
Viral host interactions
37
VIROLOGY PART iii VIRAL – HOST INTERACTIONS Dr.Riyaz Sheriff
-
Upload
riyaz-sheriff -
Category
Health & Medicine
-
view
1.507 -
download
0
Transcript of Viral host interactions

VIROLOGY PART iiiVIRAL – HOST INTERACTIONS
Dr.Riyaz Sheriff

Viral – host interactions
• Cellular level
• Individual level
• Community level
@ Cellular level
• Cellular changes seen in tissue culture plate may not be seen in clinical infection
Cell death Malignant
transformationCellular
proliferationNo effect

• Non structural proteins shut down the host protein & DNA synthesis
• Large amount of Viral components change the cellular architecture of
host cell
• Toxic effects
• Change in permeability of Host cell AUTOLYSIS
• Formation of syncytium d/t fusion of adjacent cell membranes
• Viral antigens will confer newer properties on host cell (cell
adsorption, oncogenesis)
• Changes in the host chromosome ( Measles, Mumps, Adenovirus, CMV
& Varicella)
• Inclusion bodies

Inclusion bodies
• Structures with distinct size, shape , location and staining properties
• Can be seen under light microscope after staining
• May be seen in cytoplasm or nucleus
• Generally acidophilic in nature – Pink in colour on staining with Giemsa or
Eosin methylene blue stains
• Some may be basophilic as well

Inclusion bodies
• Helps in diagnosis
– Negri bodies – intra cytoplasmic inclusion – Rabies
– Guarnieri bodies – vaccinia
– Bollinger bodies – fowl pox
– Molluscum bodies – molluscum contagiosum
– Cowdry type A – Herpes virus , Yellow fever virus
– Cowdry type B – Adeno virus, Polio virus
• Inclusion bodies my be an aggregate of virions or collection of
viral antigens or the degenerative changes produced by viral
infection.

Negri bodies – Rabies –Intracytoplasmic

Guarnieri bodies – vaccinia

Bollinger bodies – fowl pox

Molluscum bodies – molluscum contagiosum

Cowdry type A
Hepatocyte with a large intranuclear inclusion body. Surrounded by a clear halo
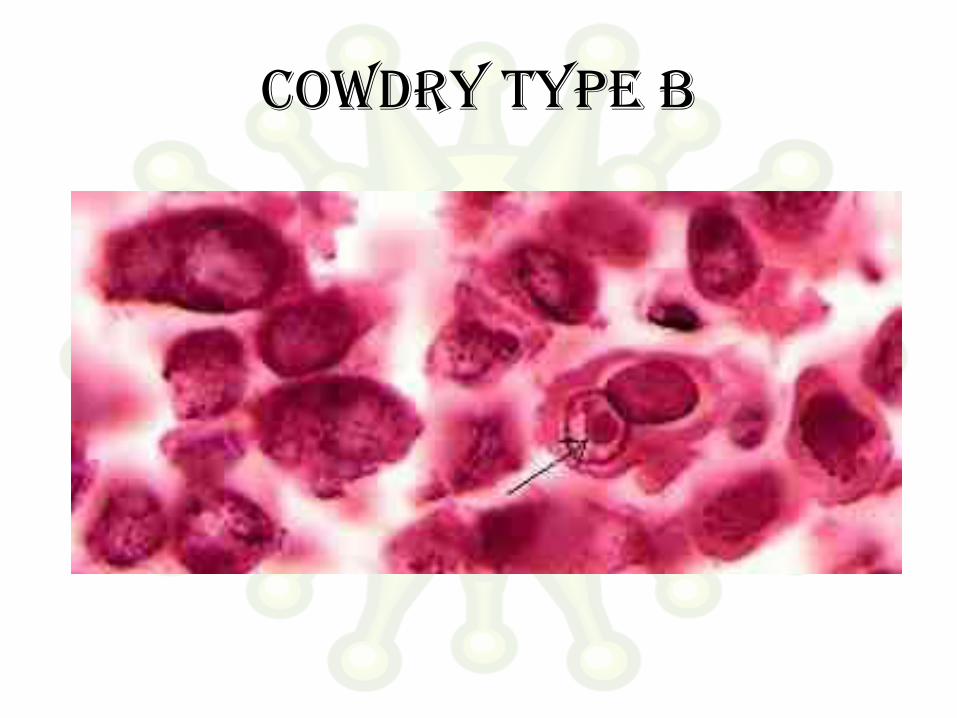
Cowdry type b

