Regulation of Ventilation, Ventilation/Perfusion Ratio, and Transport
Upload
lindsey-weaverCategory
view
277download
2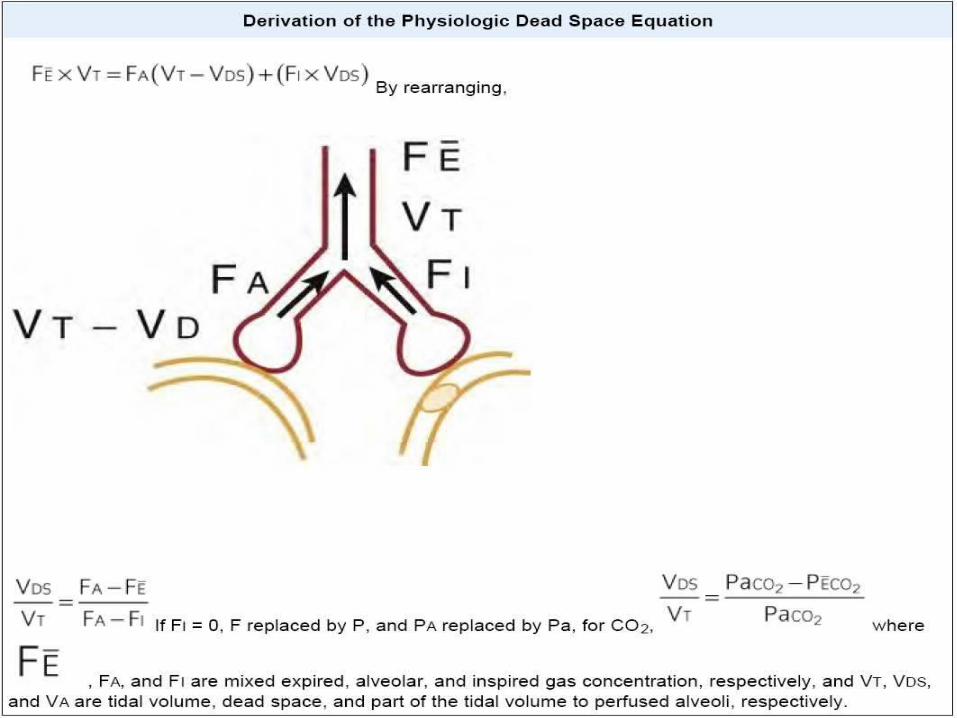
Ventilation-Perfusion Mismatch Optimum gas exchange: Ventilation and perfusion must match each other in all lung regions.
Mean ratio of approximately 1 somewhere in the middle of the lung Range of ratios from 0.5 in the bottom of the lung to 5.0 in nondependent
way of showing the matching :
multicompartmental analysis by a multiple inert gas elimination technique : (MIGET)
PAO2 - PaO2 ~ 3 to 5 mm Hg (0.4 to 0.7 kPa)
More V/Q mismatch, the PAO2 - PaO2 difference is further increased
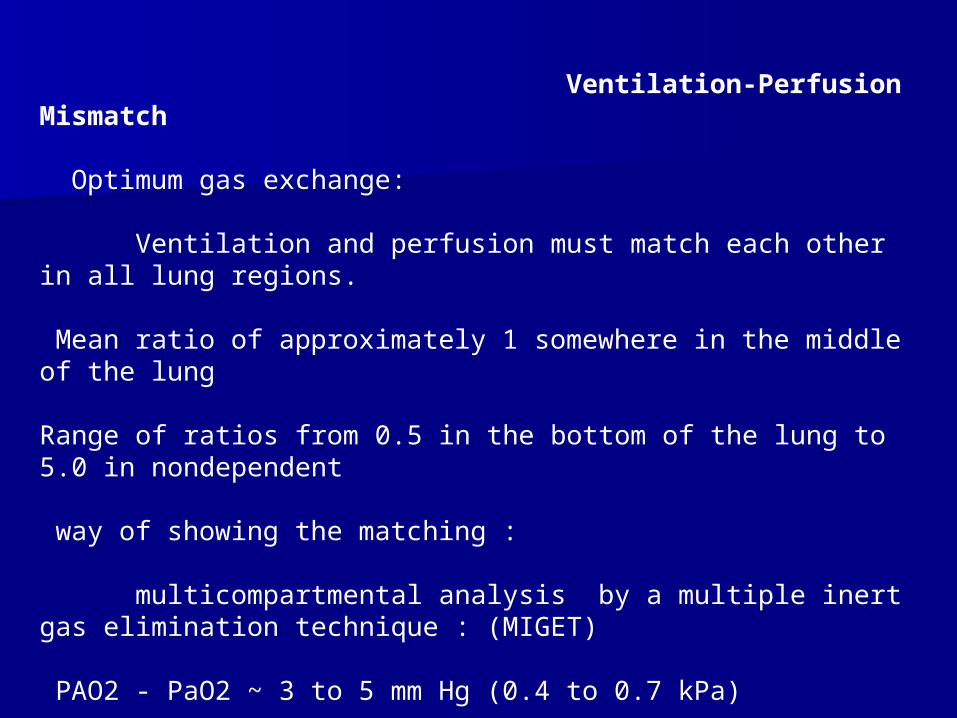
Impaired Diffusion
Reduces PaO2 can occur if the alveolar-capillary membranes are thickened: fibrosis systemic vascular diseases
Right-to-Left Shunt
2% to 3% of cardiac output in normal
In pathologic states, between nearly normal to above 50% of cardiac output Shunt increases to 25%, the rise in PaO2 will be small by giving O2 With a shunt of 30% or greater, almost no effect of added O2 can be seen
Respiratory Function During Anesthesia
Anesthesia causes an impairment in pulmonary function either:
Breathing spontaneously or
Ventilated mechanically
FIO2 is maintained at around 0.3 to 0.4.
Despite these measures : Mild to moderate hypoxemia: O2 Sat 85% to 90% ~half of all patients undergoing elective surgery . Last few seconds to up to 30minutes.
In about 20% of patients O2 Sat below 81% for up to 5 minutes
postoperative clinically significant pulmonary complications : 1% to 2% after minor surgery up to 20% after upper abdominal and thoracic surgery

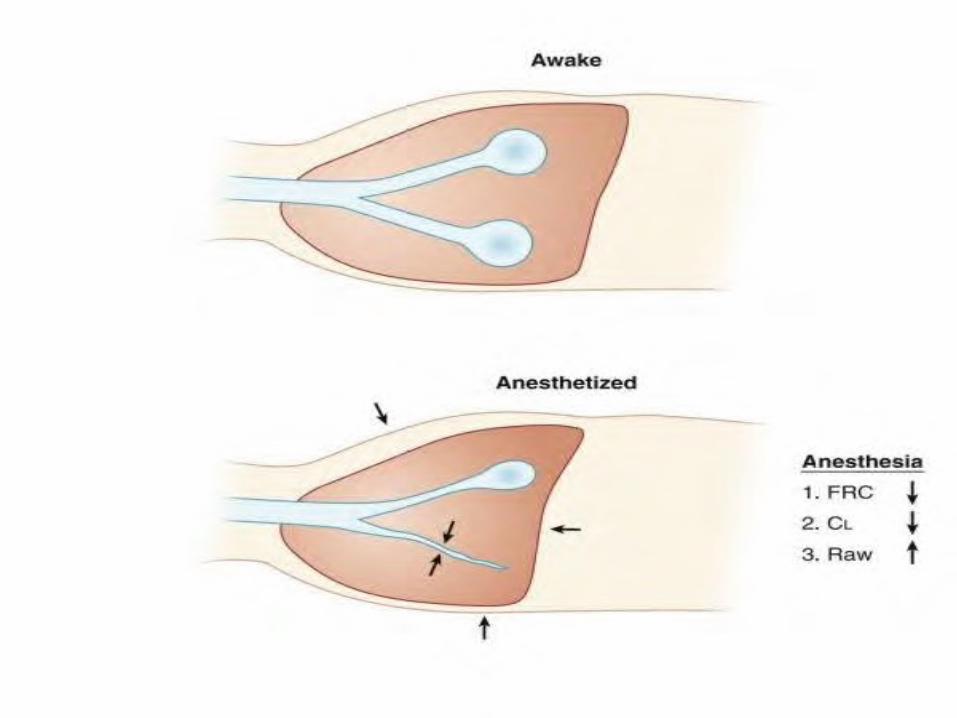
Lung Volume and Respiratory Mechanics During Anesthesia
Lung Volume
FRC, is reduced by 0.8 to 1.0 L from upright to supine 0.4- to 0.5-L decrease when anesthesia has been induced So,End-expiratory lung volume is reduced from approximately 1.5 to 2 L
Muscle paralysis and mechanical ventilation cause no further decrease in FRC.
