Venous Thromboembolism (VTE) Prevention in Obstetrics 2013...in Obstetrics . Objectives ... •...
48
Marc Carrier, MD, MSc, FRCP(C) University of Ottawa Ottawa Hospital Research Institute Venous Thromboembolism (VTE) Prevention in Obstetrics
Transcript of Venous Thromboembolism (VTE) Prevention in Obstetrics 2013...in Obstetrics . Objectives ... •...

Marc Carrier, MD, MSc, FRCP(C) University of Ottawa
Ottawa Hospital Research Institute
Venous Thromboembolism (VTE) Prevention
in Obstetrics
Objectives • Review the incidence and pathophysiology
of venous thromboembolism (VTE) during the ante and post-partum periods
• Review the risk factors for VTE • Previous VTE • Asymptomatic thrombophilia • Pre-pregnancy risk factors (IBD, etc) • Pregnancy-related risk factors
• Review the risk and benefit of pharmacological thromboprophylaxis to prevent VTE
• Ante-partum period • Postpartum period
Population Epidemiology
Retrospective cohort studies
– Antenatal VTE: ~0.5-1.0/1000 maternities1-3
• Daily antenatal risk 3-7.5x higher than non-pregnant women4
– Postpartum VTE: ~0.5/1000 maternities
• Daily postpartum risk 15-35x higher than non-pregnant women4
1-Andersen BS, Acta Obstet Gynecol Scand,1998; 2-Simpson EL, BJOG 2001; 3-Treffers PE, Int J Gynaecol Obstet 1983; 4-Anderson FA, Arch Intern Med 1991

Bourjeily G, Rodger M, Lancet, 2009
Hypercoagulable Blood ↑Procoagulant Factors:↑ Fibrinogen, ↑V, IX, X, XII and VIII ↓Anticoagulant Activity: ↓ Protein S,↑ act. Protein C resistance ↓ Fibrinolytic Activity: ↑ PAI-1 and PAI-2, ↓ t-PA activity = more thrombin generation and less clot dissolution
Stasis Iliac Vein Compression: Right iliac artery compresses left iliac vein Gravid Uterus Venodilation: Hormonally Mediated Bed Rest Immobilization

Pelvic
Calf
Pregnant
DVT1
Non-Pregnant
DVT2
Right Left Right Left
Total 12% 88% 44% 56%
Pregnant1 Non-Pregnant3
Isolated Pelvic
17% 0%
Proximal Without Calf
71% 1%
Proximal with Calf
29% 99%
Total 100% 100%
1- Chan, CMAJ, 2010 2- Ouriel, J Vasc Surg, 2000 3- Cogo, Arch Int Med, 1993
Ante-partum Thromboprophylaxis

Case 1 • 30 yo woman
– 8 weeks GA – Known Factor V Leiden (FLV) found
on family screening
• ? Ante-partum thromboprophylaxis
• She also had a DVT post trauma 5 years ago…? Thromboprophylaxis

When should we consider thromboprophylaxis?
• Assess risk benefit ratio • Risks associated with prophylactic LMWH
• Ante-partum bleeding: 0.42% • Postpartum bleeding: 0.95% • Wound hematoma, HIT: 0% • Major skin reaction/allergy: 0.96% • Osteoporosis: 0.26%
Greer IA, Blood 2005;106:401-407

