VAP Are strict diagnostic criteria advisable? Acq. Pneu Ar… · mechanically ventilated patients...
27
VAP Are strict diagnostic criteria advisable? Javier Garau, MD, PhD 18th Infection and Sepsis Symposium, Porto, 27th February 2013
Transcript of VAP Are strict diagnostic criteria advisable? Acq. Pneu Ar… · mechanically ventilated patients...
VAP
Are strict diagnostic criteria
advisable? Javier Garau, MD, PhD
18th Infection and Sepsis Symposium, Porto, 27th February 2013
• Limitations of current definitions
• Alternatives
-Streamlined definition of VAP
-VAC (?)
- New molecular methods for
microbiological diagnosis
• Conclusions
Limitations of current definitions of
VAP
• 2 major limitations of the standard VAP definition by the CDC:
(1) many of the diagnostic criteria are very subjective
(2) the definition correlates poorly with histological pneumonia
• Interpretation of these criteria is at the discretion of the physician; reasonable observers are likely to arrive at different conclusions and hence very different VAP rates.
Beyersmann J et al. Infect Cont Hosp Ep 2006
Klompas M. Am J Infect Control 2010
Schurink CA et al. Intens Care Med 20046
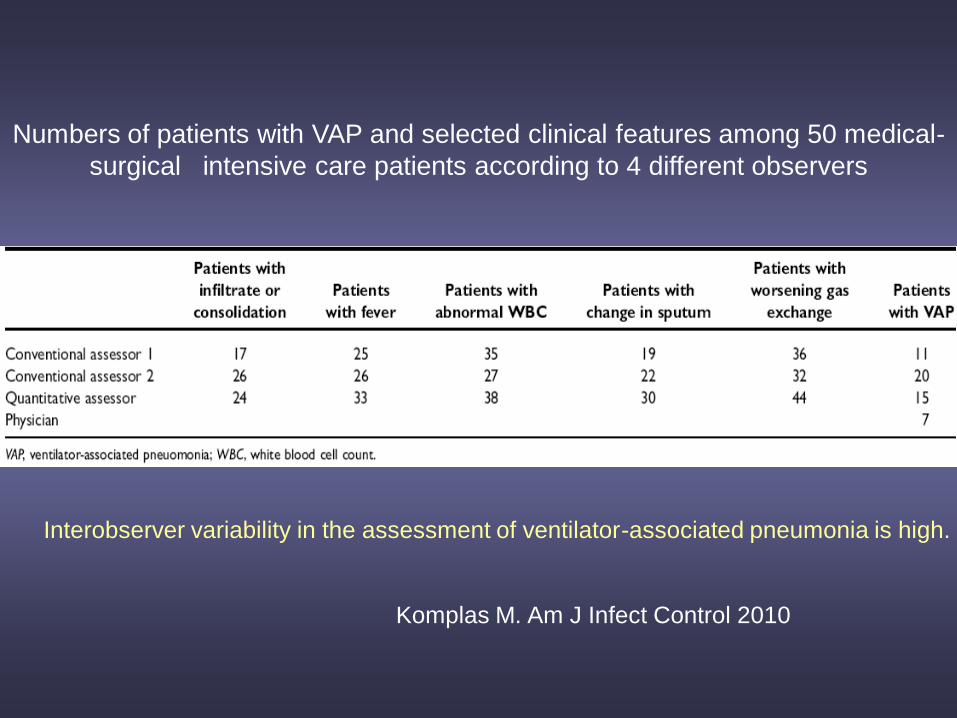
Numbers of patients with VAP and selected clinical features among 50 medical-
surgical intensive care patients according to 4 different observers
Komplas M. Am J Infect Control 2010
Interobserver variability in the assessment of ventilator-associated pneumonia is high.
