Vitamin D as a therapy for colitis: A systematic review
7
REVIEW ARTICLE Vitamin D as a therapy for colitis: A systematic review Imogen Nicholson a , A. Mark Dalzell a , Wael El-Matary b , c , ⁎ a Division of Paediatric Gastroenterology, Hepatology and Nutrition, Alder Hey Children's NHS Foundation Trust, Liverpool, UK b Section of Paediatric Gastroenterology, Department of Paediatrics, Faculty of Medicine, University of Manitoba, Winnipeg, Canada c King Saud University, Riyadh, Saudi Arabia Received 20 November 2011; received in revised form 5 January 2012; accepted 5 January 2012 KEYWORDS Inflammatory bowel disease; Crohn's; Colitis; Vitamin D Abstract Background and aim: The effect of vitamin D supplementation on immune disorders has been a topical research focus. The aim of this systematic review was to examine the current evidence of the effect of vitamin D supplementation as a therapy for colitis. Methods: The following databases were searched: MEDLINE, Pubmed, Scopus, Web of Knowl- edge, Cinicaltrials.gov and the Cochrane Central Register of Controlled Trials using the terms ‘inflammatory bowel disease’‘Crohn's disease’‘ulcerative colitis’‘colitis’ [and] ‘vitamin D’. Both human and animal studies published in English language were examined. The reference lists of included studies and review articles were manually searched for any relevant studies. Results: Four studies were included in this systematic review. All reported an improvement in disease activity with vitamin D supplementation. The only high quality human study reported a non-significant reduction of relapse rate for Crohn's disease. No major adverse effects of vita- min D supplementation were reported. Conclusions: Although there is some evidence that supplemental vitamin D, as an adjunctive treat- ment, may help in controlling colitis, this evidence is not enough to justify using vitamin D in treat- ing inflammatory bowel disease (IBD). Large high quality placebo-controlled randomised controlled trials are needed to explore a possible benefit of using vitamin D in treating IBD. Crown Copyright © 2012 Published by Elsevier B.V. on behalf of European Crohn's and Colitis Organisation. All rights reserved. Contents 1. Introduction ......................................................... 406 2. Materials and methods ................................................... 406 ⁎ Corresponding author at: AE-408, 840 Sherbrook St., Winnipeg, Manitoba, Canada R3A 1S1. Tel.: +1 204 787 2441; fax: +1 204 787 4807. E-mail address: [email protected] (W. El-Matary). 1873-9946/$ - see front matter. Crown Copyright © 2012 Published by Elsevier B.V. on behalf of European Crohn's and Colitis Organisation. All rights reserved. doi:10.1016/j.crohns.2012.01.007 Available online at www.sciencedirect.com Journal of Crohn's and Colitis (2012) 6, 405–411
-
Upload
imogen-nicholson -
Category
Documents
-
view
217 -
download
1
Transcript of Vitamin D as a therapy for colitis: A systematic review

Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2012) 6, 405–411
REVIEW ARTICLE
Vitamin D as a therapy for colitis: A systematic reviewImogen Nicholson a, A. Mark Dalzell a, Wael El-Matary b, c,⁎
a Division of Paediatric Gastroenterology, Hepatology and Nutrition, Alder Hey Children's NHS Foundation Trust, Liverpool, UKb Section of Paediatric Gastroenterology, Department of Paediatrics, Faculty of Medicine, University of Manitoba,Winnipeg, Canadac King Saud University, Riyadh, Saudi Arabia
Received 20 November 2011; received in revised form 5 January 2012; accepted 5 January 2012
⁎ Corresponding author at: AE-408, 8E-mail address: [email protected]
1873-9946/$ - see front matter. Crownrights reserved.doi:10.1016/j.crohns.2012.01.007
KEYWORDSInflammatory bowel disease;Crohn's;Colitis;Vitamin D
Abstract
Background and aim: The effect of vitamin D supplementation on immune disorders has been atopical research focus. The aim of this systematic review was to examine the current evidence ofthe effect of vitamin D supplementation as a therapy for colitis.Methods: The following databases were searched: MEDLINE, Pubmed, Scopus, Web of Knowl-
edge, Cinicaltrials.gov and the Cochrane Central Register of Controlled Trials using the terms‘inflammatory bowel disease’ ‘Crohn's disease’ ‘ulcerative colitis’ ‘colitis’ [and] ‘vitamin D’.Both human and animal studies published in English language were examined. The referencelists of included studies and review articles were manually searched for any relevant studies.Results: Four studies were included in this systematic review. All reported an improvement indisease activity with vitamin D supplementation. The only high quality human study reporteda non-significant reduction of relapse rate for Crohn's disease. No major adverse effects of vita-min D supplementation were reported.Conclusions: Although there is some evidence that supplemental vitamin D, as an adjunctive treat-ment, may help in controlling colitis, this evidence is not enough to justify using vitamin D in treat-ing inflammatory bowel disease (IBD). Large high quality placebo-controlled randomised controlledtrials are needed to explore a possible benefit of using vitamin D in treating IBD.Crown Copyright © 2012 Published by Elsevier B.V. on behalf of European Crohn's and ColitisOrganisation. All rights reserved.40 Sherbrook St., Winnipeg, M.ca (W. El-Matary).