When should we consider thromboprophylaxis?
• Benefits of prophylactic LMWH – Risk of VTE > 10% - Thromboprophylaxis – Risk of VTE < 1% - No thromboprophylaxis – Risk ≥1 but ≤ 10% - Controversial (preferences, etc)
• SOGC panel consensus Risk of VTE ≥1 %= consider thromboprophylaxis
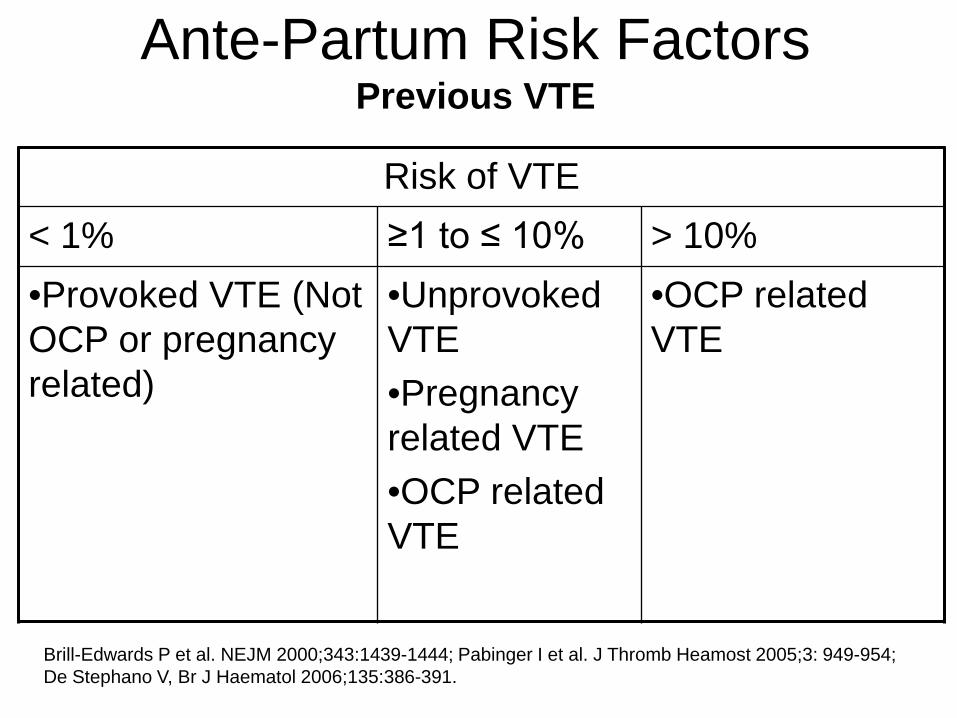
Ante-Partum Risk Factors Previous VTE
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Provoked VTE (Not OCP or pregnancy related)
•Unprovoked VTE •Pregnancy related VTE •OCP related VTE
•OCP related VTE
Brill-Edwards P et al. NEJM 2000;343:1439-1444; Pabinger I et al. J Thromb Heamost 2005;3: 949-954; De Stephano V, Br J Haematol 2006;135:386-391.

Ante-Partum Risk Factors Aymptomatic thrombophilia
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Hetero FVL •Hetero PTG •PC deficiency •PS deficiency
•Combined hetero FVL + PTG
•AT III •Homo FVL •Homo PTG
Pabinger I et al. Hematol J 2000;1:37-41; van Boven HH et al. Blood 1999;94:2590-2594; Tormene D et al. Haematologica 2001;86: 1305-1309; Middeldorp S et al. Ann Intern Med 1998;128:15-20. Zotz RB et al. Clinical Haemotalogy 2003; 16:243-259; McColl MD et al. Thromb Haemost 1997;78:1183-8; Gerhardt A et al. NEJM 2000; 342:374-80;

Ante-Partum Risk Factors Pre-pregnancy risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Diabetes •IBD •Cancer •Varicose veins •Weight/BMI •Age •Smoking
Sultan AA et al. Blood 2013;121:3953-3961; Simpson EL et al. BJOG 2001;108:56-60; Larsen TB et al. Thromb Res 2007;120:505-509; Knight M BJOG 2008;115:453-461; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.

Ante-Partum Risk Factors Pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR •Gestational diabetes •Multiple pregnancy •Bed rest (3 days to 3 weeks)
Sultan AA et al. Blood 2013;121:3953-3961; Knight M BJOG 2008;115:453-461; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.Blanco-Molina A. Thromb Haemost 2007;97:186-190.

