Vasculitis in erythema induratum of Bazin: A...
13
Vasculitis in erythema induratum of Bazin: A histopathologic study of 101 biopsy specimens from 86 patients Sonia Segura, MD, a Ramo ´n M. Pujol, MD, a Felicidade Trindade, MD, b and Luis Requena, MD b Barcelona and Madrid, Spain Background: Erythema induratum of Bazin is a mostly lobular panniculitis. There is considerable controversy in the literature about whether or not vasculitis is a histopathologic requirement to establish the diagnosis of erythema induratum of Bazin. Even accepting vasculitis as a histopathologic criterion, there is no agreement about the nature and size of the involved vessels. Objective: The main goal of our study was to investigate whether or not vasculitis was present in a large series of cases of erythema induratum of Bazin and, when vasculitis was found, to determine the nature and localization of the involved vessels. Methods: We studied 101 skin biopsy specimens from 86 patients with clinicopathologic diagnosis of erythema induratum of Bazin. Histopathologic criteria required in each case to be included in this study were: (1) a mostly lobular panniculitis with necrotic adipocytes at the center of the fat lobule; (2) inflammatory infiltrate within the fat lobule mostly composed of neutrophils in early lesions and granulomatous infiltrate in fully developed lesions; (3) significant fat necrosis; and (4) absence of other histopathologic findings that allow a specific diagnosis of other lobular panniculitis different from erythema induratum of Bazin. We also recorded the nature of the inflammatory cells involving the fat lobule, and the lesions were classified into two main categories: (1) early lesions, when the inflammatory infiltrate was mainly composed of neutrophils, with or without leukocytoclasis; and (2) fully developed lesions, when histiocytes and lipophages were the predominant inflammatory cells within the involved fat lobule. Results: Some type of vasculitis was evident in 91 cases (90.09%). A total of 47 biopsy specimens (46.5%) showed a mostly lobular panniculitis with necrotizing vasculitis involving the small vessels, probably venules, of the center of the fat lobule. Thirteen biopsy specimens (12.8%) showed a mostly lobular panniculitis with vasculitis involving both large septal veins and small vessels, probably venules, of the center of the fat lobule. Twelve biopsy specimens (11.8%) showed a mostly lobular panniculitis with vasculitis involving large septal veins, with no involvement or other septal or lobular vessels. Ten biopsy specimens (9.9%) showed a mostly lobular panniculitis with vasculitis involving large septal vessels, both arteries and veins, and necrotizing vasculitis involving the small vessels, probably venules, of the center of the fat lobule. Nine biopsy specimens (8.9%) showed a mostly lobular panniculitis with vasculitis involving large septal vessels, both arteries and veins, but with no involvement of the small blood vessels of the center of the fat lobule. Finally, 10 biopsy specimens (9.9%) showed a mostly lobular panniculitis without evidence of septal or lobular vasculitis in serial sections. Associated diseases included history of extracutaneous tuberculosis (including tuberculosis of the lung, lymph nodes, kidney, or bowel) in 12 cases (13.95%), previous episodes of superficial thrombophlebitis of the lower legs in 3 cases (3.72%), rheumatoid arthritis in one case (1.16%), Crohn disease in one case (1.16%), chronic lymphocytic leukemia in two cases (2.32%), hypothyroidism in two cases (2.32%), and positive serology for hepatitis B virus in 4 cases (4.65%) and for hepatitis C virus in 5 cases (5.81%). From the Departments of Dermatology at Hospital del Mar, Universitat Auto ´ noma, Barcelona, a and Fundacio ´n Jime ´ nez Dı ´az, Universidad Auto ´ noma, Madrid. b Funding sources: None. Conflicts of interest: None declared. Reprints not available from the authors. Correspondence to: Luis Requena, MD, Department of Dermatology, Fundacio ´ n Jime ´nez Dı ´az, Avda. Reyes Cato ´ licos 2, 28040-Madrid, Spain. E-mail: [email protected]. 0190-9622/$34.00 ª 2008 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2008.07.030 839
Transcript of Vasculitis in erythema induratum of Bazin: A...

Vasculitis in erythema induratum of Bazin:A histopathologic study of 101 biopsy specimens
from 86 patients
Sonia Segura, MD,a Ramon M. Pujol, MD,a Felicidade Trindade, MD,b and Luis Requena, MDb
Barcelona and Madrid, Spain
Background: Erythema induratum of Bazin is a mostly lobular panniculitis. There is considerablecontroversy in the literature about whether or not vasculitis is a histopathologic requirement to establishthe diagnosis of erythema induratum of Bazin. Even accepting vasculitis as a histopathologic criterion, thereis no agreement about the nature and size of the involved vessels.
Objective: The main goal of our study was to investigate whether or not vasculitis was present in a largeseries of cases of erythema induratum of Bazin and, when vasculitis was found, to determine the nature andlocalization of the involved vessels.
Methods: We studied 101 skin biopsy specimens from 86 patients with clinicopathologic diagnosis oferythema induratum of Bazin. Histopathologic criteria required in each case to be included in this studywere: (1) a mostly lobular panniculitis with necrotic adipocytes at the center of the fat lobule; (2)inflammatory infiltrate within the fat lobule mostly composed of neutrophils in early lesions andgranulomatous infiltrate in fully developed lesions; (3) significant fat necrosis; and (4) absence of otherhistopathologic findings that allow a specific diagnosis of other lobular panniculitis different fromerythema induratum of Bazin. We also recorded the nature of the inflammatory cells involving the fatlobule, and the lesions were classified into two main categories: (1) early lesions, when the inflammatoryinfiltrate was mainly composed of neutrophils, with or without leukocytoclasis; and (2) fully developedlesions, when histiocytes and lipophages were the predominant inflammatory cells within the involved fatlobule.