Copyright © 2012 Published by
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4062. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 406
anitoba, Canada R3A 1S1. Tel.: +1 204 787 2441; fax: +1 204 787 4807.
Elsevier B.V. on behalf of European Crohn's and Colitis Organisation. All

406 I. Nicholson et al.
2.1. Search strategy and eligibility criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4062.1.1. Inclusion criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4062.1.2. Exclusion criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4072.1.3. Primary outcome and reporting the PICO formula . . . . . . . . . . . . . . . . . . . . . . . . . . . . 407
2.2. Data extraction and quality assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4073. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4074. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4105. Conclusions and recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 410Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411Financial disclosure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411
1. Introduction
Vitamin D is very important in calcium homeostasis, controllingthe formation and resorption of bone.1 The immune-relatedfunction of vitamin D was not discovered until the 1980s. Theidentification of vitamin D receptors on peripheral bloodmono-nuclear cells in 1983 sparked the interest in a possible role ofvitamin D in the immune system.1,2 Vitamin D is acknowledgedas an immune system regulator.3 T-Cell mediated immunity isunder modulatory control of 1,25dihydroxycholcecalciferol,the active form of vitamin D.4,5 The absence of vitamin D wasshown to blunt the T-cell mediated immune responses. Atvery high doses of vitamin D, this effect recurred.3
Stores of vitamin D in the body comprise vitamin D2 andvitamin D3. Most body stores come from vitamin D3 whichis synthesised by the direct action of sunlight on the skin.6
A small proportion of total vitamin D is obtained from thediet, which is known as vitamin D2. This is mainly obtainedfrom fish oil or as a direct supplementation. Few food ele-ments are naturally rich in vitamin D, so its levels dependon sunlight exposure or supplementation to be replenished.6
The zenith angle of the sun determines the amount of D3produced in the skin.3,6 Geographical latitude, season andtime of day affect this angle. Countries in northern climatesreceive an oblique angle in autumn and winter. Such anangle precludes the production of vitamin D3.6,7
Inflammatory bowel disease (IBD), an immune mediateddisease of unknown aetiology that affects the gastrointesti-nal tract, is most prevalent in northern climates such asNorth America and Northern Europe.8 There are two distinctforms of IBD — Crohn's disease (CD) and ulcerative colitis(UC).8 The pathogenesis of IBD involves a complex interplaybetween genetic, environmental and immunological fac-tors.9 It has been determined that in both forms of IBD, thetissue damage results from an inappropriate or exaggeratedimmune response to luminal antigens of gut microflora. Tcells overproduce inflammatory mediators like interleukin-17 (IL-17), tumour necrosis factor α (TNF α) and interferongamma (IFN-Ý).10 The tissue damage occurs in areas thatare heavily infiltrated with activated CD4+ lymphocytes.11
