Vertebroplasty presentaion
15
Ramsin Benyamin, MD, DABIPP, FIPP The most rewarding intervention: Vertebroplasty Disclaimer President/Medical Director, Millennium Pain Center, Bloomington, Illinois Medical Director, Millennium Pain Center, Chicago, Illinois Medical Director, OSF Millennium Pain Center, Normal, Illinois Co-founder, Millennium Pain Management-Teknon Medical Center, Barcelona, Spain Clinical Assistant Professor of Surgery, College of Medicine, University of Illinois, Urbana/Champaign Adjunct Professor, Department of Biological Sciences, Illinois State University President-Elect, ASIPP Board of Directors, SIPMS Board of Examiners, ABIPP Board of Examiners, FIPP Member, Guidelines committee, ASIPP Member, Research committee, ASIPP Associate Editor, “ Pain Physician” Editorial Board, “ Pain Practice” Editorial Board, “Journal of Opioid Management” Scope of the problem Osteoporosis epidemic: - 200 million worldwide - 40 million in USA Women over 80: - 80% osteoporosis - 40% VCF 9x increased mortality Cauley et al, Osteo Intern, 2000 Self-care assistance: >50% of 1-2 VCF (8% in OA/LBP ) One VCF: 19.2% Two VCF: 24% more chance of another VCF in next year Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm 1
-
Upload
jjmclaughlin246 -
Category
Education
-
view
616 -
download
1
Transcript of Vertebroplasty presentaion

Ramsin Benyamin, MD, DABIPP, FIPP
The most rewarding intervention:
Vertebroplasty
DisclaimerPresident/Medical Director, Millennium Pain Center, Bloomington, IllinoisMedical Director, Millennium Pain Center, Chicago, IllinoisMedical Director, OSF Millennium Pain Center, Normal, IllinoisCo-founder, Millennium Pain Management-Teknon Medical Center, Barcelona, Spain
Clinical Assistant Professor of Surgery, College of Medicine, University of Illinois, Urbana/ChampaignAdjunct Professor, Department of Biological Sciences, Illinois State University
President-Elect, ASIPPBoard of Directors, SIPMS
Board of Examiners, ABIPP Board of Examiners, FIPP
Member, Guidelines committee, ASIPPMember, Research committee, ASIPP
Associate Editor, “ Pain Physician”Editorial Board, “ Pain Practice”Editorial Board, “Journal of Opioid Management”
Scope of the problemOsteoporosis epidemic: - 200 million worldwide
- 40 million in USA
Women over 80: - 80% osteoporosis
- 40% VCF
9x increased mortality Cauley et al, Osteo Intern, 2000
Self-care assistance: >50% of 1-2 VCF (8% in OA/LBP )
One VCF: 19.2% Two VCF: 24% more chance of another VCF in next year
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
1

Most common risk factors
Oral glucocorticoid use
Early menopause
Unintentional weight loss and malnutritionOther factors
20%10%
36%34%
Tannenbaum C et al. J Clin Endocrin Metab. 2002
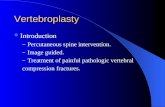
Risk of fracture from steroid use
Van Staa TP et al. J Bone Miner Res. 2000
Ris
k of
ve
rteb
ral f
ract
ure
Oral glucocorticoidusers
(n=244,235)
Age- and gender-matched controls
(n=244,235)
• 2.6-fold increase
1 2 3 4 5 6 7 8
Fracture prevalence (%)
T4T5T6T7T8T9T10T11T12L1L2L3L4
Incidence of vertebral fractures in spine
Nevitt MC et al. Bone. 1999
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
2

Consequences of VCF
Pain
ImmobilityKyphosis
More Compression
Opioid dependence
Impact of ImmobilityOsteoporosis(loss of BMD): 2% per weekMuscle wasting: 1-3% per dayLoss of Strength : 50% in 3-5 weeksConstipation, loss of appetite, fecal impactionDepression/ anxietyDecubitus ulcers: 70% in 2 weeks (70& older): 50% more nursing cost
UTI/ calculiLow FVC: 9% with each VCFAtelectasis, less effective coughing, reduced cilliaryclearance: 25-50% reduced inspiration: PneumoniaDVT: 61% in bed rest: PE in 2-12%: 0.5-10% fatal
Benefits of Vertebroplasty
Pain Relief Quick & Complete• Osteoporotic
75-90% complete relief of pain (immediately or within 72 hours)
• Neoplastic59-86% complete relief of pain ormarked reduction in opioids
Improved Mobility• within 24 hours, reduced AE (cost) in elderly Brown et al, JAmGerSoc,2004
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
3

Position Statement· American Society of Interventional and Therapeutic Neuroradiology
· Society of Interventional Radiology· American Association of Neurological Surgeons/Congress of Neurological Surgeons
· American Society of Spine Radiology
Percutaneous vertebral augmentation is a safe, efficacious, and durable procedure
in appropriate patients with symptomatic osteoporotic & neoplastic fractures
“Benefits far outweigh its risk and the risk of conservative therapy”
Jensen et al, Position Statement, JVIR, 2007
Vertebroplasty, First 1000 Levels of a Single Center: Evaluation of the Outcomes and Complications
Layton KF, Thielen KR, Koch CA, Luetmer PH, Lane JI, Wald JT, Kallmes DF, AJNR 2007
Layton KF, Thielen KR, Koch CA, Luetmer PH, Lane JI, Wald JT, Kallmes DF, AJNR 2007
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
4

