
Visualizing the Future: Technology Competency Development in Clinical Medicine, and Implications for...
11
Educational Assessment, Interventions, and Outcomes 480 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006 Visualizing the Future: Technology Competency Development in Clinical Medicine, and Implications for Medical Education Malathi Srinivasan, M.D., Craig R. Keenan, M.D., Joel Yager, M.D. Received February 2, 2006; revised May 1, 2006; accepted May 23, 2006. Drs. Srinivasan and Keenan are affiliated with the Department of Internal Medicine, University of California, Davis, Sacramento, California. Dr. Yager is affiliated with the Department of Psychiatry, University of New Mexico, Albuquerque, New Mexico. Address cor- respondence to Dr. Srinivasan, 2315 Stockton Boulevard, Sacra- mento, CA 95817; [email protected] (e-mail). Copyright 2006 Academic Psychiatry Objective: In this article, the authors ask three questions. First, what will physicians need to know in order to be effective in the future? Second, what role will technology play in achieving that high level of effectiveness? Third, what specific skill sets will phy- sicians need to master in order to become effective? Method: Through three case vignettes describing past, present, and potential future medical practices, the authors identify trends in major medical, technological and cultural shifts that will shape medical education and practice. Results: From these cases, the authors generate a series of tech- nology-related competencies and skill sets that physicians will need to remain leaders in the delivery of medical care. Physicians will choose how they will be end-users of technology, technology developers, and/or the interface between users and developers. These choices will guide the types of skills each physician will need to acquire. Finally, the authors explore the implications of these trends for medical educators, including the competencies that will be required of educators as they develop the medical curriculum. Conclusions: Examining historical and social trends, including how users adopt current and emerging technologies, allows us to anticipate changes in the practice of medicine. By considering market pressures, global trends and emerging technologies, medi- cal educators and practicing physicians may prepare themselves for the changes likely to occur in the medical curriculum and in the marketplace. Academic Psychiatry 2006; 30:480–490 T hinking about competencies related to current and emerging information technologies raises several in- teresting questions for physicians: What will they need to know about information technology in order to be effective in the future? What role will technology play in achieving high levels of effectiveness? And what specific skill sets will physicians require to achieve and maintain these levels of effectiveness? To address these questions, we paint the picture of a potential medical future, briefly outline emerging technol- ogies that will shape that future, and discuss how physi- cians may lead in the use of these technologies and, con- currently, expect to use them on a daily basis. We close by considering competencies related to medical technologies and their implications for clinical educators preparing learners for a new medical world. To quickly envision how technology has affectedmedical practice over the years, consider these brief scenarios re- garding the assessment and treatment of a mid-40s male with fever, chills, and a hacking cough. The Past, Circa 1890 A physician in a horse-drawn carriage arrives at the pa- tient’s home, summoned earlier in the day by the man’s wife, who sent her son on horseback to the physician’s of- fice several miles away. At the age of 40, the man is already approaching the end of his natural life but has now devel- oped a fever, chills, and a hacking cough. Physical exami- nation leads to the diagnosis of pneumonia, an often fatal condition. The physician prescribes a morphine tonic with alcohol to relieve the patient’s pain and dyspnea. He spends time comforting the distraught family who realizes that the patient may die. The physician will return the next day to the patient’s home. He creates a written patient record in his notebook and returns to his private hospital. Using his microscope, he sees the causative organism in
Transcript of Visualizing the Future: Technology Competency Development in Clinical Medicine, and Implications for...

Educational Assessment, Interventions, and Outcomes
480 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
Visualizing the Future:Technology Competency Development in Clinical Medicine,
and Implications for Medical Education
Malathi Srinivasan, M.D., Craig R. Keenan, M.D., Joel Yager, M.D.
Received February 2, 2006; revised May 1, 2006; accepted May 23,2006. Drs. Srinivasan and Keenan are affiliated with the Departmentof Internal Medicine, University of California, Davis, Sacramento,California. Dr. Yager is affiliated with the Department of Psychiatry,University of New Mexico, Albuquerque, New Mexico. Address cor-respondence to Dr. Srinivasan, 2315 Stockton Boulevard, Sacra-mento, CA 95817; [email protected] (e-mail).
Copyright � 2006 Academic Psychiatry
Objective: In this article, the authors ask three questions. First,what will physicians need to know in order to be effective in thefuture? Second, what role will technology play in achieving thathigh level of effectiveness? Third, what specific skill sets will phy-sicians need to master in order to become effective?
Method: Through three case vignettes describing past, present,and potential future medical practices, the authors identify trendsin major medical, technological and cultural shifts that willshape medical education and practice.
Results: From these cases, the authors generate a series of tech-nology-related competencies and skill sets that physicians willneed to remain leaders in the delivery of medical care. Physicianswill choose how they will be end-users of technology, technologydevelopers, and/or the interface between users and developers.These choices will guide the types of skills each physician willneed to acquire. Finally, the authors explore the implications ofthese trends for medical educators, including the competenciesthat will be required of educators as they develop the medicalcurriculum.
