Visual Disability Inventory: Documenting Functional Impairment Caused by Cataract
2
surgery. OccasionaIly, surgery is continued, at the risk of complications, possibly beyond control at this stage, although an urgent canthotomy may temper the loss. Such subtle bleeding is further proved by lid ecchymosis later 4 ; (2) minor oozing - that is revealed only in the first dressing as it reaches the skin. Although it raises no problem intraoperatively, it may cause postoperative anxiety, so that lid ecchymosis mandates explanation and reassurance. 3 This wider spectrum of slow imperceptible retro- bulbar hemorrhages that is more serious than the early ones which postpone surgery is weIl asserted by three respondents. Dr. Olander says, "The classic presentation of retrobulbar hemorrhage is seen less often than subclinical hemorrhage (which) makes surgery harder with difficulty in exposure, increased pressure on the vitreous .. . . " Likewise, Drs. Wallace and Fechner report postoperative lid ecchy- mosis as "disconcerting sequelae." In view of the relative frequency of such subtle hemorrhages, we must be alert throughout the entire procedure for their possible late build-up that could then chal- lenge all skills. If surgery is postponed, I prefer general anes- thesia,5.6 also for its advantage of inducing hypo- capnea when urgently needed intraoperatively in cases of choroidal vasodilation andlor transudationl hemorrhage. 7 In gratitude, I recall Ridley's receptive creativity in capturing questions even of medical students, and StaIlard's admonition to "focus on our mistakes as from them we leam most."8 M. Tadros, M.D. New York, New York REFERENCES 1. Tadros M, Gadallah A, Dwairy H. The place ofiridotomies in modern cataract surgery. XX Concilium Ophthalmologieum, Munich, 1966; Pars I Excerpta Medica, 812-814 2. Tadros M. Psycho-ophthalmology and eye surgery. XXIII Concilium Ophthalmogicum, Kyoto, 1978; Pars 11 Excerpta Medica, 1443-1447 3. Tadros M. Surgical psycho-ophthalmology and contracted sockets. In: Bosniak S, ed, Advanees in Ophthalmie Plastie and Reconstruetive Surgery, vol 8. New York, Pergamon Press, 1990; 274-279 4. Tadros MA. Psico-oftalmologia, afaquia y seudofaquia. An- ales Soc Mex De Oft 1981; 55:416 5. Duncalf D, Rhodes D. Anesthesia in Clinical Ophthalmol- ogy. BaItimore, Williams & Wilkins, 1984; 34 6. Meyers EF. Anesthetic complieations in ophthalmological patients. In: Waltman S, Krupin T, eds, Complications of Ophthalmie Surgery. Philadelphia, JB Lippincott, 1980; 13 7. Tadros MA. Hypocapnea in saving intra-operative crises. XXVI Concilium Ophthalmologicum, Singapore, 1990. In press 8. Stallard H. Eye Surgery, 4th ed. Baltimore, Williams & Wilkins, 1965; 1-3, 68-70 VISUAL DISABILITY INVENTORY: DOCUMENTING FUNCTIONAL IMPAIRMENT CAUSED BY CATARACT To the Editor: We practice ophthalmology in an age of increasing governmental regulation and control. In light of peer review evaluation, documentation of the indi- cations for cataract surgery is important. To establish the disability caused by cataract, methods have progressed from Snellen visual acuity measure- ments to contrast sensitivity, glare testing, and PAM testing. 