Results: Some type of vasculitis was evident in 91 cases (90.09%). A total of 47 biopsy specimens (46.5%)showed a mostly lobular panniculitis with necrotizing vasculitis involving the small vessels, probablyvenules, of the center of the fat lobule. Thirteen biopsy specimens (12.8%) showed a mostly lobularpanniculitis with vasculitis involving both large septal veins and small vessels, probably venules, of thecenter of the fat lobule. Twelve biopsy specimens (11.8%) showed a mostly lobular panniculitis withvasculitis involving large septal veins, with no involvement or other septal or lobular vessels. Ten biopsyspecimens (9.9%) showed a mostly lobular panniculitis with vasculitis involving large septal vessels, botharteries and veins, and necrotizing vasculitis involving the small vessels, probably venules, of the center ofthe fat lobule. Nine biopsy specimens (8.9%) showed a mostly lobular panniculitis with vasculitis involvinglarge septal vessels, both arteries and veins, but with no involvement of the small blood vessels of thecenter of the fat lobule. Finally, 10 biopsy specimens (9.9%) showed a mostly lobular panniculitis withoutevidence of septal or lobular vasculitis in serial sections. Associated diseases included history ofextracutaneous tuberculosis (including tuberculosis of the lung, lymph nodes, kidney, or bowel) in 12cases (13.95%), previous episodes of superficial thrombophlebitis of the lower legs in 3 cases (3.72%),rheumatoid arthritis in one case (1.16%), Crohn disease in one case (1.16%), chronic lymphocytic leukemiain two cases (2.32%), hypothyroidism in two cases (2.32%), and positive serology for hepatitis B virus in 4cases (4.65%) and for hepatitis C virus in 5 cases (5.81%).
From the Departments of Dermatology at Hospital del Mar,
Universitat Autonoma, Barcelona,a and Fundacion Jimenez
Dıaz, Universidad Autonoma, Madrid.b
Funding sources: None.
Conflicts of interest: None declared.
Reprints not available from the authors.
Correspondence to: Luis Requena, MD, Department of
Dermatology, Fundacion Jimenez Dıaz, Avda. Reyes Catolicos
2, 28040-Madrid, Spain. E-mail: [email protected].
0190-9622/$34.00
ª 2008 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2008.07.030
839

J AM ACAD DERMATOL
NOVEMBER 2008
840 Segura et al
Limitations: Serial sections were not performed in all cases. At least 10 sections were studied in each case.When vasculitis was evident in some of these first 10 sections, no further sections were cut, but whenhistopathologic features of vasculitis were not found in the first 10 sections, serial sections throughout thespecimen were performed looking for vasculitis. Because some type of vasculitis was evident in the first 10sections of 91 cases, serial sections were performed only in the remaining 10 cases and they failed todemonstrate clear-cut histopathologic features of vasculitis. On the other hand, this is a retrospective studythat was performed from the histopathologic slides of our files, and only the clinical information containedin the report accompanying the biopsy specimen could be recorded.
Conclusions: In our experience, vasculitis is present in most lesions of erythema induratum of Bazin, andthe nature, location, and size of the involved vessels is, from more to less frequent, as follows: (1) smallvenules of the fat lobule; (2) both veins of the connective tissue septa and venules of the fat lobule; (3) onlyveins of the connective tissue septa; (4) veins and arteries of the connective tissue septa and venules of thefat lobule; and (5) veins and arteries of the connective tissue septa. However, in some cases with allclinicopathologic features of erythema induratum of Bazin vasculitis could not be demonstrated with serialsections throughout the specimen and, therefore, the presence of vasculitis should be not considered as acriterion sine qua non for histopathologic diagnosis of erythema induratum of Bazin. ( J Am Acad Dermatol2008;59:839-51.)
Currently, the terms ‘‘erythema induratum ofBazin’’ and ‘‘nodular vasculitis’’ are used as syno-nyms by a majority of authors to describe the mostcommon variant of mostly lobular panniculitideswith vasculitis. This has not always been the case,however. This form of panniculitis was originallydescribed by Bazin1 in 1861, as subcutaneous indu-rate erythematous plaques appearing mainly on theback of the lower aspect of legs of middle-agedwomen. He classified the process as one of theerythematous benign scrofulids, using ‘‘scrofulids’’as a descriptive term to refer to deep erythematousnodules, and it seems that he did not consider thispanniculitis as a tuberculid. The link between tuber-culosis and erythema induratum was emphasizedlater, around 1900, mostly by French dermatologistswho included erythema induratum within the spec-trum of the tuberculids.2 Almost simultaneously,identical clinical cases with no evidence of tubercu-losis were reported by English authors,3,4 which ledlater to the development of the concept of erythemainduratum as nontuberculous in origin by Whitfield.5
In 1945, Montgomery et al6 in the United Statesproposed the term ‘‘nodular vasculitis’’ for Whitfielderythema induratum and described its clinical andhistopathologic features as different from those oferythema induratum of Bazin. Since then, mosttextbooks of dermatology described erythema indu-ratum of Bazin, erythema induratum of Whitfield,and nodular vasculitis as 3 different entities.7 Still,some current authors have proposed keeping thename ‘‘erythema induratum of Bazin’’ for those casesin which a causative relationship with tuberculosis isdemonstrated and refer to the remainder of cases asnodular vasculitis. In recent years, however, thereseems to be a consensus considering erythemainduratum of Bazin and nodular vasculitis as the
same entity,8,9 an opinion that we shared.10 Likeerythema nodosum, erythema induratum of Bazin iscurrently considered to be a reactive disorder relatedto several causative factors, one of which may betuberculosis, especially in some geographic areas.11
In our country, tuberculosis is by far the mostimportant causative factor for erythema induratumof Bazin, and recent polymerase chain reactioninvestigations have demonstrated Mycobacteriumtuberculosis DNA in 77% of the cutaneous biopsyspecimens of patients with this variant of panniculi-tis.12 Although the frequency varies from somegeographic areas to others, in many countries tuber-culosis is still the main causative factor for erythemainduratum of Bazin.13-20 In contrast, in those coun-tries with low prevalence of tuberculosis, this type ofpanniculitis may be a reactive process as a result ofother causative factors such as obesity, cold climate,chronic venous insufficiency, or history of thrombo-phlebitis of the lower limbs.