Conclusions: Examining historical and social trends, includinghow users adopt current and emerging technologies, allows us toanticipate changes in the practice of medicine. By consideringmarket pressures, global trends and emerging technologies, medi-cal educators and practicing physicians may prepare themselvesfor the changes likely to occur in the medical curriculum and inthe marketplace.
Academic Psychiatry 2006; 30:480–490
Thinking about competencies related to current andemerging information technologies raises several in-
teresting questions for physicians: What will they need toknow about information technology in order to be effectivein the future? What role will technology play in achievinghigh levels of effectiveness? And what specific skill sets willphysicians require to achieve and maintain these levels ofeffectiveness?
To address these questions, we paint the picture of apotential medical future, briefly outline emerging technol-ogies that will shape that future, and discuss how physi-cians may lead in the use of these technologies and, con-currently, expect to use them on a daily basis. We close byconsidering competencies related to medical technologiesand their implications for clinical educators preparinglearners for a new medical world.
To quickly envision how technology has affected medicalpractice over the years, consider these brief scenarios re-garding the assessment and treatment of a mid-40s malewith fever, chills, and a hacking cough.
The Past, Circa 1890
A physician in a horse-drawn carriage arrives at the pa-tient’s home, summoned earlier in the day by the man’swife, who sent her son on horseback to the physician’s of-fice several miles away. At the age of 40, the man is alreadyapproaching the end of his natural life but has now devel-oped a fever, chills, and a hacking cough. Physical exami-nation leads to the diagnosis of pneumonia, an often fatalcondition. The physician prescribes a morphine tonic withalcohol to relieve the patient’s pain and dyspnea. Hespends time comforting the distraught family who realizesthat the patient may die. The physician will return the nextday to the patient’s home. He creates a written patientrecord in his notebook and returns to his private hospital.Using his microscope, he sees the causative organism in

SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 481
the patient’s sputum sample. Therapeutic options are lim-ited. The physician looks through his few books on medi-cine and surgery and discusses the case with a colleaguedown the street.
The Present, Circa 2006
In his urgent care clinic, a physician sees the patient,whom he has never met, for fever, chills, and a hackingcough. The man is in the prime of his life—mid-40s witha young family. He has traveled about 20 miles by car forthis appointment, driven by his wife. The physician logsonto the hospital’s electronic medical record system andquickly reviews prior appointments and laboratory results.After diagnosing pneumonia on the basis of a quickly ob-tained chest X-ray, the physician prescribes antimicrobialagents to be picked up at the local pharmacy. The patient’swife asks about resistant bacteria and further instructionsfor care. Using the in-room desktop computer, the physi-cian does a quick online search for local bacterial resis-tance patterns and prints out current information from aproprietary medical database. The physician asks the pa-tient to call his nurse the next day. If the patient fails toimprove, he is instructed to return to the office for re-evaluation and possible hospital admission.
The Near Future, Circa 2025
A physician on call in his office in India receives a video-conference call from a patient suffering from fever, chills,and a hacking cough. The patient, located 8,500 miles awayin his local med-terminal, is a member of an internationalhealth network. In his mid-40s, he is a young man withanother 60 to 70 years of life ahead of him. The physicianpulls up the patient’s records from his computer terminal.With the patient in the med-terminal, the physician per-forms a noninvasive MRI-like scan remotely and diagnosespneumonia. Vital signs are taken automatically by meansof pressure gauges. The patient enters a biometric accesscode to allow the physician to obtain his pharmaco-ge-nomic profile from an embedded microchip to begin coun-seling. The patient’s personal digital assistant captures keywords of their conversation via voice recognition softwareand displays pertinent patient-related information for thepatient to view synchronously. The physician prescribes along-acting antibiotic, which the patient receives on-sitefrom an injection terminal. His counseling is complete af-ter the patient receives standardized information from amedical database about self-care. The patient uses a con-tinuous home monitoring device (pulse, blood pressure,
oxygenation), which routes his vital signs to the local phy-sician network to monitor trends and complications. If thepatient’s vital signs fall below acceptable parameters, anambulance network will be automatically notified and hewill be transported to a local hospital for reevaluation andadditional therapy. The Indian physician does a quick lit-erature search on aspects of caring for American patientswith pneumonia and enters his thoughts and lessonslearned into a learning portfolio for his own CME credit.The patient completes his customer satisfaction form onthe insurance company’s Web site in order to receive hisparticipation bonus of a reduced copayment.
This view of the future simply extends already existingmajor medical trends that represent market force pres-sures for cost containment (1, 2), globalization/outsourcing(3–6), and data consolidation (7–11). Another equallyplausible view of the medical future might envision betterpersonal relationships between patients and their physi-cians (12, 13), using local coverage networks and personalcommunications modalities (e.g., next evolution of e-mail,home monitoring) to allow longitudinal and home-basedinteractions. Optimists might even imagine that doctorsmight make home visits (14–16) because their patient poolhas become smaller due to their negotiated rates increas-ing and with risk pools shared across demographic groups.