A recent hypothesis linking vitamin D deficiency to devel-opment of immune-related disorders has been proposed.This argues that decreased outdoor activity and vitamin Dpoor diets have led to fluctuations in vitamin D status in de-veloped countries, particularly those that experience longwinter seasons.12,13 For people living in northern climates,vitamin D deficiency is relatively common.14 In particular,patients with IBD are likely to have a high incidence of
hypovitaminosis D.15 This could be due to a number of differ-ent mechanisms, including decreased intestinal absorption,increased intestinal loss through a protein losing enteropa-thy, and decreased exposure to sunlight. This has led someto believe that vitamin D deficiency may play a role in thepathogenesis of IBD.3
There is a mounting evidence for a link between vitamin Davailability either from the sunshine or diet and other auto-immune diseases.16 Finland has the highest rates of type 1 di-abetes in the world.17 A Finnish study involving over 12,000children, showed vitamin D supplementation decreased therisk of type 1 diabetes mellitus by 80%.17 Multiple sclerosis(MS) is similarly most prevalent in countries far from theequator, with a particularly high incidence in Scotland.18 Vi-tamin D deficiency is common in patients with MS.3 Womenwith the highest vitamin D intakes had a 40% reduction inrisk of developing MS.19 Clinical improvement of patientswith rheumatoid arthritis was strongly associated with highdose vitamin D.20
The aim of this systematic review was to examine the ev-idence assessing the effect of vitamin D for treating colitis inhumans and experimental colitis in animals, i.e. idiopathicand experimental inflammatory bowel disease.
2. Materials and methods
2.1. Search strategy and eligibility criteria
Using the terms “COLITIS”, “CROHNS”, “INFLAMMATORYBOWEL DISEASE” [and] “VITAMIN D” the following databaseswere searched for relevant papers: MEDLINE (1966 — Week 1July 2011); Pubmed (1950 — Week 1 July 2011); Scopus; Webof Knowledge; clinicaltrials.gov and the Cochrane CentralRegister of Controlled Trials (CENTRAL). In addition, the ref-erence lists of all included studies and review articles werereviewed for relevant citations.
2.1.1. Inclusion criteriaAll human (any age) and animal randomised controlled
(RCT) and cohort studies specifically investigating the effectof vitamin D supplementation on disease activity in colitis(either inducing or maintaining remission), regardlessserum levels of vitamin D. Disease activity was assessedusing any indices in humans or examination of the colonwith experimental colitis in animals. Only studies writtenin the English language were included.

407Vitamin D in colitis
2.1.2. Exclusion criteriaStudies in any language other than English, case reports,
case series, studies which examined the role of vitamin D inthe bone mineral density of IBD sufferers, studies lookinginto the effect of vitamin D receptors on disease activity, ob-servational studies commenting on vitamin D level in IBD pa-tients, but not intervening with supplements. Review articleswere also excluded, as were abstracts.
2.1.3. Primary outcome and reporting the PICO formulaP (Participants: Patients of any age with colitis or animals
with experimental colitis). I (Interventions: vitamin D sup-plementation). C (Comparisons: Patients with colitis or ani-mals with experimental colitis on placebo, any medicationor no vitamin D). O (Outcome (primary): inducing or main-taining remission of the disease). Secondary outcome wasany reported adverse effects of vitamin D in human studies.