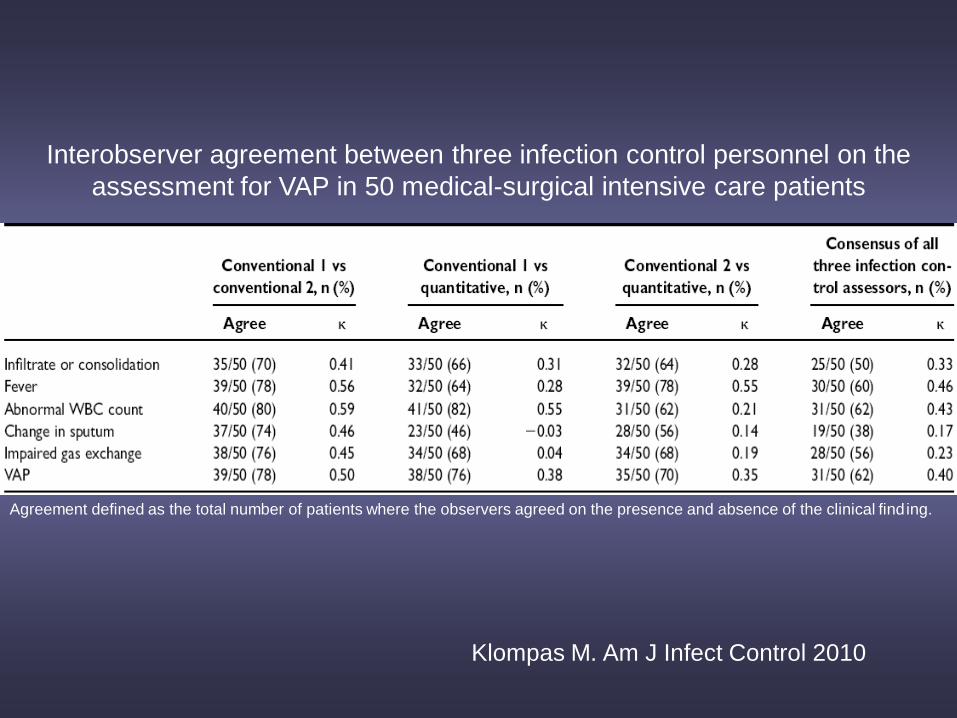
Interobserver agreement between three infection control personnel on the
assessment for VAP in 50 medical-surgical intensive care patients
Agreement defined as the total number of patients where the observers agreed on the presence and absence of the clinical finding.
Klompas M. Am J Infect Control 2010
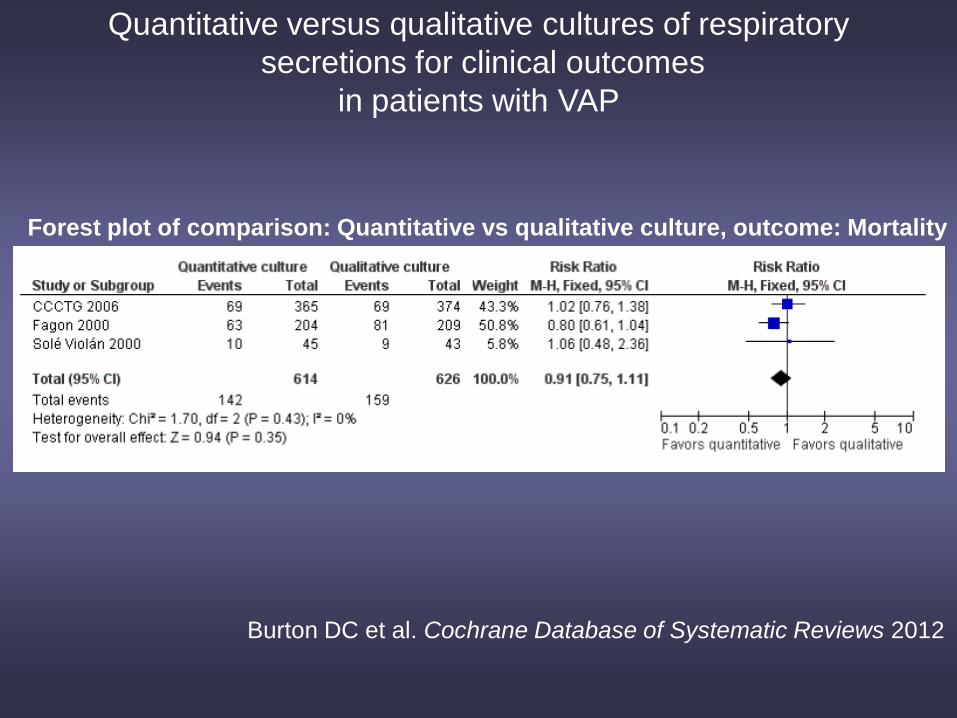
Forest plot of comparison: Quantitative vs qualitative culture, outcome: Mortality
Burton DC et al. Cochrane Database of Systematic Reviews 2012
Quantitative versus qualitative cultures of respiratory
secretions for clinical outcomes
in patients with VAP
Pulmonary Infiltrates
• The requirement for radiographic evidence
has been identified as the most
problematic because the interpretations of
radiographs and the language used in
reporting radiographic findings vary within
and among institutions.
