
Viral Encephalitis
51
I. Introduction Encephalitis is an inflammation of the brain. Most often, it is caused by a viral infection. Several different viruses can cause encephalitis. The most common are the herpes viruses, childhood viruses such as measles, and viruses transmitted by mosquito bite. There are two types of encephalitis -- primary and secondary. In primary encephalitis, a virus attacks the brain and spinal cord directly. In secondary encephalitis, the virus invades another part of your body and travels to your brain. The virus causes inflammation of the nerve cells (encephalitis) or the surrounding membranes (meningitis). Encephalitis is different from meningitis, but these two brain infections often occur together. Most cases of encephalitis are mild and don't last long. However, in some cases encephalitis can be life threatening. Arboviruses, or viruses carried by insects, are among the most common causes of viral encephalitis. Some of the major arboviruses that are transmitted by mosquito include: Eastern equine encephalitis -- This infection is relatively rare, with only a few cases reported each year. However, about half the people who develop severe symptoms die or suffer permanent brain damage.
Transcript of Viral Encephalitis

I. Introduction
Encephalitis is an inflammation of the brain. Most often, it is caused by a
viral infection. Several different viruses can cause encephalitis. The most
common are the herpes viruses, childhood viruses such as measles, and viruses
transmitted by mosquito bite. There are two types of encephalitis -- primary and
secondary. In primary encephalitis, a virus attacks the brain and spinal cord
directly. In secondary encephalitis, the virus invades another part of your body
and travels to your brain. The virus causes inflammation of the nerve cells
(encephalitis) or the surrounding membranes (meningitis). Encephalitis is
different from meningitis, but these two brain infections often occur together.
Most cases of encephalitis are mild and don't last long. However, in some cases
encephalitis can be life threatening.
Arboviruses, or viruses carried by insects, are among the most common
causes of viral encephalitis. Some of the major arboviruses that are transmitted
by mosquito include:
Eastern equine encephalitis -- This infection is relatively rare, with only a
few cases reported each year. However, about half the people who
develop severe symptoms die or suffer permanent brain damage.
La Crosse encephalitis -- usually affects children under 16 years of age in
the upper Midwestern United States. It is rarely fatal.
St. Louis encephalitis -- People in rural Midwestern and southern United
States are primarily affected. Many people have mild symptoms, although
symptoms can be severe in people over age 60. Up to 30% of infected
seniors die of the condition.
West Nile encephalitis -- Primarily affects people in Africa and the Middle
East, but outbreaks have spread across the United States. Most cases are
mild. Symptoms are most severe in older adults and people with
weakened immune systems, and it can be fatal among those populations.
Western equine encephalitis -- People in the western United States and
Canada are most at risk. It usually causes a mild infection, except in
children under 1 year of age, who can suffer permanent brain damage.
Other viruses that commonly cause viral encephalitis include:
Herpes simplex virus type 1 (HSV-1), which is responsible for cold sores
HSV-2, which is responsible for genital herpes
Varicella zoster virus, which causes chicken pox and shingles
Epstein-Barr virus, which causes mononucleosis
Childhood viruses that can cause encephalitis include:
Measles (rubeola)
German measles (rubella)
Mumps
Not all cases of encephalitis are caused by viruses. Some nonviral causes of
encephalitis include:
Bacterial infection
Fungal infection
Parasitic infection
Noninfectious causes, such as allergic reactions or toxins
Objectives:
Student Nurse Centered
1. To modify predisposing or causative factors that contributes to the health
deficit that was existed, that through history taking, and marking out of the family
genogram and constellation, the student nurse will try to study which factor
contribute to the recent situational crisis.
2. To accomplish comprehensive assessments (physical assessment) with due
regards to the role of the student nurse that may give him all the evidences and
supplemental details of the study that was conducted.
3. To critically analyze health needs and concerns of the individual who endure to
an existing health deficit provided the student nurse with activities to develop
SKILLS, KNOWLEDGE and ATTITUDE and values on health promotion and
identification and management of risk factors.
4. To acquire more knowledge about the disease and later on practice the
nursing process in carrying out the nursing plan of care and interventions.
Client Centered
The patient will be able to:
1.) Trust the student nurse, that he can offer the best and quality nursing
interventions prior to the patients coping behaviors.
2.) Acquire knowledge through the student nurse’s health teachings, that later on
within the absence of the student nurse, interventions that the patient may
benefit, and can be done by patient independence.
3.) Participate in the nursing plan of care, that both the nurse and the client) will
be participating in the care of the advocates.

II. Nursing Assessment
a. Personal History
The respondent of this study was “Girl X” (The student nurse made a
code for the patient to secure her right for every particular manner necessary;
The Student nurse named her after the code “Girl X”)
Girl X is a 10yr.old Filipino born on 17th day of May year 2000 at San Isidro
Zaragoza Nueva Ecija. She is presently residing at Barangay San Rafael,
Zaragoza Nueva Ecija. She is the youngest daughter among seven children.
Girl X is a Grade four student at Zaragoza Elementary School. Her mother
and father work as farmers and raise pigs and other livestock’s to earn a living.
According to her mother, Girl X used to play near the fields where her parent
works which made her predisposed to her present condition. Her mother also
states that Girl X has complete immunization at the nearby health center.
c. History of Past illness
According to my interview with the mother of Girl X, this was the
first time she was admitted in the hospital. The mother also stated that Girl
X had cough and colds before due to climate change, and made visits to
the RHU near them to seek some medical assistance.
d. History of Present illness
Her condition apparently started about five days prior to
hospitalization as fever, vomiting and headache for two days. She was
admitted at La Paz Hospital. She was diagnosed to have CNS infection
and was given ampicillin, gentamycin for two days and dexamethazone for
one day. Girl X was transferred to Jecson’s Medical Center per request of
her parents and on the way had convulsion with rolling of eyeballs.
On June 17, 2010, Girl X was admitted at Jecson’ Medical Center
per request of her parents because along the way she had convulsion and
rolling of eyeballs. She was then transferred to Pediatric Intensive Care
Unit for close monitoring.
III. Physical Examination
SUMMARY OF FINDINGS
On the day of admission, “Girl X’s” vitals are: Temperature; 38.4 °C,
Cardiac Rate; 142bpm, Respirations; 21 cpm, Blood Pressure:
100/60mmHg which indicate fever and Tachycardia.
On the first day of visit, her vital signs are: Temperature; 37.5, Cardiac
Rate; 100bpm, Respiratory Rate; 14cpm,
a. Nasogastric Tube present
b. Clear breath sounds during auscultation.
c. Negative verbal output
d. Presence of lyses in scalp
f. Diagnostic and Laboratory Procedures
Diagnostic &
Laboratory
Procedures
Date
Ordered
Results
in
Indications or
Purposes
Results Normal
Values
Analysis and
Interpretation
Nursing
Responsibilities
Hematology:
All result in
normal
except for:
DO:
06-17-
10
It measures the
number of WBC
in a cubic
millimeter
13.8G/L 4.1-10.9G/L The White
blood cells
exceeds the
normal value
Before:
Verify doctor’s
order.
Instruct patient