2.2. Data extraction and quality assessment
Retrieved articles were screened based on title and then ab-stract content by one author (IN) and categorised into ‘in-clude’, ‘possible’ and ‘exclude’. Where available, the fulltexts of the ‘include’ and ‘possible’ were obtained andassessed independently by the two authors (IN and WE). Anydisagreement was resolved through a consensus discussionand consulting a third author (AMD). During the process ofquality assessment, none of the authors were blinded as toany of the following: the authors, journal, institution, yearof publication or results. Quality assessment of each studywas carried out using Jadad and Higgins criteria for RCTs.21,22
3. Results
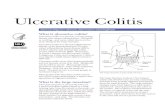
The literature search algorithm is summarised in Fig. 1. Thecharacteristics of the included and excluded studies aresummarised in Tables 1–3. Four studies were included23–26:two included human participants (Table 1) and the other
STUDIES INCLUDED BASED ON TITLE 191
INCLUDED BASED ONABSTRACT
14
STUDIES INCLUDED
2
STUDIES UNSURE
3
FINAL STUDIESINCLUDED
4
STUINC
Figure 1 Algorithm o
two included experimental animals (Table 2). All four stud-ies showed some benefits to use the vitamin D supplements.However, only two studies had results which achieved statis-tical significance. The only double-blinded RCT which was ofa good quality examined the effect of supplemental vitaminD3 in maintaining (rather than inducing) remission forCrohn's disease.26 Compared to placebo, the study reporteda non-significant reduction of relapse rate at the end of12 months (29% vs. 13%, p=0.06). There were no reportedadverse effects directly attributable to vitamin D.26
The other human study looked into the effect of 2 differ-ent forms of vitamin D on Crohn's disease activity (and bonemarkers).25 One form of vitamin D was superior in maintain-ing disease remission compared to the other form at the endof 6 weeks of the trial but not at the end of 12 months.25 Thestudy did not address adverse events of vitamin D.25
Two animal studies were included in this review (Table 3).Both studies showed a significant effect of vitamin D on exper-imental colitis.23,24 In the study by Cantorna et al., interleukin10 knockout (IL-10 KO) mice were given 0.005 mcg of 1,25-dihydroxycholecalciferol. Over a four-week period, IBD symp-toms significantly (Pb0.05) improved, compared to a cohortof vitamin D naive mice. Vitamin D deficient mice rapidly de-veloped diarrhoea and a wasting disease, which induced mor-tality.23 In contrast, supplementation with 50 IU significantlyameliorated symptoms of IBD in the mice. A separate groupwas given higher levels of vitamin D (0.2 mcg). This blockedthe progression and ameliorated the (Pb0.05) symptoms inthe IL 10-KO mice after just two weeks.23 This suggests a posi-tive correlation between level of supplementation and speedof disease-reducing action. The small intestines of deficient an-imals were significantly heavier than those supplemented, at9.9% of total body weight. This is a remarkable result of morethan double the expected proportion in a typical micepopulation. There were no significant differences in the overallbody weight of the mice in the intervention and controlgroup.23
Daniel et al. examined whether the vitamin D analogue22-Ene-25-Oxa-vitamin D has a comparable efficacy to
STUDIES EXCLUDEDBASED ONABSTRACT 178
STUDIES EXCLUDED
9
DIESLUDED 2
STUDIES EXCLUDED
1
f literature search.

Table 1 Characteristics of included studies: human.
Study N Meandiseaseduration
Methodology Purpose Intervention Assessment Definiti ofimprove nt
Conclusions Quality assessment
Mihelleret al.25
37 9.6 years Singlecentrecohort
Compare effectsof 1,25 dihydroxyvitaminand 25 hydroxyvitamin Don bone pathologyand disease activityin CD patients
Group A given ‘active’ vitaminD3 — 2×0.25 mcgs alfacalcidol/day.Group B given ‘plain’ vitaminD3 — 1000 IU cholecalciferol/day.
CDAI Significreducti ndiseaseactivitymeasur byCDAI, Cand SIB
Significantdifferencesshown at 6 weeksbut thesedisappeared by12th month
Open labelSmall cohort
Jorgensenet al.26
94 7 years Multi-centrerandomiseddoubleblindedplacebocontrolledtrial
Assess the effect ofvitamin D3 as adjunctiveagent compared to placein maintaining remissionCD, and its effect on serulevels of Vitamin D
One group given 1200 IU vitaminD3+1200 mg calcium/dayOne group givenplacebo+1200 mg calcium/day
CDAI CDAI of 0+and anincreasCDAI ofcompar tobaseline
1200 IEsupplementsincreasedvitamin D levelsbut did notsignificantlyreduce relapserate
Good double blindrandomizationprocess with adequatesequence generation.Allocation concealmentis not clear.Adequate description ofdropouts.
Table 2 Characteristics of included studies: mice models.
Study Numberofanimals
Method ofinducing colitis-like state
Purpose of study Int ntion Assessment ofdisease activity
Conclusio Qualityassessment
Cantornaet al.23
36 Transgenicbreeding ofInterleukin 10-knockout mice
Compare vitamin Ddeficiency and vitaminD sufficient mice todisease activity
No min D vs.0.0 mcgs/d calcitriolNo min D vs.0.2 g/d calcitriol
-Colon weight-Histological exam of colon-Body mass
Vitamin D gnificantly ameliorated symptoms.Higher d of calcitriol acted quicker todecrease tivity.