1 - 4 These advances in documentation of cataract-related disability have tended to involve various devices that may significantly add to the overall costs incurred. We have developed a simple check-list-type questionnaire to be completed by VISUAL DIS ABILITY INVENTORY Patient's Name l. Reading impairment A. Newspaper D. Medicine bottles __ _ B. Mai! E. Writing checks ___ _ C. Bible F. Paying bills ____ _ G. Hold things close, need good light, 01' use a magnifier _________________ _ 2. Household activities A. Cooking, able to see stove knobs, read labels, recipes _______________ _ B. Climbing stairs, holding banister ______ _ C. Walking, unable to see uneven pavement ___ _ D. Falling _________________ _ E . Shaving _______________ _ F. Bathing _________________ G. Cleaning cloth es ____________ _ H. Washing dishes _____________ _ I. Cleaning house _____________ _ J. Yard work - _____________ _ K. Care of other familv members _______ _ L. Trouble getting to doctor _________ _ M. Diffieulty shopping ___________ _ N. Lives alone ______________ _ 3. Driving A. Daytime: Glare of sun B. Night time: Headlights from ear 4. Recognizing people (ex: identify person at dOOf) A. Difficulty with depth perception 5. Hobbies A. Sewing ____ _ E. Sports ____ _ B. Stamps ____ _ F. Lawn eare _____ _ C. Gardening ___ _ G. Recreation activity _ D. Coins ______ _ H. Watehing TV ___ _ 6. Employment A. Unable to perform _____________ _ B. Injury risk _________________ _ C. Cannot drive to work _____________ _ 244 J CATARACT REFRACT SURG-VOL 17, MARCH 1991
Transcript of Visual Disability Inventory: Documenting Functional Impairment Caused by Cataract
surgery. OccasionaIly, surgery is continued, at the risk of complications, possibly beyond control at this stage, although an urgent canthotomy may temper the loss. Such subtle bleeding is further proved by lid ecchymosis later4; (2) minor oozing - that is revealed only in the first dressing as it reaches the skin. Although it raises no problem intraoperatively, it may cause postoperative anxiety, so that lid ecchymosis mandates explanation and reassurance. 3
This wider spectrum of slow imperceptible retrobulbar hemorrhages that is more serious than the early ones which postpone surgery is weIl asserted by three respondents. Dr. Olander says, "The classic presentation of retrobulbar hemorrhage is seen less often than subclinical hemorrhage (which) makes surgery harder with difficulty in exposure, increased pressure on the vitreous .. . . " Likewise, Drs. Wallace and Fechner report postoperative lid ecchymosis as "disconcerting sequelae." In view of the relative frequency of such subtle hemorrhages, we must be alert throughout the entire procedure for their possible late build-up that could then challenge all skills.
If surgery is postponed, I prefer general anesthesia,5.6 also for its advantage of inducing hypocapnea when urgently needed intraoperatively in cases of choroidal vasodilation andlor transudationl hemorrhage. 7
In gratitude, I recall Ridley's receptive creativity in capturing questions even of medical students, and StaIlard's admonition to "focus on our mistakes as from them we leam most."8
M. Tadros, M.D. New York, New York