White
Blood Cell
blood. It is used
to detect
infection or
inflammation
which
indicates the
presence of
infection.
about the
schedule of the
patient.
Explain the
procedure and
purpose to the
patient.
Tell the patient
that feeding not
required.
Instruct patient
there are no
special
measures
needed.
After:
Apply pressure
or a pressure
dressing to the
venipuncture
site.
Observe the
venipuncture
site for
bleeding.
Monitor for
signs and
symptoms of
infection.
Blood
Chemistry:
All results are
in normal
values
except for:
Serum
Potassium
06-21-
10
To check for the
level of serum
potassium in
the blood
3.30meq/L 3.40-
5.60meq/L
Hematology:
hemoglobin
06-24-
10
It evaluates the
patient’s
hemoglobin
content and
thus the iron
status and
oxygen carrying
capacity of
erythrocytes by
measuring the
number of
hemoglobin per
deciliter (100
ml) of blood.
107g/L 110-
160.0g/L
decreased
volume of
oxygen-
carrying
component
of the blood
Hematocrit
It is the
measure of the
RBC’s in the
whole blood
expressed as
percentage. It is
used to
measure and
assess
decreased
volume related
to bleeding.
0.35% 0.37-0.47% The White
blood cells
exceeds the
normal value
which
indicates the
presence of
infection.

Red Blood
Cells
To determine
the patient’s
number of red
blood cell in the
blood.
3.9million/
cubic
millimeter
4.2-
5.4million/
cubic
millimeter
Low volume
indicate
bleeding
White Blood
Cells
It measures the
number of WBC
in a cubic
millimeter
blood. It is used
to detect
infection or
inflammation
25,000cubi
c millimeter
5,000-
10,000cubi
c millimeter
Elevated
white blood
cell count
indicate
presence of
infection
Platelet
The primary
functions of a
platelet count
are to assist in
the diagnosis of
bleeding
disorders.
928g/L 140-440g/L Increase
platelet count
indicates risk
for
obstruction in
the blood
vessels.
MCHC To check for
anemia
30.8g/dl 33-37g/dl decreased
volume may
indicate
anemia
Hematology:
hemoglobin
06-29-
10
It evaluates the
patient’s
hemoglobin
content and
thus the iron
status and
oxygen carrying
capacity of
erythrocytes by
measuring the
number of
hemoglobin per
deciliter (100
ml) of blood.
101g/L 110-160g/L decreased
volume of
oxygen-
carrying
component
of the blood

Hematocrit
It is the
measure of the
RBC’s in the
whole blood
expressed as
percentage. It is
used to
measure and
assess
decreased
volume related
to bleeding.
0.33% 0.37-0.4% Decrease
volume of
hematocrit
determine a
need for red
blood cell
trnsfusion
Red Blood
Cell
To determine
the patient’s
number of red
blood cell in the
blood.
3.7million/
cubic
millimeter
4.2-
5.4million/
cubic
millimeter
Low volume
indicates
bleeding or
increased
sequestratio
n of the
spleen
White Blood
Cell
It measures the
number of WBC
in a cubic
millimeter
blood. It is used
to detect
infection or
inflammation
15.5 cubic
millimeter
5,000-
10,000cubi
c millimeter
Elevated
white blood
cell count
indicate
presence of
infection
platelet The primary
functions of a
platelet count
are to assist in
the diagnosis of
bleeding
disorders.
1074g/L 140-440g/L
Hematology:
Hemoglobin
07-05-
10
It evaluates the
patient’s
hemoglobin
content and
thus the iron
109g/L 110-160g/L decreased
volume of
oxygen
carrying
component

status and
oxygen carrying
capacity of
erythrocytes by
measuring the
number of
hemoglobin per
deciliter (100
ml) of blood.
of the blood
Hematocrit
It is the
measure of the
RBC’s in the
whole blood
expressed as
percentage. It is
used to
measure and
assess
decreased
volume related
to bleeding.
0.36% 0.37-0.4% Decrease
volume of
hematocrit
determine a
need for red
blood cell
transfusion
Red Blood
Cell
To determine
the patient’s red
blood cell in the
blood.
3.43T/L 4.20-
6.30T/L
decreased
volume
indicates
bleeding or
increased
sequestratio
n of the
spleen
Platelet The primary
functions of a
platelet count
are to assist in
the diagnosis of
bleeding
disorders.
665g/L 140-440g/L
White Blood
Cell
07-21-
10
It measures the
number of WBC
in a cubic
13.6 cubic
millimeter
5,000-
10,000cubi
c millimeter
Elevated
white blood
cell count

millimeter
blood. It is used
to detect
infection or
inflammation
indicate
presence of
infection
Platelet The primary
functions of a
platelet count
are to assist in
the diagnosis of
bleeding
disorders.
517g/L 140-440g/L
Bacteriology of the CSF 06-28-10
Exam Desired: Culture and Sensitivity Result
-Moderate growth of staphylococcus Epidermidis
Susceptible to: Resistant to:
Gentamycin Linezoid
Penicillin Trimethophrim
Tigecycline sulfamethoxazole
Imipenem oxacillin
Cefoxitin
Clindamycin
Netilcimin
Tetracycline
Novobrocin
Chloramphenicol
Piperacillin-Tazobactam
Ciprofloxacin
Erythromycin
Vancomycin
azithromycin

Chest X-Ray 07-23-10
Steaky perihilar infiltrates arenoted
Heart is not enlarged.
No other remarkable findings
IMPRESSION:
Consider pulmonary congestion
CT-Scan of the Head/Brain 06-18-10
IMPRESSION:
Normal plain cranial CT scan contrast study is suggested
IV. Anatomy and Physiology
As the most complex system, the nervous system serves as the body control
center and communications electrical-chemical wiring network. As a key
homeostatic regulatory and coordinating system, it detects, interprets, and
responds to changes in internal and external conditions. The nervous system
integrates countless bits of information and generates appropriate reactions by
sending electrochemical impulses through nerves to effector organs such as
muscles and glands. The brain and spinal cord are the central nervous system
(CNS); the connecting nerve processes to effectors and receptors serve as the
peripheral nervous system (PNS). Special sense receptors provide for taste,
smell, sight, hearing, and balance. Nerves carry all messages exchanged
between the CNS and the rest of the body.