Animalstudy
Daniel etal.24
Notstated
2,4,6-trinitrobenzenesulfonic acid(TNBS) rectalenema
Compare efficacy ofvitamin D analogue(ZK156979) with 1,25-dihydroxyvitamin D
0.1 0 mcgs/kg bodywe ZK156979 vs0.2 gs/kg body weightcal iol
-Macroscopic exam of colon-Histological exam of colon-Colon length-Colon weight-Body mass-Stool consistency-Quantity of rectal bleeding
Vitamin nalogue (ZK1569790) is as potentas 1,25-d droxyvitamin D. It does not inducehypercal mia. Both substances significantlyreduce d ase activity.
Animalstudy
408I.Nicholson
etal.
D
boofm
erve
vita05vitamc–2.ightmccitr
onme
anton i
edRPDQ15
e in70ed
ns
sioseac
D aihycaeise

Table 3 Characteristics of excluded studies.
Study Design Outcome Reason for Exclusion
Harries et al.27 Observational Under-nourished CD patients have low vitamin D levels Not interventional, measures vitamin D levelsGinanjar et al.28 Review article Some studies show that vitamin D inhibits induction of
autoimmune encephalomyelitis, thyroiditis, type-1diabetes mellitus, inflammatory bowel disease (IBD),systemic lupus erythematosus, and collagen-inducedarthritis and Lyme arthritis
Review article
Froicu et al .29 Experimental model VDR deficiency accelerated the development ofexperimental IBD in mice
Receptor status investigated, not vitamin D levels
Utilisky et al.15 Retrospective cohort study Vitamin D deficiency is common in IBD and is independentlyassociated with lower HRQOL and greater disease activity in CD.
Observational, did not give supplements butmeasured vitamin levels.
El Matary et al.30 Cross sectional analyticalstudy
Vitamin D levels are not affected by disease severity Cross sectional, not interventional, no supplementsgiven.
Cantorna3 Review article Autoimmune diseases like IBD and MS are acutely affectedby vitamin D status and vitamin D receptor signalling.
Review article
Gilman et al.31 Cross sectional observationalstudy
High proportion of CD patients have vitamin D deficiency Cross sectional observational — no supplements given
Leslie et al.32 Cohort study A minority of recently diagnosed IBD patients would havean optimal vitamin D serum levels which correlatedwith bone mineral density.
No intervention or vitamin D supplement s given
Stio et al.33 In-vitro study T lymphocyte proliferation was inhibited in the presence ofvitamin D and two vitamin D analogues — EB 1089 and KH 1060.
In vitro studyNot a human or animal study
Cantorna34 Review article Mechanisms underlying the effect of vitamin D on theimmune system.In the absence of vitamin D and the VDR, autoimmunity occursin the gastrointestinal tract due to increased numbers of IL-17and IFN-γ secreting T-cells and a concomitant reduction inregulatory T-cells
Review article
409Vitam
inDin
colitis

410 I. Nicholson et al.
active vitamin D. The analogue clearly reduced the severityof TNBS-induced colitis without hypercalcemic side effectsseen on occasion with the use of vitamin D itself. This oc-curred with potency comparable to calcitriol.24 Significantimprovement was shown in weight gain, a decrease in clini-cal activity score, and the amelioration of macroscopicsigns of colitis.24
4. Discussion
The vitamin D supplementation in the treatment of someimmune-related diseases is increasing. However, its role inthe treatment of IBD is unclear. Four studies fulfilled the in-clusion criteria of this systematic review. Two animal studiesfound that vitamin D had a statistically significant effect ondisease activity of experimental colitis.23,24 Two humanstudies documented some benefits of supplemental vitaminD in maintaining remission of Crohn's disease.25,26
Jorgensen et al. showed a robust method in a randomiseddouble-blinded placebo controlled trial.26 Although samplesize calculation was provided, one could argue that statisti-cal significance was not achieved due to type II statisticalerror.
