Interrelationship between Iron deficiency Anaemia and Vit-D deficiency
Upload
nilesh-chandraCategory
view
333download
5description

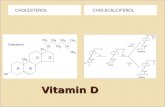
Vit D: Role in various
diseases
-Dr. Nilesh Chandra

Objectives:
Introduction
Synthesis
Actions
Diseases
Supplementation

Introduction
Not strictly a vitamin.
Only when sunlight exposure is inadequate is a dietary source required.
Main function is in the regulation of calcium absorption and homeostasis.
Most of its actions are mediated by way of nuclear receptors that regulate gene expression.

Introduction
Also has a role in regulating cell proliferation and differentiation.
Intakes considerably higher than are required to maintain calcium homeostasis reduce the risk of:◦ Insulin resistance
◦ Obesity
◦ The metabolic syndrome
◦ Various cancers.
Deficiency, leading to rickets in children and osteomalacia in adults.

Vitamin D Is Synthesized in the
Skin

Vitamin D Is Activated in Liver &
Kidney
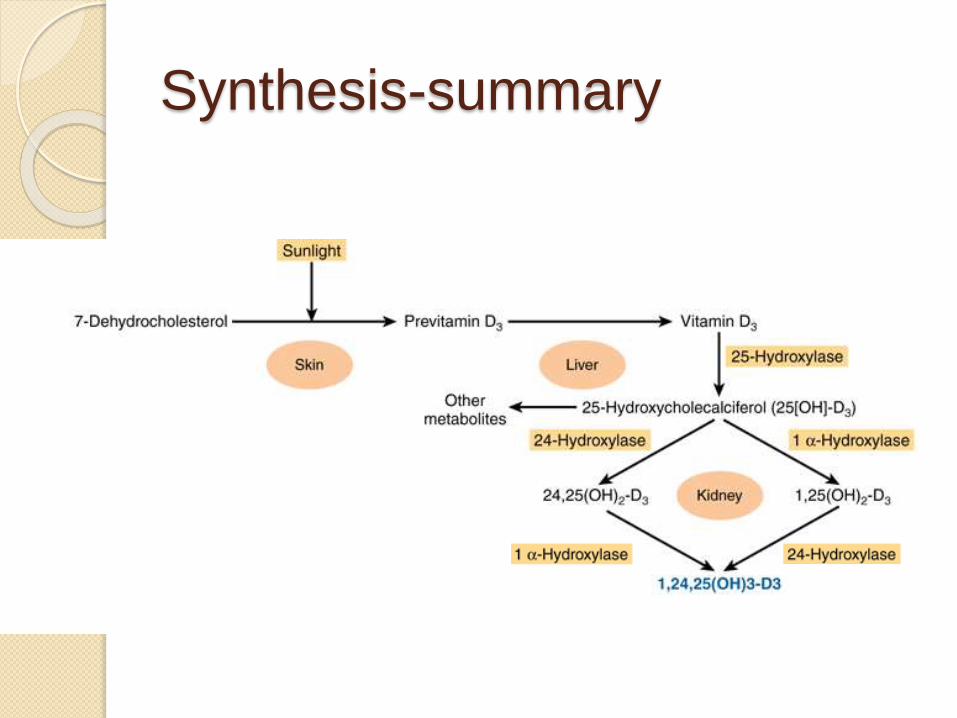
Synthesis-summary

Regulation
Calcitriol acts to reduce its own
synthesis by:
◦ inducing the 24-hydroxylase.
◦ repressing the 1-hydroxylase in the
kidney.
Other regulators are serum levels of:
◦ Phosphorus
◦ Calcium
◦ fibroblast growth factor 23 (FGF-23)
◦ parathormone (PTH)

Vit. D Receptor (VDR)
VDR: a transcription factor
Regulates expression of upto 2000
genes, directly or indirectly.
Membrane bound VDR postulated but
not yet proven.
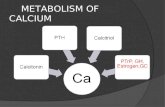
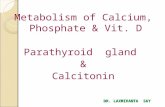
Role in calcium homeostasis
vitamin D maintains plasma calcium
concentration in three ways:
◦ it increases intestinal absorption of
calcium.
◦ it reduces excretion of calcium (by
stimulating resorption in the distal renal
tubules).
◦ it mobilizes bone mineral.

Other actions
calcitriol is also involved in:
◦ insulin secretion.
◦ synthesis and secretion of parathyroid
and thyroid hormones.
◦ inhibition of production of interleukin by
activated T-lymphocytes and of
immunoglobulin by activated B-
lymphocytes.
◦ differentiation of monocyte precursor
cells.
◦ modulation of cell proliferation.