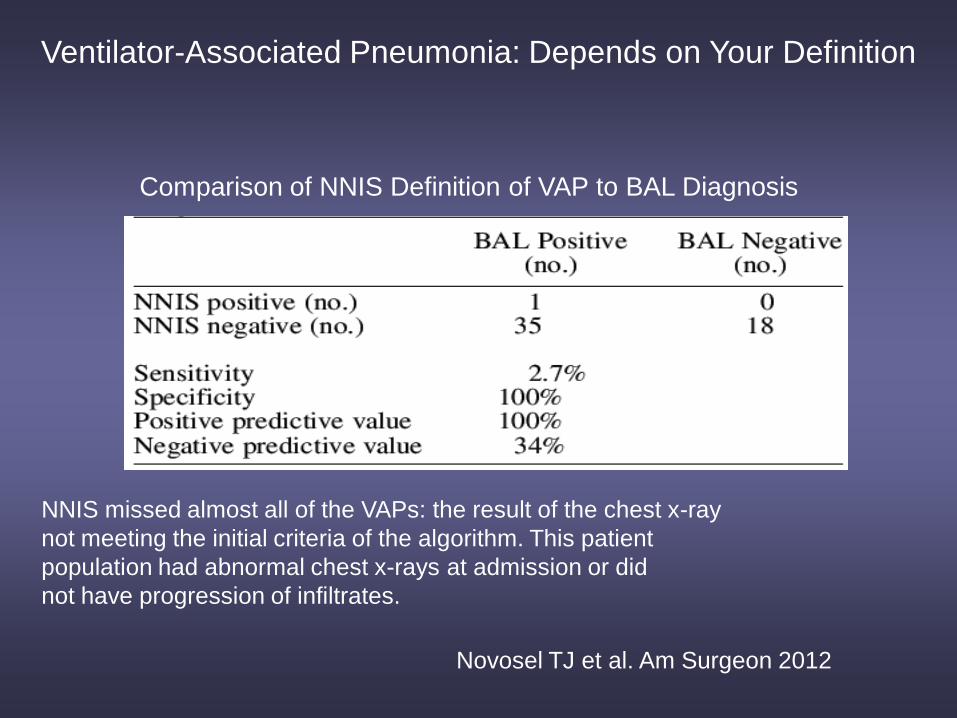
NNIS missed almost all of the VAPs: the result of the chest x-ray
not meeting the initial criteria of the algorithm. This patient
population had abnormal chest x-rays at admission or did
not have progression of infiltrates.
Comparison of NNIS Definition of VAP to BAL Diagnosis
Ventilator-Associated Pneumonia: Depends on Your Definition
Novosel TJ et al. Am Surgeon 2012
• It might be possible, however, to improve
surveillance objectivity by limiting the
definition to objective and quantifiable
components.
• Focusing on objective criteria should also
improve efficiency
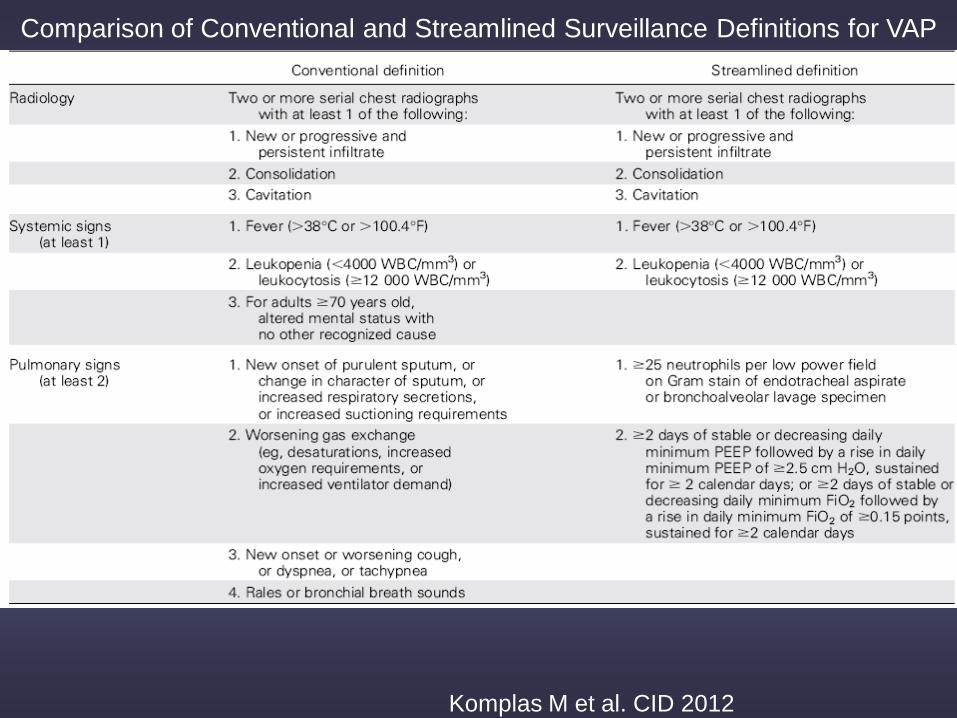
Comparison of Conventional and Streamlined Surveillance Definitions for VAP
Komplas M et al. CID 2012
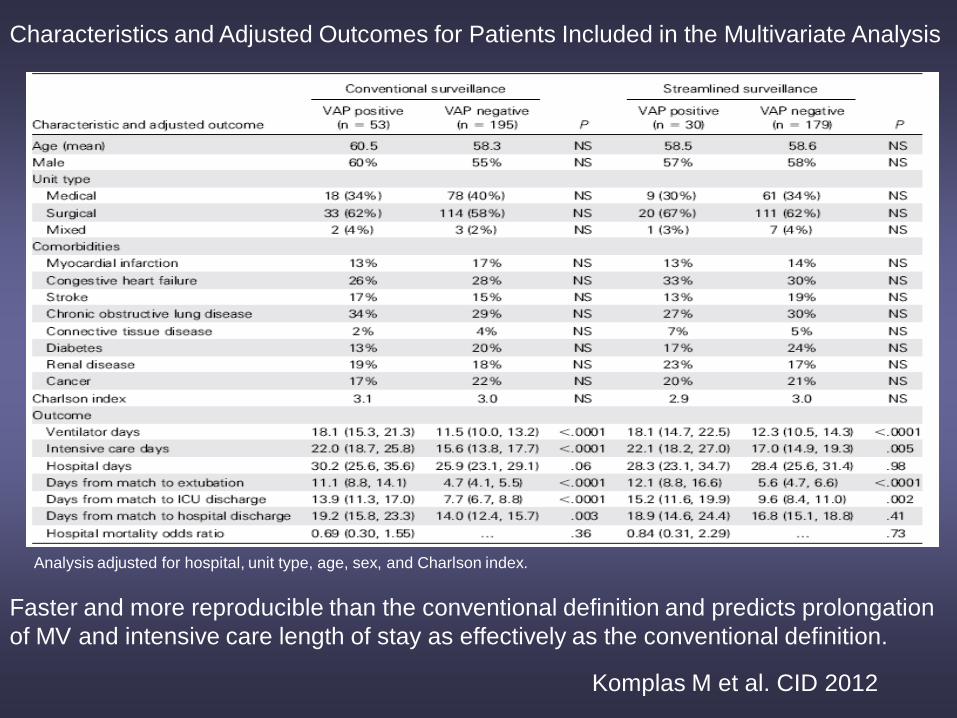
Characteristics and Adjusted Outcomes for Patients Included in the Multivariate Analysis
Analysis adjusted for hospital, unit type, age, sex, and Charlson index.
Komplas M et al. CID 2012
Faster and more reproducible than the conventional definition and predicts prolongation
of MV and intensive care length of stay as effectively as the conventional definition.
VAC
• The streamlined definition uses similar clinical criteria to the
conventional definition and therefore is likely equally prone to
mislabel VAP
• It might make more sense to focus surveillance and benchmarking
on the syndrome of ventilator-associated complications in general
rather than on pneumonia in particular
• Efforts focused on creating a new outcome measure for
mechanically ventilated patients that captures ventilator associated,
pneumonia-like events in a way that is reliable, objective, clinically
meaningful, and straightforward.
Komplas M et al. CID 2012
VAC
• We retrospectively assessed patients on mechanical
ventilation for ≥48 hours in our study ICU
• VAC was defined as a sustained increase in ventilator
settings after a period of stable or decreasing ventilator
support. Subjective measures such as radiographic
interpretations are not part of this definition
• Using electronic medical record data. We analyzed the
association between VAC and clinical diagnoses, ICU
length of stay, duration of mechanical ventilation,
antibiotic use, and mortality.