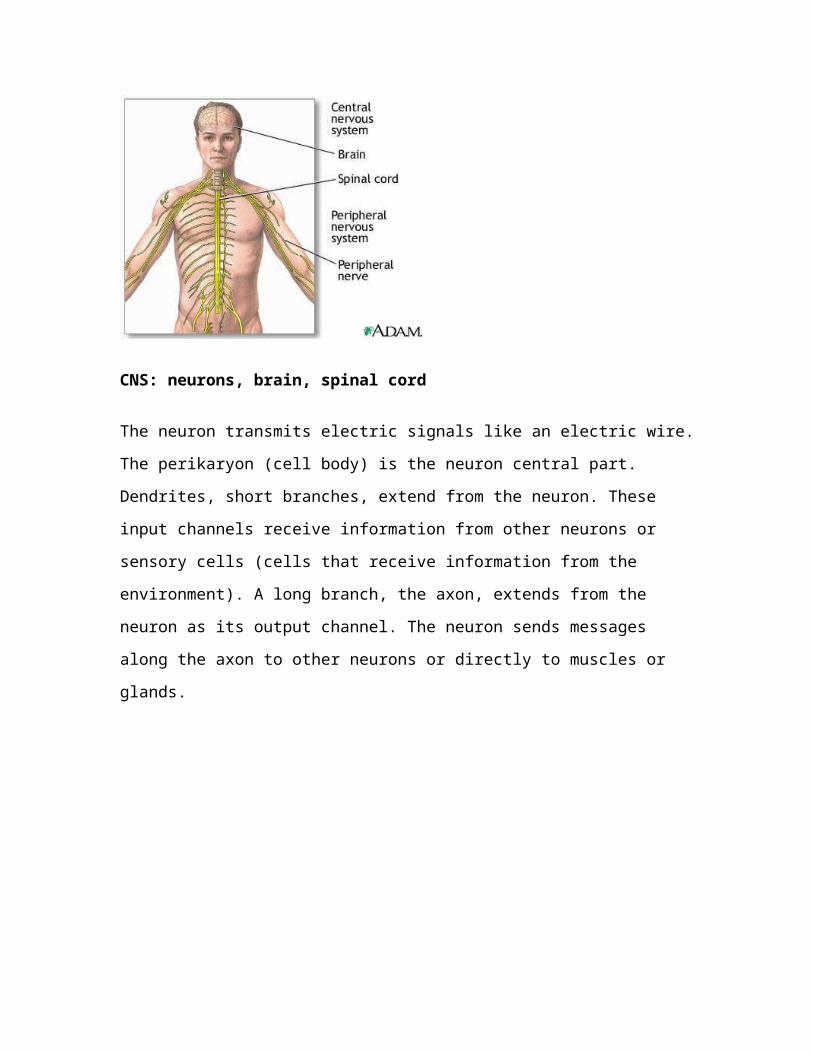
CNS: neurons, brain, spinal cord
The neuron transmits electric signals like an electric wire. The perikaryon (cell
body) is the neuron central part. Dendrites, short branches, extend from the
neuron. These input channels receive information from other neurons or sensory
cells (cells that receive information from the environment). A long branch, the
axon, extends from the neuron as its output channel. The neuron sends
messages along the axon to other neurons or directly to muscles or glands.
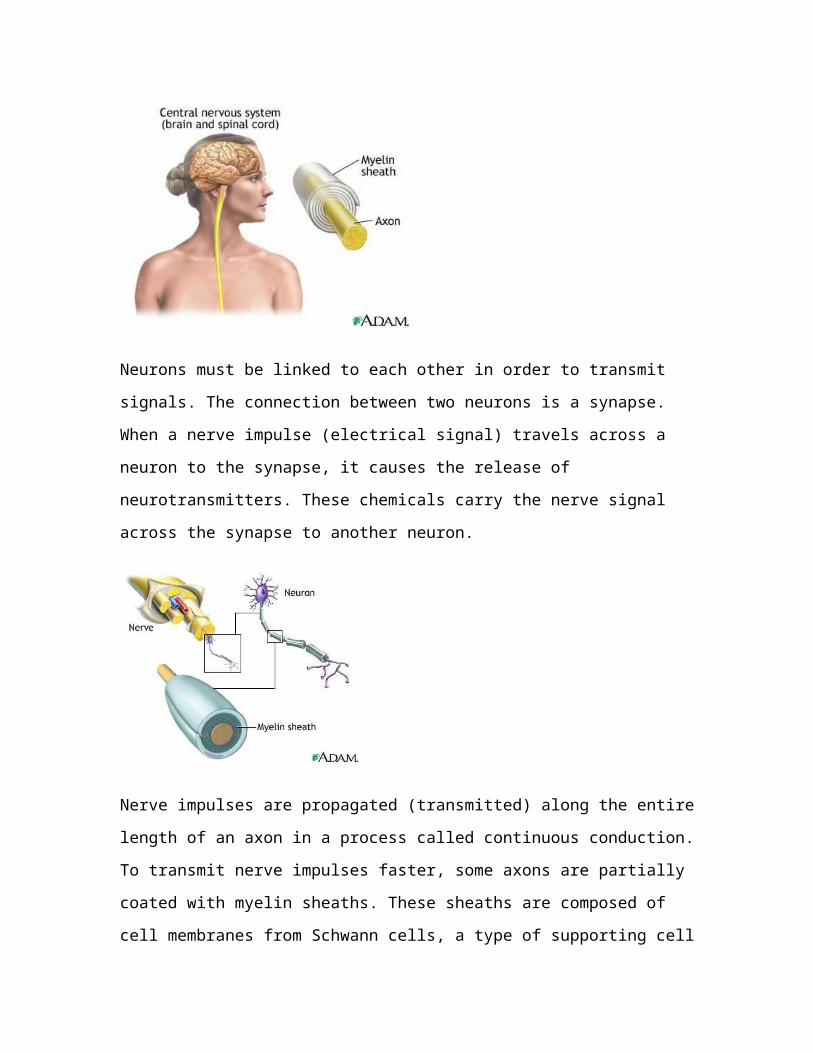
Neurons must be linked to each other in order to transmit signals. The
connection between two neurons is a synapse. When a nerve impulse (electrical
signal) travels across a neuron to the synapse, it causes the release of