The major fallacy of trying to predict a medical futurebased on present technologies or current social/economic/political trends is that major shifts are difficult to antici-pate. For instance, while functional nanotechnology andincreased domestic terrorism are recognized as near-fu-ture possibilities, the next major paradigm shift is as yetunknown. These shifts (such as Internet-based shared net-works, massive inexpensive computing power, ease of in-ternational travel, changing unemployment) have a dra-matic impact on the medical horizon in unpredictable,nonlinear ways.
Even with these uncertainties, educators are obliged toprepare their learners for near- and far-future practice sce-narios. They need to consider critical elements embeddedin these known trends, and devise strategies to help learn-ers meet those needs. Similarly, examining critical aspectsof those scenarios (Appendix 1) allows us to describe thespectrum of competencies that physicians may need to de-velop. Foreseeable major trends in medicine include:
• CommunicationEvolution of the doctor-patient relationship into amore client-supplier model (17, 18).Greater emphasis on patient responsibility forhealth (19).

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
482 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
• Information managementAvailability of high quality, transparent medical in-formation for the lay public (20, 21).Internationally available patient medical/pharmacyrecords (22, 23).Stringent new privacy standards, with biometric andother coded data schemas (24–27).User-friendly, decentralized continual education,tailored to individual practices (28).Emphasis on self-directed learning and continuingself-education (29–31).
• DiagnosisDevelopment of pharmocogenomic profiles for in-dividual patients (32–35).Inexpensive high-quality imaging techniques forclinic use (36).Creation of better home monitoring equipment forself/system management (37, 38).
• TherapyInformation management systems for physicianeducation and practice-based updates (39).Compilation of individual patient health statisticsinto searchable databases (40).Testing of complementary, alternative and tradi-tional/local medical practices (41, 42).Increasing emphasis on nonallopathic practice andancillary practitioners (43, 44).
• Quality control and locationDecentralization of medical care via telemedicinetechnologies (45, 46).International standards for medical practice, “in-ternationalizing” medicine (47, 48).Medical outsourcing to other countries for non-emergent treatment (49, 50).
Likelihood of Technology Adoptionby Physicians and Society
In medicine and the rest of society, the rate of technol-ogy introduction and adoption has been rapid. Enhancedcompetency by physicians may be directly related to tech-nology adoption. The incorporation of new technology inmedical practice is influenced by four strong forces, thefour “As,” which are driving pressures toward greater ef-ficiencies and effectiveness in medical care: accessibility,affordability, accountability, and affability (Appendix 2).These driving pressures are fluid and change over time for
any given technology. For example, as more competitorstry to develop similar products (such as Internet accessproviders [AOL, Comcast, telecom companies]), the tech-nologies will decrease in price (affordability). This de-crease in price and increase in manufacturing/distributionwill increase the consumer’s access to the technology. Witheach iteration, the consumer will find the technology easierto use and more functional (affability). Physicians will berequired to critically assess the cost-benefit-harm-limita-tions for each new technological tool and be accountablefor the use and results of the technologies in practice.
Physician Role Adoption and CompetencyDevelopment
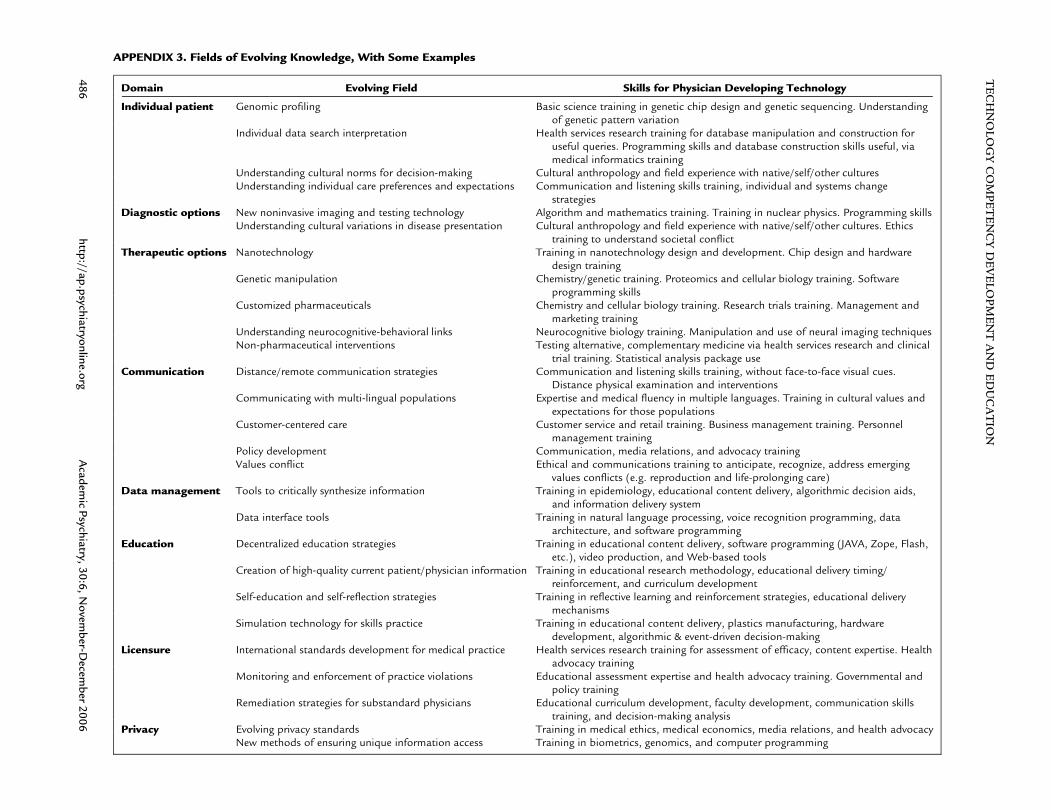
In preparation for this future, physicians will have todecide how involved they will want to be with emergingmedical technologies. Some will elect to remain “end-users” of technology, whereas others will participate in de-veloping and evolving those technologies or will interfacebetween the developers and the end-users (Appendix 3).Physicians who are on the development end of technologywill, of course, need to develop specialized expertise inthose technologies: affecting communication, diagnosticand therapeutic options, data management, self-educationstrategies and other constantly changing areas.
