Ventilator associated pneumonia - Critical Careold.criticalcare.org.za/images/presentations/Omolemo...
21
Ventilator Associated Pneumonia Omolemo Kitchin Steve Biko Academic Hospital
-
Upload
phungkhuong -
Category
Documents
-
view
215 -
download
3
Transcript of Ventilator associated pneumonia - Critical Careold.criticalcare.org.za/images/presentations/Omolemo...

Ventilator Associated Pneumonia
Omolemo Kitchin
Steve Biko Academic Hospital
Conflict of interest
Nothing to Declare
Outline
Case presentation
Diagnosis and diagnostic dilemma
Prevention
Treatment
What about VAT?
Conclusion

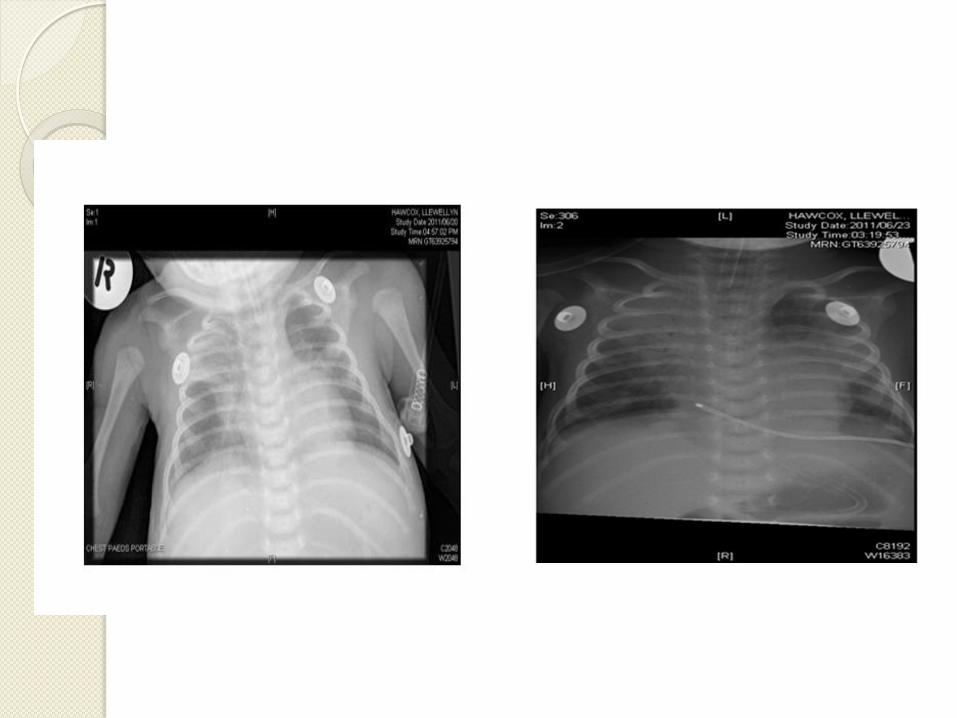
1/12 old ex-prem
Bronchiolitis
NPA- RSV
Ventilated for respiratory failure and
apnoea


48hrs after admission
Temperature increased, Wcc increased
Tachypnoea with increase in ventilator
support
Worsening chest radiograph
Blood cultures negative
Ex-tubated and discharged after 17days
(12 in PICU)

Diagnosis/Dilemma
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009

Diagnosis/Definitions
Early VAP(1-4days), late VAP(>4days)1
CPIS -no validation in paediatrics(level D)
-Points:0-2
-temperature, Wcc, tracheal aspirates, PF ratio, CXR,
semi quantitative tracheal aspirate culture.
-Score of>6 high probability of VAP
http://cd-c.gov/nhsn.1 Last accessed Jul 2011
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009

Chest radiograph-clinical suspicion( level
B)[3500 PICU pts, non-randomised]
Microbiol and clinical-B/C, BAL(level B)
Infection markers-Wcc, neutrophils,
PCT(level D)
Sputum production, WOB, auscultation-
(level D)
Fever-(level D)
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009