Miheller et al. compared 2 different forms of vitamin D.25
A significant decrease in Crohn's Disease Activity Index(CDAI) scores and CRP was shown 6 weeks into the trial.These differences in disease activity disappeared by12 months (the end of the trial).25 The trial was comparingactive to plain vitamin D, rather than vitamin D to placebo.Therefore, the absence of sustained significance in differ-ences did not undermine efficacy of vitamin D, but ratheradditional benefit gained by using an active form of it.
Quality of life information was available in the paper byMiheller et al. through the use of a HRQOL questionnaire.25
This allowed an extra dimension to the measurement of ac-tivity of IBD to be assessed. Quality of life, like disease activ-ity, improved significantly in the short term (6 weeks) butnot in the long term. This trial was not blinded so it isdebateable how accurate this information is. Such QOL as-sessment was not made in Jorgensen's study.26
It was not clear in these 2 studies the extent of sunlightexposure that the patients had. Variations in lifestyle andoccupation of participants would have led to a disparity inthe amount of sunlight received by patients.
No human studies looking at the effect of vitamin D sup-plementations in achieving remission of IBD or maintainingremission in ulcerative colitis were found. No study showedthat vitamin D or analogue supplementations are harmfulto the participants or worsen their colitis. This indicatesthat they are both well tolerated.
The studies involving an experimental model of IBD inmice showed a reduction in disease activity that achievedstatistical significance. However, the control over theamount of vitamin D the mice were able to synthesise dif-fered between the studies. In the paper by Cantorna et al.,pregnant mice of 2 weeks gestation were deprived of vita-min D. This ensured that their offspring would be completelyvitamin D deficient by week 5 of age, at entry to the study.In addition to this, trial mice were housed under ‘yellowlight,’ which prevented the synthesis of vitamin D throughtheir skin.23 In contrast, the mice used in the study by Daniel
et al. were not the offspring of vitamin D deprived mothersand were fed “standard mouse chow” from birth.24 Althoughthey were kept in a controlled environment, they were notkept under yellow light. As a consequence, they wouldhave been able to synthesise vitamin D3 through their skin.
Different methods were used to induce IBD in rodents.Daniel et al. induced colitis at the beginning of the experi-ment through rectal enemas of 2,4,6-trinitobenzenesulfonicacid (TNBS).23 In contrast, Cantorna et al. used Interleukin-10 knockout transgenic mice (Il-10 KO) raised in specificpathogen free facilities.24 These mice had endured symp-toms of IBD from birth. Perhaps one could argue that thetransgenic mice represent the chronic nature of IBD more re-liably than a TNBS-induced model.
The results from animal studies are of course limited intheir application to the human species. Nonetheless, exper-imental models are an important foundation for establishingrelationships between interventions and disease activity.
A thorough literature search was conducted for this sys-tematic review. All relevant references cited in includedstudies were followed ensuring all relevant published re-search was included. The limitations of this review includethe paucity of the studies included. Nonetheless, this high-lights the strong need for well-planned and conductedstudies addressing this objective. The role of vitamin D inmanaging IBD should be addressed not only in achieving re-mission of active IBD but also in maintaining remission. Im-portant factors that could affect the outcome like thedose, route, and duration of treatment of vitamin D shouldbe explored. Moreover, serum level of vitamin D beforeand during therapy should be carefully examined.
Neither of the human studies included patients sufferingfrom UC. Arguably the results of the review do not fairly re-flect both forms of IBD. Further research involving UC partic-ipants would be beneficial. The results of all four studies arelimited by small sample size. In the two human studies atotal of 141 participants were included.25,26
Further limitations include the exclusion of non-Englishstudies and being unable to include unpublished work andgrey literature. One would hope that at some point therewill be established methods to access unpublished studies.Attempts were made in this review to contact the authorsof one unpublished study but a reply was not received.
5. Conclusions and recommendations
There is some evidence from human studies that vitamin Dsupplementations may help in maintaining remission forCrohn's disease. However the results appear significant inmurine models of experimental colitis. The public health im-plications, of a possible link between vitamin D and IBD, war-rant further funding for research into this area. Large, multi-centre double-blinded placebo controlled trials are neededto determine further the effects of vitamin D on the diseaseactivity of IBD. The effect of vitamin D supplementationshould be evaluated not only on establishing remission butalso on maintaining remission of IBD.