These major trends will have significant implications forphysician training and competency development (51, 52).As with other professionals, all physicians will be requiredto become “technology literate”—understanding how touse basic software programs, communication/e-mail pro-grams, messaging systems, common organizers, commonpresentation-related hardware. Psychiatrists, for example,might be expected to acquire skills for interacting with re-mote patients via teleconferencing (tele-psychiatry) (53).Most of these technologies currently exist and are alreadybeing used in tele-consultation. Physicians who bridge twoassociated fields of medicine (e.g., electronic medical rec-ord development) and medical practitioners will requirefamiliarity with practice patterns/usage in the associatedfields. As physicians seek additional leadership opportu-nities, those who are dually trained will enjoy competitiveadvantages in the medical marketplace, where obtainingand disseminating medical information will become in-creasingly simple. Medical informatics, the field of man-aging and interfacing with medical information, will com-prise only a subset of the total types of skills that dualcompetency physicians may acquire.

SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 483
Implications for Medical Training
Future medical school selection committees may be in-creasingly inclined to recruit physician leaders who bringsubstantial experiences outside of medicine to their medi-cal education. Because of the increasingly rapid expansionand evolution of the knowledge base, students will need tospend more time learning to assess data critically. Withubiquitous information access, the amount of basic knowl-edge that physicians will need to memorize may decrease.They will also require skills in new ways of communicatingwith their patients via remote means. These shifts may en-courage some physicians to spend more time than in thepast understanding the systems and social implications ofpractice (health economics, health disparities, evidence as-sessment, research training, epidemiology).
Currently, the competencies outlined by the ACGME(54) are flexible enough to allow incorporation of the tech-nology-related skills into a standard residency training pro-gram. Educators will be faced with an even more compli-cated task: keeping their core curriculum (e.g.,pathophysiology) stable while incorporating new infor-mation at a reasonable pace. In Appendix 4, we havemapped a few very basic technology-related competenciesfor the end-user physician, who may have minimal inputinto technology development. Educators will need to con-sider core skill sets for each user type from a competencyperspective. Since many of the core skills affect the differ-ent areas of medical practice, educators will need to care-fully consider how “stacked” they want their competencygrids to appear.
Medical educators will be faced with the even morecomplicated tasks of retaining their fundamental core cur-riculum requirements (e.g., pathophysiology) while incor-porating new information at a reasonable pace. Traditionalmedical education models are already challenged, as medi-
cal students already acquire and assimilate knowledge viatheir wireless laptops and PDAs during classes, seminars,and at the bedside. Inexpensive, high-quality digital videorecording technologies allow easy demonstration of best/worst communication and clinical skills practices in class-rooms. As high quality core curricula become universallyavailable through the Web, educators will have to deter-mine the best use of classroom time—how much time tospend to deliver core content and/or using a small groupsetting to assess learner understanding and push skills incontent application. Each of the specific competencies thateducators will instruct or encourage will entail knowledge,skills, attitudes, and habits. Some competencies related tothe incorporation of these technologies into a medical ed-ucator’s practice are detailed in Appendix 5.
Conclusions
Cultural and technological shifts often provoke anxietyabout a loss of values or autonomy while simultaneouslyprovoking excitement about new opportunities. The prac-tice of medicine is evolving quickly, and global trends inthe marketplace place pressure to reduce cost while in-creasing quality. The American physician of the future willface international competition, and all competitors will beequipped with powerful new tools for patient care, datamanagement, and communication. Examining these majortrends can help educators understand the new technolog-ical competencies that will be required of physicians.Medical education itself will evolve in learner selection,content, and methods. Physician leaders in education willhelp guide the appropriate implementation of medicaltechnologies in practice, fostering practices that use tech-nology to increase accessible, affordable, accountable, andaffable medical care.

TE
CH
NO
LOG
YC
OM
PET
EN
CY
DE
VE
LOPM
EN
TA
ND
ED
UC
AT
ION
484http://ap.psychiatryonline.org
Academ
icPsychiatry,30:6,N
ovember-D
ecember
2006
APPENDIX 1.
Past Present Near Future
Characteristic CommunicationPatient role Passive, little medical knowledge Participatory Participatory, perhaps directivePhysician role Directive Directive or participatory Customer service orientation predominates.