Hayashi Y et al. CID 2013
VAC-DEFINITION
• “≥2 days of stable or decreasing daily
minimum PEEP or FiO2 followed by a rise
in daily minimum PEEP by ≥2.5 cm H2O
lasting ≥2 days or a rise in daily minimum
FiO2 by ≥15% lasting ≥2 days”
Komplas M et al. PLoS One 2011
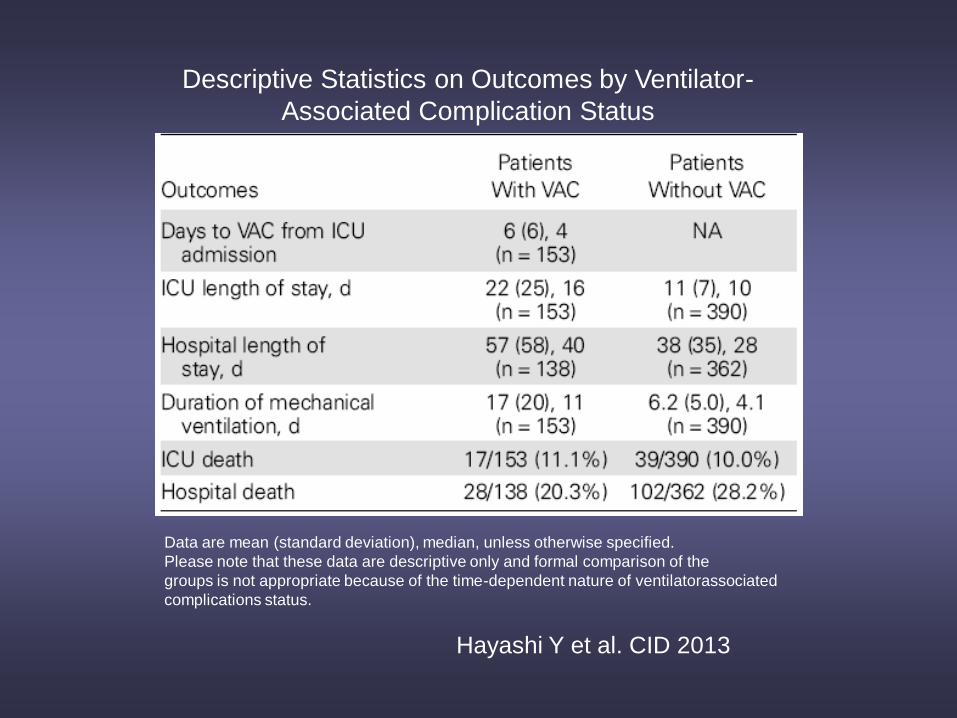
Descriptive Statistics on Outcomes by Ventilator-
Associated Complication Status
Data are mean (standard deviation), median, unless otherwise specified.
Please note that these data are descriptive only and formal comparison of the
groups is not appropriate because of the time-dependent nature of ventilatorassociated
complications status.
Hayashi Y et al. CID 2013
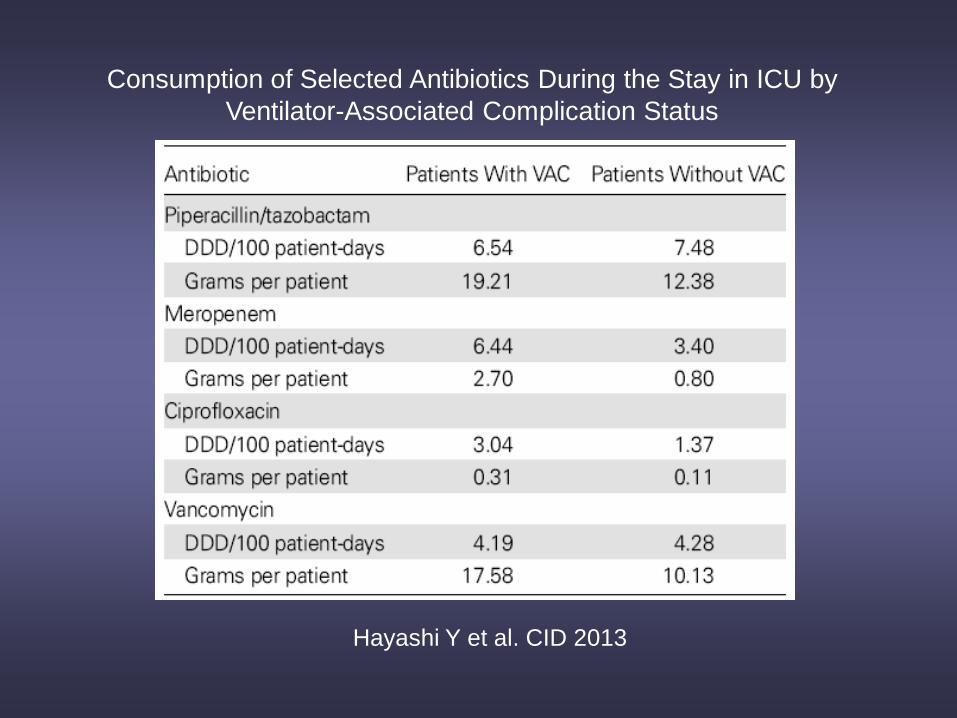
Consumption of Selected Antibiotics During the Stay in ICU by
Ventilator-Associated Complication Status
Hayashi Y et al. CID 2013
• VAC events were due to:
- “Potential VAP”
(VAC with positive culture of respiratory pathogens in respiratory
specimens plus antibiotic prescription with intention to
treat as VAP by intensivist) in 30.7%
- Atelectasis in 16.3%
- Acute pulmonary edema in 11.8%
- ARDS in 6.5%.