Ante-Partum Risk Factors Multiple pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR + preeclampsia
•Bed rest (≥ 7 days) and BMI (≥ 25 Kg/m2)
Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.
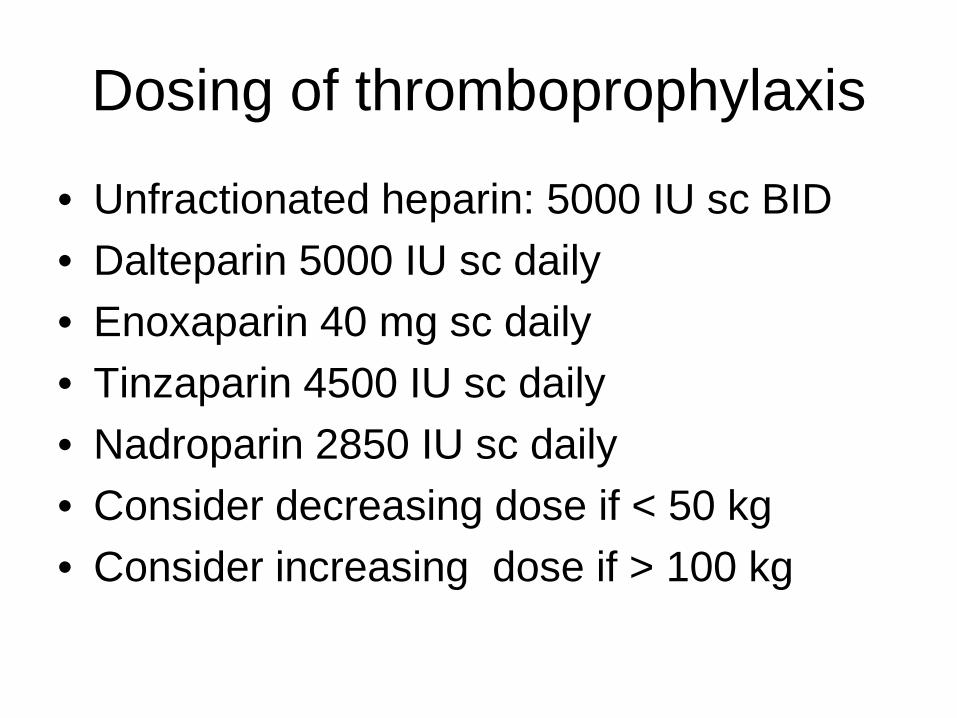
Dosing of thromboprophylaxis
• Unfractionated heparin: 5000 IU sc BID • Dalteparin 5000 IU sc daily • Enoxaparin 40 mg sc daily • Tinzaparin 4500 IU sc daily • Nadroparin 2850 IU sc daily • Consider decreasing dose if < 50 kg • Consider increasing dose if > 100 kg