Typical erythema induratum of Bazin is a diseaseof middle-aged obese women in whom erythema-tous subcutaneous nodules and plaques appearon the back of the lower aspects of the legs.Erythrocyanosis, heavy columnlike calves, erythemasurrounding follicular pores, and cutis marmorataare frequently associated changes and may bepredisposing factors. Although nonulcerated lesionsmay heal without scarring, often subcutaneous nod-ules become adherent to the skin surface and ulcer-ate. Healing of these ulcers is usually a slow processresulting in atrophic scars that allow retrospectivediagnosis in nonactive cases. Erythema induratum ofBazin is more frequent in obese women with somedegree of venous insufficiency of the lower extrem-ities, and subcutaneous nodules with ulcerationdevelop mostly during the winter months. Lesions

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 841
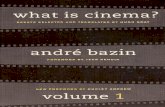
Fig 1. Early lesion of erythema induratum of Bazin showing mostly lobular panniculitis withnecrotizing vasculitis involving small vessels of center of fat lobule. A, Scanning power. B,Higher magnification showing mostly lobular panniculitis. C, Infiltrate of fat lobule was mostlycomposed of neutrophils. D, Necrotizing vasculitis involving small blood vessels of center of fatlobule. (A to D, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C, 3200;D, 3400.)
are usually tender but may be indolent or painfulonly on pressure. The course is protracted andrecurrent episodes over years, even decades, arecommon. Individual lesions tend to involute, butnew crops appear at irregular intervals. Patients witherythema induratum of Bazin are otherwise in goodhealth.
From a histopathologic point of view, erythemainduratum of Bazin is a mostly lobular panniculitis.At an early stage, the fat lobules are punctuatedthroughout by discrete collections of inflammatorycells, mostly neutrophils. There may be extensivenecrosis of the adipocytes of the fat lobule. Thesenecrotic adipocytes call for histiocytes that ingestlipid and become foamy. Epithelioid histiocytes,multinucleated giant cells, and lymphocytes contrib-ute to the granulomatous appearance of the in-flammatory infiltrate in fully developed lesions oferythema induratum of Bazin. When intense vasculardamage is present, extensive areas of caseous ne-crosis appear and the lesions show all the histopath-ologic attributes of a tuberculoid granuloma.Caseous necrosis may extend to the overlying dermisand secondarily involve the epidermis with ulcera-tion and discharge of liquefied necrotic fat.
Controversypersists in the literature aboutwhetheror not vasculitis is a histopathologic requirement toestablish the diagnosis of erythema induratum ofBazin. Even accepting vasculitis as a histopathologiccriterion, there is noagreement about thenatureof theinvolved vessel. Some investigators consider vasculi-tis as a characteristic histopathologic finding, but theyfail to establish the nature and the size of the involvedvessels.21 When the nature of the involved vessel isspecifically stated, some authors believe that they arearteries,22,23 whereas other authors favor a venousinvolvement,24,25 and still others consider that botharteries and veins are involved.26-30 The main goal ofour study was to investigate whether or not vasculitiswas always present in our cases of erythema indu-ratum of Bazin and, when vasculitis was found, todetermine the nature and localization of the involvedvessels. This study also describes the histopathologicfeatures of the largest published series of erythemainduratum of Bazin.
METHODSSkin biopsy specimens of 86 patients with clinico-
pathologic diagnosis of erythema induratum of Bazinwere retrieved from the archives of the departments

J AM ACAD DERMATOL
NOVEMBER 2008
842 Segura et al
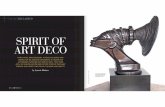
Fig 2. Fully developed lesion of erythema induratum of Bazin showing mostly lobularpanniculitis with necrotizing vasculitis involving small vessels of center of fat lobule. A,Scanning power. B, Higher magnification showing mostly lobular panniculitis. C, Granulom-atous infiltrate involving fat lobule. D, Necrotizing vasculitis of small blood vessels at center offat lobule. (A to D, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C, 3200;D, 3400.)
of dermatology at Hospital del Mar, Barcelona, Spain(22 biopsy specimens from 16 patients: 12 patientswith onebiopsy specimen, 2patientswith twobiopsyspecimens, and 2 patients with three biopsy speci-mens) and Fundacion Jimenez Dıaz, Madrid, Spain(79 biopsy specimens from 70 patients: 63 patientswith onebiopsy specimen, 5patientswith twobiopsyspecimens, and two patients with 3 biopsy speci-mens). From a clinical point of view, all patientsshowed characteristic cutaneous lesions, mostlyconsisting of erythematous nodules on the back ofthe legs. Eighty patients showed positive cutaneousdelayed hypersensitivity reaction to purified proteinderivative (positive Mantoux test result), whereas 3patients showed negative Mantoux test result and thistest was not performed in another 3 patients. Clinicaldata were obtained from patient’s medical recordsand, in each case, the demographic data, includingage and sex, location of the lesions, and associateddiseases, were recorded.
From a histopathologic point of view, the follow-ing criteria were required to include each case in thisstudy: (1) a mostly lobular panniculitis with necroticadipocytes at the center of the fat lobule; (2) inflam-matory infiltrate within the fat lobule mostlycomposed of neutrophils in early lesions and granu-lomatous infiltrate in fully developed lesions; (3)significant fat necrosis; and (4) absence of otherhistopathologic findings that allow a specific diagno-sis of other lobular panniculitis different fromerythema induratum of Bazin. Other types of mostlylobular panniculitis, including pancreatic panniculi-tis, alpha-1-antitrypsindeficiencyeassociatedpannic-ulitis, sclerosing panniculitis, and lupus panniculitiswere ruled out on the basis of the histopathologicfindings. Infective panniculitis was ruled out whenGram and periodic acideSchiff stains failed to dem-onstrate micro-organisms in cases of a mostly neutro-philic lobular panniculitis. Foreign body material wasruled out throughout polarization in those cases of a

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 843
Fig 3. Early lesion of erythema induratum of Bazin showing mostly lobular panniculitis withvasculitis involving both large septal veins and small blood vessels of center of fat lobule. A,Scanning power. B, Higher magnification showing lobular panniculitis with neutrophilicinfiltrate. C, Vasculitis involving large vein at septa. D, Necrotizing vasculitis involving smallblood vessels at center of fat lobule. (A to D, Hematoxylin-eosin stain; original magnifications:A, 310; B, 340; C, 3200; D, 3400.)
mostly lobular panniculitis with granulomatousinfiltrate.