neurotransmitters. These chemicals carry the nerve signal across the synapse to
another neuron.
Nerve impulses are propagated (transmitted) along the entire length of an axon
in a process called continuous conduction. To transmit nerve impulses faster,
some axons are partially coated with myelin sheaths. These sheaths are
composed of cell membranes from Schwann cells, a type of supporting cell
outside the CNS. Nodes of Ranvier (short intervals of exposed axon) occur
between myelin sheaths. Impulses moving along myelinated axons jump from
node to node. This method of nerve impulse transmission is saltatory conduction.
The brain has billions of neurons that receive, analyze, and store information
about internal and external conditions. It is also the source of conscious and
unconscious thoughts, moods, and emotions. Four major brain divisions govern
its main functions: the cerebrum, the diencephalon, the cerebellum, and the brain
stem.
The cerebrum is the large rounded area that divides into left and right
hemispheres (halves) at a fissure (deep groove). The hemispheres communicate
with each other through the corpus callosum (bundle of fibers between the
hemispheres). Surprisingly, each hemisphere controls muscles and glands on
the opposite side of the body. Comprising 85 percent of total brain weight, the
cerebrum controls language, conscious thought, hearing, somatosensory
functions (sense of touch), memory, personality development, and vision.
Gray matter (unmyelinated nerve cell bodies) composes the cerebral cortex
(outer portion of the cerebrum). Beneath the cortex lies the white matter
(myelinated axons). During embryonic development, the cortex folds upon itself
to form gyri (folds) and sulci (shallow grooves) so that more gray matter can
reside within the skull cavity.
The diencephalon forms the central part of the brain. It consists of three
bilaterally symmetrical structures: the hypothalamus, thalamus, and epithalamus.
The hypothalamus 'master switchboard' resides in the brain stem upper end. It
controls many body activities that affect homeostasis (maintenance of a stable
internal environment in the body).

The hypothalamus is the main neural control center (brain part that controls
endocrine glands). The pituitary gland lies just below the hypothalamus. The
pituitary gland is a small endocrine gland that secretes a variety of hormones
(organic chemicals that regulate the body's physiological processes). When the
hypothalamus detects certain body changes, it releases regulating factors
(chemicals that stimulate or inhibit the pituitary gland). The pituitary gland then
releases or blocks various hormones. Because of this close association between
the nervous and endocrine systems, together they are called the neuroendocrine
system.
The hypothalamus also regulates visceral (organ-related) activities, food and fluid
intake, sleep and wake patterns, sex drive, emotional states, and production of
antidiuretic hormone (ADH) and oxytocin. The pituitary gland produces both
these hormones.
The thalamus is a relay and preprocessing station for the many nerve impulses
that pass through it. Impulses carrying similar messages are grouped in the
thalamus, then relayed to the appropriate brain areas.

The epithalamus is the most dorsal (posterior) portion of the diencephalon. It
contains a vascular network involved in cerebrospinal fluid production. Extending
from the epithalamus posteriorly is the pineal body, or pineal gland. Its function is
not yet fully understood; it is thought to control body rhythms.
At the rear of the brain is the cerebellum. The cerebellum is similar to the
cerebrum: each has hemispheres that control the opposite side of the body and
are covered by gray matter and surface folds. In the cerebellum, the folds are
called folia; in the cerebrum, sulci. The vermis (central constricted area) connects
the hemispheres. The cerebellum controls balance, posture, and coordination.
The brain stem connects the cerebrum and cerebellum to the spinal cord. Its
superior portion, the midbrain, is the center for visual and auditory reflexes;
examples of these include blinking and adjusting the ear to sound volume. The
middle section, the pons, bridges the cerebellum hemispheres and higher brain
centers with the spinal cord. Below the pons lies the medulla oblongata; it
contains the control centers for swallowing, breathing, digestion, and heartbeat.
The reticular formation extends throughout the midbrain. This network of nerves
has widespread connections in the brain and is essential for consciousness,
awareness, and sleep. It also filters sensory input, which allows a person to
ignore repetitive noises such as traffic, yet awaken instantly to a baby's cry.
The spinal cord is a continuation of the brain stem. It is long, cylindrical, and
passes through a tunnel in the vertebrae called the vertebral canal. The spinal
cord has many spinal segments, which are spinal cord regions from which pairs
(one per segment) of spinal nerves arise. Like the cerebrum and cerebellum, the
spinal cord has gray and white matter, although here the white matter is on the
outside. The spinal cord carries messages between the CNS and the rest of the
body, and mediates numerous spinal reflexes such as the knee-jerk reflex.
Meninges, three connective tissue layers, protect the brain and spinal cord. The
outermost dura layer forms partitions in the skull that prevents excessive brain
movement. The arachnoid middle layer forms a loose covering beneath the dura.
The innermost pia layer clings to the brain and spinal cord; it contains many tiny
blood vessels that supply these organs.
Another protective substance, cerebrospinal fluid, surrounds the brain and spinal
cord. The brain floats within the cerebrospinal fluid, which prevents against
crushing under its own weight and cushions against shocks from walking,
jumping, and running.
PNS: somatic (voluntary) nervous system, autonomic (involuntary) nervous
system
The peripheral nervous system includes sensory receptors, sensory neurons,
and motor neurons. Sensory receptors are activated by a stimulus (change in the
internal or external environment). The stimulus is converted to an electronic
signal and transmitted to a sensory neuron. Sensory neurons connect sensory
receptors to the CNS. The CNS processes the signal, and transmits a message
back to an effector organ (an organ that responds to a nerve impulse from the
CNS) through a motor neuron.
The PNS has two parts: the somatic nervous system and the autonomic nervous
system. The somatic nervous system, or voluntary nervous system, enables
humans to react consciously to environmental changes. It includes 31 pairs of
spinal nerves and 12 pairs of cranial nerves. This system controls movements of
skeletal (voluntary) muscles.
Thirty-one pairs of spinal nerves emerge from various segments of the spinal
cord. Each spinal nerve has a dorsal root and a ventral root. The dorsal root
contains afferent (sensory) fibers that transmit information to the spinal cord from
the sensory receptors. The ventral root contains efferent (motor) fibers that carry
messages from the spinal cord to the effectors. Cell bodies of the efferent fibers
reside in the spinal cord gray matter. These roots become nerves that innervate
(transmit nerve impulses to) muscles and organs throughout the body.
Twelve pairs of cranial nerves transmit from special sensory receptors
information on the senses of balance, smell, sight, taste, and hearing. Cranial
nerves also carry information from general sensory receptors in the body, mostly