Normal levels
Commonly, 25 (OH)D is measured.
Analyte Conventional
Unit
SI Unit
25(OH) D 10-65 ng/ml 25-162 nmol/L
1,25 (OH) D 15-60 pg/ml 36-144 pmol/L

Causes of Vit d deficiency
Inadequate exposure to sunlight.
Inadequate dietary vit D.
Vit D malabosrption.
Severe hepatocellular disease.
Increased catabolism (e.g. drugs).
Increased loss (nephrotic syndrome).
Vit D deficiency and bone morphology
Vitamin D sufficiency leads to an
adequate calcium-phosphorus product
(Ca2+ × HPO42−) resulting in an
effective bone mineralization.
Maternal vitamin D insufficiency during
pregnancy associated with a
significant reduction in bone mineral
acquisition in infants, persisting upto 9
years of age.

In children, vitamin D deficiency with
25(OH)D levels <15 ng/mL causes:
◦ chondrocyte disorganization.
◦ hypertrophy at the mineralization front.
◦ skeletal mineralization defects.
This results in bone deformities and short
stature, the typical signs of vitamin D
deficiency rickets.
Vit D deficiency and bone morphology

Sister (right) and
brother (left)
ages 4 years and
6.5 years,
respectively,
demonstrating
classic knock-
knees and bow
legs, growth
retardation, and
other skeletal
deformities

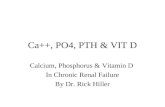
In adults low 25(OH)D and high PTH also lead to a low serum calcium ×phosphorus product.
Results in osteomalacia, i.e., a defective mineralization of the collagen matrix .
Causes a reduction of structural support.
Associated with an increased risk of fracture.
Vit D deficiency and bone morphology

A decrease in 25(OH)D leads to
secondary hyperparathyroidism.
Associated with osteoclastogenesis,
which leads to:
◦ an increase in bone resorption exceeding
osteoblast-mediated bone formation.
Can precipitate and exacerbate
osteopenia and osteoporosis in adults.
Vit D deficiency and bone morphology

Muscular health
Vitamin D deficiency is associated with:
◦ diffuse muscle pain.
◦ muscle weakness predominantly in the proximal muscle groups.
◦ a reduction in performance speed.
Vitamin D supplementation lowered the adjusted-incidence rate ratio of falls by 72% compared to those taking placebo over 5 months.

Protective role in
carcinogenesis 1,25(OH)2D inhibits carcinogenesis by
several mechanisms:
◦ promotes cyclin-dependent kinase (CDK)
inhibitor synthesis.
◦ influences several growth factors and their
signaling pathways including:
insulin-like growth factor 1 (IGF-1)
transforming growth factor β (TGFβ)
Wnt/β-catenin
MAP kinase 5 (MAPK5)
nuclear factor κB (NF-kB)

Beneficial effects on cardiovascular
risk factors and cardiovascular health
The vitamin D receptor is present in
endothelium, vascular smooth muscle, and
cardiomyocytes.
May protect against atherosclerosis
through:
◦ The inhibition of macrophage cholesterol uptake
and foam cell formation.
◦ reduced vascular smooth muscle cell
proliferation.
◦ reduced expression of adhesion molecules in
endothelial cells.
◦ inhibition of cytokine release from lymphocytes.

Protective role in Type II DM
vitamin D exerts various antidiabeticeffects.
The VDR is expressed in pancreatic beta cells and 1,25(OH)2D stimulates insulin secretion.
Improvement in vitamin D status also leads to a improvement of insulin sensitivity, mediated by upregulation of insulin receptors.
Vit D modulates inflammation, which is also thought to play a role in type 2 diabetes.
Additional benefits
Protective role has been found in:
◦ Autoimmune Disease:
Multiple Sclerosis
Type I DM
Rheumatoid Arthritis
◦ Infections, especially:
Tuberculosis
Influenza
Viral URTI
◦ Respiratory Diseases

A Schematic representation of the major causes for
vitamin D deficiency and potential health
consequences

A Schematic representation of the major causes for
vitamin D deficiency and potential health
consequences

Vit D supplementation
According to the Endocrine Society
Practice Guidelines:
Age Daily
supplementation
Safety limit
Upto 1 year 400–1000 IU up to 2000 IU
1-18 years 600–1000 IU up to 4000 IU
>18 years 1500–2000 IU up to 10,000 IU

Treatment of deficiency
According to the Endocrine Society Practice
Guidelines:
Age Initial therapy
for 6 weeks
Maintenance
Upto 1 year 2000 IU/day or 400–1000 IU/day
50,000 IU/wk
1-18 years 2000 IU/day or 600–1000 IU/day
50,000 IU/wk
>18 years ~6000 IU/day or 1500–2000
IU/day
50,000 IU/wk
(both for 8 wks)
In obese patients, patients with malabsorption syndromes,
and patients on medications affecting vitamin D
metabolism, two to three times higher doses are
recommended.

Summary
Vit D synthesis.
Actions and systems affected.
Effects of deficiency.
Treatment of deficiency.

References
Tietz Textbook of Clinical Chemistry
and Molecular Diagnosis, Fifth Edition.
Harper’s Illustrated Biochemistry, 29th
Edition.
Wacker,M and Holick, M.F . Vitamin
D—Effects on Skeletal and
Extraskeletal Health and the Need for
Supplementation. Nutrients. 2013
January; 5(1): 111–148.

THANK YOU!!