Vascular Pharmacology Phil Copeman and Alex Hammant.
22
Vascular Pharmacology Phil Copeman and Alex Hammant
-
Upload
charleen-flynn -
Category
Documents
-
view
219 -
download
0
Transcript of Vascular Pharmacology Phil Copeman and Alex Hammant.

Vascular PharmacologyPhil Copeman and Alex Hammant

Haemostasis drugs Antiplatelets
Aspirin
Clopidogrel
Abciximab, tirofiban and eptifibatide
Anticoagulants Heparin
Unfractionated
LMWH
Fondaparinux
Warfarin
Rivaroxaban
Dabigatran
Bivalirudin
Fibrinolytics
• Alteplase
• Streptokinase activator complex / anistreplase

What are the two main stages of clotting?
Primary Haemostasis – haemostatic plug formation (Platelet aggregation)
Secondary Haemostasis - clot formation (Fibrin cleavage)
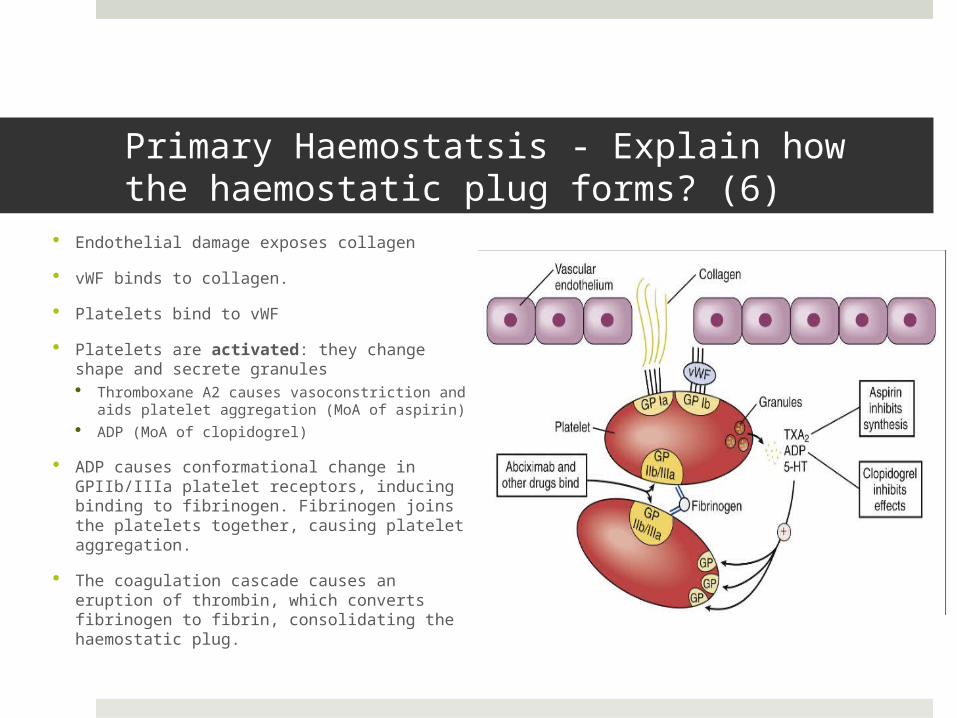
Primary Haemostatsis - Explain how the haemostatic plug forms? (6)
Endothelial damage exposes collagen
vWF binds to collagen.
Platelets bind to vWF
Platelets are activated: they change shape and secrete granules Thromboxane A2 causes vasoconstriction
and aids platelet aggregation (MoA of aspirin)
ADP (MoA of clopidogrel)
ADP causes conformational change in GPIIb/IIIa platelet receptors, inducing binding to fibrinogen. Fibrinogen joins the platelets together, causing platelet aggregation.
The coagulation cascade causes an eruption of thrombin, which converts fibrinogen to fibrin, consolidating the haemostatic plug.

