View slides
21
Joe Biegel VP, Product Management McKesson Medical Imaging Group October 23, 2007 Evolution of PACS as a Model to Predict Adoption of Digital Pathology
-
Upload
jared56 -
Category
Health & Medicine
-
view
323 -
download
1
Transcript of View slides

Joe BiegelVP, Product Management
McKesson Medical Imaging GroupOctober 23, 2007
Evolution of PACS as a Model to Predict Adoption of
Digital Pathology

A Brief History of PACS
1970’s1970’s 1980’s1980’s 1990’s1990’s 2000’s2000’s
Original concepts: Dr. T. Iinuma, “Image processing in clinical medicine – considerations of a system”, Bull., Tokyo Women Med. 44, 152 (in Japanese).
1974
Dr. Samuel J. Dwyer III describes PACS ideas at a Seminar at the University of Iowa. Dr. Judith M. Prewitt introduces the term PACS. Cardiovascular radiologist Dr. Andre Duerinckx describes the far reaching future benefits of PACS for a hospital.
1981
1st International Conference on the PACS, Newport Beach, California.
1982
US Army teleradiology project starts.
1983
Siemens/Philips start developing PACS concepts. EuroPACS starts annual meetings.
1984
US National Cancer Institute funds UCLA group under Professor Bernie Huang.
1985
Berlin BERKOM project started.
1986
PRIMIS created at VUB Brussels – to study applications of digital imaging.
1987
NATO conference in France includes topic on Imaging Networks. SCAR celebrates 10th annual meeting.
1990
US – Baltimore Veterans Hospital PACS.
UK – Hammersmith and Conquest PACS projects.
1992
Roger Baumann and Gunther Gell identify 23 large PACS worldwide with over 100 PACS projects.
1995
Baumann and Gell follow up survey – 177 large PACS identified worldwide.
2000
Multiple regional and national projects initiated. Worldwide mass adoption begins in earnest
2002

PACS Market Evolution
1990 20001985
Standards
TechnologyEnablers
Market
SolutionsOffered
ACR-NEMA
ACR-NEMA 2.0
IHE
DICOM + HL7
DICOM 3.0
Research PioneersEarly Adopters
Replacement
Mass Adoption
Single Modality Applications Departmental PACS Enterprise RIS/PACS
Multi-Modality Viewing Apps Departmental RIS/PACS
HSM Systems
NAS / SAN
Storage H/W $
Hi-Res Displays
Affordable UNIX workstations
Optical Storage Media
9-track tapes
Mainframe Computers Voice Recognition
Optical Storage Jukeboxes
TCP/IP adoption

The Evolution of Imaging IT Market Segments
1990 20101985 2000
RadiologyPACS
Market
Research PioneersEarly Adopters
Replacement
Mass Adoption
CardiologyPACS
Market
Research Pioneers
Replacement
Early Adopters
Mass Adoption
OpticalImaging
Research PioneersEarly Adopters
Mass Adoption
Replacement

Historical Radiologist Workflow
Early Perceived Value
Radiologist Workflow with RIS/PACS
Rad bar codes requisition into
dictation system
1Clerks/Tech match up films to be read
with patient’s master jacket
Films with masters are delivered to Radiologist
Is there previous in
master
Rad hangs films on view box
Rad hangs previous for review
Rad enters MRN into RIS,
finds patient, reviews results
No
Rad bar codes requisition into
dictation system
Rad dictates patient name, order, and accession
number in dictation system, and dictates report
Rad places films back into daily folder and
signs bag
Rad places signed daily with patient
master jacket aside for pickup by clerical staff.
1
Rad opens unread worklist on PACS in
dictate mode and opens first exam to be read
Rad clicks on clinical history icon to review patient’s reports and results from HIS/RIS
Dictation automatically initiated. Order information from the RIS automatically sent to dictation system.
Relevant prior studies automatically
display
Rad dictates report, and clicks next study
Patient and order level information sent from PACS
to RIS with no patient search required
Next study is loaded. Dictation is initiated, and
previous exam is marked dictated in PACS
1
1

Pathology progress, as compared to Radiology
The evolution of Digital Imaging in Radiology offers significant lessons for Pathology
Parallels with a later start, … but likely faster progress─ Radiology in 1995 vs. Path in 2005
─ Radiology today vs. Path in 2010
Moore’s law helps No need to repeat the same pitfalls
Source: Bruce Beckwith, MD – 2005 DICOM International Conference – Budapest, Hungary

Radiology c. 1995 -vs- Pathology c. 2005
RadiologyRadiology PathologyPathology
Analog image capture Analog image capture or no image capture
Single modality to multi –modality focus Single modality
DICOM standards- early formation of IHE Emerging standards
Separate workflows – RIS, Reporting, Separate workflows – APLIS, Reporting
Radiology focused Images hard to interpret for non pathologists
Storage needs seem overwhelming Extreme storage needs
Digital Imaging is more expensive than analog
Digital Imaging costs money
“Island” workflow Unstructured, collaborations, distribution
Most of spending is still on film Modest budgets

Radiology Now -vs- Pathology in 2010
RadiologyRadiology PathologyPathology
Digital Acquisition is standard Digital acquisition growing
Automatic meta-data capture Streamlined image capture with metadata
CAD assists Radiologist’s interpretation CAD interpretable portions
Many patient requests Large transactions per study
Large and constantly growing storage needs
Large storage needs, but cost barrier decreasing
Digital imaging saves money, and is required to make money
Digital pathology adds value and is required to make money
Large budgets Budgets expand into IT space
Radiology outside the dept. of Radiology walls
Remote pathology, protocols, strong links to clinical practice.