Histopathologic criteria required to establish adiagnosis of vasculitis included swelling of endothe-lial cells, leukocytoclasis, fibrinoid changes in vesselwalls, and neutrophils in and around vessel walls.This vasculitis, the main goal of our study, was notinitially considered as criterion sine qua non toinclude a case in this study when all other charac-teristic histopathologic features of erythema indu-ratum of Bazin were present. However, becausevasculitis was evident in most cases, we recorded inall those cases the nature, size, and localization of theinvolved blood vessel. We also recorded the natureof the inflammatory cells involving the fat lobule,and the lesions were classified into two main cate-gories: (1) early lesions, when the inflammatoryinfiltrate was mainly composed of neutrophils, withor without leukocytoclasis; and (2) fully developedlesions, when histiocytes and lipophages werethe predominant inflammatory cells within the in-volved fat lobule. Skin biopsy specimens were fixedin 10% buffered formalin, processed, and paraffinembedded according to conventional techniques.Hematoxylin-eosin stain was performed in sections
of each case and, in selected cases, elastic tissue stainwith orcein was performed to determine the natureof the vessels involved by vasculitis. At least 10sections were studied in each case. When vasculitiswas evident in some of these first 10 sections, nofurther sections were cut, but when histopathologicfeatures of vasculitis were not found in the first 10sections, serial sections throughout the specimenwere performed, looking for vasculitis.
RESULTSBriefly, the clinical features of the 86 patients were
the following: 69 patients were female and 17 weremale. Age ranged from 23 to 81 years (median 55.8years). All patients showed erythematous subcuta-neous nodules in the back of the legs, and in 10 casesthere were also some scattered erythematous nod-ules on the front of the legs or on the thighs. Twofemale patients also showed erythematous nodulesinvolving the buttocks and one female patient hadlesions involving both the lower and upper limbsand the trunk. Most patients had new bouts of lesionsor worsening of pre-existing nodules during thewinter. Associated diseases included history ofextracutaneous tuberculosis (including tuberculosis

J AM ACAD DERMATOL
NOVEMBER 2008
844 Segura et al
Fig 4. Fully developed lesion of erythema induratum of Bazin showing mostly lobularpanniculitis with vasculitis involving both large septal veins and small vessels, probablyvenules, of center of fat lobule. A, Scanning power. B, Higher magnification showing lobularpanniculitis with granulomatous infiltrate. C, Vasculitis involving large vein at septa. D,Necrotizing vasculitis involving small blood vessels at center of fat lobule. (A to D,Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C, 3200; D, 3400.)
of the lung, lymph nodes, kidney, or bowel) in 12cases (13.95%), previous episodes of superficialthrombophlebitis of the lower legs in 3 cases(3.72%), rheumatoid arthritis in one case (1.16%),Crohn disease in one case (1.16%), chronic lympho-cytic leukemia in two cases (2.32%), hypothyroidismin two cases (2.32%), and positive serology forhepatitis B virus in 4 cases (4.65%) and for hepatitisC virus in 5 cases (5.81%).
Histopathologically, some type of vasculitis wasevident in the first 10 sections of 91 cases (90.09%). Inthe remaining 10 biopsy specimens (9.9%), serialsections failed to demonstrate clear-cut histopatho-logic features of vasculitis. In all, 47 biopsy speci-mens (46.5%) showed a mostly lobular panniculitiswith necrotizing vasculitis involving the small ves-sels, probably venules, of the center of the fat lobule.There was no involvement of the septal vessels(small or large septal vessels). This vasculitic patternwas seen both in early lesions (with neutrophilicinfiltrate in the fat lobule, 23 cases [22.7%]) (Fig 1)and in fully developed lesions (with granulomatousinfiltrate within the fat lobule, 24 cases [23.7%])(Fig 2). Thirteen biopsy specimens (12.8%) showed
a mostly lobular panniculitis with vasculitis involvingboth large septal veins and small vessels, probablyvenules, of the center of the fat lobule. This vasculiticpattern was seen both in early lesions (5 cases [4.9%])(Fig 3) and in fully developed lesions (8 cases [7.9%])(Fig 4). Twelve biopsy specimens (11.8%) showed amostly lobular panniculitis with vasculitis involvinglarge septal veins, with no involvement or otherseptal or lobular vessels. This vasculitic pattern wasseen both in early lesions (2 cases [1.9%]) (Fig 5) andin fully developed lesions (10 cases [9.9%]) (Fig 6).Ten biopsy specimens (9.9%) showed a mostlylobular panniculitis with vasculitis involving largeseptal vessels, both arteries and veins, and necrotiz-ing vasculitis involving the small vessels, probablyvenules, of the center of the fat lobule. This vasculiticpattern was only seen in biopsy specimens of earlystages of erythema induratum of Bazin (Fig 7). Ninebiopsy specimens (8.9%) showed a mostly lobularpanniculitis with vasculitis involving large septalvessels (both arteries and veins), but with no in-volvement of the small blood vessels of the center ofthe fat lobule. This vasculitic pattern was seen bothin biopsy specimens of early lesions (8 cases [7.9%]

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 845
Fig 5. Early lesion of erythema induratum of Bazin showing mostly lobular panniculitis withvasculitis involving large septal veins, with no involvement or other septal or lobular vessels.A, Scanning power. B, Higher magnification showing lobular panniculitis. C, Inflammatoryinfiltrate of fat lobule was mainly composed of neutrophils. D, Vasculitis involving large vein atsepta. (A to D, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C andD, 3200.)