Antiplatelet drugs All antiplatelet drugs
prevent platelet aggregation

Aspirin

Clopidogrel
Normally - Binding of ADP to P2Y12 receptors causes the conformational change of GPIIb/IIIa receptors, allowing them to bind fibrinogen and cause platelet aggregation.
Clopidogrel irreversibly inhibits the P2Y12 receptor, inhibiting the effects of ADP and thereby preventing platelet aggregation.
Basically – “Clopidogrel reduces platelet aggregation by irreversibly blocking the effects of ADP on platelets”
Medical Pharmacology At A Glance, M.J. Neal
It is often used by patients in whom aspirin is contraindicated.

Clopidogrel

Should probably call itVitamin K Epoxide Reductase• Found in
liver

So…which pathway does warfarin effect?
Extrinsic pathway of coagulation

What are the contraindications of warfarin therapy?
Haemorrhagic stroke
Significant bleeding
48 hrs post partum
First trimester of pregnancy
Severe hepatic and renal impairment

Which cytochrome P450 isoform is responsible for the reduction (and thus deactivation) of warfarin?
CYP2A6

What are the side effects of warfarin?
Nausea
Vomiting
Haemorrhage
Diarrhoea
Jaundice
Hepatic dysfunction
Pancreatitis
Pyrexia
Alopecia
Purpura
Rash

If warfarin affects the extrinsic pathway, how would you measure its effect on coagulation?
Prothrombin Time
OR
INR
What is the target INR for most patients taking warfarin?
2.5
Can you think of any conditions where the target INR might be 3.5?
Recurrence of venous thromboembolism whilst on warfarin therapy
Antiphospholipid syndrome
Mechanical prosthetic heart valve
Cornary artery graft thrombosis

How long does it take for warfarin to take its therapeutic effect? Why?
2-4 days
Because it takes time for the clotting factors in the blood to be metabolised/depleted
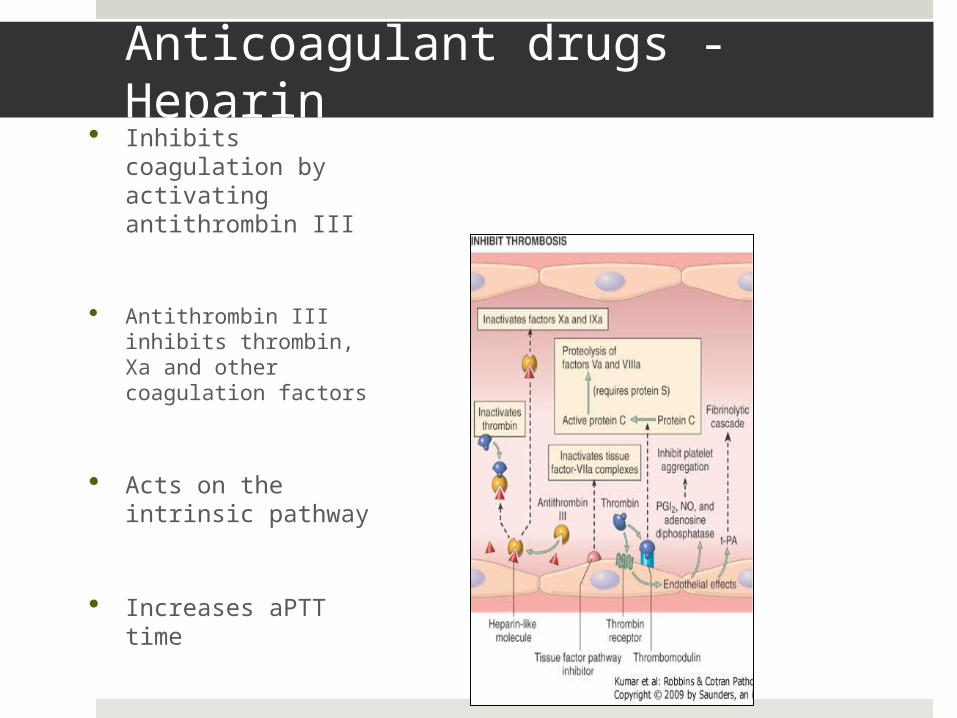
Anticoagulant drugs - Heparin Inhibits coagulation
by activating antithrombin III
Antithrombin III inhibits thrombin, Xa and other coagulation factors
Acts on the intrinsic pathway
Increases aPTT time
Reversed with protamine sulphate