Compliance and Resistance of the Respiratory System
Static compliance(total) is reduced :
From 95 to60 mL/cm H2O during anesthesia.
Static lung compliance : From a mean of 187 mL/cm H2O awake to 149 mL/cm H2O during anesthesia
The possibility increased lung resistance :merely reflects reduced FRC during anesthesia
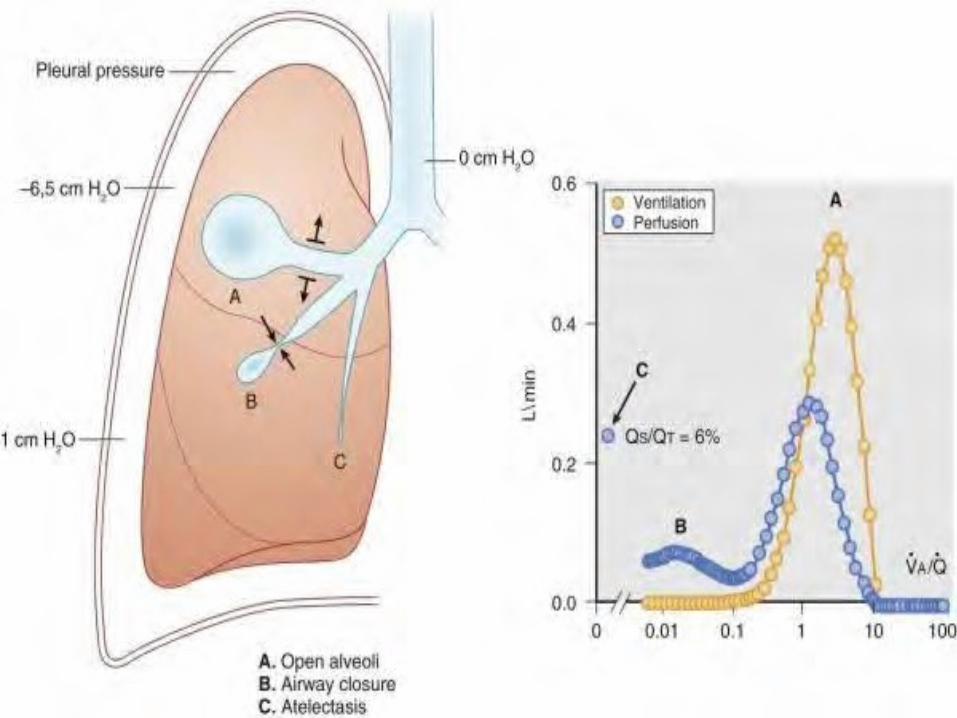
Atelectasis and Airway Closure During Anesthesia Atelectasis :
Atelectasis could not be shown on conventional chest radiography
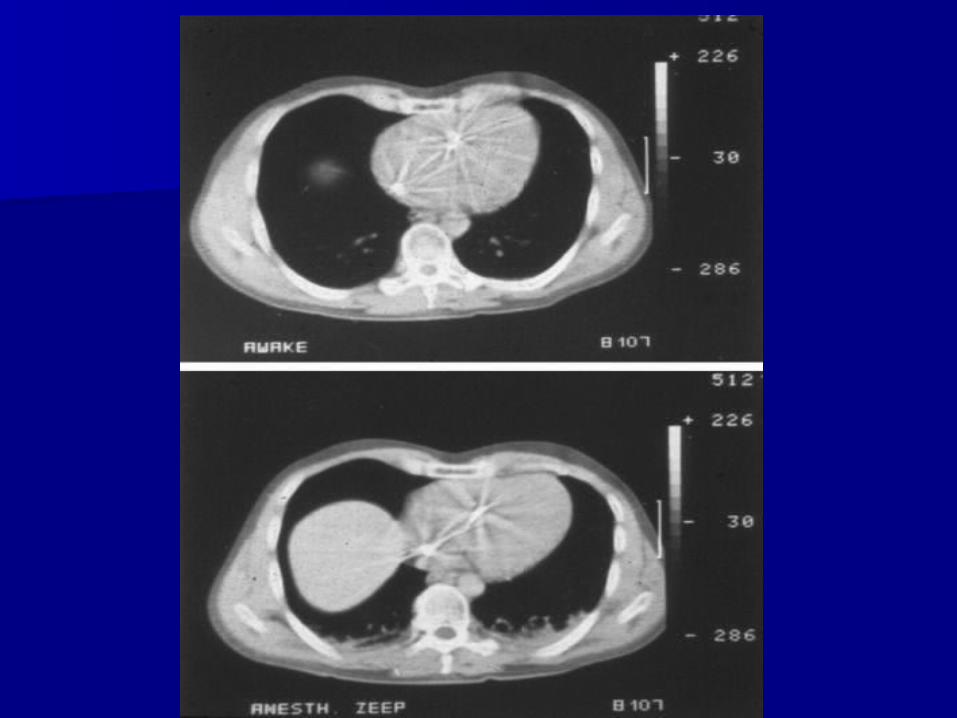
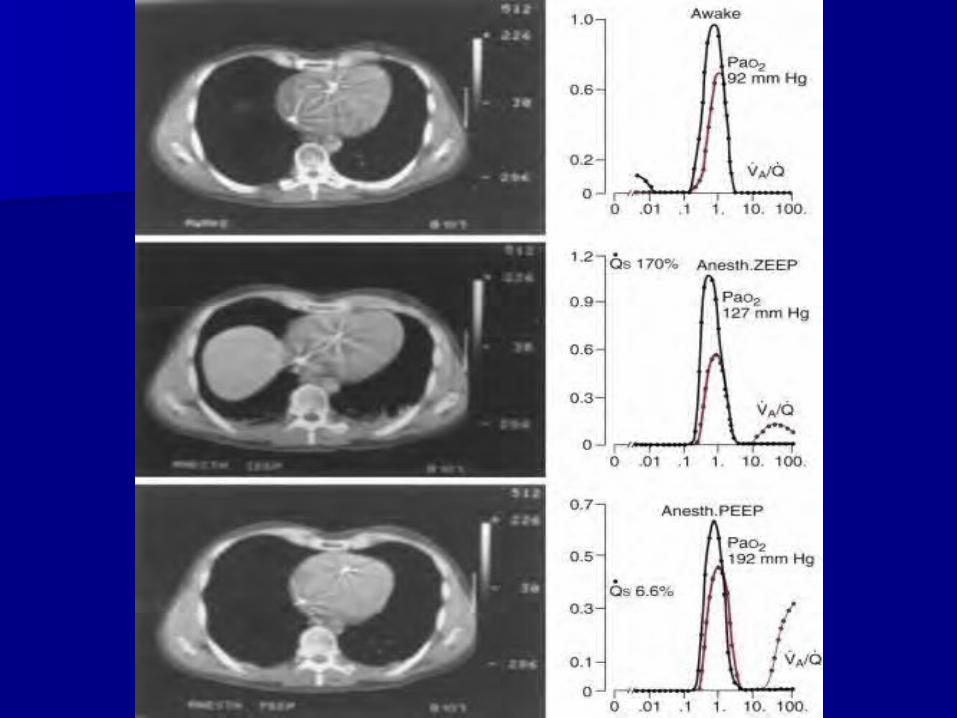
On CT with transverse exposure of the chest: Development of densities in the dependent regions shown during anesthesia
Atelectasis appears in approximately 90% of all patients who are anesthetized.