from the head region. This information is processed in the CNS; the resulting
orders travel back through the cranial nerves to the skeletal muscles that control
movements in the face and throat, such as for smiling and swallowing. In
addition, some cranial nerves contain somatic and autonomic motor fibers.
The involuntary nervous system (autonomic nervous system) maintains
homeostasis. As its name implies, this system works automatically and without
voluntary input. Its parts include receptors within viscera (internal organs), the
afferent nerves that relay the information to the CNS, and the efferent nerves that
relay the action back to the effectors. The effectors in this system are smooth
muscle, cardiac muscle and glands, all structures that function without conscious
control. An example of autonomic control is movement of food through the
digestive tract during sleep.
The efferent portion of the autonomic system is divided into sympathetic and
parasympathetic systems. The sympathetic nerves mobilize energy for the 'Fight
or Flight' reaction during stress, causing increased blood pressure, breathing
rate, and bloodflow to muscles. Conversely, the parasympathetic nerves have a
calming effect; they slow the heartbeat and breathing rate, and promote digestion
and elimination. This example of intimate interaction with the endocrine system is
one of many that explain why the two systems are called the neuroendocrine
system.
The relationship between sensory and motor neurons can be seen in a reflex
(rapid motor response to a stimulus). Reflexes are quick because they involve
few neurons. Reflexes are either somatic (resulting in contraction of skeletal
muscle) or autonomic (activation of smooth and cardiac muscle). All reflex arcs
have five basic elements: a receptor, sensory neuron, integration center (CNS),
motor neuron, and effector.
Spinal reflexes are somatic reflexes mediated by the spinal cord. These can
involve higher brain centers. In a spinal reflex, the message is simultaneously

sent to the spinal cord and brain. The reflex triggers the response without waiting
for brain analysis. If a finger touches something hot, the finger jerks away from
the danger. The burning sensation becomes an impulse in the sensory neurons.
These neurons synapse in the spinal cord with motor neurons that cause the
burned finger to pull away. This spinal reflex is a flexor, or withdrawal reflex.
The stretch reflex occurs when a muscle or its tendon is struck. The jolt causes
the muscle to contract and inhibits antagonist muscle contraction. A familiar
example is the patellar reflex, or knee-jerk reflex, that occurs when the patellar
tendon is struck. The impulse travels via afferent neurons to the spinal cord
where the message is interpreted. Two messages are sent back, one causing the
quadriceps muscles to contract and the other inhibiting the antagonist hamstring
muscles from contracting. The contraction of the quadriceps and inhibition of
hamstrings cause the lower leg to kick, or knee-jerk.

V. The Patient and His Illness
Schematic Diagram of Pathophysiology
BOOK BASED
Being very young or older adult,
Being exposed to mosquitoes or ticks,
Having a weakened immune system,
Not being immunized against measles, mumps, and rubella,
Traveling to areas where viral encephalitis is prevalent
Ingestion of pathogen or vector bite
Invasion of pathogen into the CNS
Cerebral or cerebellar dysfunction
Infectious encephalitis
Infection is seeded from point of origin to CNS
Acute febrile illness
Neuronal phase
flu-like symptoms, such as fever, sore throat, cough, and malaise
person may experience headache, stiff neck, intolerance to light, and
vomiting
50% of people with encephalitis may have seizures
Other signs and symptoms of encephalitis depend on which area of the
brain is most affected. These may include an impaired ability to use or
comprehend words or coordinate voluntary muscle movements, muscle
weakness or partial paralysis on one side of the body, uncontrollable

tremors or involuntary movements, and an inability to regulate body
temperature
PATIENT BASED
Being young,
Being exposed to mosquitoes or ticks,
Ingestion of pathogen or vector bite
Invasion of pathogen into the CNS
Cerebral or cerebellar dysfunction
Infectious encephalitis
Infection is seeded from point of origin to CNS
Acute febrile illness
Neuronal phase
flu-like symptoms, such as fever and malaise
person may experience headache, stiff neck, intolerance to light, and
vomiting
seizures
Other signs and symptoms of encephalitis depend on which area of the
brain is most affected. These may include an impaired ability to use or
comprehend words or coordinate voluntary muscle movements, muscle
weakness or partial paralysis on one side of the body, uncontrollable
tremors or involuntary movements, and an inability to regulate body
temperature

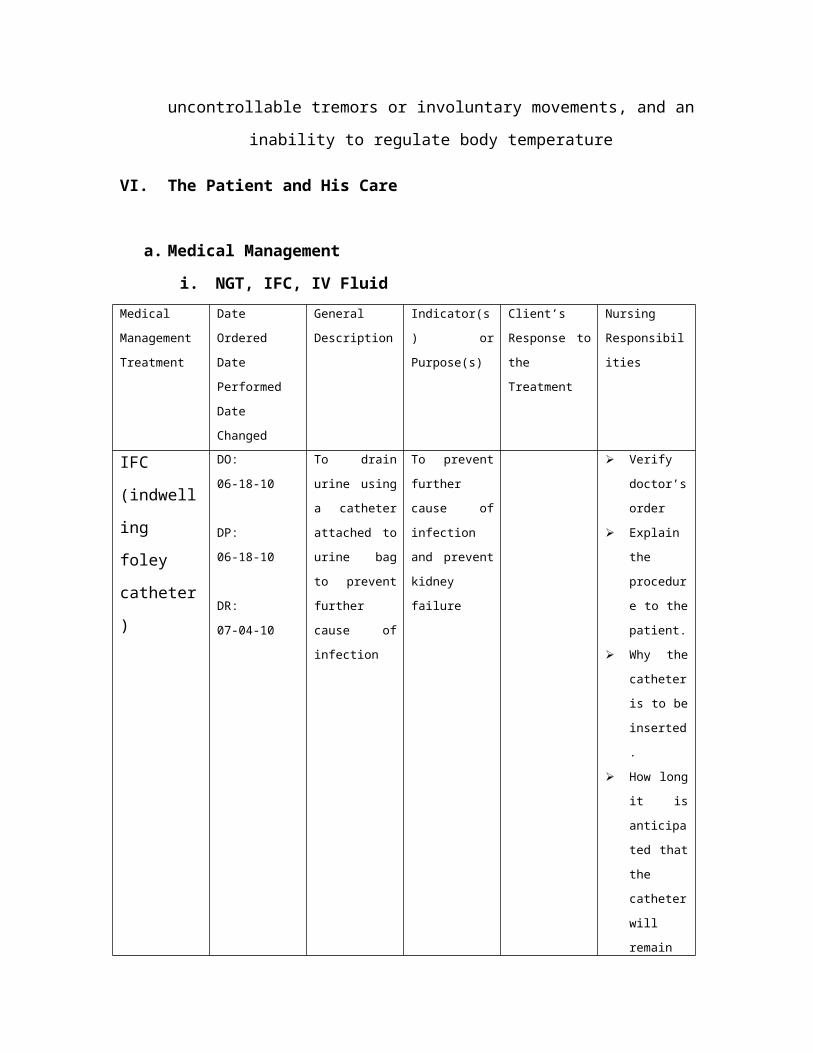
VI. The Patient and His Care
a. Medical Management
i. NGT, IFC, IV Fluid
Medical
Management
Treatment
Date Ordered
Date
Performed
Date Changed
General
Description
Indicator(s) or
Purpose(s)
Client’s
Response to
the Treatment
Nursing
Responsibilitie
s
IFC
(indwelling
foley
catheter)
DO:
06-18-10
DP:
06-18-10
DR:
07-04-10
To drain urine
using a
catheter
attached to
urine bag to
prevent further
cause of
infection
To prevent
further cause
of infection and
prevent kidney
failure
Verify
doctor’s
order
Explain
the
procedure
to the
patient.
Why the
catheter is
to be
inserted.
How long
it is
anticipated
that the
catheter
will remain
in place.
NGT
(Nasogastri
c Tube)
DO:
06-21-10
DP:
06-21-10
DR:
07-26-10
The tube is
used for
feeding or
administration
of medications
especially if the
patient has
impaired
swallowing
The tube is
used for
feeding or
administration
of medications
especially if the
patient has
impaired
swallowing or
is not able to
ingest sufficient
calories
Verify
doctor’s
order
Explain
the
procedure
to the
patient.
Why the
tube is to
be
inserted.