(Fig 8) and in fully developed lesions (one biopsyspecimen [0.9%]). In all cases with some type ofvasculitis (91 cases, 90.09%), vascular damage wasseen in all of the 10 performed sections, it waslocated at the center of the panniculitic process (Figs1 to 8), and there was not any case in which vasculitiswas identified without inflammation of the sur-rounding subcutaneous tissue. We did not find anyrelationship between the presence of histologiculceration and the nature of the inflamed vessels,because histologic ulceration was evident only in 8cases (7.9%), and two of them (1.9%) showed vas-culitis involving large arteries and veins of the septaof the subcutaneous septa, whereas the remaining 6ulcerated cases (5.94%) showed vasculitis involvingthe small blood vessels of the fat lobule without anydamage of the large arteries or veins of the connec-tive tissue septa. Extravasated red cells were seen inthe vicinity of the inflamed vessels in most cases.Finally, 10 biopsy specimens (9.9%), showed amostly lobular panniculitis without evidence of sep-tal or lobular vasculitis in serial sections and thispattern with no vasculitis was seen both in earlylesions (two cases [1.9%]) (Fig 9) and in fully
developed lesions (8 cases [7.9%]) (Fig 10). Fromthese 10 biopsy specimens without evidence ofvasculitis in serial sections, two biopsy specimenswere from the same patient. Another 3 patients withtwo biopsy specimens showed septal large venousvasculitis in one biopsy specimen, but no evidenceof vasculitis was seen in the other one. The remain-ing 5 biopsy specimens without vasculitis belongedto patients with only one biopsy specimen. Table Isummarized the histopathologic features of ourseries.
DISCUSSIONIn our experience, veins of the connective tissue
septa and small venules of the fat lobule are the mostcommon blood vessels affected by vasculitis inerythema induratum of Bazin, because 90.9% ofour cases showed some type of venous vasculitis,whereas arteries and arterioles were only involved in18.8% of the cases, and in all these cases with arterialvasculitis, some type of venous vasculitis was con-comitantly identified. In other words, no case withexclusive arterial or arteriolar vasculitis was found inour series. It was also remarkable that arterial and

J AM ACAD DERMATOL
NOVEMBER 2008
846 Segura et al
Fig 6. Fully developed lesion of erythema induratum of Bazin showing mostly lobularpanniculitis with vasculitis involving large septal veins, with no involvement or other septal orlobular vessels. A, Scanning power. B, Higher magnification showing lobular panniculitis.C, Granulomatous inflammatory infiltrate involving fat lobule. D, Vasculitis involving largevein at septa. (A to D, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C andD, 3200.)
arteriolar vasculitis was mostly seen in biopsy spec-imens with a predominant neutrophilic infiltrateinvolving the fat lobule (there was only one casewith involvement of both large arteries and veins ofthe septa and granulomatous infiltrate at the fatlobule), which probably indicates that involvementof arterial vessels of the subcutaneous fat is onlypresent in early stages of the evolution of the lesions.Curiously enough, in 10 biopsy specimens of thisseries, which showed all stereotypical clinicopatho-logic features of erythema induratum of Bazin, serialsections throughout the specimens failed to identifyclear-cut histopathologic features of vasculitis.Furthermore, in one patient of our series, whoshowed all classic clinicopathologic features of ery-thema induratum of Bazin, two biopsies wereperformed from two separate episodes of the pan-niculitic process and no evidence of vasculitis wasfound in either of the two biopsy specimens,whereas another 3 patients with two biopsy speci-mens showed vasculitis of the large septal veins inone biopsy specimen, but no histopathologic fea-tures of vasculitis could be identified in the otherone. Therefore, although rare, some cases of
erythema induratum of Bazin may show all classicclinicopathologic features of the disorder, exceptvasculitis, and thus the term ‘‘erythema induratum ofBazin’’ is more accurate than ‘‘nodular vasculitis’’ toname this process.
A review of the literature and of the most famoustextbooks of dermatology and dermatopathologyreveals considerable variation about whether or notvasculitis is present in the cutaneous lesions oferythema induratum of Bazin. Even in those casesin which vasculitis is accepted by the investigators asa characteristic histopathologic feature, controversyexists about the size, the nature, and the location ofthe involved vessels. Thus, in some textbooks, vas-culitis is described as a characteristic histopathologicfinding of erythema induratum of Bazin, but thenature, size, and location of the involved vessels arenot established.21 Ackerman22 believes that ‘‘nodularvasculitis is so named because clinically the lesion is anodule, and microscopically it is an arteritis. Thissevere vasculitis, in which neutrophils, lymphocytes,and histiocytes participate, involves a muscular arte-ria and eventuates in ischemic changes withinthe lobule or portions of the lobules supplied by

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 847
Fig 7. Early lesion of erythema induratum of Bazinshowing mostly lobular panniculitis with vasculitis involv-ing large septal vessels, both arteries and veins, andnecrotizing vasculitis involving small vessels of center offat lobule. A and H, Scanning power. B and I, Mostlylobular panniculitis with involvement of large vein ofsepta. C and J, Higher magnification showing vasculitisinvolving large vein of septa. D and K, In other areas withlobular panniculitis vasculitis involved arteries of septa. Eand L, Higher magnification showing involvement ofseptal artery. F, Neutrophilic infiltrate in fat lobule. G,
the affected artery.’’ In our opinion, however, theinvolved vessel illustrated by Ackerman22 as anexample of nodular vasculitis (erythema induratumof Bazin) is better interpreted as a vein rather than asan artery. In our view, this is a frequent mistake in thehistopathologic study of the panniculitides and vas-culitides involving the subcutaneous fat of the lowerlegs, because in these areas the veins of the connec-tive tissue septa of the subcutis show a thicker andmore compact muscular layer than the veins of thesubcutis in other areas of the skin and they often aremisinterpreted as arteries.23 Black,24 in agreementwith Ackerman,22 also considers that arteries are thevessels mainly involved in the lesions of erythemainduratum of Bazin. In contrast, Degos,25 in histextbook of dermatology, considered that erythemainduratum of Bazin is a mostly lobular panniculitiswith vasculitis mainly involving the veins of theconnective tissue septa of the subcutis. A venousvasculitis is also postulated by McKee et al26 in theirlast edition of Pathology of the Skin, because theywrote: ‘‘The histologic features [of nodular vasculitis]combine septal and lobular changes with the pres-ence of vasculitis being a sine qua non (Fig. 9.79). In abiopsy from an established lesion, the septa arewidened and chronically inflamed (Fig. 9.80). Acutevasculitis, affecting veins and venules with a heavyinflammatory cell infiltrate consisting of neutrophils,lymphocytes and histiocytes is typically present,sometimes accompanied by vessel wall necrosisand thrombosis.’’ McKee et al26 failed to establishthe location of the involved vessels, but because theyconsidered that both veins and venules were in-volved, we deduce that they interpreted that thevenous vessels of both the connective tissue septaand the fat lobule were involved. Patterson27 consid-ered that ‘‘vasculitis is frequently present and caninvolve small or medium-size vessels (Fig. 100.8). Itmay be predominantly neutrophilic, lymphocytic orgranulomatous,’’ but he did not establish whether theinvolved vessels were arterial or venous, or whetherthe vasculitic process involved the septa, the fatlobule, or both. Other authors believe that bothvenous and arterial blood vessels are involved inlesions of erythema induratum of Bazin, but discrep-ancy still persists about the size of the vessels,because whereas some of them considered that largeveins and arteries are affected,28 others stated that
Necrotizing vasculitis involving small blood vessels atcenter of fat lobule. (A to G, Hematoxylin-eosin stain;original magnifications: A, 310; B and D, 340; C, E, and F,3200; G, 3400. H to L, Elastic tissue stain; originalmagnifications: H, 310; I and K, 340; J and L, 3200.)