Currently, there are a number of on-going clinical trialsthat are addressing this topic. This holds promise that in thefuture we will have a better evidence for supporting the useof vitamin D supplementation in the treatment of IBD.

411Vitamin D in colitis
Conflict of interest
None.
Financial disclosure
None.
References
1. Bhalla AK, Amento EP, Clemens TL, Holick MF, Krane SM. Specif-ic high-affinity receptors for 1,25-dihydroxyvitamin D3 inhuman peripheral blood mononuclear cells: presence in mono-cytes and induction in T lymphocytes following activation. JClin Endocrinol Metab 1983;57:1308–10.
2. Provvedini DM, Tsoukas CD, Deftos LJ, Manolagas SC. 1,25-dihydroxyvitamin D3 receptors in human leukocytes. Science1983;221:1181–3.
3. Cantorna MT. Vitamin D and its role in immunology: multiplesclerosis, and inflammatory bowel disease. Prog Biophys MolBiol 2006;92:60–4.
4. Yang S, Smith C, Prahl JM, Luo X, DeLuca HF. Vitamin D defi-ciency suppresses cell-mediated immunity in vivo. Arch Bio-chem Biophys 1993;303:98–106.
5. Yang S, Smith C, DeLuca HF. 1 alpha, 25-Dihydroxyvitamin D3and 19-nor-1 alpha, 25-dihydroxyvitamin D2 suppress immuno-globulin production and thymic lymphocyte proliferation invivo. Biochim Biophys Acta 1993;1158:279–86.
6. Holick MF. Vitamin D: a millenium perspective. J Cell Biochem2003;88(2):296–307.
7. Webb AR, Kline L, Holick MF. Influence of season and latitude onthe cutaneous synthesis of vitamin D3: exposure to winter sun-light in Boston and Edmonton will not promote vitamin D3 syn-thesis in human skin. J Clin Endocrinol Metab 1988;67:373–8.
8. Levin AD, Wadhera V, Leach ST, Woodhead HJ, Lemberg DA,Mendoza-Cruz AC, et al. Vitamin D deficiency in children withinflammatory bowel disease. Dig Dis Sci 2011;56:830–6.
9. Lim WC, Hanauer SB, Li YC. Mechanisms of disease: vitamin Dand inflammatory bowel disease. Nat Clin Pract GastroenterolHepatol 2005;2:308–15.
10. Ardizzone S, Cassinotti A, Bevilacqua M, Clerici M, Porro GB. Vita-min D and inflammatory bowel disease. Vitam Horm 2011;86:367–77.
11. Monteleone G, Fina D, Caruso R, Pallone F. New mediators ofimmunity and inflammation in inflammatory bowel disease.Curr Opin Gastroenterol 2006;22:361–4.
12. Namgung R, Mimouni F, Campaigne BN, Ho ML, Tsang RC. Lowbone mineral content in summer-born compared with winter-born infants. J Pediatr Gastroenterol Nutr 1992;15:285–8.
13. Namgung R, Tsang RC, Specker BL, Sierra RI, Ho ML. Low bonemineral content and high serum osteocalcin and 1,25-dihydrox-yvitamin D in summer- versus winter-born newborn infants: anearly fetal effect? J Pediatr Gastroenterol Nutr 1994;19:220–7.
14. Rucker D, Allan JA, Fick GH, Hanley DA. Vitamin D insufficiency in apopulation of healthy western Canadians. CMAJ 2002;166:1517–24.
15. Ulitsky A, Ananthakrishnan AN, Naik A, Skaros S, Zadvornova Y,Binion DG, et al. Vitamin D deficiency in patients with inflam-matory bowel disease: association with disease activity andquality of life. JPEN J Parenter Enteral Nutr 2011;35:308–16.
16. Gallo RL, Lai YP. AMPed up immunity: how antimicrobial pep-tides have multiple roles in immune defense. Trends Immunol2009;30:131–41.
17. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM. In-take of vitamin D and risk of type 1 diabetes: a birth-cohortstudy. Lancet 2001;358:1500–3.