15% to 20% of the lung is regularly collapsed at the base of the lung during uneventful anesthesia
After thoracic surgery and cardiopulmonary bypass: More than 50% of the lung can be collapsed even several hours after surgery.
There is good correlation between the amount of atelectasis and pulmonary shunt as measured by MIGET.
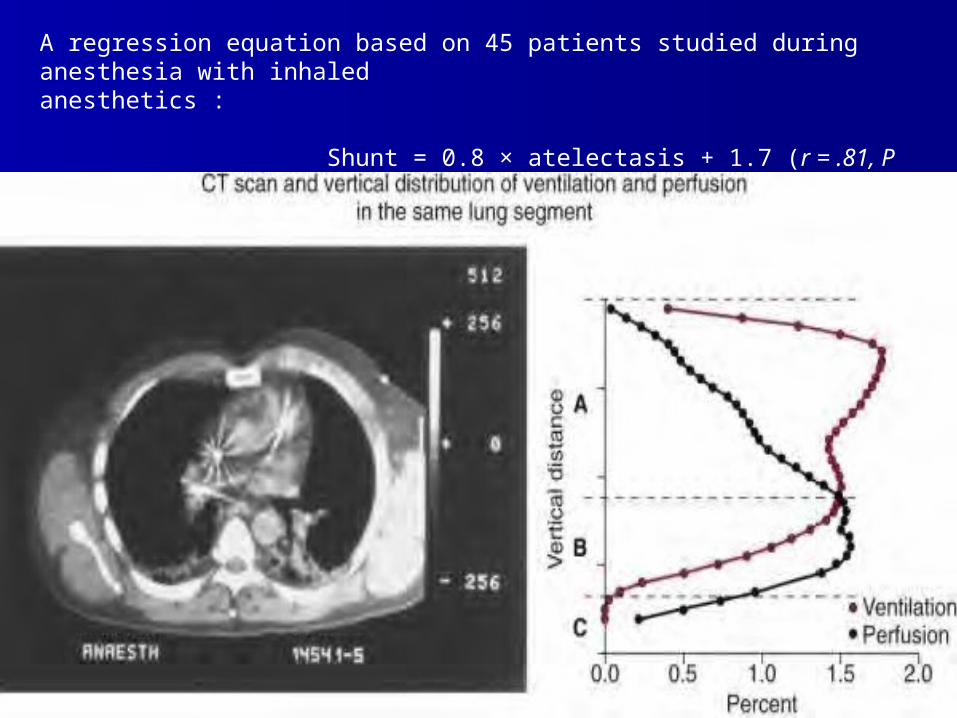
A regression equation based on 45 patients studied during anesthesia with inhaled anesthetics : Shunt = 0.8 × atelectasis + 1.7 (r = .81, P < .01)
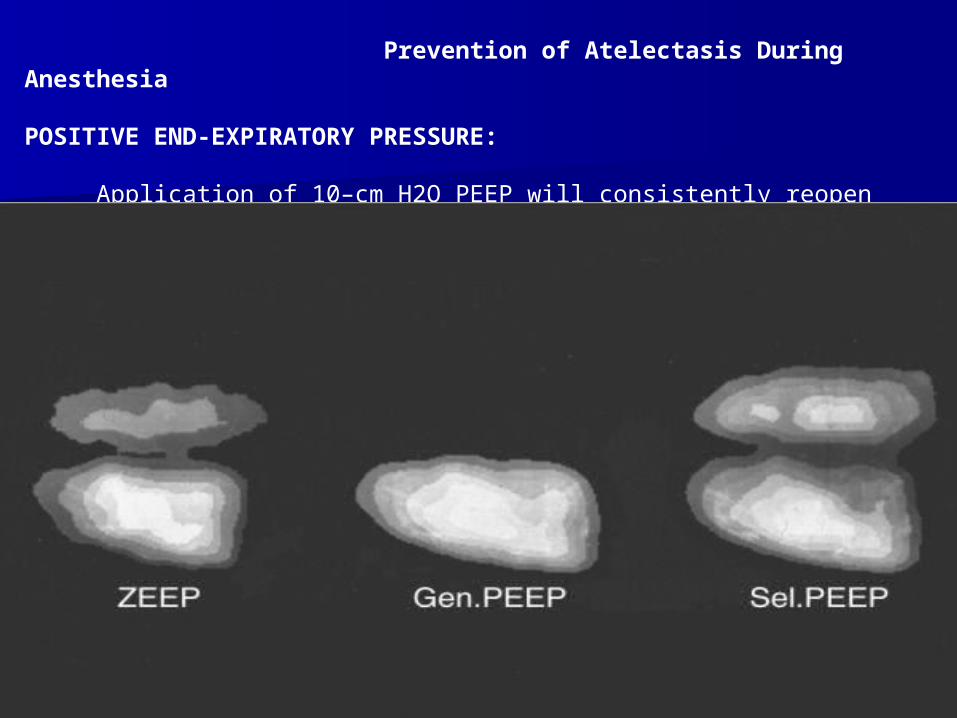
Prevention of Atelectasis During Anesthesia
POSITIVE END-EXPIRATORY PRESSURE:
Application of 10–cm H2O PEEP will consistently reopen collapsed lung tissue.
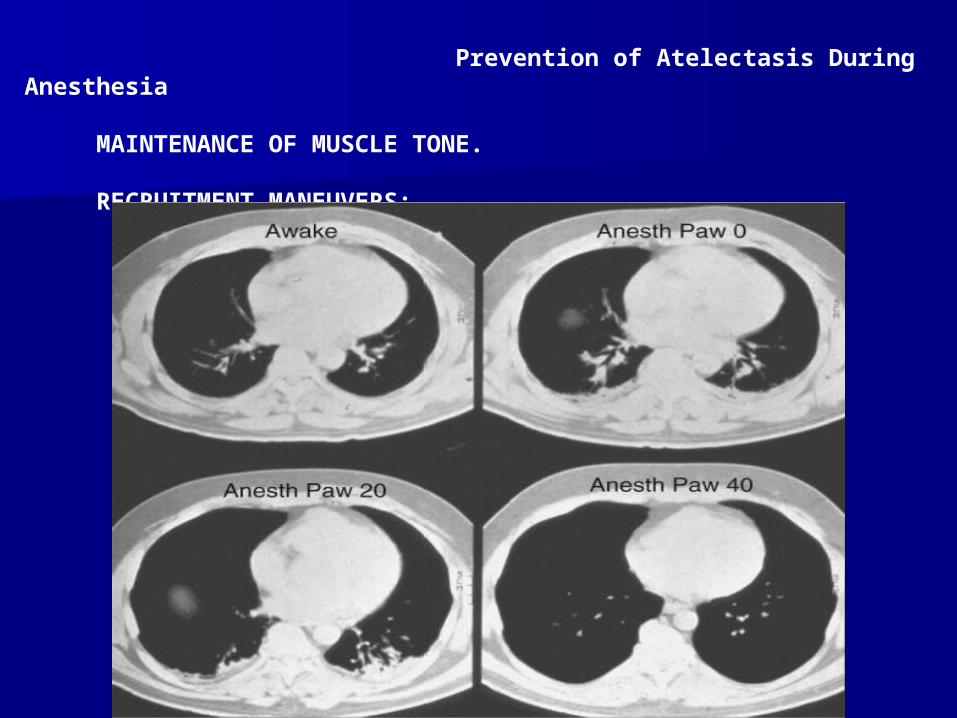
Prevention of Atelectasis During Anesthesia
MAINTENANCE OF MUSCLE TONE.