REFERENCES 1. Tadros M, Gadallah A, Dwairy H. The place ofiridotomies in
modern cataract surgery. XX Concilium Ophthalmologieum, Munich , 1966; Pars I Excerpta Medica, 812-814
2. Tadros M. Psycho-ophthalmology and eye surgery. XXIII Concilium Ophthalmogicum, Kyoto, 1978; Pars 11 Excerpta Medica, 1443-1447
3. Tadros M. Surgical psycho-ophthalmology and contracted sockets. In: Bosniak S, ed, Advanees in Ophthalmie Plastie and Reconstruetive Surgery, vol 8. New York, Pergamon Press, 1990; 274-279
4. Tadros MA. Psico-oftalmologia, afaquia y seudofaquia. Anales Soc Mex De Oft 1981; 55:416
5. Duncalf D, Rhodes D. Anesthesia in Clinical Ophthalmology. BaItimore, Williams & Wilkins, 1984; 34
6. Meyers EF. Anesthetic complieations in ophthalmological patients. In: Waltman S, Krupin T, eds, Complications of Ophthalmie Surgery. Philadelphia, JB Lippincott, 1980; 13
7. Tadros MA. Hypocapnea in saving intra-operative crises. XXVI Concilium Ophthalmologicum , Singapore, 1990. In press
8. Stallard H. Eye Surgery, 4th ed. Baltimore, Williams & Wilkins, 1965; 1-3, 68-70
VISUAL DISABILITY INVENTORY: DOCUMENTING FUNCTIONAL
IMPAIRMENT CAUSED BY CATARACT
To the Editor: We practice ophthalmology in an age of increasing
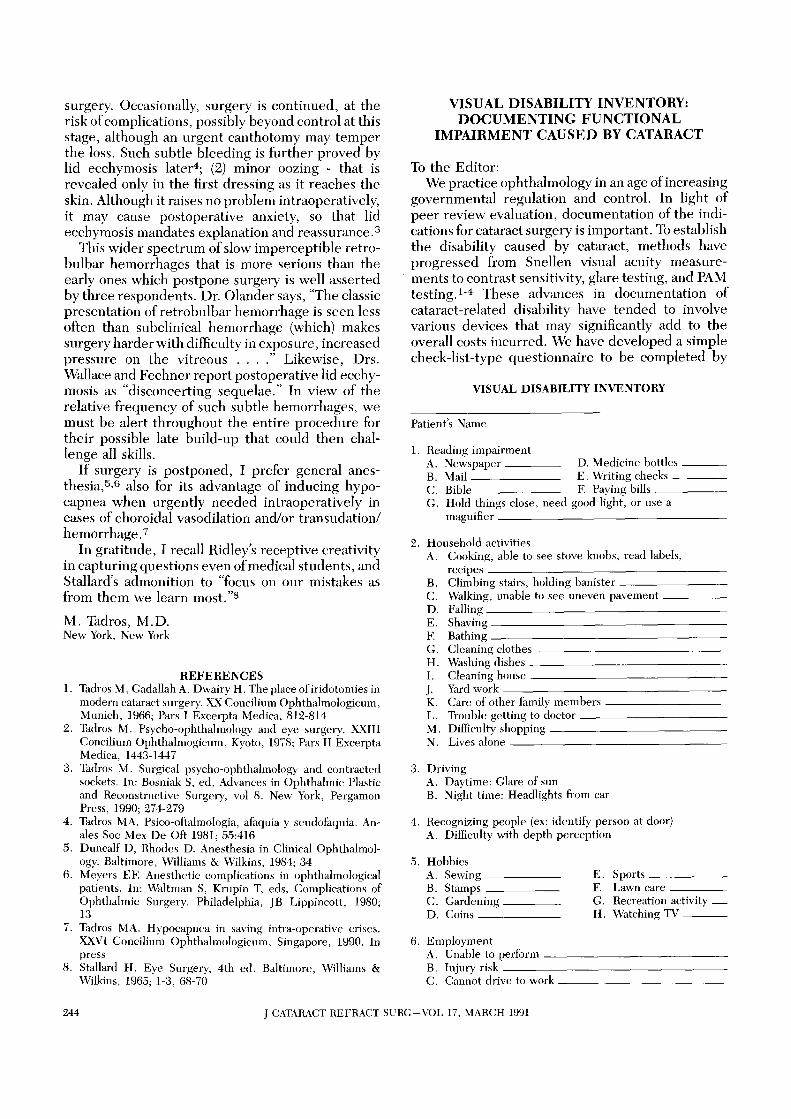
governmental regulation and control. In light of peer review evaluation, documentation of the indications for cataract surgery is important. To establish the disability caused by cataract, methods have progressed from Snellen visual acuity measurements to contrast sensitivity, glare testing, and PAM testing. 1-4 These advances in documentation of cataract-related disability have tended to involve various devices that may significantly add to the overall costs incurred. We have developed a simple check-list-type questionnaire to be completed by
VISUAL DIS ABILITY INVENTORY
Patient's Name
l. Reading impairment A. Newspaper D. Medicine bottles __ _ B. Mai! E. Writing checks ___ _ C. Bible F. Paying bills ____ _ G. Hold things close, need good light, 01' use a
magnifier _________________ _
2. Household activities A. Cooking, able to see stove knobs , read labels,
recipes _______________ _ B. Climbing stairs, holding banister ______ _ C. Walking, unable to see uneven pavement ___ _ D. Falling _________________ _ E . Shaving _______________ _ F. Bathing _________________ ~_ G. Cleaning cloth es ____________ _ H. Washing dishes _____________ _ I. Cleaning house _____________ _ J. Yard work - _____________ _ K. Care of other familv members _______ _ L. Trouble getting to doctor _________ _ M. Diffieulty shopping ___________ _ N. Lives alone ______________ _
3. Driving A. Daytime: Glare of sun B. Night time: Headlights from ear
4. Recognizing people (ex: identify person at dOOf) A. Difficulty with depth perception
5. Hobbies A. Sewing ____ _ E. Sports ____ _ B. Stamps ____ _ F. Lawn eare _____ _ C. Gardening ___ _ G. Recreation activity _ D. Coins ______ _ H. Watehing TV ___ _
6. Employment A. Unable to perform _____________ _ B. Injury risk _________________ _ C. Cannot drive to work _____________ _
244 J CATARACT REFRACT SURG-VOL 17, MARCH 1991
the patient prior to cataract surgery, which attempts to document the functional impairment caused by the cataract.