Neuraxial anesthesia
• Hold anticoagulation at the onset of labor – or day prior of planned delivery
• UFH: – Neuraxial anesthesia: No delay up to 4 hours
• LMWH: – Neuraxial anesthesia: Min of 10 to 12 hours – ? Switch from LMWH to UFH at 37 weeks
• Depends on local practices and logistics
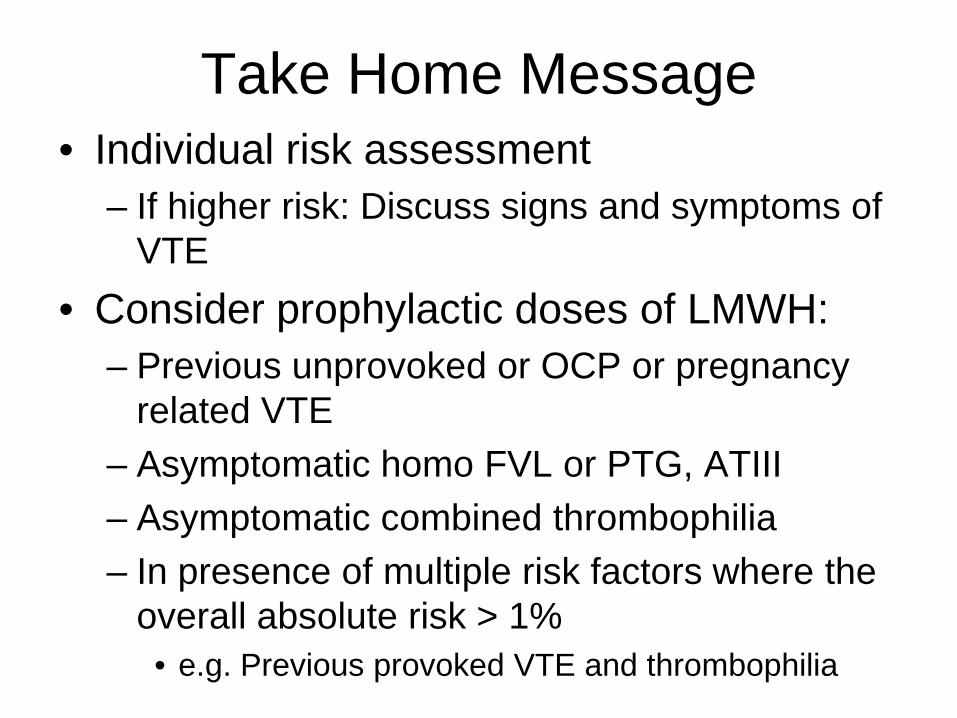
Take Home Message • Individual risk assessment
– If higher risk: Discuss signs and symptoms of VTE
• Consider prophylactic doses of LMWH: – Previous unprovoked or OCP or pregnancy
related VTE – Asymptomatic homo FVL or PTG, ATIII – Asymptomatic combined thrombophilia – In presence of multiple risk factors where the
overall absolute risk > 1% • e.g. Previous provoked VTE and thrombophilia
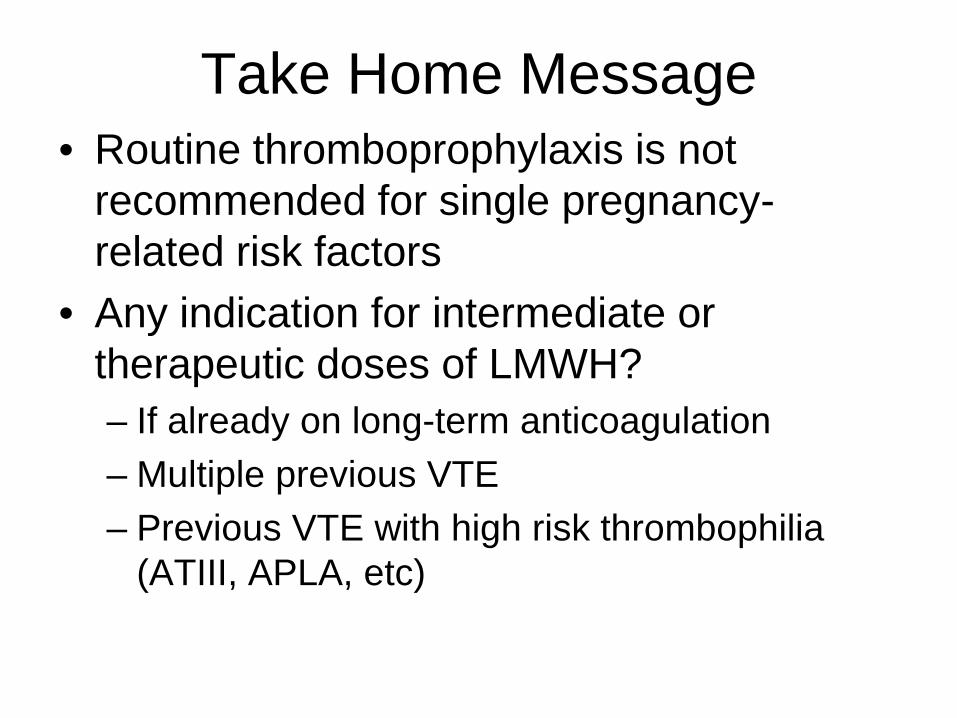
Take Home Message • Routine thromboprophylaxis is not
recommended for single pregnancy-related risk factors
• Any indication for intermediate or therapeutic doses of LMWH? – If already on long-term anticoagulation – Multiple previous VTE – Previous VTE with high risk thrombophilia
(ATIII, APLA, etc)