RECRUITMENT MANEUVERS:
Prevention of Atelectasis During Anesthesia
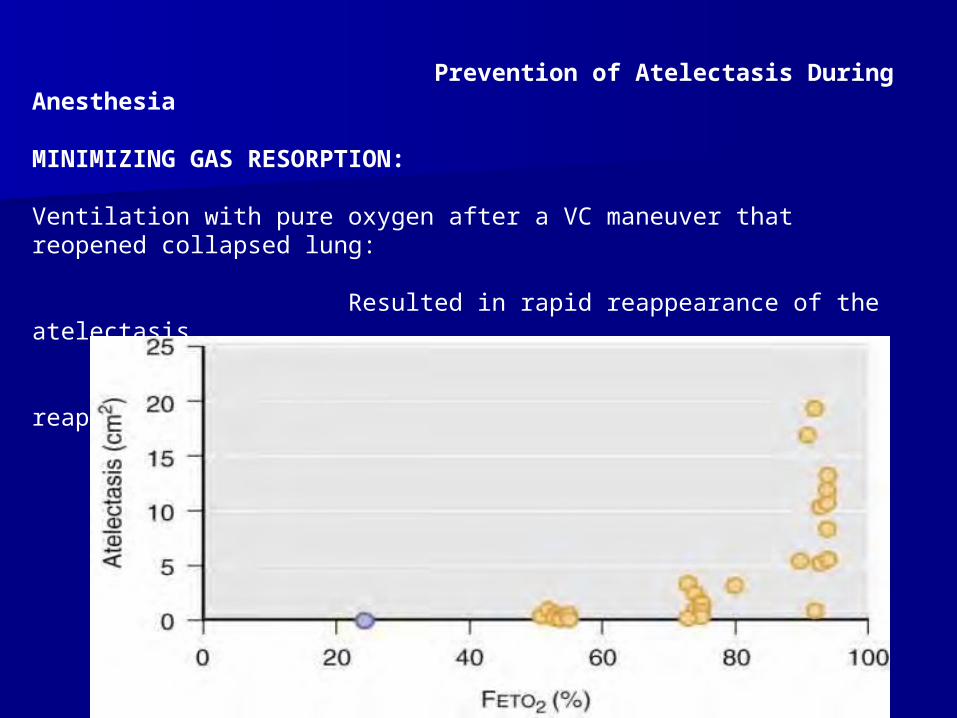
MINIMIZING GAS RESORPTION:
Ventilation with pure oxygen after a VC maneuver that reopened collapsed lung:
Resulted in rapid reappearance of the atelectasis. But 40% O2 in nitrogen is used atelectasis reappears slowly
Prevention of Atelectasis During Anesthesia
POSTANESTHETIC OXYGENATION:
Not only preoxygenation promotes formation of atelectasis but:
Also the so-called postanesthetic oxygenation at the end of the surgery.
This procedure is often combined with suctioning of the airway tree.
A VC maneuver followed by a lower O2 concentration, 40%, kept the lung open after Recruitment until the end of anesthesia.
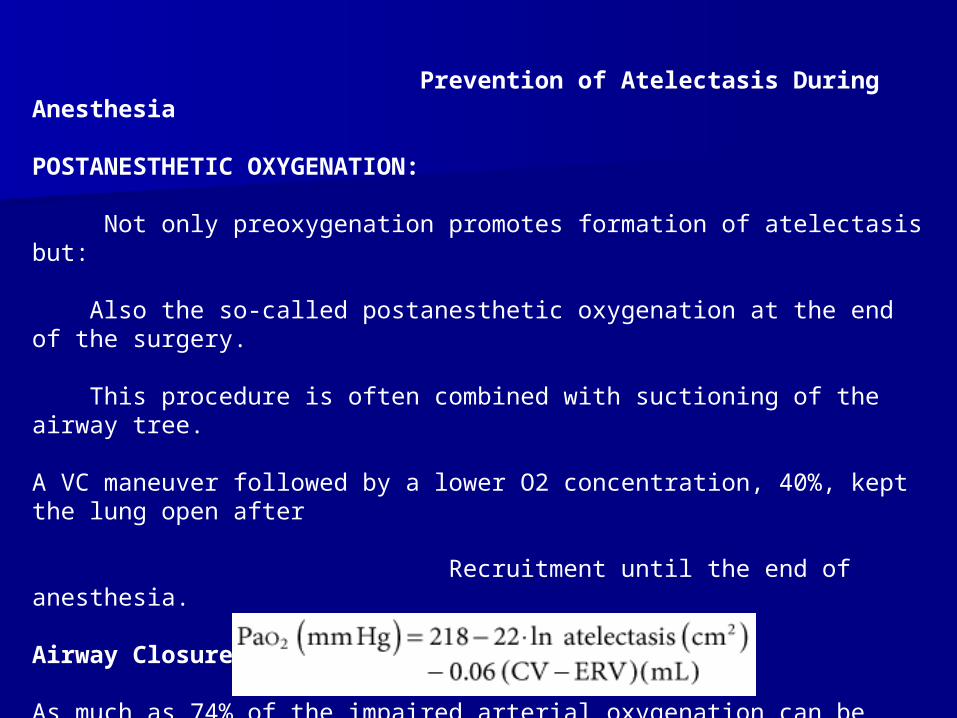
Airway Closure
As much as 74% of the impaired arterial oxygenation can be explained by atelectasis and airway closure taken together, according to the following equation.

Distribution of Ventilation and Blood Flow During Anesthesia
Distribution of Ventilation:
Redistribution of inspired gas away from dependent to nondependent has been
observed in anesthetized supine humans by isotope techniques.
PEEP increases dependent lung ventilation in anesthetized subjects in lateral position
Restoration of FRC toward awake level returns gas distribution toward awake pattern.
Distribution of Lung Blood Flow:
The lowermost portion of the lung, which was atelectatic as evidenced by simultaneous CT, was still perfused.
PEEP : reduce QT, Affect PVR Redistribution of blood flow toward dependent lung regions.