Competition increases for patient rosterPatient-physician
relationshipKnown each other intimately over time Relationship is local, but physician may not know
patientRelationship decentralized, international. Physician
may not know patientFamily role Caregivers for all patient needs When patient significantly ill, most care delivered
in the hospitalSignificant caregiving, since much medical care is
transferred to the homeDiagnosisDiagnostic options Limited to history, physical, and microscopic
examinationNon-invasive diagnostics done in specific
departments, not in physician’s direct officeNon-invasive diagnostics available at point of
interaction (terminals, offices, etc.). Homemonitoring with health-system interface
TherapyTherapeutic options Surgery, analgesics, herbal tinctures,
compounds, comfortTherapeutic options based on patient
demographics (age, smoking, ethnicity)Customized therapeutic options based on
patient’s individual genomic profileEvidence base Anecdotal medicine, case series, ‘‘eminence-
based medicine’’Evidence-based, from population-based
therapeutic outcomes dataPopulation and individual probabilistic outcomes
from international outcomes databasesInformation ManagementPatient records Individual clinic notes kept by physician Local data networks increase. Moderate privacy
standardsInternationally available records, with stringent
privacy standardsPatient outcomes
(positive, nochange, adverse)
Noted by physician, patient, and family Noted by physician, patient, and family. Adverseoutcomes tracked by health system
Patient outcomes automatically entered intointernational databases. Monitoring allowsearly adverse outcomes alerts
Medicalinformation
Learned in medical school, few updates Learned in medical school and residency programsPeriodic updates
Point of service information delivery. Informationdelivery simultaneously to patient andphysician
Continuing EducationPhysician’s
continuingeducation
Not much change since medical school. Text-based learning. Opinion leader discussions
Recertification every 5 to 10 years, with state-mandated education hours for licensure.Education is sporadic and idiosyncratic
Continual certification, each patient as acertification case. Reflection-based portfoliosystems linked to CME. Information systemsmanage CME and physician time
Physician outcomes Medical knowledge Medical knowledge, some procedural/communication skills
Medical knowledge, skills, attitudes, habits, self-reflection
Professionalinteractions
Local physicians, limited conferences Local and national meetings. Mainly localinteractions with colleagues
Virtual meetings internationally, supplementary in-person meetings

SRIN
IVA
SAN
ETA
L.
Academ
icPsychiatry,30:6,N
ovember-D
ecember
2006http://ap.psychiatryonline.org
485
Quality Control and LocationLocation Patient’s home, perhaps hospital or office Physician clinic or hospital. Geographically close Physician and patient geographically distant.
Outsourcing if non-urgentExpertise Local. Walking, horse, cart or driving distance Regional/national. Limited by time and budget
(flights)International. Telemedicine predominates when
local availability/expertise limitedAccreditation By medical schools, when certification
availableState/national organizations accredit/license
individuals, groups, hospitals, medical schoolsInternational organizations. Once quality
standards are met, practices gain access toprosperous markets
Medical EconomicsPayment Negotiated based on patient resources, often
individually bargainedInsured patients have small co-pays. Government/
safety net hospitals absorb cost for poor. Un/underinsured pay heavily
Patients may choose from catastrophic healthinsurance to complete medical coverage. Co-payment varies with patient health prevention
Insurance None Employer-based insurance, negotiated healthplans. Government insures some poor/elderly
Risk pool spread across all populations. Nationalor international health consortium and scaledrates for socio-economic status
Performancestandards
None Large practices receive increased payments to meetcrude quality standards. Minor risk adjustmentfor patient factors
Health information systems facilitate meetinginternational practice standards. Sophisticatedrisk adjustment. Best practices incentives
APPENDIX 2. Critical Characteristics of Medically-Related Technologies Influencing the Likelihood for Adoption by Medical Profession and Society
Competencies Related to Use of . . . Accessibility Accountability Affordability Affability
Laptop computers and standard software � � � �LCD projectors and presentation software � � � �Pocket information organizers � � � �Internet—information utilization � � � �Learning portfolios � � �Decision algorithms � �Distance consultations via videocam/videophone � � �Patient simulators: mega-codes � �Patient simulators: cardiac catheterizations � �Patient simulators: computer-based virtual schizophrenia patients �Voice recognition software � � � �Distance surgery �Biometric privacy modalities (retinal, fingerprint scans) �Non-invasive functional imaging (fMRI, PET, etc.) � �Nanotechnology intervention
TE
CH
NO
LOG
YC
OM
PET
EN
CY
DE
VE
LOPM
EN
TA
ND
ED
UC
AT
ION
486http://ap.psychiatryonline.org
Academ
icPsychiatry,30:6,N
ovember-D
ecember
2006
APPENDIX 3. Fields of Evolving Knowledge, With Some Examples
Domain Evolving Field Skills for Physician Developing Technology
Individual patient Genomic profiling Basic science training in genetic chip design and genetic sequencing. Understandingof genetic pattern variation
Individual data search interpretation Health services research training for database manipulation and construction foruseful queries. Programming skills and database construction skills useful, viamedical informatics training
Understanding cultural norms for decision-making Cultural anthropology and field experience with native/self/other culturesUnderstanding individual care preferences and expectations Communication and listening skills training, individual and systems change
strategiesDiagnostic options New noninvasive imaging and testing technology Algorithm and mathematics training. Training in nuclear physics. Programming skills
Understanding cultural variations in disease presentation Cultural anthropology and field experience with native/self/other cultures. Ethicstraining to understand societal conflict
Therapeutic options Nanotechnology Training in nanotechnology design and development. Chip design and hardwaredesign training
Genetic manipulation Chemistry/genetic training. Proteomics and cellular biology training. Softwareprogramming skills
Customized pharmaceuticals Chemistry and cellular biology training. Research trials training. Management andmarketing training
Understanding neurocognitive-behavioral links Neurocognitive biology training. Manipulation and use of neural imaging techniquesNon-pharmaceutical interventions Testing alternative, complementary medicine via health services research and clinical
trial training. Statistical analysis package useCommunication Distance/remote communication strategies Communication and listening skills training, without face-to-face visual cues.