• VAC events were associated with significantly increased ICU length of stay, duration of mechanical ventilation, and consumption of broad-spectrum antibiotics but not with longer hospital stays or ICU mortality.
Hayashi Y et al. CID 2013
VAC
• We believe that VAC is a more suitable surveillance
target in patients on mechanical ventilation than VAP
We support calls for improved diagnostic methods (such
as the use of pneumonia specific biomarkers) for VAP
Hayashi Y et al. CID 2013
Validation of a novel high multiplexing real-time
PCR array for the identification of key pathogens
causative of VAP and their associated R genes
• Rapid diagnosis and appropriate empirical antimicrobial therapy is of pivotal importance for the
clinical outcome of VAP.
.
• The Real-time Array PCR for Infectious Diseases (RAP-ID) is a novel technology that combines
multiplex PCR with real-time microarray detection. The VAPChip is a closed cartridge kit adapted
to the RAP-ID instrument that targets 13 key respiratory pathogens causative of VAP and 24
relevant antimicrobial resistance genes to B-lactams.
• Validation VAPChip was carried out on a collection of 292 genotypically characterized bacterial
reference and clinical isolates (including 67 bacterial isolates belonging to the oropharyngeal flora
not targeted by the array)
• The limit of detection of the assay lies between 10 and 100 genome copies/PCR and the dynamic
range is five orders of magnitude permitting at least semi-quantitative reporting of the results.
• Sensitivity, specificity and negative and positive predictive values ranged from 95.8% to 100% for
species identification and detection of resistance genes.
• Conclusions: VAPChip is a novel diagnostic tool able to identify resistant bacterial isolates by
RAP-ID technology. The results of this analytical validation have to be confirmed on clinical
specimens.
Bogaerts P et al. JAC 2013
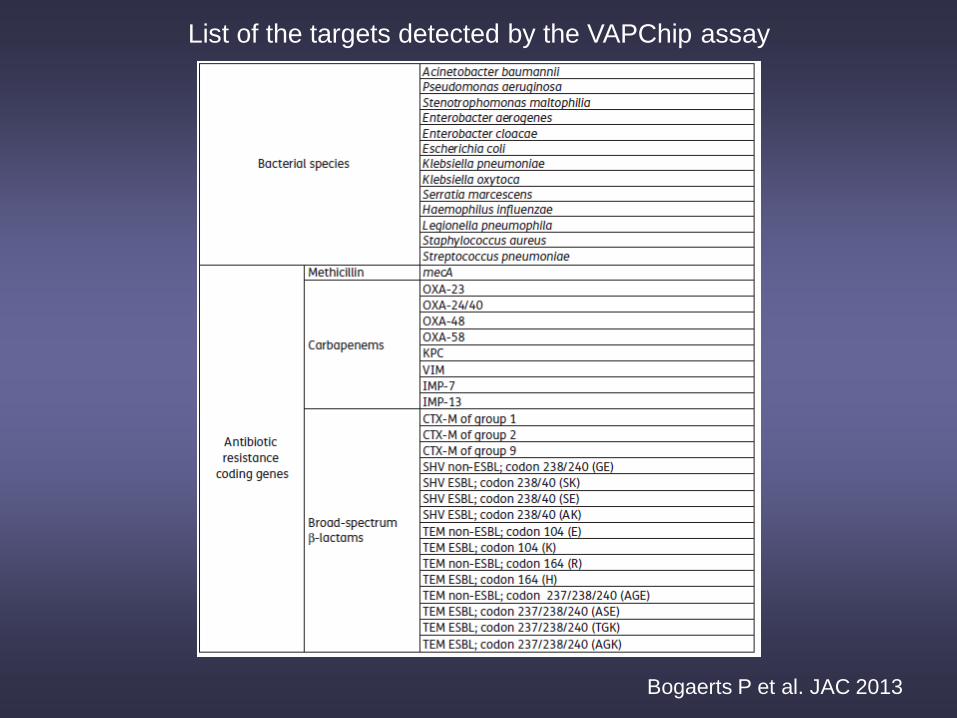
List of the targets detected by the VAPChip assay
Bogaerts P et al. JAC 2013
Repertoire of Intensive Care Unit
Pneumonia Microbiota • To highlight the different compositions of microbiota in
patients with four different types of ICU-pneumonia.
• 185 episodes of ICU pneumonia and 25 control cases.
• Using 16S rDNA gene amplification followed by clone libraries sequencing.They also used specific quantitative PCR. (qPCR) to target fastidious bacteria and a spectrum of viruses.