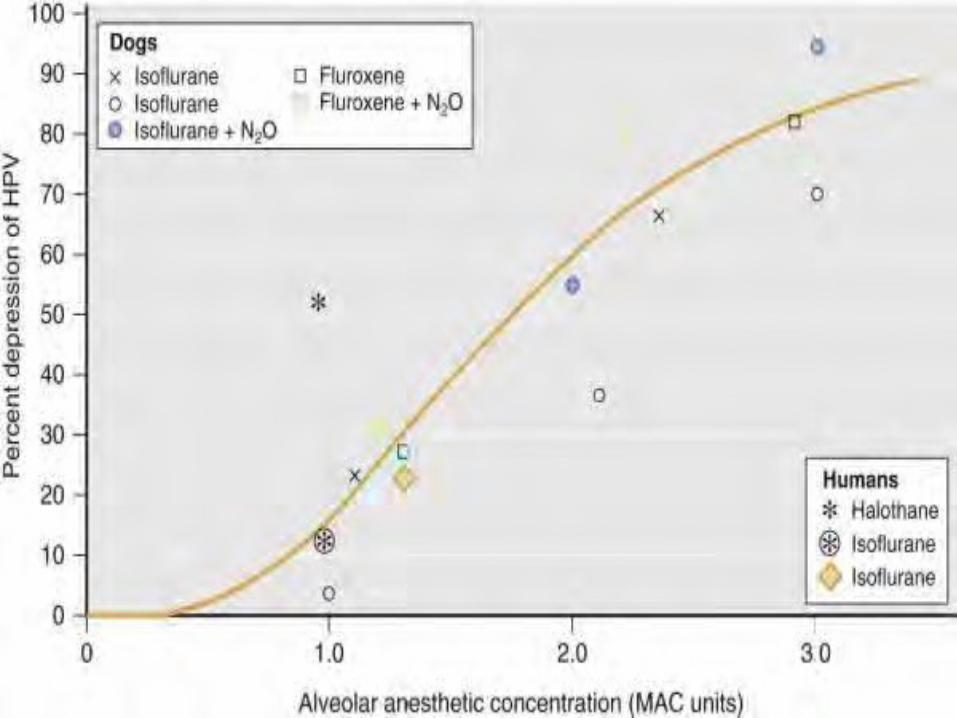
Hypoxic Pulmonary Vasoconstriction
Several inhaled anesthetics have been found to inhibit HPV in isolated lung
No such effect has been seen with intravenous anesthetics (barbiturates).
The HPV response may obscured by changes in :
Cardiac output, Myocardial contractility Vascular tone Blood volume distribution
Blood pH Lung mechanics. With no gross changes in cardiac output, isoflurane and halothane depress the HPV by 50% at a 2 MAC
Ventilation-Perfusion Matching During Anesthesia
Dead Space, Shunt, and Ventilation-Perfusion Relationships
Both CO2 elimination and oxygenation of blood are impaired :
Increased dead space ventilation? Or
High V/Q ratios?
Impairment in arterial oxygenation is more severe in: Higher ages Obesity Smokers
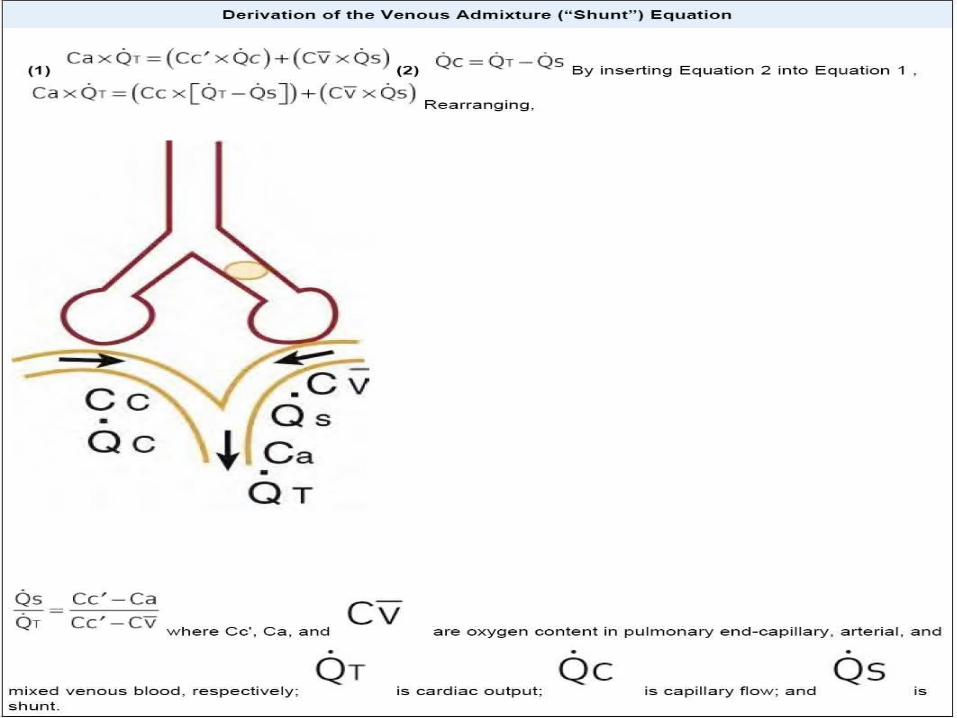
Venous admixture increased during anesthesia to approximately 10% of QT.

Factors That Influence Respiratory Function During Anesthesia
Spontaneous Breathin 1- FRC is reduced
2- Atelectasis (1&2) Same extent in spontaneously breathing as during muscle paralysis.
3- Cranial shift of the diaphrag lower, dependent portion of the diaphragm moved the most, whereas with muscle paralysis, the upper, nondependent part showed the largest displacement. 4-V/Q mismatch, increased from 0.66 to 0.83 and 0.89 from awake to spontaneous breathing and mechanical ventilation.
5-Shunt increased from 1% awake to 11% and 14% with spontaneous breathing and mechanical ventilation.
Increased Oxygen Fraction
Air (FIO2 of 0.21): Only small shunts of 1% to 2%, SDQ increased from 0.77 to 1.13.
FIO2 0.5 : Increase in shunt of 3% to 4%
FIO2 0.53 to 0.85: Shunt from 7% to 10% Thus, a certain dependence on FIO2 exist: 1-Attenuation of the HPV OR
2- further development of atelectasis and shunt in lung units with low V/Q ratios
Body Position
FRC is dramatically reduced by the combined effect of supine position and anesthesia
Upright position preserve FRC. But! No clear improvement in oxygenation was noticed
Increase V/Q mismatch In anesthetized, paralyzed , lateral and improvement in prone
Ventilation distribution is more uniform in anesthetized subjects in prone position.