J AM ACAD DERMATOL
NOVEMBER 2008
848 Segura et al
Fig 8. Early lesion of erythema induratum of Bazin showing mostly lobular panniculitis withvasculitis involving large septal vessels, both arteries and veins, but with no involvement ofsmall blood vessels of center of fat lobule. A, Scanning power. B, Involvement of both arteryand vein of septa. C, Involved artery shows intense fibrinoid necrosis of tunica intima. D,Despite intense fibrinoid necrosis of artery, internal elastic membrane is still discernible. (A toD, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C, 3200; D, 3400.)
only small and medium arteries and veins are in-volved,29 and finally others described involvement ofall sizes of arteries and veins.30 Curiously, evenwithinthe same textbook, there are discrepancies betweendifferent chapters, because in a textbook edited byFarmer and Hood, Pathology of the Skin, Olsen31
considered in the chapter of vasculitis that nodularvasculitis was ‘‘a panarteritis involving a small tomedium-sized artery, typically in the subcutis,’’whereas Dahl and Su,32 in their chapter of pannicu-litis, dealing with erythema induratum of Bazin-nodular vasculitis, described that ‘‘vasculitis, usuallylymphohistiocytic, involves venules, veins, and evenarterioles and small arteries in the pannicular septae.’’
In a recent series of 20 patients with erythemainduratum of Bazin-nodular vasculitis, the lesionswere histopathologically classified into two types:focal panniculitis (type I) and diffuse panniculitis(type II). In type I erythema induratum of Bazin-nodular vasculitis, only one artery or a small bloodvessel within the fat lobule was involved by neutro-philic vasculitis. In type II erythema induratum ofBazin-nodular vasculitis, several blood vessels ofdifferent sizes both in the septa and the fat lobule
showed features of neutrophilic vasculitis. Necrosisof the adipocytes and inflammatory response weremore intense in type II.33 In our opinion, thisclassification is difficult to apply in a particularcase, because the intensity of inflammation of thefat lobules often varies from one lobule to anotherwithin the same biopsy specimen. Furthermore, inour experience this system of classification is not ofpractical use, because in the cases that we arereporting in this series we did not find correlationbetween the intensity of inflammatory infiltratewithin the fat lobule and the number, size, nature,and location of the involved blood vessels of thesubcutis. Moreover, in some cases of erythemainduratum of Bazin with all the stereotypical clini-copathologic features of erythema induratum ofBazin-nodular vasculitis, serial sections throughoutthe block of a subcutaneous nodule did not demon-strate findings of vasculitis. Therefore, we do notconsider vasculitis as a sine qua non criterion toestablish the diagnosis of erythema induratum ofBazin when other characteristic findings are present.
Another major problem in dealing with smallblood vessel vasculitis in the context of neutrophilic

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 849
Fig 9. Early lesion of erythema induratum of Bazin. Serial sections failed to demonstratevasculitis. A, Scanning power. B, Higher magnification showing mostly lobular panniculitis.C, Inflammatory infiltrate of fat lobule was mostly composed of neutrophils. D, Still highermagnification showing neutrophils and some nuclear dust, but no evidence of vasculitis. (A toD, Hematoxylin-eosin stain; original magnifications: A, 310; B, 340; C, 3200; D, 3400.)