• Moreover, they tested samples from our patients by standardized routine culture, amoebal co-culture, blood culture, ELISA targeted antibody detection, immunofluorescent assay antigenemia and antigenuria testing as routinely performed in such cases to compare these routine tests with molecular approaches
Bousbia S et al. PLoS ONE 2012
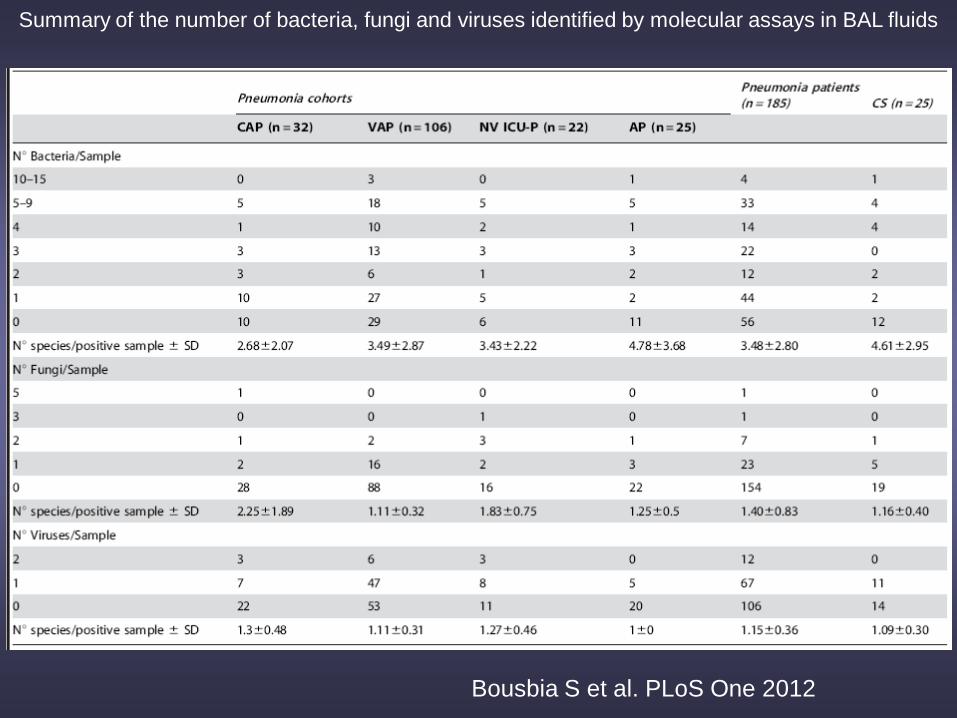
Summary of the number of bacteria, fungi and viruses identified by molecular assays in BAL fluids
Bousbia S et al. PLoS One 2012
Results
• Overall, patients exhibited 146 different species belonging to 7 different phyla (13 classes, 23 orders, 44 families and 71 genera) of which 73 had not been previously observed in BAL from pneumonia, whereas bacterial clone libraries of controls identified 38 species belonging to 4 different phyla (9 classes, 13 orders, 22 families and 27 genera).
• Moreover, 51 strictly anaerobic bacteria (35%) were found in patients versus 17 anaerobic bacteria (44%) found in controls (p=0.26)
Bousbia S et al. PLoS One 2012
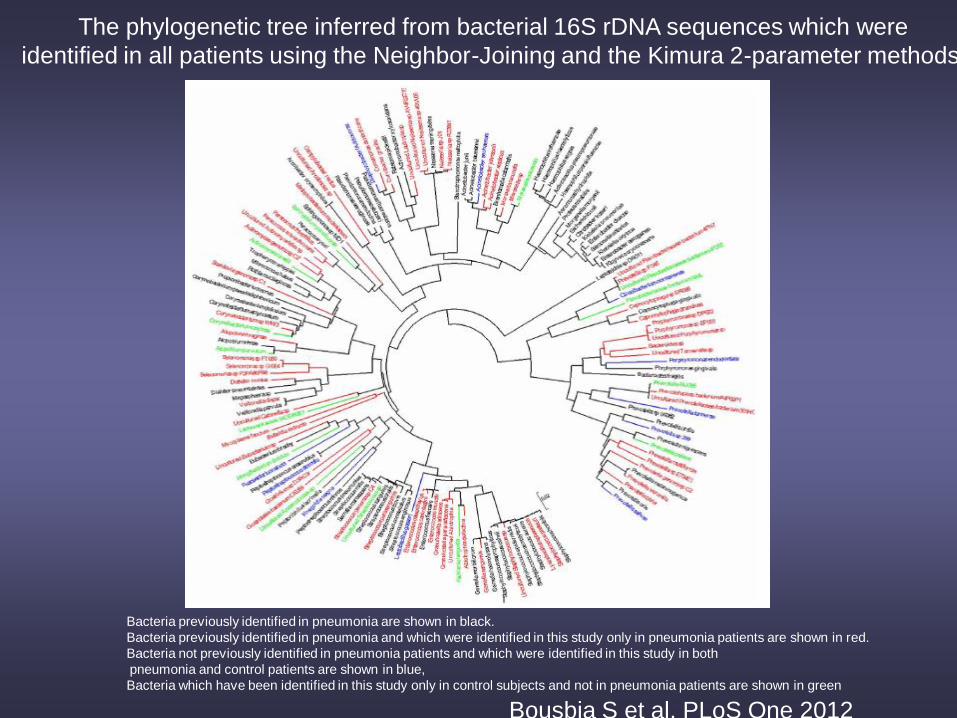
The phylogenetic tree inferred from bacterial 16S rDNA sequences which were
identified in all patients using the Neighbor-Joining and the Kimura 2-parameter methods.