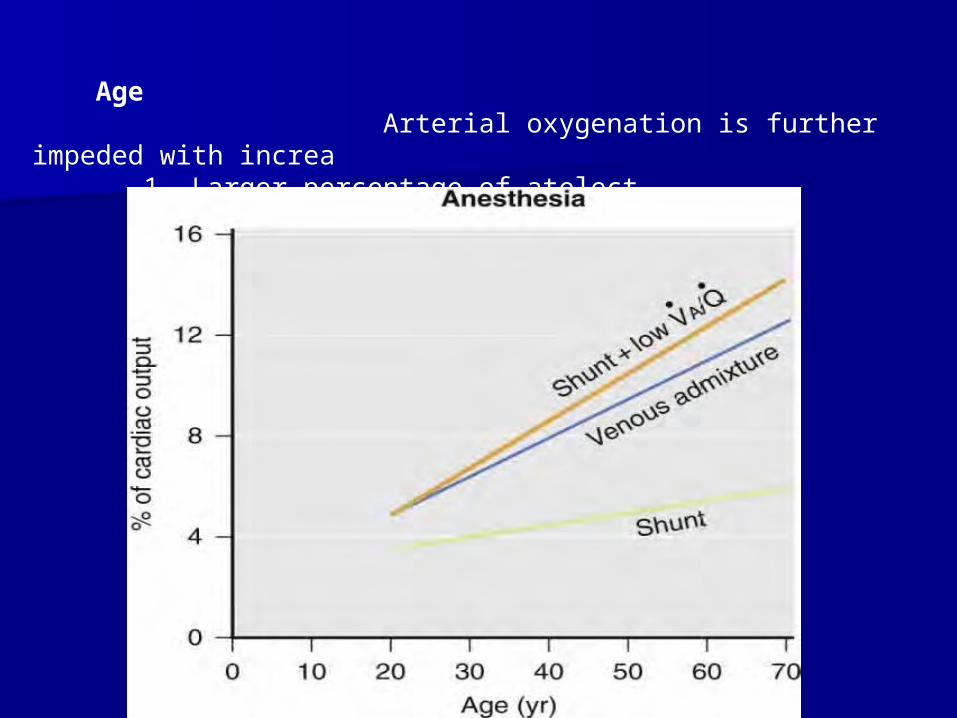
Age Arterial oxygenation is further impeded with increa 1- Larger percentage of atelect 2- Increasing V/Q mismatch
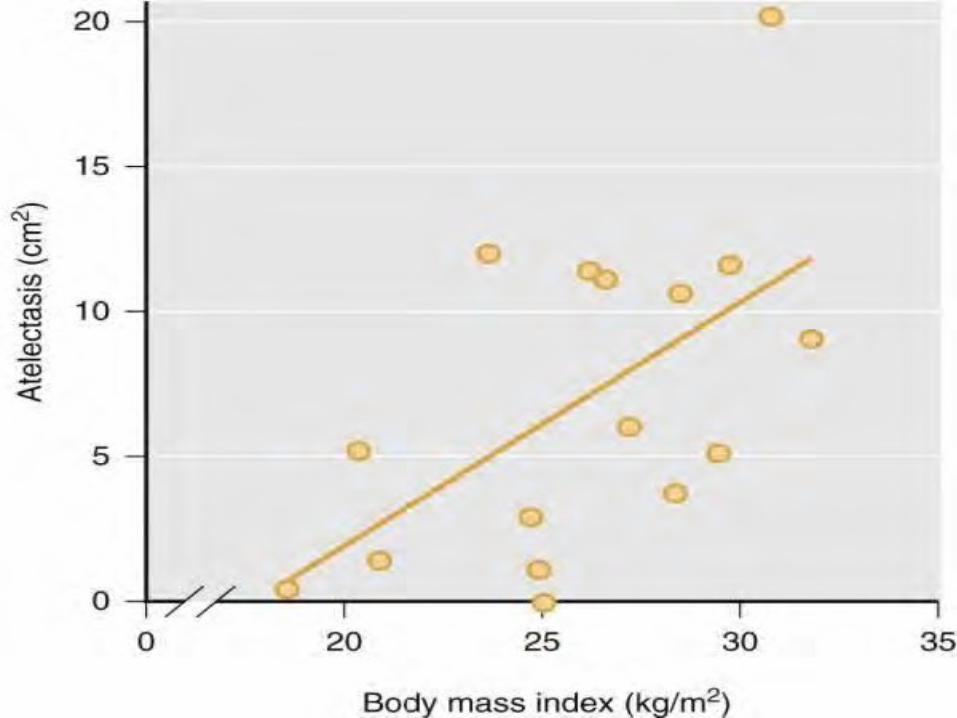
Obesity
Obesity worsens the oxygenation of blood
1- Reduced FRC
2- Promotes airway closure
3- High FIO2 will promote rapid atelectasis
Correlations between BMI and: 1- Size of atelectasis during anesthesia and postoperatvely 2- Pulmonary shunt Have been presented
Prevention:
PEEP or CPAP or FIO2=1 during induction & maintenance ?
Preexisting Lung Disease
Smokers and patients with lung disease have impairment of gas exchange: In the awake state Also during anesthesia
Considerable V/Q mismatch + large perfusion fraction to LOW V/Q regions
Interestingly, smokers with moderate airflow limitation!! May have less shunt as measured by MIGET than healthy subjects : A possible reason( for absence of atelectasis and shunt ) May be chronic hyperinflation.
Regional Anesthesia
Type and extension of motor blockade:
Extensive blocks include all of the thoracic and lumbar segments:
1- Inspiratory capacity is reduced by 20%
2- Expiratory reserve volume approaches zero
Skillfully handled regional anesthesia affects pulmonary gas exchange only minimally.
SaO2 and CO2 elimination well maintained during spinal and epidural anesthesia?
1-unchanged relationship of CC and FRC[116] 2-unaltered distributions of ventilation-perfusion ratios (MIGET,epidural anesthesia)
Lung Function After Cardiac Surgery
Cardiac surgery produces the largest atelectasis in the postoperative period
1-Both lungs collapsed 2-Patient connected to an extracorporeal pump and oxygenator
3-more than half the lung may be collapsed 1 to 2 days later 4-with a shunt that is around 20% to 30% of cardiac output
A recruitment maneuver with airway pressure of 30 cm H2O for a 20
second is sufficient to reopen the collapsed lung
Dyhr and coworkers studied 30 patients after cardiac:1- lung recruitment maneuver (LRM = four 10-second ,AWP 45 cm H2O)then ZEEP2- 12–cm H2O PEEP3- LRM plus PEEP Recruitment maneuver resulted in true opening of collapsed lung
PEEP alone caused hyperinflation of already open alveoli
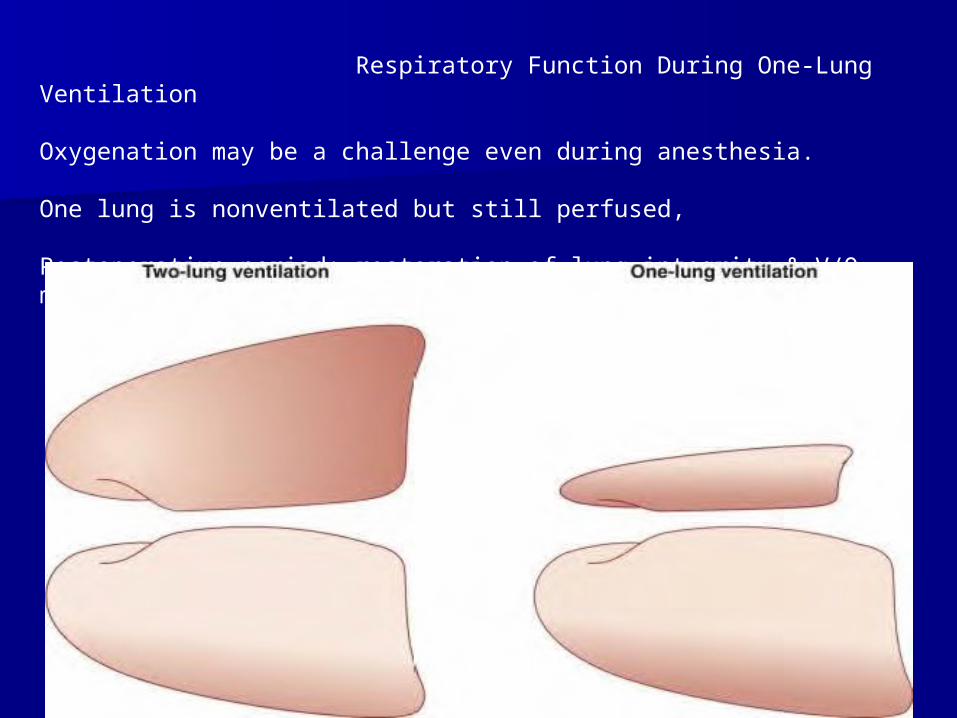
Respiratory Function During One-Lung Ventilation
Oxygenation may be a challenge even during anesthesia.