lobular panniculitis is the question of whether or notthe vascular injury is primary. Cutaneous vasculitiscan be classified into primary, secondary, or inci-dental.34 Primary vasculitis is idiopathic and impliesthat the vascular insult is the predominant patho-genic factor in the process. Examples of primarycutaneous vasculitis include most cases of cutaneousleukocytoclastic vasculitis, polyarteritis nodosa,giant cell arteritis, and antineutrophilic cytoplasmicantibodyepositive vasculitis syndromes, includingWegener granulomatosis, Churg-Strauss syndrome,and microscopic polyangiitis. In contrast, secondaryvasculitis is caused by and part of a known disease,and although inflammation is also directed at vesselwall constituents, there is one more process in wider,often inflammatory syndromes. Secondary cutane-ous vasculitic syndromes include lupuserythematosus vasculitis, rheumatoid vasculitis, ma-lignancy-induced vasculitis, infection-induced vas-culitis, and drug-induced vasculitis. Finally,incidental vasculitis refers to focal vasculitis foundwithin a predominantly neutrophilic infiltrate, suchas in venous ulcers of the lower legs or in earlylesions of herpes simplex and herpes zoster, and it isaccepted that this incidental vasculitis has no
pathogenic role in the process and the vascularcollateral damage is caused by a nonvasculitic insultto the vessels. Inflammation is not directed at thevessel, but the vessels are damaged because they arein the vicinity of the insult.34 In this sense, it might beinterpreted that the leukocytoclastic vasculitis in-volving the small blood vessels of the fat lobule seenin early lesions of erythema induratum of Bazin witha mostly neutrophilic infiltrate within the fat lobulewas a secondary infective vasculitis as a result of Mtuberculosis or even an incidental vasculitis within aneutrophilic infiltrate. However, there are severalfeatures that militate against these possibilities.Concerning infective vasculitis, M tuberculosis hasbeen demonstrated by polymerase chain reactiontechniques in cases of erythema induratum of Bazinof some countries, but not in cases from othergeographic areas and, if the process is the same inall areas,8-10 another pathogenic factor besides Mtuberculosis must be involved in the process. Finally,the vasculitic process involving the small bloodvessels of the fat lobules in most of our cases oferythema induratum of Bazin can not be interpretedas an incidental vasculitis. First of all, necrotizingleukocytoclastic vasculitis of the small blood vessels

J AM ACAD DERMATOL
NOVEMBER 2008
850 Segura et al
Fig 10. Fully developed lesion of erythema induratum of Bazin. Serial sections failed todemonstrate vasculitis. A, Scanning power. B, Higher magnification showing mostly lobularpanniculitis. C, Granulomatous infiltrate involving fat lobule. D, Higher magnification ofhistiocytic infiltrate with no evidence of vasculitis. (A to D, Hematoxylin-eosin stain; originalmagnifications: A, 310; B, 340; C, 3200; D, 3400.)
Table I. Type of involved vessels in vasculitis in 101 biopsy specimens from 86 patients with erythemainduratum of Bazin
Lobular venules
Lobular venules 1
septal veins Septal veins
Lobular venules 1
septal veins 1
septal arteries
Septal veins 1
septal arteries No vasculitis
47 Cases (46.5%) 13 Cases (12.8%) 12 Cases (11.8%) 10 Cases (9.9%)(All cases were EL)
9 Cases (8.9%) 10 Cases (9.9%)
- EL: 23 cases(22.7%)
- EL: 5 cases(4.9%)
- EL: 2 cases(1.9%)
- EL: 8 cases(7.9%)
- EL: 2 cases(1.9%)
- FDL: 24 cases(23.7%)
- FDL: 8 cases(7.9%)
- FDL: 10 cases(9.9%)
- FDL: 1 case(0.9%)
- FDL: 8 cases(7.9%)
EL, Early lesions (mostly neutrophilic infiltrate); FDL, fully developed lesions (mostly histiocytic infiltrate).
was seen not only in early lesions of our series, butalso in many biopsy specimens from fully developedlesions with a predominantly granulomatous infil-trate involving the fat lobule. Second, besides ery-thema induratum of Bazin, there are several otherpanniculitic processes with a predominantly neutro-philic infiltrate within the fat lobule, such as neutro-philic lobular panniculitis or subcutaneous Sweetsyndrome, pancreatic panniculitis, alpha-1-antitryp-sin deficiencyeassociated panniculitis, infective pan-niculitis, and factitial panniculitis, which do no showleukocytoclastic vasculitis of the small blood vesselsof the fat lobule.35 Therefore, we think that the most
common type of vasculitis seen in biopsy specimensof erythema induratum of Bazin has pathogenicsignificance and it must be considered as primaryvasculitis.
In conclusion, although there is no consensusabout the nature, size, and location of the involvedvessels in erythema induratum of Bazin, on the basisof the findings of this series, we consider vasculitis asalmost always present in lesions of erythema indu-ratum of Bazin, and the nature, location, and size ofthe involved vessels is, from more to less frequent, asfollows: (1) small venules of the fat lobule; (2) bothveins of the connective tissue septa and venules of the

J AM ACAD DERMATOL
VOLUME 59, NUMBER 5
Segura et al 851
fat lobule; (3) only veins of the connective tissuesepta; (4) veins and arteries of the connective tissuesepta and venules of the fat lobule; and (5) veins andarteries of the connective tissue septa. Because sometype of vasculitis is seen both in early and fullydeveloped lesions and because vasculitis is moreconsistently present in lesions of erythema induratumof Bazin than in other mostly lobular panniculitis, wethink that vasculitis plays an important role in thepathogenesis of this process. However, vasculitisshould not be considered as a criterion sine qua nonfor histopathologic diagnosis of erythema induratumof Bazin when all other clinicopathologic features ofthe process are consistent with that diagnosis.
REFERENCES
1. Bazin E. Lecons Theoriques et Cliniques sur la Scrofule. 2nd ed.
Paris: A. Delahaye; 1861. p. 146.
2. Cribier B, Grosshans E. Erytheme indure de Bazin: concept
et terminology obsoletes. Ann Dermatol Venereol 1990;117:
937-43.
3. Galloway J. A probable case of Bazin’s disease. Br J Dermatol
1899;11:206-7.
4. Whitfield A. On the nature of the disease known as erythema
induratum scrofulosorum. Br J Dermatol 1901;13:386-7.
5. Whitfield A. A further contribution to our knowledge of
erythema induratum. Br J Dermatol 1905;15:241-7.
6. Montgomery H, O’Leary PA, Barker NW. Nodular vascular
diseases of the legs: erythema induratum and allied condi-
tions. JAMA 1945;128:335-45.
7. Ryan TJ, Wilkinson DS. Cutaneous vasculitis (‘‘angiitis’’). In:
Rook A, Wilkinson DS, Ebling FJD, editors. Textbook of
dermatology. 1st, 2nd, and 3rd eds. Oxford: Blackwell Scientific
Publications; 1968, 1972, and 1979.
8. de Moragas JM. Nodules-on-the leg syndrome. In: Fitzpatrick
TB, Arndt KA, Clark WH Jr, Eisen AZ, van Scott EJ, Vaugan JH,
editors. Dermatology in general medicine. 1st ed. New York:
McGraw-Hill; 1971. pp. 1471-81.
