VAP Bundle
28
Department of Critical Care Medicine, Apollo Hospitals The presentation is solely meant for Academic purpose
-
Upload
apollo-hospitals -
Category
Health & Medicine
-
view
4.672 -
download
3
Transcript of VAP Bundle

Department of Critical Care Medicine, Apollo Hospitals
The presentation is solely meant for Academic
purpose

Department of Critical Care Medicine, Apollo Hospitals
PREVENTING VENTILATOR ASSOCIATED PNEUMONIA
(VAP BUNDLE)

Department of Critical Care Medicine, Apollo Hospitals
Preventing VAP
Definitions
Pathophysiology of
VAP Risk factors
Prevention of VAP Guidelines
Recent advances
Conclusion
Department of Critical Care Medicine, Apollo Hospitals
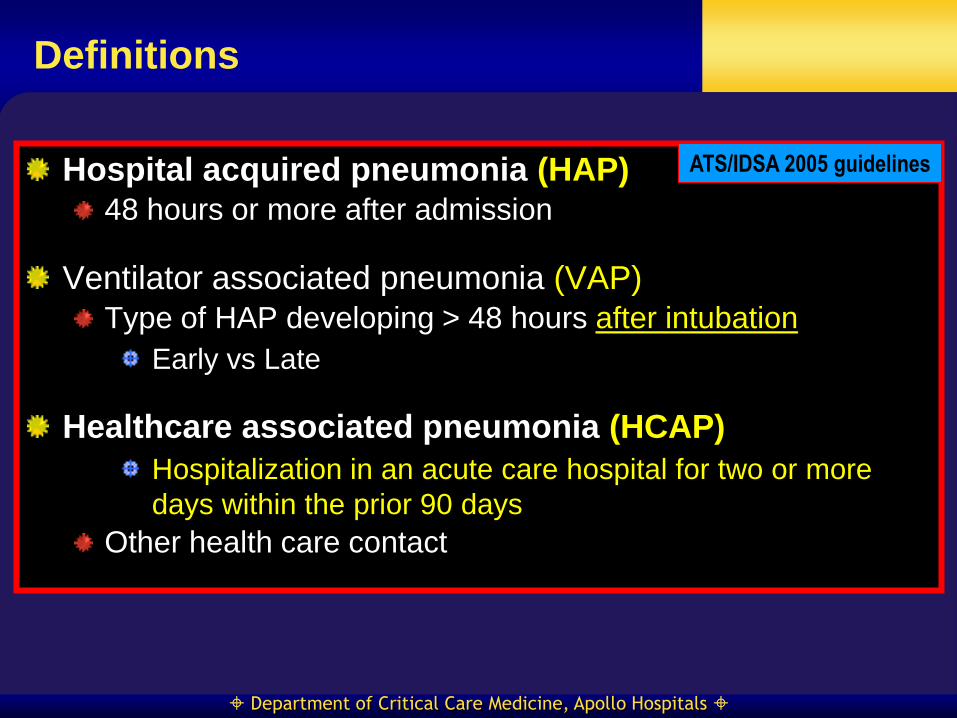
Definitions
Hospital acquired pneumonia (HAP)
48 hours or more after admission
Ventilator associated pneumonia (VAP)
Type of HAP developing > 48 hours after intubation
Early vs Late
Healthcare associated pneumonia (HCAP)
Hospitalization in an acute care hospital for two or more
days within the prior 90 days
Other health care contact
ATS/IDSA 2005 guidelines
Department of Critical Care Medicine, Apollo Hospitals
Risk Factors
It is NOT the Ventilator

Department of Critical Care Medicine, Apollo Hospitals
Risk Factors
Host related Age
Lung disease/ARDS
Immunosuppression
Unconsciousness
Body position
Antibiotic exposure
Chest surgery
Re-intubation/prolonged intubation
Device related ETT
Ventilator circuit
Orogastric and nasogastric tube
Personnel related Hand washing, Noncompliance

Department of Critical Care Medicine, Apollo Hospitals
Bacterial Colonization (Aerodigestive tract, ETT, Ventilator tubings)
Micro-aspiration (Secretions, Vent. Condensate, Aerosols)
Ventilator Associated Pneumonia
Bacteremia
Gut translocation
Bacterial inhalation
Contamination