Pathogenesis of viral infection
• Inapparent
• Apparent
– Acute
– Subacute
– Chronic
• Latent
• Persistent tolerant infections : Congenital / Neonatal infections
• Oncogenic virus
• HIV

Route of entry • Respiratory tract (Most common)
– Multiply locally Blood/Lymph Extensive multiplication Disease.
– Small pox, chicken pox
– Influenza , Rhinovirus (stay in respiratory tract itself)
• Alimentary tract
– All enveloped viruses are destroyed by bile
– Rhinovirus is inactivated by gastric juice
– Enterovirus, adenovirus, reo virus, hepatitis virus
– Some multiply in GIT and transported to target organs (eg.Polio virus)
• Genital tract
• Conjunctiva
• Skin
• Vertical transmission – Mother to baby

Route of entry • Skin
– Produce few local lesions
– Papilloma, vaccinia, cowpox & molluscum contagiosum.
– Viruses can enter through break in skin
– Abrasions – Papiloma virus
– Insect bites – Arbovirus
– Animal bites – Rabies
– Injections – Hepatitis
• Genital tract
– Human immuno deficiency virus

Route of entry • Conjunctiva
– Local disease – Adenovirus
– Systemic disease – Measles
• Vertical transmission – Mother to baby
– May occur at any stage till birth
– Usally leads to fetal death and abortion
– Maldevelopment – Rubella and Cytomegalovirus
– Many tumor virus spread via this route

Spread of virus in the body
• Studied by Fenner using mouse pox as a model

Mouse pox virus
Enters through skin
Local Multiplication
Skin & Lymphatics
Lymph Nodes Blood (Primary Viremia)
Spleen , Liver (Central foci )
Extensive multiplication
Spills into blood (Secondary
Viremia)
Clinical symptoms
Virus reaches
target organ
Multiplication CLINICAL
DISEASE

Incubation period
• Time taken for virus to spread from site of entry to
the organs of viral multiplication and causation of
disease.
• Localized diseases : Shorter incubation period
• Systemic diseases : Longer incubation period
• Incubation period shorter when directly introduced
into blood stream

Host response Depends on
1. Virulence of the infecting strain
2. Resistance of the host» Immunological
• Humoral
• Cell mediated immunity
» Non specific
• Interferon production
• Body temperature
• Age
• Malnutrition

• Viral infection liberates
– Surface antigens
– Internal antigens
– Non structural antigens
• Early proteins
– Humoral immunity
• IgG
• IgM
• IgA Mucosal surface
Blood and Tissue

Immunoglobulins on viruses
• Prevents attachment of virus to cell
• Enhances viral degradation
• Prevents release of virions from infected cell
Immunoglobulin + Complement
Surface damage of enveloped virions
Cytolysis of virus infected cells

Role of antibodies • Role of antibodies in viral infection is limited
• Antibody to internal antigen Non neutralizing
• Antibody to surface antigen varying neutralization
• Some antibodies can paradoxically increase infectivity
• May contribute to Pathogenicity
• Antibody may result in
– Complement dependent cell injury
– Immune complex type tissue injury

Role of cmi
• Plays a major role in viral infection
• Helps in recovery from viral infection
• Can cause tissue damage as well
• Deficient CMI increase in Herpes, Pox, Measles
• Most often an infection provides long lasting immunity

Non immunological responses
Macrophages phagocytose virus in blood.
Body temperature : > 39°C inhibits most virus
Exception – Herpes simplex – fever blisters
Hormones : Corticosteroids enhance viral infection.
Due to depression of immune system & inhibition of interferon synthesis
Malnutrition
Age

Interferons • Family of host coded proteins
• No direct action on virus
• Acts on host cells to make them refractory o viral infection.
• On exposure to interferon cells produce TIP (Translation Inhibition Protein)
inhibits translation of viral mRNA
• Does not affect translation of host mRNA
• Interferons are species specific.
• RNA viruses are better inducers of interferon production
• Temperature of > 40°C induces interferon secretion
• Steroids and increased O2 tension decrease interferon synthesis
• Synthesis starts in about 30mins of induction and reaches peak by 6-12 hours.