secondary to
neurological or
other deficits
impairing ability
to ingest
sufficient
nutrition.
How long
it is
anticipated
that the
tube will
remain in
place.
The
patient is
kept in
NPO prior
to the
procedure.
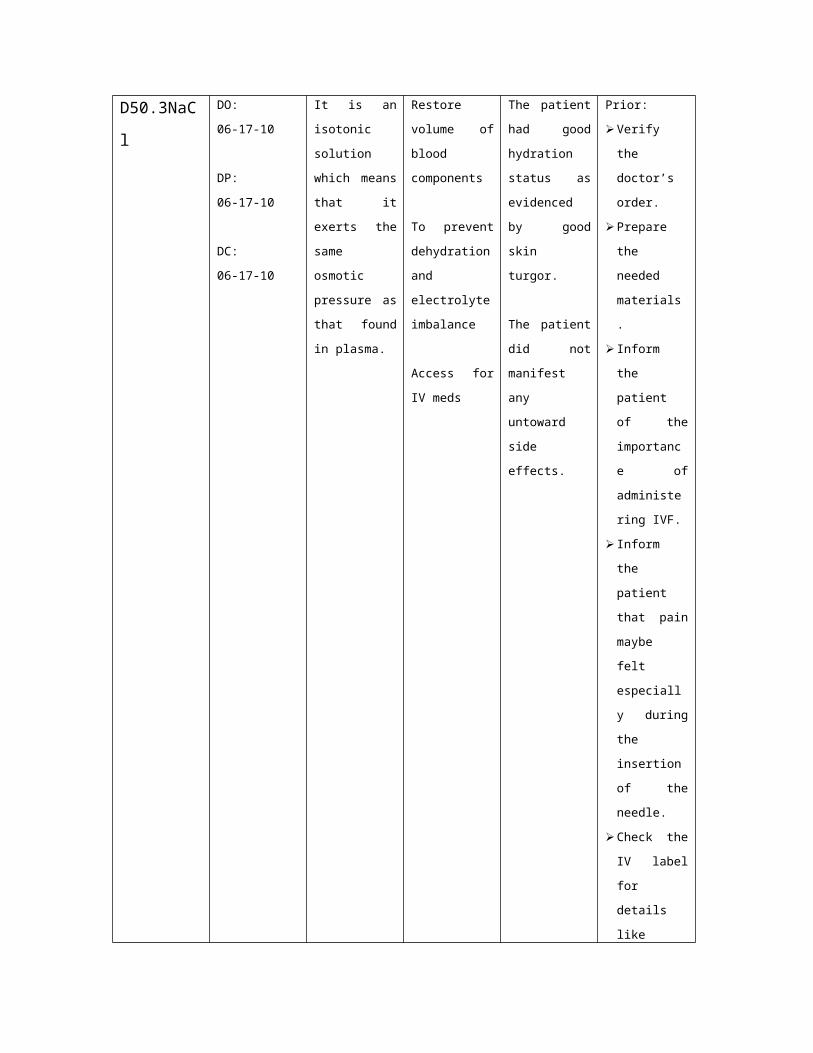
D50.3NaCl DO:
06-17-10
DP:
06-17-10
DC:
06-17-10
It is an isotonic
solution which
means that it
exerts the
same osmotic
pressure as
that found in
plasma.
Restore
volume of
blood
components
To prevent
dehydration
and electrolyte
imbalance
Access for IV
meds
The patient
had good
hydration
status as
evidenced by
good skin
turgor.
The patient did
not manifest
any untoward
side effects.
Prior:
Verify the
doctor’s
order.
Prepare the
needed
materials.
Inform the
patient of the
importance
of
administering
IVF.
Inform the
patient that
pain maybe
felt
especially
during the
insertion of
the needle.
Check the IV
label for
details like
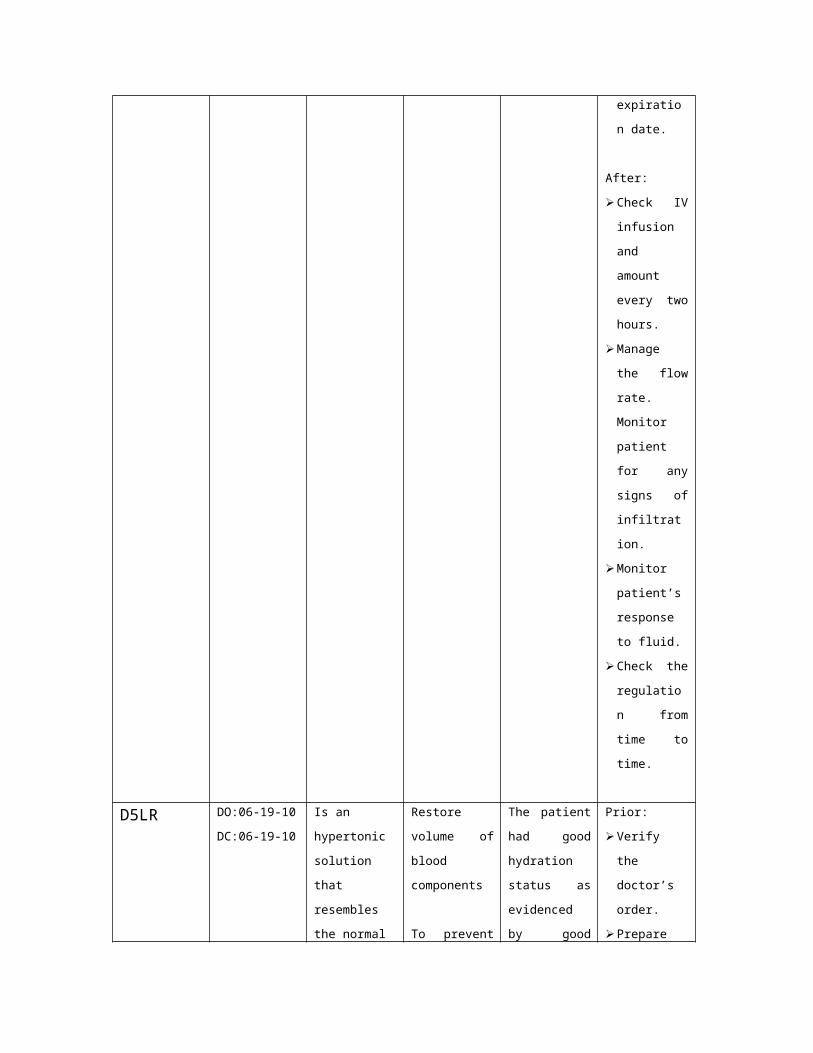
expiration
date.
After:
Check IV

