinol. 2013;9(7):434–438 doi:10.1038/nrendo.2013.75
28. Fraser WD, Milan AM. Vitamin D assays:past and present debates, difficulties, anddevelopments. Calcif Tissue Int. 2013;92(2):118–127 doi:10.1007/s00223-012-9693-3
29. Wagner CL, McNeil RB, Johnson DD, et al.Health characteristics and outcomes oftwo randomized vitamin Dsupplementation trials duringpregnancy: a combined analysis.J Steroid Biochem Mol Biol. 2013;136:313–320 doi:10.1016/j.jsbmb.2013.01.002
30. McGrath JJ, Eyles DW, Pedersen CB, et al.Neonatal vitamin D status and risk ofschizophrenia: a population-based case-control study. Arch Gen Psychiatry. 2010;67(9):889–894 doi:10.1001/archgenpsychiatry.2010.110
PEDIATRICS Volume 135, number 1, January 2015 e173 at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-1860; originally published online December 15, 2014;Pediatrics
A. MountainWhitehouse, Kun Zhu, Karina L. Allen, Merci M. Kusel, Denise Anderson and Jenny
Prue H. Hart, Robyn M. Lucas, John P. Walsh, Graeme R. Zosky, Andrew J.O.Vitamin D in Fetal Development: Findings From a Birth Cohort Study
ServicesUpdated Information &
/peds.2014-1860http://pediatrics.aappublications.org/content/early/2014/12/09including high resolution figures, can be found at:
Subspecialty Collections
n_wellnesshttp://pediatrics.aappublications.org/cgi/collection/pediatriciaPediatrician Wellnessthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-1860; originally published online December 15, 2014;Pediatrics
A. MountainWhitehouse, Kun Zhu, Karina L. Allen, Merci M. Kusel, Denise Anderson and Jenny
Prue H. Hart, Robyn M. Lucas, John P. Walsh, Graeme R. Zosky, Andrew J.O.Vitamin D in Fetal Development: Findings From a Birth Cohort Study
http://pediatrics.aappublications.org/content/early/2014/12/09/peds.2014-1860
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Univ Of Western Australia on December 16, 2014pediatrics.aappublications.orgDownloaded from
View publication statsView publication stats