Distance physical examination and interventionsCommunicating with multi-lingual populations Expertise and medical fluency in multiple languages. Training in cultural values and
expectations for those populationsCustomer-centered care Customer service and retail training. Business management training. Personnel
management trainingPolicy development Communication, media relations, and advocacy trainingValues conflict Ethical and communications training to anticipate, recognize, address emerging
values conflicts (e.g. reproduction and life-prolonging care)Data management Tools to critically synthesize information Training in epidemiology, educational content delivery, algorithmic decision aids,
and information delivery systemData interface tools Training in natural language processing, voice recognition programming, data
architecture, and software programmingEducation Decentralized education strategies Training in educational content delivery, software programming (JAVA, Zope, Flash,
etc.), video production, and Web-based toolsCreation of high-quality current patient/physician information Training in educational research methodology, educational delivery timing/
reinforcement, and curriculum developmentSelf-education and self-reflection strategies Training in reflective learning and reinforcement strategies, educational delivery
mechanismsSimulation technology for skills practice Training in educational content delivery, plastics manufacturing, hardware
development, algorithmic & event-driven decision-makingLicensure International standards development for medical practice Health services research training for assessment of efficacy, content expertise. Health
advocacy trainingMonitoring and enforcement of practice violations Educational assessment expertise and health advocacy training. Governmental and
policy trainingRemediation strategies for substandard physicians Educational curriculum development, faculty development, communication skills
training, and decision-making analysisPrivacy Evolving privacy standards Training in medical ethics, medical economics, media relations, and health advocacy
New methods of ensuring unique information access Training in biometrics, genomics, and computer programming

SRIN
IVA
SAN
ETA
L.
Academ
icPsychiatry,30:6,N
ovember-D
ecember
2006http://ap.psychiatryonline.org
487
APPENDIX 4. Relationship of Some Technology-Related Competencies to ACGME Core Competencies
ACGME Competencies
BASIC Computer and Informatics CompetenciesPatient
CareMedical
KnowledgePractice-Based
LearningInterpersonal
Communication ProfessionalismSystems-Based
Practice
Computer operation skillsDemonstrate ability to use computers, storage/back-up
(e.g., hard disk, flash drives, CD/DVD), and relevantsoftware � �
Use common peripherals, including scanners, projectors,organizers, biometrics, simulators, tele-medicine units � �
Software application competenciesWord processor skills – start, write, save, print. Use
special manuscript features (e.g., tracking, insertcomment, references) � �
Graphing and spreadsheet programs (e.g., Excel): createand use graphs, spreadsheets, and databases � �
Project management software � � � �Voice recognition software � � � �Electronic medical record use � � � � � �Software development competenciesUse of natural language processing tools � �Development of information database architecture � �Utilization, testing, and feedback of user interfaces � �Communications utilization competenciesInternet: Locate, evaluate, and select resources for
personal life-long learning and patient education � � � �E-mail and list-servs � � � � � �Videophone/videocam � � � �

TE
CH
NO
LOG
YC
OM
PET
EN
CY
DE
VE
LOPM
EN
TA
ND
ED
UC
AT
ION
488http://ap.psychiatryonline.org
Academ
icPsychiatry,30:6,N
ovember-D
ecember
2006
APPENDIX 5. Competencies Related to Use of Technology in Medical Education and Patient Education
Developing Educational MaterialBasic Knowledge: The educator should be able to describe and discuss:
Characteristics, strengths, and weaknesses of different media, including available media communication resourcesSocial, legal and ethical issues related to technology use (fair use, copyrights, accessibility, HIPAA, etc.)Role of technology/media in application of core educational principles (e.g., adult learning)
Skills: The educator should be able to:Develop, maintain, and modify a Web pageProduce electronic slides/overheads using PowerPoint or similar programs to create stills, insert videoclipsOperate basic media-related technology: video recorder/player, digital cameras, monitor/TV, LCD projectors, computer, etc.Edit voice/video files, provide high quality videos and graphicsUse these skills to produce integrated multimedia presentations, including non-linear hypermedia presentationsProduce print-based products using desktop publishing