infusion and
amount
every two
hours.
Manage the
flow rate.
Monitor
patient for
any signs of
infiltration.
Monitor
patient’s
response to
fluid.
Check the
regulation
from time to
time.
D5LR DO:06-19-10
DC:06-19-10
Is an
hypertonic
solution that
resembles the
normal
composition of
blood serum
and plasma;
potassium level
below body’s
daily
requirement;
caloric value
180.
Restore
volume of
blood
components
To prevent
dehydration
and electrolyte
imbalance
Access for IV
meds
The patient
had good
hydration
status as
evidenced by
good skin
turgor.
The patient did
not manifest
any untoward
side effects.
Prior:
Verify the
doctor’s
order.
Prepare the
needed
materials.
Inform the
patient of the
importance
of
administering
IVF. Check
the IV label
for details
like
expiration
date.
After:
Check IV
infusion and
amount

every two
hours.
Manage the
flow rate.
Monitor
patient for
any signs of
infiltration.
Monitor
patient’s
response to
fluid.
Check the
regulation
from time to
time.
D5IMB DO:
06-22-10
DC:
06-22-10
Is an
intravenous
drip, it is
balanced
multiple
maintenance
solution
containing 5%
dextrose
It is commonly
given to help
rehydrate
patients
suffering from
dehydration or
to ensure that
an ill person
take in enough
fluids.
The patient
had good
hydration
status as
evidenced by
good skin
turgor.
The patient did
not manifest
any untoward
side effects.
Prior:
Verify the
doctor’s
order.
Prepare the
needed
materials.
Inform the
patient of the
importance
of
administering
IVF. Check
the IV label
for details
like
expiration
date.
After:
Check IV
infusion and
amount
every two
hours.
Manage the
flow rate.
Monitor
patient for
any signs of
infiltration.
Monitor
patient’s
response to
fluid.
Check the
regulation from
time to time.
ii. Drugs
Generic
Name
Brand Name
Date
Ordered
Date
Performe
d Date
Changed
Route of
Administratio
n Dosage and
Frequency
Indication or Purpose Client’s
Response to
Treatment
Nursing
Responsibilities
diazepam 06-17-10 5mg IVP Adjunct in the
management of:
anxiety disorder,
treatment of status
epilepticus/uncontrole
d seizures, skeletal
muscle relaxant
Decrease in
muscle
spasm,
control
seizures.
Clarify
doctors
order
Check for
drug
allergies
Check for
the 12 R’s
Document
when drug
is given.
paracetamol 06-17-10 300mg,IVP,
every 4
hours, round
the clock
To decrease body
temperature to normal
range.
Temperatur
e returns to
normal
Clarify
doctors
order
Check for
drug
allergies
Check for

the 12 R’s
Document
when drug
is given.
ceftriaxone 06-17-10 1g IVP every
12 hours
Treatment of the
following infections
caused by susceptible
organisms: meningitis
and bone/joint
infection
hinders or
kills
susceptible
bacteria
including
many gram-
positive
organism
and enteric
gram
negative
bacilli
Clarify
doctors
order
Check for
allergies
With
antibiotics
Document
when drug
is given.
Check for
the 15 R’s
in giving
medication
s
mannitol 06-17-10 60ml/soluset
every 8hours
Adjunct in the
treatment of: acute
oliguric renal failure,
edema, increased
intracranial or intra
ocular pressure, toxic
overdose.
Urine output
is at least
30ml,
reduction of
intracranial
pressure.
Clarify
doctors
order
Document
when drug
is given.
Check for
the 15 R’s
in giving
medication
s
phenobarbita
l
06-17-10 1g/tablet,
twice a day,
via
nasogastric
tube
Anticonvulsant in
tonic-clonic (grand
mal), partiel, and
afebrile seizures in
children.
Decreased
or cessation
of seizure
activity
without
excessive
sedation
Clarify
doctors
order
Document
when drug
is given.
Check for
the 15 R’s
in giving
medication
s