In contrast to many "high tech," and often high priced forms of preoperative exams, the visual disability inventory places the emphasis on the patient as a functioning individual. Consequently, the patient, peer reviewers, and the ophthalmologist all have a clearer understanding of the real functional disability that the cataract patient is experiencing.
Donald A. Newman, M. D. Ben P. Houser, Jr., M.D. Tamaqua, Pennsylvania
REFERENCES 1. Koch DD. Glare and contrast sensitivity testing in cataract
patients. J Cataract Refract Surg 1989; 15:158-164 2. Prager TC, Urso RG, Holladay JT, Steward RH. Glare
testing in cataract patients: instrument evaluation and iden tification of sources of methodological error. J Cataract Refract Surg 1989; 15:149-157
3. Neumann AC, McCarty GR, Locke J, Cobb B. Glare disability devices for cataractous eye; a consumer's guide. J Cataract Refract Surg 1988; 14:212-216
4. Prager TC, Urso RG, Lewis JW, Ruiz RS. Methodological considerations in glare testing in patients with cataracts (letter). Arch Ophthalmol 1988; 106:1501-1502
ANOXIDANTS AND MACULAR DEGENERATION
To the Editor: We report an uncontrolled review comparing
atrophie macular degeneration (AMD) patients who have consistently ordered ICAPS Plus with those who have not consistently ordered the medication.
The relationship of anoxidantsand AMD is controversial. While Newsome et aLl report zinc effectively slowed the progression of this disease, there have been more unanswered than answered questions regarding this mode of therapy. Clearly, any treatment that helps AMD patients would be a tremendous advancement, since there presently is no treatment available for most of those afflicted by this disease. 2
We compared patients who had at least six months of follow-up with visual acuity of 20/400 or better at three study centers. The records documenting how often these patients ordered ICAPS Plus were provided by LaHaye Laboratories. We attempted to see if there was a statistically significant correlation with ordering frequency and progression of the AMD.