Types of heparin
• Unfractionated heparin• Inhibits thrombin and
Factor Xa• Administered I.V.• Unpredictable
anticoagulant activity so can only be given in hospital because its effects need to be monitored
• Can cause heparin-induced thrombocytopenia
• Low-molecular weight heparin (LMWH) • Administered
subcutaneously• More predictable –
can be given to outpatients
• Fewer side effects• Increase the effect
of antithrombin III on Factor Xa
• Less reversible with protamine sulphate than unfractionated
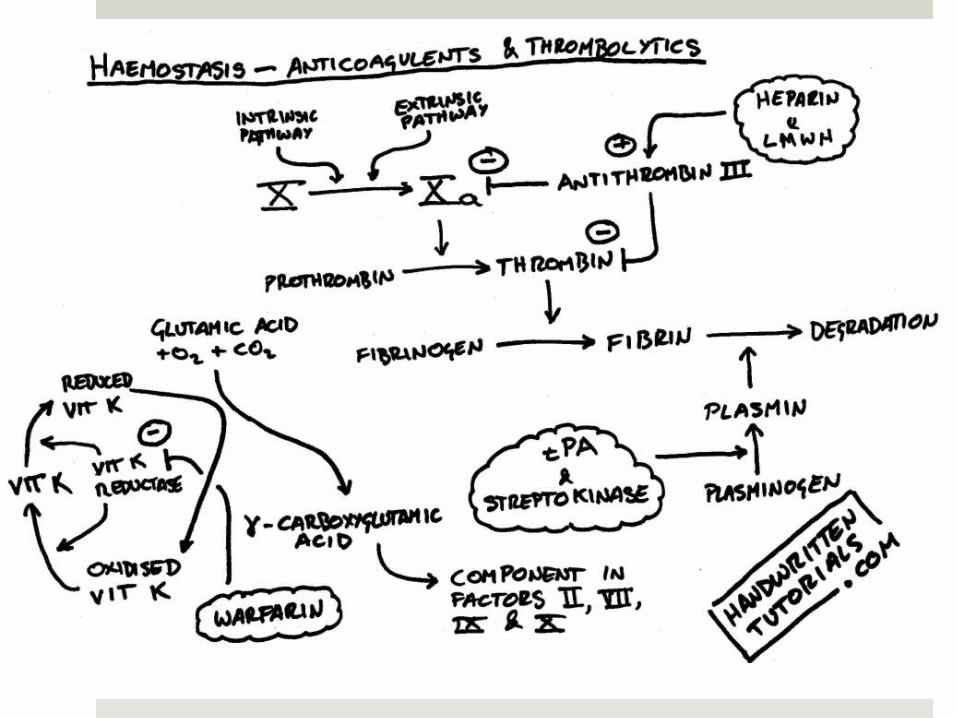
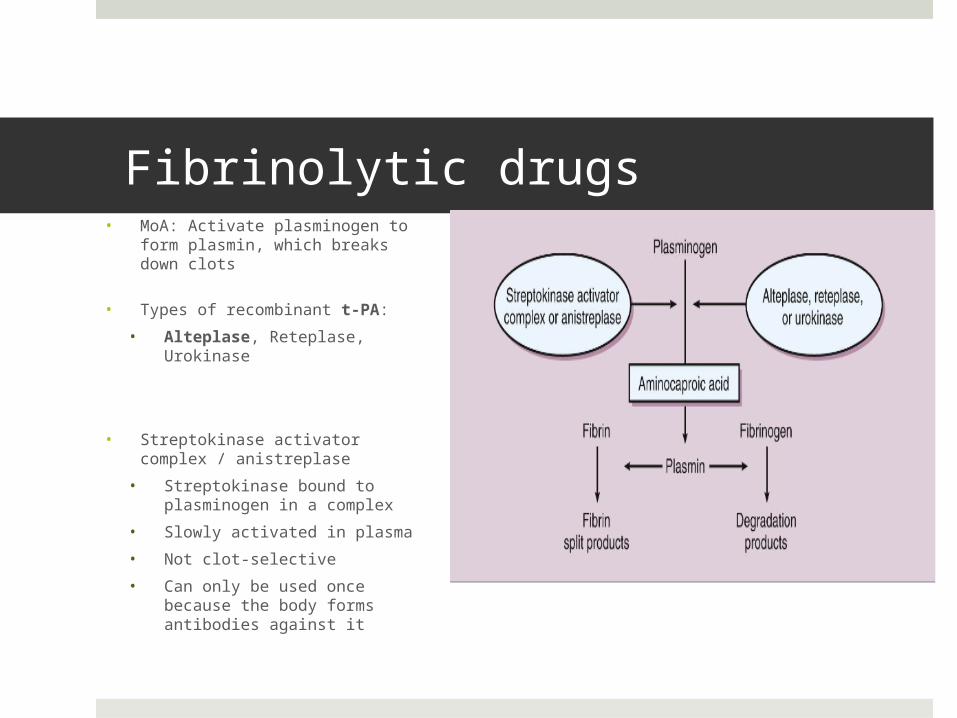
Fibrinolytic drugs• MoA: Activate plasminogen to form
plasmin, which breaks down clots
• Types of recombinant t-PA:
• Alteplase, Reteplase, Urokinase
• Streptokinase activator complex / anistreplase