Post-partum Thromboprophylaxis
Case 1 • 30 yo woman
– 8 weeks GA – Known Factor V Leiden (FLV) found
on family screening – Uncomplicated vaginal delivery – No placeta-mediated complications
• Postpartum thromboprophylaxis
• She also add a DVT post trauma 5
years ago…? Thromboprophylaxis
Postpartum VTE
• Leading cause of death in Canada • 17 maternal deaths per year • 15 to 35 fold increase in the 6 weeks following the
delivery (highest during the first 3 weeks)
• Different risk factors for postpartum vs. ante-partum VTE
• Again: – Consensus: Risk of VTE ≥1 =
Thromboprophylaxis
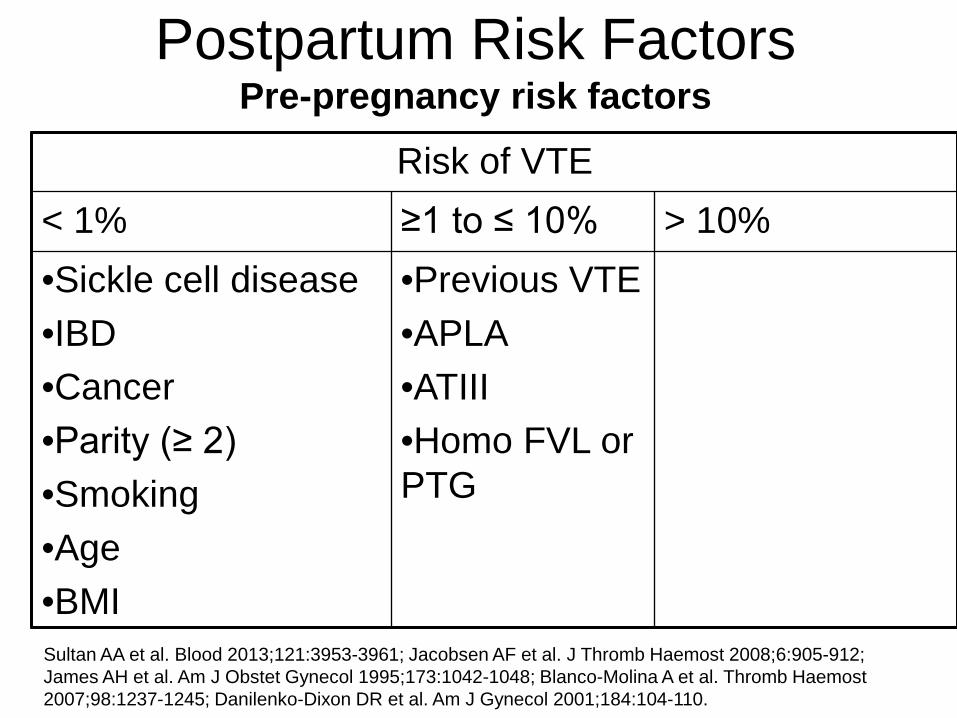
Postpartum Risk Factors Pre-pregnancy risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Sickle cell disease •IBD •Cancer •Parity (≥ 2) •Smoking •Age •BMI
•Previous VTE •APLA •ATIII •Homo FVL or PTG
Sultan AA et al. Blood 2013;121:3953-3961; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912; James AH et al. Am J Obstet Gynecol 1995;173:1042-1048; Blanco-Molina A et al. Thromb Haemost 2007;98:1237-1245; Danilenko-Dixon DR et al. Am J Gynecol 2001;184:104-110.

Postpartum Risk Factors Pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10%
•Gestational DM •IUGR •Placenta previa •Abruption •PROM •Preterm birth •Stillbirth
•Any C-section •Elective C-section •ER C-section
Sultan AA et al. Blood 2013;121:3953-3961; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912; Jacobsen AF et al. Obstet Gynecolo 2008;198:233. e1-233; Blanco-Molina A et al. Thromb Haemost 2007;98:1237-1245; Danilenko-Dixon DR et al. Am J Obstet Gynecol 2001; 2001;184:104-110.

Postpartum Risk Factors Multiple risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR + preeclampsia •C-section with infection postpartum
•> 1 liter hemorrhage + post-partum surgery •Vaginal delivery + infection postpartum •Bed rest (> 7days) + BMI ≥ 25 kg/m2
Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.
Duration of thromboprophylaxis
• Persistent risk factors – Prior VTE (highest), high risk thrombophilia, etc – 6 weeks post-partum
• Transient risk factors
– Until discharged from hospital or up to 2 weeks

Neuraxial anesthesia
• Removal of neuraxial anesthesia: – UFH:
• 4 hours after last dose – LMWH:
• 10 to 12 hours after last dose (or before next dose) • May resume LMWH 2 hours post removal