Department of Critical Care Medicine, Apollo Hospitals
Bacterial Colonization (Oropharynx, Stomach, Sinus, ETT)
Host Factors Antibiotics Gastric pH
Devices – ETT, NGT
Biofilms
Inadequate
infection control practices
Transmission

Department of Critical Care Medicine, Apollo Hospitals

Department of Critical Care Medicine, Apollo Hospitals
Prevention of VAP
General measures
Avoid invasive ventilation
Prevent colonisation
Prevent micro-aspiration
Prevent contamination of equipment
Minimize duration of invasive ventilation
ATS guidelines 2005
SHEA guidelines 2008
Department of Critical Care Medicine, Apollo Hospitals
General Measures
Adequate staffing
Contact isolation for MDR bugs
Conduct active surveillance for VAP
VAP assessment risk
Audit compliance with VAP bundle
Monitor incidence of VAP
Hand-hygiene
Use non-invasive ventilation
Educate health-care personnel
ATS guidelines 2005
SHEA guidelines 2008

Department of Critical Care Medicine, Apollo Hospitals
Hand washing
Before and after suctioning
Touching ventilator equipment
Contact with patients and patient environment
Contact with respiratory secretions
AACN Practice Alert for
VAP, 2004

Department of Critical Care Medicine, Apollo Hospitals
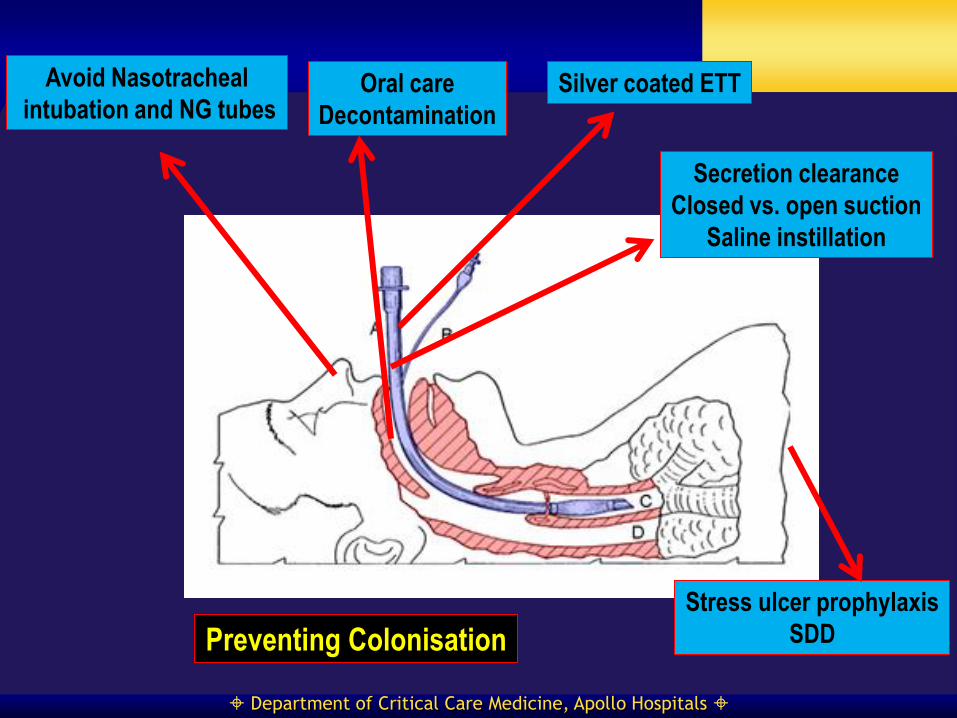
Avoid Nasotracheal
intubation and NG tubes Oral care
Decontamination
Silver coated ETT
Secretion clearance
Closed vs. open suction
Saline instillation
Stress ulcer prophylaxis
SDD Preventing Colonisation

Department of Critical Care Medicine, Apollo Hospitals
Oral Care and Decontamination
Mouth flora = Lung flora Mechanical cleaning
Decontamination –SDD vs SOD1,2
SDD = SOD2
Mortality benefit only in post-hoc analysis2
SDD- Concern about increasing resistance
Stronger data in cardiothoracic and trauma patients3
1-Chan EY et al. BMJ 2007
2-de Smet AM et al. N Engl J Med. 2009
3-O’Grady NP et al. JAMA 2012
Oral Decontamination with Chorhexidine recommended