18. Multiple Sclerosis Society Scotland. Shine on Scotland campaign.Article, 24 April 2011 http://www.mssocietyscotland.org.uk/news_and_whats_on/news_whats_on/shine_scot.html (accessed5 July 2011).
19. Munger KL, O'Reilly E, Ascherio A. Vitamin D intake and incidence ofmultiple sclerosis — reply from the authors. Neurology 2004;63:939.
20. Andjelkovic Z, Vojinovic J, Pejnovic N, Popovic M, Dujic A,Mitrovic D, et al. Disease modifying and immunomodulatory ef-fects of high dose 1 alpha (OH) D3 in rheumatoid arthritis pa-tients. Clin Exp Rheumatol 1999;17:453–6.
21. Jadad AR, Moore RA, Carroll D. Assessing the quality of reportsof randomized clinical trials: is blinding necessary? ControlClin Trials 1996;17:1–12.
22. Higgins JPT, Altman DG. Chapter 8: assessing risk of bias in in-cluded studies. In: Higgins J, Green S, editors. Cochrane Hand-book for Systematic Reviews of Interventions Version 5.0.0(updated February 2008); 2008. The Cochrane Collaboration.
23. Cantorna MT, Munsick C, Bemiss C, Mahon BD. 1,25-Dihydroxy-cholecalciferol prevents and ameliorates symptoms of experi-mental murine inflammatory bowel disease. J Nutr 2000;130:2648–52.
24. Daniel C, Radeke HH, Sartory NA, Zahn N, Zuegel U, Steinmeyer A,et al. The new low calcemic vitamin D analog 22-ene-25-oxa-vitamin D prominently ameliorates T helper cell type 1-mediatedcolitis in mice. J Pharmacol Exp Ther 2006;319:622–31.
25. Miheller P, Muzes G, Hritz I, Lakatos G, Pregun I, Lakatos PL,et al. Comparison of the effects of 1,25 dihydroxyvitamin Dand 25 hydroxyvitamin D on bone pathology and disease activityin Crohn's disease patients. Inflamm Bowel Dis 2009;15:1656–62.
26. Jorgensen SP, Agnholt J, GlerupH, Lyhne S, Villadsen GE, Hvas CL,et al. Clinical trial: vitamin D3 treatment in Crohn's disease — arandomized double-blind placebo-controlled study. AlimentPharmacol Ther 2010;32:377–83.
27. Harries AD, Brown R, Heatley RV, Williams LA, Woodhead S,Rhodes J. Vitamin D status in Crohn's disease: association withnutrition and disease activity. Gut 2007;26:1197–203.
28. Ginanjar E, Sumariyono, Setiati S, Setiyohadi B. Vitamin D andautoimmune disease. Acta Medica Indonesiana 1985;39:133–41.
29. Froicu M, Weaver V, Wynn TA, McDowell MA, Welsh JE, CantornaMT. A crucial role for the vitamin D receptor in experimental in-flammatory bowel diseases. Mol Endocrinol 2003;17:2386–92.
30. El-Matary W, Sikora S, Spady D. Bone mineral density, vitaminD, and disease activity in children newly diagnosed with inflam-matory bowel disease. Dig Dis Sci 2011;56:825–9.
31. Gilman J, Shanahan F, Cashman KD. Determinants of vitamin Dstatus in adult Crohn's disease patients, with particular emphasison supplemental vitamin D use. Eur J Clin Nutr 2006;60:889–96.
32. Leslie WD, Miller N, Rogala L, Bernstien CN. Vitamin D status andbone density in recently diagnosed inflammatory bowel disease:the Manitoba IBD Cohort Study. Am J Gastroenterol 2008;103:1451–9.
33. Stio M, Bonanomi AG, d'Albasio G, Treves C. Suppressive effectof 1,25-dihydroxyvitamin D3 and its analogues EB 1089 and KH1060 on T lymphocyte proliferation in active ulcerative colitis.Biochem Pharmacol 2001;61:365–71.
34. Cantorna M. Mechanisms underlying the effect of vitamin D onthe immune system. Proc Nutr Soc 2010;69:286–9.


