• Streptokinase bound to plasminogen in a complex
• Slowly activated in plasma
• Not clot-selective
• Can only be used once because the body forms antibodies against it
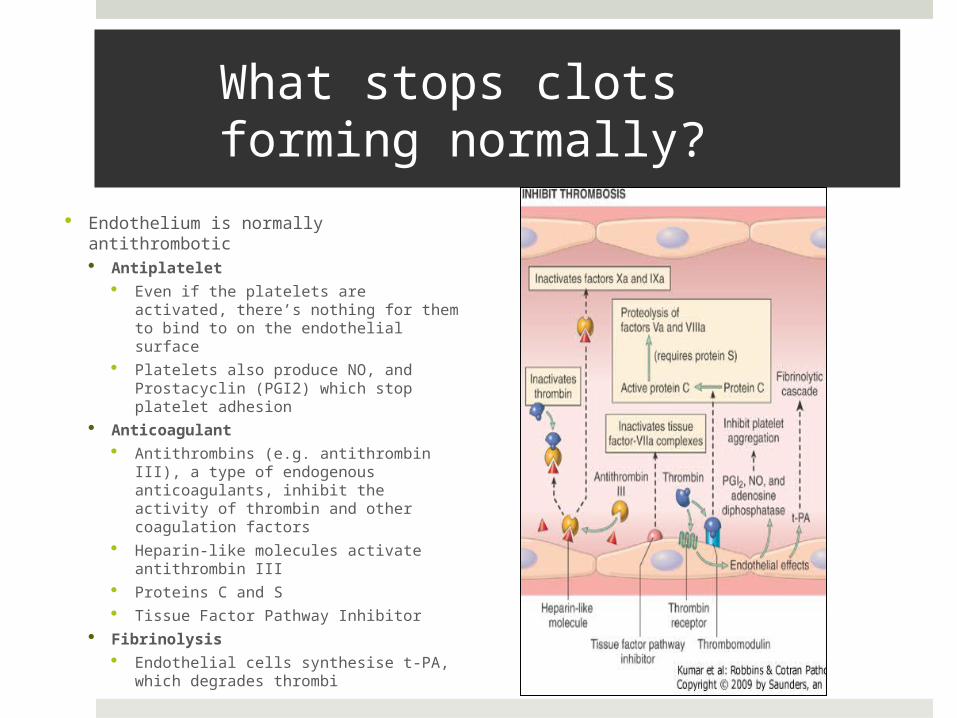
What stops clots forming normally?
Endothelium is normally antithrombotic Antiplatelet
Even if the platelets are activated, there’s nothing for them to bind to on the endothelial surface
Platelets also produce NO, and Prostacyclin (PGI2) which stop platelet adhesion
Anticoagulant Antithrombins (e.g. antithrombin
III), a type of endogenous anticoagulants, inhibit the activity of thrombin and other coagulation factors
Heparin-like molecules activate antithrombin III
Proteins C and S Tissue Factor Pathway Inhibitor
Fibrinolysis Endothelial cells synthesise t-PA,
which degrades thrombi