Department of Critical Care Medicine, Apollo Hospitals
Avoid Nasotracheal
intubation and NG tubes Oral care
Decontamination
Silver coated ETT
Secretion clearance
Closed vs. open suction
Saline instillation
Stress ulcer prophylaxis
SDD Preventing Colonisation

Department of Critical Care Medicine, Apollo Hospitals
Silver Coated ETT
Broad antimicrobial activity
Decreases bacterial adhesion
Decreases Biofilm formation
NASCENT trial – Kollef M et al. JAMA 2008
N=2003
Silver coated vs Uncoated
Primary outcome – VAP by BAL
4.8% vs. 7.5% VAP; P=0.04
NO mortality benefit
Department of Critical Care Medicine, Apollo Hospitals
Avoid Nasotracheal
intubation and NG tubes Oral care
Decontamination
Silver coated ETT
Secretion clearance
Closed vs. open suction
Saline instillation
Stress ulcer prophylaxis
SDD Preventing Colonisation

Department of Critical Care Medicine, Apollo Hospitals
Secretion Management
Secretion clearance Open vs closed suction
Saline instillation
HME vs Heated humidifier
No role for prophylactic systemic antibiotics
Department of Critical Care Medicine, Apollo Hospitals
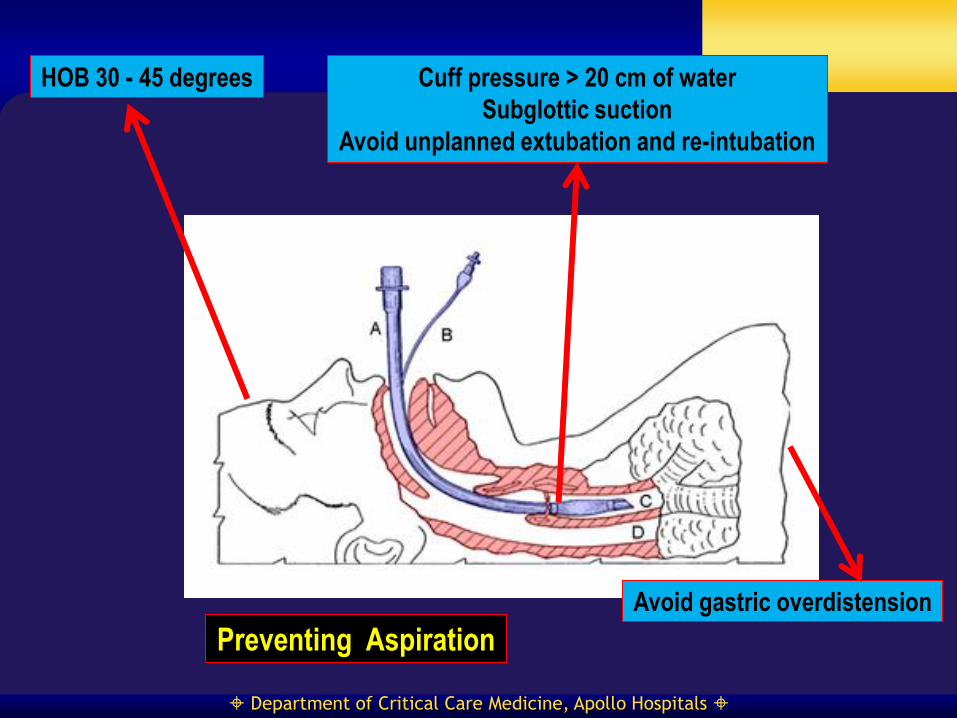
HOB 30 - 45 degrees Cuff pressure > 20 cm of water
Subglottic suction
Avoid unplanned extubation and re-intubation
Avoid gastric overdistension
Preventing Aspiration