9. Wolff K. Mycobacterial diseases: tuberculosis. In: Fitzpatrick TB,
Arndt KA, Clark WH Jr, Eisen AZ, van Scott EJ, Vaugan JH,
editors. Dermatology in general medicine. 1st ed. New York:
McGraw-Hill; 1971. pp. 1743-68.
10. Requena L, Sanchez Yus E, Kutzner H. Panniculitis. In: Wolff K,
Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, LeFFell DJ,
editors. Fitzpatricks’s dermatology in general medicine. 7th
ed. New York: McGraw Hill Medical; 2008. pp. 569-85.
11. Wolff K, Tappenier G, Wolf K. Mycobacterial diseases: tuber-
culosis and atypical mycobacterial infections. In: Fitzpatrick TB,
Eisen AZ, Wolff K, editors. Dermatology in general medicine.
3rd ed. New York: McGraw-Hill; 1987. pp. 2152-80.
12. Baselga E, Margall N, Barnadas MA, Coll P, de Moragas JM.
Detection of Mycobacterium tuberculosis DNA in lobular gran-
ulomatous panniculitis (erythema induratum-nodular vasculi-
tis). Arch Dermatol 1997;133:457-62.
13. Faizal M, Jimenez G, Burgos C, del Portillo P, Romero RE, Elkin-
Patarroyo M. Diagnosis of cutaneous tuberculosis by poly-
merase chain reaction using a species-specific gene. Int J
Dermatol 1996;35:185-8.
14. Degitz K, Messer G, Schirren H, Clessen V, Meurer M. Successful
treatment of erythema induratum of Bazin following rapid
detection of mycobacterial DNA by polymerase chain reaction.
Arch Dermatol 1993;129:1619-20.
15. Schneider JW, Geiger DH, Rossouw DJ, Jordaan HF, Victor T,
van Helden PD. Mycobacterium tuberculosis DNA in erythema
induratum of Bazin. Lancet 1993;342:747-8.
16. Schneider JW, Jordaan HF, Geiger DH, Victor T, van Helden PD,
Rossouw DJ. Erythema induratum of Bazin: a clinicopathologic
study of 20 cases and detection of Mycobacterium tuberculosis
DNA in skin lesions by polymerase chain reaction. Am J
Dermatopathol 1995;17:350-6.
17. Lopez-Estebaranz JL, Iglesias Diez L. Paniculitis lobulillar;
eritema indurado-vasculitis nodular: utilidad de la reaccion
en cadena de la polimerasa en el diagnostico etiopatogenico.
In: Peyri Rey J, editor. Actualizacion en Dermatologıa. Madrid,
Spain: Aula Medica; 1994. pp. 67-78.
18. Degitz K. Detection of mycobacterial DNA in the skin. Arch
Dermatol 1996;132:71-5.
19. Penneys NS, Leonardi CL, Cook S, Blauvelt A, Rosemberg S,
Eells LD, et al. Identification of Mycobacterium tuberculosis
DNA in five different types of cutaneous lesions by polymer-
ase chain reaction. Arch Dermatol 1993;129:1594-8.
20. Yen A, Rady PL, Cortes-Franco R, Tyring SK. Detection of
Mycobacterium tuberculosis in erythema induratum of Bazin
using polymerase chain reaction. Arch Dermatol 1997;133:
532-3.
21. Barham KI, Jorizzo JL, Grattan B, Cox NH. Nodular vasculitis. In:
Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s
textbook of dermatology. 7th ed. Oxford: Blackwell Publishing;
2004. pp. 49.18-9.
22. Ackerman AB. Histologic diagnosis of inflammatory skin
diseases. 1st ed. Philadelphia: Lea and Febiger; 1978. p. 779-
825.
23. Sanchez Yus E, Simon P, Sanz Vico D. ¿Vena o arteria? Una
cuestion decisiva en patologıa hipodermica. Piel 1987;2:213-7.
24. Black M. Panniculitis. J Cutan Pathol 1985;12:366-80.
25. Degos R. Dermatologie. Paris: Flammarion; 1953. p. 578.
26. McKee PH, Calonje E, Granter SR. Nodular vasculitis. In:
Pathology of the skin with clinical correlations. 3rd ed.
London: Elsevier-Mosby; 2005. pp. 366-9.
27. Patterson JW. Panniculitis. In: Bolognia JL, Jorizzo J, Rapini RP,
Callen JP, et al. editors. Dermatology. Barcelona, Spain: Mosby
Elsevier; 2008. pp. 1515-35.
28. Mehregan A, Hashimoto K, Mehregan D, Mehregan D. Nodular
vasculitis. In: Pinkus’ guide to dermatohistopathology. 6th ed.
Norwalk (CT): Appleton and Lange; 1995. pp. 246-7.
29. McNutt NS, Moreno A, Contreras F. Erythema induratum
(nodular vasculitis). In: Elder DE, Elenitas R, Johnson BL,
Murphy GE, editors. Lever’s histopathology of the skin. 9th
ed. Philadelphia: Lippincott-Williams and Wilkins; 2005. pp.
529-30.
30. Weedon D. Eryhema induratum-nodular vasculitis. In: Skin
pathology. 2nd ed. London: Churchill Livingstone; 2002. pp.
524-5.
31. Vasculitis Olsen TG. In: Farmer ER, Hood AF, editors. Pathology
of the skin. 2nd ed. New York: McGraw-Hill; 2000. pp. 293-326.
32. Dahl PR, Su WPD. Panniculitis. In: Farmer ER, Hood AF, editors.
Pathology of the skin. 2nd ed. New York: McGraw-Hill; 2000.
pp. 453-86.
33. Schneider JW, Jordaan HF. The histopathologic spectrum of
erythema induratum of Bazin. Am J Dermatopathol 1997;19:
323-33.
34. Carlson JA, Ng BT, Chen K-R. Cutaneous vasculitis update:
diagnostic criteria, classification, epidemiology, etiology, path-
ogenesis, evaluation and prognosis. Am J Dermatopathol
2005;27:504-28.
35. Requena L, Sanchez Yus E. Panniculitis, part II: mostly lobular
panniculitis. J Am Acad Dermatol 2001;45:325-61.