Bacteria previously identified in pneumonia are shown in black.
Bacteria previously identified in pneumonia and which were identified in this study only in pneumonia patients are shown in red.
Bacteria not previously identified in pneumonia patients and which were identified in this study in both
pneumonia and control patients are shown in blue,
Bacteria which have been identified in this study only in control subjects and not in pneumonia patients are shown in green
Bousbia S et al. PLoS One 2012
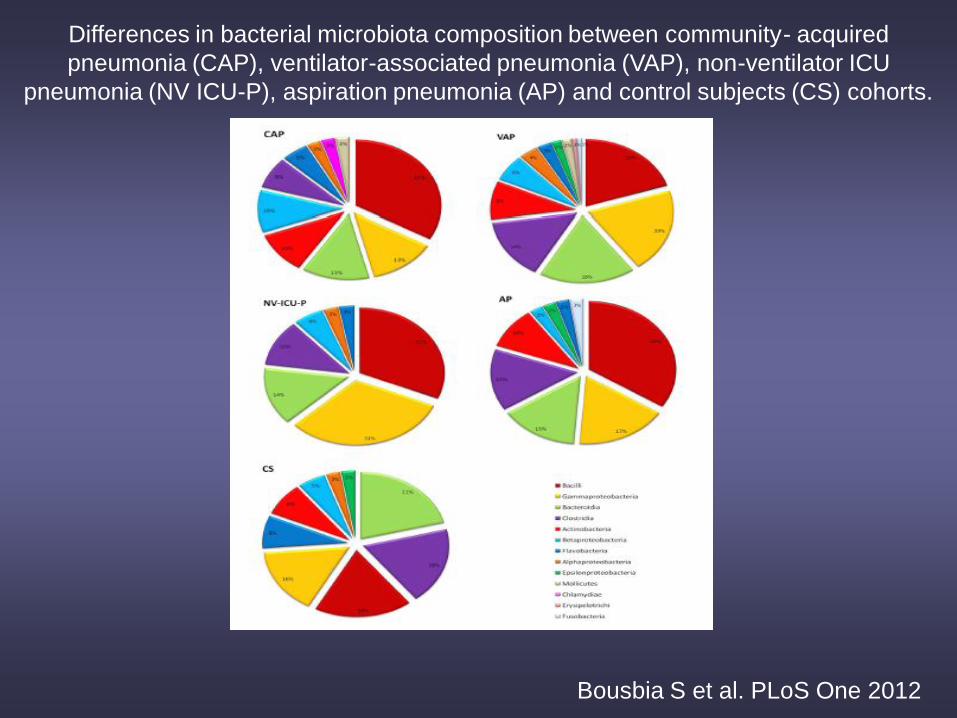
Differences in bacterial microbiota composition between community- acquired
pneumonia (CAP), ventilator-associated pneumonia (VAP), non-ventilator ICU
pneumonia (NV ICU-P), aspiration pneumonia (AP) and control subjects (CS) cohorts.
Bousbia S et al. PLoS One 2012
• Our results demonstrate that nearly 50%
of the microbial species found had not
been previously reported in lung samples
from pneumonia.
• Therefore, the composition of ICU-
pneumonia microbiota is more complex,
more extensive and more diverse than
originally expected.
Bousbia S et al. PLoS One 2012
Conclusions
• Diagnosis of VAP and its etiology is essential if we are to rationalise its management
• None of the available diagnostic tests, performed alone, can provide an accurate diagnosis of VAP.
• A diagnostic strategy incorporating several criteria seems to be a good compromise.
• Further evaluation by imaging procedures, microbiological cultures, and pneumonia specific biomarkers to refine the probability of diagnosing VAP
- Limiting the definition to objective and quantifiable components.
- Systematic use of microbiological methods
- Non-invasive vs. Invasive techniques
- Systematic use of quantitative techniques
- Explore other image diagnostic modalities
• Incorporate rapid, molecular quantitative diagnostics
• VAC is a good tool for surveillance purposes but is not going to improve our diagnostic ability of VAP