One lung is nonventilated but still perfused, Postoperative period: restoration of lung integrity & V/Q matching may take time
Measures in one lung ventilation Tusman and colleagues tested an “alveolar recruitment strategy” (ARS):
1-Increasing PAP min by min from 25 to 30, 35, finally 40 cm H2O 2- Simultaneously increasing PEEP from 5 to 10, 15, finally 20 cm H2O 3-PAP then reduced of 25 and PEEP to 5 cm H2O
This resulted :increase in PaO2 from 217 to 470 mm Hg after ARS: More of the shunt is located in the dependent lung than is generally considered.In another (Tusman ) study,ARS : Improved oxygenation Dead space decreased Slope of the CO2 curve during expiratory VT (phase III) was flatter
Measures in one lung ventilation(cont) PEEP versus ZEEP
Thoracic epidural anesthesia
Inhaled nitric oxide (NO) alone or in combination with intravenous almitrine
Positioning of the patient
Pneumoperitoneum(CO2)
1-Hypercapnia and acidosis 2-Decreased cardiaccontractility 3-Sensitization of the myocardium to the arrhythmogenic effects of catecholamines
4-Systemic vasodilation 5-Even long-lasting postoperative effects on breathing control
6-Decreased FRC and VC 7-Formation of atelectasis 8-Reduced respiratory compliance 9-Increased peak airway pressure
Nonetheless, shunt is reduced and Sao2 is mostly improved ?
Paradox: more atelectasis and less shunt !! CO2 may enhance HPV,may be the mechanism of the paradox
Physiotherapy
Physiotherapy may do more harm than good
As large an inspiration as possible and
As early in the postoperative period as possible are :
Two important factors in preventing postoperative lung complications.
Deep inspiration is done with or without a device for forced breathing
Normal Sleep
Ventilation is affected by sleep
Significant reduction in VT and inspiratory drive
Minute ventilation falls by 5% to 16% most marked during REM .
Decrease FRC (REM)
Breathing pure oxygen would also lead to the formation of atelectasis.

COCO22 Transport Transport
Carbon dioxide transport:Carbon dioxide transport:– ~9% dissolved in plasma~9% dissolved in plasma
– ~13% as carbamino compounds~13% as carbamino compounds Most combined with HbMost combined with Hb
– ~78% converted to HC0~78% converted to HC033--
COCO22 + H + H22O O H H22COCO33 H H++ + HCO + HCO33--
Haldane effectHaldane effect– Inverse relationship between amount of Hb-OInverse relationship between amount of Hb-O22 and CO and CO22
carrying capacity of bloodcarrying capacity of blood Hb binds and transports more COHb binds and transports more CO22 than O than O22
Hb buffers more HHb buffers more H++ than Hb-O than Hb-O22
– Promotes conversion of COPromotes conversion of CO22 to HCO to HCO33-- via carbonic anhydrase via carbonic anhydrase
reactionreaction
Key ConceptsKey Concepts
OO22 mostly transported in blood bound mostly transported in blood bound to hemoglobinto hemoglobin
If the PIf the PO2O2 increases Hb binds O increases Hb binds O22
If PIf PO2O2 decreases Hb releases O decreases Hb releases O22
COCO2 2 mostly transported in blood as mostly transported in blood as HCOHCO33
--
Lesser amounts of COLesser amounts of CO22 are bound to are bound to Hb or dissolved in plasmaHb or dissolved in plasma
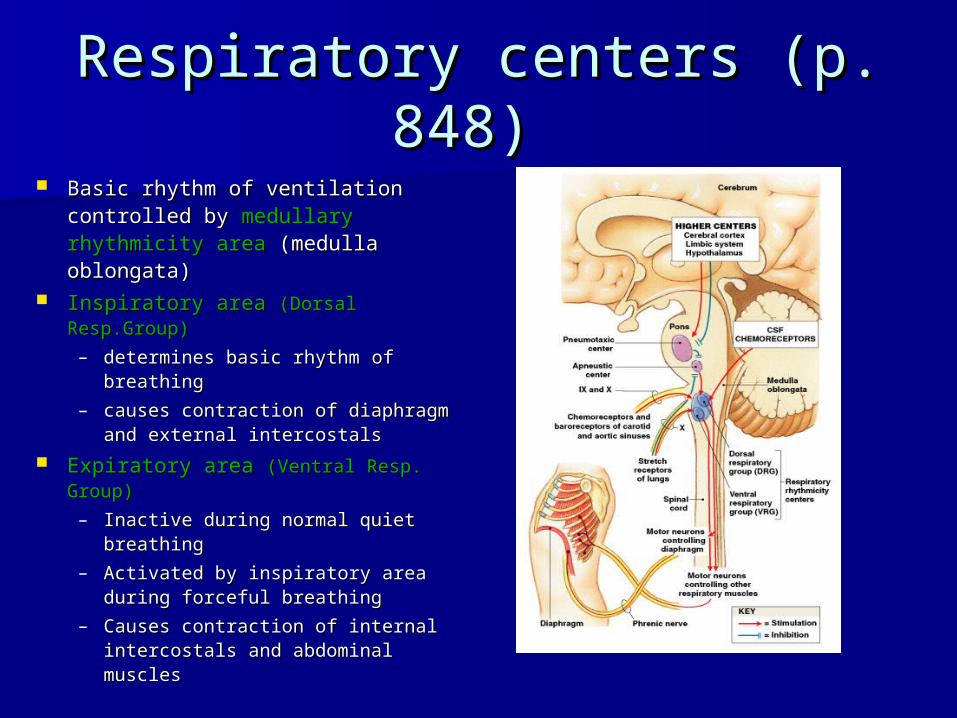
Respiratory centers (p. 848) Respiratory centers (p. 848) Basic rhythm of ventilation Basic rhythm of ventilation
controlled by controlled by mmedullary edullary rhythmicity arearhythmicity area (medulla (medulla oblongata)oblongata)
Inspiratory area Inspiratory area (Dorsal Resp.Group)(Dorsal Resp.Group)
– determines basic rhythmdetermines basic rhythm of of breathingbreathing
– causes contraction of diaphragm causes contraction of diaphragm and external intercostalsand external intercostals
Expiratory area Expiratory area (Ventral Resp. (Ventral Resp. Group)Group)
– Inactive during normal quiet Inactive during normal quiet breathingbreathing
– Activated by inspiratory area Activated by inspiratory area during forceful breathingduring forceful breathing
– Causes contraction of internal Causes contraction of internal intercostals and abdominal intercostals and abdominal musclesmuscles
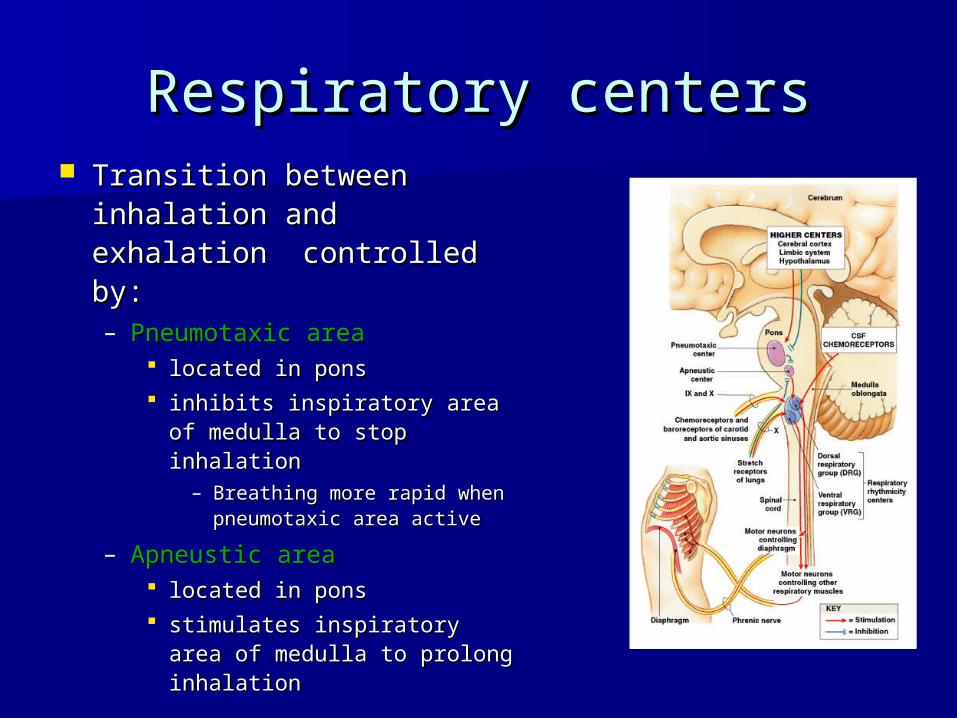
Respiratory centersRespiratory centers Transition between Transition between