Driving adoption is key
Automating the current workflow is only the first step─ Both physical slide based workflow and digitized slide workflow will
co-exist for a long time
─ Metadata (ie. patient demographic info, block/slide info) needs to be assigned to digitized WSI images
─ Manual data entry must be minimized whenever possible if WSI technology is to be incorporated into and ultimately replace existing physical slide based workflow
Economic drivers of digital pathology are evolving─ Factors from outside the department will dominate
─ Standard of care, costs & reimbursement are the keys
Solution requirements will also evolve

01010101010
1010
1010
1010
110
1010101010101010101
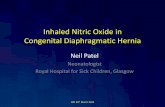
Pathology WorkflowPresent & Future
Source: Sourav Ray MD, et al: CAP, 2006
Metadata Annotation
Engine
Histology Laboratory
Physical Slides
Slide Storage
PACS10101010101
101010111011
10110101010101010
101010101
0101010101010101010010101010101010101010101101010101010101010101010101010101
10110010101010101010101010101
101010101010101010
10110010101010101010101101010101010101010
101010101
10101010101
101010110100101010101010101010
10101101
10110010101010101101010110100101010101010101010101010
10101010101010101010101010101010
10101010101010101010
Gross Specimen Pathologist Orders: Recuts,
Levels, IHC/Special Stains, Ancillary Studies
WSI unique ID # for each WSI slideH&E Data, IHC Data,
Flags, CommentsWSI or not WSI?
Block Data, Gross Description,
Gross Images
Cassettes/Blocks
3rd Party Whole Slide Imaging (WSI) Apparatus
Load with WSI Unique Slide ID#
Patient Block Slide Data attached to WSI Unique ID#
Digitized Whole Slide Images (WSI) attached to WSI Unique ID#
Annotated Whole Slide
Images (WSI)
Region of Interest (ROI) jpeg images (Direct Operation 3rd Party Imaging
Apparatus)
Request WSI Images Via WSI unique ID#
Request ROI Images
WSI Images as requested per case
Orders
Patient/Case/Block Data, Prior Reports,
Images (ROI) and WSI)
APLIS Remote Operation 3rd Party Imaging
Apparatus (TWAIN)
Region of Interest (ROI) jpeg Images
Physical Slide
Analog Optical Image

Future Pathology Workflow
The vision of automating the current workflow is a noble goal, but it is only the first step─ The true value of Digital Pathology will have to be
defined in terms of faster, improved Patient Care
Going Digital will change the practice of Pathology and will lead to a new, yet undefined workflows─ Standards, IHE will help: necessary but insufficient to
drive wide-scale adoption

DICOM in Pathology
Visible Light Supplement 15─ Included support for gross images, microscopic
images, x,y.z position, lab accession numbers
Working Group 26─ Evolving to include whole slide imaging
Growing number of imaging products targeting pathology are DICOM compliant
US Veteran’s Administration:─ Pathology imaging vendors must be DICOM
compliant

IHE-J in Pathology – Workflow/Data Structure
OrderSample
Macro Image
Slide
Block
Sample
Sample
Slide
Slide
Study Series Image
Block
Source: Tofukuji * Okuno – 2005 IHE –Japan Pathology WG

Diagnostic Imaging Cockpit = ‘vision’ under pressure
Diagnostic Imaging CockpitDiagnostic Imaging Cockpit
Departmental PACS diagnostic tools
Collateral content
3D, Fusion, CAD
Orthopaedic extensions
Enterprise Worklist
Departmental management &
reporting tools
EMR Integration
Voice Recognition
Structured Reporting: eg OB,
ER discrepancy & critical results
reporting

A
B A
B
Worklist & Case History
Gross / Low Res.Image Analysis
Digital Slides Report
This is an example text bocks for the gross image shown above. This text is so small that it is unlikey that anyone can read it. Can you? I really doubt it.
This is an example text bocks for the gross image shown above. This text is so small that it is unlikey that anyone can read it. Can you? I really doubt it.
Source: Aperio Technologies
The Pathology “Cockpit” – current focus

Pathology Next stage
Pathology CockpitPathology Cockpit
Advanced diagnostic tools
3D, Fusion, CAD
Muti-spectral imaging
Test sub-routines (histology, etc.)
Enterprise Worklist
Departmental management &
reporting tools
EMR Integration
Voice Recognition
Structured Reporting
Critical findings / ER ??
Departmental Productivity Reporting

Synergies with Diagnostic Imaging
Leverage image management infrastructure
─ Cost and expertise synergies will speed adoption
Routine access will likely create clinical use cases which will drive the adoption
─ The extent to which these use cases impact outcomes will impact market acceleration
Access needs vary─ Pathologists want access to
diagnostic image data─ Radiologists have interest in
access to summary data and no interest in WSI access

Value Points = Business Control Points
Modality = Data Acquisition Storage = Physical Storage Devices (H/W) Image Access Points = Clinical Application(s) Workflow = Order $ Data = Data-mining CAD – address the volume – may be more
formative than in Radiology Financial benefit needs to become more clear

Organic evolution is a slow, painful process with many side-tracks
Integration and interoperability with other systems is key to adoption
─ Isolated systems, IT-silos are short-lived, with limited clinical benefits
Don’t repeat the evolutionary sidetracks from the history of other clinical disciplines…
Use PACS as a starting point and build on it !!

Summary
Pathologists need PACS now─ value is immediate─ Pathologists should have PACS access now – the patient record
needs to contain relevant imaging data
If you want to accelerate the adoption-curve of digital pathology:
─ ‘Hook’ your digital Pathology plans to your PACS
It is likely that early workflows will leverage other specialties, BUT these will inevitably be transient solutions with the “real” Digital Pathology workflow to follow
─ Pathology dept specific workflow solutions are needed and must have digital path imaging as part of the workflow now.

Questions?Questions?