Percutaneous Vertebroplasty for Painful Compression Fractures in a Small Cohort of Patients with a Decreased
Expectation-Related Placebo Effect due to Dementia
METHODS: 10 patients with dementia who had vertebroplasty
RESULTS: Pain with activity decreased or resolved in 80%-100% of patients at each time point, whereas pain at rest decreased or resolved in 78%-100% of all patients at each time point. Improved mobility was reported in 80%-100% of patients at all time points. Pain medication was decreased or stopped in 67% of patients at 1 week and in 100% of patients at 6 months and 1 year.
CONCLUSION: Treatment of painful compression fractures in patients with dementia demonstrates a high rate of success regarding pain relief and mobility. This study offers additional evidence that vertebroplasty has true benefit.
Lehman VT, Gray LA, Kallmes DF , AJNR Am J Neuroradiol. 2008 Jun 12
Vertebroplasty in multiple myeloma: outcomes in a large patient series
Significant improvement in:rest pain (82%) and activity pain (89%) 65% of patients requiring fewer narcotics 70% having improved mobility
Vertebroplasty provides significant & durable pain relief
McDonald RJ, Trout AT, Gray LA, Dispenzieri A, Thielen KR, Kallmes DF, AJNR 2008
Repeat vertebroplasty for unrelieved pain at previously treated vertebral levels with
osteoporotic vertebral compression fractures
Out of 334 procedures, 15 patients with unrelieved pain in 4 to 32 days after an initial PV
Complete pain relief in 11 (73%) and partial pain relief in 4 patients (27%), in a mean follow-up of 15 months
Absent or inadequate filling of cement may be responsible for the unrelieved pain after the initial PV
He SC, Teng GJ, Deng G, Fang W, Guo JH, Zhu GY, Li GZ, Spine, 2008
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
5

Indication“Painful Compression Fracture”
Osteoporosis, Trauma, CancerAcute, Sub-acuteNot totally collapsedNo (significant) retropulsionPain consistent with imaging
Exam under FluoroscopyEstablish diagnosisEvaluate the view, fractureDecide feasibility: fluoro / CTPlan the approach (? fractured peddicle)Do NOT be a maverick!
Preparation
Antibiotics: systemic
Positioning: padding, self-positioning
Anesthesia: MAC + local
Strict sterile technique
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
6

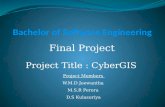
Image Guidance
High-quality fluoroscopy• Biplane• Single plane• C-arm
CT and fluoroscopy
Love the Dog!
Discography and Intradiscals Facet Joint
Medial Branch
Epidural or Intrathecal
Transforaminal
Vertebroplasty
Final needle position
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
7

Vertebral Venous Plexus
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
8

Posterior leakage
Rarely symptomatic
May require SxIntradural leakage
Too medial??
Massive Pulmonary Edema
•Insufficient polymerisation of the injected cement, probably due to an unbalanced monomer-to-powder ratio?•3 levels (T12, L1 & L2)•15 ml retrieved
Monticelli, Forensic Sci Int, 2005
More cases
Aortic embolism!: Breast Ca. 6ccRight Laterovertebral artery
Asymptomatic Amoretti, Skeletal Radiol 2007
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
9

L4 radiculopathy Pedicle fracture
No cement in the vertebrae!!!
Baumann C. Cardiovasc Intervent Radiol, 2007
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
10

Safe Deposit Area!
Trans-Pedicular approach
Vertebroplasty
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
11

Hammer!
Too far medial Too far lateral
Blind Spots !
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
12

Bi-pedicular technique
Cement injection
Radio-opaque: 30% BariumAdequate curing time: “tooth-paste”Real-time fluoro in lateralVolume of cement: 2-4ml- not correlated with pain relief- not correlated with strengthening
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
13

Final X-Ray
Finally……..
Vertebroplasty vs. Kyphoplasty
Clinical response rate is similarNo proven advantage of Kyphoplasty in:- Pain relief
- Height restoration - Complication rate
Position Statement, J Vas Interv Radiol, 2007:American Society of Interventional and Therapeutic NeuroradiologySociety of Interventional RadiologyAmerican Association of Neurological Surgeons/Congress of Neurological SurgeonsAmerican Society of Spine Radiology
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
14

EvidenceASIPP Guidelines, 2007
Level of evidence is Moderate
Final Comments
Best suited: Interventional Pain Physician (Anesthesia, PM&R, IR, Surgeon)
Not : Part-timers (Anesthesiologist, Radiologist, Spine surgeon)- Comprehensive clinic & follow-up
- Fluoroscopy/percutaneous
- Resuscitation skills
Physicians (not marketplace): determine patient selection criteria
It’s not the procedure that changes the outcome, it’s the operator
Thanks!
Midwest Pain Society Presentation 2C - Ramsin Benyamin, MD September 19, 2008 3:45 pm
15