inhalation and exhalation inhalation and exhalation controlled by:controlled by:– Pneumotaxic areaPneumotaxic area
located in ponslocated in pons inhibits inspiratory area of inhibits inspiratory area of
medulla to stop inhalationmedulla to stop inhalation– Breathing more rapid Breathing more rapid
when pneumotaxic area when pneumotaxic area activeactive
– Apneustic areaApneustic area located in ponslocated in pons stimulates inspiratory area stimulates inspiratory area
of medulla to prolong of medulla to prolong inhalationinhalation
Regulation of Respiratory Regulation of Respiratory centerscenters
Basic rhythm of ventilation coordinated by inspiratory area Basic rhythm of ventilation coordinated by inspiratory area of respiratory centre, but modified by:of respiratory centre, but modified by:– Cortical influencesCortical influences
Voluntary control over breathingVoluntary control over breathing
– Hypothalamus and limbic systemHypothalamus and limbic system Emotional stimuliEmotional stimuli
– ProprioceptorsProprioceptors Upper motor neurons of primary motor cortex also stimulate Upper motor neurons of primary motor cortex also stimulate
inspiratory areainspiratory area
– Inflation (Hering-Breuer) reflexInflation (Hering-Breuer) reflex Stretch receptors in walls of bronchi and bronchiolesStretch receptors in walls of bronchi and bronchioles
– Inhibit inspiratory and apneustic areasInhibit inspiratory and apneustic areas causes exhalation to begin to protect against overinflationcauses exhalation to begin to protect against overinflation
– ChemoreceptorsChemoreceptors Increased PCOIncreased PCO22, or reduced pH or PO, or reduced pH or PO22 causes chemoreceptors to causes chemoreceptors to
stimulate inspiratory area of respiratory centrestimulate inspiratory area of respiratory centre
Problem solvingProblem solving
Josh hyperventilates for several Josh hyperventilates for several minutes before diving into a pool. minutes before diving into a pool. Shortly after he enters the water he Shortly after he enters the water he blacks out and almost drowns. What blacks out and almost drowns. What caused this to happen?caused this to happen?
Regulation of Respiratory Regulation of Respiratory centerscenters
Rhythm of ventilation also modified by:Rhythm of ventilation also modified by:– TemperatureTemperature
temp = temp = ventilation (and vice versa) ventilation (and vice versa) sudden cold stimulus may cause apneasudden cold stimulus may cause apnea
– PainPain Sudden severe pain can cause apneaSudden severe pain can cause apnea Prolonged somatic pain increases respiratory rateProlonged somatic pain increases respiratory rate
Visceral pain may slow respiratoryVisceral pain may slow respiratory rate rate
– Irritation of airwaysIrritation of airways
– Blood pressureBlood pressure BP = BP = ventilation (and vice versa)ventilation (and vice versa)
– Attempt to reduce venous return via respiratory pump?Attempt to reduce venous return via respiratory pump?
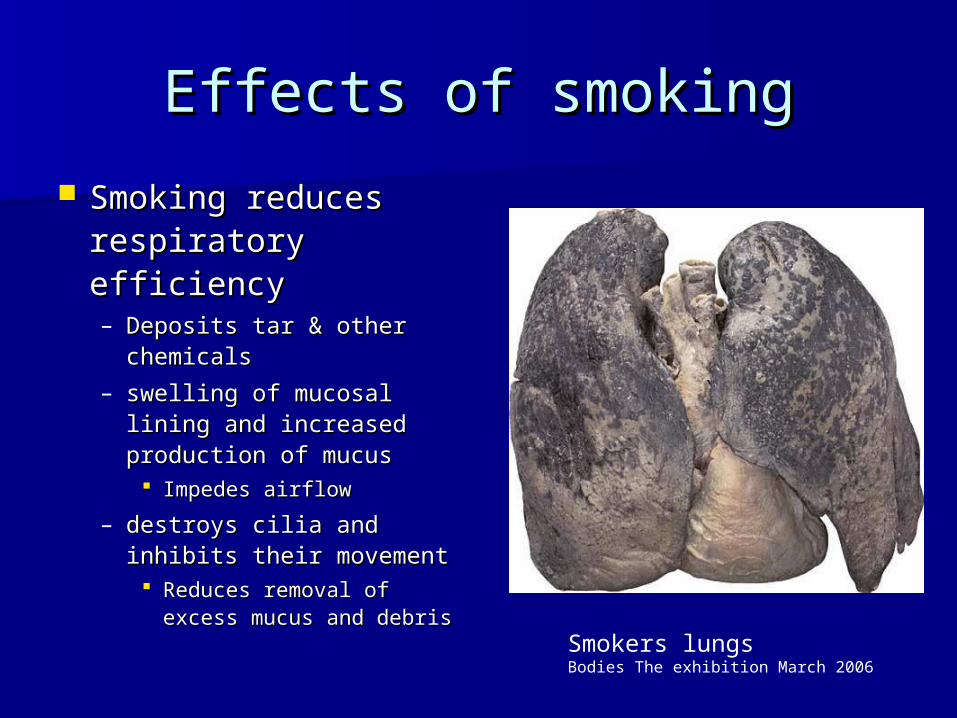
Effects of smokingEffects of smoking
Smoking reduces Smoking reduces respiratory efficiencyrespiratory efficiency– Deposits tar & other Deposits tar & other
chemicalschemicals
– swelling of mucosal lining swelling of mucosal lining and increased production and increased production of mucusof mucus Impedes airflowImpedes airflow
– destroys cilia and inhibits destroys cilia and inhibits their movementtheir movement Reduces removal of Reduces removal of
excess mucus and debrisexcess mucus and debris
Smokers lungsBodies The exhibition March 2006
SmokingSmoking
– Nicotine constricts terminal bronchiolesNicotine constricts terminal bronchioles Reduces airflow into and out of lungReduces airflow into and out of lung
– CO binds irreversibly to HbCO binds irreversibly to Hb Reduces blood oxygen carrying capacityReduces blood oxygen carrying capacity
– Destruction of elastic fibers (prime cause Destruction of elastic fibers (prime cause of emphysema)of emphysema) Reduced lung complianceReduced lung compliance Collapse of small bronchioles during Collapse of small bronchioles during
exhalationexhalation– traps air in alveoli during exhalationtraps air in alveoli during exhalation
Reduces efficiency of gas exchangeReduces efficiency of gas exchange