Diagnostic dilemma of VAP in critically
ill children(systematic review)
Gold Std-direct exam and lung tx culture
Clinical criteria: poor sens and spec vspathology
CPIS vs pathology(sen 72.7% & spec 42-85%)
Radiology: specificity(33-42%)air bronchograms, infiltrates (sens50-78%)
Microbiol: NBAL & autopsy(sen & spec 100%, n=17)
NBAL compares to BBAL
Tracheal Aspirates-low spec
VenkatachalamV, Hendley OJ, Wilson DF. Pediatr Crit Care Med 2011;12:286-96

Prevention
Infection control: hand, environmental
decontamination (level A)
Bundle approach
-Level A
peptic ulcer prophylaxis(not PICU)
Sedation vacation/readiness to extubate
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009

Level B
-Head of bed elevation
-In line suctioning(meta analysis)
-Closed system suctioning did not affect the
frequency of VAP or patient outcome1
-Oral hygiene :level B
twice daily electric tooth brushing
+chlorhexadine oral rinse vs just oral rinse:
no reduction in VAP (OR 0.78 CI 0.36-1.68)2
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009
Morrow BM, Mowzer R, Pitcher R,Argent AC. Pediatr Crit Care Med 2011, Jan 28[Epub ahead of print]1
Rello J et al. Intensive Care Med 2007;33:1066-702

Level D
-Post Pyloric feeds
-DVT prophylaxis
-Orotracheal vs nasotracheal intubation
Morrow BM, Argent AC, Jeena PM, Green RJ. SAMJ 2009

OTHERS
Ventilator circuit changes
-2 Paeds studies (n=575)
-1 Adult meta analysis(n=19,169)
-7day changes does not increase VAP’
Nurse led VAP surveillance(UK)
-VAP incidence=5.6/1000 ventilator days1
Han J, liuY. Respir Care 2010;55:467-74
Hsieh TC et al. Pediatr Neonatol. 2010;51: 37-43
Samransamruajkit et al. J Crit cAre 2010; 25:56-61
Richardson M, Hines S, Dixon G et al.1J Hosp Infect. 2010;75:220-4

Treatment
Delay in starting assoc with poor
prognosis
Consider resistance pattern of pathogens
in your hospital
Choose wisely, Start early, hit hard with
the correct dose
Deescalate rapidly, stop abruptly.
Early tracheostomy: Adult-equivocal
:No Paediatric studies Paed Crit Care Med 2011;12:286-296
SAMJ2009

What about VAT?
Adult incidence=10%
Paediatrics ?( 1 study =1.8%)
Diagnostic criteria
-Fever, no recognizable cause
-Purulent sputum production
-(+) endotracheal aspirate culture
-no radiological evidence of pneumonia
Nseir S, Ader F, Marquette CH.Curr Opin Infect Dis 2009;22:148-53

Is it a problem in Paediatrics?
If so, will treating it decrease VAP?
Will the bundles work?
Current study in Ohio-factors assoc with
VAT development and reduction of VAT
rates.
Lee AY, Brilli RJ. Pediatr Crit Care Med 2011;12:357-8
Conclusion
Diagnostic methods are inadequate
Clinical criterea is ambiguous
Gold Std not routine in children
CPIS+NBAL+radiology!
Discretional use of antibiotics
Prevention-Bundles

http://gobblegreen.com/blog/wp-content/uploads/2009/07/wash-hands-cartoon1.jpg

Acknowledgements
Prof Robin J Green
Prof Refiloe Masekela
Dr Marian Kwofie-Mensah
Dr Carla Els
Dr Debbie White
Dr Jeane’ Cloete
Dr Salome Abbot
Sr Zulu and PICU staff











![Pneumonia (Ventilator-associated [VAP] and non-ventilator ...](https://static.fdocuments.in/doc/165x107/61c3dfa934191a172140c0d5/pneumonia-ventilator-associated-vap-and-non-ventilator-.jpg)