Interferons • α leucocytes
• ß fibroblasts
• Ɣ T-Lymphocytes
• Inactivated by proteolytic enzymes
• Resist 56°C – 60°C for 30-60mins
• α & ß are resistant at pH range of 2-10
• Ɣ is labile at pH of 2
• Non toxic
• Poorly antigenic
• Cannot be estimated by routine serological methods

Use of Interferons
• Ideal candidate for prophylaxis and treatment
– Non toxic
– Non antigenic
– Diffuses freely in the body
– Wide spectrum of antiviral activity
• Drawback species specific
• Current use URTI, Warts, Herpetic keratitis &
anticancer agent in lymphomas

Biological effects of interferons
• Anti-Viral : resistance to infection
• Anti –Microbial: Resistance to intracellular infections (Toxoplasma,
Chlamydia, Malaria)
• Cellular effects : Inhibition of cell growth and proliferation, Increased
expression of MHC antigens on cell surface
• Immunoregulatory :
– Increases activity of Natural killer (NK) calls and T cells.
– Activates cell destruction activity of macrophage
– Moderates antibody formation
– Activates suppressor T cells
– Suppresses DTH
Lab diagnosis • Microscopy :
Demonstration of virus by electron microscopy
Demonstration of inclusion bodies
Fluorescent antibody techniques
• Demonstration of viral antigen:Possible when viral antigens are abundant in the lesion
Precipitation in gel
Immunofluorescence
CIE
RIA
ELISA
PCR

Lab diagnosis • Isolation of virus :
• Need proper transport media at appropriate temperature
• Processing to remove bacterial contaminants
• Inoculation in eggs
• Animal inoculation
• Tissue culture
• Virus isolation has to be correlated with clinical history
Identified by Neutralization tests

Lab diagnosis • Serological diagnosis :
• Rise in titre of antibodies during course of disease
• Examine paired sera
– Acute
– Convalescent (10-14 days later )
• When IgM alone is tested Single sample is enough
– Neutralization test
– Complement fixation
– ELISA
– Hemagglutination Inhibition

Immunoprophylaxis• Infection / vaccine Prolonged and effective immunity
• Live vaccines more effective than killed vaccines
• Successful Live vaccines
– Small pox vaccine
– Yellow fever vaccine
– Polio Vaccine ( Sabin)
• Killed vaccines prepared by inactivating viruses using Heat, Phenol,
Formalin or BPL
• Subunit vaccines
– Hepatitis B

Live attenuated vaccines
Advantages
• Single dose
• Administered by route of natural infection
• Induce immunoglobulins
• Induce CMI
• Long lasting immunity
• Economical
• Apt for mass immunizations
Disadvantages
• Remote chance of reactivation of virus
• Cannot be used in immunocompramised
• Existence of other viruses may result in lessened immune response
• Needs proper cold chain
Killed vaccines • Safe
• Stable
• Can be given as combined
vaccines
• Multiple doses
• Does not induce local
immunity or cell mediated
immunity

Chemoprophylaxis • Challenge
Viruses are strictly intracellular , use host mechanisms for replication.
Hence therapy would destroy host cell as well
• Answer
Selective inhibition of viral enzymes
– Attachment
– Transcription of viral nucleic acid
– Translation
– Replication
– Viral assembly
– Release

Antiviral agents • 1960 : First antiviral – Pox virus : Small pox eradicated by
vaccination
• 1962 : Idoxyuridine : Herpes Keratitis
• 1970 : Acyclovir : effective in Herpes
• Nucleoside analogues – Deoxyuridines
• Idoxyuridine Herpetic keraitis
• Trifluridine Less toxic
• Bromovinyldeoxyuridine Herpes & Varicella
– Adenine arabinoside• Herpetic keratitis
• Herpes simplex
• VZV
– Acyclovir herpes
– GanciclovirCytomegalovirus
– Zidovudine HIV : inhibits viral reverse transcriptase
• Protease inhibitors
– Saquinavir
– Ritonovir
– Indinavir
• Others
– Amantidine – blocks cell penetration by influenza A but not
by B&C
Antiviral agents



