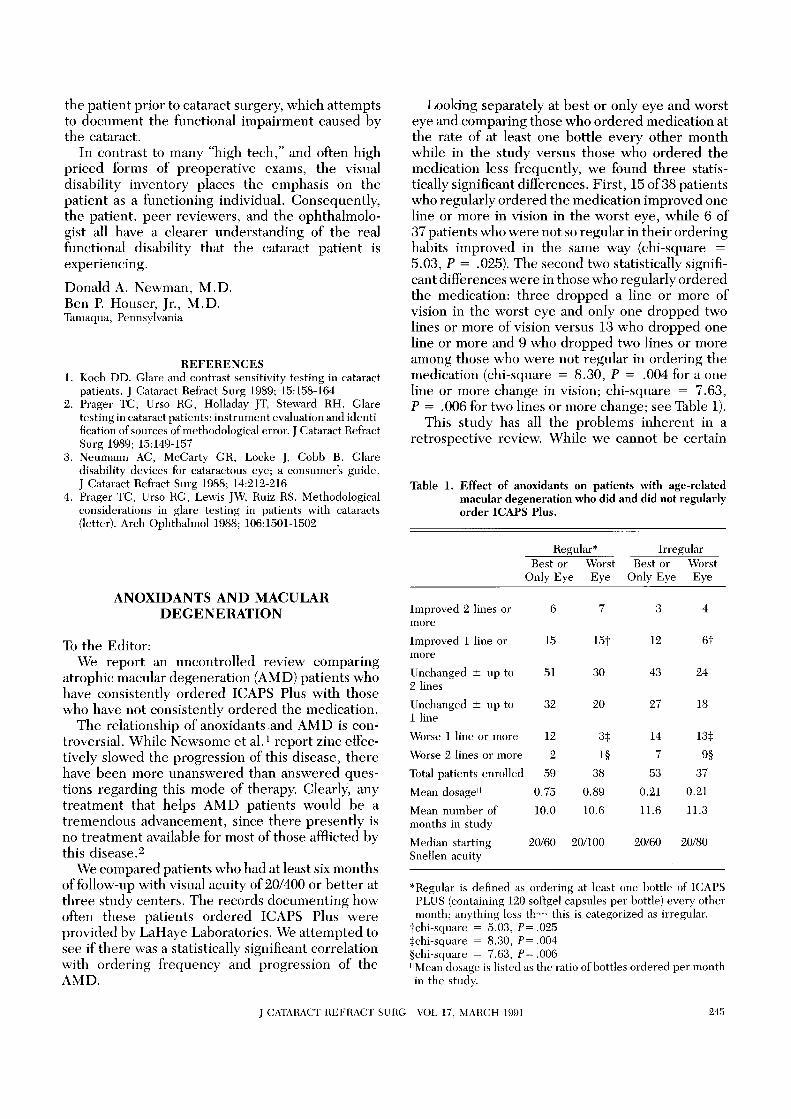
Looking separately at best or only eye and worst eye and comparing those who ordered medication at the rate of at least one bottle every other month while in the study versus those who ordered the medication less frequently, we found three statistically significant differences. First, 15 of38 patients who regularly ordered the medication improved one line or more in vision in the worst eye, while 6 of 37 patients who were not so regular in their ordering habits improved in the same way (chi-square = 5.03, P = .025). The second two statistically significant differences were in those who regularly ordered the medication: three dropped a line or more of vision in the worst eye and only one dropped two lines or more of vision versus 13 who dropped one line or more and 9 who dropped two lines or more among those who were not regular in ordering the medication (chi-square = 8.30, P = .004 for a one line or more change in vision; chi-square = 7.63, P = .006 for two lines or more change; see Table 1).
This study has all the problems inherent in a retrospective review. While we cannot be certain
Table 1. Effect of anoxidants on patients with age-related macular degeneration who did and did not regularly order ICAPS Plus.
Improved 2 lines or more
Improved 1 line or more
Unchanged ± up to 2 lines
Unchanged ± up to 1 line
Worse 1 line or more
Worse 2 lines or more
Total patients enrolled
Mean dosage"
Mean number of months in study
Median starting Snellen acuity
Regular* Best or Worst
Only Eye Eye
6 7
15 15t
51 30
32 20
12 3:j:
2 1§
59 38
0.75 0.89
10.0 10.6
20/60 20/100
Irregular Best or Worst
Only Eye Eye
3 4
12 6t
43 24
27 18
14 13:j:
7 9§
53 37
0.21 0.21
11.6 11.3
20/60 20/80
*Regular is defined as ordering at least one bottle of ICAPS PLUS (containing 120 softgel capsules per bottle) every other month; anything less th"" this is categorized as irregular.
tchi-square = 5.03, P= .025 :j:chi-square = 8.30, P= .004 §chi-square = 7.63, P= .006 "Mean dosage is listed as the ratio ofbottIes ordered per month in the study.
J CATARACT REFRACT SURG-VOL 17, MARCH 1991 245