Department of Critical Care Medicine, Apollo Hospitals
Preventing Aspiration
Supine position increases
risk and frequency of VAP
Drakulovic MB et al.
Lancet 1999
Drainage of subglottic secretions
decreases aspiration and VAP
Muscedere J et al.
Crit Care Med. 2011
Department of Critical Care Medicine, Apollo Hospitals
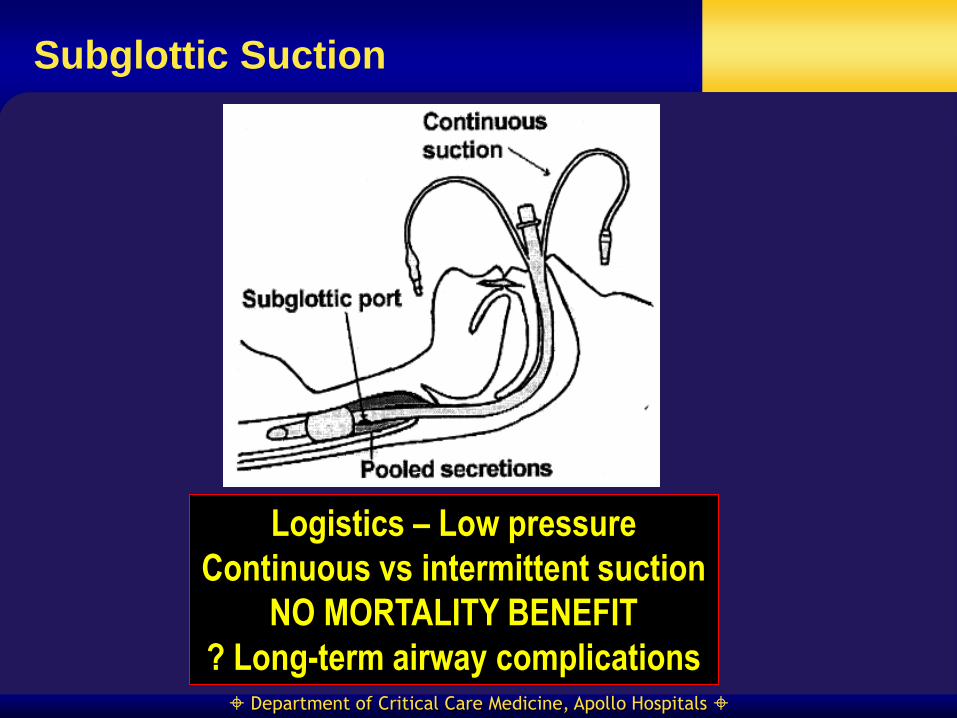
Subglottic Suction
Logistics – Low pressure
Continuous vs intermittent suction
NO MORTALITY BENEFIT
? Long-term airway complications

Department of Critical Care Medicine, Apollo Hospitals
ETT modifications
High volume low-pressure cuffs of ultrathin membrane
Minimize folds
Continuous monitoring of ETT Cuff pressure
Low volume low pressure cuffs
ETT with mucus shaver
Disrupts Biofilm
Department of Critical Care Medicine, Apollo Hospitals
Prevent Contamination of Equipments
Use sterile water to rinse reusable respiratory
equipment
Remove condensate from ventilatory circuits
Keep the ventilatory circuit closed during condensate
removal
Change the ventilatory circuit only when visibly soiled
or malfunctioning
Store and disinfect respiratory therapy equipment
properly SHEA guidelines 2008

Department of Critical Care Medicine, Apollo Hospitals
Minimize Duration of Invasive Ventilation
Spontaneous Awakening Trial
(SAT) Spontaneous Breathing Trial
(SBT)
Consider Extubation to NIV
?Tracheostomy
Department of Critical Care Medicine, Apollo Hospitals
Interventions with unclear Value
Stress ulcer prophylaxis
Need and type
Monitoring gastric residual volume
Silver coated ETT
Promising but need more data
Saline instillation during suction
Newer ETTs – Rationale robust
Data limited
Take Home

Department of Critical Care Medicine, Apollo Hospitals
Prevention of VAP - Bottomline
Adhere to good infection control practices
Avoid invasive ventilation when possible Minimize duration
Prevent colonisation Avoid nasal intubation/NGT
Oral care and decontamination – Chlorhexidine
Prevent micro-aspiration HOB elevation 30-45 degrees
Maintain ETT cuff pressure > 20 cm of water
Subglottic suction
Prevent contamination of equipments Minimize disconnections
Routine change of tubings NOT recommended
Take Home

Department of Critical Care Medicine, Apollo Hospitals

Department of Critical Care Medicine, Apollo Hospitals