Monitor
respiratory
status,
pulse, and
blood
pressure
frequently.
meropenem 06-24-10 950mg,IVP,
every 8hours
Treatment of: intra-
abdominal infections,
bacterial meningitis,
skin and skin structure
infection.
Resolution
of signs and
symptoms of
infection.
Clarify
doctors
order
Check for
allergy
Document
when drug
is given.
Check for
the 12 R’s
Observe
for signs
and
symptoms
of
anaphylaxi
s
Discontinu
e the drug
and notify
the
physician if
symptoms
occur.
Have
epinephrin
e, an
antihistami
ne, and
resuscitativ
e
equipment
close by in
the event

of an
anaphylacti
c reaction
furosemide 06-26-10 30mg, IVP,
once a day
Edema due to heart
failure, hepatic
impairment or renal
disease.
Hypertension.
Decrease
blood
pressure,
increase
urinary
output,
decrease in
edema.
Clarify
doctors
order
Document
when drug
is given.
Check for
the 15 R’s
in giving
medication
s
Monitor
respiratory
status,
pulse, and
blood
pressure
frequently.
iii. Diet
Diet Date
Ordered
Date
Performed
Date
Changed
General
Description
Indication
or Purpose
Specific
Foods
Taken
Client’s
Response
to
Treatment
Nursing Responsibilities
NPO 06-17-10 Nothing per
Orem. This
means that
nothing
should be
eaten and
nothing will
be taken.
This diet
was also
prescribed
as a pre
and post
op diet
because
anesthesia
has
stopped
the gag
reflex and
None No
reaction
noted.
Prior:
Check the doctor’s
order.
Assure IV fluid
therapy if the
patient is NPO.
Instruct SO not to
give anything
through the mouth.
During:
Assure is nothing
is taken through

motility in
the GI
tract. Thus
if food is
introduced
through the
enteral
route there
is a high
risk of
aspiration
which may
even lead
to death.
the mouth either
liquid or solid.
Assess client’s
condition.
Place “NPO”signon
the bed where the
patient can see it
always.
Remove foods and
drinks on patient’s
side.
After:
Observe patient’s
response on the
diet.
Document the date
it was ordered and
implemented.
Full
Fluid
Diet
07-26-10 It serves to
provide
nutrition to
patients
who cannot
chew or
tolerate
solid foods
This diet is
given to
patients
who are
not able to
tolerate
solid foods.
Soup There is
risk for
aspiration
Prior:
Check the doctor’s
order.
Assure IV fluid
therapy
Instruct SO not to
give any solid food
through the mouth.
During:
Assure no solid
food is taken
through the mouth
Assess client’s
condition.
After:
Observe patient’s
response on the
diet.
Document the date it was
ordered and implemented.
iv. Activities
Activity Date
Ordered
General
Description
Indication
or Purpose
Client’s
Response
Nursing Responsibilities
to
Treatment
Flat on
Bed
06-25-10 Patient is
maintained
flat on bed
Before:
Educate the patient and SO
regarding the importance of
the activity.
Explain the purpose of the
activity.
Discuss to patient some of
the specific activities to be
avoided
After:
Provide health teachings on
the importance of activity.
Monitor patient’s reaction
and response to activity.
Turn the
patient
side to side
07-03-10 The patient
turns side
to side for
at least 2-4
hours.
To avoid
bed sores
and to
facilitate
proper
blood
circulation.
The patient
did perform
the said
exercise,
however
with limited
range of
motion.
Before:
Educate the patient and SO
regarding the importance of
the activity.
Explain the purpose of the
activity.
Discuss to patient some of
the specific activities to be
avoided
During:
Assist the patient in moving
about.
After:
Provide health teachings on
the importance of activity.
Monitor patient’s reaction
and response to activity.
VII. Client’s Daily Progress in the Hospital
Client’s Daily Progress Chart

Days Admission 07-01-10 07-20-10 Discharge
Nursing Problems:
1. Risk for
aspiration.
2. Ineffective
breathing pattern
related to pain.
3. Altered
Nutrition Less than
body requirements
r/t difficulty of
swallowing
٭
*
٭
٭
*
٭
*
*
Vital Signs
BP
PR
RR
Temp.
100/60mmHg
142bpm
21cpm
38.4˚C
115/72mmHg
111bpm
26cpm
37.5°C
100bpm
14cpm
37.5°C
Medical
Management
IVF:
D50.3NaCl
D5LR
D5IMB
Drugs/Medications
Diazepam
Paracetamol
Ceftriaxone
Phenobarbital
Mannitol
Meropenem
Furosemide
Diet
*
*
٭
٭
٭
٭
*
*
٭
٭
٭
٭
*
*
NPO
Full Fluid
Activities
Flat on Bed
Turn patient side to
side
*
٭
*
*
*
VIII. Learning Derived
With this undertaking, the student nurse is expected to carry out concepts
from the lectures and maximize the student’s responsibility to take care of his
patients as part of his Related Learning Experience in the Nursing Course
Curriculum.
Student nurse is expected to undergone, Physical Assessment, and other
health and patient related events with a review of the Nursing Care Management
100, 101, 102 and 103 Basics wherein the focus is to promote wellness and
health development from recent situational crisis, that the student nurse is
expected to accomplish the nursing process in carrying out the nursing plan of
care and interventions.
In studying the case, the student nurse get familiar to the different sign
and symptoms and the different clinical manifestations of the said condition. The
student nurse is also able to find out what are the predisposing and causative
factors that is resulting for the occurrence of the clinical disorder, the
procedures/test that can be done, for a deeper evaluation of the clients condition;
what are their purposes, and how it is done, and the plan of nursing care through
carrying out the doctors’ order, the nursing interventions and considerations.
The student nurse also learned and realized that in order to make a better
case study, one must focus in reviewing the clients’ history, do comprehensive
assessments and review related articles that may help you justified the
evidences of your case.
The student nurse is also growing with his experiences at the exposures wherein
the sense of being critically and logically were developed and he can now
comprehensively analyze health needs and the concerns of his patients who
endure to an existing health deficit and then do the care and other health-
related/promotive activities to develop the student nurse’s SKILLS,
KNOWLEDGE and ATTITUDE and values on health promotion and identification
and management of risk factors with due concerns on the nursing process.
The United Methodist Church Ecumenical Christian College
COLLEGE DEPARTMENT
Bachelor of Science in Nursing 4rd Year Group VI BATCH 2011
presents
Viral Encephalitis

A Case Study
Submitted By:
Dian Rei F. Musngi
Submitted To:
Ms. Gretchen ParasClinical Instructor
JECSON’S MEDICAL CENTER
AUGUST 4, 2010




![Clinical characteristics and long-term prognosis of ... · other possible causes, such as viral encephalitis and herpes simplex encephalitis. Relapsing anti-NMDAR encephalitis [5]](https://static.fdocuments.in/doc/165x107/5f5cb978af3eab35a02f3630/clinical-characteristics-and-long-term-prognosis-of-other-possible-causes-such.jpg)