Take Home Message • Individual risk assessment
– If higher risk: Discuss signs and symptoms of VTE – Close clinical follow-up
• Consider prophylactic doses of LMWH:
– Previous VTE – ATIII def, Homo FVL or PTG, combined
thrombophilia, APLA – Strict bed rest prior to delivery (> 7 days)
• >90% of the time in bed – Peri or postpartum blood loss (> 1L) or transfusion
and concurrent postpartum surgery – Vaginal delivery and peripartum sepsis
Take Home Message • Consider prophylactic doses of LMWH if 2 or
more of the following: – Any C-section – Smoking (> 10 cigarettes/day antepartum) – BMI ≥30 kg/m2 at first antepartum visit – IUGR – Preeclampsia – Placenta previa or abruption – Peri or postpartum infection (vaginal or c-section) – Low risk thrombophilia (PC, PS, hetero FV or PT) – IBD, DM, sickle cell disease – Multiple pregnancy – Pre-term delivery
Take Home Messages
• DVT in pregnancy is likely a north (proximal) to south (distal) disease
• Individual risk assessment – If higher risk: Discuss signs and symptoms of
VTE + Close follow-up
• Consider ante and/or postpartum thromboprophylaxis in patients with risk of VTE ≥1%

Diagnosis of DVT and PE in Pregnancy
Case 1
• 30 yo woman presents at 8 weeks GA with a tender swollen left leg/buttock

Exam: left thigh/calf are >5 cm bigger than her right leg

Case 1
How would you exclude DVT? 1. Negative D-dimer alone 2. Low Wells model and negative D-Dimer 3. Single negative compression US (CUS) 4. Negative serial compression US (CUS) on
Day 1 and day 7 5. Negative compression ultrasound (CUS)
and negative MRV

Wells Clinical Model for DVT Wells P, et al. Value of Assessment of Pre-test Probability of Deep-Vein Thrombosis in Clinical Management. Lancet Vol. 350, Dec 1997, 1795-1798.
Active cancer (treatment ongoing or within past 6 months or palliative) 1
Recent paresis, paralysis or cast immobilization of lower limb (within past 4 weeks) 1
Recently bedridden for more than 3 days or major surgery within the past four weeks 1
Localized tenderness of the deep venous system 1
Oedema of entire leg 1
Calf swelling > 3 cm when compared with contralateral calf (measured 10 cm under the tibial tuberosity) 1
Pitting oedema more marked on suspected side 1
Collateral vein network (non-varicose) (replaced by previous VTE in recent versions) 1
Another diagnosis as likely or more likely than DVT -2
Total Score:
Probability is: High Intermediate Low
if total is equal to or greater than 3 if total is 1 or 2 if total is 0
Probability is: Likely Unlikely
if total is >1 if total is ≤1
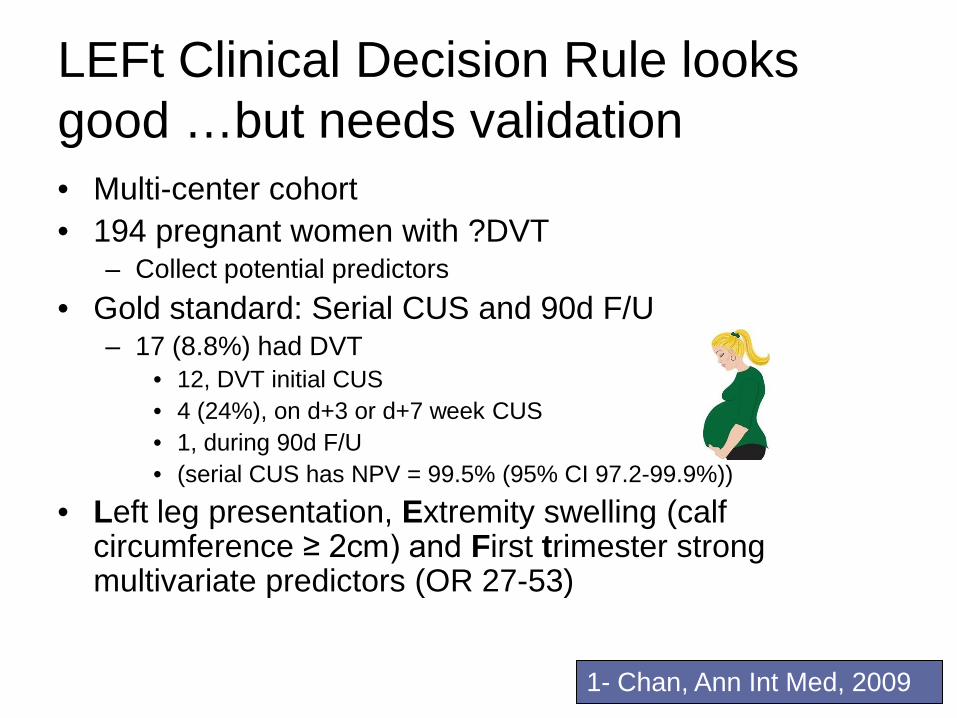
LEFt Clinical Decision Rule looks good …but needs validation • Multi-center cohort • 194 pregnant women with ?DVT
– Collect potential predictors • Gold standard: Serial CUS and 90d F/U
– 17 (8.8%) had DVT • 12, DVT initial CUS • 4 (24%), on d+3 or d+7 week CUS • 1, during 90d F/U • (serial CUS has NPV = 99.5% (95% CI 97.2-99.9%))
• Left leg presentation, Extremity swelling (calf circumference ≥ 2cm) and First trimester strong multivariate predictors (OR 27-53)
1- Chan, Ann Int Med, 2009
D-Dimer alone to exclude DVT in pregnancy looks good …but needs validation • Multi-center cohort • 149 pregnant women with ?DVT
– SimpliRED D-Dimer • Gold standard: Serial CUS and 90d F/U
– 13 (8.7%) had DVT
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007