Curriculum DevelopmentThe educator should be able to:
Identify target audience, learner needs, appropriate curricular goals, resources for curricular development/implementationDevelop creative and useful learning experiences, using media to present material in a comprehensible mannerLocate, evaluate, and select resources/material (digital information, local experts, primary documents/artifacts, text, etc.)Use technology in the discipline/subject for learning and external communicationUse technology to facilitate teaching strategies specific to the disciplineDevelop physical settings and organizational and management strategies that support active student inquiry and collaborationIncorporate media and technology for teaching where appropriate, and support learner expression in a variety of media
Educational AssessmentThe educator should be able to:
Create study designs that allow development and testing of educational hypothesisRigorously analyze data from studies for effectiveness of interventionsDemonstrate effectiveness of learning modalityDevelop performance tasks for students to locate/analyze information, synthesize, and apply information in new contextsDevelop needs assessments using tools, such as SurveyMonkeyUse appropriate technologies effectively to collect information on student learning, using a variety of methods
Dissemination of Education MaterialsCreate sustainable systems of change within institutions and nationsDevelop on-line e-learning courses using formats such as WebCT, Angel, etc.Establish on-line conferences via WebDevelop interactive Web-based curriculumDevelop and provide feedback on learning portfoliosPresent material at national educator and patient care conferencesUse media to disseminate appropriate educational material to policy makers
Some data adapted from standards developed for educators in North Carolina (tps.dpi.state.nc.us/standards.html)

SRINIVASAN ET AL.
Academic Psychiatry, 30:6, November-December 2006 http://ap.psychiatryonline.org 489
References
1. Scanlon WJ: The future of Medicare hospital payment.Health Affairs 2006; 25:70–80
2. Cromwell J, Drozd EM, Gage B, et al: Variation in patientroutine costliness in U.S. psychiatric facilities. J Ment HealthPolicy Econ 2005; 8:15–28
3. Capko J: Outsourcing: friend or foe? J Med Pract Manage2005; 21:67–71
4. Ghods AJ, Nasrollahzadeh D: Transplant tourism and the Ira-nian model of renal transplantation program: ethical consid-erations. Exp Clin Transplant 2005; 3:351–354
5. Available at http://www.medical-tourism-india.com. AccessedJan 20, 2006
6. Available at http://www.outsourceoperation.com. AccessedJan 20, 2006
7. Kleinke JD: Release 0.0: clinical information technology inthe real world. Health Aff 1998; 17:23–38
8. Kaushal R, Bates DW, Poon EG, et al: Functional gaps inattaining a national health information network: what will ittake to get there in five years? Health Aff 2005; 24:1281–1289
9. Coile RC Jr: The digital transformation of health care. Phy-sician Exec 2000; 26:8–15
10. Forkner-Dunn J: Internet-based patient self-care: the nextgeneration of health care delivery. J Med Internet Res 2003;5:e8
11. Murray E, Lo B, Pollack L, et al: The impact of health infor-mation on the Internet on health care and the physician-pa-tient relationship: national U.S. survey among 1,050 U.S. phy-sicians. J Med Internet Res 2003; 5:e17.
12. Maisels MJ, Kring EA: A simple approach to improving pa-tient satisfaction. Clin Pediatr 2005; 44:797–800
13. Bezold C: The future of patient-centered care: scenarios, vi-sions, and audacious goals. J Altern Complement Med 2005;11:S77–84
14. Alexander GC, Kurlander J, Wynia MK: Physicians in retainer(“concierge”) practice: a national survey of physician, patient,and practice characteristics. J Gen Intern Med 2005; 20:1079–1083
15. Marsh AG: A curious 21st century phenomenon: physiciansreviving the house call. Caring 2005; 24:12–16, 18–22, 24
16. Meyer GS, Gibbons RV: House calls to the elderly—a vanish-ing practice among physicians. N Engl J Med 1997; 337:1815–1820
17. Will consumerism lead to better health? Lancet 2005; 366:34318. Robinson JC: Managed consumerism in health care. Health
Aff 2005; 24:1478–148919. Kubiak T, Hermanns N, Schreckling HJ, et al: Evaluation of
a self-management-based patient education program for thetreatment and prevention of hypoglycemia-related problemsin type 1 diabetes. Patient Educ Couns 2006; 60:228–234
20. Murray E, Lo B, Pollack L, et al: The impact of health in-formation on the internet on the physician-patient relation-ship: patient perceptions. Arch Intern Med 2003; 163:1727–1734
21. Baker L, Wagner TH, Singer S, et al: Use of the Internet and