100% Sensitivity
Specificity
Negative predictive
value …40
50
60 70 80 90 0…
100
Normal D-Dimer to exclude DVT in pregnancy
95% CI: 75-100%
60% 95%CI: 52-68%
95-100% 100%
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007


Case 1
How would you exclude DVT? 1. Negative D-dimer alone 2. Low Wells model and negative D-Dimer 3. Single negative compression US (CUS) 4. Negative serial compression US (CUS) on
Day 1 and day 7 5. Negative compression ultrasound (CUS)
and negative MRV
Case 2
35 yo women 30 wks GA presents with pleuritic CP and SOB and positive D-Dimer.
How would you exclude PE? 1. Low Wells model and negative D-
Dimer 2. Compression US first then if normal do
a V/Q; normal perfusion excludes PE 3. V/Q: normal perfusion excludes PE 4. Negative CT pulmonary angiogram
alone

Wells Clinical Model for PE Points
• Clinical symptoms of DVT 3
• No alternative diagnosis more likely than PE 3
• Heart rate over 100 1.5 • History of immobilization or surgery in previous 4 weeks
1.5
• Previous DVT/PE 1.5
• Hemoptysis 1.0
• Cancer
1.0
Total Score ≤4 = negative, >4 = positive
Return to Question 5

D-Dimer looks good …but needs validation
• Multi-center cohort • 149 pregnant women with ?DVT
– SimpliRed D-Dimer
• Gold standard: Serial CUS and 90d F/U – 13 (8.7%) had DVT
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007

V/Q CXR All 3
CT
0.016
0.032
0.05
0
0.066
0.082
0.1
0.000001 Gy
Radiation Exposure to Fetus G
ray
(Gy)
0.00051 Gy
0.000013 Gy
0.00054 Gy
Possible Teratogenic Threshold 0.1Gy
Possible Oncogenic Threshold 0.01Gy
V/Q Test of Choice in Pregnancy: Disadvantages of CT over V/Q • Higher proportion of inadequate CTs in
pregnancy (up to 1/3rd)1
– Contrast timing/ IVC dilution
• V/Q normal in >70% of patients in pregnancy with ?PE2,3
1- Ridge et al, AJR, 2009; 2- Chan et al, Arch Int Med, 2002; 3-Cahill, Obstet Gynecol, 2009;
V/Q Test of Choice in Pregnancy: Disadvantages of CT over V/Q • Non-Pregnant: High “false positive” rate
with CT in an RCT1 which may worsen with ↑slices in MDCT2
• Increase lifetime risk of malignancy from radiation exposure – 150X ↑ breast radiation than V/Q – 1 in 143 in 20 y.o. non-pregnant ♀3
1- Anderson, JAMA, 2007; 2- Carrier, JTH, 2010; 3-Einstein, JAMA 2007

Case 2
30 wks GA presents with pleuritic CP and SOB and positive D-Dimer.
How would you exclude PE? 1. Low Wells model and Negative D-Dimer
2. Compression US first then if normal do a V/Q; normal excludes PE
3. V/Q: normal excludes PE 4. Negative CT pulmonary angiogram alone

Take Home Messages
• DVT in pregnancy is likely a north (proximal) to south (distal) disease
• Serial ultrasounds are required to exclude DVT in pregnancy
• V/Q scan remains test of choice for ?PE