e-mail for health care information: results from a nationalsurvey. JAMA 2003; 289:2400–2406
22. Shortliffe EH: The evolution of electronic medical records.Acad Med 1999; 74:414–419
23. Katehakis DG, Sfakianakis S, Tsiknakis M, et al: An infra-structure for Integrated Electronic Health Record services:the role of XML (Extensible Markup Language). J Med In-ternet Res 2001; 3:e7
24. Hashiyada M: Development of biometric DNA ink for au-thentication security. Tohoku J Exp Med 2004; 204:109–117
25. Pothen DJ, Parmanto B: Biometric authentication: privacyprotection or invasion? J AHIMA 2001; 72:24, 26
26. Woodward JD: Biometric scanning, law & policy: identifyingthe concerns–drafting the biometric blueprint. Univ PittsbgLaw Rev 1997; 59:97–155
27. Garner JC: Final HIPAA security regulations: a review.Manag Care Q 2003; 11:15–27
28. Allison JJ, Kiefe CI, Wall T, et al: Multicomponent Internetcontinuing medical education to promote chlamydia screen-ing. Am J Prev Med 2005; 28:285–290
29. Mandel LS, Goff BA, Lentz GM: Self-assessment of residentsurgical skills: is it feasible? Am J Obstet Gynecol 2005;193:1817–1822
30. Hiramanek N: Self-directed learning and continuing medicaleducation. Aust Fam Physician 2005; 34:879–880
31. Mamary E, Charles P: Promoting self-directed learning forcontinuing medical education. Med Teach 2003; 25:188–190
32. Ginsburg GS, Donahue MP, Newby LK: Prospects for per-sonalized cardiovascular medicine: the impact of genomics. JAm Coll Cardiol 2005; 46:1615–1627
33. Cacabelos R, Fernandez-Novoa L, Corzo L, et al: Genomicsand phenotypic profiles in dementia: implications for phar-macological treatment. Methods Find Exp Clin Pharmacol2004; 26:421–444
34. Ross JS, Schenkein DP, Kashala O, et al: Pharmacogenomics.Adv Anat Pathol 2004;11:211–220
35. Mancama D, Arranz MJ, Kerwin RW: Pharmacogenomics ofpsychiatric drug treatment. Curr Opin Mol Ther 2003; 5:642–649
36. Kobal SL, Atar S, Siegel RJ: Hand-carried ultrasound im-proves the bedside cardiovascular examination. Chest 2004;126:693–701
37. Schlaeper C, Diaz-Buxo JA: Home hemodialysis and remotemonitoring: current technology, requirements and capabili-ties. Blood Purif 2005; 23:18–22
38. Celis H, Den Hond E, Staessen JA: Self-measurement ofblood pressure at home in the management of hypertension.Clin Med Res 2005; 3:19–26
39. Duque G, Finkelstein A, Roberts A, et al: Learning whileevaluating: the use of an electronic evaluation portfolio in ageriatric medicine clerkship. BMC Med Educ 2006; 6:4
40. Joosse P, Goslings JC, Luitse JS, et al: M-study: arguments forregional trauma databases. J Trauma 2005; 58:1272–1276; dis-cussion 1277
41. Kennedy J: Herb and supplement use in the US adult popu-lation. Clin Ther 2005; 27:1847–1858

TECHNOLOGY COMPETENCY DEVELOPMENT AND EDUCATION
490 http://ap.psychiatryonline.org Academic Psychiatry, 30:6, November-December 2006
42. Harle L, Brown T, Laheru D, et al: Omega-3: fatty acids forthe treatment of cancer cachexia: issues in designing clinicaltrials of dietary supplements. J Altern Complement Med2005; 11:1039–1046
43. Ruggie M: Mainstreaming complementary therapies: new di-rections in health care. Health Aff (Millwood) 2005; 24:980–990
44. Sierpina VS, Frenkel MA: Acupuncture: a clinical review.South Med J 2005; 98:330–337
45. Harnett B: Telemedicine systems and telecommunications. JTelemed Telecare 2006; 12:4–15
46. Senapati S, Advincula AP: Telemedicine and robotics: pavingthe way to the globalization of surgery. Int J Gynaecol Obstet2005; 91:210–216.
47. Fernandez RD, Hebert GJ: Global licensure: new modalitiesof treatment and care require the development of new struc-tures and systems to access care. Nurs Adm Q 2004; 28:129–132
48. Paine L, Deshpande R, Margolis JD, et al: Up to code: does
your company’s conduct meet world-class standards? HarvBus Rev 2005; 83:122–133, 154
49. Segouin C, Hodges B, Brechat PH: Globalization in healthcare: is international standardization of quality a step towardoutsourcing? Int J Qual Health Care 2005; 17:277–279
50. Spiegel JM, Labonte R, Ostry AS: Understanding “globali-zation” as a determinant of health determinants: a critical per-spective. J Occup Environ Health 2004; 10:360–367
51. Yager J: The future of psychiatry, in Encyclopedia of the Fu-ture. Edited by Kurian GT, Molitor GTT. Mcmillan, 1995
52. Robinowitz CB, Yager J: The future of psychiatric education,in Annual Review of Psychiatry, volume 15. Edited by Dick-stein LJ, Riba MB, Oldham JM. Arlington, Va, American Psy-chiatric Publishing, 1996, pp 581–604
53. Hilty DM, Marks SL, Urness D, et al: Clinical and educationalapplications of telepsychiatry: a review. Can J Psychiatry 2004;49:12–23
54. Available at http://www.acgme.org/Outcome. Accessed Janu-ary 15, 2006.


















